
PCOS What Lies Beneath… - wesley ob/gyn · • Hyperprolactinemia • Late onset congenital...
63
Rami Mortada, MD Assistant Professor Division of Endocrinology Kansas University – Wichita PCOS What Lies Beneath…
Transcript of PCOS What Lies Beneath… - wesley ob/gyn · • Hyperprolactinemia • Late onset congenital...

Rami Mortada, MD
Assistant Professor
Division of Endocrinology
Kansas University – Wichita
PCOS
What Lies Beneath…

Outline
• PCOS definition
• Pathogenesis
• Manifestation
• Diagnosis
• Practical management
• Conclusion
PCOS • Most common endocrinopathy in female of
reproductive age: 6 - 12%
• Hyperandrogenic anovulation
• Increased risks for :
- Type 2 DM
- GDM
- Hypertension
- Dyslipidemia
- Endometrial cancer
- Cardiovascular disease

PCOS
Polycystic
ovaries Oligomenorrhea
Hyperandrogenism

PCOS
Polycystic
ovaries Anovulation
Hyperandrogenism LH/FSH
Hypertension
Obesity
Dyslipidemia
Insulin
resistance
Endometrial
hyperplasia

PCOS: NIH Definition
Anovulation Hyperandrogenism +

PCOS: Rotterdam Consensus
Definition: 2 out of 3
Polycystic
ovaries Anovulation
Hyperandrogenism

PCOS: AEPCOS Definition
Polycystic
ovaries Hyperandrogenism + Anovulation and/or

PCOS diagnosis Stein Leventhal
NIH Criteria 1990
Rotterdam 2003 ( 2of 3)
Androgen excess society 2006 ( HA +1)
Hyperandrogenism (HA)
Oligo or amenorrhra
Polycystic ovaries
Required
part of the diagnosis
Not needed

PCOS Diagnosis
• PCOS is a clinical diagnosis.
• No single confirmatory test for PCOS.
• Ovarian cysts are not required for diagnosis.
• Cysts are present on ultrasound in more than 90% of women with PCOS but also present in up to 25% of women without PCOS.
• volume ≥ 10 ml • follicles ≥ 12 • each 2–9 mm

Age 20 30
Oligomenorrhea
10
Acanthosis nigricans
Weight gain
Infertility
Gestational DM
Type 2 DM
Hirsutism
40
Miscarriages Cardiovascular Disease
0 8
SGA Early adrenarche

Criteria for Diagnosis of PCOS
– Hyperandrogenism
• Elevated serum androgen levels or • Biological expression of hyperandrogenism (acne or hirsutism)
– Ovarian Dysfunction
• Anovulation or oligo-ovulation or • Polycystic ovaries
– Absence of other causes of anovulation
• Thyroid disorders • Hyperprolactinemia • Late onset congenital adrenal hyperplasia (CAH) • Cushing’s syndrome • Ovarian and adrenal tumors

Hyperandrogenemia
• Most reliable element for diagnosis
• Rely on bioavailable testosterone testing—not total testosterone
• Progressive hirsutism is important
• Acne is less helpful
Hyperandrogenism
• Non-virilizing sign: – Hirsutism
– Acne
– Oily skin
– Abnormal menstrual cycles
– Infertility
• Virilizing sign: – Male pattern balding
– Masculinization of body habitus
– Increased libido
– Clitorimegaly
– Deepening of the voice

Pelvic Ultrasound
• Least reliable criterion
• Trans-vaginal may not be feasible
• Polycystic (or multi-follicular) ovaries are common
• Volume criterion > 10 ml applies (>7.8 in some studies)

Pathogenesis
• Complex genetic trait where genetic variants and environmental factors interact to foster the development of the disorder
• Primary Disordered Gondadotropin Secretion: Increased LH, decreased FSH secretion
• Primary Ovarian and Adrenal Hyperandrogenism
• Primary Disorder of Insulin Resistance

Insulin and Androgens
Disordered FSH/LH
secretion Hyperinsulinemia
Hyperinsulinemia
Hyperandrogenemia
Hyperandrogenemia
Hyperinsulinemia
1
2
3
+
++
+++

PCOS: an evolutionary paradox
• Why PCOS is so common ?
• Fertility first hypothesesis
• Ovarian function is higly dependant to nutrional status
• Insulin, Leptin and blood glucose decrease in period of famin
• PCOS have an ovulation/ fertility advatage in a caloric restrictive environment


Am J Hum Biol. 2009 Sep-Oct;21(5):587-98. doi: 10.1002/ajhb.20937.

Associations of PCOS with clinical conditions
PCOS present in
• Anovulatory infertility: 75%
• Oligomenorrhoea: 87%
• Hirsutism: 80%
• Infertility: 33%
• Acne to presenting to dermatology clinic: 75%
• Amenorrhoea: 30-40%
(Adams 1986, Hull 1987, Bunker 1989)

Investigation
• Bioavailable testosterone (Free + Weakly bound)
• DHEA-S
• 17 OH-P
• SHBG
• TSH
• Prolactin
• FSH, LH, Progesterone
• HgbA1c, OGTT, Glucose & insulin levels
• Fasting lipids
• 24 h urine cortisol
• Dexamethasone suppression test
• Ovarian U/S ( Intravaginal )
• CT, MRI if suspicion of adrenal tumor
Test to order Test to consider

23
Circulating Testosterone
SHBG-bound
T (tight)
44%
Albumin-
bound T
(weak)
54%
Free T
2%
Bioavailable T
Total T

What about free testosterone ?
• Free T are calculated using an analog assay:
– Inaccurate and generally report lower values
• Free T should be measured directly by equilibrium dialysis
followed by liquid chromatography plus mass spectrometry
• When in doubt check Bioavailable Testoserone

Reference
Range
Patient 1 Patient 2
Total-T 11-56
ng/dl
50 48
SHBG 30-135 nmol/l 25 186
Bioavail-T 4.1-22.6 ng/dl 26.0 5.8
Free-T 1.3-9.2 pg/ml 10 2.3
Laboratory-Why bioavailable testosterone?

Manifestations
• Acne & Hirsutism
• Oligomenorrhea
• Infertility
• Insulin resistance/ obesity

Acne & Hirsutism

Hirsutism

La Mujer Barbuda…

Types of hair Lanugo
Fetal hair
Vellus Short-fine
Unpigmented
Pre-puberty
Terminal Long-coarse
Pigmented
From vellus hair

Ferriman-Gallwey score

Treatment
• Pharmacological or direct hair removal: Very low
• Depilation: remove hair shafts from the skin surface ( shaving, depilatory cream…)
• Epilation: extract hairs to above the bulb (waxing, tweezing, plucking …)
• Bleaching
Shaving does not affect the rate or duration of the anagen phase or diameter of hair, but it yields a blunt tip which gives the illusion of thicker hair

Electrolysis
• Fine needle is inserted into the hair follicle and an electrical current is applied.
• Painful & time-consuming (each hair is treated individually)
• Side effects include erythema and post inflammatory pigment changes & scaring
• Cost effective on small area’s with sparse hair
• Can be used on any skin or hair color.

Photoepilation
• lasers and non-laser light sources(IPL).
• Hair is damaged with wavelengths of light, absorbed by its melanin pigment. Pulse durations selectively damage it without damaging surrounding tissue
• Even though hair follicles are destroyed, it is likely that vellus hair follicles remain and can continually be converted into terminal pigmented hairs when androgen excess is present.

Laser vs electrolysis
• Laser is twice as effective as electrolysis
• Laser is more expensive but less painful
• Laser is 60 times faster than electrolysis
• Laser is more potent on dark thick hair but worthless on thin unpigmented hair

Topical treatment
• Eflornithine is an irreversible inhibitor of ornithine decarboxylase,
• Does not remove hair, but acts to reduce the rate of hair growth
• Results take about 6 to 8 weeks, and once the cream is discontinued hair returns to pretreatment levels after about 8 weeks
• Systemic absorption is extremely low , Low SE profile ( skin irritation and dryness)

Treatment- Acne and Hirsuitism
• OCPs decrease androgen levels by suppressing LH and increasing SHBG.
• OCPs with low androgenic progestins (norgestimate, desogestrel) may be most effective for acne and hirsutism (Level B)
• Trial of at least 6 months before making changes in dose, changing medication, or adding medication

Which OCP to choose ?
• Progestins with low androgenicity (e.g., norgestimate, desogestrel)
• Theoretical advantages to avoiding preparations with levonorgestrel, the most androgenic progestin
• Progestins that exhibit antiandrogenic activity (drospirenone and cyproterone acetate) but increased risk of DVT
• OCPs containing either 30-35 μg ethinyl estradiol may be used for suppression of ovarian androgens
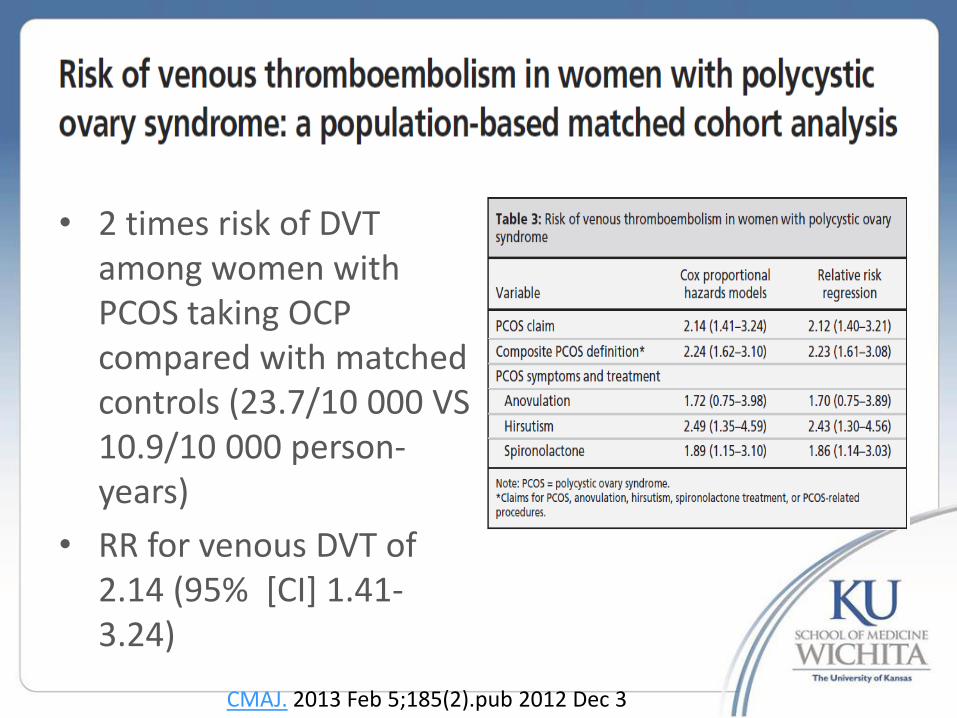
• 2 times risk of DVT among women with PCOS taking OCP compared with matched controls (23.7/10 000 VS 10.9/10 000 person-years)
• RR for venous DVT of 2.14 (95% [CI] 1.41-3.24)
CMAJ. 2013 Feb 5;185(2).pub 2012 Dec 3

Aldactone for acne and hirsutism
• Diuretic, aldosterone antagonist and blocks the androgen receptor
• Dose is 25–100 mg twice a day
• Cautions:
– Hyperkalemia
– Ambiguous genitalia in male infants
Cochrane Database Syst Rev. 2009;(2):CD000194.

Antiandrogen
• Spironolactone Dose-dependant competitive inhibition of the androgen receptor & inhibition of 5a
reductase activity. Typical dose 50- 200 mg. Monitor for hypokalemia
• Cyproterone acetate: Hirsutism & acne ( N/A USA). Progestogenic compound with anti-androgen
activity on the receptor & mild inhibition of 5a reductas,suppresses gonadotropin and androgen levels.
• Drospirenone: Anti androgen progestin used in OCPs. 3 mg (the dose used in OCPs) is equivalent to
spironolactone 25 mg and CPA 1 mg( Yaz, Yasmin, Yasmilelle)
• Finasteride: Inhibits type 2 5a reductase activity. , only a partial inhibitory. hirsutism probably involves
both type 1 &d 2 5a reductase ( 5mg is equivalent to 100 mg of spironolactone)
• Flutamide: “pure” antiandrogen with a dose response inhibition of the androgen R. ( 250-750 mg is
equivalent to 100 mg of spironolactone and 5mg of finasteride). Dose dependant liver toxicity. 250 mg is generally safe

Oligomenorrhea

Oligomenorrhea/Amenorrhea Treatment
• Weight loss ( Low glycemic index diet, aerobic exercise)
• OCPs +++
• Metformin: 500 mg BID - TID – 1/2 normalization of the menstrual function
– 1/3 Induction of ovulation
• Progesterone: – Continuous or
– Cyclic Q 1-3 months
Aim of treatment: prevent development of endometrial hyperplasia
J Clin Endocrinol Metab. 2000;85(1):139 Fertil Steril. 2006;86(1):230 .

OCP Benefits for PCOS
• Regular withdrawal bleeding
• Reduction in the risk of endometrial hyperplasia or cancer
• Reduction in LH secretion and consequent reduction of ovarian androgens
• Increased sex hormone binding globulin production and consequent free testosterone reduction
• Improvement in acne and hirsutism

Infertility

Treatment of Infertility in PCOS
• Weight loss remain the mainstay of treatment
• Clomiphene citrate: Anti-estrogenic effect on hypothalamus GnRh release; increased FSH drives the development of ovarian follicles – 80% will ovulate and 50% of PCOS women will conceive
• Add Metformin: 500 mg po BID – TID in case of insulin resistance/ obesity
• Gonadotropins – Use of low-dose
• Ovarian drilling – Fewer multiple pregnancies compared to gonadotropins

Clomid vs metformin
Ovulation Pregnancy Life birth
Metformin 29 % 12 % 7.22 %
Clomid 80 % 50 % 22.5 %
Metf+ Clomid 85 % 55 % 29 %

Insulin resistance & Obesity
Insulin resistance
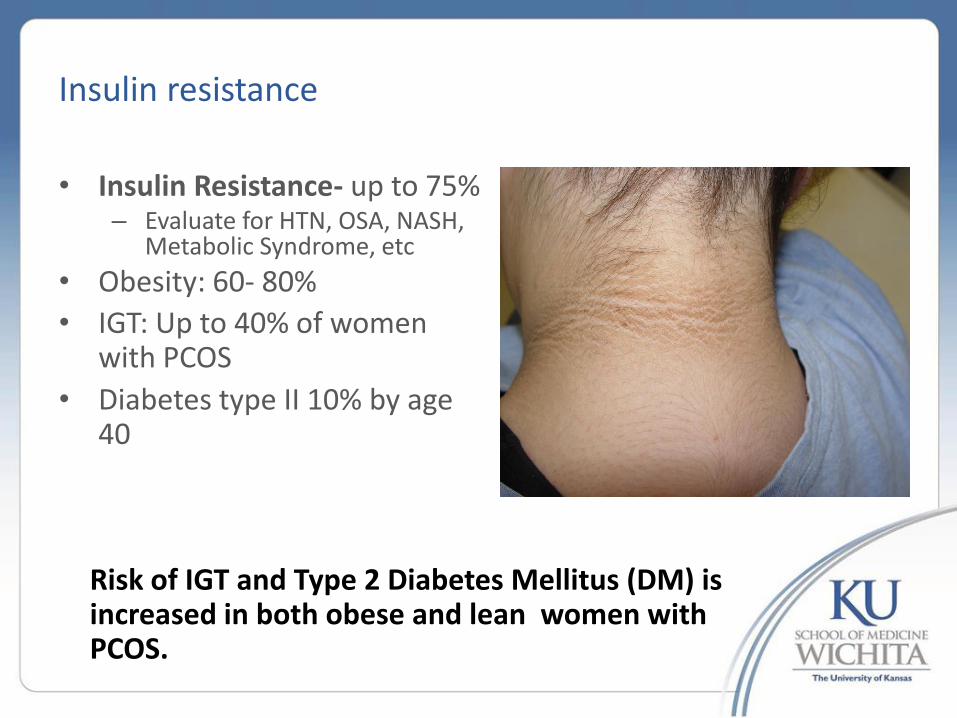
• Insulin Resistance- up to 75% – Evaluate for HTN, OSA, NASH,
Metabolic Syndrome, etc
• Obesity: 60- 80%
• IGT: Up to 40% of women with PCOS
• Diabetes type II 10% by age 40
Risk of IGT and Type 2 Diabetes Mellitus (DM) is increased in both obese and lean women with PCOS.

Rule Out Type 2 Diabetes in PCOS
• The American Diabetes Association recommends screening women with PCOS with either a fasting plasma glucose (FPG) or an oral glucose tolerance test (OGTT) by age 30.
• The oral glucose tolerance test (OGTT) is a more sensitive test for diagnosing diabetes in women with PCOS ( Level A).

Endocr Pract. 2013 Mar 25:1-14


Insulin Resistance / obesity treatment
• Low glycemic index diet
• Exercise: 150 minutes a week
• Metformin
• Thiazolidinediones
• Acarbose: limited by SE

Treatment of Impaired Glucose Tolerance/Type 2 Diabetes
• Current data is insufficient to support the use of insulin-sensitizing agents prophylactically for the prevention of diabetes in women with PCOS without impaired glucose tolerance (IGT).
• Medications, which improve insulin resistance, are the treatment of choice for women with PCOS and diabetes. These include metformin and TZDs
• Improvements in insulin sensitivity, by weight loss or
by the use of insulin-sensitizing agents, may favorably improve many risk factors for diabetes and cardiovascular disease in women with PCOS (Level B).

Glycemic index
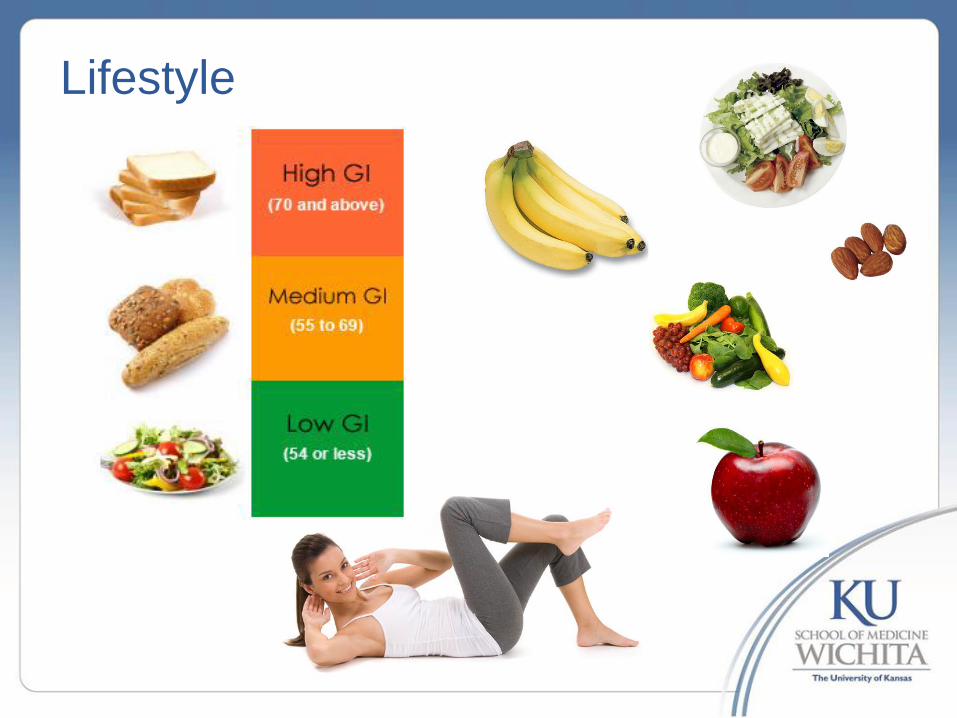
Lifestyle

Clinical Syndromes associated with Insulin Resistance • Type 2 diabetes
• Cardiovascular disease
• Essential hypertension
• Non-alcoholic fatty liver disease (NASH)
• Certain forms of cancer -breast,colon,liver,prostate
• Sleep apnea

PCOS Consequences
Endometrial Hyperplasia
• Chronic anovulation, obesity and hyperinsulinemia are associated with endometrial hyperplasia and endometrial cancer.
• Secondary to prolonged exposure to unopposed estrogen.
• Endometrial cancer risk is 3 times that of general population.

PCOS Consequences
• Dyslipidemias – 70% of women with PCOS will have abnormal lipid panels. – Elevated triglycerides and LDL and low HDL are the most
common abnormalities. – All women with PCOS should be screened with fasting
lipid panel ( Level A).
• Obesity
– 60-80% of women with PCOS are obese. – It is predominantly of the android type with increased hip
to waist ratio (>0.8).

HAIR-AN syndrome

PCOS
Ovarian Metabolic
Anovulation <6 periods/y
Hyperandrogenism PCO Obesity Insulin resistance Dyslipidemia
Clinical findings
Hirsutism Alopecia
Acanthosis Skin tags Large waist Lipodystrophy
Large waist Lipodystrophy
Tests HCG Prolactin FSH TSH Luteal-progesterone
Bioavailable-T DHEA-S 17OH-progesterone
Trans-vaginal Pelvic US Anti-Mullerian Hormone
Fasting glucose & insulin OGTT-insulin HgBA1c
Triglyceride Cholesterol HDL-C
Treatment Provera OCP Metformin
OCP Spironolactone Finastride
Low-carb diet >150 min/wk exercise Metformin Topamax
Weight loss Metformin Acarbose
Fibrates Fish-oil

Conclusion
• PCOS is a heterogeneous disorder with varying diagnostic criteria
• Core criteria are hyperandrogenism, either clinical (i.e. hirsutism) or biochemical (i.e. androgen ), oligomenorrhea reflective of oligo-ovulation, and polycystic ovaries.
• Women with PCOS tend to be insulin resistant, obese, and at risk for diabetes and an adverse cardiovascular risk profile
• Treatment should be early tends to be symptom based, with focused treatments for infertility, obesity, hirsutism.

Thank you













![Genetic Variants Associated with Hyperandrogenemia in ...GeneticsResearchInternational ofessentialgenesforreproductionanddevelopmentsuchas PPAR,HDAC,andNCOR [].Increasedactivityofboth](https://static.fdocuments.in/doc/165x107/60b3fb0e059dce1825647172/genetic-variants-associated-with-hyperandrogenemia-in-geneticsresearchinternational.jpg)




