Inside the Science of an Amazing New Surgery Called Deep ...
Upload
trinhnguyetCategory
view
216download
2
Part 1: What is Asthma?
XX
XX
The Scien
ce Insid
e
Asthma and Allergies
H E A L T H Y P E O P L E L I B R A R Y P R O J E C TAmerican Association for the Advancement of Science

Asthma andAllergies: TheScience Inside
HEALTHY PEOPLE LIBRARY PROJECTAmerican Association for the Advancement of Science

Published 2004 by The American Association for the Advancement of Science (AAAS)1200 New York Avenue, NWWashington, DC 20005
© Copyright 2004 by AAAS
0-87168-694-5
All rights reserved. Permission to reproduce this document for not-for-profit educational purposes or for use in a review is hereby granted. No part of this bookmay be reproduced, stored in a retrieval system, or transmitted in any form, or by any means, electronic, mechanical, photocopy, recording, or otherwise, for commercialpurposes without prior permission of AAAS.
This booklet is a product of the Healthy People 2010 Library Initiative funded by aScience Education Partnership Award (SEPA) from the National Center for ResearchResources at the National Institutes of Health (Grant # 5R25RR15601).
Any interpretations and conclusions contained in this booklet are those of the authorsand do not represent the views of the AAAS Board of Directors, the Council of AAAS,its membership, or the National Institutes of Health.

INTRODUCTION: ASTHMA AND ALLERGIES . . . . . . . . . . . . . . . . . . . . . 1
PART 1: WHAT IS ASTHMA? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Healthy breathing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Problems associated with asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4The symptoms of asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5The causes of asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6How asthma affects the body . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11How asthma affects lifestyle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
PART 2: WHAT ARE ALLERGIES? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Healthy immune system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Problems associated with allergies . . . . . . . . . . . . . . . . . . . . . . . . . . . 19The symptoms of allergies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20The causes of allergies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22How allergies affect the body . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25How allergies affect lifestyle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
PART 3: WHO HAS ASTHMA AND ALLERGIES? . . . . . . . . . . . . . . . . . . 31Childhood allergies and asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Uneven impact of allergies and asthma . . . . . . . . . . . . . . . . . . . . . . . 35Societal impact of allergies and asthma . . . . . . . . . . . . . . . . . . . . . . . 37
PART 4: HOW CAN ASTHMA BE TREATED AND PREVENTED?. . . . . . . 41Diagnosing and treating asthma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Preventing and controlling asthma. . . . . . . . . . . . . . . . . . . . . . . . . . . 44The relationship between allergies and asthma . . . . . . . . . . . . . . . . . 49
PART 5: HOW CAN ALLERGIES BE TREATED AND PREVENTED? . . . . . 53Diagnosing and treating allergies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Preventing and controlling allergies . . . . . . . . . . . . . . . . . . . . . . . . . . 57
T A B L E O F C O N T E N T S

PART 6: WHAT DOES RESEARCH TELL US ABOUT ASTHMA ANDALLERGIES? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61Current lines of research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61The important role of volunteers . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
CONCLUSION: Let’s Breathe Easy with Asthma and Allergies . . . . . . 71
APPENDIX 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72Sample Asthma Action Plan
Appendix 2: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Questions to Ask Your Physician about Allergies and Asthma
APPENDIX 3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76Taking Part in Research Studies — Questions to Ask
RESOURCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
BIBLIOGRAPHY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
GLOSSARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85

1
Nothing is more essential toour well-being than the ability to breathe. Most of us breathe in and out all day long withouteven giving it a thought. Yet millions of people in the UnitedStates are not so lucky. They suffer from asthma or allergies.For people with asthma, taking abreath can be extremely difficult.For people with allergies, the airthey breathe can be filled withsubstances that cause discomfort or worse.
Asthma is a chronic lung diseasein which air passages getinflamed. When this happens,airways narrow and it is difficultfor air to move from the nose andmouth to the lungs. In the UnitedStates, this disease affects mil-lions of people, many of themchildren. In fact, asthma is themost common chronic childhooddisease, affecting 1 out of every20 children. The number of peo-ple with asthma has beenincreasing since the 1980s. Thedisease affects people of all agesand races and both sexes.However, asthma is more com-mon in children than adults. It isalso more common in AfricanAmericans and Hispanics thanwhites.
An asthmatic, or a person withasthma, responds differently tocertain substances than a personwho does not have the disease.For an asthmatic, these sub-stances become triggers. A trig-ger is a factor that can bring onthe symptoms of asthma or makethe condition worse. For an asth-matic, triggers can include house-hold or industrial chemicals,tobacco smoke, dust, changes inweather, and exercise. Exposed to a trigger, an asthmatic mightexperience tightness in the chest,coughing, wheezing, and short-ness of breath.
Although asthma is common, it can be controlled and treated. It is important for an asthmatic
INTRODUCTION: ASTHMA AND ALLERGIES
Asthma affects 1 out of every 20 children.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
2
to avoid contact with any triggerknown to cause symptoms. A per-son with asthma should get continuous medical care and see a physician regularly. A doctor can measure lung function andcapacity and recommend medica-tion to reverse and prevent airwayswelling and obstruction. If thesymptoms are managed well, anasthmatic can enjoy a normal life.
Like asthma, allergies also affectmillions of people. An allergy is
the body’s overreaction tocertain substances, calledallergens. An allergic per-son responds differently toallergens than does a per-son with no allergies.Some of the most commonallergens include dustmites, cockroach drop-pings, animal dander,grass, insect venom fromstings, medications, andcertain foods. An allergicreaction can range fromsneezing and itching to
swelling of the throat and loss ofconsciousness. As with asthma,allergic reactions can be severeand even fatal.
A person with allergies shouldavoid allergens that are known tocause symptoms. People who haveexperienced severe allergic reac-tions should be under the care ofan allergist—a physician who
specializes in the treatment ofallergies. Before establishing atreatment program, an allergistwill conduct tests to determinewhich allergens are triggers for aparticular patient. The allergistmay recommend or prescribe med-ications that can reduce sensitivityto certain substances. Allergenimmunotherapy can also be usedto reduce sensitivity. A personundergoing allergen immunothera-py receives injections containingsmall amounts of the allergen towhich he or she reacts over thecourse of several years. This treatment helps the person build immunity to an allergen.Ultimately, this can mean that an allergic reaction does not occur at all.
Fortunately, there are many prom-ising areas of research on allergiesand asthma. Scientists are work-ing to discover what causes asth-ma and allergies, how to preventthem from occurring, and how totreat them. But it is also vital thateveryone who suffers from asthmaor allergies have a basic under-standing of these ailments. Thisbook contains information thatwill help asthmatics and allergysufferers take charge of their ownhealth so that they can lead full,active lives.

Healthy breathing
Healthy breathing is effortless. Aperson who is breathing normallywill not be aware of the process.Every minute of every day, thelungs expand and contract 15times. This process allows theblood to deliver oxygen to redblood cells and to take away car-bon dioxide.
Air enters the nose, where it iswarmed and moistened. Then, itenters the trachea, a single tubethat is the beginning point of theairways. The trachea divides intotwo narrower tubes calledbronchi. Each bronchus is a wayinto the lungs. As the air travelsthrough the lungs, it movesthrough progressively smallertubes called bronchioles. At thetip of the last bronchiole it enters,the air comes into contact withhundreds of millions of tiny airsacs called alveoli. These sacstake in oxygen from the air in exchange for carbon dioxide.Eventually, the lungs will exhalethe carbon dioxide.
For the exchange of oxygen forcarbon dioxide to take place, thediaphragm, a sheet of musclethat separates the chest from theabdominal cavity, must contract.When the diaphragm contracts, a partial-vacuum effect occursaround the lungs, causing them
3
Part 1: What Is Asthma?

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
4
to expand. When the lungsexpand, air pressure in the chestcavity is lower than the air pres-sure outside. This difference inpressure causes air from the outside to fill the lungs. Each time this happens, approximately 1 pint of air enters the lungs.
When you exhale, the diaphragmrelaxes. When the lungs deflate,carbon dioxide is forced out. Whilethis entire process is taking place,mucus in the air passages is trap-ping any foreign materials thathave entered your body with theair. After the mucus traps these
particles, the mucus is carriedby cilia (which look like tinyhairs) from the bottom of thelungs to the throat. Once themucus reaches the throat, it iseither swallowed or coughedout. If the mucus is not cleared,viruses, bacteria, and otherimpurities can collect in thelungs and cause infection or ill-ness. Healthy lungs are grayishpink in color. Lungs that aredamaged by pollutants canbecome blackened.
If your breathing is not healthyor normal, it might be due toallergies or even asthma.Allergies have been linked toasthma, so it is not unusual to find that a person suffersfrom both. These disorders can be treated, and sometimesthe symptoms can even be
prevented. With proper medicalcare and changes in behavior orenvironment, someone who suffersfrom allergies or asthma canbreathe comfortably and live an active life.
Problems associated with asthma
Asthma is a chronic lung diseasethat makes breathing difficult. Foran asthmatic, breathing becomesdifficult for a variety of reasons.Airways can become inflamed,restricted, or blocked, so that very
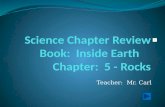
In an asthmatic person, themuscles of the bronchialtubes tighten and thicken,and the air passagesbecome inflamed and filledwith mucus, making it difficult for air to move.
In a nonasthmatic person,the muscles around thebronchial tubes are relaxedand the tissue thin, allowingfor easy airflow.

little air can travel to and fromthe lungs. The air that does getthrough these narrowed passagescan cause a high-pitched orwhistling sound called wheezing.The chest can also become tightor constricted, requiring the per-son to use more effort just tobreathe. This is called laboredbreathing.
If a lot of viscous (thick) mucus isreleased in the airways, it canproduce coughing. As the bodytries to clear the mucus from theairways, a rattling sound oftenoccurs. If the airways becomeplugged with mucus, the lungscan fully or partially collapse.This collapse can be caused by a number of conditions, from prolonged bed rest to pneumonia,and can be seen on a chest X ray.Unfortunately, when a collapsinglung is found—especially in com-bination with a rattling soundheard in the chest—asthma canbe misdiagnosed as bronchitis oreven pneumonia. Antibiotics areoften prescribed for bronchitisand pneumonia, but these med-ications are not effective againstasthma.
The symptoms of asthmaPeople with asthma experiencesymptoms that can include cough-ing, wheezing, congestion, andtightness in the chest. Most of
these symptoms are usually associated with colds or infec-tions. That is why it is importantto notice when they reoccur for no apparent reason. When thishappens, it could mean that youhave asthma. Although asthmasymptoms might resemble coldsymptoms, they must be treated differently.
A viral infection,such as a cold, mightmake it hard tosleep at night for afew days. Nighttimeasthma is very dif-ferent. It can makegetting proper restnearly impossible fora long period oftime. Some asthmat-ics have symptomsevery night. Peoplewith nighttime asth-ma often have tosleep sitting uprightin order to breathe.If these symptomsare disregarded ascold symptoms, thenthey will not be treated properly.A serious lack of rest can havedangerous consequences, especial-ly for a developing child.
Symptoms of asthma are usuallymeasured by their severity, fre-quency, and response to treat-ment. The National Institutes of
5
Part 1: What Is Asthma?

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
6
Health has defined the followingseverity levels for asthma: mildintermittent, mild persistent,moderate persistent, and severepersistent. Those with the milderform of the disease might havebrief episodes once a week.Asthmatics with the most severeform of the condition have symp-toms that won’t go away, attacksthat easily become crises, very lit-tle lung capacity, and restrictedphysical activity.
Whether symptoms appear to bemild or severe, it is crucial thatthey be evaluated. Even if youseem to experience symptoms onlyafter exercise or during the night,an examination by a physiciancan be the first step in gettingrelief. For someone who has livedwith the symptoms for a longtime, the chest tightness andbreathing difficulty can seem
almost normal. Having problemswith breathing, however, is nevernormal or healthy.
Even some less common symp-toms of asthma require emer-gency help. If an asthmatic sud-denly starts to sweat, seemslethargic (or dazed), appearsfatigued, or has difficulty speak-ing, he or she should be taken toan emergency room. If the personhas severe difficulty breathing,intense coughing, a racing pulse,or cyanosis (nail beds or lips thatare bluish in color), these are alsosigns of an emergency.
The causes of asthma
Scientists still do not know exactly what causes asthma.Researchers are investigating anumber of possibilities, including
Severity Levels for Asthma
MILD INTERMITTENT—About half of all asthma patients fall into this category, which ischaracterized by fewer than two or three asthmatic episodes per week and no difficultysleeping at night. No continuous control treatment is necessary.
MILD PERSISTENT—Patients typically have tightness and wheezing weekly, but relativelynormal lung function overall. One controlling medication is sufficient to manage the illness.
MODERATE PERSISTENT—Daily episodes characterize this stage, but the flare-ups are manageable with two medications.
SEVERE PERSISTENT—Episodes occur daily, despite therapy with more than two controllingmedications.
(Adapted from http://www.nih.gov/news/NIH-Record/03_04_2003/story06.htm)

smog, lack of exercise, obesity, toomuch exposure to indoor aller-gens, and even a lack of exposureto viruses and bacteria in child-hood, which could weaken theimmune system. It is likely that anumber of factors combine tocause asthma.
Scientists do know that manypeople with asthma also haveallergies, such as hay fever oreczema, or a family history ofallergies. Others, however, haveno history of allergies or evidenceof allergic problems. Asthma alsoseems to run in families. If oneparent has asthma, his or herchildren are more likely to haveasthma. If both parents haveasthma, there is a 40% chancethat their children will developthe disease. Although severalpeople in the same family mayhave asthma, the severity of theirsymptoms may not be the same.Even if identical twins have asth-ma, one twin might have a moresevere case of it. Scientists do notknow why this is so.
Although the exact causes ofasthma may not be known, scien-tists do know a great deal aboutwhat happens inside the bodywhen an asthma attack occurs.Specifically, three changes occurinside the airways in the lungs ofpeople with asthma. The firstchange is inflammation (orswelling), which leads to constric-tion and sensitivity.
Airway inflammation happenswhen the mucosa (or bronchialmucous membrane) swells. Theinflamed tissues make a thickmucus, which is difficult to getrid of and can often producecoughing. This inflammation then
Part 1: What Is Asthma?
7
Many childrenwho have asthma comefrom families in which their relatives alsohave asthma.
This illustrationshows the effectsasthma has on abronchiole. (left)Normal bronchi-ole; (middle) mus-cular rings con-tract and thicken,decreasing lumensize; (right)mucosal layersand their connec-tive tissue, thesubmucosa, thick-en, further closingthe lumen, whichfills with thick-ened mucus.
lumen
mucosa
muscular rings
lumen
submucosa
mucosa

leads to bronchoconstriction(or bronchospasm), in which thesmooth muscle that surrounds theairways contracts too much, nar-rowing the airways and making itdifficult to breathe. In people withasthma, inflammation also leadsto sensitivity. This means that theairways are overly sensitive (orhyperresponsive) to even minorirritants. Such irritants caninclude tobacco smoke, air pollu-tion, the common cold, or even coldair. If an asthmatic also has aller-gies, he or she can be overly sensi-tive to pollen, animal dander, ordust, for example.
Asthma can be triggered by bothallergic and nonallergic reactionsto various factors. Most asthmaattacks are of the allergic variety,resulting from exposure to triggerssuch as animal dander and mold.These triggers exist in both indoorand outdoor environments. Anasthma attack can result fromhigh levels of pollen in the air orfrom cockroach droppings inhousehold dust. A simple allergyskin test can help determine someof the triggers that cause thesymptoms. (For additional infor-mation on triggers, see the section“Causes of Allergies” on page 22.)
Nonallergic asthma can be trig-gered by exposure to viral infec-tions, shifts in air temperature,physical exertion, chemicals, med-
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
8
What Causes Occupational Asthma?
Direct exposure to irritants. Substances such ashydrochloric acid, sulfur dioxide, and ammonia can trig-ger occupational asthma in those exposed to them.Commonly used in the petroleum and chemical indus-tries, these irritants are particularly harmful to peoplewith a history of respiratory disorders.
Allergic reactions from long-term exposure. A worker’simmune system might take months or years beforedeveloping a reaction to a particular substance, but thesymptoms can be quite severe. Everyday, common sub-stances can trigger symptoms. A veterinarian can devel-op occupational asthma from exposure to animal pro-teins. A health care worker can suffer from asthmasymptoms in reaction to the powder that lines latexgloves.
Accumulation in the body. Over time, workers whoinhale certain substances can experience asthma symp-toms because of a buildup of naturally occurring chemi-cals in their bodies. For example, an insecticide that isused in farming can cause acetylcholine to build up in a farm worker’s body. This buildup can cause airwaymuscles to contract, resulting in an asthma attack.

ications, or foods. Viral infectionscan bring on asthma especially inyoung children. When someonecatches a cold, the nose, airways,throat, and lungs often feel irri-tated. This irritation can triggerasthma symptoms. A conditioncalled sinusitis—in which thehollow cavities located behind theeyes and nose get inflamed—cancause asthma. Sinusitis can bringon wheezing, headaches, cough-ing, sinus pressure or pain, andpostnasal drip. During an attackof sinusitis, excess mucus drainsinto the nose, throat, andbronchial tubes. This drainagecan trigger or aggravate asthma.
Gastroesophageal reflux dis-ease (GERD), a condition inwhich stomach acid flows upthrough the esophagus, affectsmany people who suffer fromasthma. The symptoms of GERDinclude severe heartburn, belch-ing, frequent coughing, hoarse-ness, and asthma at night, aswell as after meals and exercise.Some asthma symptoms arerelieved by medications pre-scribed for GERD.
Another type of nonallergic asth-ma is called exercise-inducedasthma. It is triggered by strenu-ous physical activity. Intense, pro-longed breathing through the
mouth can lead to coughing ortightness in the chest. Exercisingin cold, dry air can also makebreathing difficult.
Asthma symptoms that developbecause of exposure to fumes,gases, dust, or other substancesin the workplace are called occu-pational asthma. This type ofasthma can develop in an asth-matic or in someone with no his-tory of the condition. The symp-toms of occupational asthma cancontinue even after the worker isno longer exposed to the sub-stance that triggered the initialreaction. The symptoms caninclude a runny nose and eye irri-tation, as well as difficultybreathing. Occupational asthmasymptoms often grow worse asthe workweek progresses, get bet-ter over the weekend, and then
Part 1: What Is Asthma?
9

resume when the person returns towork. Smoking can also worsensymptoms, as can being exposed tosecondhand smoke.
A worker can be exposed to triggersubstances for months or yearsbefore symptoms arise. Often, thesymptoms of occupational asthmaare misdiagnosed as bronchitis.This is dangerous because it canlead the worker to return to theenvironment that caused thesymptoms. Continued exposure totriggers can be quite harmful.Employees are not the only peoplewho can be affected by harmfulsubstances in the workplace.Asthma can also occur in peoplewho live near factories that releasetrigger substances into the envi-ronment. Leaving an asthma-inducing work environment within one to two years of the initial illness can reverse occupa-tional asthma. For workers withthe disease who smoke, researchshows that those who leave the
unhealthy work envi-ronment and quitsmoking are more like-ly to recover fully thanis a worker whochanges jobs, but con-tinues to smoke.
In developed countries,occupational asthmahas become the mostcommon form of work-
related lung disease. According tothe American Academy of Allergy,Asthma, and Immunology, up to15% of asthma cases that havebeen diagnosed in the UnitedStates have some connection tojob-related factors. In certainindustries, the rate of occupationalasthma is quite high. In somemanufacturing companies, expo-sure to particular chemicals need-ed for producing plastics and foamhas resulted in symptoms in 10%of exposed workers. Inhaling a sin-gle enzyme that is used to makewashing powder has triggeredasthma in 25% of exposed workers.In the printing industry, regularexposure to gum acacia, which isused in color printing, has pro-duced asthma symptoms in 50% of the workers exposed to it.
An asthmatic can also experiencean attack as a result of taking par-ticular medications. Some of themost common medications thattrigger asthma symptoms are
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
10
Occupationalasthma is the
most commonform of work-
related lung disease in the United States.

Part 1: What Is Asthma?
11
aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs),such as ibuprofen. In fact, accord-ing to the American Academy ofAllergy, Asthma, and Immuno-logy, up to 19% of adult asthmat-ics have sensitivities to aspirin or NSAIDs. Medications calledbeta-blockers—which are takento address heart disease, highblood pressure, glaucoma, ormigraines—can prompt asthmaattacks as well.
In about 6–8% of children, certainfoods and food additives can bringon asthma symptoms. Some ofthe most common products thattrigger asthma attacks are milk,eggs, peanuts, tree nuts (forexample, walnuts or almonds),soy, wheat, fish, and shellfish.
It is important to note that anxiety alone cannot give some-
one asthma. However, emotionalfactors can make asthma symp-toms worse or attacks more fre-quent. For example, if a person isunder stress, he or she will proba-bly feel more fatigued. Thisfatigue can increase the numberof asthma symptoms or makethem more intense. An anxiousperson might be more likely tohyperventilate, which can worsenasthma symptoms.
How asthma affects the bodyIn general, if asthma symptomsare addressed early and managedconsistently, there is little risk of significant damage. Each asth-matic episode does take a toll on the body, so it is best to try to prevent symptoms whenever possible.
Breathing insmoky air from a fire can worsenasthma symptomsbecause smokecarries very smallparticles that canbuild up in yourlungs. If you haveasthma and livein an area wherewildfires are common, youshould talk toyour doctor abouta plan for smokydays.

When an asthma attack occurs, a person experiences more thanjust difficulty breathing. Theinflammation and obstruction ofthe airways, both of which com-monly occur during an asthmaattack, can be associated with per-manent changes in the body. Theairways can become permanentlynarrowed. Usually, airway obstruc-tion does not cause any seriousdamage to the lungs, heart, orother organs. However, severeasthma attacks can lead to perma-nent damage or even death.During such an episode, an asth-matic can lose consciousness orsuffer brain damage because toolittle oxygen reaches the brain.This is one of the reasons that it isvital to seek medical help as soonas possible when a severe asthmaattack occurs.
When people suffer from exercise-induced asthma, their symptomsoften appear after only brief peri-ods of activity. Their airways tendto be overly sensitive to suddenchanges in temperature andhumidity. When people exert them-selves, they often breathe cold, dry air in through the mouth. This does not allow the naturalwarming and humidifying action of the nose to take place. Peoplewith exercise-induced asthma tendto develop a reduced capacity toadd moisture and warmth to theair before it reaches the lungs.
In addition, they have more diffi-culty exercising in environmentswhere air pollution and pollen arecommon.
How asthma affects lifestyleAsthma affects daily life in manyways. Often, an asthmatic mustrestrict activities to avoid exposureto trigger substances and factors.An asthmatic must be cautiouswhen taking a new medication,tasting a new food, or entering anew environment. A person withchronic asthma must remember totake daily preventative medica-tions on time. When going out,many asthmatics must arm them-selves with “rescue” medicationsfor use in case of an attack.
Frequently changes must be madeto an asthmatic’s home or workenvironment to make breathingeasier. Sometimes, bedroom car-peting and drapes, which can behome to dust mites, should beremoved. If the parents of an asth-matic child smoke, they shouldquit. If a factory worker developsoccupational asthma from a sub-stance in his or her work area, theperson should change job locationsor professions.
For many people, a common cold is just a brief annoyance. For anasthmatic, this minor infection can produce asthma symptoms.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
12

Part 1: What Is Asthma?
13
Asthma and PregnancyStudies have shown that pregnancy can worsen asthmasymptoms, most often in the late second and early thirdtrimesters. During the last fourweeks of a pregnancy, womenfrequently report experiencingfewer symptoms. If asthma ismanaged properly throughout a pregnancy, a woman willrarely experience symptoms atthe time of labor and delivery.
One reason that asthma symptoms might worsen during pregnancy is connected toGERD. When the stomach becomes compacted to make room for a baby, heartburn and acid reflux can result, making asthma symptoms worse. Sinus infections, viral respiratory infections, and increased stress can also worsen asthma symptoms during pregnancy.
Asthma in pregnant women is treated in the same way that asthma is treated in others.What is most important is that it be treated. If it is not, there can be dangers for both themother and the child. When an asthmatic first discovers that she is pregnant, she shouldmake an appointment with her allergist or primary care physician to discuss treatment.Like any other asthmatic, a pregnant asthmatic should avoid any substances or factorsthat are known to trigger symptoms.
Sometimes a patient and a physician must weigh the risks of unmanaged asthma againstthe risks of taking medication during pregnancy. Generally, it is considered far moreimportant to control asthma symptoms. There are asthma medications that can be takensafely throughout pregnancy. Most inhaled medications are safe for pregnant women.Oral medications should be avoided unless absolutely necessary.
Generally, allergy shots are safe for a pregnant woman who was receiving them beforeconceiving. A woman should not start receiving allergy shots for the first time while pregnant. Sometimes, an allergist will lower the dosage in the shot to prevent an allergicreaction. These reactions are rare, but can be dangerous to a baby.
If a pregnant woman’s asthma is not managed properly, serious complications can result.If not enough oxygen reaches the mother’s blood, then not enough oxygen reaches thebaby’s blood. This deficiency can threaten the baby’s growth and survival. A developingbaby needs to receive a constant supply of oxygen. A baby born to a mother with unmanaged asthma can have a lower birth weight.
With some medicines, physicians are not sure whether asthma medications can be trans-ferred to a baby through breast milk. Medications such as theophylline, beta agonists,cromolyn sodium, and steroids do not seem to be dangerous to nursing babies. To man-age allergy symptoms, a nursing mother can safely use prescription antihistamines anddecongestants.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
14
Benefits of ExerciseExercise offers many physical and emotional benefits, especially for people who sufferfrom allergies or asthma. Exercise improves cardiovascular fitness, muscle strength, andstamina. Physical activity improves circulation throughout the body and one’s generalenergy level. As a result of increasing physical activity, the body uses oxygen more effi-ciently and the respiratory system strengthens. Exercise elevates the mood and reducesstress. For people with allergies or asthma, the physical benefits of exercise improve theirgeneral health. In particular, it can help them breathe easier because more blood andoxygen reach the lungs. Exercise can ease the stress and anxiety that are often associatedwith asthma attacks. People with asthma should talk with their doctor before beginninga new exercise program, particularly a strenuous one.
Influenza (the flu) can bring onmore severe symptoms for a per-son who suffers from asthma. It is very important for asthmatics toavoid exposure to these viruseswhenever possible. It is wise forasthmatics to get yearly flu vac-cines. If an asthmatic is exposed to a cold or the flu, rest and propernutrition can help to prevent thesymptoms from escalating to asthma.
Often, asthmatics have difficultywhen they exert themselves inways that require deep breathing.Sports such as soccer, basketball,
and long-distance running, whichdemand continuous exertion, aremore likely to trigger asthmasymptoms. By contrast, sports likewrestling, gymnastics, baseball,and surfing require brief bursts ofenergy, which do not seem toaggravate asthma as often. Thosewho suffer from exercise-inducedasthma are likely to find walking,slower-paced biking, hiking, anddownhill skiing easier than thepreceding sports. With treatmentand careful training, an asthmaticcan participate in almost anysport.

Part 1: What Is Asthma?
Racing to Victory overAsthma and Allergies
As a competitive swimmer, Tom Dolancouldn’t have designed a better body forhimself. At 6 feet, 6 inches tall, with armsthat seemed to stretch the width of a poollane, he wasn’t exactly a welcome sight tohis opponents.
But what no one could see was that insideDolan’s imposing physique was an athleticflaw: lungs plagued by severe asthma andallergies. At times during his training work-outs, Dolan would labor for breath and
even black out in the water. His college coach always kept an inhaler rightnext to the pool. But instead of quitting, Dolan kept training harder andswimming faster—until he made it to the U.S. Olympic team.
When he came home from the Olympics in Atlanta in 1996, it was with agold medal—and he landed on the covers of Sports Illustrated magazine anda Wheaties box. He went back in 2000 to Sydney, Australia, and this time hedid even better, capturing a gold and a silver.
“I had no superhuman qualities that helped me to overcome asthma, exceptthe fact that I had a big heart and wouldn’t allow myself to be beaten downby asthma,” says Dolan. He also possesses an iron will: When he broke hisarm at age 11, he wore a special foam cast and dragged his arm through thewater as he swam countless laps.
Dolan’s competitive spirit is legendary in his family. To get him to drink milkas a child, his father would simply pour two glasses and say, “Race you!”
But at times, asthma seemed like the one opponent that could really giveDolan trouble in the pool. Although doctors often prescribe swimming as anideal exercise for asthmatics (because the humidity and warmth of the watercan make breathing easier), it’s with the understanding that asthmatics willswim slow, steady laps. The level of training Dolan underwent to take on thetop swimmers in the world was so intense that some doctors worried that hecould risk his health.
15Dolan, continued on next page

“When I was in high school, a lot of doctors told me not to swim,” says Dolan,who took up the sport at age five because his older sister was a swimmer andhe wanted to beat her. “They were worried about all the chemicals in the poolaffecting my allergies and asthma. I really had the worst of both worlds interms of athletics. The harder and more intense my training was, the worse myasthma became. And in the fall, with tree mold, and the spring, with pollen,my symptoms got worse.”
When Dolan was in college, he found a doctor who specialized in asthma andwho put him on a carefully monitored treatment regime. That helped Dolan’ssymptoms immeasurably—as his row of gold and silver medals prove.
Dolan recently retired as a competitive swimmer and is now living inArlington, Virginia, while he interviews with various corporations and pre-pares for a second career as a businessman. It’s a sure bet he’ll be successful in whatever he does—and, in a strange way, Dolan says he owes some of hisconfidence to asthma.
“One of the most frustrating things for young people with asthma is thatthere are only so many things that are in your control. You can’t control theheat and humidity and the air quality,” Dolan says. “For an athlete in an elitepart of the game, we like to control everything. So asthma gave me a lot ofperspective on the fact that swimming is just a sport and there are a lot ofthings out there that are more important. For all the troubles asthma gaveme, it also gave me a lot on the other side to make me stronger.”
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
16

17
Healthy immune systemThe immune system is so complexthat some of the way it works isnot yet understood. What scien-tists do know is that a healthyimmune system battles infectiousagents in an effort to keep thebody free of disease. When a disease-producing organisminvades the body, the white bloodcells (called leukocytes) form akind of army that gathers togeth-er to prevent infection. Leuko-cytes also work to repair anydamage done by an invader.
Just as there are a variety of foreign materials that act asinvaders (viruses, bacteria, para-sites, and fungi), there are manytypes of white blood cells.Different ones have differentfunctions. One type, called neutrophils, ingests bacterialinvaders and produces the chemi-cals that destroy them. Whateverthe type, white blood cells worktogether to help produce thebody’s immune response.
White blood cells are assisted bylymphocytes—cells that play the
most prominent role in helpingthe body create a natural resist-ance to disease. There are twotypes of lymphocytes: B cells andT cells. B lymphocytes produceantibodies that do battle withantigens, the foreign substancesthat are created by an invader.When an invader enters the body,its antigens alert the immunesystem to the invader’s presence.
Part 2: What Are Allergies?
The immune system protectsthe body from harmful substances. The immunityresponse (inflammation) ispart of innate immunity. It occurs when tissues areinjured by bacteria, trauma,toxins, heat, or any othercause.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
18
When antibodies target the invad-er, they also send messages towhite blood cells to join the bat-tle. T lymphocytes attack cellsthat are foreign or that are infect-ed by a virus. They do this bygenerating antibodies that fightoff the foreign particles found ininvading cells. Their attack alsoincludes digesting the invaders orreleasing chemicals that candestroy them. Another job of the T cells is to help the bodyaccept—without overreacting to—the chemicals that are found inallergy shots.
Among the substances that theimmune system encounters areallergens, which can trigger aller-gic reactions in many people.Some of the most common aller-gens are pollen, mold, and animaldander, as well as cockroach and
house dust mite droppings.Scientists do not know why somesubstances are allergens for somepeople and harmless for others.
The body has two main ways ofprotecting itself. Innate immu-nity is the body’s first line ofdefense. It includes the barriersthat keep antigens from enteringyour body, such as the skin,mucus, stomach acid, the coughreflex, and enzymes in tears andskin oils. An antigen that getspast these barriers then has toface other parts of the immunesystem, such as certain whiteblood cells that “eat” microorgan-isms and dead or damaged cells.Inflammation, or swelling, is alsopart of innate immunity. Bloodvessels leak fluid into damagedtissues. This swelling keeps for-eign substances away from otherbody tissues.
Active (acquired) immunityis slightly different, occurringwhen the body responds to a foreign invader such as a virus. In active immunity, the bodyresponds to an antigen and buildsa defense that is specific to thatantigen. In other words, the firsttime the body comes in contactwith a foreign invader, it createsantibodies that attack only thatinvader. The next time the sameantigen enters the body, the

Part 2: What Are Allergies?
19
immune system is already pre-pared to fight it. In a sense, theimmune system “remembers” theantigen.
When a body has a healthyimmune system, some invaderscan be conquered before they cre-ate the condition that leads todisease. The damage from otherinvaders that succeed at first canbe minimized and repaired. Whenan immune system is not healthy,it is not able to work as well infighting off these invaders. Insome cases, an immune systembecomes so compromised that itshuts down and is unable to fightoff or contain any disease-produc-ing organisms.
Problems associated with allergiesA person with allergies has animmune system that overreacts tosubstances that do not producesymptoms in most people.Substances that are otherwiseharmless, such as animal danderor dust, can trigger a severe aller-gic reaction in a person who issensitive to them. For these peo-ple, animal dander and dustbecome allergens. A person withallergies might experience sneez-ing, wheezing, coughing, or anitchy feeling in the throat.
Allergic rhinitis (hay fever) is an inflammation of the mucousmembranes of the nose. It iscaused by the same types of sub-stances that trigger allergies.Outdoor triggers include grasses,trees, and weeds. Indoor triggersinclude mold, animal dander, andcockroach droppings. Treatmentssuch as allergen immunotherapy,medications, and, of course,avoiding the triggers can providesome relief. If not properly treat-ed, a person with rhinitis candevelop sinusitis.
There are two forms of sinusitis,a condition characterized by aninflammation of the sinuses, aplugged-up nose, a feeling thatthe face is swollen, toothache,tiredness, and fever. One type iscalled chronic sinusitis. Thiscondition is often caused by bac-terial infections and can be acause of chronic cough. Another
The animaldander frompets can trig-ger an allergicreaction in aperson who issensitive to it.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
20
type is called acute sinusitis.Also caused by bacterial infections,acute sinusitis can appear severaldays after the first sign of a cold.Exposure to tobacco smoke andchemical odors can make symp-toms worse. People with allergiesseem to be predisposed to develop-ing acute sinusitis, perhapsbecause allergies tend to lead toinflammation of the sinuses andnasal linings. The inflammationcan prevent bacteria from getting
cleared from nasal cavities. Long-term treatment for allergies cansometimes help prevent acutesinusitis from developing.
The symptoms of allergiesThe symptoms that an allergicperson experiences are determinedby the type of allergen that trig-gers the reaction, the site wherethe reaction occurs, and theimmune system’s response. Some

people suffer from symptoms thatare mainly consistent with hayfever: runny nose, congestion, and sneezing. Others experiencea reaction that is more typical of a response to a food allergy:swelling of the throat, difficultybreathing, and dizziness. Stillothers break out in hives, anitchy skin rash that forms in clusters, when exposed to a medication such as penicillin.
Allergic reactions can be quitedifferent and can range frommerely annoying to fatal. Themilder, more annoying symptomscan begin with watery, swolleneyes; an itchy, irritated nose andthroat; and hoarseness in thevoice. The nasal passages candrain profusely, through the frontof the nose or down the back ofthe throat. The symptoms cangrow more irritating as they startto reduce the person’s ability tobe active. Thick phlegm (mucoussecretions in the respiratory passages) can occur as the chestbecomes more congested. Cough-ing and sneezing can be so severethat the person becomes exhaust-ed from the effort both require.The skin can become one red,itchy, swollen rash. Abdominalcramps, vomiting, and diarrheacan make it impossible for a per-son to leave home. Still, howeverawful these symptoms sound,none is as bad as those sufferedduring anaphylaxis.
Anaphylaxis is a sudden, severeallergic reaction that can have avariety of symptoms. It is impor-tant to learn about these symp-toms, because anaphylaxis can befatal if it is not properly treated.This allergic reaction can involvemajor areas of the body at thesame time, such as the skin, therespiratory system, the gastroin-testinal tract, and the cardiovas-cular system. Symptoms canoccur within minutes of an expo-sure to a trigger (for example,after receiving an insect sting). It is important to remember,though, that sometimes symp-toms do not appear for severalhours (for example, after taking a medication).
Symptoms associated with vari-ous forms of anaphylaxis includefever, swelling throughout thebody or in one area, difficultyswallowing or breathing, nausea,
Part 2: What Are Allergies?
21
Anaphylaxis

vomiting, diarrhea, abdominal oruterine cramping, congestion, afeeling of having to urinate, hives,swelling of the lips and joints,severe anxiety, headache, itching,sneezing, coughing, and wheezing.The most dangerous symptoms ofanaphylaxis are low blood pres-sure, breathing difficulties, shock,and loss of consciousness.Sometimes anaphylactic symptomsare misdiagnosed as hyperventila-tion, anxiety attacks, low bloodsugar, or drug and alcohol intoxi-cation. A misdiagnosis can bedeadly.
There are no cures for this varietyof allergic reaction, but many
promising treatments can preventor control the symptoms. (Seepages 56–57 for information abouttreatments.)
The causes of allergiesThe exact cause of allergic reac-tions is not known. However, thereappears to be a hereditary compo-nent to the more common forms ofthe condition. If one parent hasallergies, a child’s risk of develop-ing the condition is 48%. If bothparents suffer from allergic reac-tions, the child is 70% likely todevelop allergies. When it comes to allergies, the important ques-tion to ask is not why, but what. If a person can determine—
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
22

Part 2: What Are Allergies?
through experience that is con-firmed by testing—what it is thattriggers symptoms, treatment can begin.
There is an extensive list ofknown or suspected allergens.Each person with allergies reactsto specific substances. Someonefor whom pollen is a problemmight have no allergic reaction tomold. People who are allergic tocats are not necessarily sensitiveto dogs. Some foods and medica-tions trigger reactions in people;others do not. Some people canwork in an environment in whichthey are exposed to a chemicalthat triggers an allergic reactionwithin days of their first expo-sure. For other people, this reac-tion might take years to appear.
Anaphylaxis can be caused byexposure to some common sub-stances, such as foods, medica-tions, insect bites, and certainmaterial, such as latex. Exercisecan also produce anaphylacticsymptoms, but not consistently.Allergens that induce anaphylax-is include the following:
• Foods and additives: A traceamount of peanuts, tree nuts(for example, walnuts oralmonds), shellfish, fish, milk,or eggs can trigger an allergicreaction in some people. This
reaction can occur quickly.Additives such as sulfides—found in beer, dried fruit, pick-les, and potato products—canalso cause anaphylaxis, espe-cially in asthmatics.
• Medication: There is anincreased chance of developingan allergy to medication if themedicine is given frequently, in large doses, or by injection.This reaction usually occurswithin hours of exposure.
• Insect stings: Honeybees,bumblebees, yellow jackets,hornets, wasps, fire ants, andharvester ants are the insectsthat cause most anaphylacticsymptoms, which occur withinminutes of the sting or bite.
• Latex: Those who work in thehealth care or rubber industriesare exposed to latex so oftenthat some develop allergic reac-tions to the material. Childrenwho have congenital diseaseslike spina bifida often havemany early exposures duringtheir numerous surgeries. They, too, can develop an aller-gy to latex. Certain foods thatcross-react with latex can trig-ger allergic reactions in thesesame people. These foodsinclude bananas, kiwi, avoca-dos, European chestnuts, pota-toes, tomatoes, peaches, plums,
23

cherries, and other fruits withpits.
A less common type of allergicreaction is called food-dependentexercise-induced anaphylaxis.Symptoms occur after a personexercises within 3 or 4 hours ofeating a certain food. The foodsthat have been known to causethis reaction are wheat, shellfish,fruit, milk, cereal, and fish.Usually, those who experience thereaction already have asthma aswell
as other allergies.
In some cases, a person can experi-ence what is called a biphasicreaction. This happens when ananaphylactic reaction occurs. Afterthe reaction, the symptoms goaway, only to return hours later.For this and other reasons, it isimportant for a person havingthese symptoms to stay at a hospi-tal for several hours following thefirst signs of trouble. Even if med-ical staff indicate that a person is
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
24

Part 2: What Are Allergies?
25
free to go home, it is best to sit inthe hospital lobby for a few hoursjust to make sure that the symp-toms do not return. Doing socould save the person’s life.
How allergies affect the bodyA person can be allergic only tosomething to which he or she hasalready been exposed. In otherwords, an allergic response occursafter an initial exposure to a sub-stance to which the person’simmune system is sensitive. It isreexposure to the substance thatproduces the allergic reaction.
The first time an allergen entersthe body of a person who is likelyto develop allergies, a certaintype of allergen-specific antibodyis produced. This antibody, calledimmunoglobulin E (IgE), trav-els to mast cells in many areas ofthe body. Mast cells are com-monly found in the nose, eyes,lungs, and gastrointestinal tract.IgE antibodies attach themselvesto the surfaces of these mastcells. Each IgE antibody is wait-ing for an invasion by a particular allergen.
Let’s say that a person is predis-posed to developing an allergy tocat dander. The IgE antibody forthat allergen can be found on thesurface of that person’s mast
cells. He or she might develop anallergy to cat dander only. Thismeans that the person’s allergieswill not be triggered by dog orhorse allergens, unless, of course,those allergen-specific IgE anti-bodies are present as well.
Therefore, the IgE antibodies tocat dander have “set up camp” on the mast cells. The very nexttime that the person comes intocontact with cat dander, thisallergen will enter the body. Thewaiting IgE antibodies will cap-ture these cat dander allergens.Once this happens, chemicalssuch as histamine are releasedfrom the mast cells. These chemi-cals, often called mediators, areresponsible for producing thesymptoms of an allergic reaction,such as sneezing and coughing.As the person continues to beexposed to the cat dander aller-gen, the reaction continues.Already inflamed tissues mightgrow more inflamed as thesechemicals draw other swollencells to the area.
The reaction that the person hasdepends upon the location of themast cells to which the IgE anti-bodies have attached. For exam-ple, if an allergen such as pollentouches the lining of the nose, asis common in allergic rhinitis (hay fever), the mucous mem-branes that line the nose will

become inflamed and congested.The person will experience a drip-ping nose and watery, itchy eyes. If the person continues to beexposed to the allergen that trig-gered the reaction, the symptomswill continue the same way.
A person with a very different trigger—for example, a food thatproduces eczema—will experiencesymptoms that affect the skin. For 80% of those with eczema, thiscondition—itchy, reddening, flak-ing, and peeling skin—begins inchildhood. Another skin-specificallergic reaction can occur from an infection, eating a certain food,or taking a certain medication.
Hives can cover the skinwith small or large clus-ters of itchy, red bumps.Children experience aller-gic reactions to food morefrequently than adults do.Over time, a child canbecome less sensitive tofoods that were once aller-gy triggers.
Food can also be a triggerfor anaphylaxis. A personwho is in immediate dan-ger from this severe aller-gic reaction should begiven an injection of epinephrine (adrenaline)as soon as possible.Otherwise, the episodecould be fatal. Epine-
phrine is a body chemical that isproduced naturally by the adrenalglands. Used in injections, a syn-thetic form of the chemical fightsallergic reactions in several ways.Epinephrine opens constricted airpassages, constricts dilated bloodvessels, elevates low blood pres-sure, and halts the swelling that iscommon with hives.
How allergies affect lifestylePeople with allergies suffer fromsymptoms whenever they areexposed to the provoking allergens.In some cases, a person can avoidthe trigger. If shellfish provokes an
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
26
Children haveallergic reac-tions to foodmore oftenthan adultshave. As theygrow older,they may outgrow some of these allergies.

allergic reaction, a person couldsimply avoid exposure to anyform of this food.
With other allergy sufferers,avoiding the allergen is not aseasy. If the trigger is airborne,how can a person avoid exposureif the trees, grasses, weeds, andmolds that thrive from Januaryto December each year are theculprits? Even if allergies are sea-sonal, this still means that formonths each year, the personmust avoid the outdoors. If a per-son working as a nurse developsan allergic reaction to latex, whatcan be done? There are latex-freegloves available, but latex in vari-ous forms can be found every-where within the environment inwhich the person must work. A food allergy can be so severethat simply avoiding direct contact with the food is not sufficient.
Peanut allergies are among themost common allergies in theUnited States. Children rarelyoutgrow peanut allergies. Peoplewho are allergic to peanuts find itdifficult to avoid the many formsof the nut that are triggers. A child with a peanut allergymust avoid exposure to groundnuts, mixed nuts, peanut butter,peanut oil, and peanut flour. All utensils and surfaces that are
used to prepare foods containingnuts must be avoided as well. Theprotein that causes an allergicreaction to peanuts can becomeairborne. Therefore, a child witha peanut allergy can have a reac-tion from sitting in an environ-ment in which peanuts or peanutproducts are cooked or con-sumed—for example, in a cafete-ria in which other children areeating peanut butter or in aChinese restaurant where eggrolls are being prepared.
Allergies of all types have drivenpeople to significantly restricttheir activities. Many people withsevere allergies feel as if everyenvironment holds potential dan-gers. Especially if a child is suf-fering from allergies, it is impor-tant to create an environment inwhich there is little fear of symp-toms and an expectation existsthat the child can meet the chal-lenges of daily living. Usually, a
Part 2: What Are Allergies?
27
Peanut allergiesare among themost commonallergies in theU.S.

combination of avoidance, allergenimmunotherapy, and medication isneeded to give an allergy sufferermore freedom to live a normal life.Many with allergies have had toendure the difficult side effects ofmedications that were used totreat their symptoms. At one time,antihistamines caused so muchdrowsiness that an allergy patienthad to decide whether to suffer theeffects of the allergy and remainalert or suffer the drowsinessbrought on by the medication.Today, many formulas that do not produce drowsiness areavailable.
Newer medications allow peoplewho have suffered life-threatening
allergic reactions to live more normal lives. There was a timewhen a person who had sufferedfrom anaphylaxis could not travelto any area of the world where acertain level of medical care mightnot be available. Some people wereso concerned about the availabilityof treatment that they lived closerto hospitals and ate dinner atrestaurants that were minutesaway from an emergency room.Now that epinephrine injectionsare portable and easy to adminis-ter, a dangerous insect sting orfood allergy can be treated imme-diately. Still, medical help shouldbe sought immediately after epinephrine is used.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
28
Epinephrineinjections aremore portablenow. This makesit easier for people with life-threateningallergies to leadnormal lives.

Part 2: What Are Allergies?
29Huntley-Fenner, continued on next page
Out from theShadow of AsthmaAt first, Gavin Huntley-Fenner’s asthmacame on slowly. While training with hishigh school wrestling team, he grewshort of breath whenever he ran lapsoutside in the cold. Huntley-Fennerdidn’t worry too much, though,because his symptoms were neversevere, and they disappeared in warmweather. A few years later, things grewmuch worse.
By then, his asthma attacks were so severe and frequent that he endedup in a hospital emergency room twice in one month. When he wasnear cats, his symptoms worsened. At times, it was impossible for himto climb a short flight of steps without stopping to rest. Huntley-Fennerdecided he needed to find a way to manage his disease for a lifetime.
When Huntley-Fenner puts his mind to something, the results are oftenimpressive. He earned his doctoral degree from the prestigiousMassachusetts Institute of Technology and began a research careerstudying how children learn to speak and to grasp the concepts ofnumbers and counting. His broad range of skills has made him asought-after business consultant in Southern California, where he nowlives with his wife and two children.
He approached his struggle with asthma with the same deliberate andcareful study.
“My key challenge right now as an asthmatic is that I’m on a lot ofmedication at high doses,” he says. “As I grow older and my diseaseworsens, I’m concerned that there will be less and less flexibility totreat flare-ups.”
So, with his doctor’s blessing, Huntley-Fenner tries to cut down on med-ications whenever possible, all the while being careful not to jeopard-ize his health. “Finding a doctor open to thinking through the problemwith you is important,” he recommends.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
30
His approach seems to be working. For now, Huntley-Fenner’s asthma doesn’t seem to be worsening. To keep his body strong, he seeks out waysto exercise that won’t cause an attack. “I have to be more creative in find-ing ways to keep fit,” he says matter-of-factly. “I can’t run around as muchas I would like with my kids, but we ride bikes. There are neighborhoodsoccer games that would be fun for me to join in, but I can’t. We’re manag-ing well, though. I can run on a treadmill. I can cycle. I can swim.”
For Huntley-Fenner, trying to minimize the impact his asthma has on his family is a main concern. He has worked to reduce the amount of dust and allergens in his home, which can aggravate his asthma. “We no longerhave a dog, we’ve covered our mattresses and pillows [with special cover-ings to reduce allergens], and we’ve put in wood flooring instead of carpets,” he explains.
At the same time, he is concerned that creating such a sterile environmentcould prevent his three-year-old son and eight-year-old daughter from building their own resistance to things that cause allergies. It’s a careful balancing act.
“If you’re allergic or asthmatic and you’re a parent, you might worry, ‘What is the impact of this disease on my children?’” he says. Though he is concerned that his children may develop asthma or allergies, he doesn’tlet those thoughts get the best of him.
With the care of a good doctor, proper medicine, and a healthy outlook,Huntley-Fenner has dealt with asthma head-on—and instead of anxiouslyawaiting another attack, he has pushed it into the background of his busy,fulfilling life.
“I know that asthma poses certain risks for me and my family,” he says,“but I won’t let it overshadow my life.”

31
Part 3: Who Has Asthma and Allergies
Childhood allergies and asthmaIt is estimated that, out of the 17 million Americans who sufferfrom asthma, 5 million of themare children. Childhood asthma is so common that it results innearly 3 million visits to a physi-cian and 200,000 hospitalizationseach year. Asthma often begins in early childhood. Up to 80% of children with asthma showsymptoms of the condition beforethe age of five. The first signs of asthma in infants and childrenare often a cough, a fast or noisybreathing pattern, and chest con-gestion. These asthma symptomscan be so subtle that the childrenmight not even be aware of them.For example, a child might growso accustomed to chest tightnessthat it seems normal. This is why it is crucial for parents totake note of these subtle changes.A parent’s observations could bethe basis for a physician to diag-nose the condition sooner.
Some children will outgrow thedisease, but others will not. It isjust as unclear why asthma starts
as why it goes away. Severe child-hood asthma often goes away, but mild asthma often does not. If asthma occasionally occurs inchildhood, especially as a result of viral respiratory infections,there is a greater chance that thesymptoms will ease with age. Infact, about half of all children whohave chronic asthma will havefewer symptoms or none at all byadolescence. Since older childrentend to get fewer viral respiratoryinfections, this alone mightaccount for fewer asthma attacks.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
32
It is also possible that the asthmasymptoms will remain, but thatthe triggers will change. An olderchild who once suffered from asth-ma due to viral infections couldbegin to experience attacks trig-gered by allergens or environmen-tal factors.
Childhood asthma can lead tomany absences from school. The symptoms of asthma canmake participation in a variety ofactivities difficult for children. Asa result, a child can feel left out. In addition, the symptoms of asth-ma—especially difficulty breath-ing—can leave a child feelingscared. Although having asthma ata young age can lead to restrictingactivities initially, every effortshould be made to help asthmaticslive normal lives. With propertreatment and management, manyyoung asthmatics can excel insports. In fact, a great number ofaccomplished athletes around theworld have been asthmatic. Somehave even competed in theOlympics and for professionalsports teams.
As for allergies, some of the mostserious allergy symptoms that achild can experience are triggeredby foods. Food allergies werereported in Europe as early as thebeginning of the 1900s. Physiciansaround the world have been treat-ing food allergies since the 1940s.Children account for the majorityof those affected by food allergies.In the United States, 6–8% of chil-dren and 2% of adults have foodallergies, and about 100 people dieeach year from food-related ana-phylaxis. According to a recentstudy, teens who have a food aller-gy as well as asthma are morelikely to experience anaphylaxisfor several reasons: They often
Asthma and the Olympics
Many asthmatics compete in the Olympic Games. In fact,1 in 6 of all American athletes competing in 1996 had ahistory of asthma, as did 1 in 5 competing in 1998. Someof these athletes needed to use asthma medication dur-ing competition. In 1994, asthma was most commonamong the athletes who were cyclists and mountain bik-ers. It was least common among those who competed inbeach volleyball, table tennis, and volleyball. Almost 30percent of asthmatic athletes won individual and teammedals, compared with those without asthma, who won28.7 percent.

33
dine away from home; they do notalways carry medications withthem; they might not recognizesymptoms; and even if they do,they might ignore the symptoms.
For both asthma and allergies,mild and severe forms of the con-ditions occur in children andshould be treated at the firstsigns of symptoms. Early, consis-tent treatment is important forseveral reasons. First, it couldprevent the condition from get-ting worse. In fact, there is someevidence that allergenimmunotherapy can actually helpa child outgrow allergies. Second,if symptoms are left untreated,
learning and development can be affected. Third, it is alwaysimportant to give a child what-ever he or she needs to experi-ence life in the fullest, healthiestway possible. If a child is alwayscoughing or struggling to get afull breath, he or she is less likelyto attend school, socialize, or play.Even a child with severe symp-toms should feel as normal aspossible.
To help a child manage asthmaand allergies, it is important forparents, physicians, and schooladministrators to work togetherand keep certain goals in mind:
Part 3: Who Has Asthma and Allergies
Children with asthmaor allergiesshould live asnormal a lifeas possible sothat theydon’t feel left out.

• Reduce or avoid triggers.This means establish a smoke-free, clean environment in whichanimal dander and dust miteand cockroach droppings areminimized. Also, reduce theoverall amounts of dust, mold,and mildew in the home.
• Foster an overall healthylifestyle. Make sure that thechild has a good diet, properrest, and exercise. Also, makesure that all medications areavailable and are used correctly.An asthma care plan should beclearly communicated by thechild’s health provider and givento the parent for posting athome.
• Help the child achieve emotional health. Inspire con-fidence in the child. Give thechild opportunities to achieveand succeed. Encourage thechild to see herself or himself asa healthy person, not a sicklyperson.
• Prevent symptoms fromthreatening normal living.If the child is constantly strug-gling to breathe, it will makeconcentration on schoolwork,friends, and exercise more diffi-cult. With proper managementof symptoms, exercise should beencouraged not just for thechild’s overall well-being, butalso to strengthen his or herupper respiratory system.
• Foster communication to create a supportive environ-ment. Make sure that the prin-cipal, teachers, coaches, andschool nurse are all aware of thechild’s condition and thespecifics of treatment. Makesure that the child is allowed totake medications on scheduleand follow other directions of hisor her asthma care plan. Everyeffort should be made to treatthe child normally. However, allschool personnel should be pre-pared to assist the child in caseof an allergic reaction or anasthma attack.
34
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e

35
Uneven impact of allergiesand asthmaBesides AIDS and tuberculosis,asthma is the only chronic dis-ease that has an increasing deathrate. Between 1978 and 1992, thedeath rate from asthma increased58%. Between 1980 and 1993, thedeath rate for children under 19increased 78%. More females dieof asthma than males, as do moreAfrican Americans and Hispanicsthan whites. Higher rates of asth-ma-related symptoms, hospital-izations, and death amongAfrican Americans and Hispanicsseem in part to be due to poverty,poor urban air quality, indoorallergens, inadequate informa-tion, and a lack of medical care.While African Americans makeup 12.8% of the population of theUnited States, they account for23.7% of the total number ofdeaths due to asthma.
Among Hispanics, Puerto Ricansseem to have higher death ratesfrom asthma than any othergroup. Unfortunately, scientistsdo not yet know why this is so.Recently, in the AmericanJournal of Respiratory andCritical Care Medicine, a studyrevealed that Puerto Ricans hadan annual death rate of 40.9 permillion due to asthma. CubanAmericans had a rate of 15.8, and Mexican Americans a rate of 9.2, per million. If asthma is
properly managed, however, thedeath rates due to the conditioncould decline.
When adequate medical treat-ment is not available to help pre-vent the symptoms of asthmafrom becoming severe, hospital-izations and emergency room vis-its become necessary. In general,more than four times the numberof African Americans are taken toemergency rooms because of asth-ma attacks than those of otherraces. African-American childrenare three times more likely to behospitalized for asthma thanwhite children.
A study published in the Journalof Asthma (July 1999) revealedthat hospitalization rates forasthma in New York City were 21times higher among those wholived in low-income neighbor-hoods and minority neighbor-hoods. Physicians at the NewYork Academy of Medicine stud-ied 107 children with severe orchronic asthma, most of whomwere Puerto Rican or AfricanAmerican. Only 39% of these children were using anti-inflam-matory medications daily.
There appears to be some evi-dence that certain aspects of com-munity life among Hispanics andAfrican Americans account fortheir higher rates of asthma.
Part 3: Who Has Asthma and Allergies

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
36
Every form of air pollution—ozone, sulfur dioxide, acidic airparticles—is more common inurban, minority neighborhoods.High crime rates create stress forthose who live in these areas. In2000, Harvard researchers saidthat in a study of children underthe age of 26 months, childrenwere twice as likely to have physi-cian-diagnosed asthma if theylived in areas with higher rates ofviolent crime and vacant housing.Researchers found that in thesesame areas, children over the ageof two had a 40% increased risk of being diagnosed with asthma.
Residents of high-crime areascannot control the gun violenceand the stress caused by it.
However, there is another asthmatrigger that can be reduced, whichis found inside many householdsin these areas. The NationalInner-City Asthma Study found a relationship between inner-cityresidents and asthma resultingfrom exposure to cockroach drop-pings. If measures are taken toreduce the number of cockroachesin a home, this will decrease thenumber of droppings that anasthmatic is exposed to in bed-sheets, food, bathroom towels,and carpeting.
A similar program in Seattle forlow-income children with asthmaused community-based lay healthworkers who focused on multipletriggers, including dust mites,
Air pollution is more common in urban, minority neighborhoods.

house dust, mold, moisture, environmental tobacco smoke,roaches, and rodents. This one-year Seattle Healthy Homesintervention showed a reductionin both the number of days withsymptoms and emergency clinicvisits, as well as a significantlyimproved quality of life for caregivers.
Societal impact of allergiesand asthmaIn the United States, allergies are the sixth-leading cause of allchronic diseases. Allergies candevelop at any age, even in theelderly. There are 50 million chil-dren and adults affected by aller-gies in this country alone, approx-imately 35 million of whom sufferfrom hay fever. The financialimpact of hay fever in the UnitedStates in 1996 totaled $6 billionby itself. And, in 1998, increasedabsenteeism and reduced produc-tivity due to allergies cost U.S.companies more than $250 million.
With tens of millions of sufferersin this country alone, allergiesare now considered a serious disorder. Up to 10% of the popula-tion may be at risk of allergicreaction to medications. Food-induced anaphylaxis results in30,000 visits to the emergencyroom each year. Approximately
10–17% of people working inhealth care have an allergy tolatex. Up to 4% of the populationhas experienced anaphylaxis thatwas caused by an insect sting.
Asthma also has serious conse-quences. If asthma is not man-aged properly, the cost of treatingthe condition increases. Accordingto the Asthma and AllergyFoundation of America, over thelast 10 years the costs that result-ed from adults missing workbecause of their own asthmaquadrupled. The number ofadults who stayed home to carefor children with asthmaincreased lost work time costs in1998 by $3.8 billion. That sameyear, overall costs for visits tophysicians, hospitalizations, andmedications that resulted fromasthma symptoms totaled $7.5billion. Of this total, the greatestportion was spent on hospitaliza-tions. Asthma symptoms result in1.8 million emergency room visits,10 million visits to a physician’soffice, and half a million hospital-izations each year. Among chil-dren aged 5 to 17, asthma symp-toms are the leading cause ofabsence from school—a loss ofmore than 10–14 million schooldays each year.
Asthma can also have a seriousfinancial impact on a family.When a child has to stay home
37
Part 3: Who Has Asthma and Allergies

from school because of asthmasymptoms, a parent often has tomiss a day of work. Repeated tripsto a physician’s office or emergencyroom or multiple stays in a hospi-tal can be costly even when a fami-ly is insured. When a family isuninsured, these expenses can bedevastating.
The best way to avoid the highcosts of asthma and allergies is tohave the conditions diagnosed andtreated as early and as consistent-ly as possible.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
38
Asthma symptoms result in 10 million doctor visits and 10–14 millionschool absences each year.

39
Part 3: Who Has Asthma and Allergies
Food Allergies:Avoiding a Recipe for Disaster
While spending the day with her grandmother,one-year-old Natalie Kalitsi suddenly beganacting strangely. First the little girl grew verysleepy; then red blotches broke out all overher body. She seemed to struggle to breathe.An ambulance rushed her to the hospital,where doctors questioned her grandmother:What had Natalie eaten that day?
Nothing unusual—but Natalie did have her first bite of fish. That small biteof fish was enough to almost kill her.
Today Natalie is an active, happy three-year-old with big brown eyes. Likeother toddlers, she loves going to preschool, playgrounds, and birthday par-ties. But wherever Natalie goes, a special shot that contains powerful medi-cine always follows. If Natalie accidentally eats seafood, peanuts, or dairyproducts—all of which give her allergic reactions—the shot will help herbreathe until she can be taken to a hospital.
“At first it was hard getting used to, but it’s routine now,” says Gale Kalitsi,Natalie’s mother. “Everywhere Natalie goes, I pack a special lunch box forher—it’s like a game. We even do it at birthday parties—or when she goesto her cousin’s house.”
All parents try to look out for their child’s safety, but being the mother of aseverely allergic child means that Gale must be extra careful. Before Nataliebegan to attend a preschool near her home in Bethesda, Maryland, Galecalled meetings with her teachers and the school’s director to make sure thatthey understood how serious allergies can be.
“Until you have an experience with food allergies, you don’t know howdeadly allergies can be,” says Gale. “In Natalie’s case, it can close down herair passages and kill her. Everyone who comes in contact with her needs tobe able to read food labels. And because children like to share food, or they may kiss her and have peanuts on their lips, we need to be especiallycareful.”
Kalitsi, continued on next page
Printer:
Strip in photo fromnegative provided.

So a special rule was set for Natalie’s classroom: No students could bring inpeanut-butter sandwiches for lunch.
By now, Gale is an expert at reading the labels of everything Natalie eats, butin the beginning food labels were filled with confusing words. For example,Natalie is allergic to milk, but how could Gale know that many unfamiliar-sounding ingredients such as “casein” or “whey” contained milk? Gale saysthat an organization called the Food Allergy and Anaphylaxis Network (1-800-929-4040) has been an enormous help and has even provided her with specialnote cards listing ingredients that aren’t safe for Natalie.
Gale and her husband have learned so much about food allergies that whentheir second daughter was diagnosed with an allergy to wheat, they felt confi-dent of their ability to handle her special needs. “You really need to becomean educator and a campaigner for your child,” says Gale.
But Gale and her husband recently learned they’re not the only ones watchingNatalie’s diet. Now that Natalie is growing up, she can speak up for herself.
“At the age of three, Natalie can tell you what foods make her sick, and shecan tell you what she can have,” says Gale proudly.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
40

Diagnosing and treatingasthmaWhen a physician completes anevaluation to determine whethera person has asthma, severaltests are done. In addition to aphysical exam, the physician willask questions about the person’sgeneral health and symptoms.
If the person is experiencingsymptoms at the time of theexamination, the physician willtry to rule out certain conditions.It is important to distinguishasthma from bronchitis andpneumonia, for example. Bothbronchitis and pneumonia arecaused by bacteria and can betreated with antibiotics. Butantibiotics do not work for asth-ma. It is equally important thatthe physician zero in on the spe-cific physiological causes of thesymptoms. That is, whichprocesses in the person’s body areproducing a cough or a wheeze?Different physiological causesoften respond to different treat-ments. For example, bronchocon-striction will require a differentform of treatment than airwayinflammation.
Even if it appears that no symp-toms are present at the time ofthe exam, pulmonary functiontests can detect even minorblockage or airway obstructions.These tests can help the physi-cian determine the cause of theobstruction, if there is one. Thephysician might also have thepatient perform breathing testsbefore and after exercise to recordany differences in breathingcapacity. These tests can be con-ducted either in a physician’soffice or outdoors and are impor-tant for a person who seems to besuffering from exercise-inducedasthma. 41
Part 4: How Can Asthma Be Treated and Prevented?
During officevisits, a doctoror nurse maytest a patient’sability tobreathe tohelp figure out if he or she has asthma.

42
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
A spirometer measures the abili-ty of a person to breathe out airfrom the lungs. If, after exertion,the person shows at least a12–15% decrease in the volume ofair blown out in one second—called the forced expiratoryvalue (FEV 1)—exercise-inducedasthma could be the cause.Outdoors, a portable spirometercan be used.
A device called a peak flowmeter can also measure breathingcapacity. If a peak flow meter isused, a 15–20% decrease in thevolume of air blown out indicatesthat a patient is likely to have
exercise-induced asthma. Peakflow meters may also be used todetermine when more or a differ-ent medication is needed.
Parents can help a physician eval-uate whether their child suffersfrom asthma. Perhaps they havenoticed that their child tends towithdraw from activities thatrequire physical exertion. Maybetheir child tends to cough orwheeze late at night or during acertain time of the year. Theremight be specific times when theirchild’s breathing sounds heavy ornoisy. These can all be indicationsof asthma.
A doctor may want to use a spirometer totest how much air anasthmatic can exhale.
The computer that thespirometer is hookedup to draws a graph
to show whether thepatient exhales thesame amount eachtime (normal lung
function) or less each time (asthma
or another lung condition).

Just as each person’s triggersare different, the types andseverity of symptoms vary.
This is why it is vital that eachperson understands the goals oftreatment, the approach torelieving symptoms, and his orher responsibilities for maintain-ing good health. For youngerpatients, parental involvementin treatment is crucial. As chil-dren mature, they should begiven more responsibility fortheir own asthma care.
Each person’s asthma care planis unique. The person beingtreated should actively partici-pate in making decisions abouthis or her asthma care. The bestway to do this is to learn asmuch as possible about the dis-ease. Whatever the approach totreatment is, remember the fol-lowing guidelines:
• If any part of the therapy is noteffective, discontinue it underyour doctor’s guidance.
• Do what works, unless therisks of the treatment exceedthe benefits of it.
• The side effects of the treat-ment should not be worse thanthe symptoms of asthma.
• The asthma care plan shouldbe simple and easy to follow.(An example is shown inAppendix 1 on page 72.)
Part 4: How Can Asthma Be Treated and Prevented?
43
The inhaler dispenses abronchodilaterdrug thatwidens the airways in the lungs.
Components for ManagingAsthmaIn its National Asthma Education andPrevention Program, the NationalInstitutes of Health outlined four maincomponents for managing asthma:
• Medical personnel should use objec-tive tools such as the peak flowmeter and the spirometer to assesshow severe a patient’s asthma is andthen monitor treatment accordingly.
• Patients should avoid or eliminateenvironmental factors (for example,secondhand smoke, certain foods,strenuous physical activity) that trig-ger asthma attacks.
• Patients should consult a physicianto obtain proper medications. Thegoals are to manage flare-ups in theshort term and to prevent airwayinflammation in the long term.
• The patient, the patient’s family,and health care providers shouldform a partnership to define andimplement the best treatment plan.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
44
Preventing and controllingasthmaIn trying to prevent or controlasthma attacks, it is important tokeep in mind certain overall goals:
1. Chronic symptoms such aswheezing and coughing must beminimized.
2. There should be access to dailytreatments that allow for nor-mal breathing most of the time.These are often called “con-troller medications,” such assteroid inhalers.
3. Every asthmatic should try tomaintain normal activity levels,which include exercise.
4. Symptoms should be treated assoon as they appear, in order to minimize emergency room visits and hospitalizations.These treatments are in addi-tion to controller medicationsand are often called “relievermedications,” such as albuterolinhalers.
It is never safe to withhold treat-ment. Asthma is not a conditionthat a person should hope to out-grow. Having trouble breathing isnot something that will get betteron its own. It is a symptom thatneeds to be treated. It is alwayssafer to assume that narrowingairways will not open on theirown. Mucus that blocks the pas-
sage of air to and from the lungswill not loosen on its own. If anasthmatic is under the care of aphysician, any changes—improve-ments or setbacks—will be notedand treatments adjusted.
Even someone with an active formof the disease could experiencebrief periods without symptoms,especially as a result of treatment.This does not mean that it is safeto stop using the medications. Theopposite is true. The medicationshave helped the person remainsymptom free. The best way toincrease the number of symptom-free days is to remain under thecare of a physician and followtreatment instructions.
Intervention (or “rescue”) meas-ures can be used to control andrelieve asthma symptoms oncethey start. Controller medications,also known as maintenance med-ications, can be used to preventasthma symptoms from occurring.Ideally, controller medications canlessen the need for rescue medica-tions. If some attacks can be pre-vented, then there will be fewersymptoms to control. Once anasthma attack starts, its severityusually can be controlled. Whethera person has mild or severe asth-ma, there are ways to manage thecondition. If asthma symptoms arenot managed properly, a mild casecan become severe and a severe

Part 4: How Can Asthma Be Treated and Prevented?
case can become fatal. Learn torecognize the warning signs thatan attack might be getting worse.These warning signs can be dif-ferent for each person.
Some asthma sufferers receivetreatment only in an emergencyroom. Unfortunately, due to thehigh costs of health care, thismay be a way for some people toafford treatment. But emergencycare is not the best way to treatasthma. An asthmatic needsongoing care from a physician,not just rescue measures. In addi-tion, if only the flare-ups aretreated, then controller medica-tion cannot work to preventfuture attacks. The symptomswill continue and will reach a crisis state before treatment issought, which is bad for the per-son’s overall health.
It is vital that an asthmatic usethe correct medication for his orher condition. It is also importantto use the medication as directed.Take the dosage that is pre-scribed—no more and no less.In some cases, medications needto be used daily, even on dayswhen there are no symptoms.Steroid inhalers, for example, prevent symptoms only if useddaily, as directed.
Many medications are effective in preventing and controllingasthma. Some of them are calledanti-inflammatories. They dowhat their name suggests: Theyreduce the swelling of the air-ways, so that more air can travelto and from the lungs. Inhaledmedications have the advantageof being administered directly tothe area that is inflamed or
45
An asthmaticneeds ongoingcare from adoctor, not justemergencytreatment at a hospital.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
46
obstructed. There are severaldevices used to administer inhaledmedications. Many metered doseinhalers (MDIs) use a chemicalpropellant—usually a chlorofluoro-carbon (CFC)—to force medicationout of the inhaler. Pharmaceuticalcompanies are in the process ofdeveloping other MDIs with pro-pellants that, unlike CFCs, do notdamage the ozone layer. Two typesof inhaler that deliver medicationwithout using CFCs are rotaryinhalers and dry-powderinhalers.
A device called a nebulizer deliv-ers a fine liquid mist through amask that is placed over the noseand mouth or through a mouth-piece. These devices make inhalingmedication easier, especially forinfants, children, and those unableto use a standard inhaler. Somenebulizers are small and portable,have battery packs, and can beused for travel.
Using an inhaler can be difficult at first. An asthmatic should ask a health care provider to demon-strate how to use it properly.Often, it is a challenge to directinhaled medication to the lowerairways accurately; it tends to get sprayed onto the back of thethroat. A spacer—a device thatfits on the end of an inhaler andprovides a holding chamber andone-way valves—can help adminis-
ter inhaled medication withgreater accuracy. Never overuse an inhaler.
Inhaled medications often causefewer side effects than oral med-ications do. The side effects associ-ated with inhalers vary fromheadaches to hand tremors.Sometimes these side effects canimpair learning in children. Whena child has a headache, it can bedifficult to concentrate. Handtremors can influence a child’shandwriting. It is important thatboth teachers and parents beaware of these side effects andmake an effort to note any thatoccur. In many cases, the type ordosage of medication can beadjusted to prevent side effects.
People who suffer from exercise-induced asthma can benefit fromusing a reliever-type medication,such as a short-acting bronchodila-tor, 15 minutes before starting anactivity. In one study, this form ofinhaler was effective for up to 4–6hours after inhalation in 80–90%of patients. Albuterol, pirbuterol,and terbutaline are among themedications in this category. In addition to preventing attacks,these inhalers can relieve symp-toms after they start. A longer-act-ing inhaler can provide up to 12hours of relief. If a child with exer-cise-induced asthma uses a longer-acting inhaler before leaving for

Part 4: How Can Asthma Be Treated and Prevented?
47
school in the morning, it is possi-ble that there will be no need foradditional medication during theday.
Warming up before exercise and warming down after doesmore than just stretch muscles.For those with exercise-inducedasthma, it is another way to helpprevent the chest tightness thatis caused by cold air suddenlybecoming warm in the lungs.
Each person should play an activerole in his or her asthma treat-ment plan. This is easy to do:
• Know your asthma care planand when to use your controllerand reliever medications.
• Learn both the brand names and generic names of the med-ications that are prescribed.
• Write down any side effects that result from taking thesemedications.
A young girl breathes into the face mask of a nebulizer to relieve her symp-toms of asthma. The nebulizer delivers a fine spray of an asthma drug into theface mask and then into the throat and bronchial tubes. The drug is usually abronchodilator, which reduces the constriction of the airways to the lungs thataccompanies an asthmatic attack. Nebulizers are often used to treat emergencyasthma attacks. Most patients find them easier to use than conventionalinhalers.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
48
• Report any changes in symptomsor triggers.
• Ask a health care provider anyquestion that arises, and shareany concerns.
Apart from medication, someadjustments can be made to bothindoor and outdoor environmentsto help prevent asthma attacks.According to the American LungAssociation, the best environmentto live in is smokefree. This isespecially important in homeswith children. In fact, researchshows that the children of smokersare twice as likely to have asthmaas the children of nonsmokers. Asa rule, it is best to avoid an envi-
ronment where secondhand smokeis common. Pregnant womenshould not smoke. Women who dosmoke during pregnancy can givebirth to babies who have narrowed airways.
There are many forms of indoorand outdoor pollution. Wheneverpossible, it is best to avoid all ofthem. Indoors, many children and adults are sensitive to aller-gens that are known to cause asth-ma. These allergens include every-thing from cockroach and dustmite droppings to pet dander andmold. Cockroaches can be con-trolled or eliminated by using safepesticides. Dust mites can be kept under control by doing sev-eral things regularly: Wash bed-ding in hot water (130ºF or high-er). Keep floors free of dust by vacuuming with a machine thathas a special filter. Avoid placingcarpets, rugs, drapes, and stuffed
Asthma MedicationsMedications that are often prescribed to treat asthma include the following:
Anti-inflammatories (cromolyn and nedocromil are nonsteroidal examples)—These medications reduce swelling in the airways and lungs. Anti-inflamma-tories are not as strong as inhaled corticosteroids, but they cause fewer sideeffects.
Corticosteroids—Available since 1948, these steroidal, anti-inflammatorymedications are prescribed in different forms. Creams can be applied to theskin to treat rashes. Inhalers are often recommended for asthmatics withdaily moderate or severe symptoms. Pills are prescribed for those with severeasthma. Corticosteroids decrease swelling of the bronchial tubes, reduce theamount of mucus the body produces, and calm the airways. It is important to use these medications even on days when there are no symptoms, becausethey can help maintain healthy airways.
Bronchodilators (theophylline and anticholinergics)—Often called “rescue”medications, they open the bronchial tubes so that more air can travel toand from the lungs. These medications relieve coughing, wheezing, shortnessof breath, and difficulty breathing. They are available as inhalers, tablets,capsules, liquids, or injections. They shouls not be overused. If a patient usesmore than one canister (of an inhaler) a month, a new treatment planshould be considered. One exception is a long-acting medication—called salmeterol—which is designed for daily, preventative use.
Anti-leukotrienes—These are medications taken in pill form which fight the chemicals that cause airway inflammation and which make airways lesssensitive.

Part 4: How Can Asthma Be Treated and Prevented?
49
animals in bedrooms. Irritantssuch as perfumes and strongcleaning agents or fragrances,which are found in many house-holds, should also be avoided.
Outdoors, high levels of pollenand mold can trigger asthmasymptoms in many people. Smokefrom factories and exhaust fromtrucks can also be harmful. Ondays when the air quality is con-sidered poor—often, days whenozone levels are high—doctorsmay tell patients to restrict physical activity or even to stayindoors.
Even for a person who suffersfrom occupational asthma, thereare treatments that can providesome relief. Special masks (respi-rators) can also be used to filterout allergens in the workplace.Many workers—from bakers tohairdressers—are exposed to sub-stances that trigger asthmasymptoms. After the trigger sub-stance is identified, it is impor-tant that the worker’s exposure toit be eliminated. If medications orrespirators don’t solve the prob-lem, the worker may have tomove to a location where the trig-ger substance is not present. If aworker is removed from exposurewithin 1–2 years of developingsymptoms, his or her asthma ismore likely to be reversible.Employers should monitor the
levels of these substances and tryto keep the levels low. Employerscan check for early signs of occu-pational asthma by testingemployees who are regularlyexposed to harmful substancesand ultimately can seek out non-harmful alternatives.
The relationship betweenallergies and asthmaScientists have long known thatthere is a connection betweenallergies and asthma. Many people who have one conditionwill develop the other. In fact,asthma is sometimes called anallergic disease. Both allergiesand asthma cause airway inflam-mation and narrowing of air pas-sages. In an asthmatic, this reac-tion might be caused by a respira-tory tract infection. In a personwith allergies, exposure to aninhaled allergen might cause thesame symptoms.

Allergic rhinitis (hay fever) is con-sidered a risk factor for developingasthma. According to the AmericanAcademy of Allergy, Asthma andImmunology, up to 78% of asth-matics also have allergic rhinitis.The symptoms of both conditionscan be triggered by allergens thatare either seasonal or year-round.Pollens, molds, animal dander, and dust mite and cockroach droppings are among the mostcommon trigger allergens. Somepeople have seasonal allergicasthma, a condition that occursover an extended period when high levels of allergens are common in a particular region of the country.
Many people who suffer from allergies will develop asthma.More than 50% of people who haveeczema will become asthmatic.People who have symptoms offood-dependent exercise-inducedanaphylaxis are often asthmaticsas well. Those with asthma,eczema, or allergic rhinitis are atgreater risk of having anaphylaxisat some point in their lives. Thissevere allergic reaction can occuras a result of exposure to foods,medications, latex, or insect stings.
The connection between allergiesand asthma can help physicians intreating both conditions. Forexample, the majority of asthmaattacks are triggered by allergicreactions. This means that if theallergic reactions can be controlled,the number of asthma attacks can be reduced. Many people with allergies are likely to developasthma. This means that a physi-cian should look for the early signs of asthma in such people and testtheir breathing capacity regularly.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
50

51
Part 4: How Can Asthma Be Treated and Prevented?
The Case of theUnusually HighAsthma Rates
Alexander Ortega has an inquisitive mind.Like a modern-day Sherlock Holmes, helikes to sift through facts and ponder difficult questions. A clue here, a trailpicked up there, and suddenly, the piecesof a tough puzzle all fall neatly into place. But Ortega isn’t a detective—he’s an assistant professor of epidemiology andpublic health at one of the country’s mostprestigious universities, Yale University inNew Haven, Connecticut.
Ortega’s work, however, involves seeing patterns that aren’t obvious tomost people. Right now, he’s trying to uncover the mystery behind thesky-high rates of asthma in Puerto Rican children.
Puerto Rican children have the highest asthma rates of children anywhere,with 30 percent of kids on the island suffering from the disease. Elevenpercent of children who are of Puerto Rican descent, but live in theUnited States, are also afflicted.
What Ortega wants to know—and hopes to find out—is whether thosekids are truly suffering from asthma or whether some of them have beenmisdiagnosed.
“There is a strong association between anxiety disorders in children andasthma—more specifically, to panic disorders and separation anxiety,” hesays. “The typical panic attack’s symptoms are identical to the symptomsof an asthma attack: shortness of breath, chest tightness, and wheezing.”
Could it be that thousands of children are really suffering panic attacks oranxiety, but are being treated for asthma? If that’s the case, Ortega wor-ries that the underlying mental health problems in a generation of chil-
Ortega, continued on next page

52
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
dren aren’t being treated—and, like a domino effect, their mental health problems could worsen with time and affect their own children and families.
But that isn’t the only issue Ortega is trying to sort out. If, indeed, manyPuerto Rican children are suffering from anxieties and not asthma, thenwhy aren’t doctors identifying the real problem?
One reason could be that poor children don’t have equal access to qualitymedical care and that white children in general tend to get better treat-ment. “We know that Hispanic and black kids, particularly those who live inthe inner city and are poor and on Medicaid, are much more likely to beseen by residents or non-board-certified pediatricians,” Ortega reports. Onequestion he hopes to examine is whether doctors seem more willing toreport that a child has asthma if that child is black or Hispanic.
Ortega—who himself has seasonal allergies and “wheezes in April andMay”—says that many people, upon hearing of his work, assume that he is also Puerto Rican. “Actually, I’m Mexican-American,” he notes. Growingup, he crisscrossed the United States as a “military brat,” living in Honoluluand New Mexico before attending the University of New Mexico to studyeconomics and then the University of Michigan to receive his Ph.D. in epidemiology.
Ortega hopes to be on the move again soon: He is hoping to receive fund-ing for a grant that would allow him to focus on 1,000 kids on the island ofPuerto Rico in an intensive, three-year study. That will give him a chance tocollect more clues as he keeps digging into the complicated issue of thoseunusually high asthma rates.

53
Part 5: How Can Allergies Be Treated and Prevented?
Diagnosing and treatingallergiesWhen a physician is evaluating a person for allergies, there areseveral steps involved. First, thepatient’s history is taken. Then,the patient is examined. Depend-ing on the patient’s symptoms,several tests might be done.Since some medications (espe-cially antihistamines) can affecttest results, a person should askthe health care provider whichmedications should be stoppeddays before the testing is to takeplace.
Skin (scratch or puncture)testing. In this test, a variety of substances that are commonto the region in which the personlives are evaluated. Tinyamounts of fluids containingallergens such as pollen, animaldander, dust mites, and moldsare placed just under the surfaceof the skin. Within 15–20 min-utes, swelling occurs at the siteof any substance to which theperson has an allergy. The sever-ity of the reaction can indicatethe person’s level of sensitivity.
Virtually painless, this form oftesting offers immediate resultsand almost no risk of seriousallergic reaction. This test isusually used to assess reactionsto respiratory allergens.
Intradermal testing. Thesetests are similar to scratch orpuncture tests, but are slightlymore involved. Tiny amounts ofallergens are injected under theskin. Intradermal tests are oftendone if the scratch or puncturetest results are not complete or useful.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
54
Blood (RAST) testing. In thesetests, a person’s blood is combinedwith an allergen to determinewhether any IgE antibodies react.If there is a reaction, there is likely an allergy to the tested substance. Although slightly moreexpensive than skin tests, this testis relatively painless, offers fastresults, and provides almost norisk of serious allergic reaction.Blood testing is often used to evaluate reactions to insects andmedications in people for whomskin testing is not an option.
Patch testing.For this type of test,allergen-specificadhesive patches areplaced on a person’sskin and left for 72hours. The sites thatshow swelling orredness indicate anallergic response.This form of testingis commonly used toassess reactions tometals and cosmeticadditives.
Provocative testing. This type of testing is also called challengetesting. Usually, the substance inquestion is administered in aneffort to provoke symptoms gradu-ally. A trace amount of the allergenmight be administered in anaerosol spray. The person’s reac-tion to the allergen indicates to
the physician both the nature of and the severity of the symptoms.Provocative testing can be uncom-fortable. Severe allergic reactionscan occur.
An infant’s sensitivity to a food oreven a food allergy might be diag-nosed at home first. If a parentknows that there is a family histo-ry of food allergies, there is a wayto avoid having an infant experi-ence full-blown symptoms. Bygradually introducing smallamounts of new foods—one at atime—parents can isolate a reac-tion. If a few foods are groupedtogether in a single meal, it is farmore difficult to figure out whichone is causing the reaction. If,however, a parent already suspectsthat a child has a food allergy, it isbest not to test this suspicion anyfurther at home. Safer testing canbe done in an allergist’s office.
A person can be treated for aller-gies, but not cured. The range oftreatment options provides somerelief for most people. As men-tioned earlier, one common form of treatment involves ongoingallergen immunotherapy (alsocalled allergy desensitization injections). Those who suffer fromreactions to airborne allergens and insect stings find this form of treatment quite beneficial. Over time, a series of injectionscontaining the offending allergensis given in an effort to build

Part 5: How Can Allergies Be Treated and Prevented?
55
the immune system’s defensesagainst them.
When a person first begins aller-gen immunotherapy, a very dilut-ed form of the allergen compoundis given. Gradually, more of thesubstance is added to the injec-tion. Eventually, the allergistdetermines that the optimal dosehas been reached. The allergistcould also determine that the person is at risk of developing an allergic reaction if the injec-tions continue. Whatever thedetermination is, at this point the therapy ends.
The entire process of allergenimmunotherapy can last foryears. There is some evidencethat this type of therapy worksby tricking the immune system.As increased amounts of theallergen are injected, the immunesystem starts to produce a block-ing antibody (IgG). The IgG anti-body competes with the allergyantibodies (IgE) for the allergen,takes it over, and then does twothings that halt an allergic reac-tion: It prevents the mast cellsfrom activating and it stops therelease of histamines.
Most of the oral medications thatare used to treat allergies fallinto two categories: antihista-mines and decongestants.Antihistamines prevent a
histamine—a chemical that thebody produces during an allergicreaction—from taking effect.Antihistamines are availableover-the-counter in tablet and liquid form; they are also avail-able as tablets, liquids, and injec-tions with a prescription. Decon-gestants work by shrinkingblood vessels and decreasing fluidleakage so that nasal congestionis reduced. Both liquid and tabletforms are available as over-the-counter and prescribed medica-tions. Often, antihistamines anddecongestants are combined in asingle medication to address agreater number of symptoms.
For an acute allergic reactionthat involves a great deal of con-gestion, a physician might recom-mend a decongestant in the formof drops or a nose spray. Theover-the-counter form of medica-tion should not be used for morethan three or four consecutivedays. Otherwise, it can actuallyincrease nasal congestion. A pre-scription form of this medication

can be used for a longer periodwithout producing this side effect.
Nasal steroid inhalers or sprayscan offer fast relief by reducinginflammation and swelling, as wellas by slowing the rate at whichhistamines are released. Thesesprays deliver a very fine mistdirectly into the lining of the nose.They temporarily constrict theblood vessels in the swollen tissueswithin the nose. They also tem-porarily open a larger passage toallow for the free flow of air. Whenthe effects of the spray wear off,the swelling returns. Sometimes,the swelling has grown worse.When this happens, most peoplejust reuse the spray. Unfortu-nately, a series of brief periods ofrelief can lead to longer bouts ofcongestion. It is important to notethat decongestant nasal sprays canbe overused. If a person does over-use these sprays, his or her heartrate can increase and blood pres-sure can rise.
The good news is that most allergysymptoms can be treated easilyand safely. The bad news is that,on rare occasions, an allergic reac-tion can be deadly. As we discussedearlier, anaphylaxis is a severe,sometimes fatal, allergic reaction.It is usually treated with an injec-tion of epinephrine, and antihista-mines and steroids are also given.The sooner the allergic person getstreatment, the less severe the
symptoms will be. Epinephrine can stop the progression of ana-phylaxis; antihistamines andsteroids cannot. Antihistaminesand steroids should never be giveninstead of epinephrine, because,while they can help recovery, they cannot reverse the symptomsof anaphylaxis.
Often, a person who has a severefood allergy learns about it onlyafter exposure to the trigger. Suchexposure can happen as a result of breathing in or eating the sub-stance. After the symptoms aretreated, contact an allergist for follow-up care. The allergist canhelp determine what triggercaused the reaction. This is veryimportant in preventing anaphy-laxis from happening again.
Although triggers that are foodsmay be easy to avoid, it might betrickier when the allergen is a foodadditive. This is why it is crucialto be under a doctor’s care. If ana-phylaxis happens again, the per-son might already have an injec-tion of epinephrine handy. Usingthis medicine will keep symptomsunder control until the person canbe taken to a hospital. An allergistcan even offer treatments that canhelp build immunity to some trig-gers. For example, if anaphylaxisis triggered by insect stings, ongo-ing allergy shots can help buildtolerance to the venom.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
56

Part 5: How Can Allergies Be Treated and Prevented?
57
Here are some suggestions for what can be done to assistsomeone who is experiencing anaphylaxis:
1. Ahead of time, learn enoughabout the symptoms to recog-nize when the reaction is occurring.
2. Get medical help as soon aspossible.
3. Do not allow a person who isundergoing this type of reactionto drive.
4. Even if the person receivestreatment at the location wherethe reaction occurred, it is vitalthat he or she go to an emer-gency room, where the condi-tion can be monitored.
5. Make a note of what could have caused the reaction andwhat amount of time elapsedbetween exposure and reaction.Having this information couldhelp to prevent a future reaction.
Preventing and controlling allergiesFor most allergies, preventing orcontrolling symptoms requires afew simple steps. Depending onthe severity and frequency of thereaction, almost all symptoms canbe minimized by changes in envi-ronment and the person’s behav-ior. Once the triggers are known,
they should be avoided. Changesto the home, school, and workenvironments can significantlyreduce the person’s exposure to a variety of allergens.
The most important behavioralchange that a person can make tohelp prevent and control allergiesis to use all available methods oftreatment. Allergen immunother-apy can help build toleranceagainst specific allergens. Othermedications can help prevent orcontrol symptoms that do recur. A person who suffers from aller-gies can also improve his or hergeneral health by eating nutri-tious foods, exercising regularly,and getting enough rest.
At the very beginning of life andduring early childhood, measurescan be taken to help pre-vent some allergies.Researchers have knownfor some time that breastmilk is far more nutritiousfor infants than formula,cow’s milk, or soy milk.Studies show that infantswho are breast-fed are lesslikely to develop allergies toa variety of substances. Thelower incidence of allergy inchildren who were breast-fed might result from themother’s immunities beingtransferred to the childthrough the breast milk.

Another way to help lower the riskof allergy—specifically, peanut ornut allergy—involves not exposingchildren under the age of three topeanut products. Allergists believethat one reason that there are somany children in the UnitedStates with peanut allergies mightbe the extensive early exposurethey have to peanuts. Many youngAmerican children regularly eatfoods that contain peanuts orpeanut products.
In the case of life-threateningallergic reactions, preventionis possible only if the trigger canbe completely avoided. This is difficult to do, so additional measures must be taken to controlsymptoms. If a person has had an anaphylactic allergic reaction in the past, a physician might suggest carrying a supply of epinephrine at all times.
Regardless of whether the triggeris or is not known, the symptomscertainly are. Having a supply of a medication that can offer imme-diate relief will help get the symp-toms under control until the per-son can be taken to a hospital.Since this medication is given inthe form of an injection, the personwho carries it must know how toadminister it. However, becausethere is a possibility that the per-son having the reaction might beincapable of completing the injec-tion, a companion should alsoknow how to administer it.Another measure that can helpsave the life of a person known to have anaphylactic reactions is even easier to do: Have the per-son wear a medical bracelet thatindicates to medical personnel andothers the nature of the person’s allergic condition and any possible triggers.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
58

Part 5: How Can Allergies Be Treated and Prevented?
59
A Little Bit ofDiscomfort BringsReliefEvery day when Erminia Cardenas goes towork, she performs a simple test that canchange the lives of her patients.
Cardenas, who is a licensed vocational nurse inHouston, uses tiny prongs to prick the skin onher patients’ backs. There are 80 prongs in all,and each contains something different—fromgrass pollen to mold to cat dander.
The procedure is often the first step in unlocking the mystery of what iscausing her patients’ unexplained sneezing fits, watery eyes, and even difficulty in breathing—all symptoms of allergies. For Cardenas’s patients,the test is fascinating: Could the cause of all their problems be somethingas simple as the goose-feather-stuffed comforter on their bed, or could the culprit be a type of tree that lines the streets in their neighborhood?
If one or more of the pricks begin to itch, swell, or turn red, Cardenas hasthe answer. Even though the prong pricks cause a bit of discomfort, finallylearning the cause of their difficulties can be a huge relief to patients.
“We have one patient, a young man who works on the golf course at acountry club, who came to us because he had started sneezing every timehe went out on the course,” says Cardenas. “When we tested him, he wasallergic to all the grasses and tree pollens that surrounded him on the golfcourse—he was a mess, poor thing! He said, ‘I can’t give up my job,’ so weput him on shots and he’s doing very well.”
Cardenas, whose ancestors are Mexican, considers herself lucky becauseshe doesn’t have any allergies. Neither did her parents, which was fortu-nate, since they were migrant workers who spent a lot of time outdoors in the cotton fields. As a baby, Cardenas traveled with her parents to thefields. “If they ever had allergies, it wasn’t severe—not like what thepatients I see have,” she says.
Cardenas, continued on next page

But her son suffers from watery eyes and sneezing when the season changesevery year from summer to fall. The good news is that, with treatment, evenpeople who suffer from severe allergies can control their symptoms.
“Some of our patients can even give themselves shots at home, if their symp-toms are milder,” says Cardenas.
Cardenas, a mother of three who returned to nursing after taking time off to raise her children, sounds positively maternal when she talks about herpatients. She worries that many of the patients she sees—who range from airline pilots to lawyers to fellow nurses—have such demanding jobs that theirsymptoms can worsen because of the pressure. “Sometimes because they’re sostressed at work, they don’t take care of themselves,” she says. “I think stresscan aggravate allergies.”
So can the change of seasons—and Cardenas, who talked about her job on abeautiful March day when the spring’s first flowers were pushing through theground, knew she would be in for a busy time at work.
That’s just fine for Cardenas. After all, she knows that after patients come toher office and receive a proper diagnosis and treatment, they might actually be able to sit outside and take in nature’s beauty—without suffering from asneezing fit.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
60

61
Current lines of researchThere are many promising areasof research on allergies and asth-ma. Some scientists focus onwhat causes these problems.Others concentrate on findingways to prevent allergic reactionsand asthma symptoms. Still otherresearchers try to discover new orimproved ways to treat allergiesand asthma. Because allergiesand asthma are so closely associ-ated, research on one subject canoften offer insights into the other.
Recent research into what causesallergic reactions and asthma has explored the impact of envi-ronmental factors, behaviors,genetics, and stress. If scientistscan determine which environ-ments and behaviors are morelikely to contribute to symptoms,these factors can be reduced oravoided. Identifying genetic factors might also contribute to better screening.
In 2001, scientists from theNational Institute forOccupational Safety and Health(NIOSH) studied the effects ofexposure to diesel exhaust on thelungs. Researchers were especial-ly interested in determining howbreathing diesel exhaust particu-late (DEP) affects asthma andlung infections in miners andother workers. Scientists hoped todetermine whether alveolarmacrophages (AMs), a type of
Part 6: What Does ResearchTell Us about Asthma andAllergies?

white blood cell found in thelungs, were able to capture anddestroy the DEP that was inhaled.DEP contains a mixture of chemi-cals that includes a solid carboncore called soot. As many as 1 million workers in the UnitedStates are regularly exposed to DEP.
Researchers examined cells of animals and humans during thestudy. The lung tissue of rats thatwere injected with DEP showedreduced AM function. The DEPhad affected the AMs’ ability todestroy foreign material, includingbacteria, in the lungs. This meantthat it was easier for lung infec-tions to take hold. The study foundthat miners who were exposed to high DEP levels were more like-ly to suffer from lung infections.Infections were also more likely tospread elsewhere in the body.
The study continues today. It hasbeen expanded to include mechan-ics who work with diesel-poweredvehicles. In addition to answeringa questionnaire about asthma and lung infection symptoms, the mechanics were asked to pro-vide tissue samples. The sampleswere taken from their nasal linings, which were directlyexposed to DEP.
Also during 2001, NIOSH spon-sored a related study that exam-ined the effect of exposure to poly-
cyclic aromatic hydrocarbons(PAHs) on lung immunity. PAHsare found in emissions from dieselengines. Researchers wanted toconfirm that inhaling substancessuch as PAHs changes lung immu-nity in people who are exposed tothese irritants. The changesinclude a predisposition to aller-gies, airway obstruction, and lunginfections. Nasal tissue samplingsfrom a variety of workers whowere exposed to PAHs wereobtained. Samplings from workerswho were not exposed were alsotaken. This research is ongoing.
If certain behaviors seem to pro-voke an allergic reaction or anasthma attack, physicians canadvise patients to avoid thosebehaviors. Research studies canhelp scientists test theories aboutbehaviors that influence symp-toms. A 2002 study at Brighamand Women’s Hospital in Bostonexamined whether babies with afamily history of allergies weremore likely to get asthma if theywere bottle-fed at bedtime.Researchers speculated that whena baby drinks a large amount ofliquid just before falling asleep,some of it could reach the baby’sairways. Liquid in the airways cancause irritation and narrowing,eventually leading to allergies orasthma. Researchers wonderedwhether a change in behavior—not feeding a baby a large amountof liquid at bedtime—might
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
62

Part 6: What Does Research Tell Us about Asthma and Allergies?
63
prevent the problem. A total of448 infants from families with at least one allergic or asthmaticparent were studied during the babies’ first years of life, from age two.
In the Boston study, parents wereasked to report on bedtime feed-ing practices and sleeping behav-ior. Researchers found that parents who reported (during atleast three interviews) that theyhad given their babies a bottle inbed had babies who were 50%more likely to develop wheezingbetween the ages of one and five.This group was compared withbabies whose parents did notreport giving bottles to their chil-dren at bedtime. Researchers
noted that they could not deter-mine whether this behaviorwould produce the same resultsin babies with no family historyof asthma. However, they did con-clude that wheezing could beavoided if bottles were given atbedtime only to babies who werestill fully awake, sitting up, orstanding.
Unfortunately, certain dangerouscircumstances are difficult, if notimpossible, to avoid. Researchdata can help scientists identifysome factors that trigger allergicreactions or asthma during thesecircumstances. One recent exam-ple involves the terrorist attackon the United States on Sep-tember 11, 2001. In the 5–9

weeks following the attack, a tele-phone survey was conductedamong residents of Manhattan. Ofthe 13% of residents with asthma,27% reported experiencing severesymptoms after the attack. Re-searchers attributed this increasein part to the psychological effectsbrought on by the event, as well asthe unusually high levels of smoke
and debris. The results of thisstudy indicate the impact thatthese factors (stress, smoke, andother inhaled irritants) have onasthma symptoms following a disaster.
Another area of allergy and asthma research focuses on pre-vention. Scientists know that poorair quality that results from pollu-tion can affect the frequency andseriousness of allergy and asthmasymptoms. In February 2001, theCDC examined the relationshipbetween urban transportationtrends and symptoms. During the1996 Summer Olympics in Atlanta,the city imposed a new transporta-tion strategy that involved closingthe downtown area to car traffic,increasing access to public trans-portation, and promoting suchactivities as telecommuting andcarpooling. These changes resultedin less traffic congestion and betterair quality.
The study found that the benefitsof the new strategy included a 42%decrease in asthma-related emer-gency room visits to Atlanta hospi-tals. Researchers compared thenumber of emergency room visits for asthma and nonasthmaproblems during the Olympicswith visits made during the samelength of time after the games,once the traffic strategy had been
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
64

Part 6: What Does Research Tell Us about Asthma and Allergies?
65
lifted. The study found that pro-longed improvements in air pollu-tion levels reduced the need forasthmatics to seek emergencymedical help. The study also con-cluded that changes in traffic pat-terns (rather than changes inweather patterns) were responsi-ble for general improvements inair quality in Atlanta.
In March 2001, a study funded bythe National Institute of Allergyand Infectious Disease (NIAID)examined whether high levels ofcat allergen in a home coulddecrease an allergic reaction inchildren. They theorized that,over time, a higher cat allergenlevel could alter a person’simmune response to cats.Researchers measured antibodiesto cat allergen in 226 childrenaged 12 to 14. The children werealso tested for asthma. Levels ofcat allergen were measured inthe homes of these children.Researchers discovered that inhomes with low to moderate cat allergen levels, an allergicresponse to cats was triggered inchildren. In homes with highercat allergen levels, antibody levels and rates of asthma were reduced.
The results of this study do notmean that physicians will adviseparents to keep a cat in the houseeven if a child has an allergic
reaction. However, because high-er levels of the allergen appear tohave a protective effect againstasthma in some children, moretesting should be done before thecat is removed. For example, ifthe child is wheezing and has apositive response to cat allergenduring a skin test, these may bereasons to get rid of a cat or toclean the house thoroughly.
But parents who note that a childsneezes occasionally should notnecessarily fear that he or shewill develop asthma becausethere is a cat in the household.
Another study, completed in2002, focused on a dietaryapproach to reducing asthmasymptoms. A study at theUniversity of Cambridge exam-ined whether regularly eatingoily fish such as salmon andmackerel could offer people pro-

tection against asthma symptoms.Scientists had suspected thatomega-3 fatty acids, which arefound in oily fish, could providethis benefit for people with asth-ma. These fatty acids have alreadybeen linked to increased protec-tion against heart disease andarthritis.
More than 750 volunteers providedinformation on their diets, life-styles, and asthma symptoms. In the 12 months before the studybegan, 333 of them reported suffer-ing from wheezing; 437 had notexperienced this symptom. Morethan 12% of the healthy volunteers(those who had not wheezed)reported eating oily fish at leasttwice a week. Only 7.5% of thosewho had wheezed reported eatingthat much oily fish. After takinginto account other factors (such as smoking habits), researchers
determined that regular consump-tion of oily fish reduced by half therisk of asthma attacks, wheezing,and waking up with tightness inthe chest. Scientists speculatedthat the acids might reduce thebody’s production of prosta-glandins, fatty acids which areresponsible for constricting the airways.
Treatment therapies for allergiesand asthma are also an importantarea of research. Some studiesfocus on improving conventionalways of treating asthma, whileothers attempt to identify newways to minimize symptoms.
In May 2001, researchers at theNational Heart, Lung, and BloodInstitute (NHLBI) reported on twostudies that examined whetherlong-acting beta-agonistsshould replace or be used as
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
66

Part 6: What Does Research Tell Us about Asthma and Allergies?
67
supplements to inhaled cortico-steroids. These studies showedthat using beta-agonists alonewas not as effective as using corticosteroids alone. However,using beta-agonists regularly assupplements to corticosteroids didhelp control asthma symptoms.
In the studies, people with mildto moderate asthma symptomswere examined. Patients treatedwith beta-agonists alone hadnearly four times more treatmentfailures, nearly three times moreepisodes of symptoms, and signif-icantly worse airway inflamma-
tion than those who were treatedwith corticosteroids alone. Whenpatients who were using corticos-teroids alone started using beta-agonists as supplements, theywere able to reduce the need forcorticosteroids by 50 percent.
In November 2002, the results ofanother study showed that takinga new approach to treating asth-ma could reduce symptoms.Conventional asthma treatmentsare often used after the first signof symptoms. This study, conduct-ed by scientists at GlenfieldHospital in England, examined
Allergy and Asthma Health Care ProvidersMost people first see a physician when they are young. For children, this physician iscalled a pediatrician. A pediatrician specializes in caring for babies, infants, and olderchildren. If a child seems to be experiencing allergy or asthma symptoms, usually a pedi-atrician will be the first health care provider to diagnose the condition. The pediatriciancan provide some treatment for the symptoms, especially if he or she has completedadditional training in allergy or asthma care. Adults usually consult an internist or aprimary care physician for medical diagnosis and treatment. These physicians havehad a broad range of training, which sometimes includes subspecialty work in allergy orasthma care.
To obtain additional care for allergies, sometimes a pediatrician will refer a child to anallergist. An internist or primary care physician might do the same for an adult patient.An allergist (sometimes called an immunologist) is a physician who specializes in thetreatment of allergies and asthma. For children as well as for adults, an allergist is thephysician who will probably complete any testing for allergic reactions. He or she mightalso evaluate breathing capacity. An allergist can treat a variety of allergic disorders,including asthma. The patient’s pediatrician, internist, or primary care physician shouldbe kept up to date about any test results, the diagnosis, and any decisions made abouttreatment.
A pulmonologist is a physician who specializes in treating respiratory disorders, espe-cially those of the lungs. A person who is suspected of having asthma will often consulta pulmonologist, who will coordinate care with an allergist, an internist, or a primarycare physician.

the importance of determining thelevel of airway inflammation as away to predict asthma attacks.White blood cells called eosino-phils cause inflammation in theairways. The inflammation trig-gers asthma symptoms. Research-ers determined that eosinophilsare found in phlegm several weeksbefore a person actually experi-ences an asthma attack.
Scientists studied 74 patients withmoderate to severe asthma whowere already being treated at thehospital. Half the group was treat-ed with reference to eosinophil levels in phlegm, and the otherhalf was treated conventionally.Over the course of 12 months, thepatients were assessed nine times.Those in the phlegm analysisgroup had their medication adjust-ed on the basis of changes in theireosinophil levels. There were only35 asthma attacks among patientswithin this group, compared with109 attacks among those in the regular treatment group.
In the phlegm analysis group, onlyone patient had to be hospitalizedfor asthma during the study, com-pared with six in the other group.Patients in the first group werealso less likely to take unsched-uled steroid pills to treat asthmasymptoms—24 patients did, com-pared with 73 in the second group.More than anything else, thisstudy demonstrated that even if apatient has no asthma symptoms,the inflammation in the airways isbuilding up anyway. By the timethat the patient and physician are aware of the inflammation, the asthma attack is already a certainty. This information canhelp health care providers makebetter decisions about treatmentapproaches. For example, in those
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
68

Part 6: What Does Research Tell Us about Asthma and Allergies?
69
with severe asthma, perhaps it is better to continue a constant,stable level of treatment ratherthan lessen it on the basis of alack of symptoms. Researchersfound that easing up on treat-ment therapies when inflamma-tion of the airways is about to produce symptoms is not the best approach to controllingsymptoms.
The important role of volunteers
Volunteers are crucial to the success of research into the caus-es of and treatments for asthmaand allergies. Physicians andresearchers have made manyadvances that would not havebeen possible if not for the many
volunteers who took part in med-ical studies. Clinical research tri-als, which test new medications,have helped pharmaceutical com-panies develop new therapies formany people.
If people with asthma and aller-gies were not willing to volunteerfor these trials, many new drugscould not have been tested. Thiswould mean that some of themedications that are currently in use would not have been madeavailable. The information that is gathered from these studies isenormous. Sometimes, it can leadto the development of vaccines oreven cures.
It is important that all racial andethnic groups be represented inmedical studies and trials. That

way, investigators are able to gath-er information that is useful tospecific groups. African Americansand Hispanics are especiallyencouraged to volunteer. Asthmarates are quite high within thesegroups, and often the medical careavailable to them is not adequate.Participating in medical studiescan lead to an entire community’saccess to new prevention strategiesand medications.
People choose to volunteer forstudies and trials for a variety of
reasons. Some are interested inhelping to further science. Otherswant to have an opportunity to trya new treatment. Still others wantto have access to medical care andspecialists not covered by insur-ance. Some volunteers have noinsurance at all. Many volunteersare paid to participate in studiesand trials. For most people, volun-teering gives them an opportunityto receive treatment and expandtheir knowledge about their conditions.
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
70
How New Medications Are Tested
A new drug is developed and testedin a laboratory. Here, researchersdetermine whether the drug doeswhat it is supposed to do.
The drug is tested in animals to findout about any side effects it mightcause. A wide range of dosages isgiven to animals in an effort to seewhat amounts can be dangerous tohumans. The drug is given to preg-nant animals as well, in an attemptto determine whether it will be safefor pregnant women.
Once the drug is determined to besafe for use in animals, it is sent tobe evaluated for use in humans.This is when a clinical trial begins.

71
CONCLUSION: Let’s Breathe Easywith Asthma and AllergiesAllergies and asthma have become conditions that are quite common,affecting millions of people. The good news is that both can be man-aged well enough to allow people with symptoms to live full and activelives. With the treatments that are now available, no one should havedifficulty breathing normally. People can play active roles in managingthese conditions for themselves and for others. Here’s how:
Get educated about allergies and asthma. Physicians’ offices, clinics, libraries, and the Internet are all good places to start learningmore about allergies and asthma. People who learn about the range of symptoms and treatments can help educate family and communitymembers. In some cases, this education can save lives.
Put that knowledge into practice. People who recognize symptomscan take charge of their own health care. Seek medical help after thefirst sign of symptoms. Follow the asthma care plan: avoid triggers,take medications as instructed, eat well, rest, exercise, and report anychanges in the severity or frequency of symptoms.
Encourage family and community members to learn moreabout these conditions. Helping others get educated about allergiesand asthma can lead to changes in behaviors and exposures that trig-ger symptoms. People who know how harmful secondhand smoke is are less likely to smoke. Those who realize the dangers of air pollutionare more likely to support campaigns against it. People who work inenvironments where they are exposed to harmful substances should beinformed about the risks of exposure. This information can be the basisfor establishing new policies in the workplace. Many substances cancause occupational asthma. It is in the interest of all employees tolearn more about these triggers in an effort to encourage employers toinvest in measures that can reduce exposure.
Volunteer for medical studies and trials. Participating in medicalstudies and trials can benefit many people. New treatments, vaccines,and potential cures are all evaluated within these programs. An entirecommunity can participate in a study, leading to positive change in thelives of many people.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
72
Appendix 1: Sample Asthma Action PlanName ______________________________________________________________
Date _________________________
To manage your asthma, you need to keep track of your symptoms, youruse of medicine, and your peak expiratory flow (PEF). Using your PEF as a guide, here are some tips for treating your asthma symptoms:
GREEN means Go: You’re feeling OK. Just keep using your preventive(anti-inflammatory) medicine.
YELLOW means Be Careful: You’re having some symptoms. It’s time touse your quick-relief (short-acting bronchodilator) medicine, in additionto the preventive medicine.
RED means STOP: Your symptoms are serious. You need to get helpfrom a doctor!
GREEN ZONEYour green zone is _________, which is 80% to 100% of your personalbest peak flow. Go! Breathing is good, with no cough, wheezing, or chesttightness.
ACTION:
Keep taking your usual daily medicines.
YELLOW ZONEYour yellow zone is __________, which is 50% to 80% of your best peakflow. Be careful! You may have symptoms like coughing, wheezing, orchest tightness. Your peak flow level has dropped, or you notice that youneed to use quick-relief medicine more often, you have more asthmasymptoms in the morning, or asthma symptoms are waking you up at night.

Appendix
73
ACTION:
Take ______ puffs of _________________________ (your quick-reliefmedicine). Repeat this dose every 20 minutes, up to ____ more times.Use ____ puffs regularly every 4 to 6 hours for the next 2 days.
Take ______ puffs of ___________________ (your anti-inflammatorymedicine) ______ times per day.
Start taking oral steroid medicines (or increase your dose):________________ in a dose of ____ mg every A.M. ____ P.M. _____.
Call your doctor or a hospital emergency room for advice today.
RED ZONEYour red zone is ___________, which is 50% or less of your best peakflow. Danger! Your peak flow number is very low, or you continue tofeel worse after taking more medicines according to the directions forthe yellow zone.
ACTION:
Take ______ puffs of your quick-relief medicine. Repeat this doseevery 20 minutes, up to ____ more times.
Start taking an oral steroid medicine (or increase the dose). Take_______ mg right now.
Call your doctor now! If you can’t reach your doctor, go to a hospitalemergency room.
Call your doctor at any time if you have any of the following problems:
Your asthma symptoms get worse even though you’re taking oralsteroids or
Inhaled quick-relief medicine isn’t helping you for as long as 4 hours
or
Your PEF stays at 50% of your personal best (or gets even lower),even though you’re using your action plan.

74
Important telephone numbers:
Doctor’s office _____________________________
Doctor after hours _________________________
Hospital emergency room __________________
Reviewed/Updated: 9/01Created: 9/00
This handout provides a general overview on this topic and may notapply to everyone. To find out whether the handout applies to you, and to get more information on this subject, talk to your family doctor.
Adapted from the American Academy of Family Physicians
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e

Appendix
75
Appendix 2: Questions toAsk Your Physician aboutAllergies and Asthma
1. How do I know whether I have allergies or asthma?
2. If I have no family history of allergies or asthma, is it true that I won’t get them?
3. How old does a child have to be before getting tested for allergies or asthma?
4. If I don’t have allergies or asthma, why is it important that I quit smoking?
5. If I don’t smoke in the house, will my child still be exposed to secondhand smoke?
6. Should I not get a pet until I know whether my child will develop allergies to it?
7. Why do some people have allergies to some things and not to others?
8. If I take medication for allergies or asthma, will my lungs get stronger?
9. Is it dangerous to exercise if I have exercise-induced asthma?
10. During an allergic reaction, how will I know when I should go to the emergency room?
11. During an asthma attack, how will I know when I should go to the emergency room?
12. What can happen if I overuse my inhaler?
13. Do allergy and asthma symptoms usually get better as we get older?
14. If I am allergic to one food, will I be allergic to others?
15. Why do I seem to have asthma symptoms only during the winter months?
16. If I have asthma, will my children have it, too?

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
76
Appendix 3: Taking Part inResearch Studies—Questions to AskA research study is a way of finding answers to difficult scientific orhealth questions. Here are important questions you should ask of any-one who wants you or members of your family or community to be partof a research study on high blood pressure.
1. What is the study about?Why are you doing this study?Why do you want to study me or people like me? Who else is beingstudied?What do you want to get out of this study?What will you do with the results?Have you or others done this type of study ever before? Aroundhere? What did you learn?
2. Who put this study together?Who is running or in charge of this study?Whose idea was this study?How were people like me part of putting it together?Who are the researchers? Are they doctors or scientists? For whomdo they work?Have they done studies like this before?Is the government part of this study? Who else is a part of thisstudy?Who is paying for this study?Who will make money from the results of this study?
3. How can people like me share their ideas as you do this study?How will the study be explained in my community?Of people like me, who will look at this study before it starts?Of people like me, who are you talking to as you do this study? A community advisory board?

Whom from the study can I go to with ideas, questions, or complaints?How will people like me find out about how the study is going?
4. Who is going to be in this study?What kinds of people are you looking for? Why?Are you trying to get minorities in this study?Are you including people younger than 18 years old?How are you finding people for this study?Are transportation or day care provided for people in this study?Do I need to sign to participate?Will you answer all of my questions before I sign the consent form?Can I quit the study after signing the consent form? If I quit thestudy, will anything happen to me?
5. What will I get out of this study?What are the benefits?Is payment involved? How will I be paid?Will I get free health care or other services if I participate? For how long?Will I get general health care or psychological care if I participate?For how long?
6. How will I be protected from harm?Do I stand a chance of being harmed in this study? In the future?Does the study protect me from all types of harm?If I get harmed, who will take care of me? Who is responsible?If I get harmed in any way, will I get all needed treatment? Who pays for treatment?
7. How will my privacy be protected?Who is going to see the information I give?Will my name be used with the information?What happens to the information I gave if I quit the study?Is there a written guarantee of privacy?
8. What do I have to do in this study?When did you start this study? How long will it last?How much of this study have you already done?
77
Appendix

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
78
Have there been any problems so far?Will I get treated the same as everyone else?What kinds of different treatments are offered in this study? Are there both a real and a fake treatment?
9. What will be left behind after the study is over?What will happen to the information people give? How will it be kept?What are you going to do with the results of the study?How will the public learn about the results? Will results be in places where the public can see them?Are you going to send me a copy of the results? When?What other studies are you planning to do here?
The preceding questions are from a pamphlet developed by ProjectLinCS (Linking Communities and Scientists), community advisoryboard (Durham, NC), and investigators (University of North CarolinaCenter for Health Promotion and Disease Prevention) in cooperationwith the Centers for Disease Control and Prevention, Atlanta, [email protected] For copies of this brochure, contact CDC NationalPrevention Information Network, 1-800-458-5231.

ResourcesAllergy & Asthma Network Mothers of Asthmatics (AANMA)A nonprofit membership organization dedicated to eliminating suffering and death due to asthma and allergies through education,advocacy, community outreach, and research. The website and helpline are also available in Spanish.1-800-878-4403www.aanma.org
American Academy of Allergy, Asthma and ImmunologyCall or visit their website for physician or allergist referrals.611 East Wells Street Milwaukee, WI 53202 414-272-6071 Patient Information and Physician Referral Line: 1-800-822-2762www.aaaai.org
American College of Allergy, Asthma and ImmunologyCall or visit their website for physician or allergist referrals.85 West Algonquin Road, Suite 550Arlington Heights, IL 60005Patient Information and Physician Referral Line: 1-800-842-7777allergy.mcg.edu
American Lung Association61 Broadway, 6th Floor New York, NY 10006 1-800-LUNG USA (1-800-586-4872) www.lungusa.org
Asthma and Allergy Answers: Americans with Disabilities ActAmericans with Disabilities1-800-949-4232
79

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
80
Asthma and Allergy Foundation of America1233 20th Street, NW, Suite 402Washington, DC 20036 Hot Line: 1-800-7-ASTHMA (1-800-727-8462)www.aafa.org
ClinicalTrials.govA web-based resource for finding clinical trials in need of volunteers.www.clinicaltrials.govSelect the “asthma” topic to search for asthma-related trials.
Combined Health Information DatabaseA web-based service that combines resources on asthma, allergies, andother diseases from several federal agencies. A service of the NationalInstitutes of Health.chid.nih.gov/simple/simple.html
The Food Allergy and Anaphylaxis Network (FAAN)10400 Eaton Place, Suite 107Fairfax, VA 22030-2208800-929-4040www.foodallergy.org
Healthy People 2010A nationwide health promotion and disease prevention campaign sponsored by the Department of Health and Human Services. One of the goals of the campaign is to reduce health disparities.Office of Disease Prevention and Health Promotion200 Independence Avenue SW, Room 738GWashington, DC 20201www.healthypeople.govFor information on the Healthy People 2010 Microgrant program that finances community-based prevention activities see:www.healthypeople.gov/implementation/community/
MEDLINEplusA comprehensive source of health information provided by the NationalLibrary of Medicine.www.nlm.nih.gov/medlineplus/asthma.html

81
National Center on Minority Health and Health DisparitiesPromotes minority health awareness and the elimination of health disparities through research and education. Affiliated with the NationalInstitutes of Health.6707 Democracy Blvd., Suite 800MSC 5465Bethesda, MD 20892-5465800-444-6472 or 301-402-1366ncmhd.nih.gov
National Heart, Lung, and Blood Institute (NHLBI)To obtain a copy of Asthma Guidelines, request NIH publication #97-4051 by phone or Internet.301-592-8573 or 301-251-1222www.nhlbi.nih.gov/guidelines/asthma/
National Institute for Occupational Safety and Health (NIOSH)Contact for information about occupational asthma.800-35-NIOSHwww.cdc.gov/niosh/homepage.html
National Jewish Medical and Research CenterTop respiratory hospital in America.1400 Jackson Street Denver, CO 80206www.njc.org
Native American Research Centers for HealthResearch centers that link the Native American community with healthresearch and that work to increase the number of Native American scientists and health professionals.National Institute of General Medical SciencesNational Institutes of Health45 Center Drive MSC 6200Bethesda, MD 20892-6200301-496-7301www.nigms.nih.gov
Resources

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
82
New York Online Access to HealthA searchable health information resource in English and Spanish.www.noah-health.org/index.html
Office for Human Research ProtectionsA source of information on the guidelines and ethics of research studieswith humans.Department of Health and Human ServicesThe Tower Building1101 Wootton Parkway, Suite 200Rockville, MD 20852301-496-7005www.ohrp.osophs.dhhs.gov
Office of Minority Health Resource CenterServes as a national resource and referral service on minority healthissues, including asthma and allergies. Affiliated with the U.S.Department of Health and Human Services.P.O. Box 37337Washington, DC 20013-7337800-444-6472www.omhrc.gov/omhrc/

83
BibliographyAmerican Academy of Allergy, Asthma and Immunology (AAAAI).www.aaaai.org
American Medical Association. The American Medical AssociationEssential Guide to Asthma. New York: Pocket Books, 1998.
Asthma and Allergy Foundation of America (AAFA). www.aafa.org
Barber, Marianne S. The Parent’s Guide to Food Allergies: Clear andComplete Advice from the Experts on Raising Your Food Allergic Child.New York: Owl Books, 2001.
Edelman, Norman H. and American Lung Association Asthma AdvisoryGroup. American Lung Association Family Guide to Asthma andAllergies. Boston: Little Brown & Co., 1997.
Engel, June. The Complete Allergy Book. Westport, CT: Firefly Books,1998.
Fanta, Christopher, Lynda M. Christiano, and Kenan Haver. TheHarvard Medical School Guide to Taking Control of Asthma: AComprehensive Prevention and Treatment Guide for You and YourFamily. New York: Free Press, 2003.
Food Allergy and Anaphylaxis Network (FAAN). www.foodallergy.org
Gold, Susan Dudley. Asthma. Berkeley Heights, NJ: Enslow Publishers,2000.
Goldmann, David R., Jon Ayres, David A. Horowitz, and AmericanCollege of Physicians. American College of Physicians Home MedicalGuide: Asthma. New York: Dorling Kindersley Publishing, 2000.
Goldmann, David R., David A. Horowitz, and American College ofPhysicians. American College of Physicians Home Medical Guide:Common Allergies. New York: Dorling Kindersley Publishing, 2000.
Greenberg, Alissa. Asthma. London: Franklin Watts, Inc., 2000.
Hyde, Margaret O. and Elizabeth H. Forsyth. Living with Asthma. NewYork: Walker & Co., 1995.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
84
Johns Hopkins University. Johns Hopkins Family Health Book.New York: HarperCollins, 1999.
Koerner, Celide Barnes and Anne Muñoz-Furlong. Food Allergies. NewYork, NY: John Wiley and Sons, Inc. 1998.
Lieberman, P. Understanding Asthma. Jackson, MS: University Pressof Mississippi, 1999.
May, J.C. My House Is Killing Me! The Home Guide for Families withAllergies and Asthma. Baltimore: Johns Hopkins University Press,2001.
Newman, Gerald and Eleanor Newman Layfield. Allergies. London:Franklin Watts, Inc., 1992.
Plaut, Thomas F. Children with Asthma. Amherst, MA: Pedipress,1998.
Royston, Angela. Why Do My Eyes Itch? and Other Questions aboutAllergies. Chicago: Heinemann Library, 2003.
Sardegna, Jill et al. Encyclopedia of Asthma and RespiratoryDisorders. New York: Facts on File, 2002.
Schneider, Dona and Natalie Freeman. Children’s EnvironmentalHealth: Reducing Risk in a Dangerous World. Washington, DC:American Public Health Association, 2000.
Silverstein, Alan, Virginia Silverstein, and Laura Silverstein Nunn.Asthma. Berkeley Heights, NJ: Enslow Publishers, 1997.
Steinmann, Marion and Children’s Hospital of Philadelphia. A Parent’sGuide to Allergies and Asthma. New York: Delta, 1992.
Welch, Michael J., editor, and American Academy of Pediatrics.American Academy of Pediatrics Guide to Your Child’s Allergies andAsthma: Breathing Easy and Bringing up Healthy, Active Children.New York: Villard Books, 2000.
Wood, Robert A. and Asthma Allergy Foundation of America. TamingAsthma and Allergy by Controlling Your Environment: A Guide forPatients. Baltimore: Asthma and Allergy Foundation of America,Maryland Chapter, 1995.

85
Glossaryac·tive (ac·quired) im·mu·ni·ty: acondition that develops when the bodyis exposed to various antigens andbuilds a defense that is specific to thatantigen.
a·cute si·nus·i·tis: a condition that canbe caused by bacterial infections, oftenappearing several days after the firstsign of a cold. Acute sinusitis typicallylasts 3 to 8 weeks.
air·way in·flam·ma·tion: swelling,redness, and soreness of the bronchiand bronchioles.
al·ler·gen: any substance—dust, cock-roaches, weeds, certain foods—thatcauses an allergic reaction in suscepti-ble people.
al·ler·gen im·mu·no·ther·a·py: atreatment in which gradually increas-ing amounts of an allergen are injectedinto the body over a long period in aneffort to build immunity.
al·ler·gic rhi·ni·tis (hay fe·ver): aninflammation of the mucous mem-branes of the nose.
al·ler·gist: a physician who specializesin the treatment of allergies.
al·ler·gy: the body’s overreaction to cer-tain substances, such as medications,foods, animals, and plants.
al·ve·o·li: tiny air spaces within thelungs in which oxygen from the air isexchanged with carbon dioxide from theblood.
an·a·phy·lax·is: a sudden, severe aller-gic reaction that can have a variety ofsymptoms which can involve majorareas of the body at the same time,such as the skin, the respiratory sys-
tem, the gastrointestinal tract, and thecardiovascular system. Anaphylaxis canbe fatal if it is not properly treated.
an·ti·bod·ies: proteins that are part of the body’s immune system and thattravel through the bloodstream, working to fight off disease-producing organisms.
an·ti·gens: the foreign substances thatare created by a disease-producingorganism that invades the body.
an·ti·his·ta·mine: a medication thatprevents a histamine—a chemical thatthe body produces during an allergicreaction—from taking effect.
an·ti·in·flam·ma·tor·ies: medicationsthat reduce swelling in the airways andlungs to prevent an asthma attack.
an·ti·leu·ko·tri·enes: medicationswhich fight the chemicals that causeairway swelling and which make air-ways less sensitive to triggers, prevent-ing an asthma attack.
asth·ma: a chronic lung disease inwhich the air passages get inflamedand airways narrow, making it difficultto breathe.
asth·mat·ic: a person who suffers fromasthma.
B lym·pho·cytes: cells that produceantibodies to do battle with antigens,the foreign substances created by a disease-producing organism thatinvades the body.
be·ta-block·ers: medications taken toaddress heart disease, high blood pres-sure, glaucoma, or migraines. Thesemedications can sometimes trigger anasthma attack.

86
A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
bi·pha·sic re·ac·tion: anaphylaxis inwhich symptoms often go away for atime, only to return hours later.
bron·chi: two narrow tubes that leadfrom the trachea to the lungs. Each tubeis called a bronchus.
bron·chi·oles: within a bronchus, pro-gressively narrower tubes that carry air to and from tiny air spaces calledalveoli.
bron·cho·con·stric·tion (bron·cho·spasm): a process in which the smoothmuscle that surrounds the airways con-tracts excessively. This action can triggeran asthma attack.
bron·cho·di·la·tors: “rescue” medica-tions that open bronchial tubes so moreair can travel to and from the lungs inorder to end an asthma attack.
chron·ic asth·ma: a condition sufferedby a person who experiences acuteepisodes as well as extended periods ofsymptoms, often triggered by seasonalallergens or viral infections. Rarely arethese people without asthma symptoms.
chron·ic si·nus·i·tis: a condition that is often caused by bacterial infections. Its symptoms are similar to those ofbronchial asthma. Sinusitis is consideredchronic if it lasts longer than 8 weeks.
cil·i·a: tiny hairlike structures that movemucus along respiratory passages.
cor·ti·co·ste·roids: also known assteroids, these strong medications areused in a cream form to treat skin aller-gies and in an inhaler to treat asthma.They reduce swelling in the bronchialtubes, reduce the amount of mucus thebody produces, and calm the airways.
cy·a·no·sis: a bluish discoloration in theskin due to a lack of oxygen.
de·con·ges·tant: a medication thatworks by shrinking blood vessels anddecreasing fluid leakage so that nasal
congestion is reduced.
di·a·phragm: The main muscle used forbreathing. It separates the chest cavityfrom the abdominal cavity.
dry–pow·der in·haler: an inhaler that delivers medication to the lower airways without using CFC, a chemicalpropellant.
ec·ze·ma: an allergic reaction with symptoms that affect the skin. This itchy,reddening, flaking, and peeling of theskin often begins in childhood.
e·o·sin·o·phil: a white blood cell that is thought to play a part in allergic reactions and the body’s response to parasitic diseases.
ep·i·neph·rine (a·dren·a·line): an injec-tion used to treat life-threatening allergicreactions caused by insect bites, foods,medications, latex, and other agents.
e·soph·a·gus: the tube through whichfood passes from the mouth down into thestomach.
ex·er·cise-in·duced asth·ma: a type of asthma that is triggered by strenuousphysical activity. Intense, prolongedbreathing through the mouth or exercising in cold, dry air can bringon symptoms.
food-de·pen·dent ex·er·cise-in·ducedan·a·phy·lax·is: a relatively rare allergicdisorder in which symptoms occur after aperson exercises within 3 to 4 hours ofeating a particular food.
forced ex·pi·ra·to·ry val·ue (FEV 1): aunit of measurement that indicates apatient’s capacity to breathe, sometimesbefore and after exertion.
gas·tro·e·soph·a·ge·al re·flux dis·ease(GERD): a condition in which stomachacid flows up through the esophagus.This disorder affects many individualswho suffer from asthma.

87
Glossary
his·ta·mine: a chemical present in cellsthroughout the body and released dur-ing an allergic reaction. It is responsiblefor narrowing the bronchi or airways inthe lungs during an asthma attack.
hives: an allergic reaction in which theskin becomes covered with small orlarge clusters of itchy, red bumps. It canoccur as a result of an infection, eating acertain food, or taking a certain medica-tion.
hy·per·re·spon·sive: overly sensitive;describes airways that narrow too easilyor too much in response to an irritant.
id·i·o·path·ic an·a·phy·lax·is: a severeallergic reaction whose causes areunknown.
im·mu·no·glob·u·lin E (IgE): allergen-specific antibody found in people withallergies. When an allergen invades abody, that allergen’s IgE captures theallergen, triggering allergy symptoms.
in·nate im·mu·ni·ty: the body’s abilityto resist a disease by preventing theinvading microorganism from develop-ing or by counteracting the effects of its products.
leu·ko·cytes (white blood cells):as part of the body’s immune system,cells which work to destroy foreignorganisms that enter the body. Theyalso work to repair damage done by the invaders.
long-acting be·ta-ag·o·nists: thesemedications relax muscles within theairway that cause bronchospasm. Theyalso cause the air passage ways to openwider, making breathing easier.
lym·pho·cytes: cells that play the most prominent role in helping the body create a natural resistance to disease. There are two types of lymphocytes: B cells and T cells.
mast cells: cells that are commonlyfound in the nose, eyes, lungs, and gastrointestinal tract. When an allergenstimulates the release of antibodies,they attach themselves to mast cells.Exposed again to the same allergen,mast cells release substances such ashistamine into the tissue.
me·tered dose in·ha·ler (MDI): aninhaler that uses a chemical propellant(CFC) to force medication out of theinhaler and into the lower airways.
mu·co·sa: the bronchial mucous mem-brane. When it swells, a thick mucus issecreted in the airways and an asthmaattack can occur.
na·sal ster·oid in·hal·er (or spray):delivers a very fine steroid mist directlyinto the lining of the nose. It offers fastrelief by reducing inflammation andswelling, as well as by decreasing therate at which histamines are released.
neb·u·liz·er: a device used to adminis-ter inhaled medication. It delivers a fineliquid mist through a mask that isplaced over the nose and mouth. It isused especially for infants, children, andthose unable to use a standard inhaler.
neu·tro·phils: white blood cells thatingest bacterial invaders and producethe chemicals that destroy them.
non·ste·roid·al an·ti-in·flam·ma·to·rydrugs (NSAIDs): medications such asibuprofen. These drugs can trigger asth-ma attacks.
oc·cu·pa·tion·al asth·ma: a type ofasthma that develops as a result ofexposure to fumes, gases, dust, or othersubstances at work.
peak flow me·ter: a machine thatmeasures the ability of a patient tobreathe out air from the lungs.

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
88
phlegm: mucous secretions in the respi-ratory passages.
pros·ta·glan·din: a fatty acid found inall mammals that resembles hormones inits activity—for example, controllingsmooth muscle contraction, blood pressure, inflammation, and body temperature.
pul·mo·nar·y func·tion tests: a broadrange of tests used to detect even minorblockage or airway obstruction.
ro·ta·ry in·hal·er: an inhaler that delivers medication to the lower airways without using CFC, a chemicalpropellant.
sea·son·al al·ler·gic asth·ma:a condition that occurs over an extended period, usually prompted by a personinhaling seasonal allergens that act astriggers.
si·nus·i·tis: a condition in which the hol-low cavities located behind the eyes andnose get inflamed; the condition cancause asthma symptoms.
spac·er: an attachment that fits on theend of an inhaler, provides a holdingchamber and one-way valves, and helpsdirect inhaled medication into the lowerairways with greater accuracy.
spi·rom·e·ter: a machine that measuresthe ability of a patient to breathe out airfrom the lungs. Specifically, spirometersmeasure forced expiratory value (FEV 1).
T lym·pho·cytes: special cells whichattack cells that are foreign or infected by a virus.
tra·che·a: a single tube located in frontof the esophagus. The trachea is thebeginning point of the airways.
trig·ger: a factor, such as exercise, tobacco smoke, or animal dander, thatcan bring on or aggravate the symptomsof asthma.
wheez·ing: a high-pitched or whistlingnoise that results from too little air passing through a person’s airways. This sound is often more intense whenair is forced in or out of the lungs in anexaggerated way (when a person takes a long breath) or when activity levelsincrease (during exertion).

89
Project AdvisorsPhilip Abelson, PhDAmerican Association for the Advancementof Science (AAAS)
Yolanda CuestaCuesta Multicultural Consulting
Yolanda GeorgeAmerican Association for the Advancementof Science (AAAS)
Robert D. Goldman, PhDNorthwestern University Medical School
Max Gómez, PhDWNBC, Health & Science Editor
Beatrix (Betty) Ann Hamburg, MD Cornell University Medical College
Marcia HarringtonDistrict of Columbia Public Library
Constance Hendricks, PhDChair, Graduate Nursing ProgramsSouthern University and A&M CollegeSchool of Nursing
Eric Jolly, PhDEducation Development Center, Inc. (EDC)
Betty LawrenceRochester Public Library, New York
Audrey Manley, PhDPresident Emerita, Spelman College
Marsha Lakes Matyas, PhDThe American Physiological Society
Sandra NegroSenior Librarian, Wheaton Library,Maryland
Delores Parron, PhDScientific Advisor for Capacity DevelopmentOffice of the Director, National Institutes ofHealth
Joseph Perpich, MD, PhDJ.G. Perpich, LLC
Marcy Pride, MLS, MADirector, Oyer Memorial Library Washington Bible College and Capital BibleSeminary, Lanham, Maryland
Josefina Tinajero, EdDAssociate Dean, College Of Education University of Texas at El Paso
Hypertension ContentReviewers/AdvisorsTim K. Takaro, MD, MPH, MSClinical Assistant Professor, Medicine and Environmental HealthUniversity of Washington
Rubens Pamies, MDVice Chancellor for Academic Affairs, Dean for Graduate StudiesUniversity of Nebraska Medical Center
Project Staff and ConsultantsShirley M. Malcom, Principal Investigator
Maria Sosa, Co-Principal Investigator andProject Director
Kirstin Fearnley, Project Manager
Mary Chobot, PhD, Library Consultant andProject Evaluator
Ann Williams, Art Director
Susan Mahoney and Associates, Sarah Pekkanen, Writers
Tracy Gath, Writer, Editor
Betty Calinger, Editor
Maggie Sliker, Photo Researcher
Heather Malcomson, Chickona Royster,Project Associates
Write With, Inc., Proofreader
Special thanks go to Nathan Bell, HarrietPickett, Catherine Baker, and Lisa Boesen for their assistance with the development of this series of books.
Acknowledgments

A s t h m a a n d A l l e r g i e s : T h e S c i e n c e I n s i d e
90
Cover: EyeWire ImagesPage 1: Clipart.com #31629622: Clipart.com #30244103: Clipart.com #3089600; MEDLINEplus 4: American Academy of Allergy,
Asthma & Immunology5: Clipart.com #30899147: LifeART; Clipart.com #30916568: National Institute for Occupational
Safety & Health9: Clipart.com #538470910: Clipart.com #538192511: Clipart.com #302743613: Clipart.com #3193150 14: Clipart.com #286537815: Getty Images17: MEDLINEplus18: MEDLINEplus19: Clipart.com #302504820: American Academy of Allergy,
Asthma & Immunology21: MEDLINEplus22: MEDLINEplus24: American Academy of Allergy,
Asthma & Immunology26: Clipart.com #538279327: Agricultural Research Service
#K7236-328: The Image Works #EGOR04453829: Courtesy of Gavin Huntley-Fenner30: Courtesy of Gavin Huntley-Fenner31: PhotoDisc32: Getty Images #23168433: Clipart.com #3089874
34: The Image Works #CLIC073636: The Image Works #CNRD065438: Corbis #CB06096839: Louis Rosenstock41: Indian Health Service #020642: www.photoresearchers.com
#SA518743: www.photoresearchers.com #D064045: Indian Health Service #022647: www.photoresearchers.com
#SA506648: Clipart.com #538200349: Clipart.com #320720650: Clipart.com #302448651: Courtesy of Ohio State University
Medical Center53: Breath of Life54: www.photoresearchers.com
#SA610355: The Image Works #EPIX02296357: Clipart.com #321463858: Corbis #CBO2652759: Courtesy of Erminia Cardenas61: Clipart.com #321283063: PictureQuest #73106464: Associated Press; Clipart.com
#321915265: Clipart.com #302497666: Clipart.com #308639068: Indian Health Service #018069: Clipart.com #538275770: Corbis #JA002702
Photo Credits: