![Rainy River Headwaters Stressor Identification ReportRainy River Headwaters Stressor Identification Report • [July 2019] Minnesota Pollution Control Agency 1 Executive summary Over](https://static.fdocuments.in/doc/165x107/6016ef6d4d81084af43bbf9a/rainy-river-headwaters-stressor-identification-report-rainy-river-headwaters-stressor.jpg)
PaulT.Ingmundson,PhD … · Criterion)A:)stressor’...
40
Paul T. Ingmundson, PhD South Texas Veterans Health Care System University of Texas Health Science Center at San Antonio Alamo Sleep Disorders Center
Transcript of PaulT.Ingmundson,PhD … · Criterion)A:)stressor’...
Paul T. Ingmundson, PhD South Texas Veterans Health Care System
University of Texas Health Science Center at San Antonio Alamo Sleep Disorders Center
Course Objec,ves 1) Identify changes in sleep that occur after exposure to psychological trauma
2) Identify common sleep disorders that are comorbid with PTSD
3) Discuss ways in which effective treatment of comorbid sleep disorders may facilitate recovery from PTSD

PTSD Through the Past 100 Years

PTSD: A Common Problem

Frequency of PTSD and TBI, Iraq/Afghanistan Veterans, Rand Study
PTSD: Triggered byTrauma

Traumas differ, and Responses to Trauma differ
DSM-‐V Criteria for PTSD Diagnosis Criterion A: Stressor Criterion B: Intrusion Symptoms Criterion C: Avoidance Criterion D: Negative Alterations in cognitions and mood Criterion E: Alterations in Arousal and Reactivity Criterion F: Duration Criterion G: Functional Significance Criterion H: Exclusions Dissociative Features
Criterion A: stressor • The person was exposed to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence, as follows: (one required) • Direct exposure. • Witnessing, in person. • Indirectly, by learning that a close relative or close friend was exposed to trauma. If the event involved actual or threatened death, it must have been violent or accidental. • Repeated or extreme indirect exposure to aversive details of the event(s), usually in the course of professional duties (e.g., first responders, collecting body parts; professionals repeatedly exposed to details of child abuse). This does not include indirect non-‐professional exposure through electronic media, television, movies, or pictures.
Criterion B: intrusion symptoms
• The traumatic event is persistently re-‐experienced in the following way(s): (one required) • Recurrent, involuntary, and intrusive memories. Note: Children older than six may express this symptom in repetitive play. • Traumatic nightmares. Note: Children may have frightening dreams without content related to the trauma(s). • Dissociative reactions (e.g., flashbacks) which may occur on a continuum from brief episodes to complete loss of consciousness. Note: Children may reenact the event in play. • Intense or prolonged distress after exposure to traumatic reminders. • Marked physiologic reactivity after exposure to trauma-‐related stimuli.

Criterion C: avoidance
• Persistent effortful avoidance of distressing trauma-‐related stimuli after the event: (one required) • Trauma-‐related thoughts or feelings. • Trauma-‐related external reminders (e.g., people, places, conversations, activities, objects, or situations).
Criterion D: negaEve alteraEons in cogniEons and mood • Negative alterations in cognitions and mood that began or worsened after the traumatic event: (two required) • Inability to recall key features of the traumatic event (usually dissociative amnesia; not due to head injury, alcohol, or drugs). • Persistent (and often distorted) negative beliefs and expectations about oneself or the world (e.g., "I am bad," "The world is completely dangerous"). • Persistent distorted blame of self or others for causing the traumatic event or for resulting consequences. • Persistent negative trauma-‐related emotions (e.g., fear, horror, anger, guilt, or shame). • Markedly diminished interest in (pre-‐traumatic) significant activities. • Feeling alienated from others (e.g., detachment or estrangement). • Constricted affect: persistent inability to experience positive emotions.
Criterion E: alteraEons in arousal and reacEvity • Trauma-‐related alterations in arousal and reactivity
that began or worsened after the traumatic event: (two required) • Irritable or aggressive behavior • Self-‐destructive or reckless behavior • Hypervigilance • Exaggerated startle response • Problems in concentration
• Sleep disturbance

Dura,on, Func,onal significance, Exclusionary criteria, Dissocia,on
Criterion F: duration Persistence of symptoms (in Criteria B, C, D, and E) for more than one month. Criterion G: functional significance Significant symptom-‐related distress or functional impairment (e.g., social, occupational). Criterion H: exclusion Disturbance is not due to medication, substance use, or other illness. Specify if: With dissociative symptoms. In addition to meeting criteria for diagnosis, an individual experiences high levels of either of the following in reaction to trauma-‐related stimuli: Depersonalization: experience of being an outside observer of or detached from oneself (e.g., feeling as if "this is not happening to me" or one were in a dream). Derealization: experience of unreality, distance, or distortion (e.g., "things are not real").

PTSD and the Comorbidity Matrix
Group 1: low comorbidity: 30% have lifetime major depression (62.1%) Group 2: Substance Dependent, Depressed/Anxi0us, high suicidal ideation (14.1%) Group 3: Depressed/Anxious—high suicidal ideation (23.7%)
Sleep Changes in PTSD: Comorbidi,es
� Insomnia: Insomnia complaints > PTSD symptoms
� Parasomnias: Nightmares vs. REM sleep behavior disorder
� Sleep-‐disordered breathing
Our Sleep Deprived Culture National Sleep Foundation recommends 7-‐9 hours of sleep per night for adults 50.2% of 1249 soldiers and Marines deployed to Afghanistan reported sleeping <= 5 hours/night Average sleep duration for deployed personnel 6. 5 hours2 Sleep disruption has been correlated medical problems, including: • Neurocognitive deficits • Metabolic dysregulation • Obesity • Cardiovascular disease And mental health problems, including: • PTSD • Substance abuse • Suicidal ideation

Sleep problems in PTSD � 91% of Vietnam Veterans with PTSD report sleep problems, compared to 63% of Vietnam Era veterans, and 53% of civilian controls1.
Neylan TC Marmar CR Metzler TJ et al: Sleep disturbances in the Vietnam Generation: findings from a nationally representative sample of male Vietnam veterans. Am J Psychiatry 1998 155 (7) 929-‐33
PTSD and the Comorbidity Matrix
Sleep Problems (95% of PTSD Patients)

Sleep Problems in Deployment � 50.2% of 1249 soldiers and Marines deployed to Afghanistan reported sleeping <= 5 hours/night
� Average sleep duration for deployed personnel 6. 5 hours to 6.7 hours
� Deployed personnel average 6.5 hours sleep. � Postdeployed personnel report more sleep problems. � Trouble sleeping correlated with mental health problems
Peterson AL Goodie JL, Satterfield WA, Brim WL: Sleep disturbance during military deployment. Mil Med 2008; 173 (3): 230-‐5 Seelig AD, Jacobson IG, Stimth B, et al: Sleep patterns before, during and after deployment in Iraq and Afghanistan. Sleep (2010, 33:12) 1615-‐22

Stress, Chronodisrup,on, and PTSD: a Cascade
Stress • Combat Trauma, Sexual Trauma, Disasters
Sleep Disruption
• Circadian Dysrhythmia, Sleep Deficit, Insomnia
Disease
• Metabolic disease, cardiovascular disease • Mental health problems

Environmental and genetic factors are modulated concurrently by the dual actions of the circadian clock and the stress response system, which interact closely to regulate brain function. Conversely, the psychiatric phenotype impacts the circadian clock and the stress response system PTSD
Adapted fromLandgraf, Dominic. 10/2014. Circadian clock and stress interactions in the molecular biology of psychiatric disorders Current psychiatry reports (ISSN: 1523-‐3812), 16 (10), p. 483.

The circadian clock and the stress response system interact closely. During the day BMAL1 and CLOCK proteins are expressed at high levels to activate transcription of PERs, CRYs, RORα, REV-ERBα, and CCGs, as well as to promote the activity of GRs which, in turn, elevate transcription of GC-inducible genes like FKBP5. An accessory feedback loop consists of RORα, an activator of BMAL1 expression and REV-ERBα, an inhibitor of BMAL1 expression. GCs facilitate the expression of GC-responsive clock genes and clock controlled genes (CCGs) with GRE promoter elements. At night, PER and CRY protein levels are high and repress the activity of BMAL1/CLOCK and the GR. Through feedback inhibition, FKBP5 suppresses GR activity. Due to the tight connection between the circadian clock and the stress response system, manipulations of one system naturally lead to changes in the other
Circadian mechanisms and Stress
Independent Variable
Wald Statistic (Wald F)
Significance level (Bonferroni Correction)
Odds ratio (95% CI) (OSA+Insomnia vs OSA-‐Insomnia)*
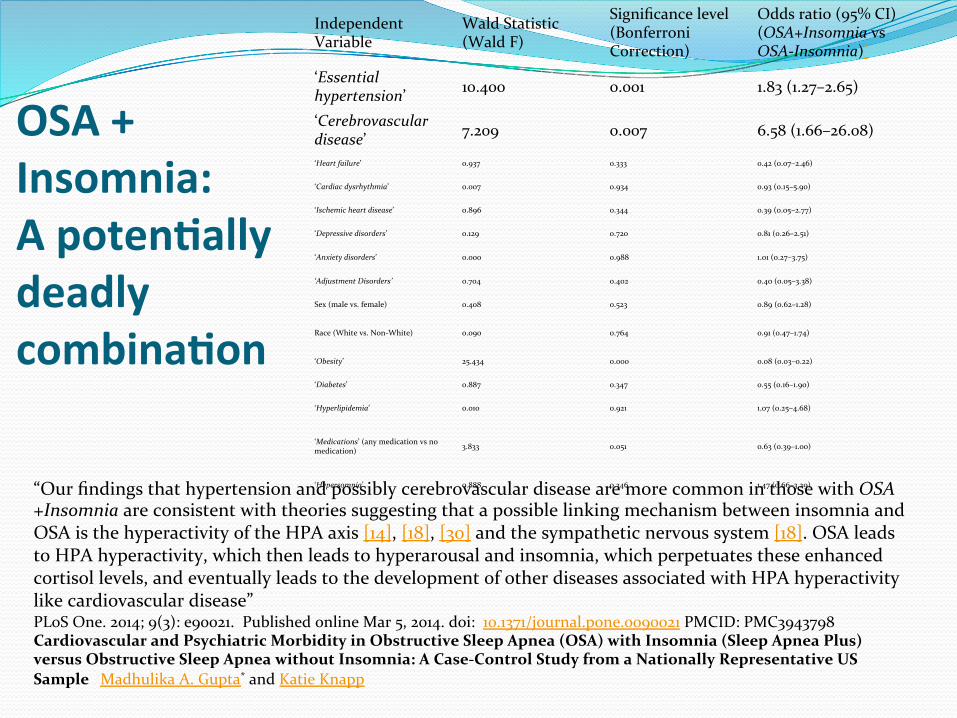
‘Essential hypertension’ 10.400 0.001 1.83 (1.27–2.65)
‘Cerebrovascular disease’ 7.209 0.007 6.58 (1.66–26.08)
‘Heart failure’ 0.937 0.333 0.42 (0.07–2.46)
‘Cardiac dysrhythmia’ 0.007 0.934 0.93 (0.15–5.90)
‘Ischemic heart disease’ 0.896 0.344 0.39 (0.05–2.77)
‘Depressive disorders’ 0.129 0.720 0.81 (0.26–2.51)
‘Anxiety disorders’ 0.000 0.988 1.01 (0.27–3.75)
‘Adjustment Disorders’ 0.704 0.402 0.40 (0.05–3.38)
Sex (male vs. female) 0.408 0.523 0.89 (0.62–1.28)
Race (White vs. Non-‐White) 0.090 0.764 0.91 (0.47–1.74)
‘Obesity’ 25.434 0.000 0.08 (0.03–0.22)
‘Diabetes’ 0.887 0.347 0.55 (0.16–1.90)
‘Hyperlipidemia’ 0.010 0.921 1.07 (0.25–4.68)
‘Medications’ (any medication vs no medication) 3.833 0.051 0.63 (0.39–1.00)
‘Hypersomnia’ 0.888 0.346 1.47 (0.66–3.29) “Our findings that hypertension and possibly cerebrovascular disease are more common in those with OSA+Insomnia are consistent with theories suggesting that a possible linking mechanism between insomnia and OSA is the hyperactivity of the HPA axis [14], [18], [30] and the sympathetic nervous system [18]. OSA leads to HPA hyperactivity, which then leads to hyperarousal and insomnia, which perpetuates these enhanced cortisol levels, and eventually leads to the development of other diseases associated with HPA hyperactivity like cardiovascular disease” PLoS One. 2014; 9(3): e90021. Published online Mar 5, 2014. doi: 10.1371/journal.pone.0090021 PMCID: PMC3943798 Cardiovascular and Psychiatric Morbidity in Obstructive Sleep Apnea (OSA) with Insomnia (Sleep Apnea Plus) versus Obstructive Sleep Apnea without Insomnia: A Case-‐Control Study from a Nationally Representative US Sample Madhulika A. Gupta* and Katie Knapp
OSA + Insomnia: A potenEally deadly combinaEon

Hypermetabolism in brain regions involved in arousal regulaEon, fear responses, and reward processing persist during REM sleep in combat veterans with PTSD.
During wakefulness, veterans with PTSD showed significantly greater relative rCMRglc in a large cluster of 70,326 contiguous voxels (MNI coordinates of voxel of maximal significance: −8, −34, −6; Z = 4.70, pFWE < 0.001), and included the premotor and supplementary motor area, medial superior and inferior frontal gyri, orbitofrontal cortex, gyrus rectus, and pars triangularis. This area also extended bilaterally into the anterior, dorsal, and posterior cingulate cortex, and into the rolandic operculum, supramarginal and angular gyri, temporal gyri, and fusiform and parahippocampal gyri. Limbic structures included in this cluster consisted of the hippocampus, amygdala, and insula, as well of the basal ganglia (putamen, caudate, and pallidum), and thalamus. Parietal regions included the postcentral gyrus, and precuneus, extended into the cuneus and occipital gyri. Finally, this region included brainstem regions involved in arousal and REM sleep regulation, including the midbrain reticular formation, left and right locus coeruleus, raphe nuclei and REM-‐sleep regulating pedunculopontine tegmentum and laterodorsal tegmentum, as well as the cerebellum. Eigenvariate values were extracted from for each veteran and group means were calculated for selected brain regions included in this significant cluster
A Window into the invisible wound of war: Functional neuroimaging of REM sleep in returning combat veterans with PTSD Anne Germain, Jeffrey James, Salvatore Insana, Ryan J. Herringa, Oommen Mammen, Julie Price, Eric Nofzinger Psychiatry Res. 2013 February 28; 211(2): 176–179.

Fig. 1 Relative cerebral glucose metabolism (rCMRglc) associated with eveningness during wakefulness (A) and REM sleep (B) in combat-exposed military veterans with posttraumatic stress symptoms. Sagittal sections correspond to the x -coordinates of the pe...
Brant P. Hasler , Salvatore P. Insana , Jeffrey A. James , Anne Germain
Evening-type military veterans report worse lifetime posttraumatic stress symptoms and greater brainstem activity across wakefulness and REM sleep
Biological Psychology, Volume 94, Issue 2, 2013, 255 - 262
http://dx.doi.org/10.1016/j.biopsycho.2013.06.007
Eveningness was associated with greater lifetime PTSD symptoms, more disturbed sleep, and more frequent and intense nightmares. Eveningness was also associated with greater brain activity in posterior cingulate/precuneus and brainstem regions across wakefulness and REM sleep, overlapping with regions related to arousal and REM sleep generation.
Evening chronotype is associated with more PTSD symptomatology

Date of download: 9/11/2014
Copyright © American Psychiatric Association. All rights reserved.
From: Sleep Disturbances as the Hallmark of PTSD: Where Are We Now?
Am J Psychiatry. 2013;170(4):372-382. doi:10.1176/appi.ajp.2012.12040432
Hypnograms for Two Combat Veterans With and Without PTSDaa Both men served in Operation Iraqi Freedom; one was 25 years old, and the other was 26. Sleep characteristics were determined with polysomnography, and baseline measurements appear on the right. REM sleep periods are denoted by thicker horizontal bars. The asterisk on the left side of each graph denotes the latency between the beginning of the time in bed and the onset of sleep, and it is shorter in the veteran without PTSD. Vertical lines after sleep onset reflect awakenings from sleep. In these examples, the veteran without PTSD shows greater sleep efficiency (total sleep time divided by total time spent in bed) despite also showing more frequent brief nocturnal awakenings and a longer wake time after sleep onset than the veteran with PTSD. The percentage of N3 sleep (stages 3 and 4 in the figure) is rather high in both veterans and is higher in the veteran without PTSD. The percentage of REM sleep is slightly higher in the veteran with PTSD.
Figure Legend:
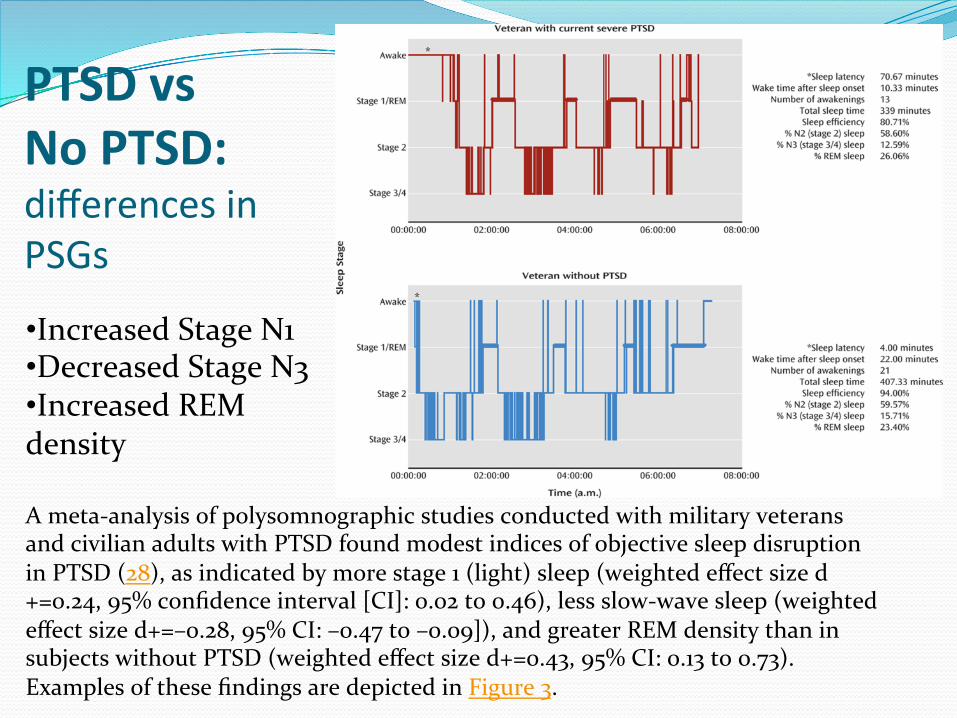
A meta-‐analysis of polysomnographic studies conducted with military veterans and civilian adults with PTSD found modest indices of objective sleep disruption in PTSD (28), as indicated by more stage 1 (light) sleep (weighted effect size d+=0.24, 95% confidence interval [CI]: 0.02 to 0.46), less slow-‐wave sleep (weighted effect size d+=–0.28, 95% CI: –0.47 to –0.09]), and greater REM density than in subjects without PTSD (weighted effect size d+=0.43, 95% CI: 0.13 to 0.73). Examples of these findings are depicted in Figure 3.
PTSD vs No PTSD: differences in PSGs
• Increased Stage N1 • Decreased Stage N3 • Increased REM density

Acute PTSD is associated with fragmented sleep and decreased REM sleep, while REM sleep may be increased in chronic PTSD
“Thus, our findings are consistent with prior literature where reduction or fragmentation of REM sleep has been observed in the acute aftermath of trauma exposure,17,20 and in acutely symptomatic populations within several years of the onset of PTSD,21,22 and the observations of undisrupted or increased REM sleep made in veterans approximately 20 y after combat exposure.25,26 Our new findings and those from the literature are consistent with processes where reactions to trauma among those in whom PTSD develops are suppressive or disruptive to REM sleep, whereas secondary processes over time promote REM sleep.”
Sleep as a predictor of suicidality
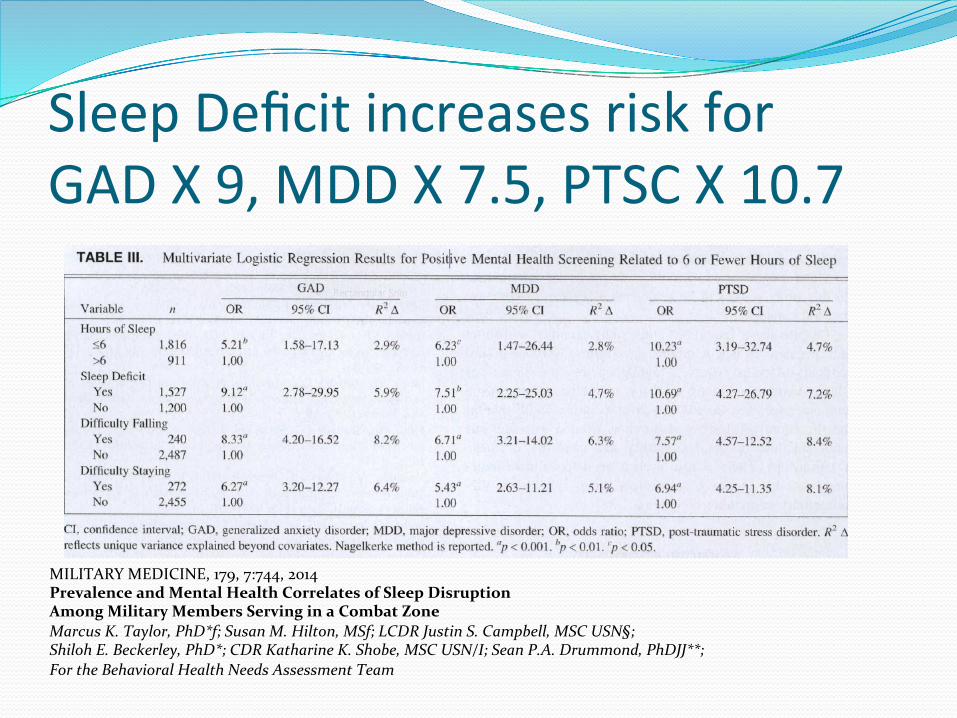
MILITARY MEDICINE, 179, 7:744, 2014 Prevalence and Mental Health Correlates of Sleep Disruption Among Military Members Serving in a Combat Zone Marcus K. Taylor, PhD*f; Susan M. Hilton, MSf; LCDR Justin S. Campbell, MSC USN§; Shiloh E. Beckerley, PhD*; CDR Katharine K. Shobe, MSC USN/I; Sean P.A. Drummond, PhDJJ**; For the Behavioral Health Needs Assessment Team
Sleep Deficit increases risk for GAD X 9, MDD X 7.5, PTSC X 10.7

Nondepressed individuals with insomnia have a two-‐fold increased risk for developing depression

Cumula,ve Incidence of Subsequent Depression Rela,ve to Sleep Complaints in Early Adulthood
Chang PP et al, Am J Epidemiol. 1997;146:105-‐114
Cum
ulative Incide
nce (%
)
Follow-‐Up Time (Years) 0 5 10 15 20 25 30 35 40
5
10
15
20
25
30
35
40
0
Yes No
Insomnia Total Cases
137 23 887 76
P = 0.0005
(n=1,045)
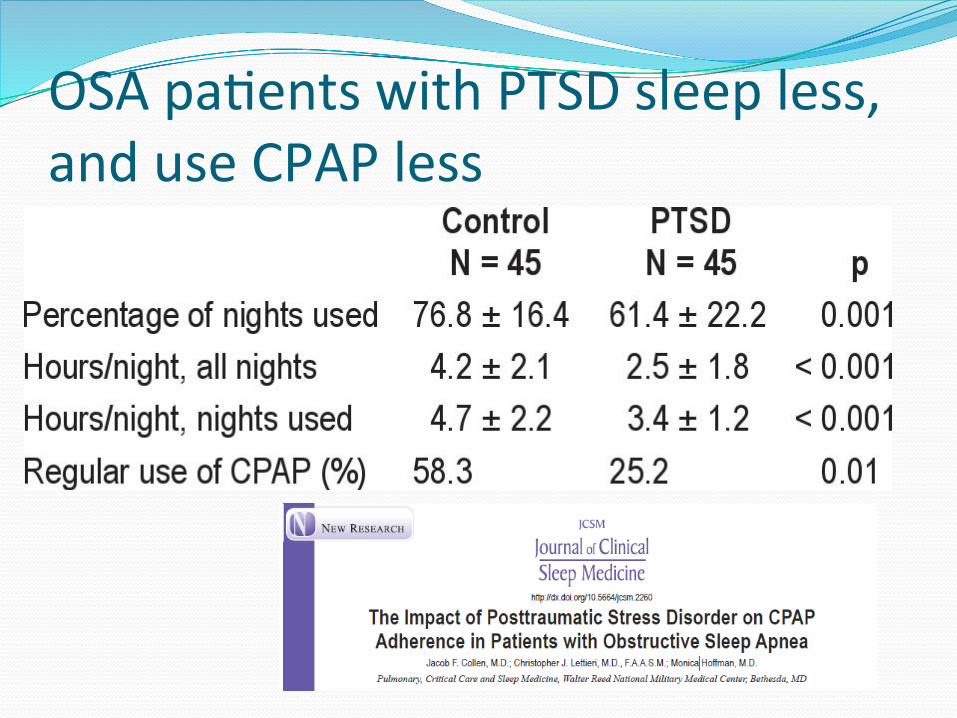
OSA pa,ents with PTSD sleep less, and use CPAP less
Treatments for Comorbid Sleep problems in PTSD
Insomnia: Cognitive Behavioral Treatment of Insomnia (CBT-‐I) Parasomnias: • alpha adrenergic antagonist (prazosin) • Imagery Rehearsal Therapy (IRT)
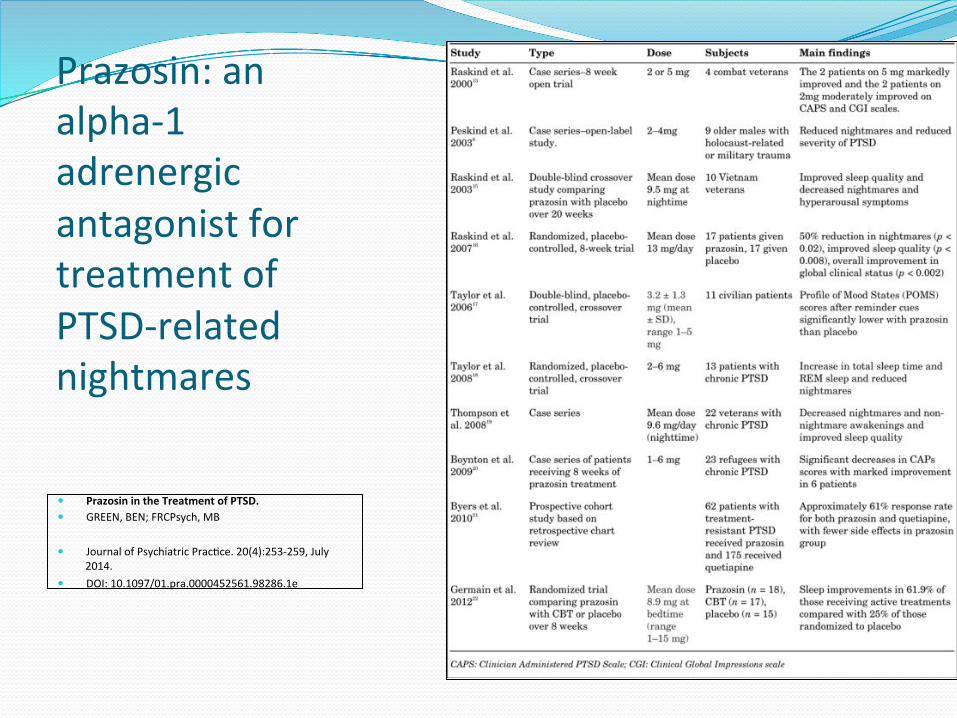
Prazosin: an alpha-‐1 adrenergic antagonist for treatment of PTSD-‐related nightmares
� Prazosin in the Treatment of PTSD. � GREEN, BEN; FRCPsych, MB
� Journal of Psychiatric Prac,ce. 20(4):253-‐259, July 2014.
� DOI: 10.1097/01.pra.0000452561.98286.1e
PTSD and Sleep: Prac,ce Points for Diagnosis
� Safe environment: Attend to patients’ concerns about lab security, preferences concerning technician gender. Hypervigilance, perimeter checking may be associated with procedure interruptions
� Home vs. Lab Testing: Different patients may have different needs/preferences
� Security blankets/transitional objects: Patient requests for service animals/companions, significant others present

PTSD and Sleep: Prac,ce Points for Treatment
� Address the comorbidities! � Insomnia: CBT-‐I first, sedating antidepressants may be appropriate of the patient also has depressive symptoms.
� Insomnia: possible contraindications for benzodiazepines and BDZ agonists
� Nightmares: � Imagery Rehearsal Therapy (IRT) � Prazosin

1. Sleep disturbances often develop into independent, comorbid sleep disorders in adults with PTSD. 2. Sleep disturbances in adults with PTSD contribute to poorer outcomes. These may include mental health consequences, including exacerbation of daytime PTSD symptom severity, anxiety, depression, irritability, impaired cognitive functioning, increased suicidality, and and more functional impairment and disability. Physical health consequences may include obesity, metabolic disturbances, and cardiovascular disease. 3. These adverse outcomes may be ameliorated by with sleep-‐focused treatment. 4. A thorough evaluation of the nature and adverse impacts of sleep disturbances on daytime symptoms and overall functioning should be integral to PTSD evaluation. Assessment and treatment of sleep disturbances need to consider the impact of comorbid PTSD.
Conclusions: Towards an Integrated Treatment of Sleep Disturbances and PTSD
5. Sleep disturbances comorbid to PTSD require targeted interventions. 6. Randomized controlled trials indicate that prazosin can reduce nightmares and insomnia in PTSD. 7. Imagery Rehearsal Therapy (IRT) is established as an effective behavioral interventions for nightmares and may relieve PTSD-‐related sleep disturbances. 8. Other pharmacological interventions such as cyproheptadine, trazodone, zaleplon, and zolpidem may also reduce nightmares and insomnia, but the evidence for efficacy in treating nightmares is weaker, and studies on patients with PTSD are lacking. 9. Behavioral insomnia treatments (CBT-‐I) have received robust empirical support, and may have better long term outcomes compared to pharmacotherapies for insomnia. 10. There is some evidence that treatment of comorbid insomnia may ameliorate symptoms of PTSD.
Towards an Integrated model-‐-‐ConEnued








![Trauma, Stressor-related and Dissociative d.o.s · Title: Microsoft PowerPoint - Trauma, Stressor-related and Dissociative d.o.s [Compatibility Mode] Author: rmillay Created Date:](https://static.fdocuments.in/doc/165x107/5e51864df7dc171e567c7224/trauma-stressor-related-and-dissociative-dos-title-microsoft-powerpoint-trauma.jpg)









