
DPG-AIDS Welcome Michelle Roland, Lead On behalf of DPG-AIDS.
ARfitpmptatatrtMbDBovDRfciJ
5
from the association
Diabetes White Paper: Defining the Delivery of NutritionServices in Medicare Medical Nutrition Therapy vsMedicare Diabetes Self-Management Training Programs
Anne Daly, MS, RD; Pam Michael, MBA, RD; Elvira Q. Johnson, MS, RD, LDN; Carolyn C. Harrington, RD;
Stephanie Patrick; Tori Bender, MSJAuttuqmd(DectccttndMabDtiq
baacftadgf(tapz
MtmboftgrpnvM
SmeDptpcsnc
da
BSTRACTegistered dietitians (RDs) have a de-ned and unique role in care for pa-ients with diabetes that differs de-ending on whether the service is foredical nutrition therapy (MNT) or
art of a diabetes self-managementraining (DSMT) program (DSMTnd diabetes self-management educa-ion [DSME] are used interchange-bly in this article). The purpose ofhis article is to describe the currentegulatory and practice frameworkhat supports nutrition care underedicare Part B for people with dia-
etes. A description of MNT andSMT provided under Medicare Partis included. The role of RDs and
ther health care professionals in-olved as program instructors inSMT programs is also addressed.evisions to the National Standards
or Diabetes Self-Management Edu-ation are discussed to clarify RDs’nvolvement in DSME programs.
Am Diet Assoc. 2009;109:528-539.
A. Daly is cofounder and director ofSpringfield Diabetes & Endocrine Cis director, ADA Nutrition Services CJohnson is principal consultant, EQC. C. Harrington is program coordCenter/Aspirus Nutrition Counselingpresident of Policy Initiatives and Aoffice. T. Bender is communicationsCoverage, Chicago, IL.
Address correspondence to: Anne DEndocrine Center, 2501 Chatham RdE-mail: [email protected] © 2009 by the American Di0002-8223/09/10903-0018$36.00/0
doi: 10.1016/j.jada.2008.11.00428 Journal of the AMERICAN DIETETIC ASSOCIATIO
ll health care professionals, in-cluding registered dietitians(RDs), must be accountable for
pholding Medicare and other regula-ions for care of patients with diabe-es. Medicare regulations define thenique program requirements thatualified providers must follow foredical nutrition therapy (MNT) and
iabetes self-management trainingDSMT) program compliance (noteSMT and diabetes self-managementducation [DSME] are used inter-hangeably in this article) (for defini-ions of terms, see Figure 1). Medi-are MNT involves comprehensivelinical care provided by licensed/cer-ified (as applicable) RDs and nutri-ion professionals. Nationally recog-ized protocols are required for theelivery of MNT services. Underedicare regulations, DSMT includes
nutrition education componentased on the National Standards foriabetes Self-Management Educa-
ion, which is endorsed by the Amer-can Diabetes Association to promoteuality education for people with dia-
trition and diabetes education,er, Springfield, IL. P. Michaelerage, Chicago, IL. E. Q.Associates, North Reading, MA.tor, Aspirus Diabetes Educationausau, WI. S. Patrick is vicecacy in ADA’s Washington, DC,anager, ADA Nutrition Services
y, MS, RD, Springfield Diabetes &uite 200, Springfield, IL 62704.
tic Association.
p
N © 2009
etes. The American Diabetes Associ-tion Education Recognition Programssesses whether or not DSMT appli-ants meet the National Standardsor Diabetes Self Management Educa-ion (1). All DSMT programs must beccredited as meeting quality stan-ards by a national accreditation or-anization approved by the Centersor Medicare & Medicaid ServicesCMS). Currently, CMS recognizeshe American Diabetes Associationnd the Indian Health Service as ap-roved national accreditation organi-ations (2).CMS has described the features ofNT and DSMT, and determined
hat provision of both benefits may beore medically effective for some
eneficiaries than receipt of just onef the benefits. Thus, health care pro-essionals must recognize and respecthe unique components that distin-uish the education and training cur-iculum included in Medicare DSMTrograms, and the nutritional diag-ostic, therapy, and counseling ser-ices provided through MedicareNT.The Standards of Practice and
tandards of Professional Perfor-ance for Registered Dietitians (Gen-
ralist, Specialty, and Advanced) iniabetes Care (3) describe levels oferformance for RDs who care for pa-ients with diabetes. In addition, theatient-focused Nutrition Care Pro-ess (NCP) for RDs also provides in-ight and language to distinguishutrition education and nutritionounseling interventions (4).MNT and DSMT services are well
efined by Medicare, but their cover-ge is not comprehensive relative to
nuent
ovJ
ina, W
dvom
al, S
ete
atient access and need. The Ameri-
by the American Dietetic Association

ctcvow
●
●
●
●
●
DDpcp2lemut5hpbo$e
itrtcuewaobpietdwf
LDTtadistsgadsadtCpcCsicvcdavMbva
vnvtDidt
Fd
an Dietetic Association (ADA) con-inuously seeks to strengthen theoverage and delivery of diabetes ser-ices provided by RDs and has devel-ped principles to guide ADA policyork in diabetes care, including:
Medicare MNT and DSMT arecomplementary but distinct pro-grams in which RDs provideunique nutrition services, consis-tent with the specific missions ofthose programs;RDs are key members of multidis-ciplinary health care teams thatprovide DSMT;RDs provide the highest quality nu-trition care and services followingADA’s NCP and evidence-based nu-trition practice guidelines for medi-cal nutrition therapy; andRDs who participate in the Medi-care Part B MNT program are re-sponsible and accountable for com-plying with related federal andstate regulations.RDs’ unique education and training
Diabetes A condition of abnormal glucose mcriteria: A fasting blood sugar level greater toccasions; a 2-h post-glucose challenge gredifferent occasions; or a random glucose tesof uncontrolled diabetes (17).
Medical nutrition therapy (MNT) A specificclinical settings that is focused on the manaindividualized nutrition assessment and a duNutrition Care Process to manage disease. MPart B) statute as “nutritional diagnostic, theof disease management which are furnishedprofessional . . . pursuant to a referral by a pcertified (as applicable) registered dietitians
Diabetes self-management training (DSMTself-management training services means edto an individual with diabetes by a certifiedindividual or entity who meets the quality stamanaging the individual’s diabetic conditiona comprehensive plan of care related to thetherapy compliance or to provide the individ(including skills related to the self-administramanagement of the individual’s condition” (2monitoring of blood glucose, education aboudeveloped specifically for patients who are ito use the skills for self-management. Underaccredited as meeting quality standards by aapproved national accreditation organization.Medicaid Services recognizes the AmericanService as approved national accreditation o
igure 1. Definitions of medical nutrition thiabetes.
gives them an ideal background to b
serve in a changing environmentfor diabetes care and treatment, in-cluding preventive, chronic, andacute care for individuals diag-nosed with diabetes and individualsidentified as at risk of developingdiabetes.
IABETES AS AN EPIDEMICiabetes affects nearly 24 millioneople in the United States, an in-rease of more than 3 million in ap-roximately 2 years, according to new007 prevalence data estimates re-eased in 2008 by the Centers for Dis-ase Control and Prevention. Thiseans that nearly 8% of the US pop-
lation has diabetes. In addition tohe 24 million with diabetes, another7 million people are estimated toave prediabetes, a condition thatuts people at increased risk for dia-etes. The 2007 total estimated costf diabetes in the United States is174 billion, including $116 billion inxcess medical expenditures and $58
bolism diagnosed using the followingor equal to 126 mg/dL on two differentthan or equal to 200 mg/dL on twoer 200 mg/dL for a person with symptoms
plication of the Nutrition Care Process inent of diseases. MNT involves in-depth
on and frequency of care using theservices are defined in federal (Medicare
y, and counseling services for the purposea registered dietitian or nutritionician.” MNT is provided by licensed/nutrition professionals (17).
nder Medicare Part B, “diabetes outpatienttional and training services furnished . . .ider . . . in an outpatient setting by an
ards . . . , but only if the physician who istifies that such services are needed underividual’s diabetic condition to ensurewith necessary skills and knowledge
of injectable drugs) to participate in theThe program includes instruction in self-et and exercise, an insulin treatment planlin-dependent, and motivation for patientsdicare Part B, all DSMT programs must benters for Medicare & Medicaid Services–rrently, the Centers for Medicare &etes Association and the Indian Healthizations (21,22).
py, diabetes self-management training, and
illion in reduced national productiv- d
March 2009 ● Journa
ty. Medical costs attributed to diabe-es include $27 billion for care to di-ectly treat diabetes, $58 billion toreat the portion of diabetes-relatedhronic complications that are attrib-ted to diabetes, and $31 billon inxcess general medical costs. Peopleith diagnosed diabetes incur aver-ge expenditures of $11,744 per year,f which $6,649 is attributed to dia-etes. The burden of diabetes is im-osed on all sectors of society—highernsurance premiums paid by employ-es and employers, reduced earningshrough productivity loss, and re-uced overall quality of life for peopleith diabetes and their families and
riends (5).
andmark Studies that have Shapediabetes Carehe aggregate costs associated withreating individuals with diabetesnd the increasing incidence of theisease reinforce the need to find andmplement diabetes programs thatuccessfully control, or even prevent,he onset of diabetes. Two landmarktudies, the Diabetes Prevention Pro-ram (6) and the Diabetes Controlnd Complications Trial study (7),emonstrated the importance of life-tyle intervention and intensive ther-py. Advances in the technology ofiabetes care and results such ashose in the Diabetes Control andomplications Trial study have ex-anded the role of RDs in diabetesare. As described in the Diabetesontrol and Complications Trialtudy findings, RDs are recognized asntegral members of diabetes healthare teams (7). As a result, RD in-olvement in diabetes care and edu-ation has increased substantiallyuring the past 10 years. Clinical tri-ls and outcomes research have pro-ided evidence for the effectiveness ofNT implemented by RDs on meta-
olic and behavioral outcomes for indi-iduals with type 1 and 2 diabetes (forsummary of evidence see Figure 2).Today, RDs may provide MNT ser-
ices for individuals with diabetes, andutrition education to these same indi-iduals through separately adminis-ered services such as recognizedSMT programs. With additional qual-
fications, such as advanced practice foriabetes care or attainment of addi-ional diabetes-specific credentials (for
etahanatert ov
apgemratiNT
rapbyhys
and
) Uuca
provndcerind
ualtion0).t dinsu
MeCeCu
Diabrgan
era
escriptions of some diabetes-related
l of the AMERICAN DIETETIC ASSOCIATION 529

Type ofintervention Reference
Studylength No. of subjects Outcome
Randomized controlled trialsMNTa only UK Protective Diabetes
Study Group, 19903 mo 3,042 newly diagnosed patients with
type 2 diabetesIn 2,595 patients who received intensive nutrition therapy (447 were primary diet failures),
hemoglobin A1c decreased 1.9% (8.9%-7.0%) during the 3 mo before studyrandomization
Franz and colleagues,1995
6 mo 179 patients with type 2 diabetes;62 in comparison group; durationof diabetes �4 y
Hemoglobin A1c at 6 mo decreased 0.9% (8.3%-7.4%) with nutrition practice guidelinescare; hemoglobin A1c decreased 0.7% (8.3%-7.6%) with basic nutrition care;hemoglobin A1c was unchanged in the comparison group with no nutrition intervention(8.2%-8.4%)
Kulkarni andcolleagues, 1998
6 mo 54 patients with type 1 diabetes,newly diagnosed
Hemoglobin A1c at 3 mo decreased 1.0% (9.2%-8.2%) with nutrition practice guidelinecare and 0.3% (9.5%-9.2%) in usual nutrition care group
MNT in combinationwith diabetesself-managementtraining
Glasgow andcolleagues, 1992
6 mo 162 patients older than age of 60 ywith type 2 diabetes
Hemoglobin A1c decreased from 7.4%-6.4% in control-intervention crossover group,whereas the intervention-control crossover group had a rebound effect; interventiongroup had a multidisciplinary team with an RDb who provided MNT
Sadur and colleagues,1999
6 mo 185 adult patients with diabetes 97 patients received multidisciplinary care and 88 patients received usual care by primarycare physician; hemoglobin A1c decreased 1.3% in the multidisciplinary care groupcompared with 0.2% in the usual care group; intervention group had a multidisciplinaryteam with the RD who provided MNT
Observational studiesCross-sectional
surveyDelahanty and Halford,
19939 y 623 patients with type 1 diabetes Patients who reported following their meal plan more than 90% of the time had an
average hemoglobin A1c level 0.9% lower than subjects who followed their meal plan�45% of the time
Expert opinion Diabetes Control andComplications TrialResearch Group,1993
Diabetes Control and Complications Trial group recognized the importance of the role ofthe RD in educating patients on nutrition and adherence to achieve hemoglobin A1cgoals; the RD is a key member of the team
Franz, 1994 Diabetes Control and Complications Trial made apparent that RDs and registered nurseswere extremely important members of the team in co-managing and educating patients
Chart audit Johnson and Valera,1995
6 mo 19 patients with type 2 diabetes At 6 mo, blood glucose levels decreased 50% in 76% of patients receiving nutritiontherapy by an RD; mean total weight reduction was �5 lb
Johnson and Thomas,2001
1 y 162 adult patients MNT intervention decreased hemoglobin A1c levels 20%, bringing mean levels �8%,compared with subjects without MNT intervention who had a 2% decrease inhemoglobin A1c levels
Retrospective chartreview
Christensen andcolleagues, 2000
3 mo 102 patients (15 type 1, 85 type 2)with duration of diabetes �6 mo
Hemoglobin A1c levels decreased 1.6% (9.3%-7.7%) after referral to an RD
Meta-analyses of trialsBrown, 1996, 1990 89 studies Educational intervention and weight loss outcomes; MNT had a statistically significant
positive impact on weight loss and metabolic controlPadgett and
colleagues, 19887,451 patients Educational and psychosocial interventions in management of diabetes (including MNT,
self-monitoring of blood glucose, exercise, and relaxation); nutrition education showedthe strongest effect
Norris and colleagues,2001
72 studies Positive effects of self-management training on knowledge, frequency, and accuracy ofself-monitoring of blood glucose, self-reported dietary habits, and glycemic control wereshown in studies with short follow-up (�6 mo)
Figure 2. Summary of evidence for use of medical nutrition therapy in patients with diabetes. aMNT�medical nutrition therapy. bRD�registered dietitian. (Reprinted with permission from:Pastors JG, Franz MJ, Warshaw H, Daly A, Arnold MS. How effective is medical nutrition therapy in diabetes care? J Am Diet Assoc. 2003;103:827-831.)
530M
arch2009
Volume
109Num
ber3

aapaqmdi
PDToDTefApSdfiDps
ttttvascpttfiattttSltsam
tc
rcampa
RasatatS
●
●
●
●
●
●
●
doo
AEGFsicbaqABfrt
Fhci
dvanced credentials, see Figure 3),nd in accordance with local scope ofractice, state licensure, payer policies,nd/or facility requirements, RDs mayualify to provide separate and comple-entary services to individuals with
iabetes, such as training on the use ofnsulin administration devices (8).
RACTICE FRAMEWORK SUPPORTINGIABETES CARE PROVIDED BY RDshe Standards of Practice and Standardsf Professional Performance for RDs iniabetes Careo reflect the current practice of di-tetics as it relates to diabetes careor Medicare and other payers,DA’s Diabetes Care and Educationractice group has published itstandards of Practice and Stan-ards of Professional Performanceor Registered Dietitians (General-st, Specialty, and Advanced) iniabetes Care (2,9). Standards ofractice (SOP) are authoritative
Certified Diabetes Educator (CDE) This creprofessionals who have a defined role as aperform some diabetes-related functions asoccupational duties. Certification is a voluntaqualified health care professionals’ knowledgprocess that demonstrates that rigorous eligCertification is not required by law for emplomay use board certification as a basis for eother considerations. The certification is conDiabetes Educators, a national, nongovernmCertification is valid for a period of 5 years.a
Board Certified-Advanced Diabetes Manademonstrates that a health care professionaassessment, recognize and prioritize complediabetes across the life span, and provide thself-management training. The certification fdiabetes problems and requires an advancedscope of advanced clinical practice includesadjustment, medical nutrition therapy, exercmanagement, and psychosocial issues. Attaitreatment and monitoring of acute and chrocompetence in advanced clinical practice ancomplexity of decision-making, which expanResearch, publications, mentoring, and contskill sets. A diabetes care professional withCDE credential. The BC-ADM certification prAssociation of Diabetes Educators and the A
igure 3. Diabetes-related credentials. aFor inttp://www.ncbde.org/documents/HB2008Finalredential, visit http://www.diabeteseducatorndex.html. Accessed May 30, 2008.
tatements that describe a compe- p
ent level of practice relatedo direct client care demonstratedhrough nutrition assessment, nu-rition diagnosis, nutrition inter-ention, and nutrition monitoringnd evaluation, including the re-ponsibilities for which RDs are ac-ountable. The Diabetes Care SOPresuppose that RDs use criticalhinking skills, analytical abilities,heories, best available researchndings, current accepted dieteticsnd medical knowledge, and the sys-ematic holistic approach of the nu-rition care process as they relate tohe standards. Three levels of exper-ise in diabetes care, the Generalist,pecialty, and Advanced Practice
evel, are represented in the diabe-es SOP and standards of profes-ional performance (SOPP) based onn RD’s acquisition and develop-ent of knowledge and skills.The SOPP in Diabetes Care are au-
horitative statements that describe aompetent level of behavior in the
tial is designed and intended foretes educator, not for those who mayt of or in the course of other routineprocess used to assess and validaten diabetes education. It is an evaluativety requirements have been met.ent in the field, although some agenciesoyment, job promotions, salary increases, ored by the National Certification Board forl, not-for-profit certification organization.
ent (BC-ADM) This credentialable to perform a complete and/or focusedata to identify needs of patients withpeutic problem solving, counseling, andses on advanced management of clinicalgree before sitting for the examination. Thenagement skills such as medicationplanning, counseling for behavior
optimal metabolic control may includecomplications. The depth of knowledge andiabetes skills affords an increasedthe traditional discipline-specific practice.ng professional development are expectedC-ADM credential may or may not hold them is jointly sponsored by the American
rican Nurses Credentialing Center.b
ation on applying for the CDE credential, visit. bFor information on applying for the BC-ADM/ProfessionalResources/Certification/BC-ADM/
rofessional role, including activities g
March 2009 ● Journa
elated to provision of services, appli-ation of research, communicationnd application of knowledge, use andanagement of resources, quality in
ractice, and continued competencend professional accountability.The diabetes SOP/SOPP identify
Ds as qualified providers of MNTnd self-management skills for per-ons with diabetes, define RD rolesnd responsibilities for diabetes nu-rition care, and identify members of
diabetes care team and benefits ofeam management. RDs use the SOP/OPP for diabetes care to:
Identify the competencies needed toprovide diabetes care inclusive ofdiabetes self-management trainingand MNT;self-assess whether they have theappropriate skill and knowledge baseto provide safe and effective diabetescare for their level of practice;identify the areas in which addi-tional knowledge and skills areneeded to practice at the General-ist, Specialty, or Advanced Practicelevel of diabetes practice;provide a foundation for public ac-countability;assist management in the planningof services and resources;enhance professional identity andcommunicate the nature of dietet-ics; andguide the development of diabetes-related dietetics education pro-grams, job descriptions, and careerpathways (2).
The SOP/SOPP constitute a veryetailed, although not exhaustive, listf specific activities for all three levelsf RD practice for diabetes care.
DA Diabetes Type 1 and 2vidence-Based Nutrition Practiceuideline for Adultsor decades, RDs and their profes-ional association, the ADA, have beennvolved in the development and appli-ation of nutrition protocols, evidence-ased nutrition practice guidelines,nd policies to provide the highestuality care to diabetes patients. TheDA Diabetes Type 1 and 2 Evidence-ased Nutrition Practice Guideline
or Adults (10) includes the most cur-ent recommendations, based on sys-ematically analyzed evidence, that
dendiabparrye i
ibiliym
mplferrenta
geml isx deraocu
dema
iseningnicd ddsinuia Bograme
form.pdf.org
uide RDs in providing quality nutri-
l of the AMERICAN DIETETIC ASSOCIATION 531

F
5
DSME standardsStandard 1 The DSME entity will have documentation of its organizational structure, mission statement, and goals and will recognize andsupport quality DSME as an integral component of diabetes care.
Standard 2 The DSME entity shall appoint an advisory group to promote quality. This group shall include representatives from the healthprofessions, people with diabetes, the community, and other stakeholders.
Standard 3 The DSME entity will determine the diabetes educational needs of the target population(s) and identify resources necessary tomeet these needs.
Standard 4 A coordinator will be designated to oversee the planning, implementation, and evaluation of diabetes self-managementeducation. The coordinator will have academic or experiential preparation in chronic disease care and education and in programmanagement.
Standard 5 DSME will be provided by one or more instructors. The instructor(s) will have recent educational and experiential preparation ineducation and diabetes management or will be a certified diabetes educator. The instructor(s) will obtain regular continuing education in thefield of diabetes management and education. At least one of the instructors will be a registered nurse, dietitian, or pharmacist. A mechanism mustbe in place to ensure that participants’ needs are met if those needs are outside an instructors’ scope of practice and expertise.
Standard 6 A written curriculum reflecting current evidence and practice guidelines, with criteria for evaluating outcomes, will serve as theframework for the DSME entity. Assessed needs of the individual with prediabetesb and diabetes will determine which of the content areaslisted below are to be provided:● Describing the diabetes disease process and treatment options.● Incorporating nutrition management into lifestyle.● Incorporating physical activity into lifestyle.● Using medication(s) safely and for maximum therapeutic effectiveness.● Monitoring blood glucose and other parameters and interpreting and using the results for self-management decision making.● Preventing, detecting, and treating acute complications.● Preventing, detecting, and treating chronic complications.● Developing personal strategies to address psychosocial issues and concerns.● Developing personal strategies to promote health and behavior change.
Standard 7 An individual assessment and education plan will be developed collaboratively by the participant and instructor(s) to direct theselection of appropriate educational interventions and self-management support strategies. This assessment and education plan and theintervention and outcomes will be documented in the education record.
Standard 8 A personalized follow-up plan for ongoing self-management support will be developed collaboratively by participants andinstructor(s). A patient’s outcomes and goals and the plan for ongoing self-management support will be communicated to the referringprovider.
Standard 9 The DSME entity will measure attainment of patient-defined goals and patient outcomes at regular intervals using appropriatemeasurement techniques to evaluate the effectiveness of the educational intervention.
Standard 10 The DSME entity will measure the effectiveness of the education process and determine opportunities for improvement usinga written continuous quality improvement plan that describes and documents a systematic review of the entity’s process and outcome data.
American Association of Diabetes Educators Standards for Outcomes Measurement of DSME1. Behavior change is the unique outcome measurement for diabetes self-management education.2. Seven diabetes self-care behavior measures (listed below) determine the effectiveness of diabetes self-management education at
individual, participant, and population levels.3. Diabetes self-care behaviors should be evaluated at baseline and then at regular intervals after the education program.4. The continuum of outcomes, including learning, behavioral, clinical, and health status, should be assessed to demonstrate the
interrelationship between DSME and behavior change in the care of individuals with diabetes.5. Individual patient outcomes are used to guide the intervention and improve care for that patient. Aggregate population outcomes are
used to guide programmatic services and for continuous quality improvement activities for DSME and the population it serves.
AADE 7 Diabetes Self-Care Behaviors● Healthful eating● Being active● Monitoring● Taking medication● Problem solving● Reducing risks● Healthful coping
igure 4.
32 March 2009 Volume 109 Number 3

tisMaaaaatastfi
tcsrRpdocdieacahaaa
dksfltgthtpc
TtGefo
LMF(
PDNStpdfDdquuvbatesnmDu
Scslhp“DsdswpactttaDbh
fDitDcir
ssvpdpd2hm
ISSattctopoTrpo(ppacctmso
NpRs“r
4FoAEcms
ion care. The companion Toolkit (11)ncludes MNT Protocols—the plan oret of steps RDs apply when providingNT, which define the level, content,
nd frequency of nutrition care that isppropriate for a disease or conditionccording to the setting in which theyre implemented. The MNT protocolsre designed to assist RDs and pa-ients/clients in making decisionsbout appropriate nutrition care forpecific disease states or conditions inypical settings based on researchndings.The Evidence-Based Nutrition Prac-
ice Guidelines and protocols also in-orporate steps of the NCP as thetandard process of care, and incorpo-ate standardized language to helpDs document care provided to theatient/client as well as offer a stan-ardized framework for measuringutcomes. These steps describe theomprehensive assessment, nutritioniagnosis, interventions, and behav-oral as well as clinical outcomes to bexpected as MNT is implemented byn RD during a series of visits or en-ounters. The NCP is unique to RDsnd describes the steps RDs use toelp patients or groups of patientschieve or maintain their nutritionnd health goals for health promotionnd/or disease prevention (4).The guidelines and protocols were
eveloped to enhance the uniquenowledge, critical thinking, andkills of RDs, as well as to provideexibility for RDs to empower pa-ients to make behavior changes re-arding their food choices and achievehe desired clinical outcomes. CMSas specified that RDs must use na-ionally recognized protocols whenroviding MNT to Medicare benefi-iaries with diabetes (12).
In addition to the ADA Diabetesype 1 and 2 Evidence-Based Nutri-
ion Practice Guideline for Adults andestational Diabetes, additional dis-ase-specific guidelines and protocolsor co-morbidities have been devel-ped. These include Disorders of
™™™™™™™™™™™™™™™™™™™™™™™igure 4. National Standards for Diabetes Seutcomes management for DSMEa, and Amemerican Association of Diabetes Educators. Thducators. Diabetes Educator. 2005;31:487-51urrently under Medicare Part B, although the May include prediabetes. Coverage changes a
ervices will be determined through the rulemakin
ipid Metabolism, Adult Weightanagement, Hypertension, Heart
ailure, and Chronic Kidney Disease13).
RACTICE FRAMEWORK SUPPORTINGIABETES CAREational Standards for DSMEimilar to the evidence-based nutri-ion practice guidelines that RDs ap-ly for MNT, national standards foriabetes education are also in placeor services provided by recognizedSMT programs. The DSME Stan-ards are a blueprint that definesuality DSME, allowing diabetes ed-cators to provide evidence-based ed-cation. These Standards are re-iewed approximately every 5 yearsy key organizations and federalgencies within the diabetes educa-ion community (14). Health care pay-rs, such as Medicare, cover DSMTervices when these services are fur-ished by a certified provider whoeets quality standards such as theSME Standards (described in Fig-re 4).The recently released 2007 DSME
tandards outline changes in theomposition of the DSME program in-tructors. For example, Standard 5 noonger requires a DSMT entity toave both an RD and registered nurseroviding DSMT training. Rather,one or more instructor(s) will provideSME,” and “at least one of the in-
tructors will be a registered nurse,ietitian, or pharmacist” (15). Thetandard specifies that the instructorill have recent educational and ex-eriential preparation in educationnd diabetes management or will be aertified diabetes educator. If a pa-ient’s needs are outside an instruc-or’s scope of practice and expertise,hen the program still must ensurend document that the patient’sSME needs are met (15). It shoulde noted that as of this writing, CMSas not provided comment on the ef-
™™™™™™™™™™™™™™™™™™™™™™™™anagement Education (DSME) (14), Americann Association of Diabetes Educators (AADE)cope of Practice, Standards of Practice, and StMedical nutrition therapy and diabetes self-maicare Improvements for Patients and Providersuthorized effective January 1, 2009. Details
g process.March 2009 ● Journa
ect of the revised Standard 5 withSMT regulatory language included
n Medicare Manuals and Transmit-als. In addition, interpretation ofSME Standard 5 on Medicare
laims processing procedures and re-mbursement to solo instructors en-olled in Medicare is not clear.A new Standard 8 requires a per-
onalized follow-up plan for ongoingelf-management support that is de-eloped collaboratively by partici-ants and instructor(s). This stan-ard was added to help improveatients’ long-term outcomes achieveduring the education process. The007 standards also emphasize be-avioral goal setting and measure-ent of outcomes achieved (15).
ssues Raised with the 2007 Nationaltandards for DSME/DSMTtandard 5 references MNT as a keyrea of expertise within the DSMTeam: “The team should have a collec-ive combination of expertise in thelinical care of diabetes, medical nu-rition therapy, educational method-logies, teaching strategies, and thesychosocial and behavioral aspectsf diabetes self-management” (15).his MNT reference underscores theole of RDs on DSMT multidisci-linary teams. However, MNT cannly be provided by licensed/certifiedas applicable) RDs and nutritionrofessionals (MNT regulations andolicies are described in Figure 5),nd is a separate and unique Medi-are Part B service with its own set ofoverage policies. CMS determinedhat the provision of both benefitsay be more medically effective for
ome beneficiaries than receipt of justne of the benefits (16).Another example in which the 2007ational Standards for DSME incor-orate references to MNT provided byDs is found in Standard 6. Thistandard addresses the need for awritten curriculum reflecting cur-ent evidence and practice guide-
™™™™™™™™™™™™™™™™™™™™™™™sociation of Diabetes Educators standards ofen diabetes self-care behaviors. aData from:ards of Professional Performance for Diabetesement training for prediabetes are not coveredadds coverage for preventive services, which
uded as part of the new Medicare preventive
™™ ™™lf-M Asrica seve S and
2. b naged Act
re a incl
l of the AMERICAN DIETETIC ASSOCIATION 533

F
5
MNT regulations and policies● A registered dietitian (RD) or nutrition professionalc must provide MNT services. Medicare enrollment is required prior to providing the
MNT service.● Basic coverage of MNT for the first year a beneficiary receives MNT with a diagnosis of either renal disease or diabetes is 3 hours.
Additional hours are considered to be medically necessary and covered if the treating physician determines that there is a change inmedical condition, diagnosis, or treatment regimen that requires a change in MNT and orders additional hours during that episode ofcare. Nonphysicians are unable to make a referral to an RD for Medicare MNT services.
● An RD/nutritionist may choose how many units of the MNT code are performed at each visit.● Payment will be made under Current Procedural Terminology (CPT) codes 97802, 97803, 97804; G codes G0270 and G0271 when
additional MNT is ordered in the same year.● Services may be provided either on an individual or group basis without restrictions.● The treating physician must make a referral and indicate a diabetes or renal diagnosis.● Basic coverage in subsequent years for MNT for renal disease or diabetes is 2 hours. Additional MNT in subsequent years is considered
to be medically necessary and covered if the treating physician determines that there is a change in medical condition, diagnosis, ortreatment regimen that requires a change in MNT and orders additional hours during that episode of care.
DSMT regulations and policies: Initial training● Initial training is furnished to a beneficiary who has not previously received initial or follow-up training under Healthcare Common Procedure
Coding System G0108 or G0109; is furnished in increments of no less than 1⁄2 hour; and is furnished within a continuous 12-month period.● Training does not exceed a total of 10 hours for the initial training. The 10 hours of training can be done in any combination of 1⁄2-hour
increments. They can be spread over the 12-month period or less.● With the exception of 1 hour of individual training, training is usually furnished in a group setting, although not all group members need
be Medicare beneficiaries.● The 1 hour of individual training may be used for any part of the training including insulin training.● Medicare covers training on an individual basis if no group session is available within 2 months of the date the training is ordered; the
beneficiary’s physician (or qualified nonphysician practitioner) documents in the beneficiary’s medical record that the beneficiary hasspecial needs resulting from conditions that will hinder effective participation in a group training session; or the physician ordersadditional insulin training.
● Payment to nonphysician practitioners billing on behalf of a DSMT program (G0108 or G0109) should be made at the full fee-schedulerate and should not be paid at 85% of the fee schedule like other nonphysician practitioner services. This is because the payment is forthe DSMT program and is not being made for the services of a single practitioner. Nonphysician practitioners who bill on behalf of aDSMT program are subject to mandatory assignment.d
DSMT follow-up training● Follow-up training consists of no more than 2 hours individual or group training for a beneficiary each year.● Group training consists of 2-20 individuals not all of whom need be Medicare beneficiaries.● Follow-up training is furnished any time in a calendar year following a year in which the beneficiary completes the initial training (eg,
beneficiary completes initial training in November 2007; therefore, the beneficiary is entitled to 2 hours of follow-up training beginning inJanuary 2008).
● Training is furnished in increments of no less than 1⁄2 hour.● The physician (or qualified nonphysician practitioner) treating the beneficiary must document in the beneficiary’s medical record that the
beneficiary is diagnosed with diabetes.
Billing DSMT services (2)The Centers for Medicare & Medicaid Services (CMS) DSMT transmittals indicate “only one person or entity from the program bills Medicarefor the whole program,” and “the benefit provided by the program may not be subdivided for the purposes of billing Medicare.” Thefollowing individuals and facilities, who become accredited, may bill for Medicare-covered DSMT services:● A hospital can be the biller without any reassignment. When the DSMT program is accredited under a dietitian or [other CMS recognized
provider], and he or she works for a hospital, then the dietitian or provider would need to reassign his or her benefits to the hospital;then the hospital bills for the DSMT services.
● A physician, as the program physician advisor, can be the certified provider and bill Medicare using the physician’s Medicare providernumber.
● An RD, who has a Medicare provider number and is part of the DSMT program, can bill on behalf of the DSMT program.
Designated certified providers of DSMT (17)CMS regulations indicate, “A designated certified provider bills for DSMT provided by an accredited DSMT program. Certified providers mustsubmit a copy of their accreditation certificate to the contractor. The statute states that a ‘certified provider’ is a physician or otherindividual or entity designated by the Secretary that, in addition to providing outpatient self-management training services, provides otheritems and services for which payment may be made under title XVIII, and meets certain quality standards. CMS is designating all providersand suppliers that bill Medicare for other individual services, such as hospital outpatient departments, renal dialysis facilities, physicians,and durable medical equipment suppliers, as certified. All suppliers/providers who may bill for other Medicare services or items and whorepresent a DSMT program that is accredited as meeting quality standards can bill and receive payment for the entire DSMT program.”
(continued)
igure 5. Diabetes self-management training (DSMT) and medical nutrition therapy (MNT) Medicare regulations and benefit coverage policies.ab
34 March 2009 Volume 109 Number 3

lauclspPseMsDnPM
stcbpcvmp
DaA
cpiUdpt(atDaMim
F
ines,” where the curriculum criteriare further described as, “the curric-lum is dynamic and needs to reflecturrent evidence and practice guide-ines.” Several references cited in thisection of the standards reflect RD-rovided MNT and the Standards ofractice and Standards of Profes-ional Performance for Registered Di-titians in Diabetes Care. ReferencingNT highlights RDs’ role in diabetes
ervices and as key members ofSMT teams, yet also blends compo-ents of the two separate Medicareart B MNT and DSMT programs for
Examples of coordination of MNT and DSExample #1: DSMT program initiated firstThe treating physician/qualified nonphysicianprevious diabetes education, to the recognizMedicare beneficiary would benefit from MNmedically necessary and refers the beneficiahours MNT)
Example #2: Physician refers beneficiaryA Medicare beneficiary with newly diagnoseinitial MNT (3 hours initially—additional houchange in medical condition, diagnosis, or trRD determines that the Medicare beneficiaryto discuss medical necessity for initial DSMTinitial DSMT. Total hours: 13 (3 hours MNT
Example #3: Follow-up MNT and DSMT bAt Year 2 a Medicare beneficiary with type 2Medicare provider. Both services were proviprimary care physician to the DSMT programfor follow-up MNT. Total hours: 4 (2 hours D
aBased on Centers for Medicare & Medicaid Services Mewith diabetes or renal disease) must make a referral andsigned by a physician or qualified nonphysician practitiobSources: Program Memorandum Intermediaries, TransmMedicare & Medicaid Services Web site. http://www.cmsTransmittal AB-02-151: Clarification Regarding Non-PhyCommon Working File Edits for DSMT & Medical NutritAB02151.pdf. Accessed March 8, 2008.cFor Medicare Part B coverage of MNT, only an RD or nlicensed or certified in a state as of December 21, 2000 (or higher degree granted by a regionally accredited collegin nutrition or dietetics, as accredited by an appropriatemay be completed after the completion of the degree) a(documentation of the supervised dietetics practice maya dietitian or nutrition professional by the state in which tmet this requirement if he or she is recognized as a “regabove.dAssignment is an agreement between Medicare and cerproviders or suppliers agree to receive direct payment frapproved amount is composed of the Medicare Part B paand co-pay amounts.eBackground information: Qualifying beneficiaries with direferral from the physician/qualified nonphysician practitan RD Medicare provider for additional hours of MNT beyoregimen that requires a change in MNT; and orders add
igure 5. (Continued).
edicare beneficiaries. m
MNT and DSMT should remain aseparate, complementary programso allow individuals with diabetes ac-ess to quality care offered throughoth covered benefits. Failure to com-ly with each benefit’s regulationsould be grounds for revoking the pro-ider/entity billing privileges and ter-inating the provider/entity from
articipation in Medicare (17).
escription of RD-Provided Medicare MNTnd DSMT Nutrition Educationccording to CMS regulations, RDs
benefitse (not inclusive of all program design
en physician referral to RD Medicare proviactitioner refers the Medicare beneficiary, withDSMT program. The nurse educator who perfohe nurse communicates with the physician a
for initial MNT provided by an RD Medicare pr
MNT for diabetes and DSMT (Service Yearpe 2 diabetes is referred by his or her treatinvailable based on medical necessity and if thment regimen that requires a change in MNT)uld benefit from a DSMT program offered atd the physician determines that DSMT is med10 hours DSMT)
fits (Service Year 2)abetes has completed an initial DSMT programduring the same episode of care (12 monthsr additional insulin instruction and cardiovascT and 2 hours MNT)
e MNT regulations, treating physicians (defined as a primarcate a diagnosis of diabetes or renal disease. Medicare regreating the beneficiary and maintained in the beneficiary’sA-03-009: Medical Nutrition Therapy Services for Beneficia.gov/transmittals/downloads/A03009.pdf. Accessed Septemn Practitioners Billing on Behalf of a Diabetes Outpatient STherapy (MNT). Centers for Medicare & Medicaid Services
on professional may provide the services. “Registered dietiare not required to meet any other requirements); or an indiniversity in the United States (or an equivalent foreign degre
nal accreditation organization recognized for this purpose (s completed at least 900 hours of supervised dietetics prathe form of a signed document by the professional/facility
ervices are performed. In a state that does not provide for led dietitian” by the Commission on Dietetic Registration or
ypes of Medicare Part B providers and suppliers of health che Medicare Part B program and agree to accept the Medint and the applicable deductible and co-pay. The provider o
es are eligible for 2 hours of follow-up DSMT and 2 hours. Both services can provide follow-up in a group or individue initial 2 hours of follow-up MNT if the physician determinesl hours of MNT during the episode of care.
ay provide the nutrition education a
March 2009 ● Journa
omponent of an accredited DSMTrogram, as well as MNT to qualify-ng Medicare Part B beneficiaries.nder the revised DSME Stan-ards, RDs may serve as the solorogram instructor to provide allhe program educational content15). It is important for compliancend payment to distinguish betweenhe nutrition education content of aSMT program and the separatend unique MNT services. Theedicare-accredited DSMT program
ncludes 1 hour of individual assess-ent and 9 hours of group classes,
for MNT (Service Year 1)pe 2 diabetes who has not receiveds the initial assessment indicates that theRD. The physician determines that MNT iser. Total hours: 13 (10 hours DSMT and 3
both benefits occurring simultaneouslyhysician to an RD Medicare provider foreating physician determines that there is athe course of the nutrition assessment, ancal hospital. The RD contacts the physicianlly necessary and refers beneficiary for
nd received initial MNT from an RDhe beneficiary is referred by his or herrisk reduction instruction, and to the RD
e physician or specialist coordinating care for beneficiaryons for DSMT indicate the training order/referral must bein the DSMT’s program records.with Diabetes or Renal Disease—Correction. Centers for2, 2004. Program Memorandum Intermediaries/Carriers,
Management Training Services (DSMT) Program and theb site. http://www.cms.hhs.gov/Transmittals/Downloads/
or nutrition professional” means a dietitian or nutritionistl who, on or after December 22, 2000, holds a bachelor’sith completion of the academic requirements of a programcademic requirements of a nutrition or dietetics programunder the supervision of an RD or nutrition professional
t supervised the individual) and is licensed or certified asure or certification, the individual will be deemed to haveuccessor organization, or meets the requirements stated
quipment and supplies. To accept assignment means theapproved amount as payment in full for the service. Theplier must make a reasonable effort to collect deductible
llow-up MNT annually based on medical necessity and aetting. The treating physician can refer the beneficiary toe is a change in medical condition, diagnosis, or treatment
MT s)
, th derpr ty
ed rmT. T ndry ovid
for 1)—d ty g prs a e treat . Inwo a loan ica
and
enedi a
ded ). Tfo ular
SM
dicar y carindi ulati
ner t fileittal ries.hhs ber 2sicia elf-ion We
utriti tianthey viduae or u e) wnatio the and ha cticebe in thahe s icensister its s
tain t are eom t careyme r sup
abet of foioner al snd th theritiona
nd the curriculum covers nine con-
l of the AMERICAN DIETETIC ASSOCIATION 535
Fn
5
•
•
•
16
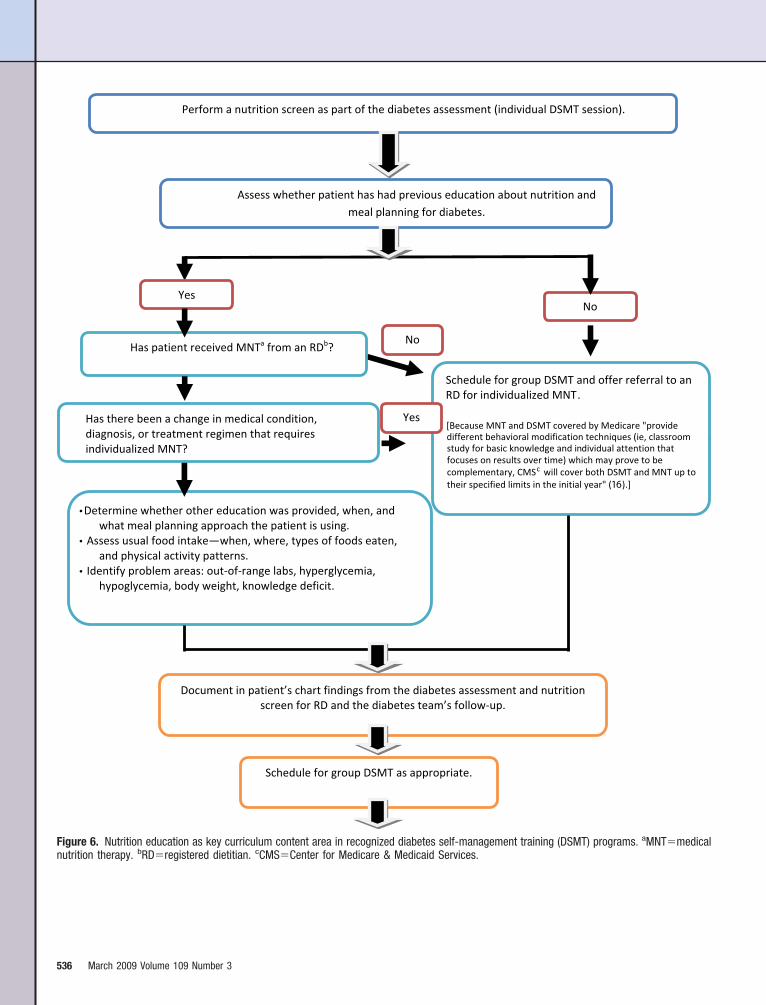
igure 6. Nutrition education as key curriculum content area in recognized diabetes self-management training (DSMT) programs. aMNT�medical
utrition therapy. bRD�registered dietitian. cCMS�Center for Medicare & Medicaid Services.36 March 2009 Volume 109 Number 3

trlv
oma
abs
F
ent areas, one of which is “incorpo-ating nutritional management intoifestyle” (Figure 6). MNT for indi-
o
o o o o
igure 6. (Continued).
iduals with diabetes is provided h
ver several visits and includesore intensive nutrition counseling
nd a therapy regimen that relies
eavily on follow-up and feedback to wMarch 2009 ● Journa
ssist patients with changing theirehavior(s) over time. Figure 7 de-cribes the unique steps RDs apply
hen providing MNT.l of the AMERICAN DIETETIC ASSOCIATION 537

NPOPTectntstidtdcbipsiMtwogptd
cmpwhuaivpevdutaittMrwtrm
bM“
ipBiianamlttDRstF
CRdoppgaRps
F vide
5
UTRITION EDUCATION ACTIVITIESROVIDED BY PROGRAM INSTRUCTORSF NATIONALLY RECOGNIZED DSMTROGRAMShere may be instances in which sev-ral of the key members of a multidis-iplinary diabetes team (ie, a regis-ered nurse, RD, and pharmacist) areot available to provide DSMT educa-ion, so one qualified program in-tructor administers all content forhe program. CMS DSMT regulationsndicate that, “In a rural area, an in-ividual who is qualified as a regis-ered dietitian and as a CDE [certifiediabetes educator] that is currentlyertified by an organization approvedy CMS . . . may furnish training ands deemed to meet the multidisci-linary team requirement” (18). [Ithould be noted that as of this writ-ng, CMS has indicated that the
edicare Benefit Policy Manual, Sec-ion 300.2 (2), will be updated to alignith language in the Electronic Codef Federal Regulations (18).] Solo pro-ram instructors are expected toractice only at the level at whichhey are competent, which will vary
Application of Nutrition Care Process (NC
Nutrition screen/referral
Nutrition assessment
Nutrition diagnosis
Nutrition intervention
Nutrition monitoring and evaluation
Nutrition documentation (supports all steps othe Nutrition Care Process)
Outcomes management systems
igure 7. Medical nutrition therapy (MNT) pro
epending on the practitioner’s edu- q
38 March 2009 Volume 109 Number 3
ation, training, and experience. Also,embers of all health disciplines who
rovide DSMT need to be familiarith the boundaries of their ownealth profession, which may be reg-lated by national or state agencies orccrediting bodies (15,17). Expertisen diabetes care develops throughenues such as experience, advancedractice, additional certified diabetesducator and/or board certified–ad-anced diabetes management cre-entials (see Figure 3), continuing ed-cation, individual study, and men-orship. However, in cases where theccredited DSMT program does notnclude an RD, solo program instruc-ors should make recommendationso the referring physician to orderNT provided by an RD. The sepa-
ate and individualized MNT sessionsill help ensure that a patient’s nu-
rition needs and goals are incorpo-ated into the overall diabetes treat-ent plan.As described in the American Dia-
etes Association’s Standards ofedical Care in Diabetes—2008 (19),
achieving nutrition-related goals re-
MNT Provided by RD (for individual)
The physician provider sends RD writtenincludes information regarding currendiagnoses.
RD performs a comprehensive nutrition2 Evidence-Based Nutrition Practice Gbest available current knowledge andand other resources.
After analyzing assessment data, RD minconsistent carbohydrate intake (NI-5intake throughout the day, day to daynot consistent with recommended paneeds.
RD provides counseling and, with clientbehavioral model, including problemand self-monitoring.
Plan follow-up over multiple visits to asthe nutrition diagnoses and medical c
RD monitors hemoglobin A1c, microalbugoals for food plan/intake, activity, an
Implements changes to MNT (eg, patiencounseling) in future visits based on
RD documents MNT initial assessment,shares with referring physician and k
Based on RD analysis, critical thinking,history and other healthcare professiooutcomes data. Analyze and share windicated. Implement improvements t
d by registered dietitians (RDs).
uires a coordinated team effort that p
ncludes the active involvement of theerson with prediabetes or diabetes.ecause of the complexity of nutrition
ssues, it is recommended that a reg-stered dietitian who is knowledge-ble and skilled in implementingutrition therapy into diabetes man-gement and education be the teamember who provides MNT.” Simi-
arly, an RD is recommended to be theeam member who provides the nutri-ion education component of theSMT curriculum; however, when anD is not available to teach the groupession, the non-RD program instruc-or may perform tasks described inigure 6.
ONCLUSIONSDs have a defined and unique role iniabetes care that differs dependingn whether the service is for MNT orart of a DSMT program. RDs mayarticipate in recognized DSMT pro-rams as a sole program instructor ors part of a multidisciplinary team.Ds or other qualified health carerofessionals who operate as solo in-tructors in DMST programs must
ferral for MNT for diabetes. The referralbs, medications, and other medical
essment utilizing the Diabetes Type 1 andeline for Adults and Toolkit, as well as theidence, client data, medical record data,
initial nutrition diagnosis(es); for example,4), inconsistent timing of carbohydrater a pattern of carbohydrate intake that isn based on physiological or medication
termines interventions using the cognitive-ing, motivational interviewing, goal setting,
with behavior/lifestyle changes relative toition/disease(s).uria, body mass index, serum lipid levels,ther behavior changes.trition goals, nutrition intervention, andomes and assessments at each visit.
rition diagnosis(es) and intervention(s);s copy on file.review of data from the patient’s medical
s, RD aggregates individual and populationquality improvement department/group asNT services based on results.
P)
ret la
assuidev
akes.8., otter
, desolv
sistondmind ot nuoutc
f nuteepandnal
itho M
ractice only at the level at which

tdtcnamacDspnd
dRcCmEGsmDNMfrr
vsurfimcctincMobb
R
1
1
1
1
1
1
1
1
1
1
2
2
2
hey are competent, which will varyepending on an individual’s educa-ion, training, and experience. Healthare practitioners who provide DSMTeed to be familiar with the bound-ries of their own profession, whichay be regulated by national or state
gencies or accrediting bodies. Inases where RDs are not part ofSMT teams, referral to an RD for
eparately administered MNT is ap-ropriate to ensure that an individualutrition plan is integrated into theiabetes plan of care.The Standards of Practice and Stan-
ards of Professional Performance foregistered Dietitians (Generalist, Spe-
ialty, and Advanced) in Diabetesare (3) describe levels of perfor-ance for RDs in diabetes care.vidence-Based Nutrition Practiceuidelines (10) and Toolkits (11)
erve as guides for RDs for imple-enting quality MNT services.SMT-recognized programs rely onational Standards for Diabetes Selfanagement Education as the basis
or the program curriculum and theespective health care professional’sole in the program.
All health care professionals in-olved in diabetes care have a respon-ibility and must be accountable tophold Medicare and other diabetesegulations. Medicare regulations de-ne the unique program require-ents for diabetes services. A health
are professional’s recognition of theomplementary nature of the educa-ion and training curriculum includedn Medicare DSMT programs and theutritional diagnostic, therapy, andounseling services provided throughedicare MNT will allow the greatest
pportunity for individuals with dia-etes to receive quality care throughoth services.
eferences1. Education Recognition Program. American
Diabetes Association Web page. http://professional.diabetes.org/recognition.aspx?cid�57995. Accessed September 22, 2008.
2. Medicare Benefit Policy Manual. Section300—Diabetes Self-Management TrainingServices. Centers for Medicare & MedicaidServices Web site. http://www.cms.hhs.gov/Manuals/downloads/bp102c15.pdf. AccessedSeptember 22, 2008.
3. Kulkarni K, Boucher JL, Daly A, Shwide-Slavin C, Silvers BT, O’Sullivan Maillet J,Pritchett E. American Dietetic Association:Standards of practice and standards of pro-
fessional performance for registered dieti-tians (generalist, specialty, and advanced) indiabetes care. J Am Diet Assoc. 2005;105:819-824.
4. Lacey K, Pritchett E. Nutrition Care Processand Model: ADA adopts road map to qualitycare and outcomes management. J Am DietAssoc. 2003;103:1061-1072.
5. American Diabetes Association. Economiccosts of diabetes in the US in 2007. DiabetesCare. 2008;31:1-20.
6. Knowler WC, Barrett-Connor E, Fowler SE,Hamman RF, Lachin JM, Walker EA,Nathan DM; Diabetes Prevention ProgramResearch Group. Reduction in the incidenceof type 2 diabetes with lifestyle interventionor metformin. N Engl J Med. 2002;346:393-403.
7. Diabetes Control and Complications TrialResearch Group. The effect of intensivetreatment of diabetes on the developmentand progression of long-term complicationsin insulin-dependent diabetes mellitus.N Engl J Med. 1993;329:977-986.
8. The role of the registered dietitian in teach-ing and in administration of injectable med-ications used in diabetes management. Dia-betes Care and Education Dietetic PracticeGroup Web site. http://www.dce.org/files/2007_Winter_Statement_on_Injectable_Medication_DCE-OCTE.pdf. Accessed July 18, 2008.
9. O’Sullivan Maillet J, Skates J, Pritchett E.American Dietetic Association: Scope of die-tetics practice framework. J Am Diet Assoc.2005;105:634-640.
0. Diabetes 1 and 2 Evidence Analysis Project.American Dietetic Association EvidenceAnalysis Library Web site. http://www.adaevidenceslibrary.com/topic.cfm?cat�1615.Accessed September 10, 2008.
1. Nutrition Practice Guidelines CurrentlyAvailable Online. American Dietetic Associa-tion Evidence Analysis Library Web site.https://www.adaevidencelibrary.com/category.cfm?cid�14&cat�0#DM_Toolkit. AccessedSeptember 10, 2008.
2. Electronic Code of Federal Regulations: Def-initions, § 410.130, Subpart G—Medical Nu-trition Therapy, 66 FR 55331, Nov. 1, 2001.Government Printing Office Web site. http://ecfr.gpoaccess.gov/cgi/t/text/textidx?idno�42;region�DIV1;type�boolean;c�ecfr;cc�ecfr;sid�9537ebba42c27284de612af465eba549;q1�410.140;rgn1�Section;op2�and;rgn2�Section;op3�and;rgn3�Section;rgn�div5;view�text;node�42%3A2.0.1.2.10#42:2.0.1.2.10.2.35.2. Accessed May 30, 2008.
3. Evidence Analysis Library Guideline List—Diseases & Conditions Topics. American Die-tetic Association Evidence Analysis LibraryWeb site. https://www.adaevidencelibrary.com/topic.cfm?cat�3781. Accessed September10, 2008.
4. Funnell MM, Brown TL, Childs BP, HaasLB, Hosey GM, Jensen B, Maryniuk M, Pey-rot M, Piette JD, Reader D, Siminerio LM,Weinger K, Weiss MA. National standardsfor diabetes self-management education. Di-abetes Care. 2007;30:1630-1637.
5. Funnell M. National standards for diabetesself-management education: What do theymean for providers? Rev Endocrinol. 2007;1:51-53.
6. NCD decision memo for medical nutritiontherapy benefit for Diabetes & ESRD(CAG-00097N). Centers for Medicare &Medicaid Services Web site. http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?from2�
viewdecisionmemo.asp&id�53&. AccessedMay 25, 2007.March 2009 ● Journa
7. Medicare Claims Processing Manual: Chap-ter 4–Part B Hospital, Section 300. Centersfor Medicare & Medicaid Services Web site.http://www.cms.hhs.gov/manuals/downloads/clm104c04.pdf. Accessed May 25, 2007.
8. Electronic Code of Federal Regulations:Quality standards for deemed entities, §410.144 subpart H—Outpatient diabetesself-management training and diabetes out-come measurements. Government PrintingOffice Web site. http://ecfr.gpoaccess.gov/cgi/t/text/textidx?idno�42;region�DIV1;type�boolean;c�ecfr;cc�ecfr;sid�9537ebba42c27284de612af465eba549;q1�410.140;rgn1�Section;op2�and;rgn2�Section;op3�and;rgn3�Section;rgn�div5;view�text;node�42%3A2.0.1.2.10#42:2.0.1.2.10.8. AccessedOctober 2, 2008.
9. American Diabetes Association. Standardsof medical care in diabetes—2008. DiabetesCare. 2008;31(suppl 1):S12-S54.
0. US Federal Code of Regulations: PartE—Miscellaneous Provisions: Definitions ofservices, institutions, etc, Sec. 1861. [42U.S.C. 1395x]. Social Security Administra-tion Web site. http://www.ssa.gov/OP_Home/ssact/title18/1861.htm. Accessed May 30,2008.
1. Medicare Program. Expanded coverage foroutpatient diabetes self-management train-ing and diabetes outcome measurements,Part 4, Subpart H. US Government PrintingOffice Web site. http://frwebgate.access.gpo.gov/cgibin/getdoc.cgi?dbname�2000_register&docid�00-32703-filed.pdf. Accessed May 30,2008.
2. Medicare Learning Network. Medicare pre-ventive services: Diabetes-related services.Centers for Medicare & MedicaidServices Web site. http://www.cms.hhs.gov/MLNProducts/downloads/DiabetesSvcs.pdf. Accessed May 31, 2008.
l of the AMERICAN DIETETIC ASSOCIATION 539


















