Patricia Nez Henderson, MD,...
32
Patricia Nez Henderson, MD, MPH Black Hills Center for American Indian Health Rapid City, South Dakota
Transcript of Patricia Nez Henderson, MD,...

Patricia Nez Henderson, MD, MPH Black Hills Center for American Indian Health
Rapid City, South Dakota

Disclosure Disclosed no conflict of interest

OBJECTIVE
Discuss how policies can address inequities in prevention, diagnosis and treatment of people living with diabetes in Indian Country

• 2.2 times higher— Likelihood of American Indians and Alaska Natives to have diabetes compared with non-Hispanic whites
• 68%— Percent increase in diabetes from 1994 to 2004 in American Indian and Alaska Native youth aged 15-19 years
• 30% — Estimated percent of American Indians and Alaska Natives who have pre-diabetes
Source: American Diabetes Association
DIABETES IN INDIAN COUNTRY

0
5
10
15
20 Pe
rcen
t
Year
AIAN
US
Source: IHS Program Statistics and National Diabetes Surveillance System. Age-adjusted to the 2000 US standard population with the exception of 1981–1993 data for AIAN, which was age-adjusted to the 1980 US standard population.
Prevalence of Diagnosed Diabetes AIANs compared to U.S. population: 1980-2004
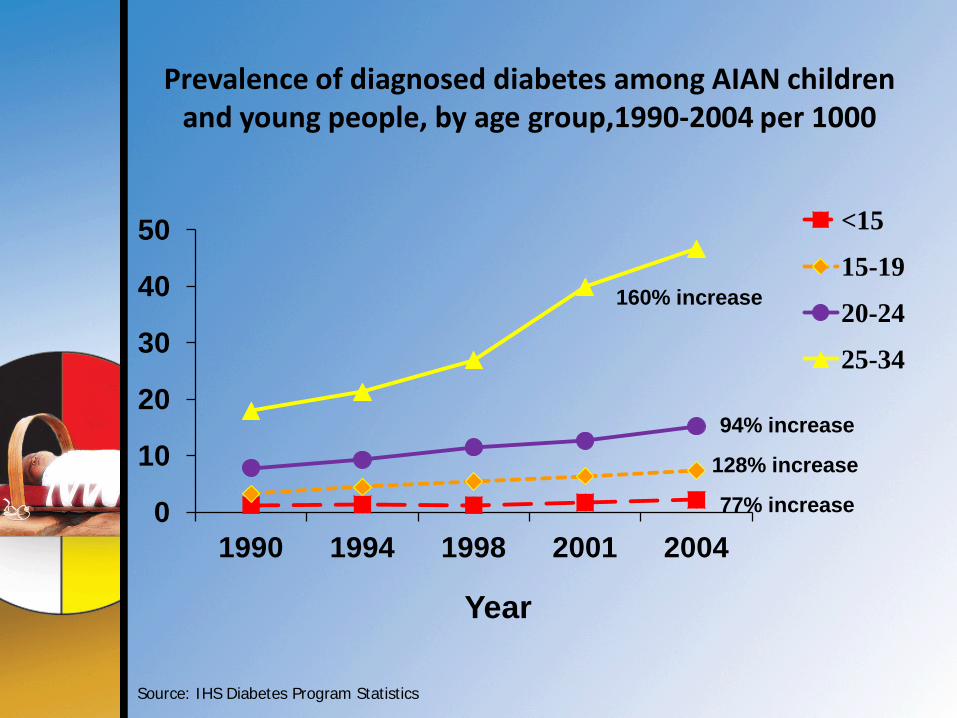
Prevalence of diagnosed diabetes among AIAN children and young people, by age group,1990-2004 per 1000
0
10
20
30
40
50
1990 1994 1998 2001 2004
<15
15-19
20-24
25-34
Source: IHS Diabetes Program Statistics
Year
160% increase
94% increase
128% increase
77% increase

Age-Adjusted Prevalence of Obesity and Diagnosed Diabetes Among U.S. Adults Aged
18 Years or older Obesity (BMI ≥30 kg/m2)
Diabetes
1994
1994
2000
2000
No Data <14.0% 14.0-17.9% 18.0-21.9% 22.0-25.9% >26.0%
No Data <4.5% 4.5-5.9% 6.0-7.4% 7.5-8.9% >9.0%
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
2010
2010

Risk Factors Having prediabetes
Being 45 or older
Having a family history of diabetes
Being overweight
Not exercising regularly
Having high blood pressure
Having low HDL, also known as "good”
cholesterol and/or high levels of triglycerides
Certain racial and ethnic groups
Women who had gestational diabetes

ENVIRONMENT

ENVIRONMENT

ENVIRONMENT

Special Diabetes Program for Indians (SDPI)
Congress established SDPI through the Balanced Budget Act of 1997.
SDPI provides grants for diabetes treatment and prevention services to 404 IHS, Tribal, and Urban Indian health programs.
Focused on reducing risk of diabetes in high risk individuals.
$30 million per (1998-2002)
$150 million per (2012-2013)
http://www.ihs.gov/MedicalPrograms/Diabetes/HomeDocs/Resources/FactSheets/2012/Fact_Sheet_SuccessInterv_508c.pdf

Increase Access to Diabetes Treatment and Prevention Services
1997* 2010 Diabetes clinics 31% 71% Diabetes clinical teams 30% 94% Diabetes patient registries 34% 94% Nutrition services for adults 39% 89% Access to registered dietitians 37% 77% Culturally tailored diabetes education programs 36% 99% Access to physical activity specialists 8% 74% Adult weight management programs 19% 76%
http://www.ihs.gov/MedicalPrograms/Diabetes/HomeDocs/Resources/FactSheets/2012/Fact_Sheet_SuccessInterv_508c.pdf

Few tribes have passed policies for breastfeeding at workplaces and public places.
Navajo Nation Council tabled a legislation that would have increased excise taxes on junk food.
Tribes have passed tobacco-free policies throughout the country BUT most casinos are exempted.
Some tribes have passed wellness policies to give their employees an hour plus for exercise during lunch time.
TRIBAL POLICY EFFORTS

TRIBAL POLICY EFFORTS

TRIBAL POLICY EFFORTS Facebook Friend’s Views • Smoke-free policies • Banning > 24 oz soda drinks and
limit 12 packs of soda at grocery store
• Policy for breastfeeding • Increasing taxes on junk food • Health food/snack in work
sponsored meetings and tribal sponsored events
• No more fry bread policy • Work wellness policy • Share –use policies that allow
school or church properties for physical activities for communities.

TRIBAL POLICY EFFORTS

STEPS TO INTRODUCING POLICY Documenting the problem
Needs assessment Educate, Educate, Educate
Educate yourself –become the expert Educate the Community, Tribal Leaders
Media, presentations, surveys, polls, readiness assessment Build Coalition Passing Policies
Learn how local laws are passed Build your core team Find your “champion” Take head count of elected officials early and often Keep an eye on the opposition If you don’t have the votes, stop and regroup and EDUCATE

TEAM Navajo

Bilagáana bi’ Na’toh ba’át’e’ hóló

• Promoting Community Tobacco free events • Pow-wows • Rodeos • Ceremonial gatherings • Walks/Runs
• Radio shows • Billboards • Newspapers/Radio Ads • Art Contest
Towards A Healthier Navajo Nation

91% of the Navajo Nation Supports a “Commercial Tobacco-free Nation" in all work places and public places with no exemptions. How Do Our ELECTED Leaders Reflect our Views When It Counts?
Towards A Healthier Navajo Nation



TRIBAL POLICY EFFORTS
Bates number 2072277904

The Navajo Nation Commercial Tobacco Free Act 2008
The Navajo Nation Commercial Tobacco Free Act 2009
The Navajo Nation Commercial Tobacco Free Act 2011
Protect People from Secondhand Smoke

TRIBAL POLICY EFFORTS
Increased taxes on tobacco products: 2006 ($1.00) and 2011 (60 cents)
Educating leaders on increasing taxes again and changing tax structure for products.

TEAM Navajo “With the rates of obesity and diabetes rapidly increasing on the Navajo Nation, runners of Team Navajo are dedicated to addressing this health epidemic one mile at a time. Team Navajo dedicated countless hours to train for this life changing event with a goal to inspires our communities to live a healthy lifestyle and be in harmony. HOZHO”

TRIBAL POLICY EFFORTS
Breast feeding in public and workplaces
Healthier school lunches
Grocery and convenient stores food placement
Increasing excise taxes on junk food
Ban of biggie size soda drinks
Limit EBT purchases to healthy foods


Contact Information: Patricia Nez Henderson [email protected]
“With Sovereignty Comes Responsibility, Responsibility of the Health of Our People”