
Pectoral muscle segmentation: A review
10
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 j o ur nal homep age : w ww.intl.elsevierhealth.com/journals/cmpb Pectoral muscle segmentation: A review Karthikeyan Ganesan a,∗ , U. Rajendra Acharya a,b , Kuang Chua Chua a , Lim Choo Min a , K. Thomas Abraham c a Department of ECE, Ngee Ann Polytechnic, Singapore 599489, Singapore b Department of Biomedical Engineering, Faculty of Engineering, University of Malaya, Malaysia c Singapore Anti Tuberculosis Association (SATA) CommHealth, Singapore a r t i c l e i n f o Article history: Received 16 February 2012 Accepted 30 October 2012 Keywords: Breast cancer Pectoral muscle segmentation Digital mammography Automated techniques Computer-aided diagnosis a b s t r a c t Mammograms are X-ray images of breasts which are used to detect breast cancer. The pec- toral muscle is a mass of tissue on which the breast rests. During routine mammographic screenings, in Medio-Lateral Oblique (MLO) views, the pectoral muscle turns up in the mam- mograms along with the breast tissues. The pectoral muscle has to be segmented from the mammogram for an effective automated Computer Aided Diagnosis (CAD). This is due to the fact that pectoral muscles have pixel intensities and texture similar to that of breast tissues which can result in awry CAD results. As a result, a lot of effort has been put into the segmentation of pectoral muscles and finding its contour with the breast tissues. To the best of our knowledge, currently there is no definitive literature available which provides a comprehensive review about the current state of research in this area of pectoral muscle segmentation. We try to address this shortcoming by providing a comprehensive review of research papers in this area. A conscious effort has been made to avoid deviating into the area of automated breast cancer detection. © 2012 Elsevier Ireland Ltd. All rights reserved. 1. Introduction X-ray mammography is a widely used method to screen women for early detection of breast cancer. A large number of mammograms generated each year calls for an accurate and fast interpretation of the images. Two major factors which affect mammographic screening are the radiologist’s level of expertise and the high volume of cases examined in a screening programme. Double reading on screening data could improve accuracy, but manpower limitations and a high level of intra-observer variability restricts its deployment. Computerized mammographic image analysis can improve both speed and accuracy apart from avoiding intra-observer discrepancies. One of the main obstacles in computerized mammographic image analysis is the presence of pectoral ∗ Corresponding author. E-mail address: [email protected] (K. Ganesan). muscles in the mammograms. The pectoral muscle is a visibly dominant region in most medio-lateral oblique (MLO) views of mammograms. The success of CAD techniques depend on an accurate differentiation between the pectoral muscle and breast tissue mass [7]. Locating the pectoral muscle in a mammogram is also use- ful in obtaining local information from its edge. An internal analysis of this region can be used to detect the presence of abnormal axillary lymph which is an indicator of the manifes- tation of occult breast carcinoma [1]. It has also been identified that the area overlying the pectoral muscle is a common loca- tion for cancers to develop and is particularly checked by radiologists to reduce false negatives. It is therefore necessary to segment out the pectoral muscle before lesion detection [2]. One of the main reasons for trying to identify and remove the pectoral muscle is to reduce error and computational 0169-2607/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.cmpb.2012.10.020
Transcript of Pectoral muscle segmentation: A review

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57
j o ur nal homep age : w ww.int l .e lsev ierhea l th .com/ journa ls /cmpb
Pectoral muscle segmentation: A review
Karthikeyan Ganesana,∗, U. Rajendra Acharyaa,b, Kuang Chua Chuaa,Lim Choo Mina, K. Thomas Abrahamc
a Department of ECE, Ngee Ann Polytechnic, Singapore 599489, Singaporeb Department of Biomedical Engineering, Faculty of Engineering, University of Malaya, Malaysiac Singapore Anti Tuberculosis Association (SATA) CommHealth, Singapore
a r t i c l e i n f o
Article history:
Received 16 February 2012
Accepted 30 October 2012
Keywords:
Breast cancer
Pectoral muscle segmentation
Digital mammography
Automated techniques
a b s t r a c t
Mammograms are X-ray images of breasts which are used to detect breast cancer. The pec-
toral muscle is a mass of tissue on which the breast rests. During routine mammographic
screenings, in Medio-Lateral Oblique (MLO) views, the pectoral muscle turns up in the mam-
mograms along with the breast tissues. The pectoral muscle has to be segmented from the
mammogram for an effective automated Computer Aided Diagnosis (CAD). This is due to
the fact that pectoral muscles have pixel intensities and texture similar to that of breast
tissues which can result in awry CAD results. As a result, a lot of effort has been put into
the segmentation of pectoral muscles and finding its contour with the breast tissues. To the
best of our knowledge, currently there is no definitive literature available which provides a
Computer-aided diagnosis comprehensive review about the current state of research in this area of pectoral muscle
segmentation. We try to address this shortcoming by providing a comprehensive review of
research papers in this area. A conscious effort has been made to avoid deviating into the
area of automated breast cancer detection.
radiologists to reduce false negatives. It is therefore necessary
1. Introduction
X-ray mammography is a widely used method to screenwomen for early detection of breast cancer. A large numberof mammograms generated each year calls for an accurateand fast interpretation of the images. Two major factorswhich affect mammographic screening are the radiologist’slevel of expertise and the high volume of cases examined ina screening programme. Double reading on screening datacould improve accuracy, but manpower limitations and ahigh level of intra-observer variability restricts its deployment.Computerized mammographic image analysis can improve
both speed and accuracy apart from avoiding intra-observerdiscrepancies. One of the main obstacles in computerizedmammographic image analysis is the presence of pectoral∗ Corresponding author.E-mail address: [email protected] (K. Ganesan).
0169-2607/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reshttp://dx.doi.org/10.1016/j.cmpb.2012.10.020
© 2012 Elsevier Ireland Ltd. All rights reserved.
muscles in the mammograms. The pectoral muscle is a visiblydominant region in most medio-lateral oblique (MLO) viewsof mammograms. The success of CAD techniques depend onan accurate differentiation between the pectoral muscle andbreast tissue mass [7].
Locating the pectoral muscle in a mammogram is also use-ful in obtaining local information from its edge. An internalanalysis of this region can be used to detect the presence ofabnormal axillary lymph which is an indicator of the manifes-tation of occult breast carcinoma [1]. It has also been identifiedthat the area overlying the pectoral muscle is a common loca-tion for cancers to develop and is particularly checked by
to segment out the pectoral muscle before lesion detection [2].One of the main reasons for trying to identify and remove
the pectoral muscle is to reduce error and computational
erved.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 49
tions
laimgetaac
fttnepbaam
ttmItpwtd
sppofie
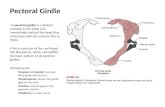
Fig. 1 – MLO and CC projec
oad in the algorithm. Several methods based on a widerray of mathematical theories have been proposed fordentification and removal of pectoral muscle. For pectoral
uscle segmentation, knowledge about the type of mammo-raphic image obtained is very important. A mammographicxam usually consists of four images (Fig. 1) correspondingo each breast scanned in two views- mediolateral (MLO) viewnd craniocaudal (CC) view. The MLO projection is taken underpproximately 450 angle and shows part of the pectoral mus-le. The CC projection is a top-down view of the breast.
A major issue in segmenting the pectoral muscle arisesrom the fact that the density and texture information ofhe pectoral muscle is almost similar to that of the breastissues. As a result of this, pixel based segmentation tech-iques [48,51,61] and techniques based on curvature of thedge of the pectoral muscles [45,50,52,54] are not sufficient torovide accurate results for a wide range of datasets. Waveletased segmentation techniques [47,68], active contour basedpproaches [59,62,63,70] and model based algorithms [56] havelso been tried for the segmenting pectoral muscles fromammographic images.It is quite evident from the listed literature that extrac-
ion of pectoral muscle is not a trivial task. It is extremelyricky given the fact that the delineation between the pectoral
uscle and breast tissue is not evident in most cases [10,12].n some cases, it is also noticed that the pectoral muscle isotally absent. This random variability in the position of theectoral muscle combined with its similarity to breast tissuesith respect to its density makes its segmentation an arduous
ask [55]. As a result of these complications, many techniquesiscussed in literature are not totally automatic.
Several authors assumed the pectoral muscle to be atraight line [8,9] while some require an initial guess for theosition of the contour. In reality, the margin between theectoral muscle and breast tissues is either concave, convex
r a mixture of both. Moreover, the variation of the marginrom one mammogram to another becomes so complex thatt cannot be generalized with any single geometrical or math-matical model [51].of a left and right breast.
Wok et al., approximated the contour between breast tis-sues and the pectoral muscle as a straight line and used Houghtransform to find the contour [46]. This approximation seemedto produce a generally acceptable result. But, it must be notedthat a few assumptions were made about the pectoral muscle:the muscle is located in the top left quarter of the image, thestraight line estimating the muscle edge intersects the top andleft edges of the image inside the breast region and the inten-sity of the muscle is generally higher than that of the adjoiningparenchyma. These assumptions are not isolated and can beseen in several other works which estimate the contour usinga straight line approximation [2,51].
The rest of the paper is arranged in the following order: abrief introduction to breast cancer screening; intensity basedapproaches for pectoral muscle segmentation; line detec-tion techniques for pectoral muscle segmentation; statisticaltechniques for pectoral muscle segmentation; wavelet basedsegmentation techniques; other advanced techniques andconclusion.
2. Breast cancer screening
2.1. Introduction
Breast cancer is the most commonly diagnosed cancer inwomen. The lifetime probability of a woman developing breastcancer is one in 8.9 and the lifetime probability of death due tocancer is one in 26.8 [3]. Early detection of cancer gives a highrate of survival. Localized cancer detection can lead to a sur-vival rate of 97.5% over a 5-year period, whilst cancer whichhas spread to distant organs lead to a survival rate of just 20.4%[3]. Mammographic screening is the most popular method atpresent for breast cancer detection. Mammographic imagesprovide adequate evidence of abnormality including extrane-
ous masses and calcifications apart from subtle signs such asbilateral asymmetry and architectural distortions. [4]. But ahigh level of dependence on human examination of mammo-graphic images leads to an unprecedented amount of false
m s i n
50 c o m p u t e r m e t h o d s a n d p r o g r ainterpretations. A study gives an estimate for the sensitivityof screening mammography at 85–90% [5]. Misinterpretationof breast cancer signs accounted for 52% of the errors and over-looking signs accounted for 43% of missed abnormalities. In acomparative study made by Blanks et al. [6], double reading ofmammograms was found to provide greater sensitivity thansingle reading without increasing recall rates. But a glaringproblem in this method is the requirement of a huge amountof skilled man power which is rare and expensive in mostplaces [42,43,49].
3. Intensity based approaches for pectoralmuscle segmentation
Intensity based segmentation methods depend on the inten-sity differences between breast tissues and the pectoralmuscle. These techniques can be highly affected by the factthat the intensity changes between pectoral muscle and breasttissues are generally negligible. This results in a highly incon-sistent segmentation result when intensity based techniquesare used for segmentation of pectoral muscles. Nevertheless,several researchers have tried to utilize different techniquesto attain a sufficiently good segmentation with intensity fea-tures [46,48,51]. Apart from pure intensity based approaches,histogram based approaches followed by other stages ofprocessing are discussed [14–16].
Every intensity based method works on the assumptionthat the grayscale intensity of the pectoral muscle could behigher than its surrounding tissues [24,28,33]. This is one of thereasons that different studies present varying rates of successwith intensity based segmentation techniques. Saltanat et al.[51], used pixel mapping of the form shown in (1) to map exist-ing pixel values in an exponential scale. After this mapping, aspecialized thresholding algorithm was developed for regionextraction. The result of this process was a mapped image inwhich brighter regions were enhanced further resulting in theimage being divided into regions with enhanced contrast.
I′(x, y) = eI(x,y)
x(1)
In (1), x had a value of 40. From our experimentation, it wasseen that we get a varying value of the mapped image forvarying values of x. It can be deduced that the best value ofx can be varied according to the set of images in hand. Oncethe regions have been exponentially mapped, thresholdingand region growing operations can be performed more effec-tively with lesser overflow of regions. A method for pectoralmuscle extraction based on watershed transformation wasdiscussed in [58]. In this technique, watershed transforma-tion (WaT) was applied on the gradient of a mammogram andwatershed regions were extracted. The reason for applyingWaT on gradient images was that catchment basin boundariescan effectively be located at higher gradient points than theoriginal image itself [11]. A smoothing operation on this trans-
formed image and a merging algorithm was further carried outto extract pectoral muscles.Roshan et al. [61], discussed a connected component label-ing algorithm to identify contour tracing. This algorithm
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57
works by grouping components from pixel values within a par-ticular threshold into a same class. Though this componentlabeling algorithm was designed for general contour tracing,applications for mammograms were provided as an examplewith promising results. A simple seeded region growing withmorphological operations has been used with good effect byNagi et al. in [65]. This method of region growing is based onpixel intensities that follows the general mathematical nota-tion of a region growing operation as seen in (2). A set of rulesfor merging these segmented regions into groups or classeswas further devised to segment out regions of interests (ROI).
T = {x /∈ Uni=1Ai|N(x) ∩ Uni=1Ai /= ∅} (2)
where T is the set of as-yet unallocated pixels which bordersone of the regions described in (2). N(x) is the set of immediateneighbours of the pixel x in consideration. Ai is the startingseed and n is the total number of seeds.
Very simple histogram based thresholding techniquesalong with morphological operations has been used in [13].Pectoral muscle removal was part of a larger process and themethodology used by the authors seems to provide quite a sat-isfactory result. David et al.[67], used a simple region growingtechnique with limitations to the size of the region of interest.This region was obtained from an initial seed point and thenrefined by using morphological operators.
Along with intensities, gradients have also been exten-sively used to find the line of separation of the pectoral muscle[17,18]. The work done in [18] combines the advantages ofa multiresolution scheme along with the intensity gradienttechniques. A global thresholding technique acts as a key toits initial results followed by a sobel operation based gradientoperation. Similary, [17] uses a two-level histogram thresholdto obtain the breast region and this region was then used totrack the boundary of the pectoral muscle and the breast usingthe gradient.
4. Line detection techniques for pectoralmuscle segmentation
Line detection techniques have been popularly used for pec-toral muscle segmentation. This is due to the fact that pectoralmuscle boundaries have been assumed by some authors to bea straight line as described in Section 1. Karssemeijer [8] wasone of the first authors to report the findings using a straightline approximation of the pectoral muscle. A Hough transformwas used to find the peak in Hough space with the correctgradient magnitude and orientation, length of projected lineand corresponding pectoral area. The general representationof a straight line for the Hough Transform computation [52] isspecified as:
� = (x − xo) cos � + (y − yo) sin � (3)
where (xo, yo) is the origin of the coordinate system of theimage located at the center of the image, and � and � repre-sent, respectively, the distance and angle between (xo, yo) andthe coordinates (x, y) of the pixel being analyzed.

s i n
laast
toglafiedbb
pwtr
R
wim
mbtridpeot[uAcaWw
5i
BcUduofma
c o m p u t e r m e t h o d s a n d p r o g r a m
Yam et al. [9], used the Hough transform too, but refined theinear approximation into a curved pectoral boundary using
dynamic programming method. Though Hough transformnd linear approximation have been claimed to be good in alltated works, there is no conclusive validation done in any ofhe works.
Kwok et al. [53], used a linear approximation to find the pec-oral edge too, but followed it with a refinement process basedn cliff detection. Cliff detection is a heuristic dynamic pro-ramming methodology in which the linearly approximatedine is iteratively refined into a curved path using a searchlgorithm.This process is iteratively carried out until the besttting curve is obtained. Cliff detection is used for pectoraldges since they ignore intensity rise and detect intensityrops only. It is also claimed to be more robust to noise andright spots on the image, thereby giving fewer scattered androken edges [53].
In all methods which assume a linear approximation of theectoral muscle, it is seen that the region of interest (ROI) inhich the pectoral muscle is assumed to be present is taken as
he top left quarter of the image which can be mathematicallyepresented by relation (4).
i = {(x, y) : 0 ≤ x < nx/2, 0 ≤ y < ny/2} (4)
here nx and ny are the size of the x and y coordinates of themage and Ri is the region of interest (ROI) in which the pectoral
uscle is assumed to be present.Weidong et al. [54], used a polyline fitting algorithm to
odify a linear approximation to fit the pectoral edges in aetter way. Hough transform was used for identification ofhe straight lines in conjunction with an elastic thread algo-ithm for extraction of the pectoral muscle. Elastic threads a method used to fit low-curvature curves. This methodepends on the gradient of the line along with a compactnessarameter. The compactness parameter, also referred to aslasticity, depends on the difference between the magnitudef gradient of the image and an exponential function based onhe distance between the current point and the initial point.54]. A high precision is claimed to be obtained because of thesage of these two techniques in conjunction with each other.n optimal threshold curve and local mean square deviationurve was calculated to attain the segmentation thresholdccording to the gray-level distribution of the mammogram.ith this, the Hough transform and elastic thread calculationsere accomplished.
. Statistical techniques for pectoral muscledentification
reast structures have been studied according to differentategories based on their texture, appearance and densities.sing this information, several statistical parameters can beeduced and inferred. Breast density patterns are classifiedsing several techniques [19–21]. A majority of these meth-
ds depend on statistical classification of the pixel intensitiesound in mammograms. Approaching the problem of pectoraluscle identification in a similar direction, authors have beenble to statistically identify this muscle region in an effective
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 51
manner [15,20]. For instance, [15] used skewness and fractaldimensions to classify breast densities. Though this was per-formed with a focus on tumor classification, it can easily beextended to pectoral muscle delineation. Peter and Sue [20],have used texture-based discrimination between fatty anddense breast types using granulometric techniques and tex-ture masks. The difference in density between pectoral muscleand breast tissues can be used for segmentation using statis-tical techniques.
One of the methods in literature which has used proper-ties of densities and texture to identify the pectoral boundaryis described in [45]. In this technique, the end points of thepectoral muscle is identified by using Support Vector Regres-sion (SVR). Once the end points are detected, the boundaryof the pectoral muscle is detected by finding the shortestpath between these end points. This algorithm was devel-oped based on a graph theory approach and is explained inAlgorthm1 [45].
The weighted graph is calculated by considering the pixelsas nodes and edges connecting adjacent pixels as arcs. Theweight of the edge connecting adjacent pixels is calculatedusing (5). Using this, the weights of every connecting pixel iscalculated and the shortest distance between the end pointsis obtained.
f̂ (g) = fl + (fh − fl)exp(ˇ(255 − g)) − 1exp( ̌ ∗ 255) − 1
(5)
where fl, fh, ̌ ∈ R: 0< ∞and g is the minimum of the gra-dient computed on the two incident pixels. For 8-neighborpixels, the weight is set to
√2 times of the value. fl, fh, ̌ were
experimented with random values and the values of theseparameters were set at 2, 32 and 0.025 respectively.
The path bewteen two end points v and u is consideredto the shortest when the total cost between the two of themis the least among all v-to-u paths. The distance between asource vertex v and target vertex u can be denoted by d(v, u).All possible paths from v to u can be denoted as sub-graphs� . The distance from the node v to a sub-graph �, d(v, �), isthe total cost of the shortest path between v and �.
d(v, �) = min d(v, u) ; u ∈ � (6)
Algorithms such as the Dijkstra algorithm [26] can be usedto solve and optimize the shortest path problem arising indeducing the best path between two adjacent points. But, adrawback with this method might be that the search mightresult in a false short path at the edges of the image whenthe search approaches the borders. To overcome this problem,[27], proposed to convert the image into polar coordinates atthe initial stages of processing. Rest of the search algorithm inthis technique follows the method described in [45].
Algorithm 1. Pectoral Boundary detection using SVRStep 1: Compute endpoints of the contour using SVR models.Step 2: If either of the endpoints is outside the range of the
image, stop process.
Step 3: Compute the weighted graph using (4).Step 4: Compute muscle contour as the shortest distancebetween the end points.

m s i n
52 c o m p u t e r m e t h o d s a n d p r o g r aApart from SVR based methods, [22] described two imagesegmentation methods based on adaptive pyramids andminimum spanning trees. A method for choosing the longeststraight line in Radon-domain as an approximation to thepectoral muscle localization has been discussed in [23]. Agraph cut method using Bezier curve smoothing is discussedin [25]. A discrete Markov chain and an active contour modelwere used for pectoral muscle isolation in [63]. Most of thesetechniques use graph cut methods, considering the pixelsas nodes and arcs as the edges connecting these pixels, asdiscussed in [45].
A technique based on joint normal distribution is discussedin [50]. In this technique, the possibility of a pixel to be in thehigh frequency region is measured. This probability value pro-vides knowledge of the contours of the breast and pectoralmuscles. This value is found using a goodness of fit measureusing the statistical features of pixel distribution of the image.In this method, the distribution of pixels in the mammogramis modeled as a poisson distribution and the goodness of fit ofthe test image to the modeled poisson distribution is studied.Based on the likelihood values, the pixels are classified intoeither of the two classes- breast or pectoral muscle. The char-acteristic homogeneity of pectoral muscles when compared tobreast tissues is put to good use in the goodness of fit measure.
In [29], an isocontour map was formed to make a topolog-ical analysis of image intensities. [30] uses a morphologicalapproach for delineating the pectoral muscle. Log-likelihoodimages are constructed by analyzing the local texture of mam-mograms in [31]. A registration based multi-atlas algorithm isdiscussed in [32]. This technique estimates the pectoral regionby registering pre-annotated database and a target image.
6. Wavelet based segmentation technique
Wavelets have been used for a wide range of image processingtechniques for a long time. Due to its similarity to short-term fourier transform, wavelets have been widely used topin pointing the frequency and its spatial occurrence in animage. Wavelet based segmentation methods have been usedto extract features from mammograms due to its in-builtability to obtain spatial frequency information from images[16,20,36,60]. Dyadic wavelet decomposition has been used forpectoral muscle detection [34]. In this work, the importance ofdecomposition levels has been discussed in detail. Decompo-sition of images using wavelets can be performed at differentlevels based on the size of the object of interest. For instance,location of larger objects such as the pectoral muscles canbe obtained at a higher level of decomposition compared tomicrocalcifications [47].
Ferrari et al. have presented a Gabor wavelet filter bank forenhancing the pectoral muscle edge, using ROI containing thepectoral muscle [52]. Wavelet filters were used to detect pec-toral muscle by knowing the approximate angle of the muscle[52]. True pectoral muscle edges were then detected by a sepa-rate post-processing method. This was carried out by selecting
valid lines of pectoral muscle boundary detected by checkingfor specific threshold values.Mustra et al. [47] used a hybrid method using contourdetection and wavelet decomposition to detect the pectoral
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57
muscle. In this method, a Sobel filter was used to find theedges in the fourth level dyadic wavelet decomposed image.A smoothened curve was drawn on this image to segment thepectoral muscle. In this way, segmented pectoral muscle caneasily be removed. A fourth level decomposition is used in thismethod since it preserves enough rough details while at thesame time does a very good job in removing fine details likenoise and granulation. A biorthogonal spline wavelet is usedin this work.
Ferrari et al. [52], have described a hybrid method to obtainthe delineation of pectoral muscle using Gabor wavelets andpectoral edge using Hough transform. Before this process,the ROI is extracted according to the following geometric andanatomical constraints:
(1) The pectoral muscle is considered to be a straight linelimited to an angle (�) between 1200 and 1700 withrespect to the lower right corner of the rectangular region-of-interest box obtained using Eq. (4). As always, allmammograms are oriented in such a way that the pectoralmuscles are always located on the top left of the image.
(2) After low-pass filtering by convolution with a Gaussiankernel, the pectoral muscle appears on mammograms as adense region with nearly homogeneous gray-level values.
The above constraints are not limited to [52], but used in amajority of other works which use geometrical and anatom-ical constraints for extraction of the ROI with respect topectoral muscles.
Enhancement of directional and piecewise-linear struc-tures was obtained using the Gabor filter technique describedin [35,37,52]. The combination of magnitude and phase fromdifferent levels of wavelet decompositions holds the key tothis. A Gabor filter in frequency domain can be represented as[52]:
(u, v) = 12��u�v
exp
{− 1
2
[((u − W)2
�2u
+ v2
�2v
]}, for (u, v) /= (0, 0)
= 0, for (u, v) = (0, 0)(7)
where �u = 1/(2��x) and �v = 1/(2��y) with � representing thevariance along the direction specified. The wavelet designstrategy used here is in such a way that the filters capturemaximum information with minimum redundancy.
An advantage of using wavelet decomposition for pectoralmuscle identification is that an exact reconstruction of theimage is not needed. Instead, the pectoral edge informationgiven by the wavelet decomposition is sufficient. As a result,instead of using wavelet coefficients, the magnitude of the fil-ter response was used [52]. An edge flow algorithm proposedby [69] was used to detect relevant edges from the waveletdecomposed (WD) images. The phase and magnitude of theWD images were used to represent the edge-flow vector. Adetailed description of this method can be found in [69].
A fractal analysis of mammograms has been discussed byGeorgsson et al. [38] and Qi Guo et al. [39]. In both the afore-mentioned studies, different tissues in mammograms havebeen differentiated with a considerable accuracy by using

s i n
flutf
bgfwttviHHiQitu
7i
Accclp[btf[mTetct
wi
E
wef
E
wtrp
c o m p u t e r m e t h o d s a n d p r o g r a m
ractal geometry and fractal analysis. In these methods, theacunarity of the fractals have been successfully studied andsed in the segmentation of different mammographic struc-ures. Support Vector Machines (SVMs) coupled with fractaleatures have been used for automated classification [39].
Image features such as edge and ridges of the breasts haveeen successfully extracted in multiple scales using mono-enic signals [68]. Local phase information derived from theseeatures were used to extract structural information. Alongith the orientation information simultaneously computed,
he pectoral muscle lining can be extracted. The strength ofhis algorithm lies in the fact that the local phase does notary much in contrast. As a result, there is not much variabil-ty observed with respect to various datasets. In this method,ilbert transform was used to extract multiple scales. Thoughilbert transform is used in a 1D case, the Riesz transform
s used to extend it to 2D or an arbitrarily higher dimension.uadrature filters are used to derive local amplitude and phase
nformation at multiple scales. Phase and amplitude informa-ion in conjunction with each other is found to provide annique value for pectoral muscle boundaries [68].
. Other techniques for pectoral muscledentification
part from the techniques described in Sections 4– 7, dis-usses other techniques which cannot be grouped under aommon category due to their specialized nature. An activeontour based segmentation methods evolved from Sethian’sevel set approach [40], though widely used in several imagerocessing techniques including color image segmentation
41], were also used in the segmentation of pectoral muscleorders. This is due to the fact that the gradient informa-ion required to compute the velocity function for level setunctions is very poor in mammograms. But, a few authors59,62,63,70] have attempted to use active contour based seg-
entation to extract border information from mammograms.hough these works have exclusively been performed toxtract different breast regions on a broad scale, it is never-heless a direction towards extraction of pectoral muscle. Itan be seen from the literature discussed above that theseechniques can well be used towards this area of research.
Active contour methods are based on a level set approachhich involves minimization of the energy function Etot seen
n (9) [40].
tot = Eint + Eext + Eim (8)
here Etot is the total energy of the contour, Eint is the internalnergy, Eext the external energy and Eim the energy derivedrom the image.
tot =∫ 1
0
{12
[˛|�′(s)|2 + ˇ|�′′(s)|2 + Eext[�(s)]]}ds (9)
here ̨ and ̌ are weighting parameters that control respec-ively the tension and rigidity of the snake. Tension andigidity refers to the elasticity and the shape maintainingarameters of the active contour. �′(s) and �′′(s) denote the
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 53
first and second derivatives of the contour. A snake basedrepresentation as seen in (9) consists of an internal term,external term and an image term respectively. The internalterm (v′(s), v′′(s)) is the property of the evolving contour itselfwhich depends on its smoothness along the curve and itsability to stretch and bend. The external term (˛, ˇ) is a userdefined constraint and can be obtained from prior knowledgeof the structure to be recovered. Image term (Eext) is obtaineddirectly from the image.
Eim(x, y) = −||∇I(x, y)||2 (10)
where ∇ is the gradient operator. ̨ and ̌ are experimentallycalculated and the best value is set according to the problemin hand.
One of the main goals of using active contour based tech-niques is for limiting the region of interest in which CAD hasto be performed. Most methods found in literature are basedon combining histogram thresholding techniques along withmore elaborate techniques discussed in previous sections. In[59], contour growing was proposed based on a seed pointselected from a scale-space edge detected image. This seedpoint is detected based on the gradient magnitude of this edgedetected image. In [62], a deformable active contour model isdemonstrated for identification of the breast boundary. This iscarried out using the minimization of energy described in (8)and (9). Gradient information from the mammograms is usedin order to obtain Eim and inherent properties of the activecontour along with the external image information is used incalculation of Eint and Eext.
Wang et al [63] have identified the pectoral muscle bound-ary by adopting the technique proposed in [52] along withactive contour method. In this work, a method based on dis-crete time Markov chain (DTMC) and an active contour modelis used to automatically detect the pectoral muscle boundary.DTMC is used to model the continuity and uncertainty of thepectoral muscle. This can be used to obtain a rough boundaryof the pectoral muscle. Once a rough boundary is obtained, anactive contour model is applied to refine the detection results[63].
Markov processes are relatively simple statistical tech-niques, in which the future occurrences of events depend onlyon the immediate past and the values prior to them do notaffect the results. A mathematical definition of the same canbe seen in (11) [63].
p(n−1)(n)ij
= P(Xn = j|Xn−1 = i) (11)
where n ∈ I, i, j ∈S, Xn represents a random variable at time n.From (11), n-step transition probabilities can be easily derivedby considering the previous time step probability given by (11)and the current time step probability. Once an initial end pointof the pectoral muscle is detected, DTMC is used to identify arough estimate of the pectoral edge line using intensity infor-mation of the image. This is described in detail in [63].
The calculation of DTMC is performed after the extraction
of ROI using (4). The rough muscle edge obtained using theabove technique is refined to get a smoother edge by usingactive contours as described in (8) and (9). The method usedby Wang et al. [63] is very similar to the one used by Ferrari et al.
54 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57
Table 1 – Listing of major methods and results obtained.
Authors Method used Feature used Results obtained (in %)
Sultana et al. [48] Mean-shift 84Saltanat et al. [51] Intensity based methods Pixel value based mapping 92Camilus et al. [58] Watershed transformation 99Kwok et al. [46] Iterative cliff detection 84Kwok et al. [2] Line detection Cliff detection 94.5Weidong et al. [54] Polyline fitting and elastic thread 95Marina et al. [63] Statistical techniques Multi-image Bayesian causal independence 87Wang et al. [44] Markov chains 91Mustra et al. [47] Wavelet decomposition 85Xiao-Bo et al [52] Wavelet methods Monogenic signals at multiple scales 96.8Ferrari et al [68] Gabor wavelets 93
eneri
Ferrari [62] Active contour Gin [62] and they reported an high accuracy using this method.Smoothened pectoral boundary was reported using a graphtheory approach in [66]. An active contour technique was pro-posed along with this to smoothen a pectoral muscle boundaryobtained using an Adaptive Pyramid (AP) and Minimum Span-ning Tree (MST) algorithm. Comparatively good results wereobtained in this study.
Inclusion tree based boundary detection method has beenused in [29] for mammograms in which intensity contour ofthe pectoral muscle was quasi-concentric. This graph basedapproach is similar to the node-arc theory followed in tradi-tional graph cut methods.
Apart from a single view CAD system, effort has been madeto extend CAD of mammograms to multiple view systems inwhich projections are made from different views to obtain abetter view and in turn a better diagnostic result [44]. In thismethod, multiple views are analyzed simultaneously and thecorrelation among corresponding regions in different viewsare preserved.
This technique is worked out within the framework of aBayesian approach which makes it statistically significant andeasier to validate. The basic idea of this method is to com-pute the likelihood of paired regions on Medio-lateral Oblique(MLO) and Craniocaudal (CC) views. An acyclic directed graph(ADG) was used to compute this likelihood [44]. An ADG isextremely similar to a DTMC, given that both the models areacyclic graphs with causal independence. The dependenciesbetween multiple views of an object are discussed in detail inthe study and their effect and classification accuracy in sep-arating breast tissues from pectoral muscle is also discussed[44].
8. Discussion
In general, there has not been much work with respect topectoral muscle segmentation using intensity based tech-niques. A few works which have been presented basedon this technique do not provide specific segmentationaccuracies in terms of numbers, which makes it quite dif-
ficult to compare different methodologies. So, it can besafe to assume that this technique is not popular amongresearchers working on the problem. The general accuracyfor this technique varies from 84% to 99% proving that therec active contour 99
is wide variability in the success rate using this method.Table 1.
From available literature, it is seem that pectoral muscleedge detection using line estimation techniques are not veryeffective when used in isolation. But, it can become quite con-venient in conjunction with other techniques as seen fromthe discussions in previous sections. Also, an initial guess ofthe pectoral edge using a straight line estimate can be fol-lowed up by a polyline fitting or other methodologies, whichmight give a sufficiently satisfactory result. General accuracyobtained shows quite a wide range as it varies between 84%and 95%.
It is seen that statistical methods have a better chance ofworking on a wide range of images compared to the othertechniques. Also, these methods are proven to be more robustwhen used on a new set of data. Because of very minimalassumptions while working with statistical techniques, theaccuracy and precision rates are usually high with these meth-ods. Wavelet decomposition based segmentation techniquesprovide conclusive evidence about their superiority in provid-ing a solution to the problem of pectoral muscle identification.The accuracy rates using statistical techniques do not havea high variability rate with the values ranging from 87% to91% while the accuracy rates for wavelet decomposition basedtechniques vary from 85% to 93%. While other methods do notwork quite well on an universal level, wavelet based methodsseem to function quite well in all types of datasets as seen fromthe results provided in literature discussed in the relevantsections. Along with wavelets, fractals and multi-scale analy-sis techniques based on Hilbert transform seem to provide areasonably good segmentation result.
Active contour based segmentation of pectoral muscle hasnot really taken off as an active area of research as seen fromthe very few number of literature that is available in the open.But, from the available research results, it is clearly visible thatthe theoretical background of this technique, which has beenapplied vastly to various fields of image processing, has thepotential to be used in pectoral muscle boundary detection.A good backing for this argument can be given by the factthat Ferrari et al. obtained a accuracy rate of 99% [62] usingthis technique. Though the problem of spurious edges and a
local minima would persist, conjunction of the active contourtechnique with other methodologies such as histogram basededge detectors, wavelet decomposition and Markov models
s i n
cd
9
Tipsdsra
dnrwclep
r
c o m p u t e r m e t h o d s a n d p r o g r a m
an provide promising results as seen from the literature andiscussion.
. Conclusion
he discussions seen in the above sections show that theres not one specific method which works perfectly well for theroblem of pectoral muscle segmentation. In most cases, theolution provided is more targeted towards a particular set ofata or a particular problem in hand. There are few genericolutions available for the pectoral muscle detection. As aesult, it is very difficult to quantify the results obtained fromvailable research papers.
Research in Computer Aided Diagnosis (CAD) for automaticetection of breast cancer has been going on for a long timeow. But, from the survey done, it is seen that the number ofesearch papers on the topic of pectoral muscle segmentation,hich is a preliminary step for CAD in detection of breast can-
er is really low. Also, the techniques followed in the availableiterature are very limited and has tremendous scope to bexpanded, wherein several new theories can be applied to theroblem in hand.
e f e r e n c e s
[1] M.J. Homer, Mammographic Interpretation: A PracticalApproach, McGraw-Hill, Boston, MA, 1997.
[2] S.M. Kwok, R. Chandrasekhar, Y. Attikiouzel, M.T. Rickard,Automatic pectoral muscle segmentation on mediolateraloblique view mammograms, IEEE Transactions on MedicalImaging 23 (September (9)) (2004) 1129–1140,doi:10.1109/TMI.2004.830529.
[3] A. Jemal, L.X. Clegg, E. Ward, L.A.G. Ries, X. Wu, P.M. Jamison,P.A. Wingo, H.L. Howe, R.N. Anderson, B.K. Edwards, Annualreport to the nation on the status of cancer, 1975-2001, witha special feature regarding survival, Cancer 101 (1) (2004)3–27.
[4] M.J. Homer, Mammographic Interpretation: A PracticalApproach, second ed., McGraw-Hill, New York, 1997.
[5] R.E. Bird, T.W. Wallace, B.C. Yankaskas, Analysis of cancersmissed at screening mammography, Radiology 184 (3) (1992)613–617.
[6] R.G. Blanks, M.G. Wallis, S.M. Moss, A comparison of cancerdetection rates achieved by breast cancer screeningprogrammes by number of readers, for one and two viewmammography: Results from the UK National HealthService Breast Screening Programme, The Journal of MedicalScreening 5 (4) (1998) 195–201.
[7] S. Ciatto, M.R.D. Turco, G. Risso, S. Catarzi, R. Bonaldi, V.Viterbo, P. Gnutti, B. Guglielmoni, L. Pinelli, A. Pandiscia, F.Navarra, A. Lauria, R. Palmiero, P.L. Indovina, Comparison ofstandard reading and computer aided detection (CAD) on anational proficiency test of screening mammography,European Journal of Radiology 45 (2003) 135–138.
[8] N. Karssemeijer, Automated classification of parenchymalpatterns in mammograms, Physics in Medicine and Biology43 (1998) 365, doi:10.1088/0031-9155/43/2/011.
[9] M. Yam, M. Brady, R. Highnam, C. Behrenbruch, R. English, Y.
Kita, Three-dimensional reconstruction ofmicrocalcification clusters from two mammographic views,IEEE Transactions on Medical Imaging 20 (June (6)) (2001)479–489, doi:10.1109/42.929614.b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 55
[10] Petroudi, S.; Kadir, T.; Brady, M. Automatic classification ofmammographic parenchymal patterns: a statisticalapproach, Engineering in Medicine and Biology Society,2003. Proceedings of the 25th Annual InternationalConference of the IEEE, vol. 1, pp. 798-801, 17–21 September,2003, doi:10.1109/IEMBS.2003.1279885.
[11] V. Grau, A.U.J. Mewes, M. Alcaniz, R. Kikinis, S.K. Warfield,Improved watershed transform for medical imagesegmentation using prior information, IEEE Transactions onMedical Imaging 23 (April (4)) (2004) 447–458,doi:1109/TMI.2004.824224.
[12] L. Vincent, P. Soille, Watersheds in digital spaces: an efficientalgorithm based on immersion simulations, IEEETransactions on Pattern Analysis and Machine Intelligence13 (June (6)) (1991) 583–598, doi:10.1109/34.87344.
[13] K. Thangavel, M. Karnan, Computer aided diagnosis indigital mammograms: detection of Microcalcifications bymeta heuristis algorithms, ICGST-GVIP Journal 5 (7) (2005).
[14] B. Ulrich, L. Maryellen, Robert A. Giger, Robert M. Schmidt,Dulcy E. Nishikawa, Kunio Doi Wolverton, Automatedsegmentation of digitized mammograms, AcademicRadiology 2 (January (1)) (1995) 1–9,doi:10.1016/S1076-6332(05)80239-9, ISSN 1076-6332.
[15] J.W. Byng, N.F. Boyd, E. Fishellï?‘œ, R.A. Jong, M.J. Yaffe,Automated analysis of mammographic densities, Physics inMedicine and Biology 41 (1996) 909,doi:10.1088/0031-9155/41/5/007.
[16] J.J. Heine, M. Kallergi, S.M. Chetelat, L.P. Clarke,Multiresolution wavelet approach for separating the breastregion from the background in high resolution digitalmammography, Computational Imaging and Vision 13 (1998)295–298.
[17] J.Mï?‘œndez Arturo, G.Tahoces Pablo, J.Lado Marï?‘œa,Josï?‘œL. Miguel Souto, Juan J.Vidal Correa, Automaticdetection of breast border and nipple in digitalmammograms, Computer Methods and Programs inBiomedicine 49 (May (3)) (1996) 253–262,10.1016/0169-2607(96)01724-5, 0169-2607.
[18] N. Karssemeijer, G.M. te Brake, M.A.O. Thijssen, J.H.C.L.Hendriks, L.J.T.O. van Erning, Combining single viewfeatures and asymmetry for detection of mass lesions,Digital Mammography (1998) 95–102.
[19] N.F. Boyd, J.W. Byng, R.A. Jong, E.K. Fishell, L.E. Little, A.B.Miller, G.A. Lockwood, D.L. Tritchler, M.J. Yaffe, Quantitativeclassification of mammographic densities and breast cancerrisk: results from the Canadian National Breast ScreeningStudy, Journal of the National Cancer Institute 87 (9) (1995)670–675, doi:10.1093/jnci/87.9.670.
[20] M. Peter, A. Sue, Classification of breast tissue by textureanalysis, Image and Vision Computing 10 (June (5)) (1992)277–282, 10.1016/0262-8856(92)90042-2, 0262-8856.
[21] Manik. V and Andrew. Z, Classifying Images of Materials:Achieving Viewpoint and Illumination Independence,Lecture Notes in Computer Science, 2002, 2352/2002,255-271, DOI: 10.1007/3-540-47977-5 17.
[22] Fei Ma, B. Mariusz, P.S. John, J.B. Murk, Two graph theorybased methods for identifying the pectoral muscle inmammograms, Pattern Recognition 40 (September (9)) (2007)2592–2602, 10.1016/j.patcog.2006.12.011,0031-3203.
[23] S.K. Kinoshita, P.M. Azevedo-Marques, R.R. Pereira, J.A.H.Rodrigues, R.M. Rangayyan, Radon-domain detection of thenipple and the pectoral muscle in mammograms, Journal ofDigital Imaging 21 (1) (2008) 37–49,doi:10.1007/s10278-007-9035-6.
[24] H. Byung-Woo, S. Bong-Soo, Segmentation of regions of
interest in mammograms in a topographic approach, IEEETransactions on Information Technology in Biomedicine 14(January (1)) (2010) 129–139, doi:10.1109/TITB.2009.2033269.
m s i n
56 c o m p u t e r m e t h o d s a n d p r o g r a[25] K.S. Camilus, V.K. Govindan, P.S. Sathidevi, Computer-aidedidentification of the pectoral muscle in digitizedmammograms, Journal of Digital Imaging 23 (5) (1988)562–580, doi:10.1007/s10278-009-9240-6.
[26] E.W. Dijkstra, A note on two problems in connexion withgraphs, Numerische Mathematik 1 (1) (1959) 269–271,doi:10.1007/BF01386390.
[27] Cardoso, J.S.; Domingues, I.; Amaral, I.; Moreira, I.;Passarinho, P.; Santa Comba, J.; Correia, R.; Cardoso, M.J.Pectoral muscle detection in mammograms based on polarcoordinates and the shortest path, Engineering in Medicineand Biology Society (EMBC), 2010 Annual InternationalConference of the IEEE, pp. 4781–4784, August 312010–September 4 2010, doi: 10.1109/IEMBS.2010.5626634.
[28] Mirzaalian, H.; Ahmadzadeh, M.R.; Sadri, S. Pectoral MuscleSegmentation on Digital Mammograms by NonlinearDiffusion Filtering, Communications, Computers and SignalProcessing, 2007. PacRim 2007. IEEE Pacific Rim Conferenceon, pp. 581-584, 22-24 Aug. 2007 doi:10.1109/PACRIM.2007.4313303.
[29] H. Byung-Woo, S. Bong-Soo, Segmentation of regions ofinterest in mammograms in a topographic approach, IEEETransactions on Information Technology in Biomedicine 14(January (1)) (2010) 129–139, doi:10.1109/TITB.2009.2033269.
[30] M.C. Isabela, L.M.S. Luz, A.V. Alvarenga, A.F.C. Infantosi,W.C.A. Pereira, C.M. Azevedo, An automatic method fordelineating the pectoral muscle in mammograms, IFMBEProceedings 18 (Part 2) (2008) 271–275,doi:10.1007/978-3-540-74471-9 63.
[31] J. Grim, P. Somol, M. Haindl, J. Danes, Computer-aidedevaluation of screening mammograms based on localtexture models, IEEE Transactions on Image Processing 18(April (4)) (2009) 765–773, doi:10.1109/TIP.2008.2011168.
[32] J.E. Iglesias, N. Karssemeijer, Robust initial detection oflandmarks in film-screen mammograms using multipleFFDM atlases, IEEE Transactions on Medical Imaging 28(November (11)) (2009) 1815–1824,doi:10.1109/TMI.2009.2025036.
[33] M. Goodsitt Mitchell, Heang-Ping Chan, Bob Liu, Shankar V.Guru, A. Ray Morton, Shyam Keshavmurthy, Nick Petrick,Classification of compressed breast shapes for the design ofequalization filters in X-ray mammography, Medical Physics25 (1998) 937, doi:10.1118/1.598272.
[34] A. Mencattini, M. Salmeri, R. Lojacono, M. Frigerio, F. Caselli,Mammographic images enhancement and denoising forbreast cancer detection using dyadic wavelet processing,IEEE Transactions on Instrumentation and Measurement 57(July (7)) (2008) 1422–1430, doi:10.1109/TIM.2007.915470.
[35] S.G. Mallat, A theory for multiresolution signaldecomposition: the wavelet representation, IEEETransactions on Pattern Analysis and Machine Intelligence11 (July (7)) (1989) 674–693, doi:10.1109/34.192463.
[36] R.M. Rangayyan, R.J. Ferrari, J.E.L. Desautels, A.F. Frere,Directional analysis of images with Gabor wavelets, in:Proceedings XIII Brazilian Symposium on ComputerGraphics and Image Processing, 2000, pp. 170–177,doi:10.1109/SIBGRA.2000.883910.
[37] R.J. Ferrari, R.M. Rangayyan, J.E.L. Desautels, A.F. Frere,Analysis of asymmetry in mammograms via directionalfiltering with Gabor wavelets, IEEE Transactions on MedicalImaging 20 (September (9)) (2001) 953–964,doi:10.1109/42.952732.
[38] G. Fredrik, J. Stefan, Christina Olsï?‘œn, Fractal Analysis ofMammograms (1998), Lecture Notes in Computer Science4522/2007 (2007) 92–101, doi:10.1007/978-3-540-73040-8 10.
[39] G. Qi, S. Jiaqing, F.R. Virginie, Characterization andclassification of tumor lesions using computerizedfractal-based texture analysis and support vector machines
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57
in digital mammograms 4 (1) (2006) 11–25,doi:10.1007/s11548-008-0276-8.
[40] R. Malladi, J.A. Sethian, B.C. Vemuri, Shape modeling withfront propagation: a level set approach, IEEE Transactions onPattern Analysis and Machine Intelligence 17 (February (2))(1995) 158–175, doi:10.1109/34.368173.
[41] C. Daniel, R. Mikael, D. Rachid, A review of statisticalapproaches to level set segmentation: integrating color,texture, motion and shape 72 (2) (1987) 195–215,doi:10.1007/s11263-006-8711-1.
[42] T. Ojala, J. Nï?‘œppi, O. Nevalainen, Accurate segmentationof the breast region from digitized mammograms,Computerized Medical Imaging and Graphics 25 (January (1))(2001) 47–59, doi: 10.1016/S0895-6111(00)00036-7, ISSN:0895-6111.
[43] R.B. Dubey, M. Hanmandlu, S.K. Gupta, A comparison of twomethods for the segmentation of masses in the digitalmammograms, Computerized Medical Imaging andGraphics 34 (April (3)) (2010) 185–191, doi:10.1016/j.compmedimag.2009.09.002,ISSN: 0895-6111.
[44] V. Marina, F. Nivea, S. Maurice, J.F. Peter, Lucas, K. Nico, Anadvanced probabilistic framework for assisting screeningmammogram interpretation, Studies in ComputationalIntelligence 309/2010 (2010) 371–395,doi:10.1007/978-3-642-14464-6 17.
[45] I. Domingues, J.S. Cardoso, I. Amaral, I. Moreira, P.Passarinho, J. Santa Comba, R. Correia, M.J. Cardoso, Pectoralmuscle detection in mammograms based on the shortestpath with endpoints learnt by SVMs, Engineering inMedicine and Biology Society (EMBC), in: 2010 AnnualInternational Conference of the IEEE, August 312010–September 4 2010, 2010, pp. 3158–3161,doi:10.1109/IEMBS.2010.5627168.
[46] S.M. Kwok, R. Chandrasekhar, Y. Attikiouzel, Automaticpectoral muscle segmentation on mammograms by straightline estimation and cliff detection, in: IntelligentInformation Systems Conference, The Seventh Australianand New Zealand 2001, 18–21 November 2001, 2001, pp.67–72, doi:10.1109/ANZIIS.2001.974051.
[47] M. Mustra, J. Bozek, M. Grgic, Breast border extraction andpectoral muscle detection using wavelet decomposition, in:IEEE EUROCON 2009, EUROCON ’09, 18–23 May 2009, 2009,pp. 1426–1433, doi:10.1109/EURCON.2009.5167827.
[48] A. Sultana, M. Ciuc, R. Strungaru, Detection of pectoralmuscle in mammograms using a mean-shift segmentationapproach, in: 2010 8th International Conference onCommunications (COMM) 2010, 10–12 June 2010, 2010, pp.165–168, doi:10.1109/ICCOMM.2010.5509003.
[49] M. Rangaraj, Rangayyan, J. Fï?‘œbio, J.E. Ayres, Leo Desautels,A review of computer-aided diagnosis of breast cancer:toward the detection of subtle signs, Journal of the FranklinInstitute 344 (May–July (3–4)) (2007) 312–348,doi:10.1016/j.jfranklin.2006.09.003,ISSN: 0016-0032.
[50] L. Li, W. Jian, W. Tianhui, Breast and pectoral musclecontours detection based on goodness of fit measure, in:2011 5th International Conference on Bioinformatics andBiomedical Engineering (iCBBE), 10–12 May 2011, 2011, pp.1–4, doi:10.1109/icbbe.2011.5780195.
[51] N. Saltanat, M.A. Hossain, M.S. Alam, An efficient pixel valuebased mapping scheme to delineate pectoral muscle frommammograms, in: 2010 IEEE Fifth International Conferenceon Bio-Inspired Computing: Theories and Applications(BIC-TA), 23–26 September 2010, 2010, pp. 1510–1517,
doi:10.1109/BICTA.2010.5645272.[52] R.J. Ferrari, R.M. Rangayyan, J.E.L. Desautels, R.A. Borges, A.F.Frere, Automatic identification of the pectoral muscle in

s i n
[70] A.W. Michael, S. Alexei, Segmentation of the breast region in
c o m p u t e r m e t h o d s a n d p r o g r a m
mammograms, IEEE Transactions on Medical Imaging 23(February (2)) (2004) 232–245, doi:1109/TMI.2003.823062.
[53] M.K Sze, R.A. Chandrasekhar, Y. Attikiouzel, Automaticassessment of mammographic positioning on themediolateral oblique view, in: 2004 International Conferenceon Image Processing ICIP ’04., vol. 1, 24–27 October 2004,2004, pp. 151–154, doi:10.1109/ICIP.2004.1418712.
[54] X Weidong, L. Lihua, L.A Wei, Novel pectoral musclesegmentation algorithm based on polyline fitting and elasticthread approaching, in: The 1st International Conference onBioinformatics and Biomedical Engineering, ICBBE 2007, 6–8July 2007, 2007, pp. 837–840, doi:10.1109/ICBBE.2007.218.
[55] S. Tzikopoulos, H. Georgiou, M. Mavroforakis, N.Dimitropoulos, S. Theodoridis, A fully automated completesegmentation scheme for mammograms, in: 16thInternational Conference on Digital Signal Processing, 5–7July 2009, 2009, pp. 1–6, doi:10.1109/ICDSP.2009.5201262.
[56] X. Weidong, S. Xia, A model based algorithm to segment thepectoral muscle in mammograms, in: Proceedings of the2003 International Conference on Neural Networks andSignal Processing, vol. 2, 14–17 December 2003, 2003, pp.1163–1169, doi:10.1109/ICNNSP.2003.1281076.
[58] K. Camilus, V. Govindan, P. Sathidevi, Pectoral muscleidentification in mammograms, Journal of Applied ClinicalMedical Physics, North America 12 (March) (2011).
[59] Robert Martï?‘œ, Arnau Oliver, David Raba, Jordi Freixenet,Breast Skin-Line Segmentation Using Contour GrowingLecture Notes in Computer Science, vol. 4478, Springer,Springer Berlin/Heidelberg, 2007, pp. 564–571,doi:10.1007/978-3-540-72849-8 71, ISBN: 978-3-540-72848-1.
[60] April Khademi, S. Farhang, Anastasios Venetsanopoulos,Krishnan Sridhar, Region, Lesion and Border-BasedMultiresolution Analysis of Mammogram Lesions LectureNotes in Computer Science, vol. 5627, Springer,Berlin/Heidelberg, 2009, pp. 802–813,
doi:10.1007/978-3-642-02611-9 79, ISBN: 978-3-642-02610-2.[61] D.Y. Roshan, K. Harada, A connected component labelingalgorithm for grayscale images and application of thealgorithm on mammograms, Proceedings of the 2007 ACM
b i o m e d i c i n e 1 1 0 ( 2 0 1 3 ) 48–57 57
symposium on Applied Computing 1-59593-480-4 (2007)146–152, doi:10.1145/1244002.1244040.
[62] R. Ferrari, A. Frï?‘œre, R. Rangayyan, J. Desautels, R. Borges,Identification of the breast boundary in mammograms usingactive contour models, Medical and Biological Engineeringand Computing 42 (2) (2004) 201–208,doi:10.1007/BF02344632, ISSN: 0140-0118.
[63] Leim Wang, Miao-liang zhu, Li-ping Deng, Xin Yuan,Automatic pectoral muscle boundary detection inmammograms based on Markov chain and active contourmodel, Journal of Zhejiang University - Science 11 (2) (2010),doi:10.1631/jzus.C0910025, ISSN:1869-1951,111-118.
[65] J. Nagi, S. Abdul Kareem, F. Nagi, S. Khaleel Ahmed,Automated breast profile segmentation for ROI detectionusing digital mammograms, in: 2010 IEEE EMBS Conferenceon Biomedical Engineering and Sciences (IECBES), November30 2010–December 2, 2010, pp. 87–92,doi:10.1109/IECBES.2010.5742205.
[66] Ma Fei, B. Mariusz, P.S John, J.B Murk, Validation of GraphTheoretic Segmentation of the Pectoral Muscle, LectureNotes in Computer Science, 2006, 4046/2006, 642-649, DOI:10.1007/11783237 86.
[67] R. David, O. Arnau, M. Joan, P. Marta, E. Joan, BreastSegmentation with Pectoral Muscle Suppression on DigitalMammograms, Lecture Notes in Computer Science, 2005,3523/2005, 153-158, DOI: 10.1007/11492542 58.
[68] P. Xiao-Bo, B. Michael, H. Ralph, Declerck J., The Use ofMulti-scale Monogenic Signal on Structure OrientationIdentification and Segmentation, Lecture Notes in ComputerScience, 2006, 4046/2006, 601-608, DOI: 10.1007/11783237 81.
[69] Wei-Ying Ma, B.S. Manjunath, EdgeFlow: a technique forboundary detection and image segmentation, IEEETransactions on Image Processing 9 (August (8)) (2000)1375–1388, doi:10.1109/83.855433.
mammograms using active contours, VisualCommunications and Image Processing 5150 (2003)1995–2006, doi:10.1117/12.503210.













![[PPT]Appendicular Skeleton Pectoral Girdle and Upper … · Web viewAPPENDICULAR SKELETON PECTORAL GIRDLE AND UPPER LIMB PECTORAL GIRDLE scapula humerus clavicle CLAVICLE sternal](https://static.fdocuments.in/doc/165x107/5b1c49a87f8b9a2d258f98c3/pptappendicular-skeleton-pectoral-girdle-and-upper-web-viewappendicular-skeleton.jpg)
