Just a Ding? The NFL responds to research on football-related concussion.
Upload
protectthebrainCategory
view
218download
0description
Seediscussions,stats,andauthorprofilesforthispublicationat:http://www.researchgate.net/publication/7482989
Concussioninprofessionalfootball:brainresponsesbyfiniteelementanalysis:part9.ARTICLEinNEUROSURGERYDECEMBER2005ImpactFactor:3.03DOI:10.1227/01.NEU.0000186950.54075.3BSource:PubMed
CITATIONS69
DOWNLOADS281
VIEWS240
6AUTHORS,INCLUDING:
LiyingZhangWayneStateUniversity67PUBLICATIONS1,238CITATIONS
SEEPROFILE
AlbertKingWayneStateUniversity127PUBLICATIONS3,078CITATIONS
SEEPROFILE
KingYangWayneStateUniversity204PUBLICATIONS3,134CITATIONS
SEEPROFILE
Availablefrom:KingYangRetrievedon:18June2015
CLINICAL STUDIES
CONCUSSION IN PROFESSIONAL FOOTBALL: BRAINRESPONSES BY FINITE ELEMENT ANALYSIS: PART 9
David C. Viano, Dr. med,Ph.D.ProBiomechanics, LLC,Bloomfield Hills, Michigan,Bioengineering Center,Wayne State University,Detroit, Michigan
Ira R. Casson, M.D.Department of Neurology,Long Island Jewish Medical Center,New Hyde Park, New York,and Department of Neurology,Albert Einstein College of Medicine,Bronx, New York
Elliot J. Pellman, M.D.ProHEALTH Care Associates, LLPLake Success, New York
Liying Zhang, Ph.D.Bioengineering Center,Wayne State University,Detroit, Michigan
Albert I. King, Ph.D.Bioengineering Center,Wayne State University,Detroit, Michigan
King H. Yang, Ph.D.Bioengineering Center,Wayne State University,Detroit, Michigan
Reprint requests:David C. Viano, Dr. med, Ph.D,ProBiomechanics, LLC,265 Warrington Road,Bloomfield Hills, MI 483042952.Email: [email protected]
Received, March 3, 2005.
Accepted, September 8, 2005.
OBJECTIVE: Brain responses from concussive impacts in National Football Leaguefootball games were simulated by finite element analysis using a detailed anatomicmodel of the brain and head accelerations from laboratory reconstructions of gameimpacts. This study compares brain responses with physician determined signs andsymptoms of concussion to investigate tissue-level injury mechanisms.METHODS: The Wayne State University Head Injury Model (Version 2001) was usedbecause it has fine anatomic detail of the cranium and brain with more than 300,000elements. It has 15 different material properties for brain and surrounding tissues. Themodel includes viscoelastic gray and white brain matter, membranes, ventricles, craniumand facial bones, soft tissues, and slip interface conditions between the brain and dura. Thecranium of the finite element model was loaded by translational and rotational accelera-tions measured in Hybrid III dummies from 28 laboratory reconstructions of NFL impactsinvolving 22 concussions. Brain responses were determined using a nonlinear, finiteelement code to simulate the large deformation response of white and gray matter. Strainresponses occurring early (during impact) and mid-late (after impact) were compared withthe signs and symptoms of concussion.RESULTS: Strain concentration hot spots migrate through the brain with time. In 9 of22 concussions, the early strain hot spots occur in the temporal lobe adjacent to theimpact and migrate to the far temporal lobe after head acceleration. In all cases, thelargest strains occur later in the fornix, midbrain, and corpus callosum. They signifi-cantly correlated with removal from play, cognitive and memory problems, and loss ofconsciousness. Dizziness correlated with early strain in the orbital-frontal cortex andtemporal lobe. The strain migration helps explain coup-contrecoup injuries.CONCLUSION: Finite element modeling showed the largest brain deformations oc-curred after the primary head acceleration. Midbrain strain correlated with memoryand cognitive problems and removal from play after concussion. Concussion injurieshappen during the rapid displacement and rotation of the cranium, after peak headacceleration and momentum transfer in helmet impacts.
KEY WORDS: Concussion, Finite element modeling, Football helmets, Head injury, Injury mechanisms,Sport injury
Neurosurgery 57:891-916, 2005 DOI: 10.1227/01.NEU.0000186950.54075.3B www.neurosurgery-online.com
Computer models are now capable ofsimulating fine anatomic detail andtissue-level characteristics for impactsleading to injury (74, 75). The current studyuses this powerful tool to study the mecha-nisms of concussion signs and symptoms byinvestigating strain and strain rate in thebrain. Accelerations measured in Hybrid IIIdummy reconstructions of National FootballLeague (NFL) game concussions were used as
input to the cranium of the finite element (FE)model (122, 123).FE models have assisted researchers study-
ing brain contusion (25, 150), subdural hema-tomas (64, 65), brain edema (101), and braindeformation (94, 152, 153, 155, 165, 167, 168).However, there has been limited FE analysisof concussion and diffuse axonal injury. Ruanet al. (134, 135) and Zhou et al. (175, 176)indicated that shear stress and strain re-
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 891
sponses could be the injury indicator for diffuse axonal injuryand subarachnoid hematoma. Bandak and Eppinger (17) sug-gested that an accumulated volume of elements exceeding atolerable principal strain, referred to as the cumulative straindamage measure, was related to diffuse axonal injury.The Wayne State University Head Injury Model (WSUHIM)
Version 2001 is themost sophisticated FEmodel of the brain (171,172, 173). It has a long history of development and validationsince 1993, and it has been subjected to many investigations andimprovements (134, 135, 136, 170, 171, 174, 175, 176). Al-Bsharatet al. (7) modified an earlier FE model developed by Zhou et al.(176) to simulate large relative motion between the brain and thecranium, showing that proper modeling of the interface betweencranium and brain was a factor in predicting brain injury. Thisparalleled work by Bandak et al. (18), although the NationalHighway Traffic Safety Administration model only simulatedthe upper portion of the brain.All FE numerical simulations rely on experimental studies
of brain injury to determine material responses and predictfailures. There have been investigations into brain contusion(3, 72, 76, 96, 115, 132), subdural hematoma (91), diffuse axonalinjury (4, 5, 10, 15, 16, 43, 70, 86, 88, 107, 125, 133, 146, 147),concussion (1, 49, 50, 112, 156), brain displacement (35, 47, 57,81, 128, 129), directional sensitivity of injury (42, 60), and headimpact tolerances (108, 110, 113). Physical models have beenused to bridge information from cadaver and animal researchto FE modeling. These studies provide insights into braininjury mechanisms (8, 20, 34, 52, 53, 55, 59, 61, 66, 67, 68, 86,163). However, none of the above studies have used injurydata from in-depth study of on-field football concussions todetermine brain responses related to injury.Sports-relatedmild traumatic brain injury (MTBI) has received
attention because of the large number of people affected at thehigh school and college levels; however, sport injury is just aportion of the overall incidence of mild to serious brain injury.With the advent of airbags and safety belt use in automobilecrashes and the introduction of improved protective devices insport, the incidence of serious-fatal brain injury has been decreas-ing (6, 21, 77, 78, 87, 149, 151, 157). Football helmets have devel-oped an effective padding system, which has prevented severehead injuries in NFL players, however, they have only recentlystarted addressing designs to prevent concussion, and much lesshas been understood of the biomechanics of concussion. Therecent work of the NFL MTBI Committee has aimed at advanc-ing the understanding of concussions (117123, 162) and promot-ing improved helmet designs to prevent concussion.Current standards for head injury risk assessment use the
Gadd Severity Index (SI) and Head Injury Criterion (HIC),which are based on the resultant translational acceleration atthe center of gravity (cg) of the head (39, 158). These criteriaare based on the Wayne State University tolerance curve,which was based on head accelerations from animal concus-sions and cadaver cranium fractures from rigid, flat surfaceimpacts on the forehead (80). These criteria are used in safetystandards to assess head protection against automobile andsport injuries. However effective these criteria may be, it is
believed that they cannot account for the complex motion ofthe brain in a deformable cranium. Foremost, the criterianeglect the contribution of head angular acceleration to injuryand the directional sensitivity of brain injuries, and local fail-ure modes of brain tissue are not currently specified (4345).On the basis of research conducted over the past 4 decades,
a widely held belief is that angular acceleration is more dam-aging than linear acceleration (44, 45), even though in anyhead impact, both forms of acceleration occur. Research on theeffects of angular acceleration has been pursued more vigor-ously than that on the effects of linear acceleration in anattempt to find a tolerance limit for angular acceleration andvelocity (43, 86, 126). Although there has been considerableresearch on brain injury, the biomechanical focus has been onwhich of the two types of head acceleration cause injury.There has been much less attention on specific brain responsesthat are the underlying cause for neural tissue injury. Tissuerelated strain, strain-rate, and product of strain and strain-rateare relevant to neural injury (161).This article studies brain response at the tissue level. The
responses include strain, strain rate, and product of strain andstrain rate, which were determined for NFL football impactscausing concussion or severe helmet loadings without injury.Brain responses were simulated using the 2001 version of theWSUHIM FE model, which simulates the essential anatomicfeatures of a human head and brain and has been validatedwith cadaver data (172, 173). The FE model determines intra-cranial pressure, stress, and strain in the brain from headaccelerations measured in NFL impact reconstructions (104106, 121, 122). Statistical analyses have been conducted todetermine initial concussion predictors and to estimate injuryprobability. The strongest correlation of concussion was withthe product of strain and strain rate (174).In this study, brain responses with concussion were studied
through the use of NFL head impact data to establish relationshipsbetween brain responses and injury. Concussion in NFL footballprovided a unique living laboratory to study mechanisms ofinjury and human tolerance with possible extrapolation to the gen-eral population. Performing game impact reconstructions using theHybrid III dummy (13) in laboratory reconstructions provided in-puts to the anatomically detailed FEmodel to predict the extent andseverity of brain responses for each game impact. The goal was todetermine brain responses associated with specific signs, symp-toms, andoutcomes of concussion. This approach is unlike previousstudies, which determined tolerance limits for human head injurybased on head input kinematics either scaled from animal data ornoninjurious volunteer test results. The ultimate goal was to im-prove the understandings of helmet designs to reduce concussion infootball and other contact sports.A case-by-case computer simulation was carried out using
the head kinematics obtained from laboratory reconstructionsof game impacts to drive a FE model. Brain tissue responseswere calculated to identify sites of high deformation. Thesetissue-level responses were used to study injury mechanisms.A validated FE model along with tissue tolerance data offereda means of identifying and quantifying the incidence of con-
VIANO ET AL.
892 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
cussion. Concussion is an injury with many signs and symp-toms, which can have their origin in specific regions of thebrain as well as from diffuse injury. It is also a threshold injuryin the spectrum of brain injuries involving contusion, diffuseaxonal injury, and coma.Twenty-two NFL concussions were known to interrupt brain
function, whereas an additional six cases of severe impact with-out injury were used to determine a threshold for loss of brainfunction. Head kinematics of the helmeted Hybrid III headformwas defined by three translational and three rotational accelera-tion components in an anatomic, body-fixed reference frame. Thedata were measured directly from the laboratory reenactment ofthe head collisions and were used as input to the WSUHIM. Bydefining the outer surface of the cranium as a rigid body andapplying the head kinematics at the head cg, the loading bound-ary conditions of the head were prescribed.
MATERIALS AND METHODS
Finite Element Model of the Head and Brain
This study used the latest version of the WSUHIM (Version2001). This model has a fine mesh representing the humancranium, membranes, brain, and ventricles in three-dimensional (3D) FEs (172174). The average characteristiclength of the brick or shell elements was approximately 2 mm.Such a fine mesh size enabled more detailed and accuratemodeling of anatomic features of the human head. The grossgeometry of the head was taken from the model by Al-Bsharatet al. (7), whereas the boundaries between anatomic structureswere based on anatomic drawings (90). The model simulatesthe essential anatomic features of a 50th percentile male head,including the scalp, cranium with an outer table, diplo, andinner table, dura, falx cerebri, tentorium, pia, sagittal sinus,transverse sinus, cerebrospinal fluid (CSF), hemispheres of thecerebrum with distinct white and gray matter, cerebellum,brainstem, lateral ventricles, third ventricles, and bridgingveins. The 50th percentile Hybrid III head is used on the 50th
and 95th percentile Hybrid III dummy, so it is relevant toaverage and larger sized males.For this study, the cranium was assumed rigid, and the trans-
lational and rotational acceleration from laboratory reconstruc-tions of concussion impacts in the NFL were used to load thehead (122, 123). The accelerations define the motion of the headcg, and they were transferred to the cranium boundary nodes toload the brain in a manner identical to the motion of the HybridIII dummy in the game reconstruction. The face, scalp, andthree-layer cranium assume rigid bodies while maintaining thehead weight and moment of inertia. This also reduced compu-tational time because cranium accelerations were the means toload the brain. The cranium-brain model consisted of 281,800nodes and 314,500 elements and amass of 4.5 kg. Themesh of themodel was developed using a preprocessor (HyperMesh, Ver-sion 3.1, Altair Engineering, Inc., Troy, MI). A nonlinear explicitFE solver (PAM-CRAS, Version 2000, ESI Group, Paris, France)was used for model analysis. The results were plotted using aninteractive graphics postprocessor (PAM-VIEW Version 2000,ESI, Paris, France). For this FE model, it takes approximately 36hours to complete a 20 ms simulation using a PC with 2.7 GHzPentium IV using a Linux operating system.
Skull and Dural Partition
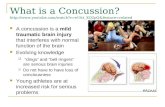
Figure 1 shows the sagittal and coronal section through thecranium of the WSUHIM version 2001. The dimensions of theinterior volume include a 171 mm length, 138 mm width, and152 mm height. The cranium resembles a sandwich structurecontaining cancellous and cortical bones. The cranium modelwas meshed with three layers to represent an outer table,diplo, and inner table. The base of the cranium includes theforamen magnum, which has a characteristic diameter of 31mm. The falx cerebri, tentorium, and sinus (superior sagittalsinus, transverse sinus, and straight sinus) are also shown. Thefalx has a maximum depth of 40 mm and thickness of 1 mm,whereas the tentorium has depth of 51 mm. The craniumweighs 1.3 kg.
FIGURE 1. Skull, falx cerebra, tentorium, and dura-sinus.
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 893
Brain Model
Figure 2 shows the representation of the brain. It includescerebrum with gray and white matter, brainstem, and cerebel-lum (90). The right and left hemispheres of cerebrum areconnected internally by a corpus callosum. The length andtransverse diameter of the brain are 167 mm and 134 mm,respectively. The midbrain of the brainstem is located in theopening of the tentorium. The medulla oblongata is repre-sented in the posterior cranial fossa just superior to the level ofthe foramen magnum. The brainstem diameter measures 7mm. The brain weighs 1.4 kg.
Subarachnoid Space
The dura mater is firmly attached to the internal surface ofthe cranium. The outer layer of the arachnoid membraneslides freely with respect to the innermost layer of the dura.The subarachnoid space is filled with CSF. The CSF and thearachnoid trabaculae suspend the brain in the cranium.Several algorithms were reviewed by Al-Bsharat et al. (7) to
determine which one was the most suitable to model the CSFlayer and brain-cranium interface. The best approach was tomodel the CSF with solid elements in addition to the definitionsliding interface between the dura and the CSF. The model useda low shear modulus solid, which allowed relative displacementbetween the brain and the craniumas well as intracranial pressure tomatch that obtained experimentally.Pudenz and Shelden (128), and
Meaney (91) suggested that pure-sliding condition was a realistic in-terface for the simulation of head-brain kinematics. According toUeno et al. (155), separation of thebrain from the dura mater is un-likely to occur in blunt head im-pacts because of nearly incom-pressible nature of the brain tissue.
Bridging Veins and Ventricles
Figure 3 shows the bridgingveins and lateral and third ventri-
cles. Ten pairs of bridging veins were included with length of8 to 17 mm and orientation of 160 to 1100 on the basis ofpublished data (108a). The lateral ventricle has a length of 102mm and width of 66 mm, whereas the third ventricle has alength, width, and height of 33, 20, and 5 mm, respectively.The intracranial membranes, CSF, ventricles, and blood ves-sels weigh 0.26 kg.The lateral and third ventricles are explicitly modeled using
solid elements because fluid elements are not available in thecurrent simulation code. A shear modulus that is lower than thatof the subarachnoid CSFwas assumed for thematerial propertiesof the ventricles. No sliding was defined in the interface betweenthe ventricular CSF and the ventricular cavity.
Face Model
Because the input acceleration was to the cranium, whichwas assumed rigid, the face was not a factor except for its massin the simulations. However, for completeness, it will be de-scribed. The FE face model consists of 14 bones, two zygo-matic bones in the cheek, two maxillae forming the upper jaw,most of the side walls of the nose, and front part of the hardpalate, two palate bones forming the rest of the hard palateand part of the floor and side walls of the nasal cavity, twolacrimal bones (one in each eye socket or orbit), two nasal
FIGURE 2. Representation of the brain.
FIGURE 3. Bridging veins, ventricle, and brainstem.
VIANO ET AL.
894 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
bones forming the bridge of the nose, two turbinate bonesinside the nose, one vomer forming the posterior and inferiorpart of the nasal septum, and one mandible forming the lowerjaw. The face geometry was based on magnetic resonanceimaging and computed tomography scans from the VisualHuman Project database available from the National Libraryof Medicine (Bethesda, MD). The images were transverse sec-tions scanned at 1 mm intervals along the vertical axis of thebody and scaled to the cranial size of the 50th percentile malehead model. Because of the irregularity and complexity of thefacial bony structures, the bone geometry was simplified andsmoothed while preserving the structural features of the hu-man face. The facial model consisted of 36,400 elements with amass of 0.78 kg and was integrated with the cranial model.
Material Properties
Table 1 gives the material properties used to simulate theviscoelastic brain. Biological materials display both elastic andviscous properties. Brain tissue is a hydrated soft tissue con-sisting of approximately 78% water. It is similar to a soft gelwhen defined as an engineering material (61). Experimentalcharacterization of brain materials from a variety of speciessuggests that brain tissue exhibits incompressible viscoelasticbehavior (38, 41). The bulk modulus of brain tissue was similarto water, with a value of approximately 2.00 GPa according toStalnaker (145) and 2.10 GPa according to McElhaney et al.(89). Traditionally, the material behavior of the brain has beenapproximated by a Kelvin (viscoelastic) model, which is acombination of linear springs and dashpots. The behavior ofthis material is characterized as viscoelastic in shear with thedeviatoric stress rate dependent on the shear relaxation mod-ulus, whereas the hydrostatic behavior of the brain was con-sidered elastic. The shear modulus of the viscoelastic brainmaterial was expressed by:
Gt G G0 Get (1)
where G0 is the short-term shear modulus, G is the long-termshear modulus, is a decay constant, and t is the duration (170).The cerebral hemispheres are composed of white matter
and gray matter. The neuroarchitecture of brain tissue isnaturally inhomogeneous and anisotropic. The shear mod-ulus of the white matter was assumed to be 25% higher than
that of the gray matter be-cause of the fibrous natureof the white matter to incor-porate different materialcompositions of white andgray matter. The brain wasmodeled as isotropic be-cause anisotropic propertiesof the brain are not avail-able at present. The materialproperties assigned to thebrain did consider the re-gional differences between
the cerebrum white matter and the brainstem.Pieropaoli and Basser (124) indicated that some regions of
white matter could be modeled as a transversely isotropic struc-ture and gray matter as isotropic structures on the basis ofmagnetic resonance diffusion tensor images of the brain neuro-architecture. Experimental results obtained from oscillatoryshear tests of pig brain tissue revealed that the complex shearmodulus for the brainstem regionwas 80% larger than that of thecerebrum tissue at large strain (11). These regional differencescan affect the mechanical stress or strain response during animpact. In addition, the upper brainstem is considered by manyresearchers as a critical anatomic substrate responsible for main-taining the state of consciousness (3, 28, 29, 54, 70, 85, 125, 132).The short-term shear modulus assumed for the brainstem was80% higher than that for the cerebral white matter.Studies have characterized the brain shear properties (38, 41,
143, 144). Reported shear moduli varied from one study to an-other. Recently, Arbogast et al. (12) reported that the instanta-neous shear moduli were 1040 Pa for white matter in the brainstem and 680 Pa for gray matter in an experimental study usingpig brain. In their study, the brain tissues were dissected fromadult pigs, and vibratory shear forces were applied while thebrain sample was placed between two parallel plates. Shearmoduli were calculated for these tissues as a function of excita-tion frequency. However, the experimental results did not fullyreflect the tethering effect of the blood vessels in an intact brainbecause of the dissection of the brain tissue alters the property ofthe complex network of blood vessels.In the current model, the material properties for the solid
elements representing the CSF have the bulk modulus of waterand a very low shear modulus. This considered a combinedeffect of fibrous trabaculae and the fluid nature of the CSF. Theaverage thickness of the CSF layer was less than 2 mm. Alow-friction slip algorithm is used tomodel the interface betweenthe dura and the arachnoid membrane. In addition, the interfacealgorithm allows no separation of the two layers in contact andtherefore prevents the formation of a gap in the arachnoidmembrane-dura interface. From the numerical stability point ofview, allowing separation is prone to result in an excessivedistortion of the soft brain elements and to generate unrealisticintracranial pressures when a gap is developed.
TABLE 1. Viscoelastic material properties simulating the brain
Brain tissue Density g/ccShear modulus
Decay constant s1 Bulk modulus GPaG kPa G8 kPa
Gray matter 1.06 10.0 2.0 80 2.19
White matter 1.06 12.5 2.5 80 2.19
Brainstem 1.06 22.5 4.5 80 2.19
Cerebellum 1.06 10.0 2.0 80 2.19
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 895
Dobrin (33) reported that the vascular wall of small arteries(4mm in diameters) containmainly smoothmuscleswith somecollagen fibers. Collagen contributes to the load bearing roleunder large tensions (131). Although complete and detailed in-formation regarding the material properties of the cerebral ves-sels are lacking, Viano (159) reported that the Youngs modulusof the human aorta ranged from 360 kPa to 400 kPa. This valueis significantly higher than that measured from dissected braintissues. In a recent simulation of a two-dimensional brain modelwith explicit modeling of cerebral vessels, Bae et al. (14) reportedthat the maximum principal stress was higher with the inclusionof the vasculature in the brain. Both studies indicate that thecerebral blood vessels contribute to the overall stiffness of thebrain tissue in vivo, particularly when the vessels are closelyattached to brain tissue and anchored or tethered to structuresoutside of the brain.The shear moduli used to model the brain were assumed to
be approximately one order of magnitude higher than thosereported by Arbogast et al. (11) to compensate for the effect ofvascular structures. The values used for brain materials wereapproximately one third of those defined in previous versions(7, 172, 173). They are the lowest that can be used withoutcausing permanent deformation to the brain structure andwere selected to match the experimental results.Table 2 gives the Youngs modulus of 31.5 MPa and other
properties for the fax cerebri and tentorium membranes. Thevalues used for the membranes were in the range found in theliterature (41, 89, 93). An elastic-plastic material model wasused for cortical and cancellous bones of the face. Damageelements available in the PAM-CRASH material model wereintroduced to predict bony fracture. The element eliminationoption was used. This option removes any element with astrain that exceeds a preset ultimate strain magnitude in eachtime step. A Youngs modulus of 560 MPa was assumed forthe cancellous bone of the face. The value used for cancellousbone was in the range found in the literature (mandibularcondyle: 431 MPa [46], Mandible body: 273 MPa [23], vertebralbody: 316 MPa [63], proximal femur: 441 MPa [82], and prox-imal tibia: 635 MPa [32]) and [97].
A Youngs modulus of 13 GPa was reported for the humanmandible (23). When using a Youngs modulus of over 10 GPa,the model responses were very stiff. One possible reason isthat the highly porous characteristic of the human facial bonystructure was not explicitly implemented in the current model.As such, the stiffness of the cortical bone was adjusted andassumed to be approximately 50% (Youngs modulus of 6GPa) lower than those reported in literature or those usedpreviously that did provide a realistic deflection (7, 172, 175).An ultimate strain and stress of 1.6% and 4.5 MPa wereassumed for the cortical bone of the face, respectively (46). Anultimate strain of 4.5% and an ultimate stress of 4.9 MPa weredefined for cancellous bone (169).Nasal cartilage (hyaline cartilage) was defined as an elastic
material under dynamic loading, even though it has been char-acterized as a biphasic viscoelastic material by Mow and Hayes(98). Its Youngs modulus was assumed to be 30 Mpa, and itsPoissons ratio was taken to be 0.45 (58, 98, 99). The facial skinand underlying superficial muscle were assumed to be elastic,with an assumed Youngs modulus of 1 MPa. The stress-strainrelation was derived based on data reported by Yamada (169),Melvin and Evans (92), and McElhaney et al. (89). Material prop-erties of the remaining components of the WSUHIM used in thisstudy were consistent with those of previous studies.Table 3 gives the facial material properties. Facial bone re-
sembles a sandwich structure containing cancellous and cor-tical layers except in the nasal bone where the cancellous layeris not well developed. The cortical layer of the bone in the faceother than the mandible is thinner than the inner and outertables of the cranium. The thin layer of the facial bone wasmodeled with 1-mm-thick shell elements, whereas the cancel-lous bone was modeled with solid elements of varying thick-ness. The maxillary sinuses and ethmoid cells were modeled.The nasal cartilages form the external and internal framework
of the nose. The modeled cartilages included septal, lateral, andalar cartilage of the nose and were connected and attached to theadjacent facial bones. During impact, soft tissues such as muscle,skin, and fatty tissue of the face serve primarily to distributeapplied loads over the irregularly shaped bony structure. Thesoft tissues weremodeled as solid elements covering the face andwere directly attached to the outer surface of the facial bones.
TABLE 2. Elastic material properties of the heada
Elastic materialDensityg/cc
Poissonsratio
Modulus (GPa) stiffnessN/mm
Falx, tentorium 1.13 0.45 E 0.0315b
CSFa 1.04 G 1.0E-06c
Ventricle 1.04 K 2.19d
Bridging Vein 1.13 0.48 0.219
a CSF, cerebral spinal fluid.b E: Youngs modulus.c G: shear modulus.d K: Bulk modulus.
TABLE 3. Elastic material properties for the face
MaterialDensityg/cc
Elastic modulusMpa
Poissonsratio
Cortical 2.10 6000 0.25
Cancellous 1.00 560 0.30
Cartilage 1.50 30 0.45
Soft Tissue 1.10 1.0 0.45
Ligament 1.00 32 0.40
VIANO ET AL.
896 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
Their thickness varied from 3.0 mm at the nose to 8.0 mm at thezygoma, 8.75 mm at the maxilla, and 10 mm at the mandibularregions. The temporomandibular articulation (jaw joint) was alsoincluded and stabilized by ligaments. The facial masses, skin,and tissues move with the cranium because of the imposedacceleration in these simulations.
Model Validation with Experimental Data
Nahum intracranial pressure data
Cadaver head impact tests were used to validate intracranialand ventricular pressures in the FE brain model. Nahum et al.(102) conducted forehead impacts at 4.4 to 13.0 m/s using flat,rigid 5 to 6 kg mass covered with padding. Pressure transducerswere placed in five regions of the brain to measure intracranialpressure changes during impact in the frontal region adjacent tothe impact area, posterior and inferior to the coronal and squa-mosal suture, parietal areas inferior to the lambdoidal suture onboth sides, and the posterior fossae in the occipital area. Thepadding material was not defined, so padding stiffness wasadjusted until the difference in coup pressure was within 10%of the experiment. This resulted in an elastic modulus of 49 MPa.Predicted coup and contrecoup pressures correlated in time his-tory and peak for five of the six tests, indicating amodel responsegenerally within 15% (170).
Trosseille intracranial pressure data
The FE model was also subjected to intracranial and ventric-ular pressure validation using data reported by Trosseille et al.(152). In their study, cadaver head impacts were carried out at 7m/s with a 23.4 kg mass loading the facial region. A 12-accelerometer array was attached to the occipital region to mea-sure 3D head kinematics. Miniature pressure transducers wereplaced in the subarachnoid space and ventricles. Validation wascarried out for one test with complete three translational andthree rotational accelerations at the head cg, intracranial pres-sures measured in the frontal and occipital lobes, and ventricularpressures in the lateral and third ventricles. The cranium in theFE model was assumed rigid, so the head accelerations could betransferred to the brain boundary bones. The calculated pres-sures matched in time and peak values up to 14 ms (170).
Brain motion data
The validity of the FE model to simulate brain motion withrespect to the cranium was tested using cadaver head impacts.Relative motion between the cranium and the brain was deter-mined at different regions of the brain with high-speed biplanarx-rays combined with radio-opaque neutral-density targets(NDTs) embedded in the cranium and brain (57, 75). Two col-umns of five to six NDTs were implanted in the temporoparietaland occipitoparietal regions approximately 10 mm apart.The head and neck was removed at the second thoracic ver-
tebra (T2), inverted, and attached to a trolley fixture. A 152 mmdiameter impactor struck the occiput at 2 to 4 m/s, and braintarget motion was videoed by x-ray contrast at 250 frames/
second. Skull kinematics were determined using the 3 to 22 to 2accelerometer array (114) mounted on the apex of the cranium.Motion analysis was limited to the resultant displacement in a
laboratory coordinates. Some aspects of this validation are de-scribed by Al-Bsharat et al. (7). Hardy et al. (57) transformed thetarget motion onto an anatomic coordinate systemwith its originat the head cg. Skull accelerations were applied to the FE modelcg to validate it against cadaver brain motion for a 2 m/s impact.The peak resultant linear and angular accelerations were 24 gand 1,813 rad/s2, respectively. The overall brain motion in FEshowed the same figure-eight motion as in the experiment,reaching 3 to 6 mm excursion at 24 to 26 ms. The excursions ofbrain targets at different locations in the model resembled theexperimental data with some exceptions (170). Coronal and sag-ittal sections were selected from the model to map displacementcontours in other regions of the brain. The superior corner of thelateral ventricle, the caudate nucleus, the amygdala, and thehippocampus experienced displacements of 4 to 5 mm as did theanterior commissure, midbrain, and temporal lobes. The braincortex sustained displacements of 3 mm at the precentral gyrusand postcentral gyrus.Figure 4A compares the three components (x, y, and z) of
brain displacement between the FE model and experiment fortwo targets (a3 and p3). These two targets were located at thetransverse plane through the anterior commissure and pinealbody. The model predicted greater y-displacement (3 mm) butless z displacement than that measured at a3. For p3, both yand z displacements matched experimental measurements.The brain excursion trends predicted by the model resemblethose patterns observed in experiments.When brain displacements were compared for each NDT,
the FE y-displacement was lower than the experiment (3 mm),whereas the z-displacement was greater, up to 25 ms for theanterior targets 1 and 2. For anterior target 3 and 4, the modelpredicted greater y-displacement (3 mm) than that measured.For the posterior targets, the FE model predictions matchedthe experimental data at target 3 and over predicted at target2 and 4. The geometrical and structural features may affect thedegree of brain motion at certain targets location. For instance,relative motions predicted for targets a1 and p5 (targets lo-cated near the top of the brain and lateral ventricle) may beaffected by the brain-cranium interface and ventricular fluid.
Validation of Brain Motion in Higher-SpeedSagittal Impacts
Cadaver test C383-T1 was a frontal head impact generatingsagittal plane motion with a peak resultant linear acceleration of62 g and rotational acceleration of 2739 rad/s2 (57). Figure 4Bcompares the brain-cranium relative motions between modelpredictions and experimental measurements at two target (a3and p4) locations. These two targets were located at the sameposition as those for the coronal motion analysis. The displace-ments compared were in x (anterior-posterior) and z (inferior-superior) directions because the head moved mainly in the sag-ittal plane. The first 50 ms of displacements is of interest as it is
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 897
relevant to the duration of collision sustained by football players.The model displacements in z-direction were comparable withthe test data in terms of magnitude. However, x-displacementswere under predicted by the model, and the predicted directionswere opposite to the direction of x-displacement seen in experi-mentally. The inconsistency in displacement direction may be aconsequence of the difference in the cg location between thecadaver head and the FE model.When displacements are compared for eachNDT, the x-direction
relative displacements for anterior and posterior targets 1, 2, and 3
predicted by the model wereless than those observed exper-imentally. On the other hand,displacements for both anteriorand posterior targets 4, 5, and 6predicted by model were com-parable with the experimentalvalues. The average maximumbrain excursion was approxi-mately 3 mm predicted by themodel and 5 mm obtainedexperimentally.
Parametric Study ofBrain Responses
Whereas pressure re-sponses validated well, thecorrelation between model-predicted relative displace-ments and experimentalmeasurements was less satis-factory at some NDT loca-tions. Several factors maycontribute to the variations.First, the geometry and ma-
terial properties used by theWSUHIM might be differentfrom those cadaver headstested. Therefore, it is unreal-istic to expect an exact matchbetween experimental mea-surements and model predic-tions. Second, the model as-sumed a rigid cranium,whereas the cadaver headmay deform during impact.Third, the test setup we usedwas quite complex, and there-fore experimental artifactsmight exist. Fourth, the exper-imental methods used to de-rive material properties arecomplex and subject to manyinfluencing factors. Fifth, thevolume compliance of FE
model is assumed equal to that of water and is several orders inmagnitude great than that of the human (160). The last factoralone contributes to lower brain displacements with translationalacceleration.A series of parametric studies was conducted to confirm the
sensitivity of brain response to varying viscosity defined forthe shear relaxation modulus. Three new simulations, namely,the 0.1BModel, 0.5BModel, and 10BModel, were conducted inthis parametric study using a decay constant that was 0.1 ( 8 s-1), 0.5 (40 s-1), and 10 (800 s-1) times that used in the
FIGURE 4. A, comparison of the brain/cranium relative motion for two targets (a3 and p3) between model predictions andexperimental measurements for Test 291-T1. These two targets were located at the tranverse plane through the anteriorcommissure and pineal body. A2 and p3 were approximately 10 mm anterior and 30 mm posterior to the cg of the head,respectively. B, comparison of the brain/cranium relative motion for target a3 and p4 between model predictions andexperimental measurements for Test C383-T1. C, relative displacements in the x- and z-directions observed experimentallyand from baseline model or from the 10B Model for targets a3 and p4.
VIANO ET AL.
898 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
baseline model, respectively. Figure 4C shows the relativedisplacements in the x- and z-direction observed experimen-tally and from baseline model or from the 10BModel fortargets a3 and p4. The results show that both the peak relativedisplacement and time predicted by the 10BModel increasedas compared with the original model. As a result of thisincrease, model predictions correlated better with experimen-tal data (z-components at a3 and p4). A decay constant that is10 times that of the original value increased the peak relativedisplacement by as much as 40% at all target locations. Resultsbased on this cadaver appear to indicate that the magnitude ofthe decay constant has an effect on brain deformations andshould be measured experimentally in the future to identifyan appropriate value for use in modeling long-duration headimpacts. Although it may be advisable to use decay constantof 600 to 1000 seconds-1 for the simulation of brain displace-ments for long-duration impacts, this study uses the com-monly used value of 80 seconds-1. This appears to give a goodbalance in the validity of brain displacements, deformation,and pressure for the loading conditions in the helmet impacts.
Head Accelerations from NFL Game Reconstructions ofConcussion Impacts
Details of the game film selection and analysis of concussiveimpacts can be found in Pellman et al. (122, 123). For thisstudy, a short overview of the laboratory methods is provided.When an MTBI occurred on the field, it was reported toBiokinetics and Associates Ltd. (Ottawa, Ontario, K1H 1E1,Canada), the engineering group contracted to analyze andreconstruct game impacts. Network tape of games was ob-tained from the NFL and subsequently analyzed. In additionto concussion impacts, cases of significant head impact werealso selected for analysis. During 1996 to 2001, 182 cases wereobtained on video for analysis. The initial analysis determinedthe impact location on the helmet and contact (helmet,ground, shoulder, etc.). Sixty-one percent of the collisionsinvolved helmet-to-helmet impacts (122).Biokinetics determined the feasibility of determining the 3D
impact velocity, orientation, and helmet kinematics. At least twoclear views were necessary to make this analysis. For those caseswhere the 3D impact velocity could be analyzed, a laboratorysetup with crash dummies was made to re-enact the game col-lision. Helmets were placed on the dummies in the laboratoryreconstructions, and the velocity and orientation of impact wassimulated along with the subsequent helmet kinematics. A num-ber of significant impacts were also reconstructed where MTBIdid not occur to study nonconcussion impacts. In total, 28 NFLhelmet-to-helmet collisions were reconstructed, 22 involved con-cussion of the struck player, and 6 no injury.
Laboratory Reconstruction Techniques
The laboratory reconstruction involved two Hybrid III maledummies. A helmeted head-neck assembly representing thestruck player was attached to a 7.1 kg mass simulating the struckplayers torso and guided in freefall from a height to match the
impact velocity determined from video analysis of the gamecollision. Impact was against another helmeted head-neck assem-bly attached to the torso and pelvis of the Hybrid III dummy.This dummy was suspended by flexible cables.Acceleration was measured in both dummy heads. The cg of
the head is a reference point, which is defined by its position inthree orthogonal axes. The motion of the head cg is defined bythree orthogonal components of velocity and acceleration. Theacceleration is translational even though the trajectory is curvi-linear. Because the head cg moves in space under translationalacceleration, it can also rotate about the head cg. This involvesrotational acceleration, and there are three orthogonal axes forrotational acceleration and velocity. When the head is assumedrigid, as in the dummy, the three axes of translational and rota-tional acceleration define themotion sequence of the head duringimpact. The sign convention had positive z-axis from the neckupward through the top of the head (138). The positive x-axis isforward, and the positive y-axis is through the left ear.Each headform was equipped with standard accelerometers
at the head cg and nine linear accelerometers set up in aso-called 3 to 22 to 2 configuration to determine rotationalacceleration by the method of Padgaonkar et al. (114). Theanalysis is valid for accelerometers coincident with the originof head cg or coincident with one of the axes. Deviations fromthis were required in the headform configuration used in thesetests, and a correction for centripetal and Coriolis accelerationwas made according to DiMasi (30, 31).High-speed video recorded head kinematics in the reconstruc-
tion. The camera was positioned identical to one of the viewsfrom the game video. This allowed a one-to-one comparison ofthe game and reconstruction kinematics and facilitated fine ad-justments in the impact orientation and alignment of the labora-tory impact to closely match the helmet kinematics in the game.An extensive analysis was conducted to isolate and quantifysources of variability in the reconstructions (105). This workshowed the reconstructions to be repeatable and with minimalerror for this type of testing. Every effort was made to reducepotential errors in the laboratory reconstructions.
FE Model Simulations
The three translational and three rotational accelerations at the cgof the head were used as input into the WSUHIM to simulate thegame impact. By defining the cranium as a rigid body, the FEcranium is moved in the same way as the Hybrid III in the labora-tory reconstruction. The primary duration ofNFL impactswas 15 to20ms, and thedurationof the simulationwas 30ms to capture braindisplacements and deformation. Twenty-eight cases of struck play-ers were analyzed in this study including helmet-facemask, helmet-helmet, and helmet-ground impacts. Biomechanical responses inthe brain included intracranial pressure,maximumshear stress, firstprincipal strain, and first principal strain rate to assess the associa-tion between FE model responses and injury, signs, and symptomsand other on-field outcomes.
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 899
Grouping of Game Impacts and FE Simulations
The reconstructed game collisions were grouped in fourtypes (AD) depending on the orientation of the helmet con-tact. With eyes forward being the 0 reference, four quadrantsfrom front to back of the helmet were defined with left sideimpacts reflected to the right side. The categories included A:0 to 45, B: 45 to 90, C: 90 to 135, and D: 135 to 180.Details of this classification and grouping of head accelera-tions can be found in Pellman et al. (122).
Correlation with Concussion Signs and Symptoms
The individual brain responses for the reconstructed cases ofconcussion were used to compare the sites of high-strain re-sponse, with the clinical signs and symptoms occurring in theplayers as reported by the team physicians. Although some ofthe 32 signs and symptoms cannot be localized to sites in thebrain, a number may arise from specific brain regions. Hotspots were identified as regions of the brain with high relativestrain responses in comparison with surrounding areas. Theywere visualized as colored regions in the FE simulation at vari-ous times in the strain and strain-rate response of the brain.Because of consistency in the simulated brain responses, hotspots in various regions of the brain were shown during theearly response, which coincided with the peak in translationalacceleration. The mid and late responses occurred after the pri-mary impact acceleration during the rapid displacement of thecranium. The mid and late responses were combined for thisanalysis because the sites and level of strain and strain-rate werefound to be similar. This provides two brain deformations (strainand strain-rate) at two times (early and mid-late). The initialinterest was to also report on the product of strain and strain-rate; but the FE code does not have that as a standard output, soit could not be systematically determined from the simulation.
Head Injury Tolerances
Head accelerations were used to determine the SI and HIC headinjury criteria (137). In addition, the peak rotational acceleration androtational velocity was used to assess injury risks. Details of theseparameters can be found in Pellman et al. (122, 123).
Statistical Analyses of Concussion
The significance of differences in responses for the struckplayer with concussion or no injury was determined using thestandard t test with two-tail distribution. Before this analysis,Levenes test for variance was run to determine whether the ttest could assume equal variance for a comparison (62). Forthose cases with P 0.05 in the Levenes test, the t testassumed unequal variance. The t test was performed using thestandard analysis package in Excel. The regression analysiswas also used from Excel, which determined the average and95% confidence interval for a linear fit between response data.
RESULTS
Head and Brain Responses: Example Case 124
Case 124 from the NFL game reconstructions is presented toillustrate head and brain responses in the helmet impacts. Figure 5shows the headdynamicsmeasured in theHybrid III dummy. Plotson the left show the translational response and those on the right,the rotational response. The primary impact causes a rise in trans-lational acceleration to a peak in 8 ms, and the impact is essentiallyover by 15 ms. This causes a delta V of 6.2 m/s and 42 mmdisplacement of the head cg at 15ms. The initial rotation is about thez-axis and then it shifts to the y and x direction, causing a resultantrotational velocity of 26 r/s and rotation of 110 at 15ms. Between 15and 25ms, head displacement increases to 115mmand the rotationto 240. These responses are secondary to the momentum exchangein the impact, but the craniummotion continues to deform the brainbecause of the rapid motion.Figure 6 shows the distortion of the brain at 15 ms and 25 ms.
The impact displaces and rotates the cranium, producing curva-ture in the midline between the hemispheres at 15 ms. Thisfocuses deformation in the midbrain at 25 ms, with substantialdistortion of brain tissues. The displacement time histories showthe lag in brain motion at the midbrain (center), particularly inthe y-displacement, which approaches 6 mm at 25 ms. The dis-placements under the impact point (impact) and along the axis ofloading (remote) show earlier and lower responses.Figure 7 shows hot spots of strain and strain-rate at three times
in the impact. The early pattern occurs at 8 ms during peak headacceleration while strain is gradually increasing in magnitude. Thehot spots are in the temporal lobe adjacent to the impact site in thisoblique lateral collision. The mid response is at 18 ms and occursafter the primary impact. It shows a shift in hot spots to thetemporal lobe in the far side of the brain. By the late response at 22ms, the hot spots have moved to the midbrain regions includingthe fornix and Ammon. Nine of the 22 concussions showed thisspecific migration of strain from the near to far temporal lobes andthen to the midbrain. When condition D was excluded, it occurredin approximately half of the cases. All 22 concussions showed thelater strain hot spots in the regions of the fornix, midbrain, andcorpus callosum.
Correlation of Concussion with Head andBrain Responses
Table 4 shows the significant correlations between the occur-rence of concussion and Hybrid III head and FE brain responses.Only correlationswith P 0.10 are given from themany possibleanalyses conducted with the 28 laboratory reconstructions andFE modeling of the brain responses of struck players. The fulldata is given in the Appendix. The strongest correlation of con-cussion was with HIC and SI, which are measures of head injuryseverity from the Hybrid III dummy. There was also significantcorrelation with head delta V and peak translational and rota-tional acceleration, but the P values were lower in significance.For the FE simulations, mid-late strain and strain-rate in themidbrain and fornix showed the strongest correlation with the
VIANO ET AL.
900 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
occurrence of concussion of all regions of the brain. This wasconsistent with the hot spots moving to the midbrain regionlater in the brain response, as shown in the example case. Theaverage mid-late strains are in the range of 0.35 to 0.45 with
concussion and they are statistically lower without injury. Theaverage strain-rates are in the range of 60 to 80 1/s with concus-sion and are statistically lower without injury. These correlationsindicate that concussion is related to brain deformations occur-
FIGURE 5. Hybrid III head dynamics for Case 124, including 3D trans-lational and rotational acceleration of the cranium. The x, y, and z compo-
nents of the response and resultant are given. Integration gives the compo-nent translational and rotational velocities and displacements of the head.
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 901
ring after the primary head impact and momentum transfer. Thisphase of the response involves rapid displacement and rotation ofthe head once the delta V and rotational velocity have occurred.
Correlation of Signs, Symptoms and Outcomes withHead and Brain Responses
Table 5 shows the significant correlations between specificsigns, symptoms, and outcomes of concussion and Hybrid IIIand FE brain responses. Again, only correlations with P 0.10are shown from the many possible analyses conducted. Therewere only 11 significant correlations. Interestingly, none of theHybrid III responses correlated with specific signs, symptoms,
or outcomes. Return to play is a measure of theseverity of concussion in terms of signs and symp-toms affecting memory, cognition, and somaticfunction (119). Mid-late strains of 30% in the fornixcorrelated with not returning to play. Mid-latestrain-rate of 78 1/s in the corpus callosum alsocorrelated with removal from play.Memory and cognition problems correlated
with mid-late strains of 30 to 50% in the fornix andmidbrain and strain-rates over 90 1/s in the mid-brain. Loss of consciousness occurred in only fourconcussed players but correlated with mid-latestrain-rates over 100 1/s in the midbrain. Dizzi-ness was common after concussion. It correlatedwith early strains of 14 to 18% in the orbital frontalcortex and temporal lobe.
Correlation of Direction of Helmet Impactwith Head and Brain Responses
Table 6 shows the significant correlations betweenthe direction of helmet impact and early and mid-late FE brain and Hybrid III responses. Only corre-lations with P 0.10 are shown. There were only 10significant correlations. Six of the differences werebetween direction B and C with primarily mid-latestrain and strain-rate in regions of the midbrain.There was a significant difference in rotational ve-locity. Three difference were found between direc-tion D and the others in HIC and delta V, which areconsistent with direction D being falls to the groundwith loading of the back of the helmet versus direc-tions AC being essentially helmet-to-helmet im-pacts either oblique on the face mask (A) or lateralon the helmet shell (B and C).
DISCUSSION
FE Strain Hot Spots Versus the Signs,Symptoms, and Outcome of Concussion
This study is unique. It is the first of its kind tocorrelate the physical forces occurring in concussion
(biomechanics) with the clinical characteristics (neurobiology) ofactual injured players. How the physical forces acting uponspecific brain regions are manifested as clinical signs and symp-toms is unknown, but deformation of brain tissue is the under-lying biomechanical cause for neurobiological affects on func-tion. It can be postulated that the strain or strain-rates measuredby the FE model can cause purely physiological dysfunction,including biochemical changes, without anatomic correlates,submicroscopic anatomic injury, microscopic anatomic lesions,or gross anatomic lesions in the affected brain regions.Clinical symptoms or signs can arise from the injury to the af-
fected brain areas by many possible means. The affected brainregion may be responsible for a certain brain function, and this
FIGURE 6. Deformation pattern of the FE brain elements from a superior view of thehemispheres at 15 and 25 ms for Case 124, along with brain displacements along the axisof impact adjacent to the contact (impact), central, and remote (contrecoup).
VIANO ET AL.
902 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
FIGURE 7. Strain, strain-rate, and product of strain and strain-rate hotspots early (8 ms) during the head acceleration, and mid (18 ms) to late (22 ms)during the free-motion displacement and rotation of the head. Hot spots are
areas of the brain with high levels of response relative to the surrounding tissuesof the brain. They show regions of the brain with proportionally greater defor-mation. The arrow shows the direction of impact in the early response.
CONCUSSION IN PROFESSIONAL FOOTBALL
function may be directly impaired or lost by injury to that region.The affected brain region may have an inhibitory effect upon thefunction(s) of one or many other brain structures, and the injurymay result in the over-expression of those other functions. Theaffected brain area may serve as a relay station between other brainregions, and injury may disrupt the communication between mul-tiple brain structures.When analyzing the clinical effects of brain lesions, including
in this article those purely physiological dysfunctions caused byphysical forces, it must be remembered that symptoms fromlesions of a part of the nervous system are not to be equated withthe function of that part. As Adams and Victor (2) stated, symp-toms of a lesion in a region are the product of both a loss ofcertain functions and the functional activity or over activity ofportions of the nervous system that remain intact. Although theresults of this study may aid in the understanding of MTBI andperhaps general brain functioning, one must be cautious in in-terpreting the findings.
Return to Play
The clinical severity ofMTBI was correlated with thestrain-strain rates in the FEmodel. In earlier articles, theauthors have used a functionalapproach to determining con-cussion severity (119, 120).Those studies demonstratedthat players who were out ofplay for more than 7 days hadmore MTBI signs and symp-toms than those who were outfor less than 7 days (120) andthat players who were re-moved from play but returnedlater that game hadmore signsand symptoms of MTBI thanthose who returned to thegame immediately after injury(120). Only two of the playersin this present FE analysiswere kept out of play for morethan 7 days. This was toosmall a number to allow forstatistical analysis. The abilityor inability to return to play onthe day of the injury was usedas a marker of concussion se-verity. Players who returnedto play on the day of the injury(immediately returned andrested and returned) wereconsidered to have sustained aless severe concussion thanthose who did not return toplay on the day of the injury.
This obviously includes the two players who were out for morethan 7 days.Statistical analysis of these two groups is summarized in
Table 5 and showed a correlation between high strain or strain-rates in the mid-late time frame in the fornix and the corpuscallosum and not returning to play on the day of the injurybecause of a more severe concussion. High strains in the fornixalso correlated with memory impairments. The authors pre-vious studies demonstrated that clinical memory or cognitiveimpairments were correlated with delayed return to play (119,120). This may explain why high strain in the fornix is relatedto this marker of concussion severity. The correlation withhigh strain-rates in the corpus callosum may have anotherexplanation. The corpus callosum is the largest of the whitematter brain structures that contain fibers linking the left andright cerebral hemispheres (9). Disruption of these pathwaysmight result in impairment of many brain functions and delayreturn to play after MTBI.
TABLE 4. Significant t test results P < 0.10 for the occurrence of concussion versus the hybrid IIIand finite element responses. Finite element brain responses are for strain and strain rates in regionsof the brain early or latea
Concussed(n 22)
No injury(n 6) t
t testdf
P
Mean SD Mean SD
Hybrid III responsesHICa,b 339 215 121 64 4.14 26 0.000SIa,b 422 270 154 82 4.03 25 0.000Translational acc (g) 90 32 60 24 2.18 26 0.039Delta Vb (m/s) 6.9 2.0 5.0 1.1 3.07 15 0.008Rotational acc (r/s2)a,b 6106 1984 4235 1716 2.10 26 0.046
FE modeling straina
Parahipp, uncal regionsa,b Early 0.108 0.094 0.043 0.037 2.57 22 0.017Midbrain Mid-late 0.344 0.140 0.226 0.111 1.91 26 0.067Thalamus, hypothala Mid-late 0.376 0.193 0.208 0.122 2.01 26 0.055Fornix and/or midbrain Mid-late 0.448 0.176 0.217 0.153 2.92 26 0.007Hypothalamus Mid-late 0.373 0.178 0.210 0.138 2.07 26 0.049Ammon, parahippa Mid-late 0.416 0.165 0.170 0.111 3.42 26 0.002Orbito-frontal-temporal Mid-late 0.317 0.139 0.193 0.149 1.90 26 0.069
FE modeling strain ratea
Orbito-frontal temporal Early 60.0 26.8 33.7 19.6 2.23 26 0.034Temporal Early 55.0 29.0 30.7 15.5 1.96 26 0.061Parahippa,b Early 34.5 28.2 17.0 9.3 2.46 25 0.021Midbrain Mid-late 79.3 37.4 36.3 16.3 2.72 26 0.012Thalamus Mid-late 74.4 37.6 43.8 25.7 1.86 26 0.074Fornix and/or midbrain Mid-late 81.5 39.7 45.2 25.5 2.11 26 0.044Ammon, parahippa Mid-late 70.4 29.9 43.2 21.5 2.08 26 0.048Orbito-frontal-temporal Mid-late 61.4 27.6 36.7 18.0 2.06 26 0.049
a Acc, accelerations; FE, finite element; SI, Gadd Severity Index; HIC, head injury criterion; hypothal, hypothalamus;Parahipp, parahippocampal.b Based on Levenes test for equality of variances. Sig 0.05 and unequal variance is assumed for the t test.
VIANO ET AL.
904 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
Earlier studies have shown that the corpus callosum is acommon site of axonal injury and white matter lesions after
closed head injury; and white matter lesions in the corpuscallosum are a part of the spectrum of diffuse axonal injury
TABLE 5. Significant t test results P < 0.10 for the occurrence of specific signs symptoms and outcomes from concussion versus finiteelement brain responses. Finite element brain responses are strain and strain rates in regions of the brain early or latea
n Mean SD n Mean SD t test df P
Return to play No YesFornix Strain Mid-late 16 0.318 0.125 12 0.199 0.136 2.393 26 0.024Corpus callosumb Strain rate Mid-late 16 78.1 40.5 12 54.9 24.0 1.886 25 0.071
Loss of consciousness Yes NoMidbrain Strain rate Mid-late 4 105.8 40.9 24 64.2 35.2 2.145 26 0.042
Memory problems Yes NoFornix Strain Mid-late 10 0.334 0.150 18 0.229 0.124 1.99 26 0.057Fornix and/ormidbrain
Strain Mid-late 10 0.491 0.210 18 0.347 0.170 1.97 26 0.060
Cognitive problems Yes NoMidbrain Strain rate Mid-late 6 93.8 38.6 22 63.6 36.3 1.783 26 0.086
Cranial nerve problems Yes NoOrbito-frontaltemporal
Strain Early 12 0.164 0.103 16 0.104 0.066 1.866 26 0.073
Hypothalamus Strain Mid-late 12 0.410 0.190 16 0.284 0.158 1.917 26 0.066Ammon, parahippa Strain Mid-late 12 0.443 0.189 16 0.303 0.161 2.103 26 0.045
Dizziness Yes NoOrbital-frontal cortex Strain Early 9 0.176 0.099 19 0.108 0.075 1.994 26 0.057Temporal lobe Strain Early 9 0.146 0.070 19 0.095 0.069 1.800 26 0.083
a FE, finite element; Parahipp, parahippocampal.b Based on Levenes test for equality of variances. Sig 0.05 and unequal variance is assumed for the t test.
TABLE 6. Significant t test results P < 0.10 for the direction of impact versus hybrid III dummy and finite element brain responses.Finite element brain responses are strain and strain rates in regions of the brain early or latea
n Mean SD n Mean SD t test df P
Impact directions A CMidbraina Strain rate Mid-late 11 83.6 50.0 6 48.2 22.9 1.99 15 0.064
B CRotational velocity (r/s) 9 38.9 12.8 6 25.2 12.2 2.07 13 0.058Fornix and/or midbrain Strain Mid-late 9 0.477 0.153 6 0.292 0.182 2.14 13 0.052Ammon plus parahippa Strain Mid-late 9 0.436 0.168 6 0.272 0.176 1.82 13 0.092Temporal Strain rate Early 9 64.2 24.1 6 42.2 20.5 1.84 13 0.089Midbrain Strain rate Mid-late 9 72.8 27.2 6 48.2 22.9 1.82 13 0.091Orbito-frontal-temporal Strain rate Mid-late 9 70.4 32.4 6 42.5 22.3 1.83 13 0.090
D A B CHICa 2 644 122 26 265 193 2.71 26 0.012Delta Vb 2 8.4 0.1 26 6.3 2.0 5.19 26 0.000
D B CHICa 2 644 122 15 306 228 2.02 15 0.062
a HIC, head injury criterion; Parahipp, parahippocampal.b Based on Levenes test for equality of variances. Sig 0.05 and unequal variance is assumed for the t test.
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 905
after head trauma (48, 146, 164). Such lesions are a sign ofmore severe injury. High strain rates in the mid-late timeframe in the corpus callosummay be related to the presence ofsuch white matter lesions, perhaps by direct causation. Thiscould explain the link between high strain rates in the corpuscallosum and the clinical marker of severity of MTBI.The present study demonstrated a significant correlation
between high strain or strain-rates in the mid-late time framein the midbrain, the fornix, and the corpus callosum andcognitive/memory problems, loss of consciousness, or inter-val to full functional recovery (i.e., as manifested by ability toreturn to play). All of these structures are in the deep midlinebrain regions. This suggests that protective devices that couldlower the mid-late time frame strain-strain rates in these mid-line brain regions might lessen the severity of MTBI.
Loss of Consciousness
Loss of consciousness occurs infrequently with concussionin the NFL (118). Many authors have suggested that it is aresult of upper brainstem dysfunctions (109, 139, 142, 164).The results of the present study confirm these earlier state-ments. High strain rates during the mid-late time frame in themidbrain are statistically correlated with the occurrence of lossof consciousness. This is most likely caused by dysfunction inthe ascending reticular activating system, which plays a majorrole in the maintenance of consciousness (109, 139, 142, 164).
Memory and Cognitive Problems
For the purposes of this analysis, cognitive problems includeddifficulties with immediate recall and disorientation, whereasmemory problems included retrograde or anterograde amne-sia, information processing difficulties, and altered attentionalprocesses. These probably are artificial, arbitrary distinctions.The authors therefore will discuss cognitive and memoryproblems together. Cognitive and memory functions are sub-served by complex interactions between many areas of thebrain. It is generally accepted that the functions of short-termmemory, including immediate recall, are subserved by themedial temporal lobes (hippocampus, parahippocampus) andmedial diencephalic structures (22, 56, 71, 164). It is thereforeof great interest to note that in this study there was no corre-lation between high strains and/or strain-rate in these ana-tomical structures and clinical cognitive or memory dysfunc-tions. This study did reveal a correlation between cognitiveand memory problems and high strain and/or strain-rate inthe midbrain and fornix during the mid-late timeframes. Therelationship with high strain in the fornix can be understoodbecause the fornix is one of the main outflow pathways fromthe hippocampus (69).Dysfunction in the outflow from one of the regions specif-
ically associated with short-term memory function could beexpected to result in clinical memory impairments. The corre-lation between high midbrain strain and strain-rate, and clin-ical memory and/or cognitive impairments is not so easilyexplained. One of the clinical symptoms included in this anal-
ysis was attention problems. This function is at least par-tially related to levels of arousal and alertness. Its is wellknown that the ARAS arises in the midbrain and connectswith widespread areas of the limbic lobes and cerebral hemi-spheres, and modulates consciousness, arousal and alertness(139, 164). Perhaps high strain and/or strain-rate in the mid-brain impair the functioning of the ARAS, secondarily result-ing in clinical difficulties with attention.The midbrain is interconnected by multiple pathways to the
diencephalon, the temporal lobes, the limbic lobes, and mul-tiple other areas of both cerebral hemispheres (139, 164). Highstrain or strain-rates in the midbrain could affect some or all ofthese pathways, resulting in clinically apparent dysfunction insome or all of those other brain areas. In this way, cognitive ormemory impairments of seemingly medial temporal lobe andmedial diencephalic origin could arise secondarily to mid-brain dysfunction. Another possible way to explain the corre-lation with midbrain strain and strain-rate is more biome-chanical and less neurobiological.
Cranial Nerve Problems
Symptoms and signs listed under cranial nerve problemsin this study included dizziness, blurred vision, vertigo, pho-tophobia, tinnitus, diplopia, nystagmus, abnormal pupils, andhearing loss. In the entire cohort of NFL MTBIs over a 6 yearperiod, dizziness was by far the most common of these symp-toms with blurred vision, vertigo, photophobia, tinnitus, anddiplopia occurring less frequently (118). Among the 28 caseswhich are included in this FE model analysis, dizziness oc-curred in nine cases, photophobia in four cases, and none ofthe other symptoms occurred in more than one case each.Thus, most of the cranial nerve problems in this study weredizziness.The correlation between cranial nerve problems and high
early strain-rate in the orbital frontal cortex is most likely areflection of the correlation between dizziness and high earlystrains in the orbital frontal cortex. The correlation betweencranial nerve problems and high strain in the mid-late timeframe in the hypothalamus and parahippocampal/Ammonshorn regions of the medial temporal lobes requires furtherexplanation. There are numerous connections between thelimbic lobes, including the parahippocampal gyri and Am-mons horn, the hypothalamus, and the midbrain (56, 69, 164).It is possible that high strains in the hypothalamus and limbicstructures could disrupt these pathways and result in brain-stem symptomatology. There was no correlation between cra-nial nerve symptoms and high strain or strain-rates in poste-rior fossa structures (brainstem, cerebellum). It is possible thatmany of the MTBI symptoms ascribed to the brainstem byclinical neurologists are really of cerebral origin.
Dizziness
Dizziness is a nonspecific complaint that encompasses awide variety of sensory experiences including lightheaded-ness, wooziness, faint feeling, unsteadiness, feelings of ab-
VIANO ET AL.
906 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
normal movement, rotary sensations of true vertigo, and notfeeling right in the head (164). True vertigo most likely indi-cates vestibular dysfunction of central or peripheral origin (37,164). The other dizziness symptoms noted above are notori-ously difficult to localize. All of the above sensations can beexperienced by MTBI patients.The results of the present study indicate that there is at least
some role of central nervous system dysfunction involved inthe generation of dizziness after MTBI. The correlation be-tween early strain in the orbitofrontal cortex and the temporallobe cortex and dizziness suggests that cerebral injury plays arole in the development of sensations of dizziness after MTBI.It is possible that orbitofrontal and temporal lobe injury di-rectly results in the symptoms of dizziness, but it is alsopossible that early high strain in these regions is only a markerof high strains in more diffuse areas of the brain resulting indizziness.It is of some interest to note that high strain and strain-rates
in the brainstem or cerebellar regions did not correlate withthe presence of dizziness. Many of the sensations that fallunder the rubric of dizziness (i.e., unsteadiness, sensations ofabnormal movement, true vertigo) are often considered to beindicators of brainstem-cerebellar-vestibular dysfunction. Thepresent results indicate that high strain or strain-rates in theseareas are not correlated with dizziness. This, however, doesnot rule out the possibility that the early high strains in theorbitofrontal and temporal cortices disinhibit brainstem cere-bellar regions from higher cortical control and thus result indizziness. The present study cannot address the role of innerear dysfunction in the generation of dizziness after MTBIbecause of technical difficulties in evaluating strain and strain-rates in that area with the FE model.
Biomechanics
Migration of hot spots
The FE model shows a delayed response of the brain forimpact acceleration of the cranium. An early, low strain re-sponse occurs during the primary impact. This is focused tothe regions of the brain adjacent to the impact site (coup site).Because the NFL concussion impacts are primarily oblique orlateral, the early region of hot spot strain is in the temporallobe. Hot spots during the mid-response move to the oppo-site side on the brain from the impact loading (contrecoupsite). This is the far-side temporal lobe. Late in the response,the hot spots move to the midbrain above the brainstem andnear midline.This migration of hot spots is not a wave propagation
phenomena as that would occur at much shorter durationsthan occur in the FE simulation. The migration appears to bedriven by the motion of the head secondary to the delta V andduring the rapid free-motion displacement and rotation of thecranium. To our knowledge, this type of timing for the migra-tion of strain has not been reported for concussions and offersinsights into the possible underlying mechanisms of injury
related to head kinematics and the various signs and symp-toms of MTBI in players.
Coup-Contrecoup Injury
Much has been written about coup-contrecoup injuries tothe brain. The classical definition of coup injuries are thoseadjacent to the site of head impact and have been thought tobe related to the local deformation of the cranium and braindirectly under the impact. Contrecoup injuries have oftenbeen restricted to brain contusions on the opposite side of thebrain in line with the axis of impact; however, the originaldefinition was for any brain contusions away from the directsite of impact. There have been many theories for coup andcontrecoup injury, including wave propagation, cavitation,and cranium deformation (26, 27, 49, 51, 111). The FE model-ing offers a new mechanism for contrecoup injury associatedwith rather long-duration head impacts involving helmets andpadding. This is related to the migration of relatively highstrain and strain-rate from the coup region during the primaryimpact to the contrecoup regions of the brain during the rapidmotion of the cranium after the primary impact. Clearly, de-pending on the tolerance to strain, brain injuries can occur atdifferent times in the near and far temporal lobes and mid-brain regions over the 30 ms brain response.
Injury Criteria
The correlation of Hybrid III responses with concussion andnot the specific signs, symptoms, and outcomes is particularlyinteresting. The initial analyses showed the strongest correla-tion of concussion with HIC and SI. These are the traditionalmeasures of head injury risk that have widespread use in allkinds of automotive, sport, and defense safety evaluations. Atthe time, it was comforting to see that the risk for concussionin the NFL could be accurately predicted by traditional mea-sures of translational acceleration. The measurement of rota-tional accelerations was encouraged for research purposes,even though there was an inherent relationship between trans-lational and rotational acceleration (123).Surprisingly, the Hybrid III head responses did not correlate
with any of specific signs, symptoms, and outcomes of con-cussion. There was no correlation with return to play, which isarguably a good indicator of the more severely injured play-ers. No Hybrid III measures correlated with players experi-encing memory, cognitive, or somatic problems after injury.It was interesting that strain and strain-rate responses in
specific regions of the brain and phases of the brain responsecorrelated with return to play, cognitive, and memory prob-lems (Table 5). The mid-late strain and strain-rate in the mid-brain, fornix, parahippocampus, Ammon horn, and corpuscallosum correlated with the more severe signs and symptomsof concussion. These correlations imply that FE models andtissue-level injury criteria may provide effective means ofaddressing specific concussion injuries, particularly the onesresponsible for removal from play and longer recovery times.Clearly, the prevention of memory and cognitive problems
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 907
with concussion would be an important new focus forresearch.The use of FE models and strain-related injury criteria may
offer new insights into the timing of concussion injuries andaffected locations. It is further possible that new means ofpreventing concussion can be devised if attention is given toreducing the mid-late strain and strain-rate in the midbrain.Currently, helmet designs are evaluated for the performancein reducing HIC and SI, which assess the loading during theprimary impact. Little attention has been paid to means ofreducing strain effects occurring mid-late or after the primaryimpact. The role of the neck and neck musculature may beadditional factors, particularly the change in orientation of thehead with respect to the neck and deformation of thebrainstem.Obviously, more study will be needed to develop concepts
to reduce mid-late strains in the midbrain. Improved paddingin the helmet is one means of reducing the energy transfer inthe impact and head dynamics early and mid-late or themigration of strain to the midbrain late in the response. Theremay be other means of changing the mid-late response byinterventions that work after the primary impact.
Tissue Level Injury Criteria
Previous studies have shown that the product of strain andstrain-rate is an important predictor of brain and spinal cordinjury, including contusion and loss of function (161). Theproduct of strain and strain-rate is proportional to the energyabsorbed by tissue deformation. It is a cellular level formula-tion of the Viscous criterion, which has been shown to be agood predictor of soft tissue injury to the heart, lungs, andliver, including interruption of cardiac function and ventricu-lar fibrillation (19). It is unfortunate that modern FE codes donot give the product of strain and strain-rate as a standard oroptional output from simulation. In the future, this importantmeasure of injury risk should be determined because it tracksbrain injury risks, including concussion.
Concussion and the Direction of Impact
The statistical analyses showed that mid-late strain andstrain-rate were higher in the midbrain and fornix for A (045) and B (4590) direction impacts than C (90135). Thiswas an unexpected difference. A and B impacts are frontaloblique on the facemask and helmet, whereas C in laterallyoblique from the rear. The practical implications of this find-ing are unclear. HIC and SI were similar for the B and Cimpact directions, and the mid-late strain was statisticallyhigher for the B direction. This implies a greater vulnerabilityfor midbrain strain for the same HIC or SI. Because mid-latestrain in the midbrain correlated with the more severe signs,symptoms, and outcomes of concussion, the assessment ofinjury risk may ultimately be more complicated than justevaluating HIC and SI.
Limitations
Laboratory reconstructions
Extra effort was taken to determine the validity and accu-racy of measuring the 3D impact velocity from the NFL gamevideo and rotational acceleration in the Hybrid III dummy(105). However, there is an additional limitation in how real-istically the response of the Hybrid III dummy simulates theactual players head in the helmet. Although care was taken toclosely match helmet kinematics before and after the impact,there has been no means to determine possible difference inthe head interaction with the helmet padding and face mask.This is thought to be a small source of error but one that hasnot been quantified.
FE head model volume compliance of the brain-craniumsystem
One of the possible limitations of the FE model is therepresentation of the volume compliance of the brain in thecranium. The material property of brain is close to the bulkmodulus of water and therefore incompressible. The foramenmagnum is the only opening in the cranium, which does notallow much volume compliance during impact. Physiologicalstudies have shown a bilinear compliance with an initial lowresponse rising to a stiffer level after fluid volume is added(160). However, even the stiffer level is more than two ordersin magnitude lower than the bulk modulus of water.In the initial modeling, various simulations were made with
a bulk modulus of brain tissue reduced by two orders fromthat of water to better mimic the volume compliance in situ.However, even with these reductions, the brain still behavedas an incompressible fluid. Simulations in this study used thepreviously used properties, which makes the model behave asif there was a fluid contained in a relatively closed container.This substantially reduces the brain displacement and defor-mation caused by translational acceleration, which may limitthe realism of the overall simulation.Additional runs were made with case 124 using either the
translational or rotational acceleration input to compare theresponses. Figure 8 is consistent with earlier FE studies (154)and shows that the brain response is dominated by the rota-tional acceleration because the high bulk modulus preventsappreciable displacement and strain for translationalacceleration.Because concussion was strongly correlated with measures
of translational acceleration and delta V, the appropriate mod-eling of the volume compliance of the brain-cranium systemmay lead to different hot spots. There are reasons to believethe model is reasonably representative of the human response,and there is a strong correlation between rotational and trans-lational acceleration. However, this remains unproven and anunquantified source of error, which requires additional eval-uation and study.
VIANO ET AL.
908 | VOLUME 57 | NUMBER 5 | NOVEMBER 2005 www.neurosurgery-online.com
Model material properties and geometry
There is another possible limitation with the FE model inassuring validity in the various material properties used tosimulate the brain and model the detailed geometry of thebrain. In total, 15 different tissue types were modeled and theproperties taken from the literature. However, there is quitevariability in the reported properties of various tissue, andmuch of the data involved animal studies and in vitro prep-arations after death of animals and humans. It is unclear howthese properties actually mimic the in vivo properties of hu-man brain. Some parametric analysis was conducted to ex-plore the sensitivity of the model responses to variations in thematerial properties, but an exhaustive study has not beenmade. These aspects may be important to the specific levels ofstrain and strain-rate associated with injury but would notaffect the relative comparison between the simulated cases. Itis felt that the correlations with concussion and the signs andsymptoms would not be greatly influenced and are reliable.
Skull response in helmet impacts
The cranium in the FE simulation is assumed to be rigid sothat the measured accelerations from the Hybrid III dummy inthe reconstruction can be a applied to the boundary as theinput load to the model. However, the cranium has compli-ance and can deform under load. This is not considered asignificant limitation because the helmet shell and paddingdistribute forces over a broad area of the cranium, reducingthe concentration of stress that might locally bend craniumbone. In addition, the forces in these impacts would only causesmall deformations of the cranium, which are not consideredsufficient to alter the response of the brain.
Bridging veins
The helmet impacts caused sufficient brain motion that theFE simulation of the bridging veins was not stable in somecases. This required the bridging vein calculation to be turnedoff for several runs because of excessive deformation at thebrain insertion points. Future simulation efforts need to mod-ify this aspect for improved, stable performance.
Vestibular effects
It was not possible to study deformation in the vestibularregion because the main anatomic structures of the auditorysystem are extracranial, and the cranium was assumed rigid.The vestibulocochlear nerve (VIIth cranial nerve) is a sensorynerve that is responsible for the sense of hearing and the senseof balance and body position. Clinically, problems with thevestibulocochlear nerve may result in deafness, dizziness, tin-nitus, vertigo, and vomiting. Anatomically, the VIIIth cranialnerve travels through the internal auditory meatus and entersthe brainstem at the junction of the pons and medulla lateralto the facial nerve. The auditory component of the nerveterminates in a sensory nucleus (cochlear nucleus), which islocated at the junction of the pons and medulla. The strain andstrain-rate response predicted by the model at these locationsmay alter the sensory nerve function and be responsible forthe signs and symptoms sustained by the player if the mag-nitude is sufficiently high. On the basis of the model predic-tion, the level of the strain and strain-rate induced at thejunction area was quite low as compared with those at mid-brain region.
Concussion
The NFL research used a very broad and inclusive defini-tion of concussion to capture as many possible cases as pos-sible. From 1996 to 2001, only 7% of the concussion involvedplayers out 7 days, and even these most severely affectedplayers showed a rapid recovery of function in a few days.Forty-nine percent of players were removed from play, whichrepresents another subsample of the more severely injuredplayers with concussion. Removal from play often involvedmemory, cognition, or somatic problems that lead team phy-sicians to prohibit return to player on the day of injury.
FIGURE 8. Determination of brain responses for translational, rotational,and combined head acceleration for Case 124.
CONCUSSION IN PROFESSIONAL FOOTBALL
NEUROSURGERY VOLUME 57 | NUMBER 5 | NOVEMBER 2005 | 909
Obviously, concussion is a term covering a broad spectrum ofmild brain injury. It is interesting that the Hybrid III andmid-latestrain and strain-rate in the midbrain correlated with concussion.However, it may be more interesting that no Hybrid III responsecorrelated with any specific sign, symptom, or outcome of con-cussion. It is obvious that FE model and Hybrid III correlationsdepend on the definition of concussion and the particular signsand symptoms that make it up. When return to play was con-sidered, no Hybrid III response and only two FE responsescorrelatedwith that subgroup. A larger collection of cases and FEmodeling would be needed to shed more light on this aspectbecause these results are limited by the 28 NFL cases (22 concus-sions) reconstructed.Furthermore, there may be a natural selection of athletes
that make it to the NFL because players more prone to con-cussion may have been weeded out during high school andcollege play. Brain responses shown here may represent thoseof players who are most resistant to the damaging effects ofneural deformation during head impact.
Research Methodology
This is the first time, to our knowledge, that local deforma-tions of the brain have been used to correlate with the signsand symptoms of concussion. We believe there is a limitationin not being able to validate the research methods, whichinvolved the integration of laboratory and analytical ap-proaches. Each step builds upon the previous. The steps in-volved analysis of game video to determine impact velocityand helmet kinematics, laboratory reconstructions using in-strumented Hybrid III dummies wearing helmets, and FEmodeling of brain responses using the meas
![Bryan Concussion General Audience - 2015.pptx [Read-Only] · 2015-09-03 · CONCUSSION ‐16,400,000 MTBI and Post‐Concussion Syndrome ‐ 141,000 Concussion Management ‐1,550,000](https://static.fdocuments.in/doc/165x107/5fb548e39d237d0cb0684f4f/bryan-concussion-general-audience-2015pptx-read-only-2015-09-03-concussion.jpg)