
Patient Safety for the Newly Licensed Practical Nurse the possibility of „human error‟ and other...
20
State of Nebraska Transition Grant Copyright 2011 Patient Safety for the Newly Licensed Practical Nurse Education Module
Transcript of Patient Safety for the Newly Licensed Practical Nurse the possibility of „human error‟ and other...

State of Nebraska Transition Grant
Copyright 2011
Patient Safety for the
Newly Licensed Practical
Nurse Education Module
2
Title: Patient Safety
Introduction
Safety, the freedom from psychological and physical injury is a basic human need. Healthcare
provided in a safe manner and in a safe environment is essential for a patient‟s well being. Providing a
safe environment reduces the risk of accidents and health care costs. Safety is a need for everyone but
vulnerable groups are more at-risk. Infants, children, older adults, those who are ill, the physically and
mentally challenged, those who are illiterate, and the poor are at high risk for safety issues.
A culture of safety is an atmosphere of mutual trust in which all staff members talk freely about
safety problems and how to solve them, with no fear of blame or punishment. To be effective, the nurse
needs to understand the factors that contribute to a safe environment in the home, community and
healthcare facility. The nurse assesses the environment for threats to safety.
The nurse should be knowledgeable about how alterations in mobility, sensory function, and
cognitive function affect a patient‟s safety. A safe environment means meeting the patient‟s basic needs,
reducing physical hazards and eliminating transmission of pathogens.
Accidents in the healthcare environment can be classified in three ways: patient-inherent
accidents, procedure related accidents and equipment related accidents.
Patient-inherent accidents are those in which the patient is the primary cause of the accident.
This category includes: seizures, self-inflicted cuts, injuries, burns, ingestion or injection of foreign
substances, falls, fires and other changes in the patient status that places them at risk for injury.
Procedure-related accidents are caused by healthcare providers and include medication and fluid
administration errors, improper application of external devices, improper performance of procedures such
as dressing changes, hand-washing, body mechanics, catheter insertion and improper use of oxygen
equipment. Medication errors continue to be one of the most frequent causes of preventable harms in
health care.
Equipment-related accidents result from malfunction, disrepair or misuse of equipment or from
electrical hazards.
Nurses need basic understanding of types of disasters such as tornadoes and hurricanes, floods,
bioterrorism and chemical spills. When disaster strikes, rapid response is crucial so it is important to
know workplace policies related to disaster response.
Nurses should develop situational awareness that focuses on the art of patient observation.
Being able to periodically observe the patient, family and the environment promotes a safer patient care
environment and helps the nurse develop care priorities and focus attention to clinical detail.
Nurses must be involved in the creation of a culture of patient safety. This includes using
leadership skills, teamwork and effective communication with members of the healthcare team.
Teaching and learning should be evidence-based and patient-centered.
Learning Outcomes:
Upon completion of this education module, the newly licensed practical nurse will:
1. Evaluate the patient‟s environment for safety hazards.
2. Recognize changes in the patient‟s condition that make the patient at risk for injury.
3. Discuss the possibility of „human error‟ and other commonly used unsafe practices in the health care
environment.
4. Utilize appropriate clinical tools for documenting and assessing safety of patients.
3
5. Describe factors that can create a culture of safety in your work place.
6. Describe the benefits and limitations of safety enhancing technology.
7. Define terminology related to patient safety such as sentinel event, never event, hand-offs,
medication reconciliation, and root cause analysis.
8. Discuss the impact of national patient safety standards, initiatives and regulations of the
National Patient Safety Foundation and Joint Commission.
Interactive Exercises:
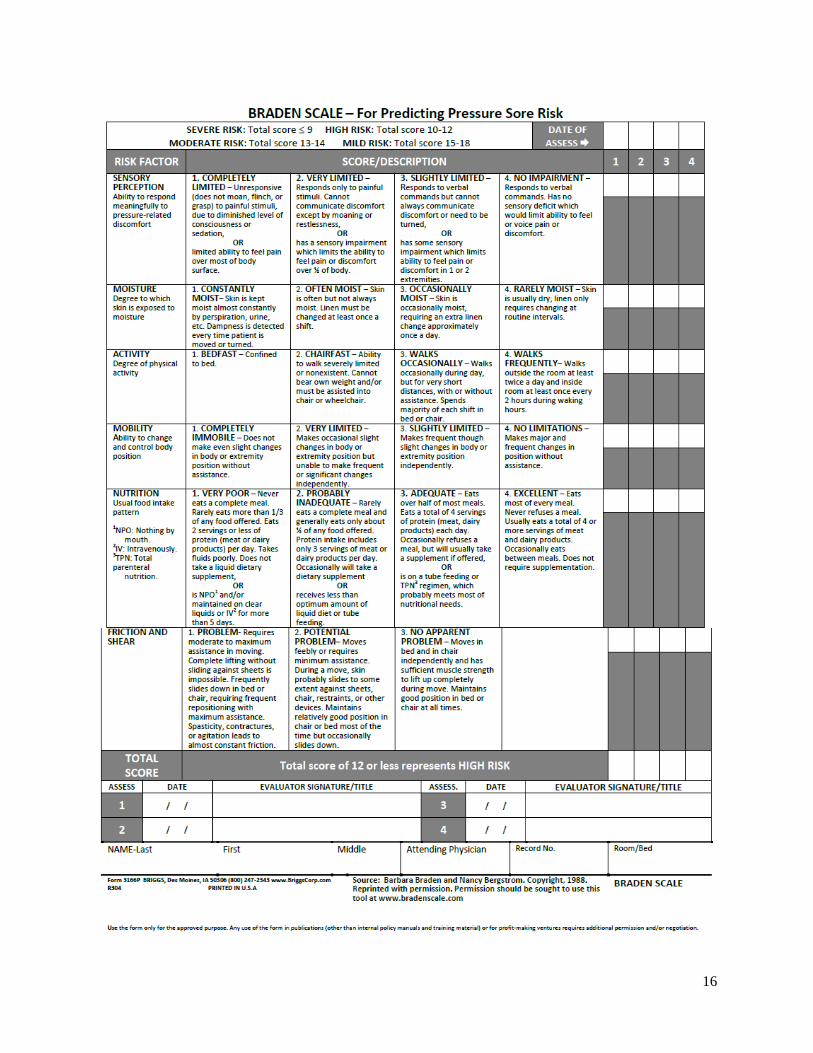
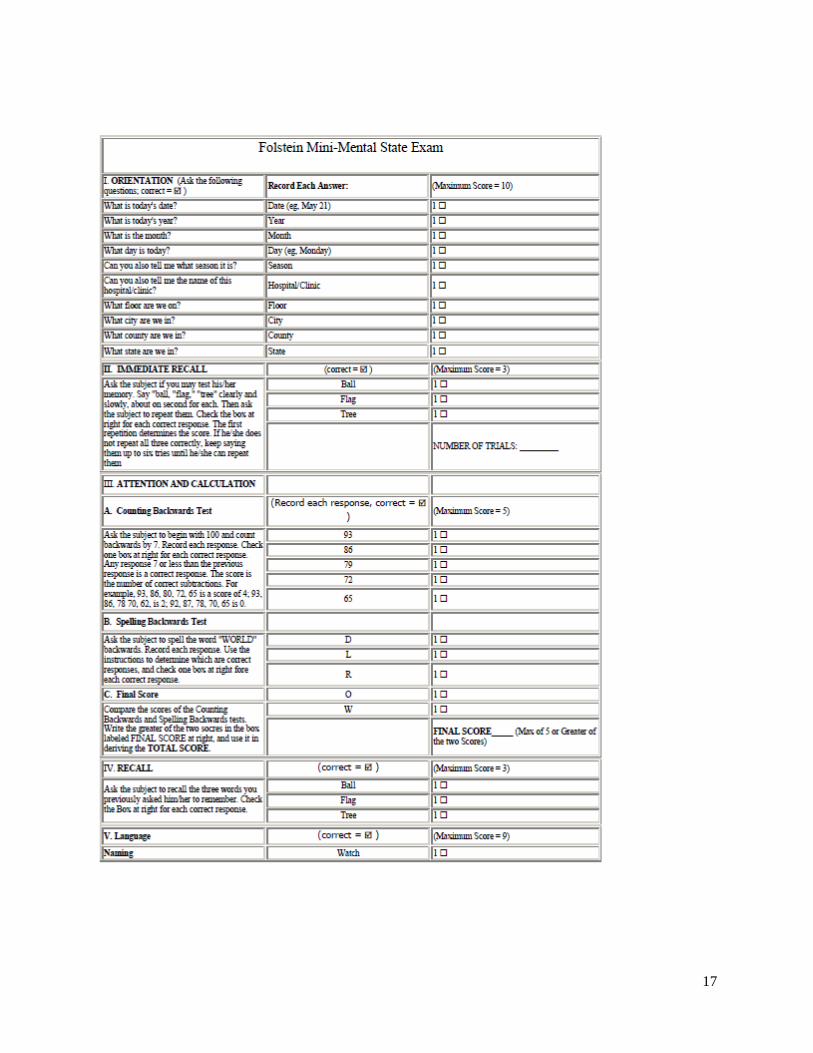
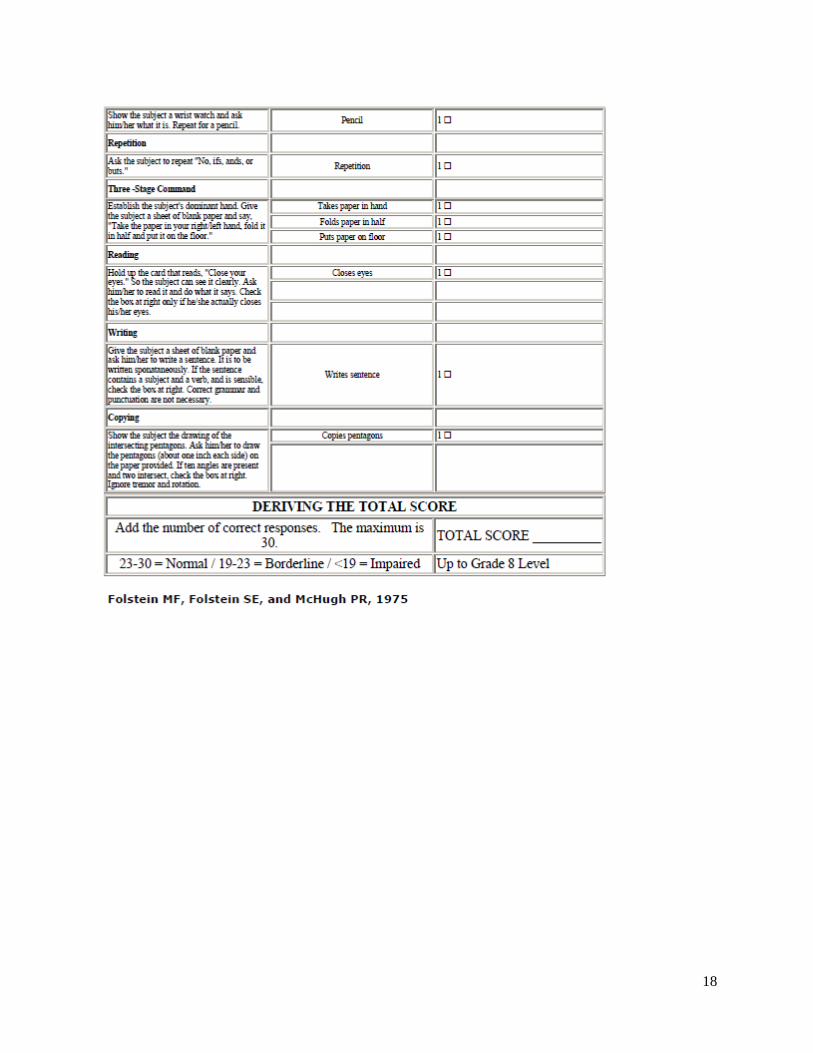
1. Identify the level of safety risk for a patient after completing a fall assessment tool, Braden Scale,
Mini Mental Examination and an Activities of Daily Living (ADLs) Tool. (Use the tools at your
facility or see Appendix A.)
2. Utilize the 60 second situational assessment found under supplemental resources to evaluate a
patient at your work place. Have your preceptor do the assessment as well. Compare your results
and discuss the differences.
3. Review the content on Root Cause Analysis at the following sites with your preceptor. Review five
incident reports or medication/procedure errors and develop a root cause diagram for the incident.
Review the root cause analysis with your preceptor and describe what went wrong and why. How
could the incident have been prevented? What is the accountability of the new LPN? Does your
quality improvement committee utilize this process? The second website goes through the process
of evaluating an incident using an example. http://www.patientsafety.gov/vision.html
http://www4.va.gov/ncps/CogAids/RCA/index.html
4. Research at least five charts for unsafe abbreviations utilized by nurses. Review the Joint
Commission site for the „Do Not Use List‟ at http://www.jointcommission.org/
5. Volunteer to be a member of your facility‟s safety committee. Review the guidelines and duties of
the committee.
6. Review the medication administration record for five to ten patients. Utilizing the Institute of Safe
Medication Practice (ISMP) website to identify which patient medications are on the high alert list
and why. http://www.ismp.org/Tools/highalertmedications.pdf
7. Monitor UAPs and NAs transfers of patients utilizing mechanical lifts and transfer techniques and
identify any safety concerns. Discuss these with your preceptor.
8. Define what is meant by a sentinel event. Discuss the LPN role when a sentinel event has occurred
with your direct supervisor. Review the Joint Commission website.
10. Define what is meant by a culture of patient safety. What is included in the culture? After
reviewing the following website would you say that the facility you work at has an adequate culture
of patient safety? Refer to the website.
http://www.med.umich.edu/patientsafetytoolkit/culture/chapter.pdf
4
11. Monitor medication aides or other nurses when administering medications and giving patient care.
Do they utilize the six rights? Describe safety precautions used or not used in providing care. If
you identify any safety concerns, how will you communicate the need for change? Refer to the example
below: Excerpts and table adapted from the QSEN Constructive Criticism Tool at
http://www.qsen.org/teachingstrategy.php?id=133
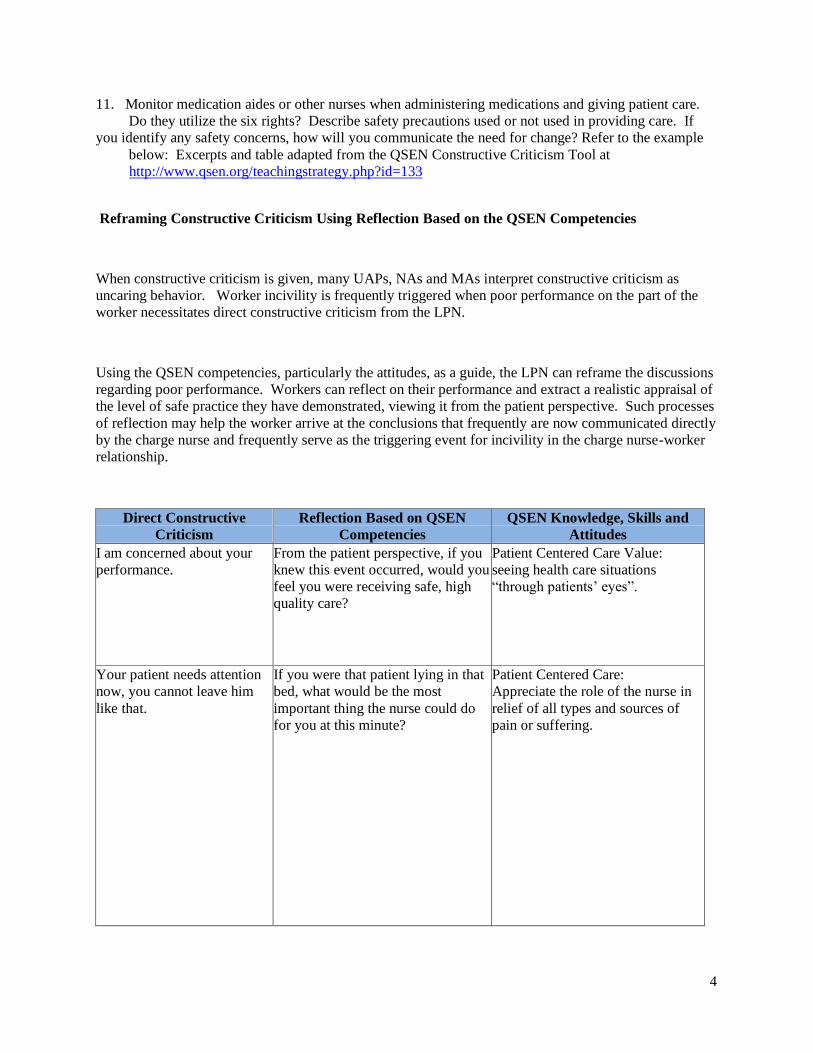
Reframing Constructive Criticism Using Reflection Based on the QSEN Competencies
When constructive criticism is given, many UAPs, NAs and MAs interpret constructive criticism as
uncaring behavior. Worker incivility is frequently triggered when poor performance on the part of the
worker necessitates direct constructive criticism from the LPN.
Using the QSEN competencies, particularly the attitudes, as a guide, the LPN can reframe the discussions
regarding poor performance. Workers can reflect on their performance and extract a realistic appraisal of
the level of safe practice they have demonstrated, viewing it from the patient perspective. Such processes
of reflection may help the worker arrive at the conclusions that frequently are now communicated directly
by the charge nurse and frequently serve as the triggering event for incivility in the charge nurse-worker
relationship.
Direct Constructive
Criticism
Reflection Based on QSEN
Competencies
QSEN Knowledge, Skills and
Attitudes
I am concerned about your
performance.
From the patient perspective, if you
knew this event occurred, would you
feel you were receiving safe, high
quality care?
Patient Centered Care Value:
seeing health care situations
“through patients‟ eyes”.
Your patient needs attention
now, you cannot leave him
like that.
If you were that patient lying in that
bed, what would be the most
important thing the nurse could do
for you at this minute?
Patient Centered Care:
Appreciate the role of the nurse in
relief of all types and sources of
pain or suffering.

5
Can you hear what you are
saying and understand what
your body language conveys?
You spoke to him like he was
a child. No wonder he is
refusing.
Think about how the patient feels
being told all day by others, what he
has to do. How can you present this
to him and still allow him to be part
of the decision?
Patient Centered Care Value:
continuous improvement of own
communication and conflict
resolution skills
Direct Constructive
Criticism
Reflection Based on QSEN
Competencies
QSEN Knowledge, Skills and
Attitudes
The report you gave was
missing very important
information. How will the
nurse know what is going on?
You need to use SBAR.
How could you have ensured that
your report included all the
information needed so that the
receiving nurse could provide safe
care to the patient?
Teamwork and Collaboration:
Appreciate the risks associated with
handoffs among providers and
across transitions in care.
You are responsible for that
lab report not being
communicated in a timely
manner.
How should critical lab reports be
managed? Why do we do it that
way?
Teamwork and Collaboration:
Acknowledge own potential to
contribute to effective team
functioning.
You do not assist your peers. What can you do to put that patient
at the center of care?
Teamwork and Collaboration:
Respect the centrality of the
patient/family as core members of
any health care team.
Why would you do it that
way?
Is there a scientific basis for how
you are doing that?
Evidence-based Practice:
Appreciate strengths and
weaknesses of scientific bases for
practice.
You need to demonstrate
immediate improvement.
What strategies can you use in your
own practice to prevent this
problem/error/risk?
Quality Improvement:
Appreciate the value of what
individuals and teams can do to
improve care.
You need to be more careful. In retrospect, what aspects of your
practice in this situation would you
change to provide safer patient care?
Quality Improvement:
Value own and others‟
contributions to outcomes of care in
local care settings.
6
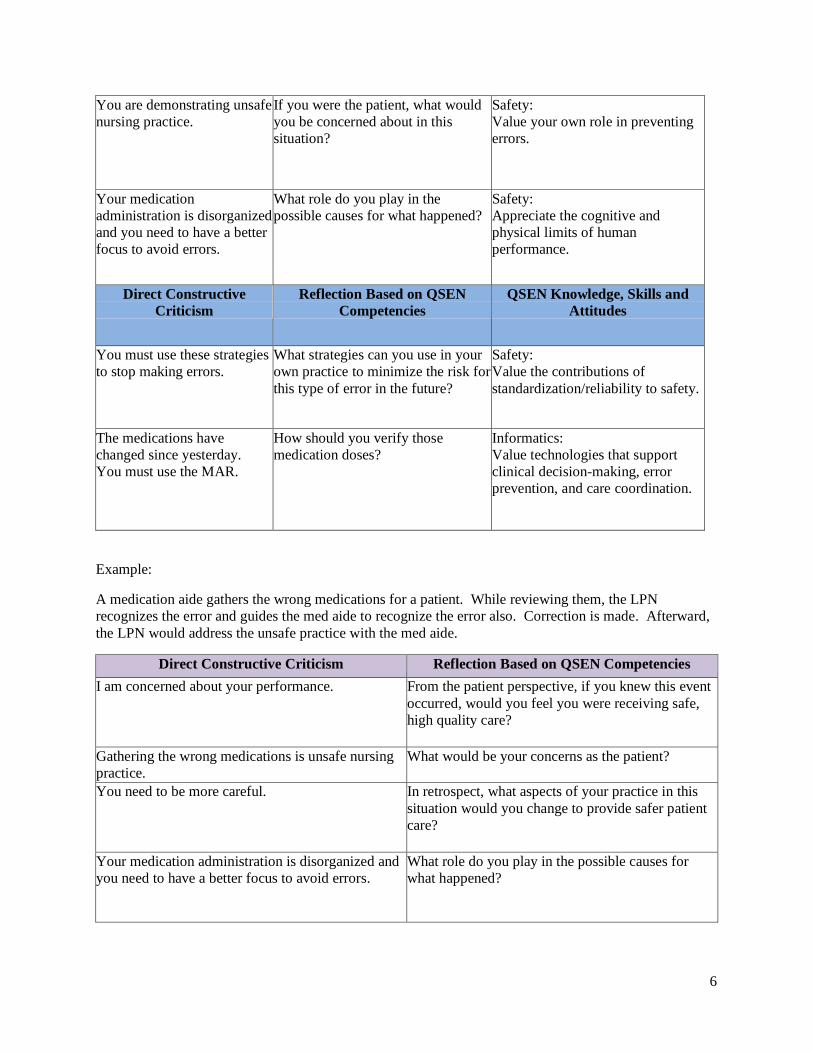
You are demonstrating unsafe
nursing practice.
If you were the patient, what would
you be concerned about in this
situation?
Safety:
Value your own role in preventing
errors.
Your medication
administration is disorganized
and you need to have a better
focus to avoid errors.
What role do you play in the
possible causes for what happened?
Safety:
Appreciate the cognitive and
physical limits of human
performance.
Direct Constructive
Criticism
Reflection Based on QSEN
Competencies
QSEN Knowledge, Skills and
Attitudes
You must use these strategies
to stop making errors.
What strategies can you use in your
own practice to minimize the risk for
this type of error in the future?
Safety:
Value the contributions of
standardization/reliability to safety.
The medications have
changed since yesterday.
You must use the MAR.
How should you verify those
medication doses?
Informatics:
Value technologies that support
clinical decision-making, error
prevention, and care coordination.
Example:
A medication aide gathers the wrong medications for a patient. While reviewing them, the LPN
recognizes the error and guides the med aide to recognize the error also. Correction is made. Afterward,
the LPN would address the unsafe practice with the med aide.
Direct Constructive Criticism Reflection Based on QSEN Competencies
I am concerned about your performance. From the patient perspective, if you knew this event
occurred, would you feel you were receiving safe,
high quality care?
Gathering the wrong medications is unsafe nursing
practice.
What would be your concerns as the patient?
You need to be more careful. In retrospect, what aspects of your practice in this
situation would you change to provide safer patient
care?
Your medication administration is disorganized and
you need to have a better focus to avoid errors.
What role do you play in the possible causes for
what happened?
7
I want you to do three checks with medication
administration, verifying the medication against the
medication administration record and use the six
rights as a way of decreasing potential errors.
What strategies can you use in your own practice to
minimize the risk for this type of error in the future?
It is important that you demonstrate immediate
improvement so that you provide safe care to
patients.
What outcome in your own performance would you
want to see after this experience?
12. Observe patient identification by other staff members. Discuss with your preceptor your facility‟s
policy on how to identify patients that are alert, children, patients who are confused, and those
with sensory problems. Be aware of color coding for bracelet identification and picture
identification.
13. Review the policy for fires in the facility and observe staff as they go through a fire drill. Participate
in a staff debriefing after the. Identify any issues that resulted from lack of attention to safety.
14. Learn the codes of safety for lost persons, fire, chemical spills, bioterrorism, tornadoes, floods, and
poisons. Know where the MSDS instructions are in the facility.
15. Prepare a room for a patient who has active seizure precautions. Include equipment to use with
this patient. Review the procedure on care of a client with seizures in your facility policy manual.
Is there a patient care guideline that should be followed when caring for this patient? Discuss the
policy and guideline with your preceptor.
16. Teach patients how to reduce hazards in their rooms and when discharged to home.
17. What is the agency policy on handling equipment that is broken, non-operable or unsafe? Discuss
this with your preceptor. With your preceptor, review equipment on your unit such as wheelchairs,
transfer devices, carts, shower chairs, chairs, light fixtures, etc. and identify any safety concerns.
How should these be handled?
18. Read the policy at your facility on bioterrorism.
19. Define „Never Events‟. Discuss examples of never events that have occurred by just „googling‟ the
words “never event”. Refer to the website about the incident in Fremont Nebraska on unsafe
practices by nurses in a cancer clinic. http://aneverevent.com/
http://en.wikipedia.org/wiki/Never_events
20. Complete a transfer form for a patient leaving the hospital or for a patient being sent to the
hospital. Keep in mind the need for medication reconciliation. Why is this important for the safety
of the patient? Refer to the ISMP website http://www.ismp.org/
21. What is the importance of making sure that your „hands off‟ between shifts in complete and
accurate? Listen to report on a group of patients. Did you have any questions at the end
of report? Give report on a group of patients. Did you include everything in report?

8
References
Agency for Healthcare Research and Quality (2008). Patient safety and quality: an evidence-based
handbook for nurses. United States Department of Health and Human Services. Excerpts
retrieved on October 23, 2010 at http://www.ahrq.gov/QUAL/nurseshdbk/
Altmiller G. (2010). Reframing constructive criticism using reflection based on QSEN competencies.
Retrieved on October 23, 2010 at http://www.qsen.org/teachingstrategy.php?id=133
Benner, P., Malloch, K., Sheets, V. (2010). Nursing pathways for patient safety. National Council
of State Boards of Nursing (NCSBN). Mosby, Inc.
Berman, A., Snyder, S., McKinney. D. (2011). Nursing Basics for Clinical Practice. Pearson Education
Inc. New Jersey.
Centers for Disease Control and Prevention. (2009). Hand hygiene in healthcare settings. Retrieved
on October 23, 2010 at http://www.cdc.gov/handhygiene/
Centers for Disease Control and Prevention. (2009). Infection control guidelines. Retrieved on October
23, 2010 at http://www.cdc.gov/ncidod/dhqp/guidelines.html
DeRosier J. and Stalhandske E. (2010). Root cause analysis. United States Department of Veteran
Affairs. Retrieved on October 23, 2010 at http://www.patientsafety.gov/vision.html
http://www4.va.gov/ncps/CogAids/RCA/index.html
Finkelman, A. and Kenner, C. (2007). Teaching IOM: Implications of the Institute of Medicine Reports
for
Nursing Education. American Nurses Association.
Folstein Mini Mental Examination. Retrieved on October 23, 2010 at
http://www.utmb.edu/psychology/ClinPsych/Assessments/MMSE.pdf
Institute for Safe Medication Practices. (2010). http://www.ismp.org/
Levett-Jones, T., Hoffman, K., Dempsey, J., Jeong, S. , Noble, D., Norton, C., Roche, J., Hickey, N.
(2010). The 'five rights' of clinical reasoning: An educational model to enhance nursing students' ability
to identify and manage clinically 'at risk' patients. Nurse Education Today, 30 (6), 515-520.
Katz Index of Activities of Daily Living and Barthel ADL Index Assessment Tools. Retrieved on
October 23, 2010 at http://web.missouri.edu/~proste/tool/funct/index.htm
Modak I., Sexton J. , Lux, T., Helmreich, R., Thomas E. (2007). Measuring safety culture in ambulatory
setting: the safety attitudes questionnaire-ambulatory version. Journal of General Internal
Medicine. Retrieved on October 23, 2010 at
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2227589/?tool=pubmed
Never Events. Retrieved on October 24, 2010 at http://aneverevent.com/ or examples on
http://en.wikipedia.org/wiki/Never_events
Potter, P., Perry, A. (2011). Fundamentals of Nursing. (7th
ed.) St. Louis: Mosby-Elsevier.
JCAHO http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/
Safety Culture. Retrieved on October 23, 2010 at
http://www.med.umich.edu/patientsafetytoolkit/culture/chapter.pdf

9
Struth, D., Grbach W., Vincent E., Heil J., Simpson C. (2009). 60 second situational assessment.
Retrieved on October 23, 2010 at http://www.qsen.org/teachingstrategy.php?id=89
Appendix
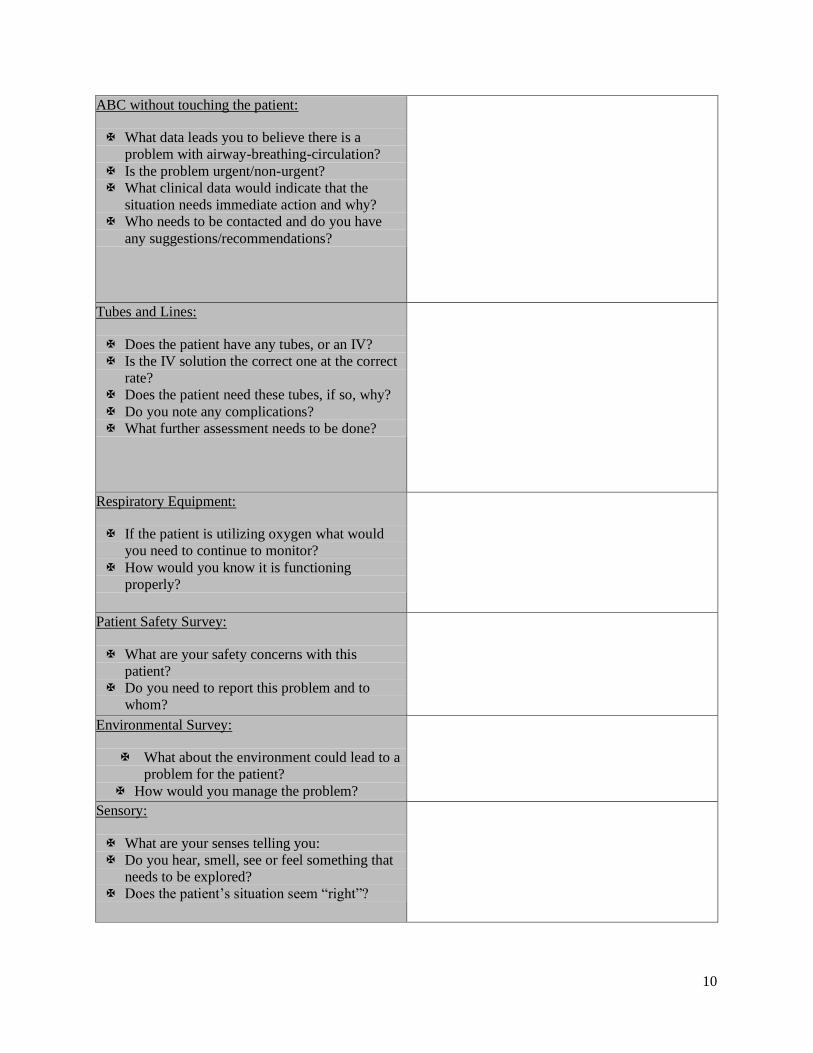
UPMC Shadyside School of Nursing 60 Second Situational Assessment
Directions – Enter a patient‟s room and observe the patient, family and environment for up to 60 seconds,
while reviewing the following questions in your mind.
10
ABC without touching the patient:
What data leads you to believe there is a
problem with airway-breathing-circulation?
Is the problem urgent/non-urgent?
What clinical data would indicate that the
situation needs immediate action and why?
Who needs to be contacted and do you have
any suggestions/recommendations?
Tubes and Lines:
Does the patient have any tubes, or an IV?
Is the IV solution the correct one at the correct
rate?
Does the patient need these tubes, if so, why?
Do you note any complications?
What further assessment needs to be done?
Respiratory Equipment:
If the patient is utilizing oxygen what would
you need to continue to monitor?
How would you know it is functioning
properly?
Patient Safety Survey:
What are your safety concerns with this
patient?
Do you need to report this problem and to
whom?
Environmental Survey:
What about the environment could lead to a
problem for the patient?
How would you manage the problem?
Sensory:
What are your senses telling you:
Do you hear, smell, see or feel something that
needs to be explored?
Does the patient‟s situation seem “right”?

11
What additional information would be helpful for
further clarification of the situation?
What questions are unanswered and what answers
are unquestioned?
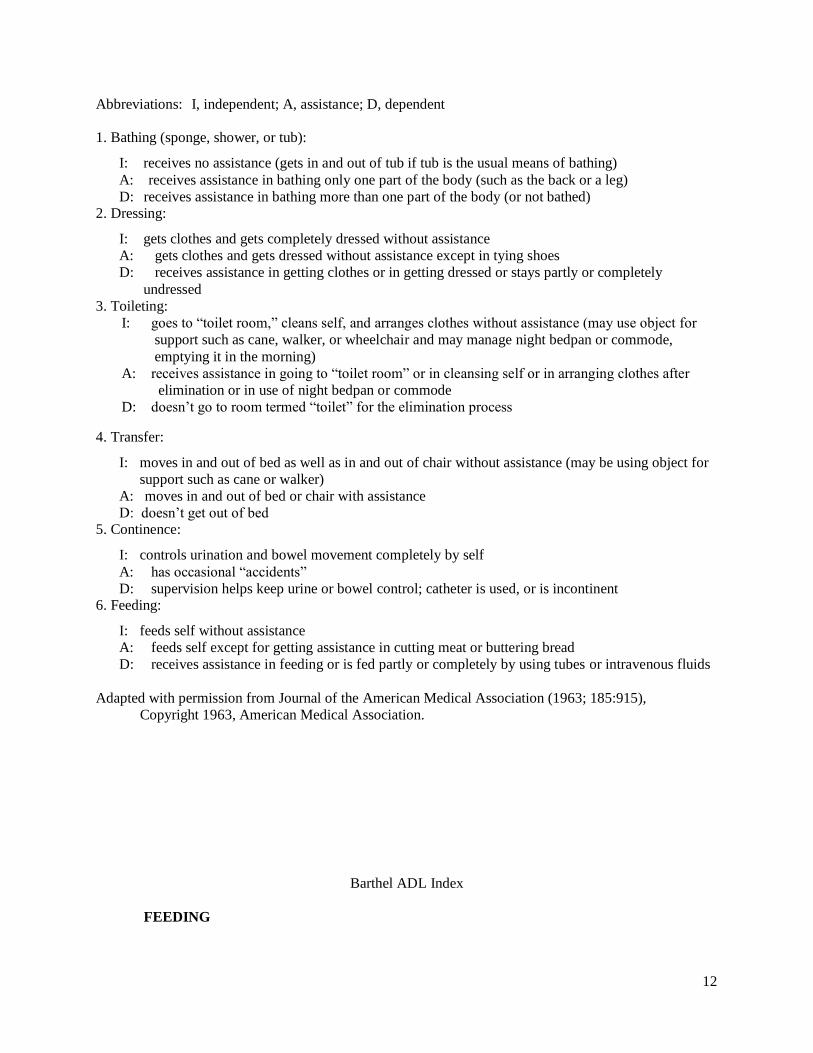
Katz Index of Activities of Daily Living
12
Abbreviations: I, independent; A, assistance; D, dependent
1. Bathing (sponge, shower, or tub):
I: receives no assistance (gets in and out of tub if tub is the usual means of bathing)
A: receives assistance in bathing only one part of the body (such as the back or a leg)
D: receives assistance in bathing more than one part of the body (or not bathed) 2. Dressing:
I: gets clothes and gets completely dressed without assistance
A: gets clothes and gets dressed without assistance except in tying shoes
D: receives assistance in getting clothes or in getting dressed or stays partly or completely
undressed
3. Toileting:
I: goes to “toilet room,” cleans self, and arranges clothes without assistance (may use object for
support such as cane, walker, or wheelchair and may manage night bedpan or commode,
emptying it in the morning)
A: receives assistance in going to “toilet room” or in cleansing self or in arranging clothes after
elimination or in use of night bedpan or commode
D: doesn‟t go to room termed “toilet” for the elimination process
4. Transfer:
I: moves in and out of bed as well as in and out of chair without assistance (may be using object for
support such as cane or walker)
A: moves in and out of bed or chair with assistance
D: doesn‟t get out of bed 5. Continence:
I: controls urination and bowel movement completely by self
A: has occasional “accidents”
D: supervision helps keep urine or bowel control; catheter is used, or is incontinent 6. Feeding:
I: feeds self without assistance
A: feeds self except for getting assistance in cutting meat or buttering bread
D: receives assistance in feeding or is fed partly or completely by using tubes or intravenous fluids
Adapted with permission from Journal of the American Medical Association (1963; 185:915),
Copyright 1963, American Medical Association.
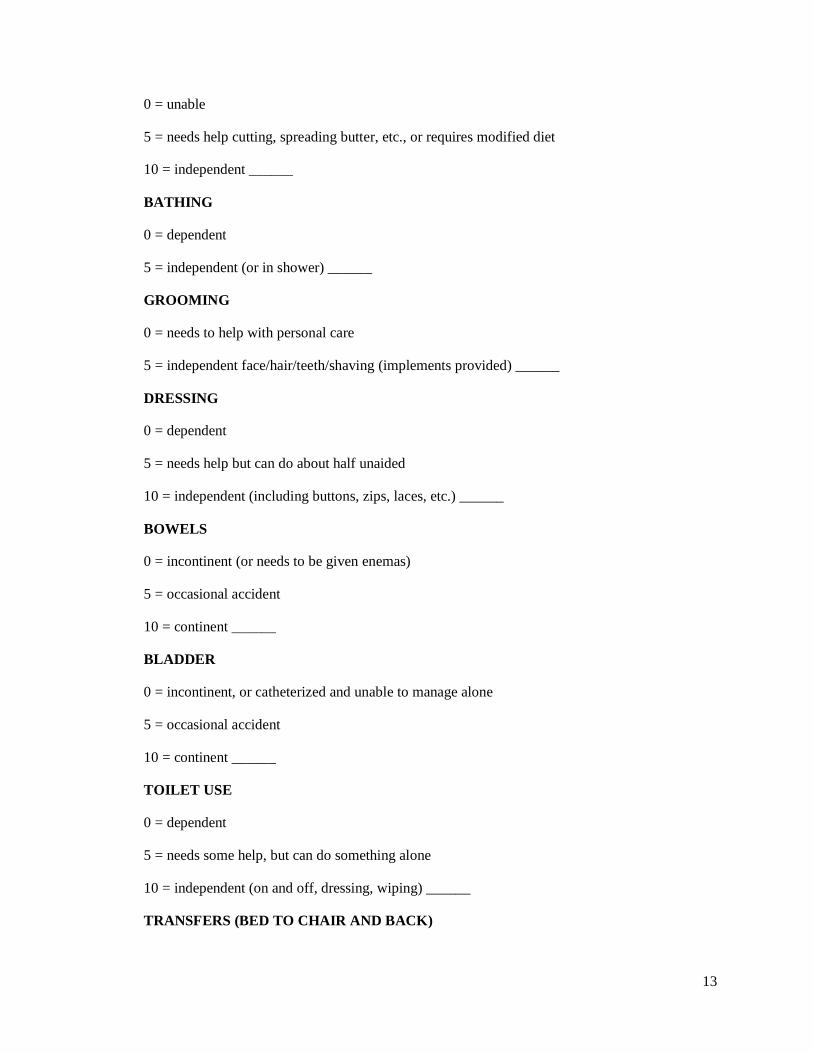
Barthel ADL Index
FEEDING
13
0 = unable
5 = needs help cutting, spreading butter, etc., or requires modified diet
10 = independent ______
BATHING
0 = dependent
5 = independent (or in shower) ______
GROOMING
0 = needs to help with personal care
5 = independent face/hair/teeth/shaving (implements provided) ______
DRESSING
0 = dependent
5 = needs help but can do about half unaided
10 = independent (including buttons, zips, laces, etc.) ______
BOWELS
0 = incontinent (or needs to be given enemas)
5 = occasional accident
10 = continent ______
BLADDER
0 = incontinent, or catheterized and unable to manage alone
5 = occasional accident
10 = continent ______
TOILET USE
0 = dependent
5 = needs some help, but can do something alone
10 = independent (on and off, dressing, wiping) ______
TRANSFERS (BED TO CHAIR AND BACK)
14
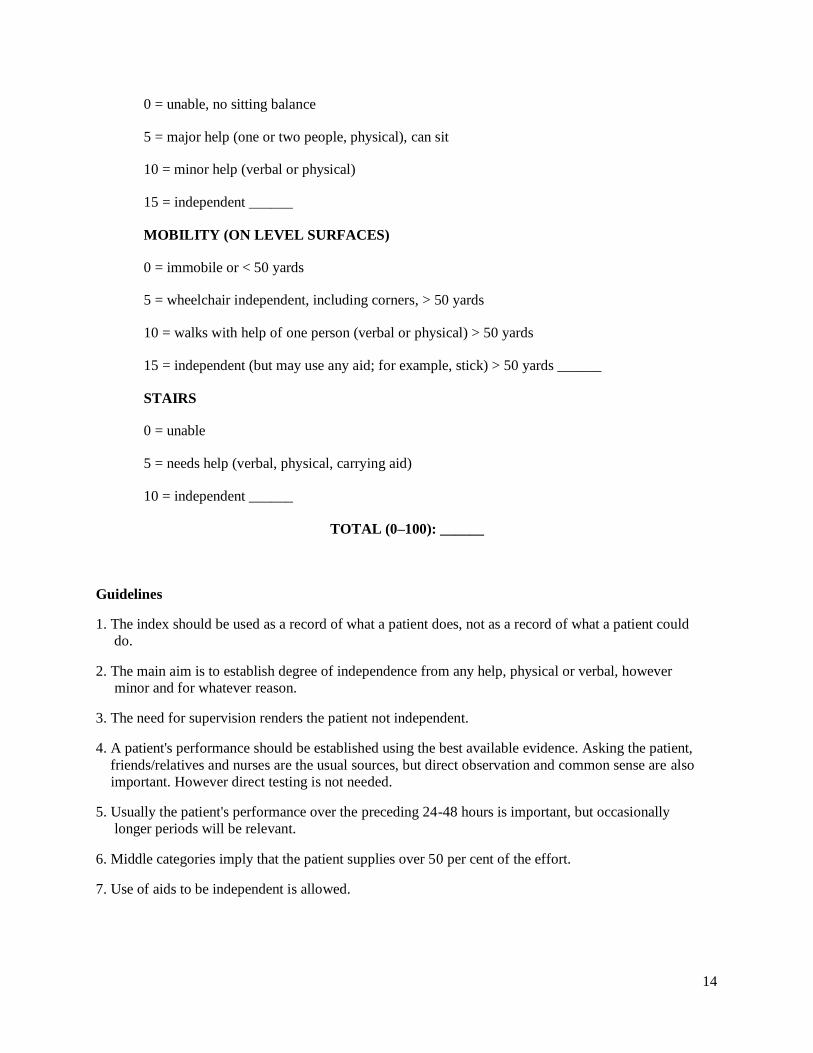
0 = unable, no sitting balance
5 = major help (one or two people, physical), can sit
10 = minor help (verbal or physical)
15 = independent ______
MOBILITY (ON LEVEL SURFACES)
0 = immobile or < 50 yards
5 = wheelchair independent, including corners, > 50 yards
10 = walks with help of one person (verbal or physical) > 50 yards
15 = independent (but may use any aid; for example, stick) > 50 yards ______
STAIRS
0 = unable
5 = needs help (verbal, physical, carrying aid)
10 = independent ______
TOTAL (0–100): ______
Guidelines
1. The index should be used as a record of what a patient does, not as a record of what a patient could
do.
2. The main aim is to establish degree of independence from any help, physical or verbal, however
minor and for whatever reason.
3. The need for supervision renders the patient not independent.
4. A patient's performance should be established using the best available evidence. Asking the patient,
friends/relatives and nurses are the usual sources, but direct observation and common sense are also
important. However direct testing is not needed.
5. Usually the patient's performance over the preceding 24-48 hours is important, but occasionally
longer periods will be relevant.
6. Middle categories imply that the patient supplies over 50 per cent of the effort.
7. Use of aids to be independent is allowed.

15
16
17
18
19
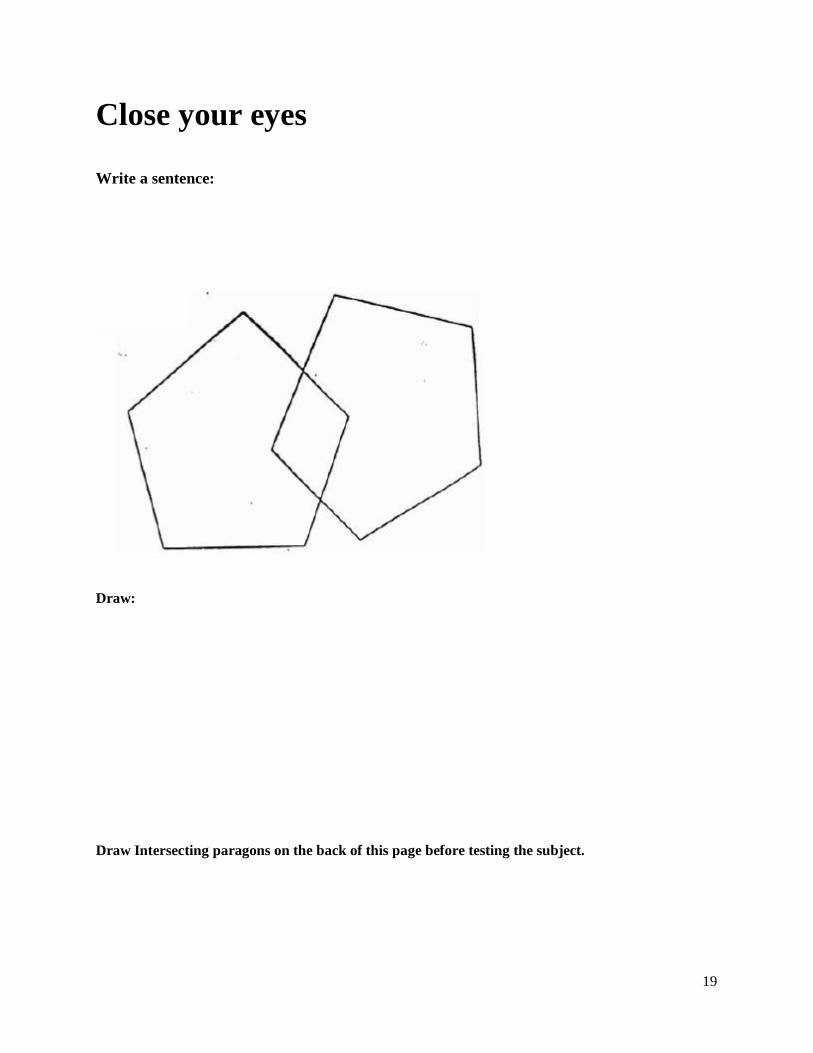
Close your eyes
Write a sentence:
Draw:
Draw Intersecting paragons on the back of this page before testing the subject.

20


















