
Functional Neuro-anatomy of the Visual System: A Coarse Course Jay Hegdé.

9/6/16
1
Inofficeelectrodiagnostics:whatcanitdoforyou
NathanLighthizer,O.D.,F.A.A.OAssistantProfessor,NSUOCOChiefofSpecialtyCareClinics
ChiefofElectrodiagnosticsClinic
CourseOutline/Objective
• Whatiselectrodiagnosticstesting?• VisualPathway– BasicUnderstanding• VEP• ERG
• Fullfieldflash• Pattern• mfERG
• EOG• ClinicalCases
VisualPathway• Upstream Photoreceptors
Mid-retinallayers
Ganglioncelllayer
NFL/OpticNerve
OpticChiasm
OpticTract
• Downstream LGN
VisualCortex
TheVisualEvokedPotential(VEP)OBJECTIVELYmeasuresthefunctionalityofwhichstructure?
A. PhotoreceptorsB. RPElayerC. GanglioncelllayerD. Nervefiberlayer&
opticnerveE. Entirevisualpathway
WhichofthefollowingisanindicationtoperformaVEP?A. GlaucomaB. TraumaticbraininjuryC. OpticneuritisD. AmblyopiaE. UnexplainedvisionlossF. VFdefectG. Alloftheabove
VisuallyEvokedPotential(VEP)
• AKAVisuallyEvokedResponse(VER)• Flashvs.Pattern
• Measurestheentirevisualpathway• Fromcorneatooccipitallobe
• 3electrodes• Ground• Reference• Measuring->occipitallobe
• 1”aboveinion

9/6/16
2
Reference Ground Active
VEPElectrodes
LATENCY(ms)
AMPLITUDE(µv)
• Amplitudeusuallytranslatestotheamountofaxonsconductingalongthevisualpathway
• Latencyusuallytranslatestothemyelinstatusofthevisualpathway
VEP
WhyVEP?
• Manyopticnervediseasesareasymptomaticbecausecentralvisionisnotaffecteduntillateinthedisease1
• Diagnosisandmanagementofopticnervedisordersareoftenbasedonstructuralorsubjectivevisualfieldtests2
1 Glaucoma. American Optometric Association. www.aoa.org2 Prata, Tiago MD, G. De Moraes MD, J. Liebmann MD, R. Ritch, C. Tello MD. (2009). Diagnostic Ability of Fast Transient Visual Evoked Potential
for Glaucoma Assessment [Poster & Abstract] American Academy of Ophthalmology. 128
VEPisanobjective,functional testthatcanhelpdiscriminatebetweenhealthyandglaucomatouseyes2
VEPandGlaucoma:WellDefinedScience
TheVisualEvokedPotentialinGlaucomaandOcularHypertension:EffectsofCheckSize,FieldSize,andStimulationRate
InvestOphthalmol VisSci 24:175-183,1983
“IncreasedpatternVEPlatencywassignificantlycorrelatedwithboththeseverityandlocationofvisualfielddefectsandthedegreeofcuppingandpalloroftheopticdisc.”Theauthorsofthispaperareworldrecognized
electrophysiologyspecialistform NewEnglandMedicalCenterandUniversityofChicago
“ThefindingthatisofclinicalimportanceisthepresenceofabnormallylongVEPlatenciesinsomepatientswithocularhypertension.TheabnormalprolongationofVEPlatencyintheseeyesmayreflectsubclinicalopticnervelesionsthathavenotbeenuncoveredwithothertechniques.”
9/6/16
3
AdditionalClinicalPapers
• Repeatabilityofshort-durationtransientvisualevokedpotentialsinnormalsubjects.TelloC,DeMoraesCG,PrataTS,DerrP,PatelJ,SiegfriedJ,LiebmannJM,RitchR.DocOphthalmol.2010Jun;120(3):219-28.Epub2010Jan29.
• ShortDurationTransientVisualEvokedPotentialsinGlaucomatousEyes.PrataTS,LimaVC,DeMoraesCG,TrubnikV,DerrP,LiebmannJM,RitchR,TelloC.JGlaucoma.2011May10.[Epubaheadofprint]
• Short-durationtransientvisualevokedpotentialforobjectivemeasurementofrefractiveerrors.AnandA,DeMoraesCG,TengCC,LiebmannJM,RitchR,TelloC.DocOphthalmol.2011Dec;123(3):141-7.Epub2011Sep20.
dead Suffering Alive
Glaucoma
VEP
OCTHRTGDX
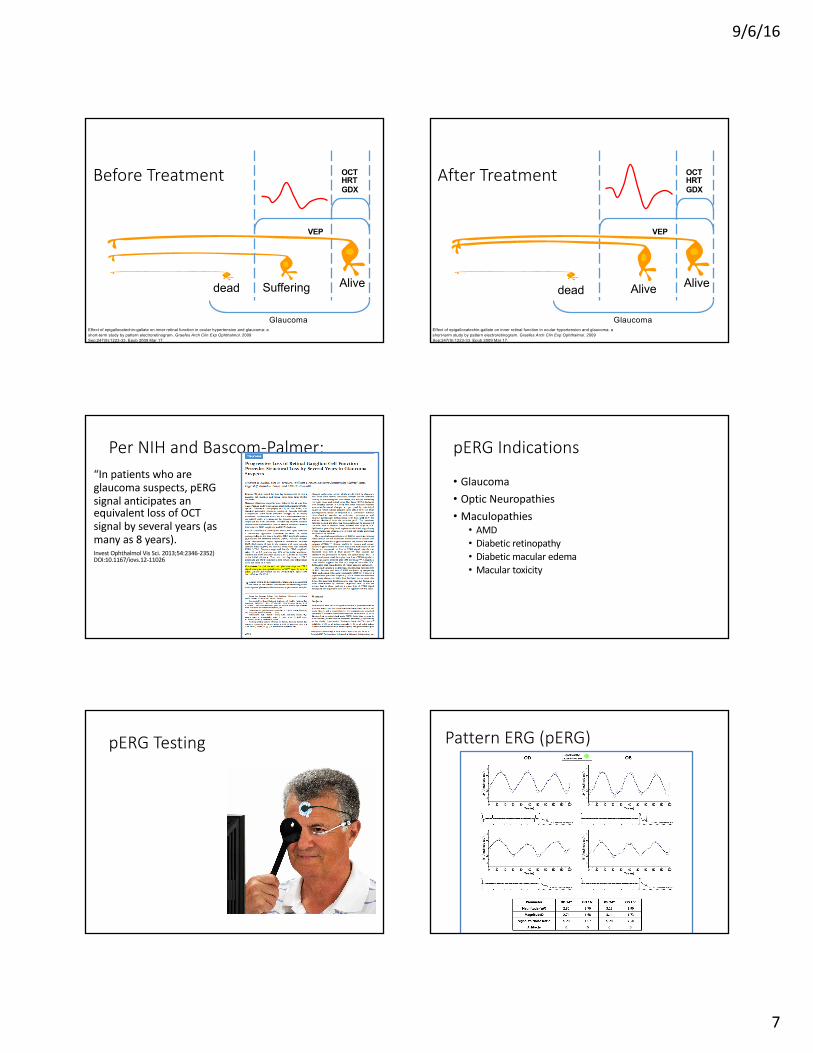
BeforeTreatment
Effect of epigallocatechin-gallate on inner retinal function in ocular hypertension and glaucoma: a short-term study by pattern electroretinogram. Graefes Arch Clin Exp Ophthalmol. 2009 Sep;247(9):1223-33. Epub 2009 Mar 17.
Alive
Glaucoma
VEP
OCTHRTGDX
Alivedead
AfterTreatment
Effect of epigallocatechin-gallate on inner retinal function in ocular hypertension and glaucoma: a short-term study by pattern electroretinogram. Graefes Arch Clin Exp Ophthalmol. 2009 Sep;247(9):1223-33. Epub 2009 Mar 17.
WhyVEP?
• Manyopticnervediseasesareasymptomaticbecausecentralvisionisnotaffecteduntillateinthedisease1
• Diagnosisandmanagementofopticnervedisordersareoftenbasedonstructuralorsubjectivevisualfieldtests2
1 Glaucoma. American Optometric Association. www.aoa.org2 Prata, Tiago MD, G. De Moraes MD, J. Liebmann MD, R. Ritch, C. Tello MD. (2009). Diagnostic Ability of Fast Transient Visual Evoked Potential
for Glaucoma Assessment [Poster & Abstract] American Academy of Ophthalmology. 128
VEPisanobjective,functional testthatcanhelpdiscriminatebetweenhealthyandglaucomatouseyes2
HowtheLXProtocolworks• Lowcontrasttestingdemonstratesdegradationofmagnocellularpathways
• Anearlyindicationofglaucoma
• Highcontrasttestingdemonstratesdegradationofparvocellularpathways
• Anearlyindicatorofcentralvisionlossandissuescausedbyproblemsbeforesignalreachesopticnerve
**patientshouldbetestedwithbestcorrectedvision**
MainIndications
• Glaucoma
•***Glaucomasuspects***
• MultipleSclerosis
• IschemicOpticNeuropathy
• TraumaticBrainInjury
• Amblyopia
• OtherNeuropathies
•Unexplainedvisionloss
•VFdefect
•FDT
ASSESSMENTOFNEURO-VISUALFUNCTION

9/6/16
4
ASSESSMENTOFNEURO-VISUALFUNCTION
ASSESSMENTOFNEURO-VISUALFUNCTION
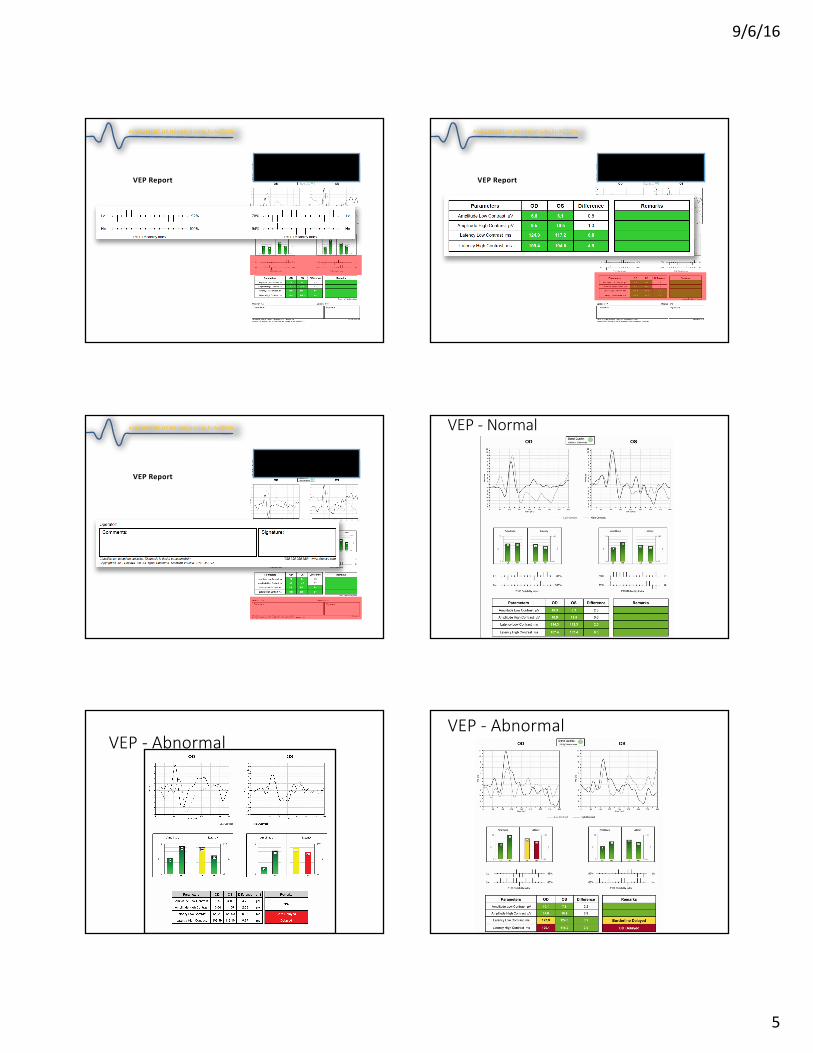
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION
9/6/16
5
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION
VEPReport
ASSESSMENTOFNEURO-VISUALFUNCTION VEP- Normal
VEP- AbnormalVEP- Abnormal

9/6/16
6
VEPabnormal- AsymmetryPatternERG(pERG)
• ERG’sareelectricalsignalsthatareameasureoftheelectrophysiologicalactivityattheretina
• ***Mid-retinallayers,ganglioncelllayer,andnervefiberlayer***
• Objectivelymeasuresretinalfunction**
• ERG’scanhelpimprovesensitivityandspecificityindiagnosingopticneuropathiesandmaculopathies likeglaucomaandmaculardegenerationwhenusedinconjunctionwithothertests
• CanalsohelpthecliniciandifferentiatebetweenretinalandopticnervedisorderswhenusedinconjunctionwithVisualEvokedPotential(VEP).
pERG AdvancedProtocols
1. ConcentricStimulusFields• Drugtoxicity• Diabeticmacularedema• AMD
2. ContrastSensitivity• Glaucoma• Diabeticretinopathy
pERG
1.ConcentricStimulusFields• Stimulusdeliveredat15flips/second• BCVA
• Pt shouldbeproperlyrefractedfor24”
• 24”testingdistance• 100%contrast
• Righteye(OD)thenLeftEye(OS)• 25secondsat24degrees• 25secondsat16degrees
pERG
2.ContrastSensitivity• Stimulusdeliveredat15flips/second• BCVA
• Pt shouldbeproperlyrefractedfor24”
• 24”testingdistance• 85%and15%
• Righteye(OD)thenLeftEye(OS)• 25secondsatHighContrast(Hc)• 25secondsatLowContrast(Lc)
PerNIHandBascom-Palmer:“Inpatientswhoareglaucomasuspects,pERGsignalanticipatesanequivalentlossofOCTsignalbyseveralyears(asmanyas8years).InvestOphthalmol VisSci.2013;54:2346-2352)DOI:10.1167/iovs.12-11026
9/6/16
7
dead Suffering Alive
Glaucoma
VEP
OCTHRTGDX
BeforeTreatment
Effect of epigallocatechin-gallate on inner retinal function in ocular hypertension and glaucoma: a short-term study by pattern electroretinogram. Graefes Arch Clin Exp Ophthalmol. 2009 Sep;247(9):1223-33. Epub 2009 Mar 17.
Alive
Glaucoma
VEP
OCTHRTGDX
Alivedead
AfterTreatment
Effect of epigallocatechin-gallate on inner retinal function in ocular hypertension and glaucoma: a short-term study by pattern electroretinogram. Graefes Arch Clin Exp Ophthalmol. 2009 Sep;247(9):1223-33. Epub 2009 Mar 17.
PerNIHandBascom-Palmer:“Inpatientswhoareglaucomasuspects,pERGsignalanticipatesanequivalentlossofOCTsignalbyseveralyears(asmanyas8years).InvestOphthalmol VisSci.2013;54:2346-2352)DOI:10.1167/iovs.12-11026
pERG Indications
• Glaucoma• OpticNeuropathies• Maculopathies
• AMD• Diabeticretinopathy• Diabeticmacularedema• Maculartoxicity
pERG Testing PatternERG(pERG)
9/6/16
8
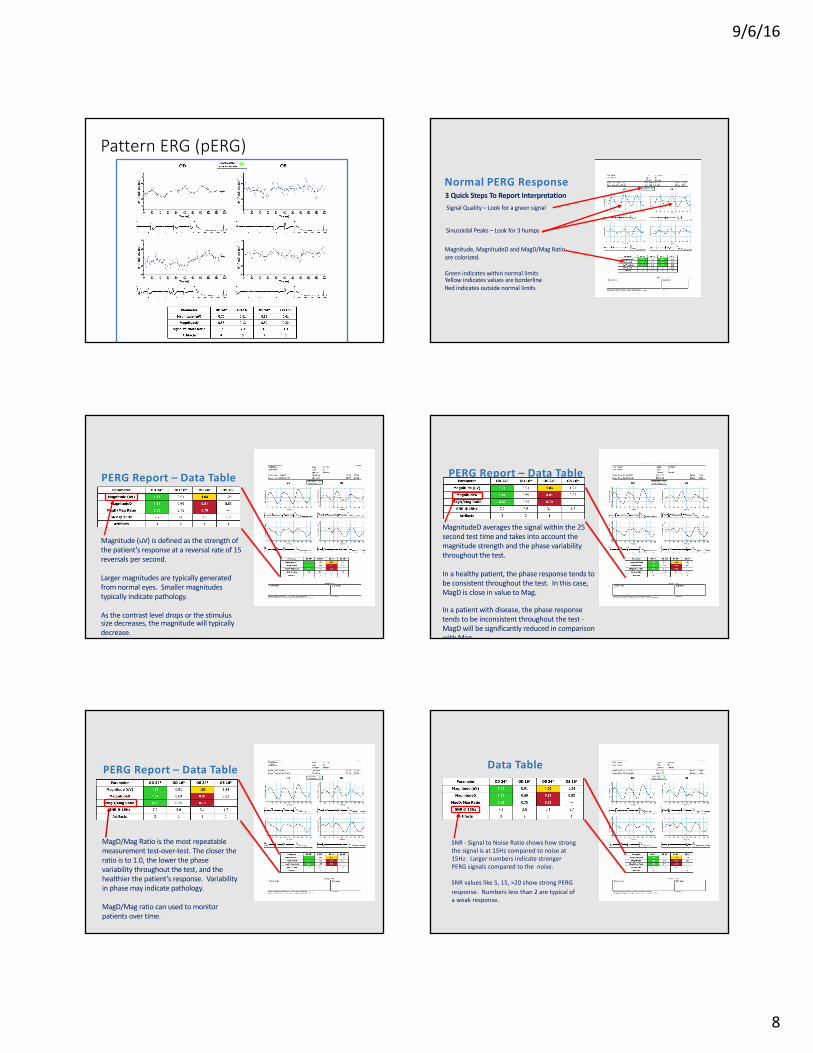
PatternERG(pERG)
NormalPERGResponse
Magnitude,MagnitudeD andMagD/MagRatioarecolorized.
GreenindicateswithinnormallimitsYellowindicatesvaluesareborderlineRedindicatesoutsidenormallimits
3QuickStepsToReportInterpretationSignalQuality– Lookforagreensignal
SinusoidalPeaks– Lookfor3humps
PERGReport– DataTable
Magnitude(uV)isdefinedasthestrengthofthepatient’sresponseatareversalrateof15reversalspersecond.
Largermagnitudesaretypicallygeneratedfromnormaleyes.Smallermagnitudestypicallyindicatepathology.
Asthecontrastleveldropsorthestimulussizedecreases,themagnitudewilltypicallydecrease.
PERGReport– DataTable
MagnitudeD averagesthesignalwithinthe25secondtesttimeandtakesintoaccountthemagnitudestrengthandthephasevariabilitythroughoutthetest.
Inahealthypatient,thephaseresponsetendstobeconsistentthroughoutthetest.Inthiscase,MagD iscloseinvaluetoMag.
Inapatientwithdisease,thephaseresponsetendstobeinconsistentthroughoutthetest-MagD willbesignificantlyreducedincomparisonwithMag.
PERGReport– DataTable
MagD/MagRatioisthemostrepeatablemeasurementtest-over-test.Theclosertheratioisto1.0,thelowerthephasevariabilitythroughoutthetest,andthehealthierthepatient’sresponse.Variabilityinphasemayindicatepathology.
MagD/Magratiocanusedtomonitorpatientsovertime.
DataTable
SNR- SignaltoNoiseRatioshowshowstrongthesignalisat15Hzcomparedtonoiseat15Hz.LargernumbersindicatestrongerPERGsignalscomparedtothenoise.
SNRvalueslike5,15,>20showstrongPERGresponse.Numberslessthan2aretypicalofaweakresponse.

9/6/16
9
DataTable
Artifactsarecausedbyblinkingorpatientmovement.Theyaredetectedandcounted.Ahighnumberofartifactswilleffecttheamountofdatathatcanbeanalyzed.
Thegoalistohavealownumberofartifacts.Wewantthepatienttobecomfortableandblinkwhennecessary,butnotexcessively.Thegoalislessthan10.IftestsresultsshowArtifactsgreaterthan10,thetestshouldberepeated.
AbnormalPERG
Missing3humps
Yellowindicatesvaluescomparedtonormalareborderline
Redindicatesvaluesareoutsidenormallimits
Operator: Salazar,Andres Eye Centers of Florida, PA #2 - 4771
Comments: - Grating Size: 64 Signature:
Diagnosis is doctor's responsibility. PERG recorded using skin electrodes. (16,12,23,15)Copyright © 2015 Diopsys, Inc. All Rights Reserved. Software Version: 2.18.5118-VX
First Name: Kathryn DOB: 11/16/1979Last Name: Coiro Age: 35Patient ID: Gender: FemaleExam Date: 2015-05-11 OD:+1.50 BCVA: 20/30Exam Time:03:32:10 PM OS:+1.50 BCVA: 20/15
OD Signal Quality:
OS 62dBµV 60Hz noise
Time (ms)0 20 40 60 80 100 120 140 160 180 200
24°
Am
plitu
de( u
V)
-4
-2
2
4
Time (ms)0 20 40 60 80 100 120 140 160 180 200
24°
Am
plitu
de(u
V)
-4
-2
2
4
Time (ms)0 20 40 60 80 100 120 140 160 180 200
16°
Am
plitu
de(u
V)
-4
-2
2
4
Time (ms)0 20 40 60 80 100 120 140 160 180 200
16°
Am
plitu
de(u
V)
-4
-2
2
4
Parameter OD 24° OD 16° OS 24° OS 16°
Magnitude (uV) 3.90 2.45 3.73 2.28
MagnitudeD 3.66 2.31 3.61 2.09
MagD/Mag Ratio 0.94 0.94 0.97 0.92
SNR (dB) 14.3 10.9 14.1 9.6
Artifacts 1 0 5 2
Scott Wehrly, MDOperator: Rivas,Nicole Lake Eye Associates - 9448
Comments: - Grating Size: 64 Signature:
Diagnosis is doctor's responsibility. PERG recorded using skin electrodes. (8,9,7,8)Copyright © 2015 Diopsys, Inc. All Rights Reserved. Software Version: 2.18.5218-VX
Last Name: ALLAIRE DOB: 1/9/1943First Name: SANDA Age: 72Patient ID: 460 Gender: FemaleExam Date: 2015-07-14 OD:+1.00 +0.75 x75 BCVA: 20/20Exam Time:01:16:32 PM OS:+1.00 +0.50 x95 BCVA: 20/20
OD Signal Quality:
OS 61dBµV 60Hz noise
Time (ms)0 20 40 60 80 100 120 140 160 180 200
24°
Am
plitu
de(u
V)
-1
1
2
Time (ms)0 20 40 60 80 100 120 140 160 180 200
24°
Am
plitu
de(u
V)
-1
1
2
Time (ms)0 20 40 60 80 100 120 140 160 180 200
16°
Am
plitu
de( u
V)
-1
1
2
Time (ms)0 20 40 60 80 100 120 140 160 180 200
16°
Am
plitu
de( u
V)
-1
1
2
Parameter OD 24° OD 16° OS 24° OS 16°
Magnitude (uV) 1.01 1.25 1.24 1.17
MagnitudeD 0.75 0.46 0.72 0.54
MagD/Mag Ratio 0.74 0.37 0.58 0.46
SNR (dB) 0.3 2.4 2.3 1.3
Artifacts 1 0 0 0
ApplyingtoYourPracticeVEP
1. Glaucoma&glaucomasuspects
2. Unexplainedvisionloss3. Transientvisionloss4. UnexplainedVF
defects5. UnreliableVF6. Opticneuropathies7. Opticneuritis/MS8. Amblyopia9. TBI
FlashERG1. RP&itsvariants2. Cone
dystrophies&Rodmonochromat
3. Symptoms:• “Night
blindness”• Restricted
peripheralfields
• Colorvisiondeficits
PERG1. Glaucoma&glaucoma
suspects2. UnexplainedVF
defects3. UnreliableVF4. Opticneuropathies5. Maculopathies
1. AMD2. Diabeticmacular
edema3. Highriskmeduse
(Plaquenil)4. GeneralizedDR


















