
PDC_2015_People Side of Change
47
The People Side of Change Managing Expectations Early to Eliminate Workarounds Post Occupancy Informing the transition process
-
Upload
upali-nanda -
Category
Design
-
view
103 -
download
0
Transcript of PDC_2015_People Side of Change

The People Side of Change
Managing Expectations Early to Eliminate Workarounds Post
OccupancyInforming the transition process

Jennie Evans, RN, BS, EDAC, LEEP AP, Lean Six Sigma CE
Associate Principal and Sr. Vice President
HKS Architects
Adeleh Nejati, PhD, MArch, EDAC
Architect and Design Researcher
HKS Architects
Meredith Slosberg, MBA, FACHE, CSC Lean Six Sigma Green Belt
Deployment Leader
Organizational Effectiveness
Akron Children's Hospital
Acknowledgment: Center for Advanced Design Research and EvaluationPrincipal Investigator: Upali Nanda
1. Articulate the relationship between project planning and transition planning for people.
2. Identify opportunities to deploy change engagement directives during the project planning and implementation process.
3. Identify why change engagement is necessary, and effective, in all planning and design projects, based on systematically collected data.
4. Learn about three key talking points to begin conversations about implementation in your organization.

275,000 sf patient care tower
75 bed NICU
39 room emergency department
6-OR outpatient surgery center
High risk delivery area
Continuing to deliver on the promises that were written in 1890, our campus expansion will enhance the high quality, compassionate and family-centered care that we have delivered to the communities we serve for over 120 years.


Pre-Design Design Transition Occupancy
Visioning
Emerging Trends
Current to Future State
Site Visits
Site Visits
Dept. Mock Ups
Spaghetti Diagrams
Expectation
Check Survey
Ambassadors
Pulse points
Leadership Training
Ambassadors
Trials
Post Design Mock-up
Pulse Points
Expectation
Check Survey
Akron: Integrating Design and Change Management
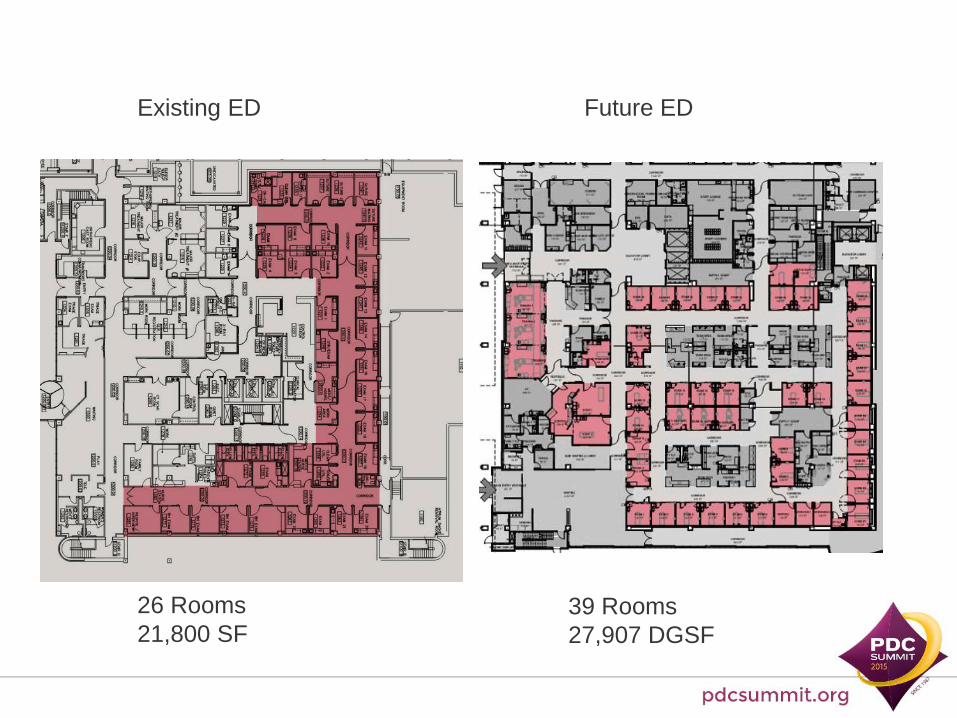
Existing ED Future ED
39 Rooms
27,907 DGSF
26 Rooms
21,800 SF

Future NICUExisting NICU
59 Beds
27,843 SF63 Private / 6 Twin = 75 Beds
68,179 DGSF

• Preparedness must consider model of care and work flow differences in
• Team Collaboration
• Visibility
• Walking distances
• Care delivery processes
• Post-occupancies identify spaces are not always used as intended
• Communication pathways are not established• Team collaboration / Devices are under utilized
• Decentralized work stations are not used• Visibility of peers
• Nurse servers are not used• Walking Distances
Recent survey of healthcare administrators cites failure to create buy-in as one of the top 2 barriers to sustainable change.
• American College of Healthcare Executives, Journal of Healthcare Management

progress
productivity(effort)
project management timeline
human response to change
goal
change management area of impact
endings exploration
new beginnings
Source: Pritchett LLC

Pre-Design Design Transition Occupancy
Visioning
Emerging Trends
Current to Future State
Site Visits
Site Visits
Dept. Mock Ups
Spaghetti Diagrams
Expectation
Check Survey
Ambassadors
Pulse points
Leadership Training
Ambassadors
Trials
Post Design Mock-up
Pulse Points
Expectation Check
Survey
Akron: Integrating Design and Change Management

Survey 1
Survey 2
June 2013
Oct 2013
May 2014
ED Timeline
Survey 3
Survey 4
Jan 2015
June 2015
1. Leader Training Starts2. Trials Start3. Town Halls4. Pulse Points Start5. Trauma Room Mock up6. Ambassadors
Design Phase Complete

1. Leader Training Starts2. Focus Groups
Survey 1
Survey 2
Design Phase Complete
June 2013
Oct 2013
June 2014
NICU Timeline
Trials Start
Survey 3
Survey 4
Nov 2015
June 2015

• Awareness
• Language and storytelling
• Messaging
• On-going dialogue
• Values and Key Behaviors
• Pulse Points

Formalize it
Overt communicate
Venues
− Daily Huddles
− Staff meetings
− Department meetings
− Governance councils
− Town halls
− Focus groups
− Email and intranet
− Ambassadors
− Surveys

NICU Focus Groups, Focused Voice
Fears
• Loneliness
• Lack of help from fellow nurses
• Increased dependence on technology
• Looking incompetent for asking for help
Leadership Advocacy
• Communication technology
• Simulation time
• Parent/family expectations
Single room line of sight and patient safety

When town halls don’t work
Prn/evenings/week-ends/tight shifts
1:10 ratio
Flash drives or intranet
Consistent regular messaging from leadership to staff and back
Regular meetings for Ambassadors


• Respiratory
• Fast Track
• Distance to Transport
• Suture Cart
• Communication devices
• Pulse Ox
• Staffing Model
• Supply carts
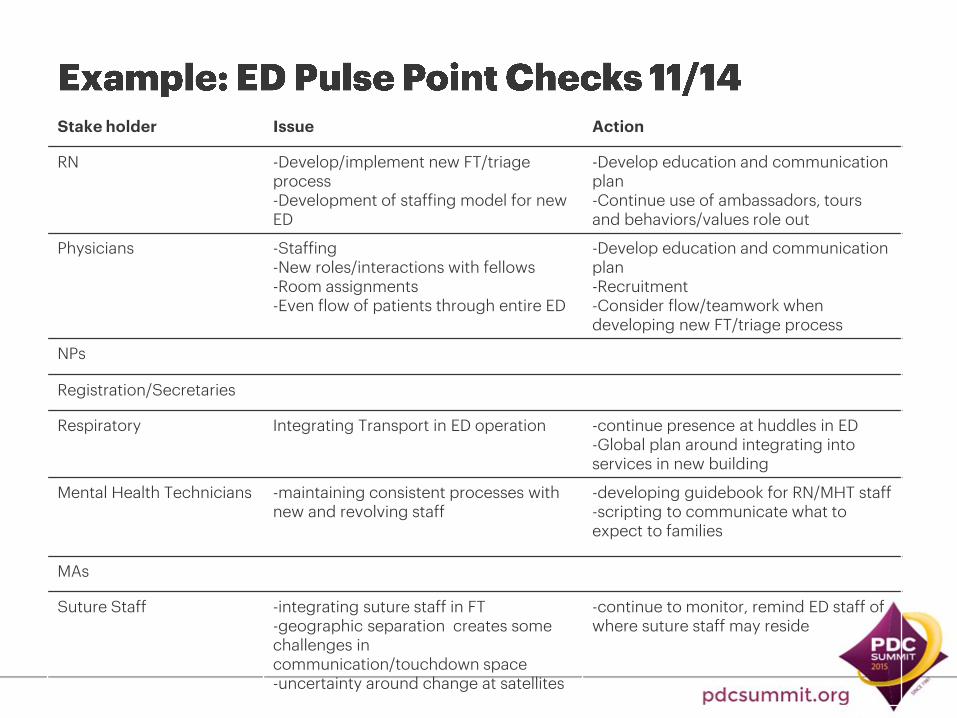
Stake holder Issue Action
RN -Develop/implement new FT/triage process-Development of staffing model for new ED
-Develop education and communicationplan-Continue use of ambassadors, tours and behaviors/values role out
Physicians -Staffing-New roles/interactions with fellows-Room assignments-Even flow of patients through entire ED
-Develop education and communicationplan-Recruitment-Consider flow/teamwork when developing new FT/triage process
NPs
Registration/Secretaries
Respiratory Integrating Transport in ED operation -continue presence at huddles in ED-Global plan around integrating into services in new building
Mental Health Technicians -maintaining consistent processes with new and revolving staff
-developing guidebook for RN/MHT staff-scripting to communicate what to expect to families
MAs
Suture Staff -integrating suture staff in FT-geographic separation creates some challenges in communication/touchdown space-uncertainty around change at satellites
-continue to monitor, remind ED staff of where suture staff may reside

To do a regular check in with the staff to assess their perceptions, expectations and level of preparedness for the move
To use the survey results to inform specific change engagement initiatives
To analyze the survey to understand how involvement in the design of the new facility, and new processes, contributes to staff preparedness and adaptation for the new move

ED 1: N= 47ED 2: N= 88
14.9
51.1
31.9
4.34.59.1
68.2
18.2
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
Leadership Medical staff Clinical staff Non-clinical staff
% o
f P
art
icip
an
ts
Job Role
ED 1 ED 2
12.8
6.4
48.9
10.68.5
2.1
10.69.111.4
42.0
9.1 8.010.2 9.1
0.0
10.0
20.0
30.0
40.0
50.0
60.0
< 6 mths < 1 yr 1-5 yrs 6-10 yrs 10-15 yrs 15-20 yrs > 20 yrs
% o
f P
art
icip
an
ts
Years of Experience
ED 1 ED 2
ED Survey Demographic
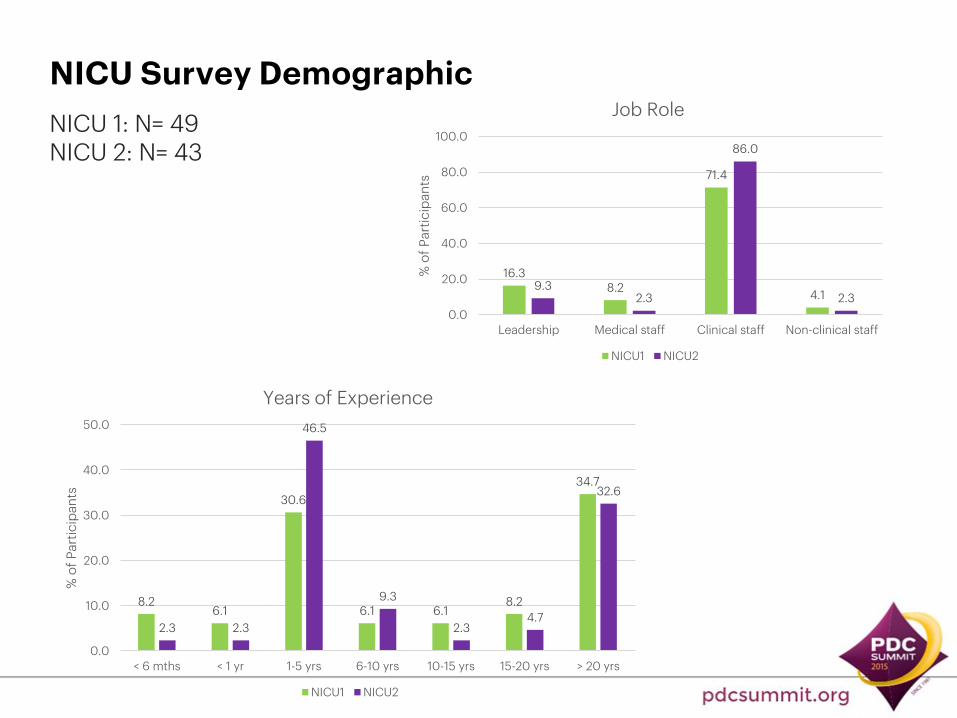
16.38.2
71.4
4.19.3
2.3
86.0
2.3
0.0
20.0
40.0
60.0
80.0
100.0
Leadership Medical staff Clinical staff Non-clinical staff
% o
f P
art
icip
an
ts
Job Role
NICU1 NICU2
8.26.1
30.6
6.1 6.18.2
34.7
2.3 2.3
46.5
9.3
2.34.7
32.6
0.0
10.0
20.0
30.0
40.0
50.0
< 6 mths < 1 yr 1-5 yrs 6-10 yrs 10-15 yrs 15-20 yrs > 20 yrs
% o
f P
art
icip
an
ts
Years of Experience
NICU1 NICU2
NICU 1: N= 49NICU 2: N= 43
NICU Survey Demographic

Level of Involvement and
Knowledge
Type of Involvement in the
Facility Design
Type of Involvement in the
Process Design
Perception of Preparedness
How prepared do you feel to work in the new environment?
Perception of Adaptation
To what extent do you feel your involvement in/ knowledge of design
will help you adapt to your new environment?
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state
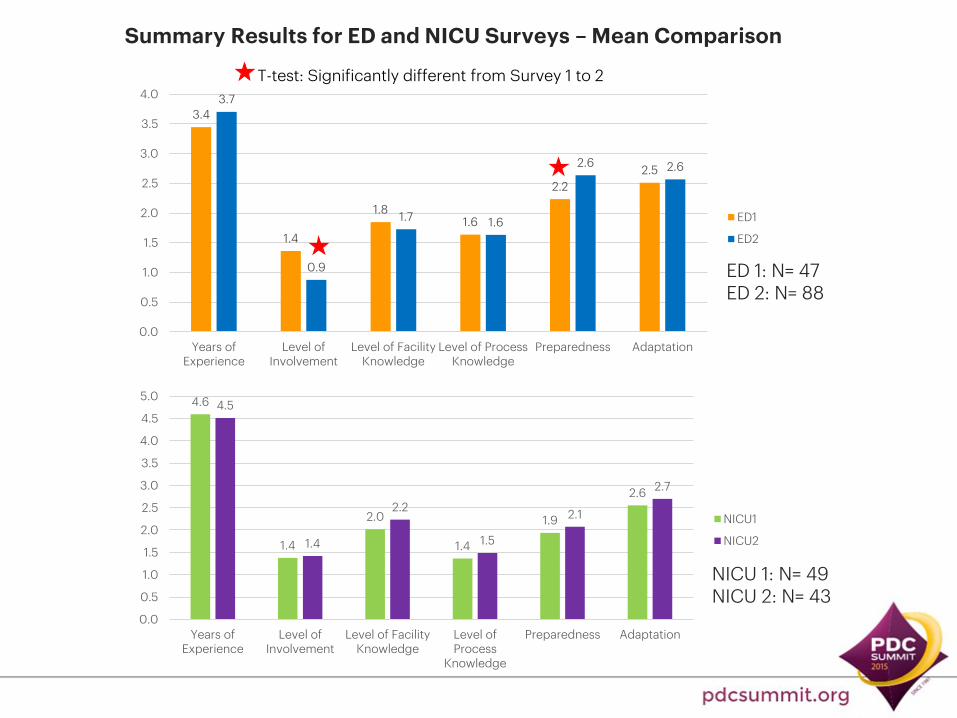
3.4
1.4
1.81.6
2.2
2.5
3.7
0.9
1.7 1.6
2.6 2.6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Years ofExperience
Level ofInvolvement
Level of FacilityKnowledge
Level of ProcessKnowledge
Preparedness Adaptation
ED1
ED2
Summary Results for ED and NICU Surveys – Mean Comparison
T-test: Significantly different from Survey 1 to 2
NICU 1: N= 49NICU 2: N= 43
ED 1: N= 47ED 2: N= 88
4.6
1.4
2.0
1.4
1.9
2.6
4.5
1.4
2.2
1.5
2.1
2.7
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Years ofExperience
Level ofInvolvement
Level of FacilityKnowledge
Level ofProcess
Knowledge
Preparedness Adaptation
NICU1
NICU2

Importance of involvement in design phase will be a recurring theme today
For ED, a range of activities informed preparedness including: 10 trials Ambassadors Leadership training Interactive mock-up of trauma room
Some leadership/staff trust issues were more pressing. Only a small core group involved. Leadership matters!

27.731.9
29.8
10.68.0
36.439.8
15.9
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Not at all A little bit Moderately so Very much so
% o
f P
art
icip
an
ts
ED1
ED2
32.7
44.9
18.4
4.1
14.0
65.1
16.3
2.3
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Not at all A little bit Moderately so Very much so
% o
f P
art
icip
an
ts
NICU1
NICU2
NICU 1: N= 49NICU 2: N= 43
ED 1: N= 47ED 2: N= 88

23.421.3
36.2
19.1
10.2
39.8
33.0
17.0
0.0
10.0
20.0
30.0
40.0
50.0
Not at all A little bit Moderately so Very much so
% o
f P
art
icip
an
ts
ED1
ED2
10.2
42.9
28.6
18.4
7.0
39.5
30.2
23.3
0.0
10.0
20.0
30.0
40.0
50.0
Not at all A little bit Moderately so Very much so
% o
f P
art
icip
an
ts
NICU1
NICU2
NICU 1: N= 49NICU 2: N= 43
ED 1: N= 47ED 2: N= 88

Level of involvement in the
facility design
Level of Knowledge of New Facility
Level of Knowledge of New Process
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state[S1, S2]
[S1]
ED Survey Result
Level of Involvement & Knowledge
[S1]
[S2]
CorrelationPredictionSurvey 1Survey 2
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state[S1, S2]
Level of Knowledge of New Facility
Level of Knowledge of New Process
Level of involvement in the
facility design
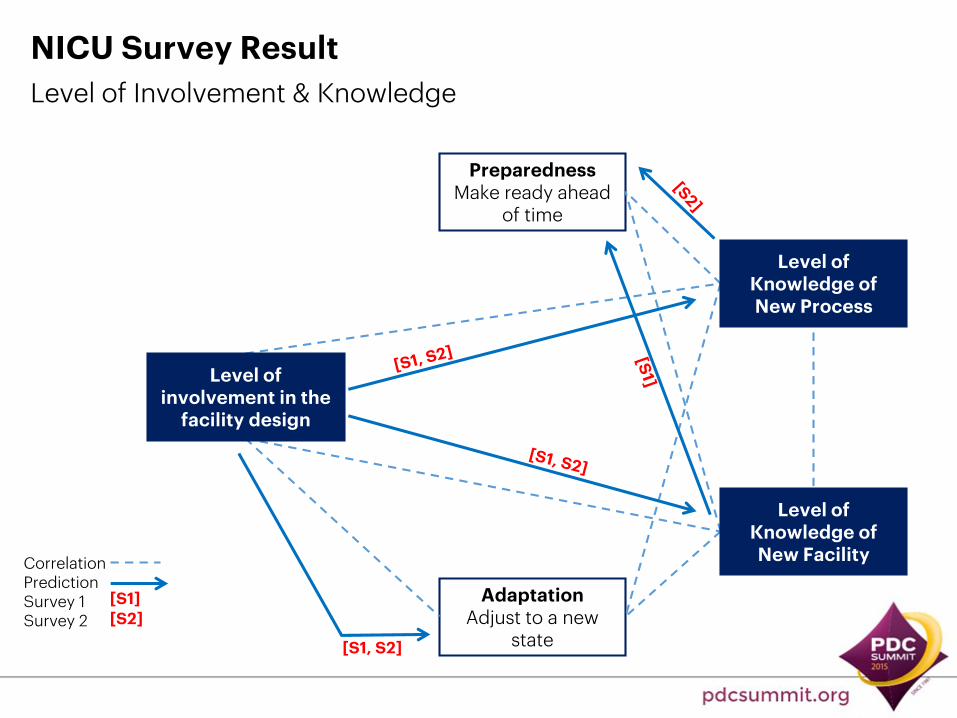
NICU Survey Result
Level of Involvement & Knowledge
[S1]
[S2]
CorrelationPredictionSurvey 1Survey 2

Level of involvement in the
facility design
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state
Level of Knowledge
Process
Facility
ED only
Summary Result
Level of Involvement & Knowledge

Being involved in facility design was key:
• To increase knowledge of process and knowledge of environment
• To increase ED’s perceptions of both preparedness and adaptation
• To increase NICU’s perception of adaptation but not preparedness
This points to how the future design configuration affectsthe current model of care. The new NICU design has a hugeimpact on current model of care. The new ED is a larger space but has less impact on the model of care. Preparedness and adaptation seem to be more closely aligned when the new model of care is similar to the old model of care.

Knowledge of facility and knowledge of process did not have the same impact on each group.
• Knowledge of process and facility increased NICU’s perception of their ability to be ready ahead of time.
• Knowledge of facility increased ED’s perception of their ability to adjust to the new space.
• Knowledge of process increased ED’s perception of their ability to be ready ahead of time.
Since our goal is to have our employees ready to utilize the space in a way that is congruent with intended use we need to pay attention to providing them with both types of information. However, one group may need a certain type of information more than the other and at different times in the transition process.

Pre-Design Design Transition Occupancy
Part of design team
Tour mock up
Patient care processes
Choosing design options
Workshop report outs
Regular communication
Part of design team
Tour mock up
Patient care processes
Choosing design options
Workshop report outs
Regular communication
Trialing new equip/ tech
Trial new equip/tech
Leadership training
Focus groups
Regular communication
Trial new equip/tech
Leadership training
Focus groups
Regular communication

13
23
96 7
27
7
20
49 11
69
0
10
20
30
40
50
60
70
80
Part of theDesign Team
Tour Mock-up Create PatientCare Processes
Choose DesignOptions
AttendWorkshopsreport outs
RegularCommunication
Nu
mb
er
of
Pa
rtic
ipa
nts
ED1
ED2
1013
10
16
8
38
5
13
7 63
39
0
10
20
30
40
50
60
70
80
Part of theDesign Team
Tour Mock-up Create PatientCare Processes
Choose DesignOptions
AttendWorkshopsreport outs
RegularCommunication
Nu
mb
er
of
Pa
rtic
ipa
nts
NICU1
NICU2
NICU 1: N= 49NICU 2: N= 43
ED 1: N= 47ED 2: N= 88

NICU 1: N= 49NICU 2: N= 43
ED 1: N= 47ED 2: N= 88
46.9
14.3
28.6
44.2
9.3
34.9
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Trial of NewEquipment &Technology
Leadership Training Focus Groups
% o
f P
arti
cip
ants
NICU1
NICU2
23.421.3
31.9
35.2
6.8
12.5
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Trial of New Equipment& Technology
Leadership Training Focus Groups
% o
f P
arti
cip
ants
ED1
ED2

Involved in trialing new equipment and technology
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state
Involved in leadership training
Involved in focus groups
Part of the design team
Toured the mock up
Involved in creating the patient care processes in the new department
Involved in choosing unit design options for the new department
Attended the workshop report outs either in person or via webex
Receive and read regular communication on your unit design
Ty
pe
of
Inv
olv
em
en
t in
F
ac
ility
De
sig
n
Ty
pe
of
Inv
olv
em
en
t in
P
roc
ess
De
sig
n
[S1]
[S1]
[S2]
PredictionSurvey 1Survey 2
ED Results

PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state
[S2]
Involved in trialing new equipment and technology
Involved in leadership training
Involved in focus groups
Part of the design team
Toured the mock up
Involved in creating the patient care processes in the new department
Involved in choosing unit design options for the new department
Attended the workshop report outs either in person or via webex
Receive and read regular communication on your unit design
[S1]
[S2]
PredictionSurvey 1Survey 2
Ty
pe
of
Inv
olv
em
en
t in
F
ac
ility
De
sig
n
Ty
pe
of
Inv
olv
em
en
t in
P
roc
ess
De
sig
n
NICU Results

Part of the design team
PreparednessMake ready ahead
of time
AdaptationAdjust to a new
state
Touring the mock up Creating the patient
care processes Attending the
workshop report outs
ED
Trialing new equip/ tech
Leadership training Focus groupsNICU
ED & NICU
Summary Result
Type of Involvement
Process design involvement is more critical when the model of care changes

Key Learnings: Type of Involvement
• Being part of design team led to both more adaptation and preparedness for ED and NICU
• ED’s involvement in design activities led to more adaptation
• NICU’s involvement in process activities led to more preparedness
We’ve said this multiple times. Being actively involved in the design phase of the project matters when it comes to being prepared and adapting to a new space.
Type of involvement produces different results. Understanding the type of involvement that leads to either adaptation or preparedness help leaders selectthe best activities for change engagement.

Summary of ED Qualitative Results
ED1 and ED2 ED1 ED2
Excited about
Newness, clean environment, more space, better patient flow and processes.
Concerned aboutProximity to main hospital, adjusting to changes, staffing issues
Lack of involvement in design, not enough computers.
Communications
Facility designers Should have
Involved more staff, considered PICU and or locations, design issues.
Management/ senior leadership should have
Involved more staff, considered PICU and or locations
Design issues
CommentsLooking forward to prepare for move, see new building, staffing.

Summary of NICU Qualitative Results
NICU1 and NICU2 NICU1 NICU2
Excited about Private rooms, clean and new environment
Windows New equipment
Concerned about Staffing, patient safety Size of unit vis-à-vis response time, not able to see babies constantly, how to get help in emergent situations, not having enough time with babies (parent satisfaction), distance between patients and supplies
Nurse safety, staff morale, proximity of staff
Facility designers Should have
Involved more staff members
Designed private rooms and pods
Made rooms smaller
Management/ senior leadership should have
Considered staffing Involved more staff Be concerned about staff concerns
Comments Familiarize with space and processes before moving, tour facility, staffing
Have concerns addressed Discuss workflow and processes, practice on new communicationsystem

Pre-Design Design Transition Occupancy
Akron: Integrating Design and Change Management
Visioning
Emerging Trends
Current to Future State
Site Visits
Site Visits
Dept. Mock Ups
Spaghetti Diagrams
Expectation
Check Survey
Ambassadors
Pulse points
Leadership Training
Ambassadors
Trials
Post Design Mock-up
Pulse Points
Expectation Check
Survey

progress
productivity
(effort)
project management timeline
human response to change
GO
LIVE
endings exploration
new beginnings
human response to change
post go-live!
Source: Pritchett 2013 and Meredith Slosberg 2014

Design Team Recommend the need for pre-
design operational planning with cross-functional teams
Choose design team members who will serve as ambassadors
- Provide job descriptions
Implement initiatives to engage staff who are not at design table
- Collect responses to specific questions
- Post images / drawings
- Communicate
- Solicit constant feedback
Healthcare Leadership Integrate Change Engagement
concepts into the design/project plans
Create early dialogue with all staff and continue through post go-live
− go to the people
− use many modalities
Establish ambassador program
− how to get many voices while maintain a small decision-making group
Establish pulse point checks and continue three to six months post occupancy

• What interventions help staff prepare and adapt and when should they be implemented?
• What kind of ripple effect do these results (with the staff) have on the patient and family?
• What role does leadership play in the staff’s willingness to adapt and be prepared?
• What design process is the most effective for preparing staff for their new environment?



















