PBHCI Project Sustainability Analyzing Clinical Workflows to Support Integrated Care and Seamlessly...
17
PBHCI Project Sustainability Analyzing Clinical Workflows to Support Integrated Care and Seamlessly Maximize Revenue 1:00 – 2:00 PM ET 3/15/2012
-
Upload
zachery-hollingshed -
Category
Documents
-
view
213 -
download
0
Transcript of PBHCI Project Sustainability Analyzing Clinical Workflows to Support Integrated Care and Seamlessly...

PBHCI Project Sustainability
Analyzing Clinical Workflows to Support Integrated Care and Seamlessly Maximize
Revenue
1:00 – 2:00 PM ET
3/15/2012
Sustainability
• Administrative/Infrastructure• Clinical• Financial
Sustainability - Financial• Answers the question “How will my organization sustain
the PBHCI efforts at the end of the grant period?”
• Supports implementation of grant expectation
“Funds under this program may not be used to supplant financing of medical services that are eligible for payment or reimbursement from third- party payers (i.e. Medicaid or Medicare).”(Section 2 of RFA)
1
Level 1 Reimbursement Analysis
• Level 1 – Overarching Clinical Workflow Analysis - Does it support best clinical practice while maximizing reimbursement?
Level 1 Financial Required Knowledge
• Services – What are the existing billing codes (HCPCS/CPT) in your state that could be used? What are the relationships between billing requirements, services and diagnosis? E.G. Case Management
• State regulations – What codes are “turned on” and what are the associated state regulations for payment? – Interim Billing Worksheets
• Staff – What licenses and credentials are needed to bill each of the codes? Are you using billable professionals or peers?
• Third-party payer conditions – Can you determine if services are reimbursable by an insurer?
Example of Required Knowledge(Payer is CA Medicaid)
Evaluation and Management (new patient) • CPT Code 99211-99205• Diagnostic code- May be used only with a physical health diagnosis• Billable service• MD, Physician’s Assistant, Advance Practice Nurse
Health and Behavior Assessment • CPT Code 96150• Diagnostic code - secondary to physical health diagnosis• Billable service• Advance practice nurse, psychologist or social worker (different rates?
LINKING WORKFLOW TO BILLING: A CRITICAL STEP FOR SUSTAINABILITY
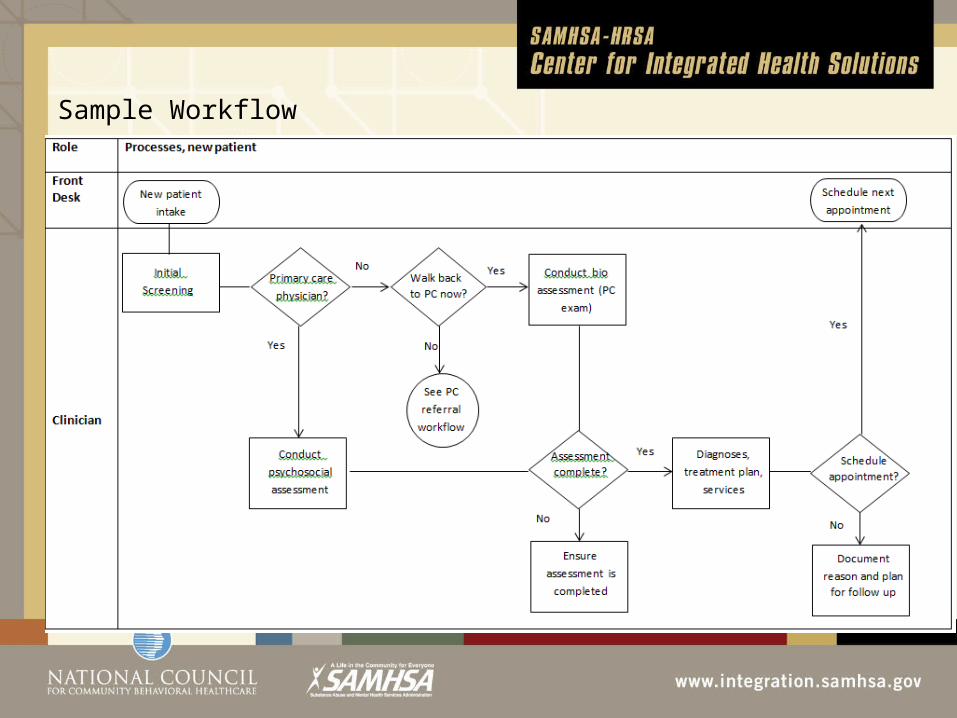
Sample Workflow

Intake and Screening
Intake - Front Desk – Reception generally not reimbursable
Initial Screening/Assessment and/or /Existing Consumer Visit With A Clinician•Is this a billable BH service? •For what credential?•Are you billing for it?•What can you do to make this billable?
• Different clinician credentials• Include billable services (i.e., collecting
vitals for all patients on BH side)
Primary Care Provider DeterminationInitial Screen Decision Point
Critical to Integration of Care
•Can the patient identify their primary care physician?
• If yes, do you have a collaborative relationship?
• Can you exchange patient information (CCD)?
• If no, would they like to see your PC provider?
Connecting with Primary CareMaking sure the connection happens•What is next step? •Is warm handoff billable directly to primary care provider (two services in one day)•When does the Nurse Care Manager get involved? Is a NCM billable?•Is billing in place for PC?
Assessment
n
• Does the assessment include MH, SA and physical health risk tools?
• Does it incorporate non-billable workflows that are currently done separately? (i.e., NOMS data collection)
• Does the clinician license/credential ensure maximum payment?
• Are the initial planned services billable? Can you make them billable?
• If no payers, does the treatment plan include a process for identifying payers?
• Is the treatment plan an integrated plan shared by primary care and behavioral health care?
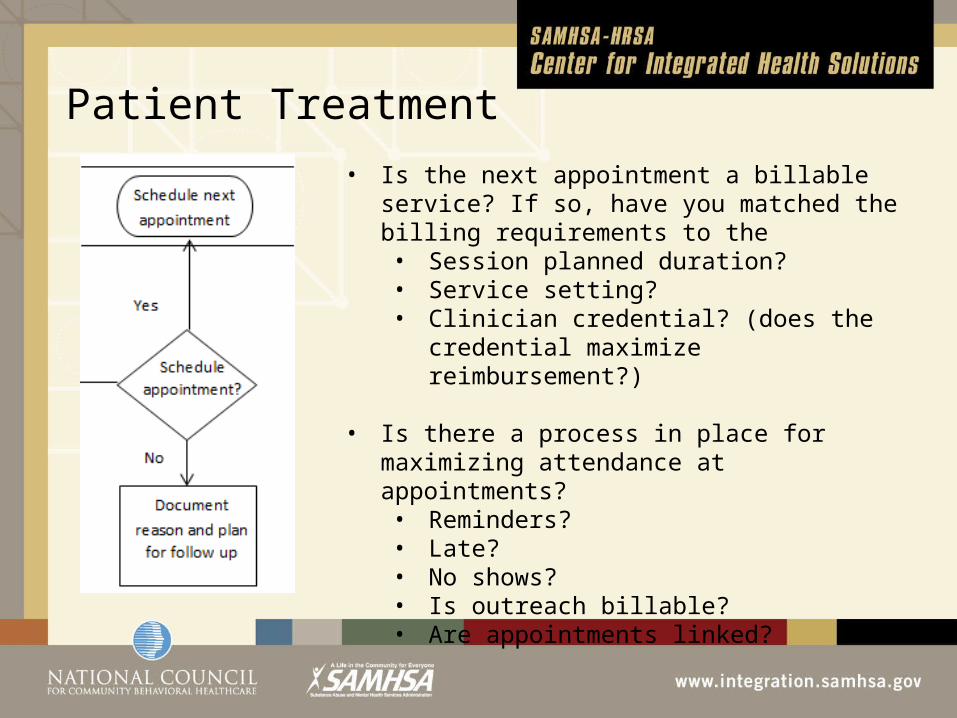
Patient Treatment
,• Is the next appointment a billable service? If so,
have you matched the billing requirements to the • Session planned duration?• Service setting?• Clinician credential? (does the credential
maximize reimbursement?)
• Is there a process in place for maximizing attendance at appointments?• Reminders?• Late?• No shows?• Is outreach billable?• Are appointments linked?
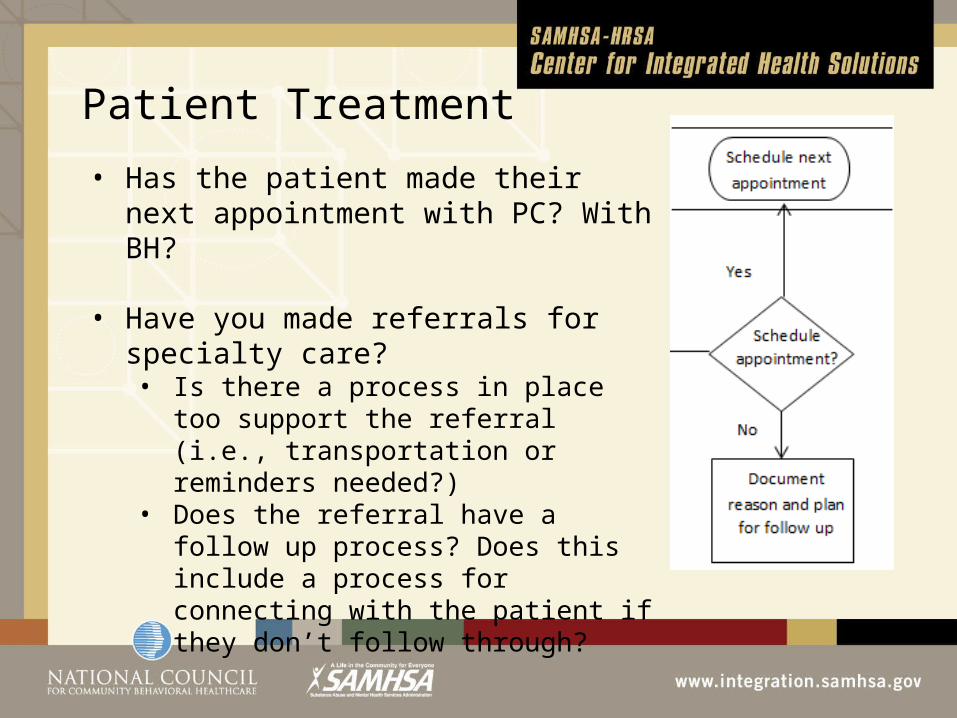
Patient Treatment
• Has the patient made their next appointment with PC? With BH?
• Have you made referrals for specialty care? • Is there a process in place too support
the referral (i.e., transportation or reminders needed?)
• Does the referral have a follow up process? Does this include a process for connecting with the patient if they don’t follow through?
How many patients need to be seen?Question #1
• Do you know how much money your organization needs to make in order to support your integrated care vision? Key elements - number of consumers seen; how often are they seen per year; payer mix; reimbursement per visit
Question #2
• Have you identified the baseline caseloads for both primary care and behavioral health clinicians? (i.e., NP = 750, PC = 1500 at 3 visits per patient per year, 15-20 minute visits)
Question #3
• Are your clinicians seeing enough patients to meet the financial need?
QUESTIONS & PROBLEM SOLVING
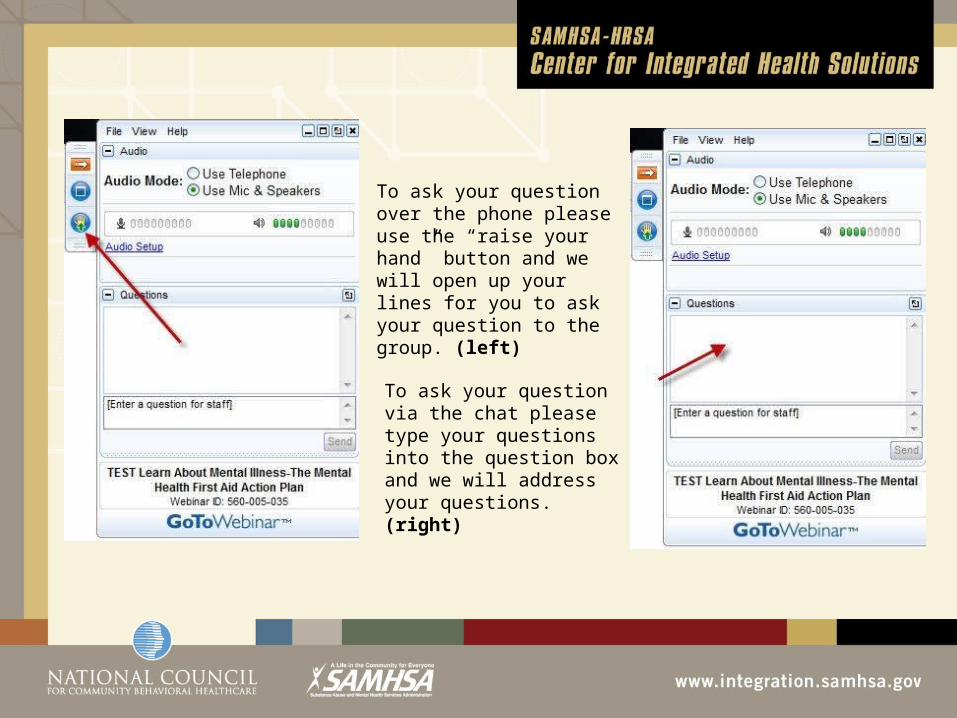
To ask your question over the phone please use the “raise your hand” button and we will open up your lines for you to ask your question to the group. (left)
To ask your question via the chat please type your questions into the question box and we will address your questions. (right)