Patofisiologi Dan Tatalaksana DM

of 6
-
Upload
rohishatulilmiyah -
Category
Documents
-
view
215 -
download
0
Transcript of Patofisiologi Dan Tatalaksana DM
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
1/6
41JMAJ, January/ February 2010 Vol. 53, No. 1
Research and Reviews
Pathophysiology of Type 2 Diabetes and
Its Treatment Policy
JMAJ 53(1): 4146, 2010
Kohei KAKU*1
Abstract
Impaired insulin secretion and increased insulin resistance, the main pathophysiological features of type 2diabetes, jointly contribute to the development of this disease. Recently, it has become widely recognized that the
functional pancreatic cell mass decreases over time and type 2 diabetes is a progressive disease. Studiessuggest the possibility that the Japanese may have many genes susceptible to diabetes including thrifty genes.
Various environmental factors, added to these genetic factors, are considered responsible for the onset ofdisease, and the number of patients is increasing rapidly reflecting recent lifestyle changes. Impaired insulinsecretion is characterized by lowered glucose responsiveness. In particular, the decrease in postprandial-phase
secretion is an essential pathophysiological condition. Glucolipotoxicity, if left untreated, results in the decreasein the functional pancreatic cell mass. The goal of diabetes treatment is to secure a quality of life (QOL) and
lifespan comparable to those of healthy people, and a prerequisite for this is the prevention of onset andprogression of vascular complications. The need for earlier initiation of proactive intervention must be empha-sized, as well as the importance of comprehensive (blood sugar, blood pressure, and lipids) intervention in
attaining this goal.
Key words Type 2 diabetes, Impaired insulin secretion, Insulin resistance
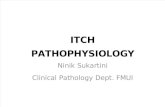
tion and insulin resistance and environmentalfactors such as obesity, overeating, lack of exer-cise, and stress, as well as aging. It is typically amultifactorial disease involving multiple genesand environmental factors to varying extents. Afact considered important in pathogenesis is thatJapanese show lower insulin secretory capacityafter sugar loading, suggesting smaller potentialfor pancreatic cell function than Western
people. It has also been pointed out that Japaneseindividuals may have many diabetes-sensitivegenes including thrifty genes. The number ofdiabetic patients is increasing rapidly reflectingthe changes in lifestyle (Fig. 1).Genetic factors involved in the pathogenesis ofdiabetes
The development of type 2 diabetes is clearlyassociated with a family history of diabetes. The
*1 Professor, Diabetes and Endocrine Division, Department of Internal Medicine, Kawasaki Medical School, Kurashiki, Okayama, Japan
([email protected]_m.ac.jp).
This article is a revised English version of a paper originally published in the Journal of the Japan Medical Association (Vol.138, No.1, 2009,
pages 2832).
Introduction
Diabetes is a group of metabolic disorders char-acterized by a chronic hyperglycemic conditionresulting from insufficient action of insulin. Themain pathophysiological features of type 2 diabe-tes, which represents a great majority of diabeticcases in Japan, are impaired insulin secretion andincreased insulin resistance. The impairment of
pancreaticcell function notably shows progres-sion over time.
Etiology and Pathophysiology of Type 2Diabetes
Etiology
Type 2 diabetes is caused by a combination ofgenetic factors related to impaired insulin secre-
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
2/6
42 JMAJ, January/ February 2010 Vol. 53, No. 1
significantly higher concordance rate betweenmonozygotic twins than between dizygotic twinssuggests the considerable involvement of geneticfactors.1 The pathogenesis has been assumed
to involve genetic abnormality in the moleculesrelated to the regulatory system of glucosemetabolism. The analyses of candidate genestargeted at glucose-stimulated insulin secretionof pancreatic cells and the molecules compris-ing the molecular mechanism for insulin actionhave identified genetic abnormalities that can beindependent causes of pathogenesis, includingthose in glucokinase genes, mitochondrial genes,and insulin receptor genes. Recently, a genome-wide association study (GWAS) has identifiedthe mutation in the KCNQ1 gene related to
insulin secretion abnormality as an important
disease-susceptible gene associated with thepathogenesis of diabetes in Asian ethnic groupsincluding the Japanese.2
The genetic abnormalities reported so far,
all combined, explain about 30% of the geneticfactors for diabetes, and our understanding ofgenetic factors is expected to be practically com-plete in the near future. According to the currentclassification of disease types, diabetic caseswith identified genetic abnormality are classifiedunder those due to other specific mechanismsor diseases.Roles of environmental factors
Aging, obesity, insufficient energy consumption,alcohol drinking, smoking, etc. are independentrisk factors of pathogenesis. Obesity (particularlyvisceral fat obesity) due to a lack of exercise
is accompanied by a decrease in muscle mass,induces insulin resistance, and is closely associ-ated with the rapid increase in the number ofmiddle- and high-aged patients. The changes indietary energy sources, particularly the increasein fat intake, the decrease in starch intake, theincrease in the consumption of simple sugars,and the decrease in dietary fiber intake, contri-bute to obesity and cause deterioration of glucosetolerance. Even mild obesity (BMI 25) causesa 4- to 5-fold increase in the risk of developingdiabetes, if accompanied by the increase in vis-
ceral fat mass. The Japanese are prone to visceral
Kaku K
4-fold increase in fat intakein 50 years (no change intotal energy intake)
Environmental factors
Lifestyle changes
High fat/lack of exercise
6-fold increase to23 million in 50 years
Obesity
Insulin resistance
Relative insufficiency of insulin action
Development of type 2 diabetes
Genetic factors
The insulin secretory capacityof Japanese is one-half thatof Western people
Decreased insulin secretion
Interaction
More than 30-fold increase in 50 years
8.9 million patients
13.2 million pre-diabetics
Fig. 1 Etiology and pathophysiology of type 2 diabetes in Japanese
Table 1 Factors causing increase in visceral fat
1. Stress-related factors
Overeating, especially excessive intake of simple sugars
Smoking
Increase in alcohol intake
Disorders of nervous and endocrine systems: increase
in cortisol, abnormality in sex hormone secretion
2. Lowered energy consumption due to a lack of exercise
3. Genetic factors
4. Aging
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
3/6
43JMAJ, January/ February 2010 Vol. 53, No. 1
fat accumulation due to hyperalimentation, andrisk factors for diabetes are linked to the accu-mulation of visceral fat (Table 1).
Pathophysiology
Impaired insulin secretion and insulin resistancecontribute more or less jointly to the develop-ment of pathophysiological conditions.Impaired insulin secretion
Impaired insulin secretion is a decrease in glu-cose responsiveness, which is observed beforethe clinical onset of disease. More specifically,
impaired glucose tolerance (IGT) is induced bya decrease in glucose-responsive early-phaseinsulin secretion, and a decrease in additionalinsulin secretion after meals causes postprandialhyperglycemia. An oral glucose tolerance test(OGTT) in IGT cases generally indicates anover-response in Western and Hispanic indivi-duals, who have markedly high insulin resistance.On the other hand, Japanese patients oftenrespond to this test with decreased insulin secre-tion. Even when an over-response is seen in per-sons with obesity or other factors, they show adecrease in early-phase secretory response. The
decrease in early-phase secretion is an essentialpart of this disease, and is extremely important asa basic pathophysiological change during theonset of disease in all ethnic groups.3
Impaired insulin secretion is generally pro-gressive, and its progression involves glucosetoxicity and lipo-toxicity. When untreated, theseare known to cause a decrease in pancreatic cell mass in animal experiments. The progressionof the impairment of pancreatic cell functiongreatly affects the long-term control of blood glu-cose. While patients in early stages after disease
onset chiefly show an increase in postprandial
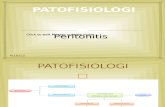
blood glucose as a result of increased insulinresistance and decreased early-phase secretion,the progression of the deterioration of pancreatic cell function subsequently causes permanentelevation of blood glucose (Fig. 2).Insulin resistance
Insulin resistance is a condition in which insulinin the body does not exert sufficient action propor-tional to its blood concentration. The impairmentof insulin action in major target organs such asliver and muscles is a common pathophysiologi-cal feature of type 2 diabetes. Insulin resistance
develops and expands prior to disease onset.The investigation into the molecular mecha-nism for insulin action has clarified how insulinresistance is related to genetic factors and envi-ronmental factors (hyperglycemia, free fatty acids,inflammatory mechanism, etc.). Known geneticfactors, include not only insulin receptor andinsulin receptor substrate (IRS)-1 gene poly-morphisms that directly affect insulin signals butalso polymorphisms of thrifty genes such as the3 adrenergic receptor gene and the uncouplingprotein (UCP) gene, associated with visceralobesity and promote insulin resistance. Glucolipo-
toxicity and inflammatory mediators are alsoimportant as the mechanisms for impaired insu-lin secretion and insulin signaling impairment.
Recent attention has focused on the involve-ment of adipocyte-derived bioactive substances(adipokines) in insulin resistance. While TNF-,leptin, resistin, and free fatty acids act to increaseresistance, adiponectin improves resistance.
Clinical tests to assess the extent of insulinresistance include homeostasis model assessmentfor insulin resistance (HOMA-IR), insulin sensi-tivity test (loading test), steady-state plasma glu-
cose (SSPG), minimal model analysis, and insulin
PATHOPHYSIOLOGY OF TYPE 2 DIABETES AND ITS TREATMENT POLICY
Reduction of postprandial insulin secretion Reduction of basal insulin secretion
Postprandial hyperglycemiaOverworking of pancreatic cells
Progressionof apoptosis
Decrease in pancreatic cell mass
Enhancement of insulin resistance
Glucose toxicity and lipo-toxicity are crucially involved in pathophysiological progression
Fig. 2 Pathophysiological progression of type 2 diabetes as seen from pancreaticcell function
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
4/6
44 JMAJ, January/ February 2010 Vol. 53, No. 1
clamp technique. The Matsuda index 4 is now gain-ing recognition as a relatively simple procedurethat can simultaneously evaluate insulin resis-
tance in the liver and muscles. After performingOGTT, this index is calculated by the formula:Matsuda Index10,000/ (FPGFPI) (meanPGmean PI), where FPG is fasting plasma glu-cose and FPI is fasting plasma insulin.
A more convenient way to estimate the degreeof resistance is to check for the presence of highfasting blood insulin, visceral obesity, hypertri-glyceridemia, etc.
Treatment Policy for Type 2 Diabetes
The goal of diabetes treatment is to secure a
quality of life (QOL) and lifespan comparableto those of healthy people, and a prerequisitefor attaining this goal is the prevention of onsetand progression of vascular complications. Therisk of macrovascular disease such as cardio-vascular disorders (atherosclerotic lesions) isincreased already in individuals with marginalblood glucose levels, underscoring the need forearly intervention.
Effective treatment to control vascularcomplications
Reports on the interventions to prevent the onset
of diabetes, control complications, and improveprognosis have demonstrated the following facts:(1) lifestyle improvement and anti-diabetic drugs
(-glucosidase inhibitor, metformin, thiazolidine)to treat IGT suppress the risk of developingtype 2 diabetes,57 (2) SU drugs, metformin, andinsulin are effective in controlling both micro-vascular disease and macrovascular disease, andearlier intervention is essential to the controlof macrovascular disease,811 (3) comprehensiveintervention including blood pressure and lipidmanagement is extremely effective in controllingvascular complications and reducing mortalityrate,12,13 and (4) pioglitazone suppresses therecurrence of cardiovascular disorders.14 Earlierand more comprehensive (including blood glu-
cose, blood pressure, and lipid) intervention ismore effective in controlling vascular complica-tions and improving prognosis.
The treatment paradigm for type 2 diabetes
Early initiation of intervention is also importantfor curbing the progression of pathophysiologicalconditions. Early efforts to remove the effect ofglucose toxicity as much as possible and to pre-serve pancreatic cell function are essential pre-requisites for long-term management of diabetes.Microvascular disease is more closely associated
with long-term blood glucose control. The treat-
Kaku K
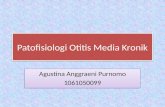
Impaired glucosetolerance Hypertension Dysl ipidemia Obesity
Lifestyle improvement
Pharmacological intervention
Macrovascular disease
Early-stage diabetes
Overt diabetes
Microvascular disease
Lifestyle improvement
Pharmacological intervention
Fig. 3 The management paradigm for type 2 diabetes: prevention of onset andproactive management of early-stage diabetes
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
5/6
45JMAJ, January/ February 2010 Vol. 53, No. 1
PATHOPHYSIOLOGY OF TYPE 2 DIABETES AND ITS TREATMENT POLICY
ment paradigm needs to be considered from theviewpoints of not only controlling vascular com-plications but also preventing the progression ofpathophysiological conditions. In this sense, it isnecessary to move up the treatment schedule(Fig. 3). Ideally, the aim should be to prevent theonset of diabetes among individuals with IGT(primary prevention). In addition to proactive
intervention for lifestyle improvement, we need
to accelerate the debate about whether to usepharmacological intervention.
The flow of treatment
The treatment algorism for type 2 diabetes rec-ommended in Europe and the U.S., based on theresults of United Kingdom Prospective DiabetesStudy (UKPDS),8,9,11 aims at cost-effective care
in which lifestyle improvement and metformin
Fig. 4 Flow of treatment for patients with type 2 diabetes
New diabetic patient
Blood sugar, HbA1c, body weight (recent changes)
Checks for urinary ketone bodies, complications, and contraindication for exercise therapy
Instructions on dietary therapy
Is insulin therapy indicated? Yes Begin insulin therapy
No
No
No
Does the patient show poor blood sugar control?
HbA1c 8.0%, FPG 160mg/dl, 2-hour postprandial glucose 220mg/dl
Dietary and exercise therapies
Poor control?
HbA1c6.5%, FPG 130mg/dl, 2-hour postprandial glucose 180mg/dl
Continue treatment
Yes
In addition to dietary therapy:
Obese patient (BMI 25)
Begin non-insulin-secreting agents (be cautious of contraindication): single
or combined use of GI agents, TZD agents, and BG agents.
Consider positively the use of TZD agents in patients with macrovascular
complications.
Non-obese patient (BMI 25)
Begin insulin secretion stimulator.
Glinide, low-dose SU drug (gliclazide 1020 mg, glimepiride 0.51 mg)
Combined use of non-insulin-secreting agents.
Yes
Patient shows progression of obesity: Review dietary and exercise therapies.
No progression of obesity:
Increase, switch, or combine drugs targeting at HbA1c 6.5%
(5.8% for prevention of macrovascular disease).
Switch from glinides to low-dose SU agents or increase the dose of SU agents.
Upper limit of the SU dose: up to one-half of the maximum dose.
GI agents: glucosidase inhibitors, BG agents: biguanides, TZD agents: thazolidines.
-
7/27/2019 Patofisiologi Dan Tatalaksana DM
6/6
46 JMAJ, January/ February 2010 Vol. 53, No. 1
are started at the same time and patients showingpoor response are subsequently treated with theadditional use of SU drugs and insulin therapy.On the other hand, the common practice in Japanis to select appropriate oral hypoglycemic agentswhen the patient has failed to achieve the bloodglucose control target despite sufficient patienteducation on the nature of diabetes and dietarytherapy and exercise therapy for 2 to 3 months.There are five groups of oral agents currentlyin use: SU drugs, fast-acting insulin secretionstimulators (glinides), biguanides, thiazolidines,and -glucosidase inhibitorssome of these arethe drugs developed after UKPDS. In view of
the difference between Japanese and Westernpopulations in the pathophysiological features ofdiabetes, and considering our own stance on theblood glucose control target and treatment para-digm, it is logical that we need treatment guide-lines that are different from those in Westerncountries.
The important elements in determining treat-ment policy include history taking, the presentdisease control status as seen from blood glucoseand HbA1c levels, present and past obesity, andthe presence or absence of complications. Since
early initiation of strict blood glucose control isimportant, the use of anti-diabetic agents should
not be delayed. The flow of treatment and thesuggestions on the use of drugs are summarizedin Fig. 4.
The recent results from the Action to ControlCardiovascular Risk in Diabetes (ACCORD)study indicate the possibility that abrupt inten-sive therapy may occasionally lead to poor prog-nosis.15 On the other hand, intensive therapy hasbeen reported to achieve better control of car-diovascular risk in the patients with a shorterhistory of illness.16 The treatment of patientswith long-standing illness and a long history ofpoor blood glucose control, as well as those withadvanced vascular damage, should aim at gradual
improvement of blood glucose control ratherthan a rapid decrease to HbA1c 6%.
Conclusion
With the soaring number of patients reflectingpopulation aging, diabetes demands broaderinvolvement of non-specialist physicians thanother diseases. Earlier intervention and con-tinued treatment are the keys to achieving thetreatment goals. The importance of close collabo-ration between specialists and non-specialist
physicians continues to increase.
References
1. Pyke DA. Diabetes: the genetic connections. Diabetologia.1979;17:333343.
2. Unoki H, Takahashi A, Kawaguchi T, et al. SNPs in KCNQ1 are
associated with susceptibility to type 2 diabetes in East Asianand European populations. Nat Genet. 2008;40:10981102.
3. Abdul-Ghani MA, Matsuda M, Jani R, et al. The relationshipbetween fasting hyperglycemia and insulin secretion in subjectswith normal or impaired glucose tolerance. Am J Physiol
Endocrinol Metab. 2008;295:E401E406.
4. Matsuda M, DeFronzo RA. Insulin sensitivity indices obtainedfrom oral glucose tolerance testing: comparison with theeuglycemic insulin clamp. Diabetes Care. 1999;22:14621470.
5. Chiasson JL, Josse RG, Gomis R, et al. Acarbose for preventionof type 2 diabetes mellitus: the STOPNIDDM randomised trial.Lancet. 2002;359:20722077.
6. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction inthe incidence of type 2 diabetes with lifestyle intervention or
metformin. N Engl J Med. 2002;346:393403.7. Buchanan TA, Xiang AH, Peters RK, et al. Preservation of
pancreatic beta-cell function and prevention of type 2 diabetes
by pharmacological treatment of insulin resistance in high-risk
hispanic women. Diabetes. 2002;51:27962803.8. Intensive blood-glucose control with sulphonylureas or insulin
compared with conventional treatment and risk of complications
in patients with type 2 diabetes (UKPDS 33). UK ProspectiveDiabetes Study (UKPDS) Group. Lancet. 1998;352:837853.
9. Effect of intensive blood-glucose control with metformin on com-
plications in overweight patients with type 2 diabetes (UKPDS34). UK Prospective Diabetes Study (UKPDS) Group. Lancet.1998;352:854865.
10. Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetestreatment and cardiovascular disease in patients with type 1
diabetes. N Engl J Med. 2005;353:26432653.11. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of
intensive glucose control in type 2 diabetes. N Engl J Med.
2008;359:15771589.
12. Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention andcardiovascular disease in patients with type 2 diabetes. N EnglJ Med. 2003;348:383393.
13. Gaede P, Lund-Andersen H, Parving HH, et al. Effect of a mul-tifactorial intervention on mortality in type 2 diabetes. N Engl JMed. 2008;358:580591.
14. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondaryprevention of macrovascular events in patients with type 2 dia-
betes in the PROactive Study (PROspective pioglitAzone ClinicalTrial In macro-Vascular Events): a randomised controlled trial.Lancet. 2005;366:12791289.
15. Action to Control Cardiovascular Risk in Diabetes Study Group,
Gerstein HC, Miller ME, et al. Effects of intensive glucose lower-ing in type 2 diabetes. N Engl J Med. 2008;358:25452559.
16. Duckworth W, Abraira C, Moritz T, et al. Glucose control and
vascular complications in veterans with type 2 diabetes. N EnglJ Med. 2009;360:129139.
Kaku K