PCYC corporate presentation 29 August 2014 RE TBdoc.xueqiu.com/148db96d21e2073fea865e21.pdf ·...
49
1 Pharmacyclics ® Corporate Presentation September 2014
-
Upload
vuongnguyet -
Category
Documents
-
view
215 -
download
0
Transcript of PCYC corporate presentation 29 August 2014 RE TBdoc.xueqiu.com/148db96d21e2073fea865e21.pdf ·...

1
Pharmacyclics®
Corporate PresentationSeptember 2014

2
During the course of this presentation we will make statements that constitute forward-looking statements. These statements may include operating expense projections, the initiation, timing and results of pending or future clinical trials, the actions or potential action of the FDA, the status and timing of ongoing research, corporate partnering activities and other factors affecting Pharmacyclics’ financial condition or operations. Such forward-looking statements are not guarantees of future performance and involve risks, uncertainties and other factors that may cause actual results, performance or achievements to vary materially from those expressed or implied in such statements. These and other risk factors are listed from time to time in reports filed with the Securities and Exchange Commission (SEC), including but not limited to, reports on Forms 10-Q and 10-K. Pharmacyclics does not intend to update any forward-looking information to reflect actual results or changes in the factors affecting the forward-looking information.
Safe Harbor Statement

3
Making a difference for the betterment of patients
Our MissionTo build a viable biopharmaceutical company that designs, develops and commercializes novel therapies intended to improve quality of life, increase duration of life and resolve serious medical healthcare needs.To identify and control promising product candidates based on exceptional scientific development and administrational expertise, develop our products in a rapid, cost-efficient manner and to pursue commercialization and/or development partners when and where appropriate.We exist to make a difference for the better and these are important times to do just that.
4
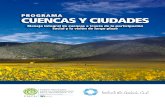
Pharmacyclics Pipeline
Molecule & Program / Indication Discovery / Preclinical
Phase I
Phase II
Phase III
IMBRUVICA (ibrutinib) : Bruton’s tyrosine kinase (BTK) inhibitor for Oncology *
Chronic Lymphocytic Leukemia
Mantle Cell Lymphoma
Diffuse Large B-cell Lymphoma
Multiple Myeloma
Follicular / Marginal Zone Lymphoma
Waldenstrom’s Macroglobulinemia
Abexinostat HCI (PCI-24781) : Histone deacetylase (HDAC) inhibitor for Oncology **
Follicular Lymphoma and Mantle Cell Lymphoma
PCI-27483 : Factor VIIa Inhibitor
Excipient, Drug Delivery
New BTK inhibitor for Autoimmune Diseases
Autoimmune Disease*Janssen Biotech: global partnership ** Servier: ex-U.S. partnership
APPROVEDAPPROVEDAPPROVEDAPPROVED

5
IMBRUVICA (ibrutinib - PCI-32765)
• IMBRUVICA is an oral therapy that targets an importantpathway in B-cell malignancies. Over 3500 patientstreated in company sponsored clinical trials.
• IMBRUVICA is approved for the treatment ofpatients with mantle cell lymphoma and chronic lymphocyticleukemia who have received at least one prior therapy and
for all CLL patients with del17p.
• IMBRUVICA has demonstrated in clinical trials:o Tumor reduction (response) in heavily pretreated patientso Responses in patients previously treated with
chemotherapy and with aggressive diseaseo Durable responses with many patients still on drug after
prolonged periods of timeo Patient tolerability demonstrated
6
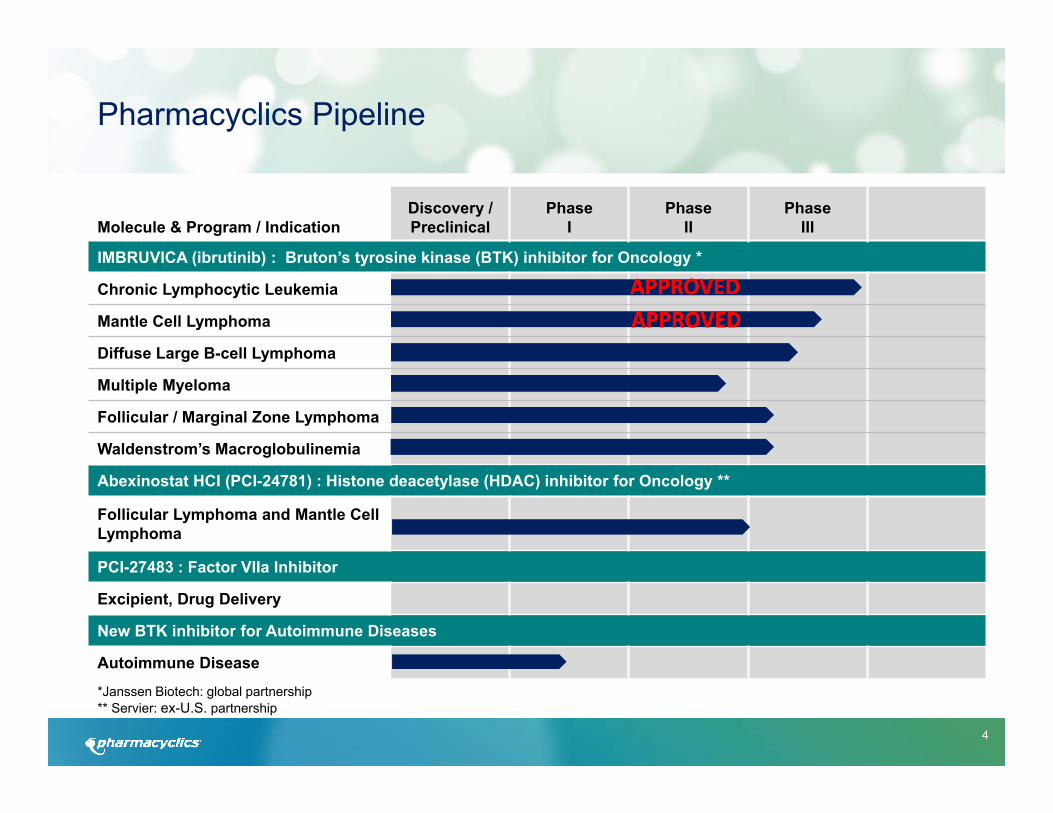
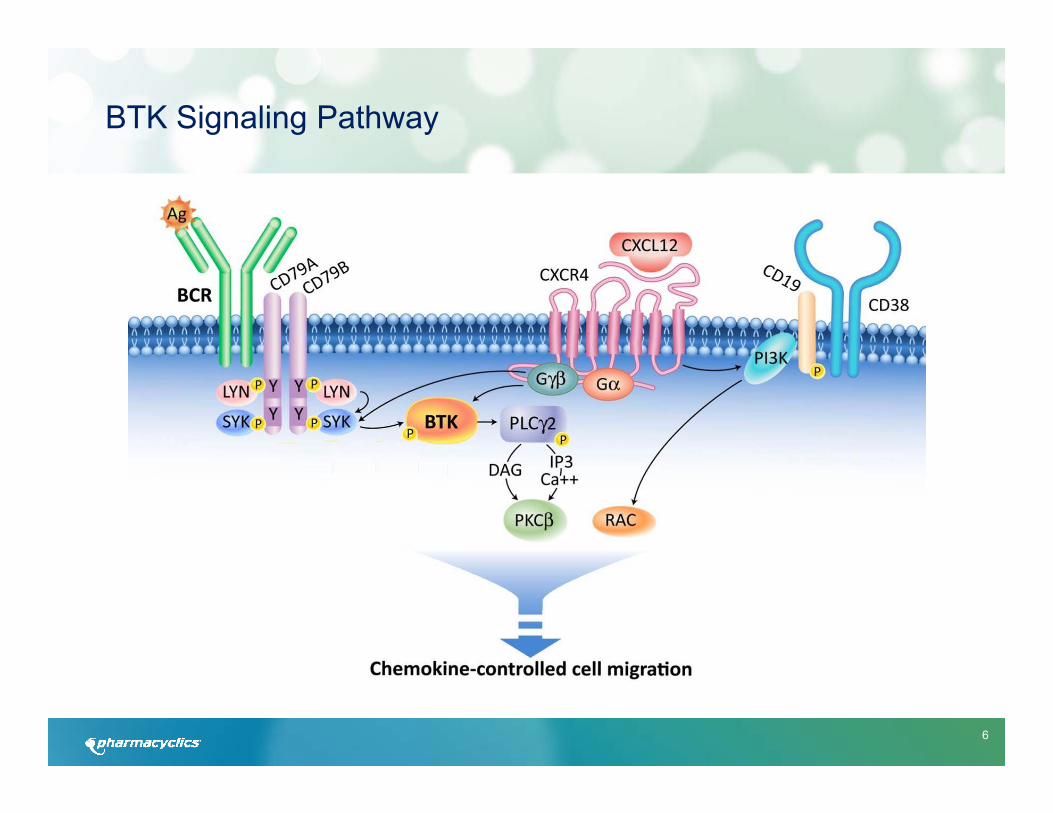
BTK Signaling Pathway

7
From: de Rooij et al, Blood 119: 2590-2594
Mechanism of BTK: IMBRUVICA (ibrutinib – PCI-32765) Blocks Malignant B-cell Growth and Proliferation
integrinBTK
ibrutinib
BCRCXCR4CXCR5CCR7
ibrutinib
ibrutinib
CLL LN PB
adhesion + migration survival + proliferation apoptosis
Chronic Lymphocytic Leukemia Cell Lymph Node Peripheral Blood
8
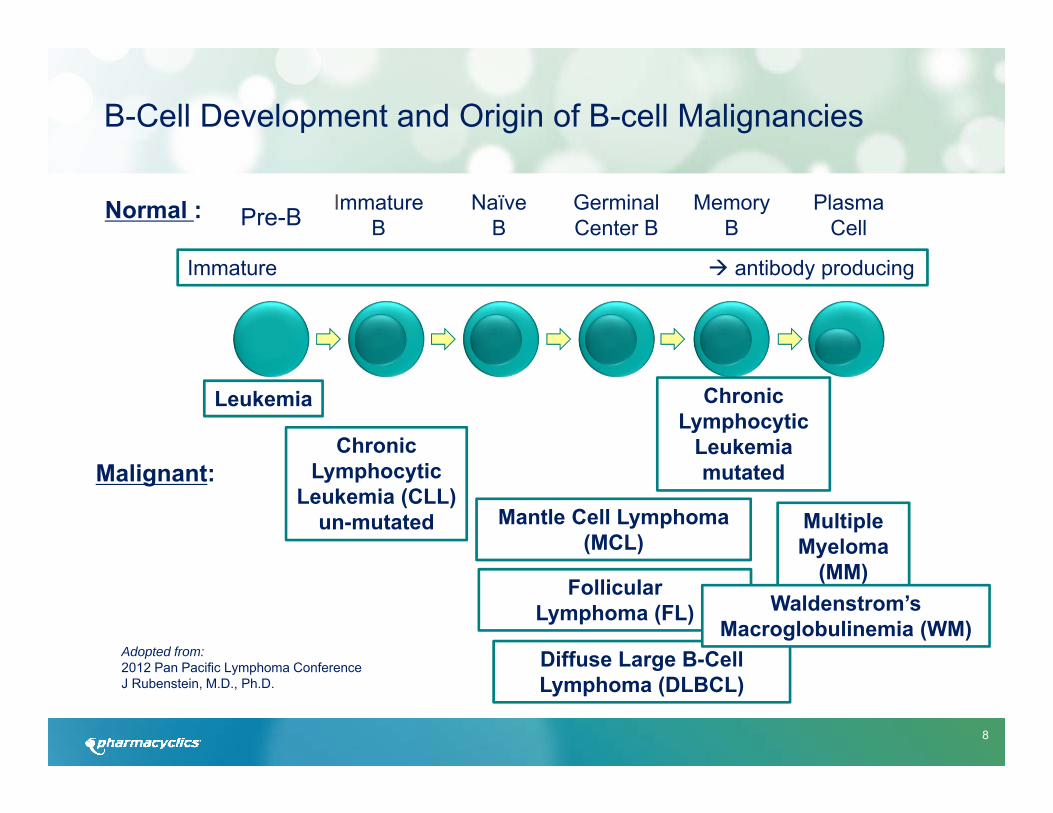
B-Cell Development and Origin of B-cell Malignancies
Pre-B ImmatureB
NaïveB
GerminalCenter B
MemoryB
PlasmaCell
Malignant:
Leukemia
Chronic Lymphocytic
Leukemia (CLL)un-mutated Mantle Cell Lymphoma
(MCL)Multiple Myeloma
(MM)
Adopted from:2012 Pan Pacific Lymphoma ConferenceJ Rubenstein, M.D., Ph.D.
Normal :
Immature antibody producing
Chronic Lymphocytic
Leukemia mutated
Follicular Lymphoma (FL)
Diffuse Large B-Cell Lymphoma (DLBCL)
Waldenstrom’sMacroglobulinemia (WM)

9
Phase III
7
2
1
1*
1*
1
0
12
IMBRUVICA Trials Across Histologies(Company / Investigator Sponsored Trials as of Q2 2014)
CLL/SLL
MCL
WM
FL
MZL
DLBCL
MM
Total Studies
16
6
1
4
1
6
2
38
Phase I/II
7159 Total Patients
Anticipated Enrollment
*FL/MZL is a joint, singular Phase III study
0Other 2

10
IMBRUVICA - Key Studies
Histology
CLL/SLL
MCL
WM
FL
MZL
DLBCL
MM
Other
Relapsed/Refractory CombinationTreatment Naive
Relapsed/Refractory
Single-Agent
11
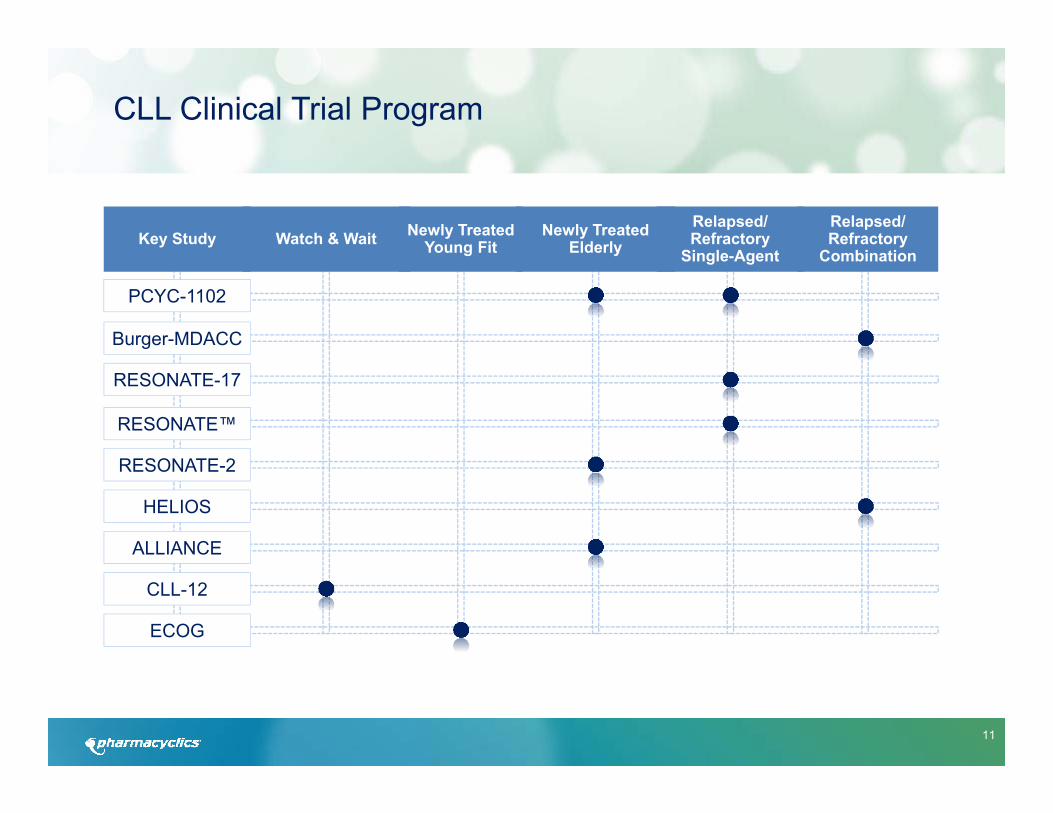
CLL Clinical Trial Program
PCYC-1102
Burger-MDACC
RESONATE-17
RESONATE™
RESONATE-2
HELIOS
Key Study
ALLIANCE
CLL-12
ECOG
Watch & Wait Newly Treated Young Fit
Newly Treated Elderly
Relapsed/ Refractory
Combination
Relapsed/ Refractory
Single-Agent

12
Targeting 8 Major Hematological Diseases Clinical Program Overview of IMBRUVICA
CLL/SLL
MCL
DLBCL
FL
MM
MZL
STUDY ID DESCRIPTION PHASE 2 PHASE 3WM PCYC‐1127 Rituximab vs. rituximab + ibrutinib
CLL3001 HELIOS (BR vs. BR + ibrutinib)
CLL3002 BRILLIANCE (ibrutinib vs. rituximab)
PCYC‐1112 RESONATETM (ibrutinib vs. ofatumumab)
PCYC‐1103 Single‐agent ibrutinib
PCYC‐1117 RESONATETM‐17 (Single‐agent ibrutinib)
PCYC‐1115 RESONATETM‐2 (ibrutinib vs. chlorambucil)
MCL3001 RAY (ibrutinib vs. temsirolimus)
MCL2001 SPARK (Single‐agent ibrutinib)
PCYC‐1104 Single‐agent ibrutinib
MCL3002 SHINE (BR vs. BR + ibrutinib)
PCYC‐1106 Single‐agent ibrutinib
PCYC‐1123 ibrutinib + lenalidomide + rituximab vs. ibrutinib + lenalidomide
PCYC‐1124 ibrutinib + lenalidomide + DA‐EPOCH‐R
DBL3001 PHOENIX (R‐CHOP vs. R‐CHOP + ibrutinib)
FLR3001 SELENE (ibrutinib + BR or R‐CHOP)
FLR2002 DAWN (Single‐agent ibrutinib)
PCYC‐1125 ibrutinib + rituximab
PCYC‐1111 Ibrutinib ± dexamethasone
PCYC‐1119 ibrutinib + carfilzomib
PCYC‐1121 Single‐agent ibrutinib
Active, Not Recruiting
Active, Not Recruiting
Active, Recruiting
Active, Not Recruiting
Active, Rollover Protocol
Active, Not Recruiting
Active, Not Recruiting
OUS Only Active, Not Recruiting
Active, Not Recruiting
Closed, Not Recruiting
Active, Recruiting
Active, Not Recruiting
Active, Recruiting
US Only ‐ Active, Recruiting
Active, Recruiting
Active, Recruiting
Active, Not Recruiting
Active, Recruiting
Active, Recruiting
Active, Recruiting
Active, Recruiting
RELAPSED OR REFRACTORY
RELAPSED OR REFRACTORY
TREATMENT NAïVE
RELAPSED OR REFRACTORY
TREATMENT NAïVE
RELAPSED OR REFRACTORY
TREATMENT NAïVE
RELAPSED OR REFRACTORY
TREATMENT NAïVE
RELAPSED OR REFRACTORY
RELAPSED OR REFRACTORY
13
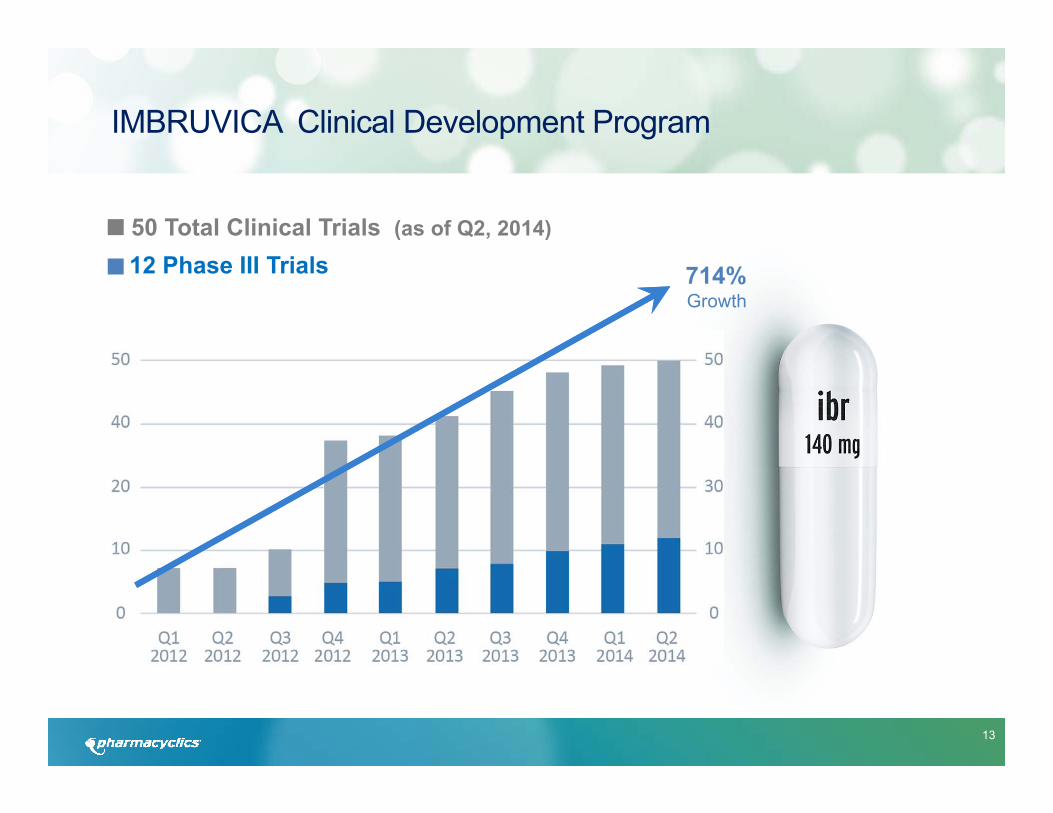
IMBRUVICA Clinical Development Program
714% Growth
50 Total Clinical Trials (as of Q2, 2014)
12 Phase III Trials

14
Clinical Development Plan: Select Studies of IMBRUVICA in CLL/SLL Patients
PCYC/JNJ/ISTs Phase Study ID Status Line of
Therapy# of
PatientsTrial 1stReleased Study Design
CLL
I PCYC‐1108 compl RR 33 Feb‐11 i+FCR; i+BR
II
PCYC‐1103 active RR 200 Jun‐10 Roll Over Study
PCYC‐1117RESONATE‐17 active RR 111 Jan‐13 Monotherapy in 17p
PCYC‐1102 compl TN/RR 133 May‐10 Monotherapy
Burger‐MDACC active RR 40 Feb‐12 i+R in high risk pts
Burger‐MDACC recruit RR 208 Dec‐13 i vs iR
III
PCYC‐1112RESONATE active RR 350 Jun‐12 i vs Ofa
(Cross‐over added 8/13/13)
PCYC‐1115RESONATE‐2 active TN 272 Jan‐13 i vs Chlorambucil in Elderly
HELIOS active RR 580 Sept‐12 i+BR
CLL3002 recruit RR 150 Oct‐13 i vs R (in China)
Woyach recruit TN 523 Jun‐13 i vs iR vs BR in Elderly
CLL‐12 recuit TN 302 ASH ’13 i vs Placebo; Watch & Wait (German Study Group)
ECOG recruit TN 519 ASH ’13 iR vs. FCR; Young Fit

15
Randomized Comparison of Ibrutinib Versus Ofatumumab in Relapsed or Refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: Results From the Phase III RESONATETM Trial (Hillmen, EHA 2014)
• A total of 195 previously treated CLL/SLL patients were assigned to receive ibrutinib monotherapy until PD or unacceptable toxicity.
• Trial was stopped due to statistically significant improvement in Progression Free Survival and Overall Survival versus Ofatumumab.
• Median time on study was 9.4 mosat interim analysis.
• Investigator Assessment of ORR was 85% for ibrutinib (2%CR, 68%PR,15%PR-L) vs. 23% for Ofa. IRC assessment of ORR was 63% for ibrutinib (43% PR, 20% PR-L) vs. 4% for Ofa.
(57 pts on Ofa arm crossed over after confirmed PD)
16
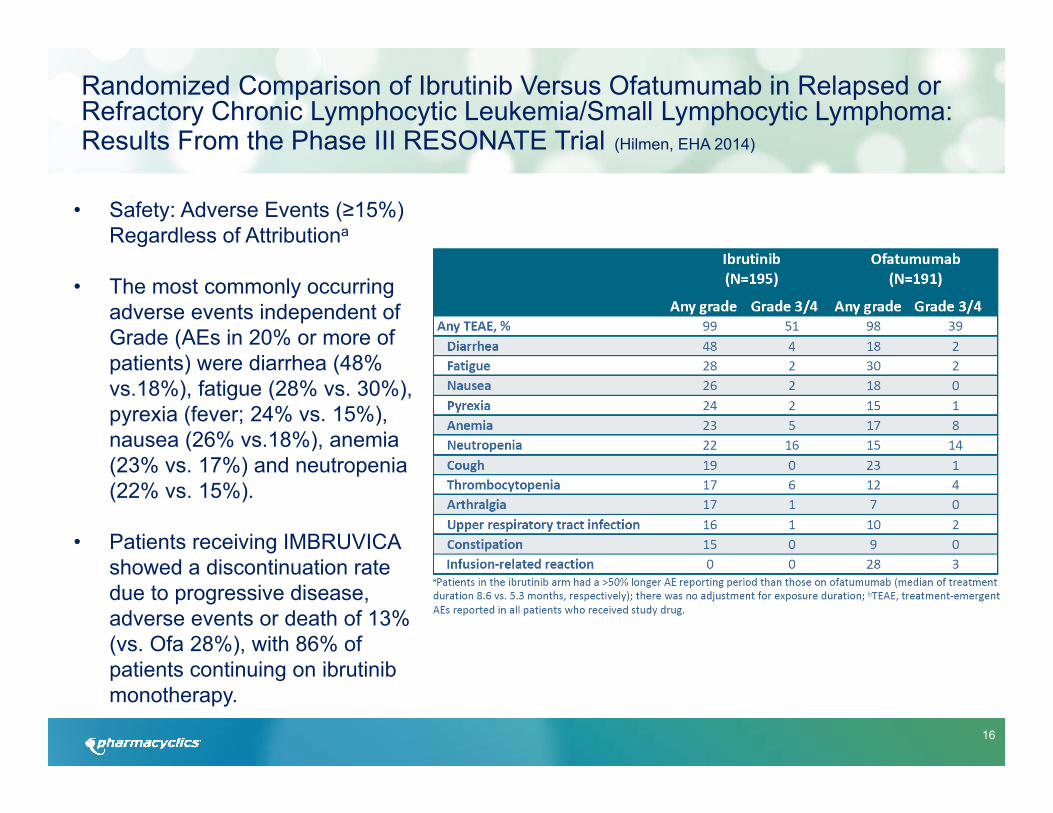
Randomized Comparison of Ibrutinib Versus Ofatumumab in Relapsed or Refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: Results From the Phase III RESONATE Trial (Hilmen, EHA 2014)
• Safety: Adverse Events (≥15%) Regardless of Attributiona
• The most commonly occurring adverse events independent of Grade (AEs in 20% or more of patients) were diarrhea (48% vs.18%), fatigue (28% vs. 30%), pyrexia (fever; 24% vs. 15%), nausea (26% vs.18%), anemia (23% vs. 17%) and neutropenia (22% vs. 15%).
• Patients receiving IMBRUVICA showed a discontinuation rate due to progressive disease, adverse events or death of 13% (vs. Ofa 28%), with 86% of patients continuing on ibrutinibmonotherapy.
17
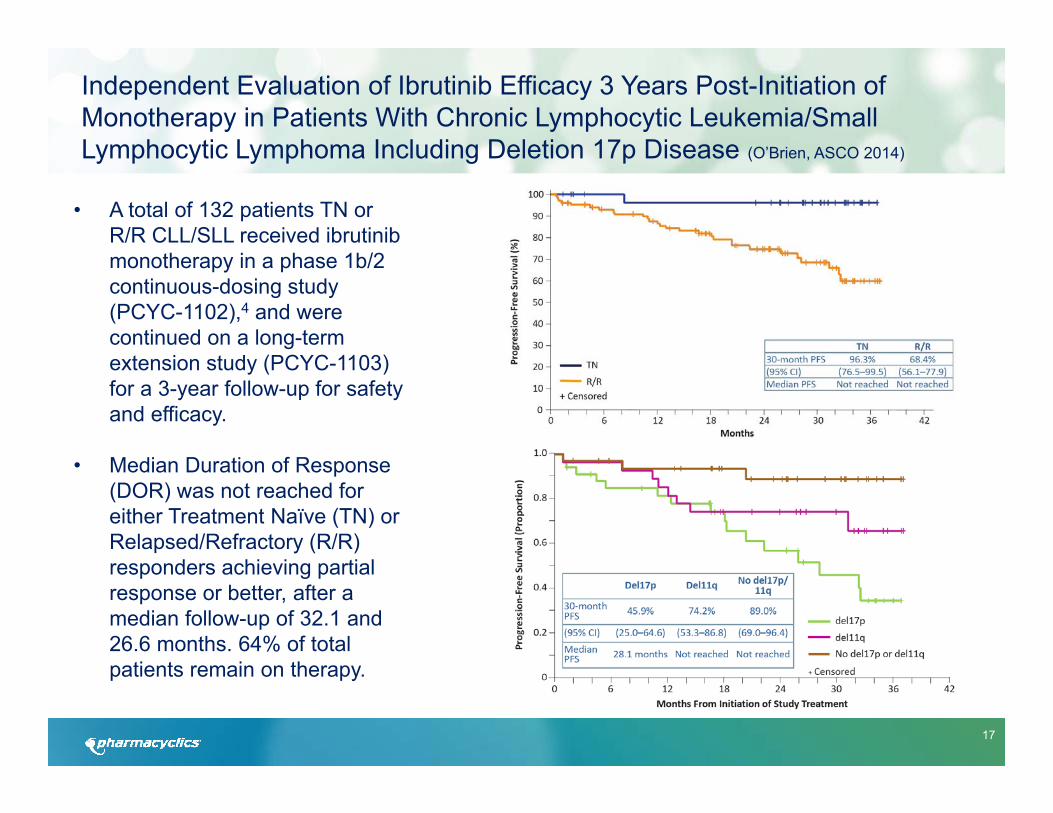
• A total of 132 patients TN or R/R CLL/SLL received ibrutinibmonotherapy in a phase 1b/2 continuous-dosing study (PCYC-1102),4 and were continued on a long-term extension study (PCYC-1103) for a 3-year follow-up for safety and efficacy.
• Median Duration of Response (DOR) was not reached for either Treatment Naïve (TN) or Relapsed/Refractory (R/R) responders achieving partial response or better, after a median follow-up of 32.1 and 26.6 months. 64% of total patients remain on therapy.
Independent Evaluation of Ibrutinib Efficacy 3 Years Post-Initiation ofMonotherapy in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Including Deletion 17p Disease (O’Brien, ASCO 2014)
18
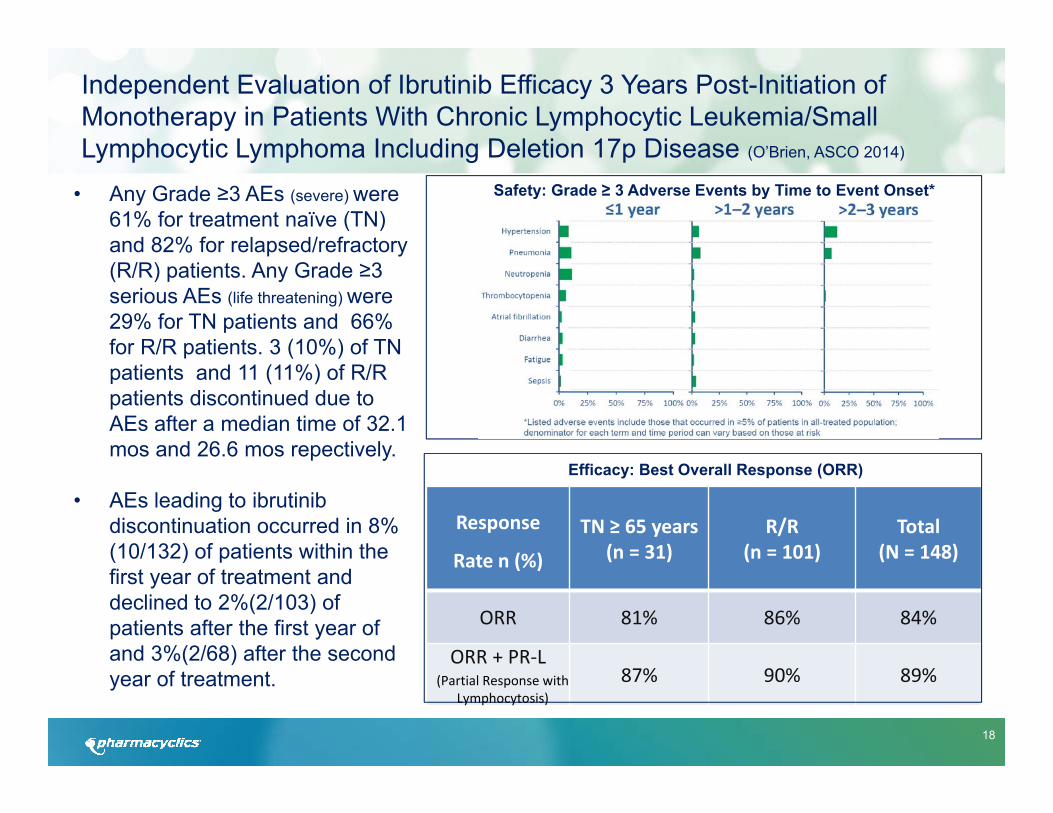
• Any Grade ≥3 AEs (severe) were61% for treatment naïve (TN) and 82% for relapsed/refractory (R/R) patients. Any Grade ≥3 serious AEs (life threatening) were 29% for TN patients and 66% for R/R patients. 3 (10%) of TN patients and 11 (11%) of R/R patients discontinued due to AEs after a median time of 32.1 mos and 26.6 mos repectively.
• AEs leading to ibrutinib discontinuation occurred in 8% (10/132) of patients within the first year of treatment and declined to 2%(2/103) of patients after the first year of and 3%(2/68) after the second year of treatment.
Response
Rate n (%)
TN ≥ 65 years (n = 31)
R/R(n = 101)
Total(N = 148)
ORR 81% 86% 84%
ORR + PR‐L87% 90% 89%
Safety: Grade ≥ 3 Adverse Events by Time to Event Onset*
Efficacy: Best Overall Response (ORR)
(Partial Response with Lymphocytosis)
Independent Evaluation of Ibrutinib Efficacy 3 Years Post-Initiation ofMonotherapy in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Including Deletion 17p Disease (O’Brien, ASCO 2014)
19
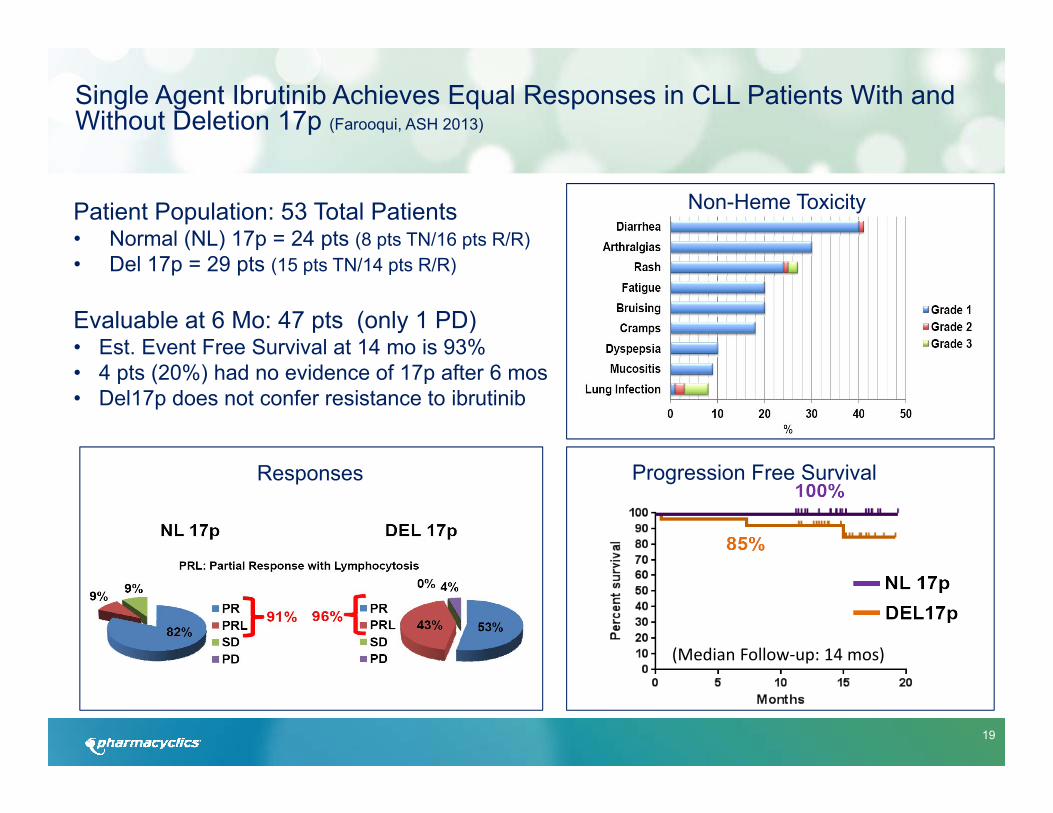
Single Agent Ibrutinib Achieves Equal Responses in CLL Patients With and Without Deletion 17p (Farooqui, ASH 2013)
Patient Population: 53 Total Patients• Normal (NL) 17p = 24 pts (8 pts TN/16 pts R/R)• Del 17p = 29 pts (15 pts TN/14 pts R/R)
Evaluable at 6 Mo: 47 pts (only 1 PD)• Est. Event Free Survival at 14 mo is 93%• 4 pts (20%) had no evidence of 17p after 6 mos• Del17p does not confer resistance to ibrutinib
Non-Heme Toxicity
Responses Progression Free Survival
(Median Follow‐up: 14 mos)

20
Ibrutinib in combination with rituximab (iR) is well tolerated and induces a high rate of durable remissions in patients with high-risk CLL: new, updated results of a Phase II trial in 40 patients (Burger, ASH 2013)
• i+R resulted in a ORR of 95% in high risk pts. 78% of patients were progression free after 18 mos.
• The ORR in the 20 pts with del17p or TP53 mutation was 90% (16 PR, 2 CR).
• Treatment generally was well tolerated, with infectious complications (6 cases of pneumonia and 3 cases of upper respiratory infections) being the most common complication. There were two Grade 3, possibly related AEs: mucositis (n=1), and peripheral neuropathy (n=1). Milder toxicities included Grade 1-2 bruising (n=7), Grade 1 subdural hematoma (n=1), fatigue (n=2), bone pain, myalgias, and arthralgia (n=5), or diarrhea (n=1).

21
• 31 treatment naïve pts treated with ibrutinibmonotherapy.
• After median follow-up of 22.1 mos, ORR was 71% (13% CR)
• Est. PFS: 96.3% at 24 mos(Figure A)
• Est. Overall Survival: 96.6% at 24 mos(Figure B)
Ibrutinib as initial therapy for elderly patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: an open-label, multicentre, phase 1b/2 trial (O’Brien, Lancet 2013)
22
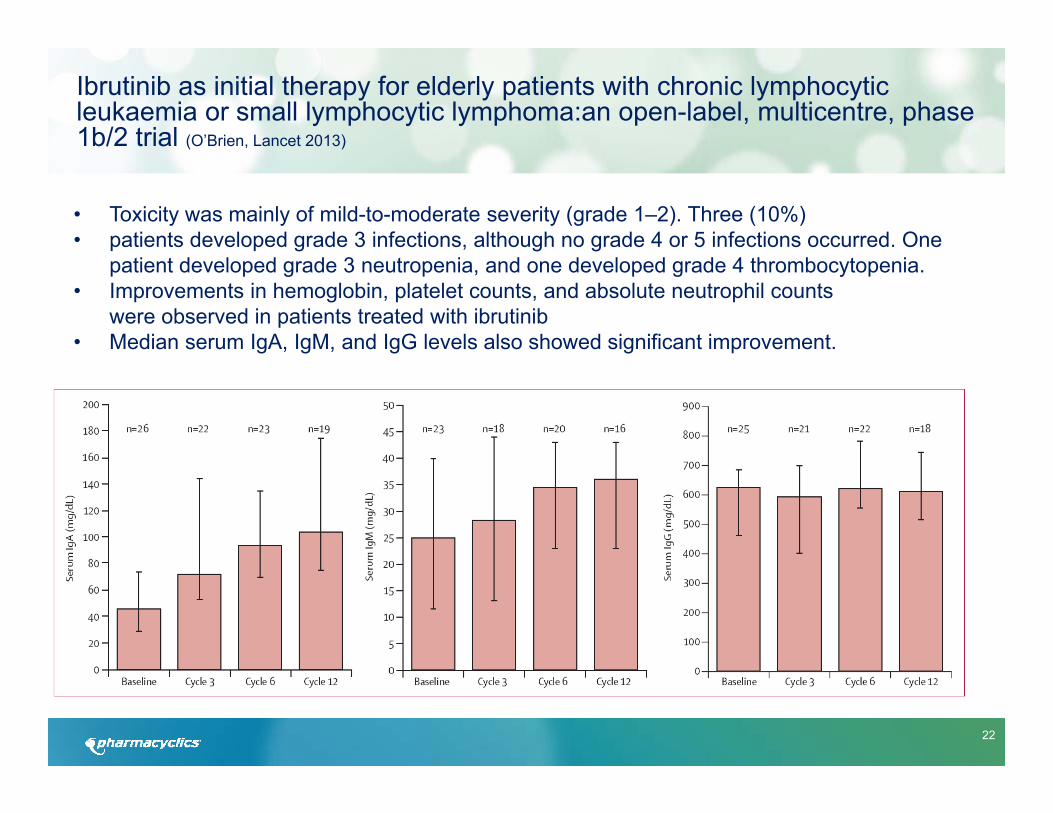
• Toxicity was mainly of mild-to-moderate severity (grade 1–2). Three (10%)• patients developed grade 3 infections, although no grade 4 or 5 infections occurred. One
patient developed grade 3 neutropenia, and one developed grade 4 thrombocytopenia.• Improvements in hemoglobin, platelet counts, and absolute neutrophil counts
were observed in patients treated with ibrutinib• Median serum IgA, IgM, and IgG levels also showed significant improvement.
Ibrutinib as initial therapy for elderly patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma:an open-label, multicentre, phase 1b/2 trial (O’Brien, Lancet 2013)
23
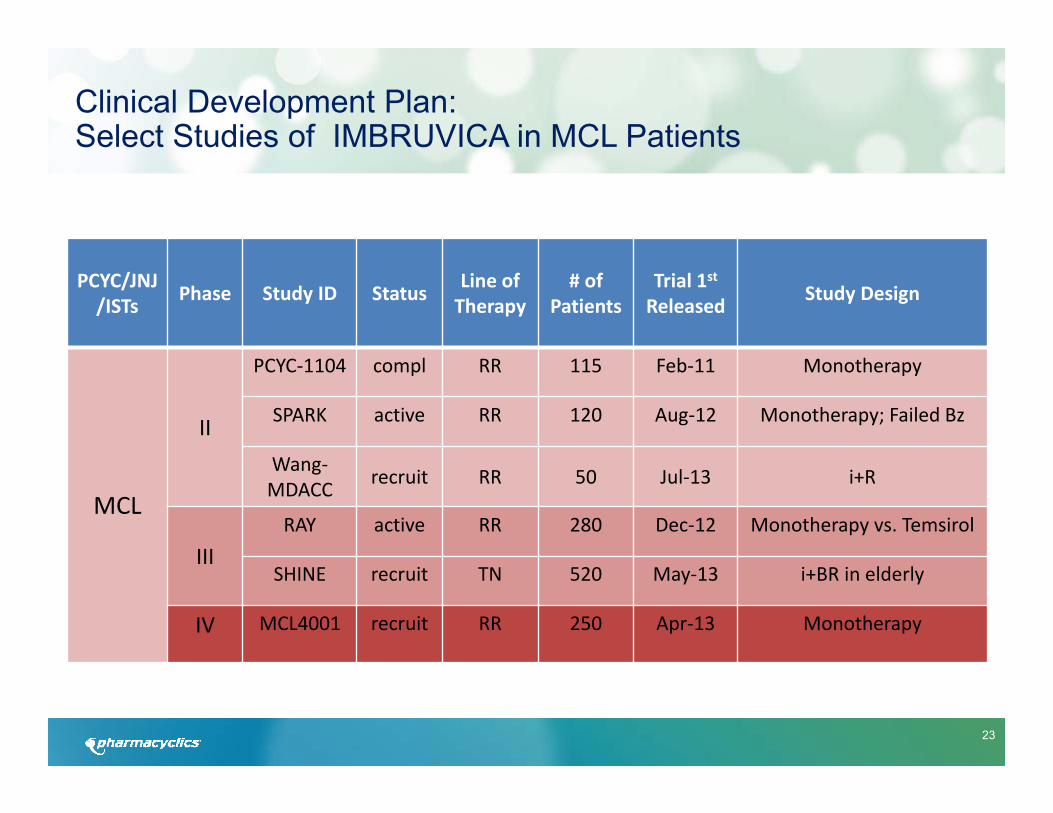
Clinical Development Plan: Select Studies of IMBRUVICA in MCL Patients
PCYC/JNJ/ISTs Phase Study ID Status Line of
Therapy# of
PatientsTrial 1stReleased Study Design
MCL
II
PCYC‐1104 compl RR 115 Feb‐11 Monotherapy
SPARK active RR 120 Aug‐12 Monotherapy; Failed Bz
Wang‐MDACC recruit RR 50 Jul‐13 i+R
IIIRAY active RR 280 Dec‐12 Monotherapy vs. Temsirol
SHINE recruit TN 520 May‐13 i+BR in elderly
IV MCL4001 recruit RR 250 Apr‐13 Monotherapy

24
Highlights EHA 2013: Phase II Monotherapy Trial in Relapsed/Refractory MCL Patients-Long Term Follow Up (Rule, EHA 2013)
PATIENT CHARACTERISTICS FOR ALL TREATED POPULATION
Bortezomib‐Naïve(N = 63)
Bortezomib‐Exposed(N = 48)
Total(N = 111)
Median Age, yrs (Range) 66 (46‐83) 69 (40–84) 68 (40–84)
Gender: Male 46 (73%) 39 (81%) 85 (77%)
ECOG Status: 0 ‐ 12> 2
53 (84%)9 (14%)1 (2%)
46 (96%)2 (4%) 0 (0%)
99 (89%)11 (10%)1 (1%)
Prior Regimens:Median (Range)≥ 3 regimens
2 (1‐5)31 (49%)
3 (1‐5)30 (63%)
3 (1‐5)61 (55%)
Median Months Since Diagnosis (Range) 29 (3‐213) 48 (7‐223) 42 (3‐223)

25
Hematological AE
Bleeding events ≥ grade 3 occurred in 5% of patients
Non‐Hematological AE
.
0% 10% 20% 30% 40% 50% 60%
NeutropeniaThrombocytopenia
Anemia
0% 10% 20% 30% 40% 50% 60%
DiarrheaFatigueNausea
Oedema peripheralDyspnea
ConstipationUpper respiratory tract infection
VomitingDecreased appetite
CoughPyrexia
Abdominal painContusion
Rash
Grade 1Grade 2Grade 3Grade 4Grade 5
Highlights EHA 2013: Treatment Related and Unrelated AEs Occurring in >15% of MCL Patients (Rule, EHA 2013)
26
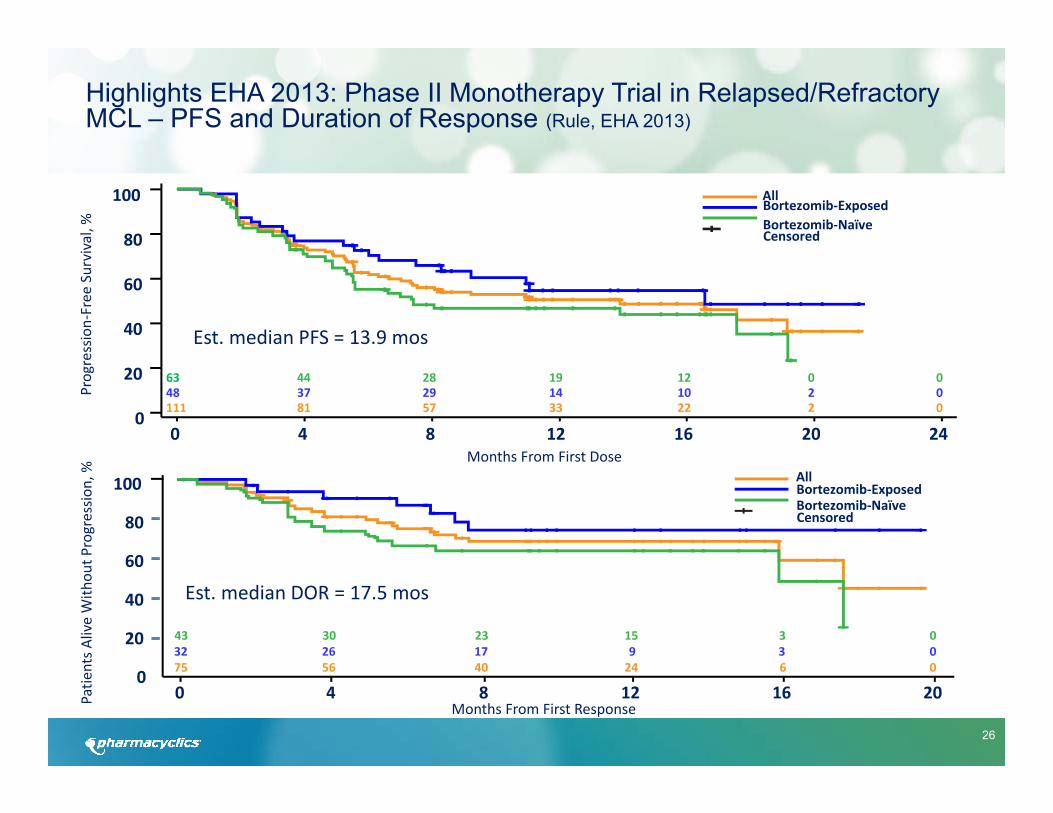
Highlights EHA 2013: Phase II Monotherapy Trial in Relapsed/Refractory MCL – PFS and Duration of Response (Rule, EHA 2013)
100
0
80
20
40
60
240 4 128 16 20
Progression‐Free
Survival, %
Months From First Dose
AllBortezomib‐ExposedBortezomib‐NaïveCensored
111 81 57 33 22 048 37 29 14 10 063 44 28 19 12 0
220
100
0
80
20
40
60
200 4 128 16Months From First Response
75 56 40 24 6 032 26 17 9 3 043 30 23 15 3 0
AllBortezomib‐ExposedBortezomib‐NaïveCensored
Patie
nts A
live With
out P
rogressio
n, %
Est. median PFS = 13.9 mos
Est. median DOR = 17.5 mos
27
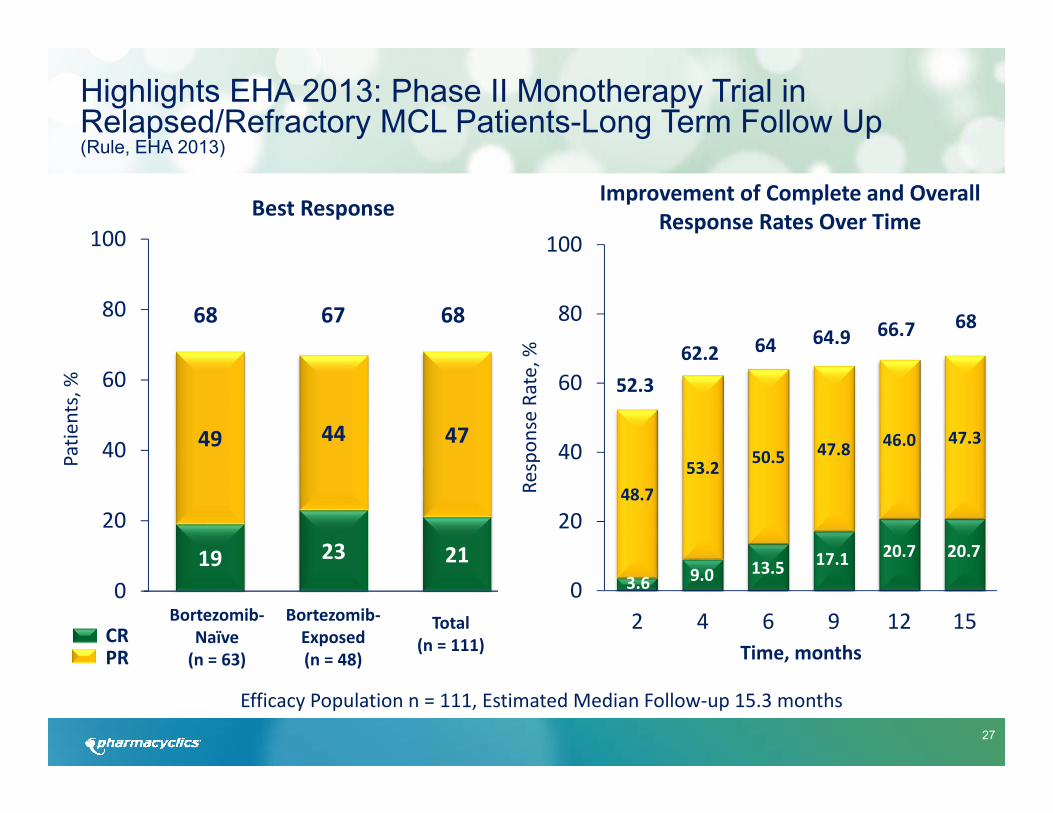
Best Response
19 23 21
49 44 47
0
20
40
60
80
100
Bortezomib‐Naïve(n = 63)
Bortezomib‐Exposed(n = 48)
Total(n = 111)
68 67 68
Efficacy Population n = 111, Estimated Median Follow‐up 15.3 months
CRPR
Patie
nts, %
48.753.2 50.5 47.8 46.0 47.3
0
20
40
60
80
100
2 4 6 9 12 15
Respon
se Rate, %
Time, months
66.7 68
52.362.2 64 64.9
Improvement of Complete and Overall Response Rates Over Time
Highlights EHA 2013: Phase II Monotherapy Trial in Relapsed/Refractory MCL Patients-Long Term Follow Up (Rule, EHA 2013)
3.6 9.0 13.5 17.1 20.7 20.7

28
Clinical Development Plan: Select Studies of IMBRUVICA in DLBCL Patients
PCYC/JNJ Phase Study ID Status Line of Therapy
# of Patients
Trial 1stReleased Study Design
DLBCLII
DLB1002 active TN 32 Jun‐12 i+RCHOP; DLBCL, MCL, FL
PCYC‐1106 active RR 125 May‐11 Monotherapy
PCYC‐1123 recruit RR 110 ASH ’13 i+R+Len vs. i+Len
PCYC‐1124 recruit RR 56 ASH ’13 i+Len+DA‐EPOCH‐R
III DBL3001 recruit TN 800 Sept‐13 i+RCHOP vs. RCHOP
29
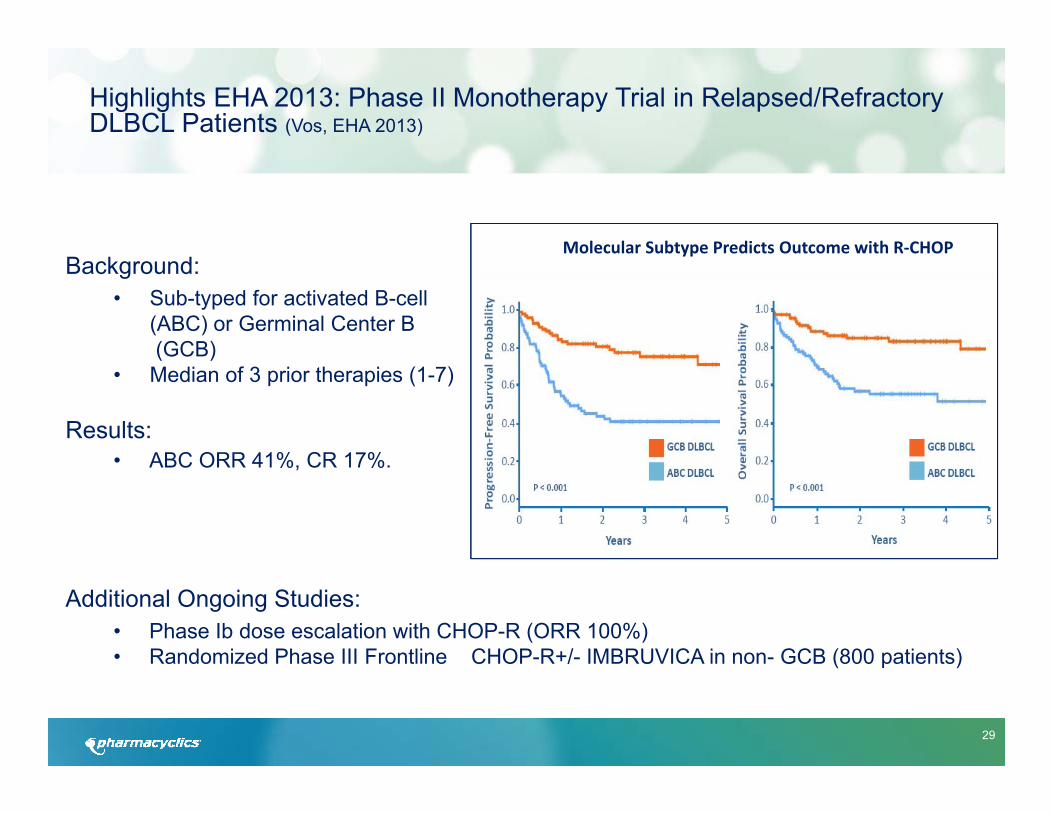
Highlights EHA 2013: Phase II Monotherapy Trial in Relapsed/Refractory DLBCL Patients (Vos, EHA 2013)
Background:• Sub-typed for activated B-cell
(ABC) or Germinal Center B(GCB)
• Median of 3 prior therapies (1-7)
Results: • ABC ORR 41%, CR 17%.
Additional Ongoing Studies:• Phase Ib dose escalation with CHOP-R (ORR 100%)• Randomized Phase III Frontline CHOP-R+/- IMBRUVICA in non- GCB (800 patients)
Molecular Subtype Predicts Outcome with R‐CHOP
30
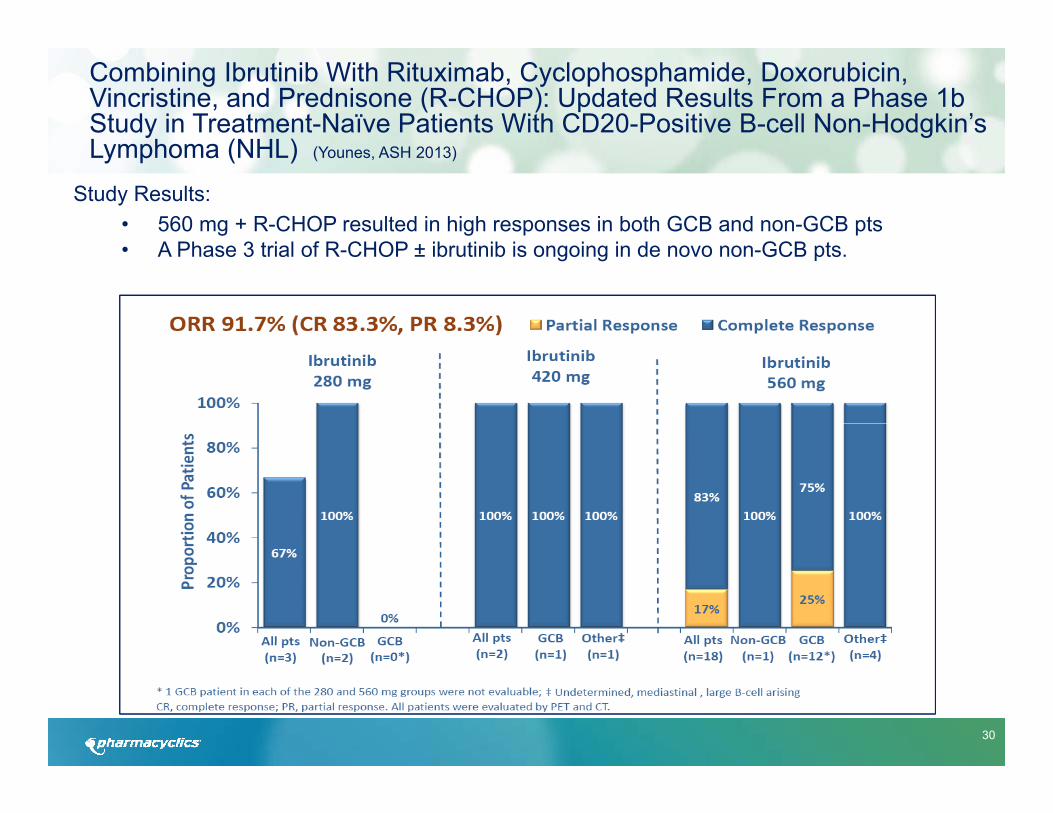
Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP): Updated Results From a Phase 1b Study in Treatment-Naïve Patients With CD20-Positive B-cell Non-Hodgkin’s Lymphoma (NHL) (Younes, ASH 2013)
Study Results:• 560 mg + R-CHOP resulted in high responses in both GCB and non-GCB pts• A Phase 3 trial of R-CHOP ± ibrutinib is ongoing in de novo non-GCB pts.
31
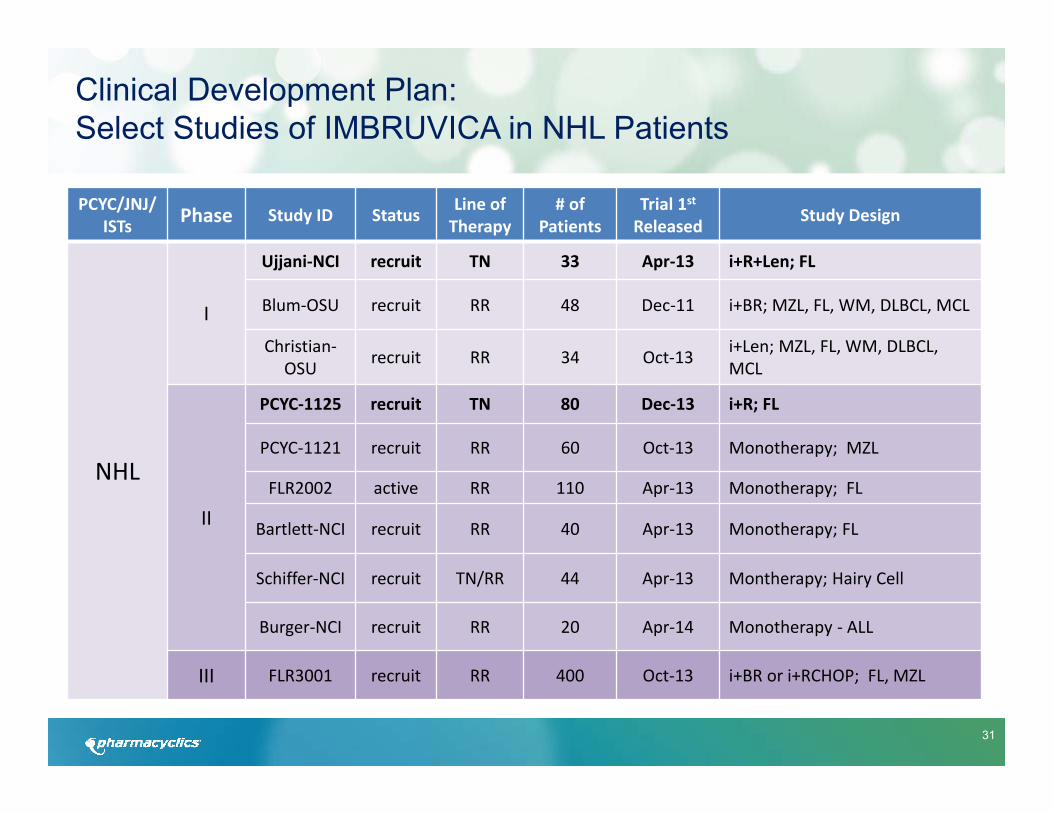
Clinical Development Plan: Select Studies of IMBRUVICA in NHL Patients
PCYC/JNJ/ ISTs Phase Study ID Status Line of
Therapy# of
PatientsTrial 1stReleased Study Design
NHL
I
Ujjani‐NCI recruit TN 33 Apr‐13 i+R+Len; FL
Blum‐OSU recruit RR 48 Dec‐11 i+BR; MZL, FL, WM, DLBCL, MCL
Christian‐OSU recruit RR 34 Oct‐13 i+Len; MZL, FL, WM, DLBCL,
MCL
II
PCYC‐1125 recruit TN 80 Dec‐13 i+R; FL
PCYC‐1121 recruit RR 60 Oct‐13 Monotherapy; MZL
FLR2002 active RR 110 Apr‐13 Monotherapy; FL
Bartlett‐NCI recruit RR 40 Apr‐13 Monotherapy; FL
Schiffer‐NCI recruit TN/RR 44 Apr‐13 Montherapy; Hairy Cell
Burger‐NCI recruit RR 20 Apr‐14 Monotherapy ‐ ALL
III FLR3001 recruit RR 400 Oct‐13 i+BR or i+RCHOP; FL, MZL

32
Highlights ASH 2012: Phase I Monotherapy Trial Subset of Relapsed/Refractory Follicular Lymphoma Patients (Fowler, ASH 2012)
Background:• Prior chemoimmunotherapy• Median of 3 prior therapies (1-5)
Results:• 16 subjects enrolled: ORR=44%• Trend for dose response
o 9 patients >5.0 mg/kg with ORR: 56% (3 CRs and 2 PRs) and median estimated Progression Free Survival = 19.6 months
Study initiated by Janssen:• Single arm monotherapy IMBRUVICA Phase II trial in relapsed / refractory follicular
patients• Primary endpoint Overall Response Rate
33
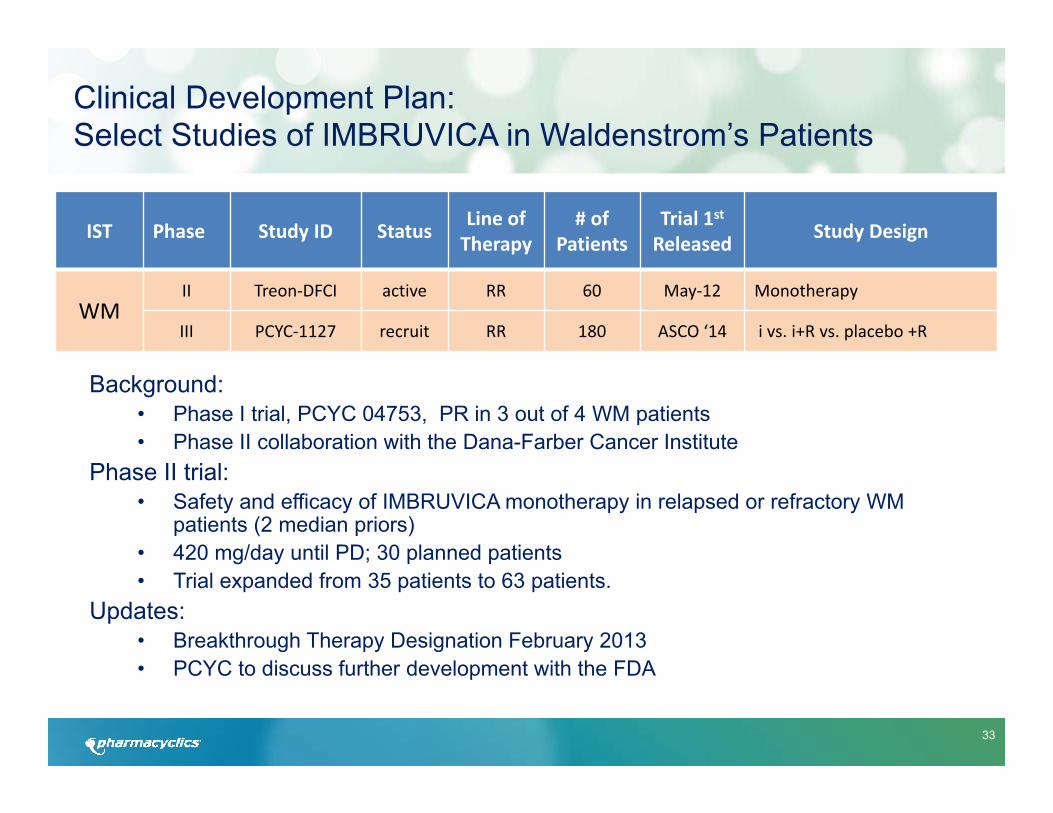
Background:• Phase I trial, PCYC 04753, PR in 3 out of 4 WM patients• Phase II collaboration with the Dana-Farber Cancer Institute
Phase II trial:• Safety and efficacy of IMBRUVICA monotherapy in relapsed or refractory WM
patients (2 median priors)• 420 mg/day until PD; 30 planned patients• Trial expanded from 35 patients to 63 patients.
Updates:• Breakthrough Therapy Designation February 2013• PCYC to discuss further development with the FDA
Clinical Development Plan: Select Studies of IMBRUVICA in Waldenstrom’s Patients
IST Phase Study ID Status Line of Therapy
# of Patients
Trial 1stReleased Study Design
WMII Treon‐DFCI active RR 60 May‐12 Monotherapy
III PCYC‐1127 recruit RR 180 ASCO ‘14 i vs. i+R vs. placebo +R
34
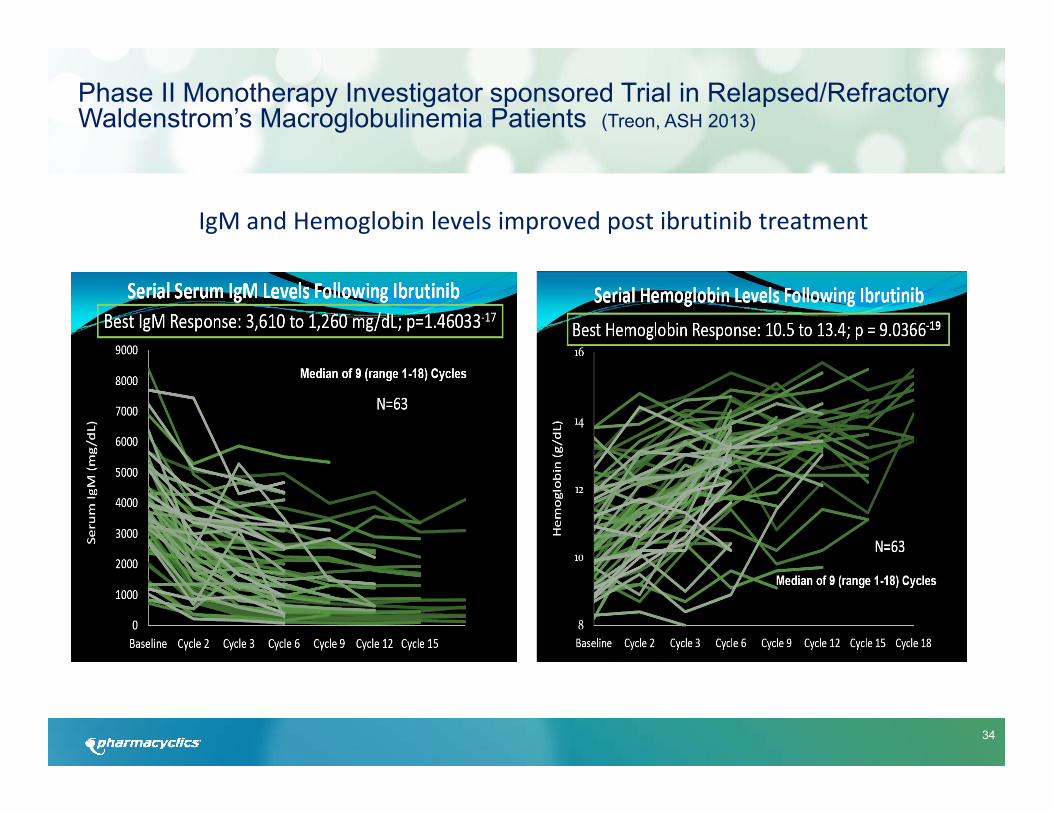
Phase II Monotherapy Investigator sponsored Trial in Relapsed/Refractory Waldenstrom’s Macroglobulinemia Patients (Treon, ASH 2013)
IgM and Hemoglobin levels improved post ibrutinib treatment
35
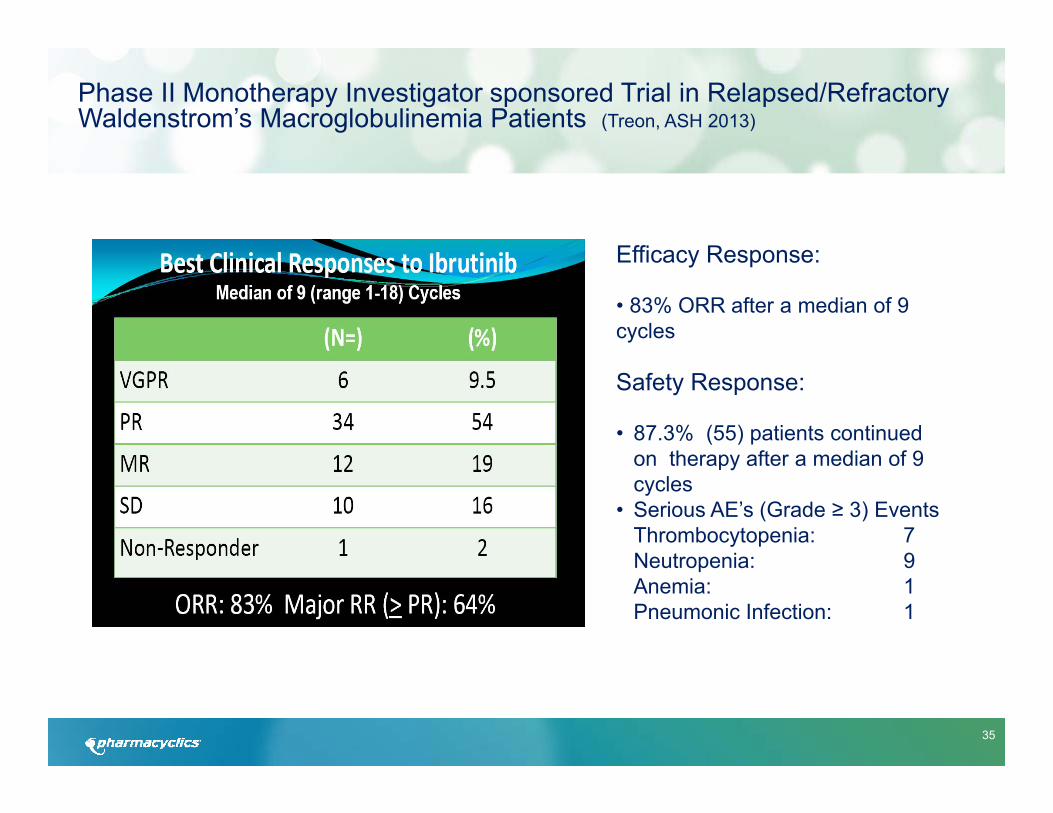
Phase II Monotherapy Investigator sponsored Trial in Relapsed/Refractory Waldenstrom’s Macroglobulinemia Patients (Treon, ASH 2013)
Efficacy Response:
• 83% ORR after a median of 9 cycles
Safety Response:
• 87.3% (55) patients continued on therapy after a median of 9 cycles
• Serious AE’s (Grade ≥ 3) EventsThrombocytopenia: 7Neutropenia: 9Anemia: 1Pneumonic Infection: 1

36
Highlights ASH 2012: Phase II Monotherapy Trial in Relapsed/Refractory MM Patients (Vij, ASH 2012)
Background• Median of 4 prior treatments• Prior bortezomib and lenalidomide
Results• Signals of biologic and clinical activity• 5/13 patients had a reduction in paraprotein , 1 PR in combo with dexamethasone• Decreases in biomarkers of bone metabolism, angiogenesis and chemotaxis were observed
Ongoing Study• Cohorts 1-3 were not expanded (420mg, 560 mg with dex, 840mg) as they did not achieve desired
results.• A pre-specified boundary of response was met with cohort 4, a 840 mg dose of IMBRUVICA in
combination with dexamethasone. The Company has expanded the fourth and final dosing cohort to 43 patients (840mg with dexamethasone) as it crossed a minimum pre-defined boundary of efficacy.
Clinical Development Plan: Select Studies of IMBRUVICA in Multiple Myeloma Patients
PCYC/JNJ Phase Study ID Status Line of Therapy
# of Patients
Trial 1stReleased Study Design
MMI PCYC‐1119 recruit RR 176 Dec‐13 i+Carfilzomib
II PCYC‐1111 recruit RR 164 Mar‐12 Monotherapy or i+Dex

37
Clinical Development Plan: IMBRUVICA in Graft vs. Host Disease Patients
PCYC/JNJ Phase Study ID Status Line of Therapy
# of Patients
Trial 1stReleased Study Design
GvHD I PCYC-1129 recruit RR 39 Jul-14 Monotherapy
Background• Graft-versus-host disease (GvHD) develops in patients who have undergone allogeneic (donor) stem cell or
bone marrow transplant. Because the tissue or cells come from a donor, they recognize the patient’s cells as foreign and attack the patients body through an immune response. The probability of GvHD occurring depends on the match between the patient and the donor. Approximately 35-50% of the 10,000 allogeneic transplants in the U.S. develop chronic graft-versus-host disease.
PCYC-1129Primary Outcome Measures• Phase Ib: Number of dose-limiting toxicities as a measure of safety profile to determine recommended dose
of ibrutinib [ Time Frame: 28 treatment days after last subject enrolled in Phase 1 dose level(s).]• Phase II (Efficacy): Overall cGVHD response rate defined as the proportion of evaluable subjects who
achieve a NIH-defined Complete Response (CR) and Partial Response (PR) over all subjects who were treated with recommended phase 2 dose [ Time Frame: When the last subject completes 6 months of treatment.]
38
Breakthrough Therapy Designations and Regulatory Progress
• IMBRUVICA received Full (regular) Approval on July 28, 2014 for the treatment of patients with chronic lymphocytic leukemia (CLL) who have received at least one prior therapy, and for the treatment of all CLL patients with deletion of the short arm of chromosome 17 (del 17p CLL).
• European Medicines Agency recommended Full Approval on July 25, 2014 for the treatment of adult patients with CLL who have received at least one prior therapy and with relapsed/refractory MCL. A positive opinion was also received for the treatment of adult CLL patients with del17p or TP53 mutation who are treatment naïve.
• IMBRUVICA received accelerated approval on November 13, 2013 for the treatment of patients with MCL who have received at least one prior therapy.
• FDA approved Breakthrough Designations for IMBRUVICA in:o Relapsed/Refractory Mantle Cell Lymphoma (MCL) - Feb 2013o Waldenstrom’s Macroglobulinemia (WM) - Feb 2013o Chronic Lymphocytic Leukemia (CLL) with deletion 17p - Mar 2013

39
IMBRUVICA®
Received Full Approval for two CLL indications on July 28, 2014 and Accelerated Approval for one MCL indication on November 13, 2013.
Label includes: Statistically Significant Improvement in Overall Survival (HR=0.22, p<0.0001) and Progression Free Survival (HR=0.43, p<0.05) for Previously Treated CLL Patients vs. Ofatumumab
Indications: CLL and MCL Patients who have received at least one prior therapyCLL Patients with Del 17P (all lines)

40
“[IMBRUVICA] is a revolutionary blood cancer drug.”
Headlines and Highlights….Approval Grabs Attention of Top Tier Media
FDA speedily approves Imbruvica, a treatment
for rare lymphoma
J&J-Pharmacyclics Win U.S. Approval for
Breakthrough Drug
41
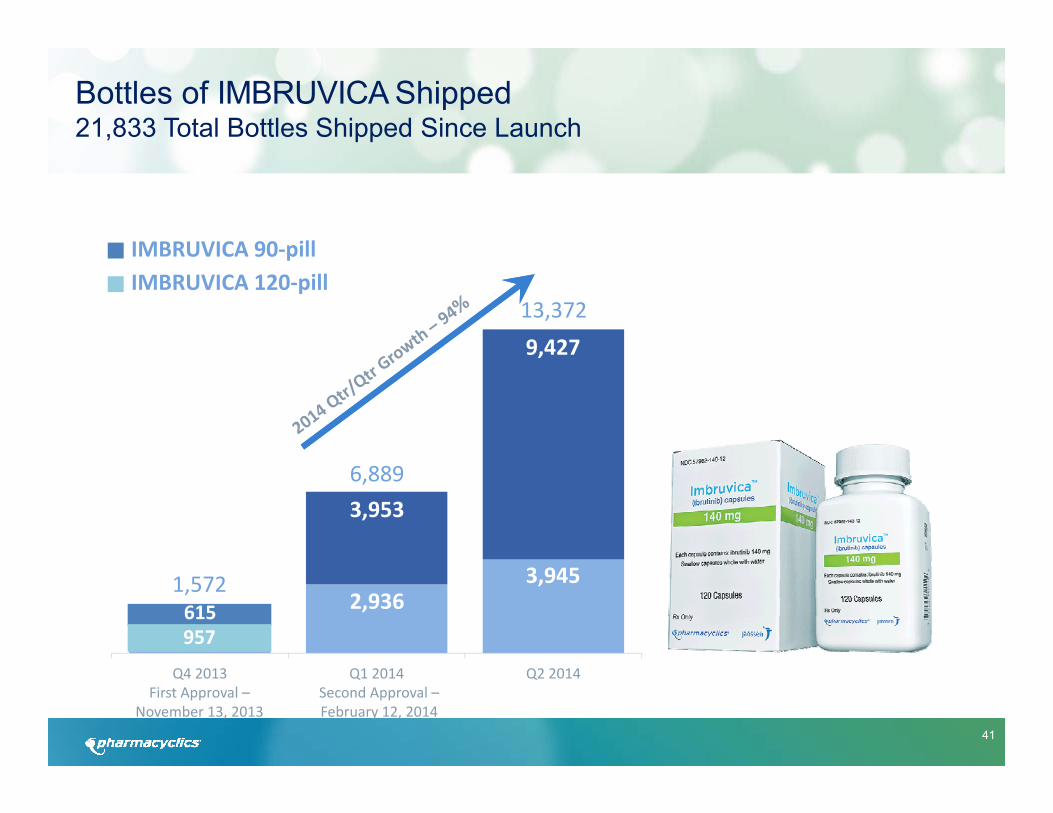
Q4 2013 Q1 2014 Q2 2014First Approval –
November 13, 2013Second Approval –February 12, 2014
13,372
6,889
1,572
9,427
3,945
3,953
2,936615957
Bottles of IMBRUVICA Shipped 21,833 Total Bottles Shipped Since Launch
IMBRUVICA 90‐pillIMBRUVICA 120‐pill

42
Patient Populations (G7) in Major Hematological Malignancies
US All Major Markets3
Incidence Prevalence Incidence Prevalence
CLL/SLL 20,6001 121,2002 41,0001 267,0001
MCL 2,9001 11,3002 6,5001 38,2001
WM 1,5004 12,0002 6,0004 23,0004
DLBCL 25,0001 112,0002 54,1001 367,0001
FL 13,7001 63,0002 28,5001 245,0001
MM 20,0001 77,0001 48,0001 183,0001
TOTAL 83,700 396,5002 184,100 1,123,2001
1 © 2014 DR/Decision Resources, LLC. All rights reserved. Reproduction, distribution, transmission or publication is prohibited.2 IMS patient claims estimates for July 2013‐June 2014. Note: This information is an estimate derived from the use of information under license from the following IMS Health Incorporated information service: IMS Oncology Tracking Reports for the period July 2013 to June 2014. IMS expressly reserves all rights, including rights of copying, distribution and republication.3 Major markets include: US, UK, Spain, Germany, France, Italy, and Japan 4 WM Foundation estimate Pharmacyclics, Inc. makes no representation with respect to the accuracy or reliability of this information. Investors are advised to independently verify this informationbefore using it to make investment decisions.

43
CLL/SLL & MCL US Prevalence Patient Estimates
CLL/SLL MCL
Diagnosed Incidence 1 20,600 2,900
Prevalence 2 121,200 13,300
No Therapy 2 54,700 2,400
1L Therapy 2 23,300 4,800
2L Therapy 2 10,300 1,400
3L+ Therapy 2 7,000 1,000
*Other 2 (All these patients are between lines of therapy; 1/3 received maintenance, 2/3 were not on therapy in observation period)
25,900 3,700
1 © 2014 DR/Decision Resources, LLC. All rights reserved. Reproduction, distribution, transmission or publication is prohibited. Reprinted with permission. 2 IMS patient claims estimates for July 2013‐June 2014. Note: This information is an estimate derived from the use of information under license from the following IMS Health Incorporated information service: IMS Oncology Tracking Reports for the period July 2013 to June 2014. IMS expressly reserves all rights, including rights of copying, distribution and republication.Pharmacyclics, Inc. makes no representation with respect to the accuracy or reliability of this information. Investors are advised to independently verifythis information before using it to make investment decisions.

44
Histone Deacetylase Inhibitor: Abexinostat
• Abexinostat is optimized for half-life, oral bioavailability, and potency and synergizes with DNA-damaging agents. A new formulation has been developed and recently patented.
• Partnered ex-US with Servier, in Phase I/II program in Europe
• Phase 2 PCYC study in lymphoma completed and presented at ASH 2012, further updates presented at ICML in Lugano, June 2013
• Combination therapies between HDAC and other agents are being investigated.

45
Factor VIIa Inhibitor: PCI-27483
• First small-molecule FVII-specific inhibitor targeting the tissue factor (TF) pathway
• Tissue factor is upregulated in certain tumors. TF:VIIa complex induce signaling pathways that lead to increase in cancer cell migration and invasion
• Phase II pancreatic cancer trial completed, results provided at ASCO, June 2013
• Further usage of PCI-27483 are currently being investigated
46
BROAD PATENT COVERAGE:Our lead product candidates have issued US and European composition of matter patents and are covered by various issued/pending patent applications in other major markets
• BTK Inhibitor, IMBRUVICA® (ibrutinib - PCI-32765) covered by issued/pending patents projected until Dec 2026 – with a potential patent term extension to Nov. 2027. (Pharmacyclics also owns pending patent applications in the U.S. and internationally covering specifically crystalline and polymorph forms of IMBRUVICA as well as the use of IMBRUVICA for the treatment of various types of cancer).
• Factor VIIa Inhibitor, PCI-27483 covered by issued/pending patents projected until2023
• HDAC Inhibitor, PCI-24781 with new formulation covered by issued/pending patents projected until 2035
Strong Patent Portfolio
47
Worldwide collaboration to broaden and accelerate the development of IMBRUVICA in oncology, signed in December 2011
• $150M upfront; milestones $250M for continued development progress, $225M for regulatory progress and $350M for approval
• Global development plan defined, each company leading the development for specific indications. Development costs shared 40% Pharmacyclics and 60% Janssen for multiple phase III trials
• 50/50 profit split. Pharmacyclics will book sales and lead commercialization strategy in the US; Janssen will be responsible for the same outside the US
• Development and commercialization activities managed through a shared governance structure
Collaboration with Janssen Biotech to Develop and Commercialize IMBRUVICA

48
Key Corporate Data
GENERAL
- Founded- Location- Employees as of 06/30/2014
1991Sunnyvale, CA
557
SELECT FINANCIAL INFORMATION
- Net Product Sales Q2/2014 $109.5 M
- Non-GAAP Total Costs and Expenses Q2/2014 $132.9 M*
- Cash & Cash Equivalents as of 06/30/2014 $678.0 M**
- Basic Shares Outstanding as of 06/30/2014 75.3 M
Janssen Biotech, Inc. contractual milestones remaining:Development Progress $ 50 million Regulatory Progress $ 70 millionApproval $ 200 million
$ 320 million (earned as of 08/05/14: upfront $150M, $200M in development milestones, $155M in Regulatory Progress, $150M Approval)
•Non GAAP Expenses do not include $17.2M in stock-based compensation expense.
** Cash does not include net $24.7M payment due to Janssen under the collaboration agreement.
49
PharmacyclicsMaking a difference for the
betterment of patients