Managing the difficult platelet refractory patient Managing the difficult platelet refractory...
8
1 Managing the difficult platelet refractory patient BSHI Diploma Training Day Manchester 27 th Nov 2015 Dr Colin Brown PhD FRCPath Consultant Clinical Scientist NHSBT Colindale Centre HLA Selected Platelets • Causes of platelet refractoriness • Role of the NHSBT H&I laboratory • Selection of HLA compatible platelets • Importance of patient follow up • Case studies – patient management Platelets • How are they formed • Lifespan in the body • Platelet count (range) • Antigen expression • Function • Disorders • Transfusion Platelet Products • Pooled Platelets (Buffy Coat Derived) – Adult dose from 4 ABO-identical donors – platelet count >240x10 9/ dose – Leucocyte depleted – leucocyte count <5x10 6 /dose • Apheresis single donor (count as above)
Transcript of Managing the difficult platelet refractory patient Managing the difficult platelet refractory...

1
Managing the difficult platelet refractory patient
BSHI Diploma Training Day
Manchester 27th Nov 2015
Dr Colin Brown PhD FRCPath
Consultant Clinical Scientist
NHSBT Colindale Centre
HLA Selected Platelets
• Causes of platelet refractoriness
• Role of the NHSBT H&I laboratory
• Selection of HLA compatible platelets
• Importance of patient follow up
• Case studies – patient management
Platelets
• How are they formed
• Lifespan in the body
• Platelet count (range)
• Antigen expression
• Function
• Disorders
• Transfusion
Platelet Products
• Pooled Platelets (Buffy Coat Derived)
– Adult dose from 4 ABO-identical donors
– platelet count >240x109/dose
– Leucocyte depleted
– leucocyte count <5x106/dose
• Apheresis single donor (count as above)

2
Post Transfusion Increments
In a stable pt, the expected increment after 1 adult dose = 30-40 x 109/L
CCI = P1 - P0 (109L) X Body Surface Area (m2)
platelets transfused 1011
Corrected count increment (CCI)
P0 = Platelet count before transfusion (109/l)
P1 = Platelet count after transfusion (109/l)
Platelet refractoriness
• Poor increment (<10 x 109/L or CCI <7.5 ) after at least
two consecutive transfusions of random donor platelets
• Platelet count are taken 1hr post transfusion
Patients likely to receive multiple platelet transfusion
Assess transfusion response
Test for HLA specific
antibodies
HLA Antibody Test Result
Positive Use HLA selected
platelets
Negative
Poor response to random donor platelets on 2 or more occasions
Good Response to
HLA selected platelets
Poor response to
HLA selected platelets
Continue
transfusing HLA selected platelets
Test for HLA
antibodies at regular intervals
Provide ABO compatible, “A”
grade matches if possible
Test for HPA specific antibodies
HPA Antibody
Test Result
Positive Negative
Factors associated with non-
immune platelet destruction
Absent Present
Treat CauseDecide about further platelet
transfusion based on clinical status of the patient e.g. increase dose of platelets or
discontinue prophylactic transfusions
Consider trial of HLA selected
platelets
Provide HLA and
HPA selected platelets
Consider 1. Non immune
consumption2. ABO antibodies
Guidelines for the Management of Refractoriness to Platelet Transfusion
Poor Response Good Response
Continue transfusing HLA
selected platelets
Positive Use HLA selected
platelets
Good Response to HLA selected
platelets
Poor response to HLA selected
platelets
Continue transfusing HLA
selected platelets
Test for HLA antibodies at
regular intervals
Provide ABO compatible, “A”
grade matches if possible
Test for HPA specific antibodies
HPA Antibody Test Result
Positive Negative
Provide HLA and HPA selected
platelets
Consider 1. Non immune consumption2. ABO antibodies
Negative
Factors associated with non-immune platelet destruction
Absent Present
Treat CauseDecide about further platelet transfusion based on clinical status of the patient e.g. increase dose of platelets or discontinue prophylactic transfusions
Consider trial of HLA selected
platelets
Poor Response Good Response
Continue transfusing HLA
selected platelets
“Non-immune” refractoriness
• Old/poorly stored platelets, small dose
• Splenomegaly, hepatomegaly
• DIC (infection, septicaemia, malignancy)
• Infection (CMV)
• Fever
• Antibiotics, esp amphotericin B, ambisome, vancomycin, ciprofloxacin,
3
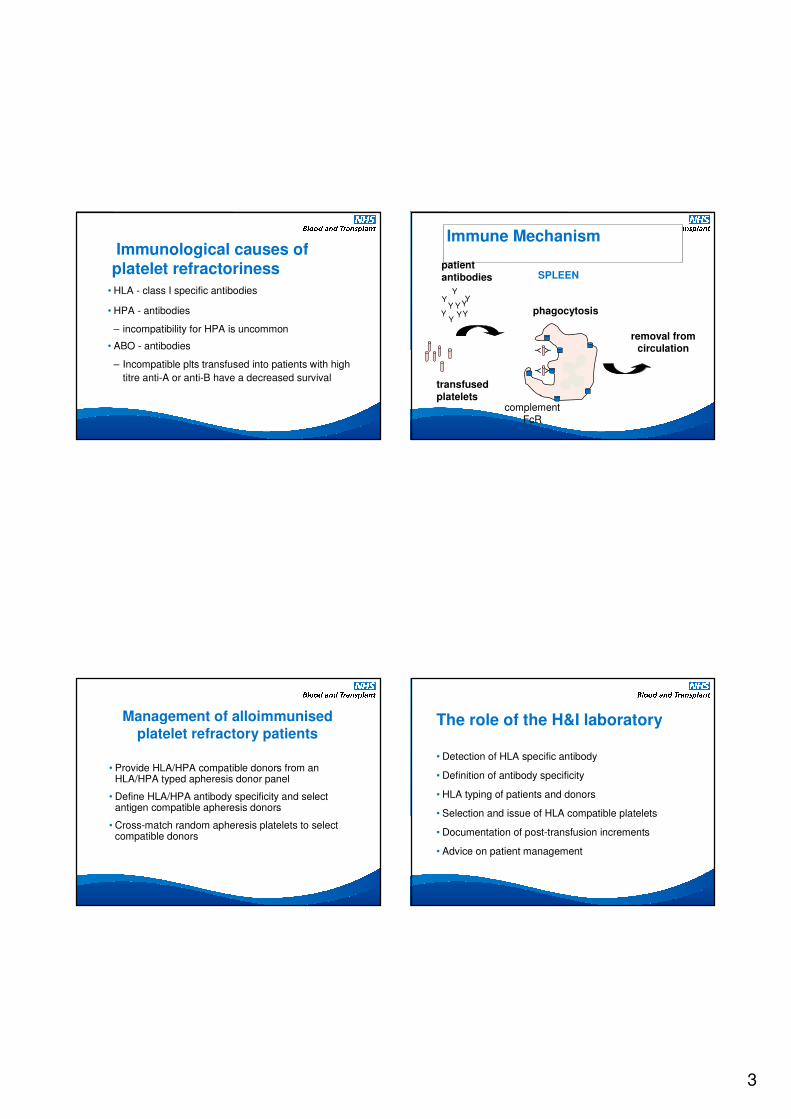
Immunological causes of platelet refractoriness
• HLA - class I specific antibodies
• HPA - antibodies
– incompatibility for HPA is uncommon
• ABO - antibodies
– Incompatible plts transfused into patients with high
titre anti-A or anti-B have a decreased survival
Immune Mechanism
removal from circulation
phagocytosis
SPLEENpatient
antibodies
transfused
platelets
Y
Y
Y
Y
YYY
Y YY
YY
YY
complement FcR
Management of alloimmunised
platelet refractory patients
• Provide HLA/HPA compatible donors from an HLA/HPA typed apheresis donor panel
• Define HLA/HPA antibody specificity and select antigen compatible apheresis donors
• Cross-match random apheresis platelets to select compatible donors
The role of the H&I laboratory
• Detection of HLA specific antibody
• Definition of antibody specificity
• HLA typing of patients and donors
• Selection and issue of HLA compatible platelets
• Documentation of post-transfusion increments
• Advice on patient management

4
A match = No mismatch
The donor and patient are not serologically mismatched for the four antigens of the A and B loci.
donor A*01-A*02 / B*08-B*44
patient A*01-A*02 / B*08-B*44
donor* A*01-A*01 / B*08-B*08
patient A*01-A*02 / B*08-B*44
*homozygous donor
01
08
03
07
Patient 1
02
44
01
08
Patient 2
26
38
01
08
Patient 3
01
08
32
14
Patient 4
24
44
01
08
Patient 5
29
44
01
08
Patient 6
02
07
01
08
Patient 7
02
15
01
08
Patient 8
01
08
01
08Homozygous donor
HLA Homozygous Donors
B match (B1-B4) = Mismatched
The donor and patient are mismatched
B1 donor: A*01-A*02 / B*08-B*27
patient: A*01-A*69 / B*08-B*27
B2 donor: A*01-A*02 / B*08-B*07
Not all mismatches are the same
B1 donor: A*36-A*68 / B*08-B*27
patient: A*01-A*68 / B*08-B*27
antibody: negative
B1 donor: A*01-A*03 / B*08-B*27
patient: A*01-A*02 / B*08-B*27
antibody: anti-A3
5
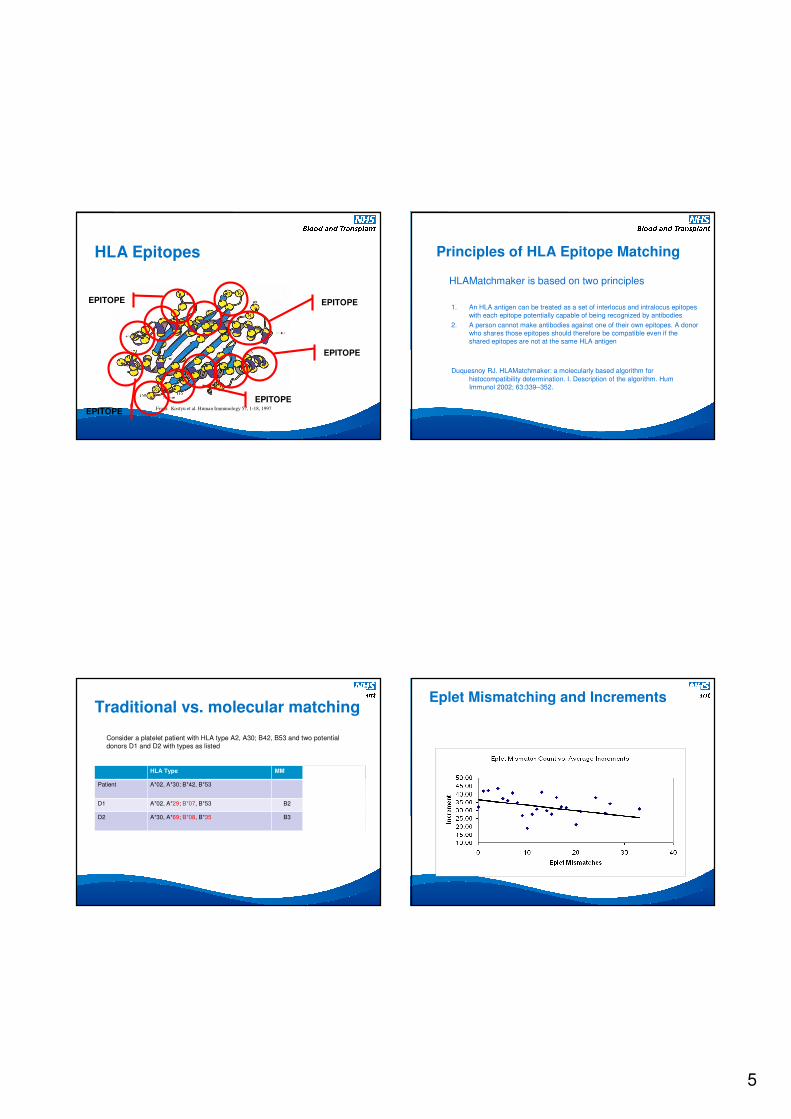
HLA Epitopes
From: Kostyu et al. Human Immunology 57, 1-18, 1997
EPITOPE
EPITOPE
EPITOPE
EPITOPE
EPITOPE
Principles of HLA Epitope Matching
HLAMatchmaker is based on two principles
1. An HLA antigen can be treated as a set of interlocus and intralocus epitopes
with each epitope potentially capable of being recognized by antibodies
2. A person cannot make antibodies against one of their own epitopes. A donor
who shares those epitopes should therefore be compatible even if the
shared epitopes are not at the same HLA antigen
Duquesnoy RJ. HLAMatchmaker: a molecularly based algorithm for
histocompatibility determination. I. Description of the algorithm. Hum
Immunol 2002; 63:339–352.
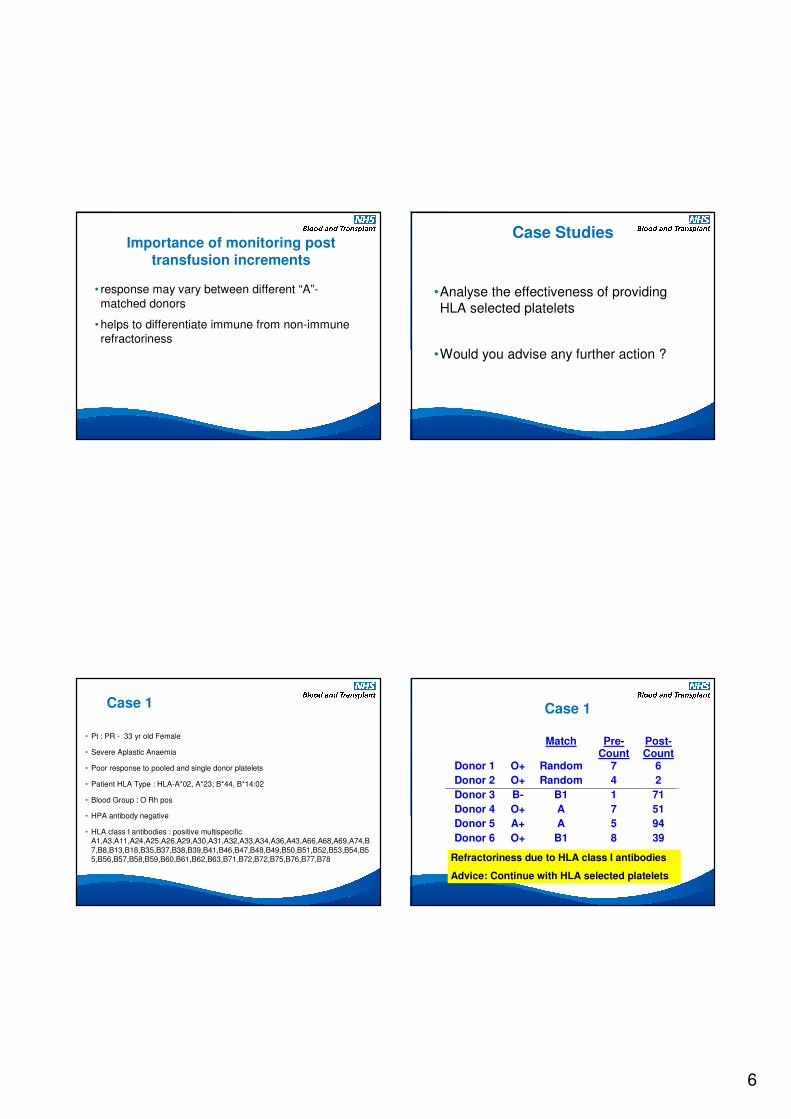
Traditional vs. molecular matching
Consider a platelet patient with HLA type A2, A30; B42, B53 and two potential
donors D1 and D2 with types as listed
HLA Type MM Epitopes
Patient A*02, A*30; B*42, B*53
D1 A*02, A*29; B*07, B*53 B2 8
D2 A*30, A*69; B*08, B*35 B3 1
Eplet Mismatching and Increments
6
Importance of monitoring post
transfusion increments
• response may vary between different “A”-
matched donors
• helps to differentiate immune from non-immune
refractoriness
Case Studies
•Analyse the effectiveness of providing
HLA selected platelets
•Would you advise any further action ?
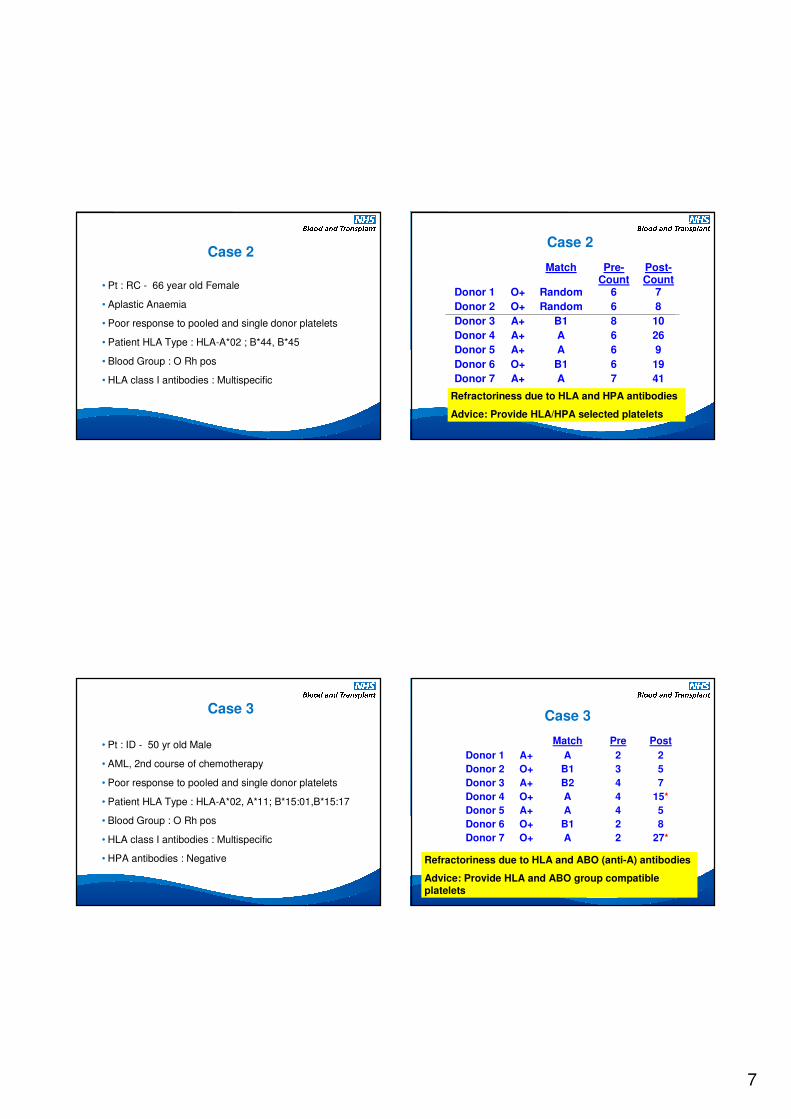
Case 1
• Pt : PR - 33 yr old Female
• Severe Aplastic Anaemia
• Poor response to pooled and single donor platelets
• Patient HLA Type : HLA-A*02, A*23; B*44, B*14:02
• Blood Group : O Rh pos
• HPA antibody negative
• HLA class I antibodies : positive multispecific A1,A3,A11,A24,A25,A26,A29,A30,A31,A32,A33,A34,A36,A43,A66,A68,A69,A74,B
7,B8,B13,B18,B35,B37,B38,B39,B41,B46,B47,B48,B49,B50,B51,B52,B53,B54,B55,B56,B57,B58,B59,B60,B61,B62,B63,B71,B72,B72,B75,B76,B77,B78
Match Pre-Count
Post-Count
Donor 1 O+ Random 7 6
Donor 2 O+ Random 4 2
Donor 3 B- B1 1 71
Donor 4 O+ A 7 51
Donor 5 A+ A 5 94
Donor 6 O+ B1 8 39
Case 1
Refractoriness due to HLA class I antibodies
Advice: Continue with HLA selected platelets
7
Case 2
• Pt : RC - 66 year old Female
• Aplastic Anaemia
• Poor response to pooled and single donor platelets
• Patient HLA Type : HLA-A*02 ; B*44, B*45
• Blood Group : O Rh pos
• HLA class I antibodies : Multispecific
Match Pre-Count
Post-Count
Donor 1 O+ Random 6 7
Donor 2 O+ Random 6 8
Donor 3 A+ B1 8 10
Donor 4 A+ A 6 26
Donor 5 A+ A 6 9
Donor 6 O+ B1 6 19
Donor 7 A+ A 7 41
Case 2
Refractoriness due to HLA and HPA antibodies
Advice: Provide HLA/HPA selected platelets
Case 3
• Pt : ID - 50 yr old Male
• AML, 2nd course of chemotherapy
• Poor response to pooled and single donor platelets
• Patient HLA Type : HLA-A*02, A*11; B*15:01,B*15:17
• Blood Group : O Rh pos
• HLA class I antibodies : Multispecific
• HPA antibodies : Negative
Match Pre Post
Donor 1 A+ A 2 2
Donor 2 O+ B1 3 5
Donor 3 A+ B2 4 7
Donor 4 O+ A 4 15*
Donor 5 A+ A 4 5
Donor 6 O+ B1 2 8
Donor 7 O+ A 2 27*
Case 3
Refractoriness due to HLA and ABO (anti-A) antibodies
Advice: Provide HLA and ABO group compatible
platelets
8
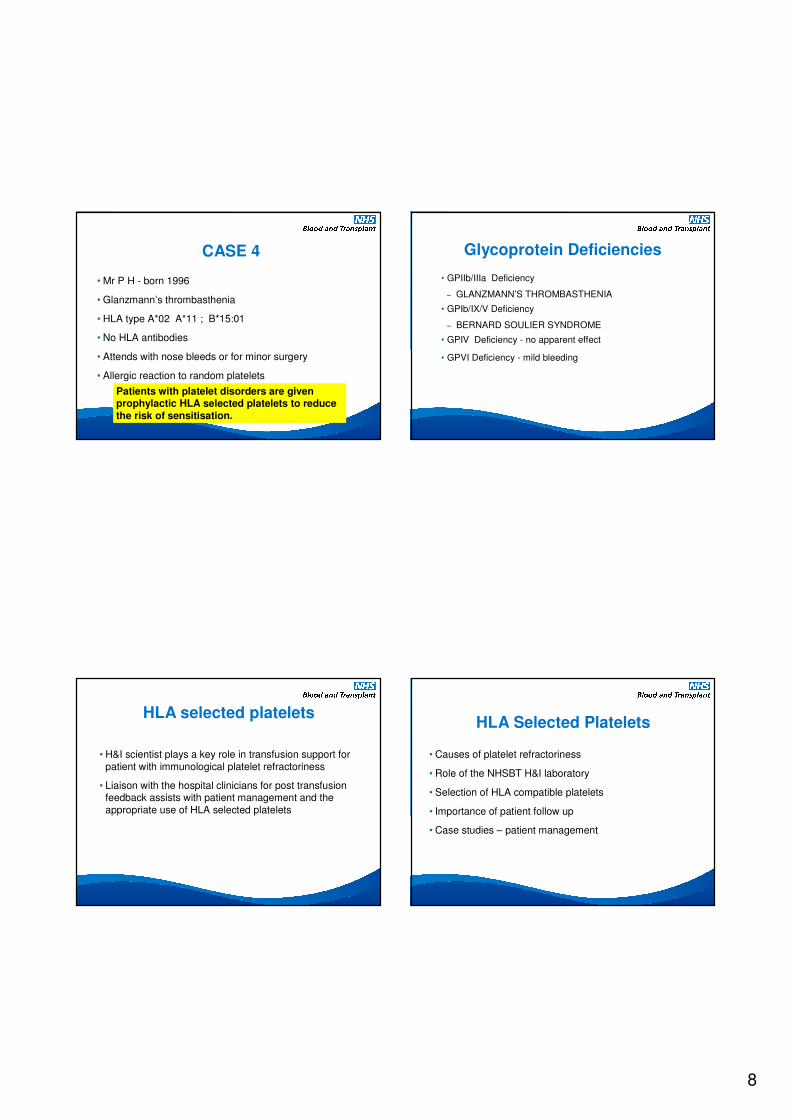
CASE 4
• Mr P H - born 1996
• Glanzmann’s thrombasthenia
• HLA type A*02 A*11 ; B*15:01
• No HLA antibodies
• Attends with nose bleeds or for minor surgery
• Allergic reaction to random platelets
Patients with platelet disorders are given prophylactic HLA selected platelets to reduce
the risk of sensitisation.
Glycoprotein Deficiencies
• GPIIb/IIIa Deficiency
– GLANZMANN’S THROMBASTHENIA
• GPIb/IX/V Deficiency
– BERNARD SOULIER SYNDROME
• GPIV Deficiency - no apparent effect
• GPVI Deficiency - mild bleeding
HLA selected platelets
• H&I scientist plays a key role in transfusion support for
patient with immunological platelet refractoriness
• Liaison with the hospital clinicians for post transfusion feedback assists with patient management and the
appropriate use of HLA selected platelets
HLA Selected Platelets
• Causes of platelet refractoriness
• Role of the NHSBT H&I laboratory
• Selection of HLA compatible platelets
• Importance of patient follow up
• Case studies – patient management