Pattern of ocular manifestations in patients with sarcoidosis in developing countries
4
Introduction Sarcoidosis is a multisystemic, granulo- matous disease of unknown aetiology that may affect any organ system. It is characterized by the accumulation of T lymphocytes and mononuclear phago- cytes with the formation of non-caseat- ing epitheloid granulomas in affected organs (Newman et al. 1997). The aeti- ology of the disease is unknown, although genetic, environmental and infectious agents have been hypothes- ized as triggers (Moller 1997). It commonly affects young and middle- aged adults. On presentation, almost 90% of patients will have an abnormal chest radiograph in the form of infiltrates, although not all may be symptomatic (Neville et al. 1983). The extrapulmonary manifestations of the disease include involvement of the skin, nervous system, eye, heart, liver and a variety of other organs (Baughman 2004). Ocular manifestations of the disease have been reported in 25–50% of patients with histologically proven disease. Ocular inflammation from sarcoidosis may involve the eye, the tissue around the eye or the orbit. Multiple parts of the eye may be involved. Uveitis is the most common ocular manifestation and is potentially vision-threatening (Bradley et al. 2002). The incidence of ocular sarcoidosis (OS) in industrialized countries has been found to vary, with higher rates reported in London and New York (27% and 20%, respectively) than in France and Eastern Europe (11% and 4%, respectively) (James et al. 1976; James & Hosoda 1994). Even the pat- tern of disease has been found to vary, with anterior uveitis predomin- ant in some races and posterior uveitis in others (Hunter & Foster 1994). Sarcoidosis was hitherto thought to be uncommon in developing countries, but, with the availability of transbron- chial lung biopsy and increasing Pattern of ocular manifestations in patients with sarcoidosis in developing countries Aman Khanna, 1 Updesh Sidhu, 2 Gurkirat Bajwa 1 and Vineeta Malhotra 3 1 Department of Ophthalmology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India 2 Department of Respiratory Medicine, Dayanand Medical College and Hospital, Ludhiana, Punjab, India 3 Department of Pathology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India ABSTRACT. Purpose: Sarcoidosis is increasingly diagnosed in developing countries, although it was earlier thought to be uncommon. We describe the pattern of ocular manifestations in sarcoidosis in India. Methods: A total of 48 consecutive patients with histologically confirmed sar- coidosis, referred to a teaching university hospital, underwent a detailed oph- thalmological examination, irrespective of whether they had eye symptoms or not. Results: Ocular involvement was seen in 14 (29%) patients. The mean age at presentation was 50 years, and neither two peaks of incidence nor a female preponderance could be demonstrated. The majority of patients had chronic disease. Posterior uveitis was distinctly more common (12 ⁄ 14) than anterior (5 ⁄ 14) uveitis. Conjunctival involvement was uncommon. These findings differ from those reported in the Western literature. Conclusions: Eye involvement is common in sarcoidosis in India and may occur without ocular symptoms. Posterior segment involvement is more com- mon than has been reported. Ophthalmologists need to be aware of ocular involvement in this disease as untreated disease can have significant visual con- sequences. Key words: sarcoidosis – ocular sarcoidosis – uveitis – developing countries – granuloma Acta Ophthalmol. Scand. 2007: 85: 609–612 ª 2007 The Authors Journal compilation ª 2007 Acta Ophthalmol Scand doi: 10.1111/j.1600-0420.2006.00791.x Acta Ophthalmologica Scandinavica 2007 609
-
Upload
aman-khanna -
Category
Documents
-
view
215 -
download
0
Transcript of Pattern of ocular manifestations in patients with sarcoidosis in developing countries

Introduction
Sarcoidosis is a multisystemic, granulo-matous disease of unknown aetiologythat may affect any organ system. It ischaracterized by the accumulation of Tlymphocytes and mononuclear phago-
cytes with the formation of non-caseat-ing epitheloid granulomas in affectedorgans (Newman et al. 1997). The aeti-ology of the disease is unknown,although genetic, environmental andinfectious agents have been hypothes-ized as triggers (Moller 1997). It
commonly affects young and middle-aged adults. On presentation, almost90% of patients will have an abnormalchest radiograph in the form ofinfiltrates, although not all may besymptomatic (Neville et al. 1983). Theextrapulmonary manifestations of thedisease include involvement of the skin,nervous system, eye, heart, liver and avariety of other organs (Baughman2004). Ocular manifestations of thedisease have been reported in 25–50%of patients with histologically provendisease. Ocular inflammation fromsarcoidosis may involve the eye, thetissue around the eye or the orbit.Multiple parts of the eye may beinvolved. Uveitis is the most commonocular manifestation and is potentiallyvision-threatening (Bradley et al. 2002).
The incidence of ocular sarcoidosis(OS) in industrialized countries hasbeen found to vary, with higher ratesreported in London and New York(27% and 20%, respectively) than inFrance and Eastern Europe (11% and4%, respectively) (James et al. 1976;James & Hosoda 1994). Even the pat-tern of disease has been found tovary, with anterior uveitis predomin-ant in some races and posterior uveitisin others (Hunter & Foster 1994).Sarcoidosis was hitherto thought tobe uncommon in developing countries,but, with the availability of transbron-chial lung biopsy and increasing
Pattern of ocular manifestationsin patients with sarcoidosis indeveloping countries
Aman Khanna,1 Updesh Sidhu,2 Gurkirat Bajwa1 and VineetaMalhotra3
1Department of Ophthalmology, Dayanand Medical College and Hospital,Ludhiana, Punjab, India2Department of Respiratory Medicine, Dayanand Medical College and Hospital,Ludhiana, Punjab, India3Department of Pathology, Dayanand Medical College and Hospital, Ludhiana,
Punjab, India
ABSTRACT.
Purpose: Sarcoidosis is increasingly diagnosed in developing countries,
although it was earlier thought to be uncommon. We describe the pattern of
ocular manifestations in sarcoidosis in India.
Methods: A total of 48 consecutive patients with histologically confirmed sar-
coidosis, referred to a teaching university hospital, underwent a detailed oph-
thalmological examination, irrespective of whether they had eye symptoms or
not.
Results: Ocular involvement was seen in 14 (29%) patients. The mean age at
presentation was 50 years, and neither two peaks of incidence nor a female
preponderance could be demonstrated. The majority of patients had chronic
disease. Posterior uveitis was distinctly more common (12 ⁄14) than anterior
(5 ⁄14) uveitis. Conjunctival involvement was uncommon. These findings differ
from those reported in the Western literature.
Conclusions: Eye involvement is common in sarcoidosis in India and may
occur without ocular symptoms. Posterior segment involvement is more com-
mon than has been reported. Ophthalmologists need to be aware of ocular
involvement in this disease as untreated disease can have significant visual con-
sequences.
Key words: sarcoidosis – ocular sarcoidosis – uveitis – developing countries – granuloma
Acta Ophthalmol. Scand. 2007: 85: 609–612ª 2007 The Authors
Journal compilation ª 2007 Acta Ophthalmol Scand
doi: 10.1111/j.1600-0420.2006.00791.x
Acta Ophthalmologica Scandinavica 2007
609

physician awareness, it is being diag-nosed more frequently. Epidemiologi-cal features in developing countriesthat differ from those in Westernindustrialized countries include age,sex, mode of presentation and coursein systemic sarcoidosis (Gupta &Gupta 1990). The disease is stillconfused with tuberculosis and isoften treated as such. Data fromdeveloping countries on the patternof ocular involvement are sparse. Westudied the pattern of ocular diseaseand tried to establish whether therewere any significant differencesfrom that reported in the Westernliterature.
Materials and Methods
Study design
Between June 1998 and June 2001, allpatients referred to the OphthalmologyDepartment at Dayanand MedicalCollege and Hospital with a confirmeddiagnosis of sarcoidosis were includedin the study. A total of 48 patientswere included. Of these, the recordsfor 12 patients were studied retrospec-tively and 36 patients were examinedprospectively. The study was approvedby the institutional review board andethics committee.
Diagnosis of sarcoidosis
The criteria for diagnosis of sarcoido-sis were derived from the descriptionof sarcoidosis proposed by the Sev-enth International Conference on Sar-coidosis and Other GranulomatousDisorders (Yamamoto et al. 1992).Specifically, it required the presence ofappropriate clinico-radiological fea-tures with the histopathologicaldemonstration of non-caseating epi-theloid cell granulomas with a negat-ive stain for acid fast bacilli in atransbronchial lung biopsy sample.Cases were excluded from the study ifthe diagnosis of sarcoidosis was ques-tionable or a causal agent was foundto be associated with the granuloma-tous inflammation.
Ophthalmological evaluation
Near and distance visual acuity wereassessed using standard Snellen andJaeger charts. Anterior segment exam-ination was performed with torchlightand the slit-lamp. All patients were
screened for evidence of keratocon-junctivitis sicca by Schirmer’s tear testusing standardized methodology andwithout local anaesthesia. More than10 mm moistening on the filter paperwas taken as normal. Intraocularpressure was recorded with a Gold-mann applanation tonometer. Fundusexamination was performed usingboth direct and indirect ophthalmos-copy after dilating both pupils withtropicamide and phenylephrine. Theposterior pole was further evaluatedby slit-lamp biomicroscopy using a+90 D lens. Fundus fluorescein angi-ography was performed in selectedpatients who manifested fovealinvolvement.
Results
A total of 48 patients were enrolled.They included 23 (48%) men and 25(52%) women. The mean age at pres-entation was 46 years (range 27–68 years). Male patients were on aver-age younger than females (44 versus
47 years). Most of the patients werein the 41–50-year age group.
Ocular involvement attributable tosarcoidosis was diagnosed in 14patients (29%; seven men and sevenwomen). The mean age of patientswith ocular sarcoidosis was 50 years(range 33–65 years). Men were onaverage older than women (56 versus43 years). The maximum number ofpatients presenting with ocular sarcoi-dosis were in the 41–50-year age group(Table 1). Twelve patients were symp-tomatic; 10 had blurring of vision, onehad redness of the eye ⁄photophobiaand one had dryness of the eye.
The manifestations of OS in thepatients included in our study werevaried and included almost all partsof the eye. The anterior segment wasinvolved in five (36%) patients withOS. Chronic granulomatous uveitis,exemplified clinically by mutton-fatkeratic precipitates, iris nodules andsynechiae, was the most commonanterior segment manifestation, occur-ring in four (29%) cases. Acute irido-cyclitis characterized by ciliaryinjection, aqueous cells and flare andfine keratic precipitates, but withoutevidence of chronic inflammation, wasnoted in one (7%) case. One (7%)case showed conjunctival involvementin the form of a solitary conjunctivalnodule, which on biopsy showed non-caseating granulomatous inflamma-tion, suggestive of sarcoidosis.
Orbital involvement was seen in one(7%) case, in the form of lacrimalgland involvement as demonstratedby decreased tear production onSchirmer’s test.
Table 1. Age and sex distribution of patients
with ocular sarcoidosis (n ¼ 14).
Age
(years)
Men
(n ¼ 7)
Women
(n ¼ 7)
Total
(n ¼ 14) (%)
0–30 0 0 0
31–40 0 3 3 (21)
41–50 2 4 6 (43)
51–60 4 0 4 (29)
61–70 1 0 1 (7)
Total 7 7 14 (100)
Mean age
(Age range)
56
(33–50)
43
(50–65)
50
(33–65)
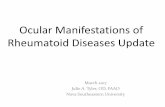
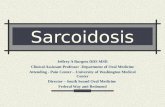
Fig. 1. Snowball opacities in a 60-year-old woman.
Acta Ophthalmologica Scandinavica 2007
610

Posterior segment involvement wasobserved in 12 (86%) cases with OS.The vitreous was the most commonposterior structure involved. It wasaffected in 11 (79%) cases with OS.Cellular reaction ranged from min-imal, with a few vitreous cells orclumps of cells signifying intermediateuveitis in seven (50%) cases, to densevitreous opacities or vitreous snow-balls (Fig. 1) along with snowbankingin four (29%) cases.
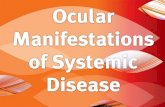
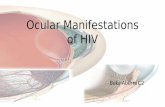
Choroidal involvement was seen innine (64%) patients with OS. Smallmultiple granulomas characterized thedisease manifestation in the choroids(Fig. 2). The retina was involved insix (43%) cases with OS. Retinalinvolvement consisted of anterior andmid-peripheral retinal phlebitis withexudation in six (43%) cases. None ofthe cases showed any evidence of ret-inal or choroidal neovascularization.
Macular involvement in the form ofcystoid macular oedema was seen inone (7%) case. The same case (7%)had optic nerve involvement manifes-ted by oedema of the optic nerve head.
In nine (64%) of 14 patients withOS, the posterior segment, but not theanterior segment, was affected. In theremaining three (21%) cases, com-bined anterior and posterior segmentinvolvement was seen. Involvement ofthe anterior segment alone, withoutposterior segment involvement, wasseen in only two (14%) of 14 cases.The anatomical localization of ocularsarcoidosis is shown in Table 2.
Discussion
Sarcoidosis is now seen in parts ofIndia and other developing countriesalmost as frequently as in Westernindustrialized countries (Jindal et al.2000). In our series of 48 patients withsarcoidosis, the incidence of ocularinvolvement was 29%. Earlier studiesof sarcoidosis from the Indian subcon-tinent showed ocular involvementvarying from 8% to 16%, with onestudy showing an incidence of 40%,although none of these studies evalu-ated eye findings in detail, as ours did(Sharma & Mohan 2002). The meanage of involvement in our patientswas 50 years. This is by contrast withreports from Western industrializedcountries, where the incidence of OSshows two peaks, one at 20–30 yearsand another at 50–60 years (Rothovaet al. 1989). Most patients were 40–60 years old, and none was below30 years of age, which reflects a higherage distribution than in the West.
Colder climates may favour youngerpresentation and female preponder-ance (Yamaguchi et al. 1989). Themean age of female patients present-ing with OS was lower than that ofmales. A similar trend was seen in theACCESS (A Case-Control EtiologicStudy of Sarcoidosis) trial, whichshowed OS to be more common infemales under 40 years of age andmales over 40 years of age (Baughmanet al. 2001). Ocular involvement wasseen equally among both sexes, unlikein the Western literature, wherefemales show a preponderance of thedisease (James 1986).
The most common ocular findingsreported in Western industrializedcountries are uveitis (30–70%) andconjunctival nodules (40%) (Jabs &John 1986; Hunter & Foster 1994). Inour series, uveitis was also the mostcommon finding and was seen in allpatients, but conjunctival involvementwas found in only one subject. Anterioruveitis is a very common manifestationof OS that occurs in 22–70% ofpatients, especially in Africans(Obenauf et al. 1978). Among Whitepatients, especially elderly women,posterior uveitis tends to be common(Rothova 2000). A German studyreported an incidence of posterior uvei-tis of 60% (Hassenstein et al. 2003).
The most striking feature of ourstudy was the high incidence of poster-ior uveitis. Various studies reportedearlier have shown a preponderanceof anterior over posterior uveitis(Rothova et al. 1992). Cystoid macularoedema was seen in only one patient. Ithas been reported to occur in 19)72%of patients with OS in Western indus-trialized countries (Rothova et al.1998). Lacrimal gland involvement wasseen in only one patient. It is notewor-thy that two patients had asympto-matic ocular involvement. Despite thehigh frequency of eye involvement insarcoidosis, patients do not undergoroutine eye examination. One studyfound that only 44% patients hadundergone documented eye examina-tions, with half of them having signsand symptoms of ocular involvement(Dresner et al. 1986).
The major strength of our study isthat it highlights the fact that ocularmanifestations of sarcoidosis are com-mon in this part of the world, witheye involvement being demonstratedin almost one-third of patients. In
Fig. 2. Choroidal granulomas in a 48-year-old man.
Table 2. Anatomical localization of ocular
sarcoidosis.
Ocular structure
Cases
n (%)
Lids and orbit 1 (7)
Conjunctiva 1 (7)
Cornea 0
Sclera 0
Iris and ciliary body 5 (36)
Lens 0
Choroid 9 (64)
Vitreous 11 (79)
Cells 7
Snowballs 4
Retina 6 (43)
Cystoid macular oedema 1 (7)
Optic nerve 1 (7)
Acta Ophthalmologica Scandinavica 2007
611

developing countries, a substantialportion of these patients are treatedfor tuberculosis, with potentially dis-astrous visual consequences and expo-sure to the toxicity of antituberculardrugs. We hope this study will gener-ate awareness about the diseaseamongst ophthalmologists in this partof the world. Our study does have thelimitation that only patients referredto the eye department of a teachinghospital were included in the data.Data derived from such a databasecould have introduced a selection biasas not all patients are privilegedenough to come to a tertiary care hos-pital in a developing country such asIndia. Therefore, we admit that directconclusions on the incidence of ocularsarcoidosis cannot be drawn from ourstudy. In addition, we studied ourpatients at one time-point only andsome patients may have developedsigns of ocular disease later.
In conclusion, our study demonstra-ted significant eye involvement in sar-coidosis patients and differingepidemiological features from earlierseries conducted in Western industrial-ized countries. Severe visual loss wasuncommon, probably because of lessermacular involvement. Diagnosis of thedisease in the eye is not difficult but itrequires an index of awareness and acomprehensive eye examination. Sar-coid patients benefit from an interdis-ciplinary evaluation at periodicintervals. Our study highlights the sig-nificant incidence of posterior segmentinvolvement and the consequent bene-fit to patients of indirect ophthalmos-copy after pupillary dilatation, ratherthan the anterior segment examinationwith a slit-lamp that is common prac-tice in developing countries.
References
Baughman RP (2004): Pulmonary sarcoidosis.
Clin Chest Med 25: 521–530.
Baughman RP, Teirstein AS, Judson MA
et al. (2001): Clinical characteristics of pati-
ents in a case-control study of sarcoidosis.
Am J Respir Crit Care Med 164: 1885–1889.
Bradley D, Baughman RP, Raymond L &
Kaufman AH (2002): Ocular manifesta-
tions of sarcoidosis. Semin Respir Crit
Care Med 23: 543–548.
Dresner MS, Brecher R & Henkind P (1986):
Ophthalmology consultation in the diagno-
sis and treatment of sarcoidosis. Arch
Intern Med 146: 301–304.
Gupta SK & Gupta S (1990): Sarcoidosis in
India: a review of 125 biopsy proven cases
from eastern India. Sarcoidosis 7: 43–49.
Hassenstein A, Bialasiewicz AA, Knospe V &
Richard G (2003): Incidence of ocular
manifestations in patients with histologi-
cally confirmed systemic sarcoidosis. Klin
Monatsbl Augenheilkd 220: 414–417.
Hunter DG & Foster CS (1994): Ocular man-
ifestations of sarcoidosis. In: Albert DM &
Jakobiec FA (eds). Principles and Practice
of Ophthalmology. Philadelphia: WB Saun-
ders 443–450.
Jabs DA & Johns CJ (1986): Ocular involve-
ment in chronic sarcoidosis. Am J Ophthal-
mol 102: 297–301.
James DG (1986): Ocular sarcoidosis. Ann N
Y Acad Sci 465: 551–563.
James DG & Hosoda Y (1994): Epidemiol-
ogy. In: James DG (ed). Sarcoidosis and
other Granulomatous Diseases. Los
Angeles: Marcel Dekker 729–743.
James DG, Neville E & Siltzbach E (1976): A
worldwide review of sarcoidosis. Ann N Y
Acad Sci 278: 321–334.
Jindal SK, Gupta D & Aggarwal AN (2000):
Sarcoidosis in developing countries. Curr
Opin Pulm Med 6: 448–454.
Moller DR (1997): Aetiology of sarcoidosis.
Clin Chest Med 18: 695–706.
Neville E, Walker AN & James DG (1983):
Prognostic factors predicting the outcome
of sarcoidosis: an analysis of 818 patients.
Q J Med 52: 525–533.
Newman LS, Rose CS & Maier LA (1997):
Sarcoidosis. N Engl J Med 336: 1224–1234.
Obenauf CD, Shaw HE, Sydnor CF & Klint-
worth GK (1978): Sarcoidosis and its
ophthalmic manifestations. Am J Ophthal-
mol 86: 648–655.
Rothova A (1998): Posterior segment involve-
ment in ocular sarcoidosis. In: Ohno S,
Aoki K, Usui M & Uchio E (eds). Uveitis
Today. Amsterdam: Elsevier 207–210.
Rothova A (2000): Ocular involvement in
sarcoidosis. Br J Ophthalmol 84: 110–116.
Rothova A, Alberts C, Glarius E, Kijlstra A,
Buitenhuis HJ & Breebaart AC (1989):
Risk factors for ocular sarcoidosis. Doc
Ophthalmol 72: 287–296.
Rothova A, Buitenhuis HJ, Meenken C,
Brinkman CJ, Linssen A, Alberts C,
Luyendijk L & Kijlstra A (1992): Uveitis
and systemic disease. Br J Ophthalmol 76:
137–141.
Sharma SK & Mohan A (2002): Sarcoidosis:
global scenario and Indian perspective.
Indian J Med Res 116: 221–247.
Yamaguchi M, Hosoda Y, Sasaki R et al.
(1989): Epidemiological study on sarcoido-
sis in Japan: recent trends in incidence and
prevalence rates and changes in epidemio-
logical features. Sarcoidosis 6: 138–146.
Yamamoto M, Sharma OP & Hosoda Y
(1992): The 1991 descriptive definition of
sarcoidosis. Sarcoidosis 9: 33–34.
Received on November 24th, 2005.
Accepted on July 13th, 2006.
Correspondence:
Dr Gurkirat Bajwa
Professor of Ophthalmology
220 A, Sarabha Nagar
Ludhiana 141 001
Punjab
India
Tel: + 91 98726 11441
Fax: + 91 161 230 2620
Email: [email protected],
Acta Ophthalmologica Scandinavica 2007
612