Patient s Name: Date - jaxhealth.com circle YES or NO to the following questions: ... Designated...
15
1 Shircliff Way Jacksonville, FL 32204 PHONE: (904) 308-1956 FAX: (904) 308-5910 Patient’s Name: Date: Please circle YES or NO to the following questions: YES NO Do you have insurance? Name of Insurance Carrier: ___________________ Member ID number: ________________________ YES NO Are you over the age of 65? YES NO Have you ever been in the military? YES NO Do you have minor children in custody? YES NO Are you under the age of 21? YES NO Have you been deemed disabled by Social Security? YES NO Do you have a disability case pending? YES NO Are you pregnant? YES NO Are you a U.S. Citizen? Please indicate the reason(s) you are applying for HOPE: (You may check more than one) □ Outstanding hospital bills □ I am a Diagnostic Cardiology patient □ I was admitted as an inpatient to SVMC from the Emergency Room and I am in need of continuation of care. □ I was referred by a physician: Physician’s Name:___________________ □ I wish to renew my HOPE benefits □ Other (please explain): **APPLICATIONS CAN TAKE UP TO 45 DAYS TO PROCESS**
Transcript of Patient s Name: Date - jaxhealth.com circle YES or NO to the following questions: ... Designated...

1 Shircliff Way Jacksonville, FL 32204
PHONE: (904) 308-1956 FAX: (904) 308-5910
Patient’s Name: Date:
Please circle YES or NO to the following questions:
YES NO Do you have insurance? Name of Insurance Carrier: ___________________ Member ID number: ________________________
YES NO Are you over the age of 65?
YES NO Have you ever been in the military?
YES NO Do you have minor children in custody?
YES NO Are you under the age of 21?
YES NO Have you been deemed disabled by Social Security?
YES NO Do you have a disability case pending?
YES NO Are you pregnant?
YES NO Are you a U.S. Citizen?
Please indicate the reason(s) you are applying for HOPE:
(You may check more than one)
□ Outstanding hospital bills
□ I am a Diagnostic Cardiology patient
□ I was admitted as an inpatient to SVMC from the Emergency Room and I am in need of continuation of care.
□ I was referred by a physician: Physician’s Name:___________________□ I wish to renew my HOPE benefits
□ Other (please explain):
**APPLICATIONS CAN TAKE UP TO 45 DAYS TO PROCESS**

HOPE APPLICATION INSTRUCTIONS-PLEASE READ
□ Application Checklist for HOPE Please provide copies of all required documents. Applications are not accepted without all of the documents required. Applications received without all required documents will be returned.
□ Financial Assistance/HOPE Application Please complete all sections of this page: List all family members that live in the same house or are temporarily absent from the home. Family is defined as everyone that lives in the same house that is related to you by birth, marriage or adoption.
□ List All Family Members Please complete all sections of this page: List all family members that live in the same house or are temporarily absent from the home, even if they are already included on the previous page.
□ Financial Information Release (FL residents only) Please sign and date on the signature(s) line. If married, patient and spouse must sign
□ Designated Representative (GA residents only) Please sign and date
□ Appointment of Designated Representative (FL residents only) Please sign on the “Signature of Customer” line and date. Do not enter a name for the representative. This will be an R1 employee.
□ HIPPA Authorization Form Please sign and date
□ R1 Authorization for Patient Representation Please sign and date
□ Financial Assistance Agreement Please initial all lines, sign, and date
□ Authorization for Release of Protected Health Information Please sign and date
□ Affidavit of Support Please sign and date
□ Homeless Attestation Form Please sign and date

Application Checklist for HOPE
Patient:
Photo ID
Copy of Social Security Card Previous year Income Tax Return (not 1099 or W2)
OR Verification of Non Filing (visit www.irs.gov/form 4506-T for instructions)
Income Verification for Family: (Family is defined as everyone that
lives in the same house that is related by birth, marriage or adoption. Previous year Income Tax Return (not 1099 or W2) OR Verification
of Non Filing (visit www.irs.gov/form 4506t for instructions)
If employed; All pay stubs from the last 3 months (paid weekly=12 stubs, bi-weekly=6 stubs, etc.)
If unemployed and receiving no income (patient only); Affidavit or Letter or Support written and signed by someone other than yourself, with a copy of their photo ID.
If you receive or are receiving Unemployment Compensation; Letter of Benefits
If you receive Social Security; Letter of Benefits. This is the letter you received stating how much you receive each month, not the 1099 from the previous year.
Proof of any other income you are receiving (i.e. child support, pension, retirement, etc.) This would be a statement from the provider.
If you are Homeless; Homeless Attestation Form.
If you are Self Employed; a current year-to-date Profit & Loss statement, if you were self-employed in the previous year; previous year tax returns Schedule C.
**NOTE** Bank statements are not acceptable proof of income.
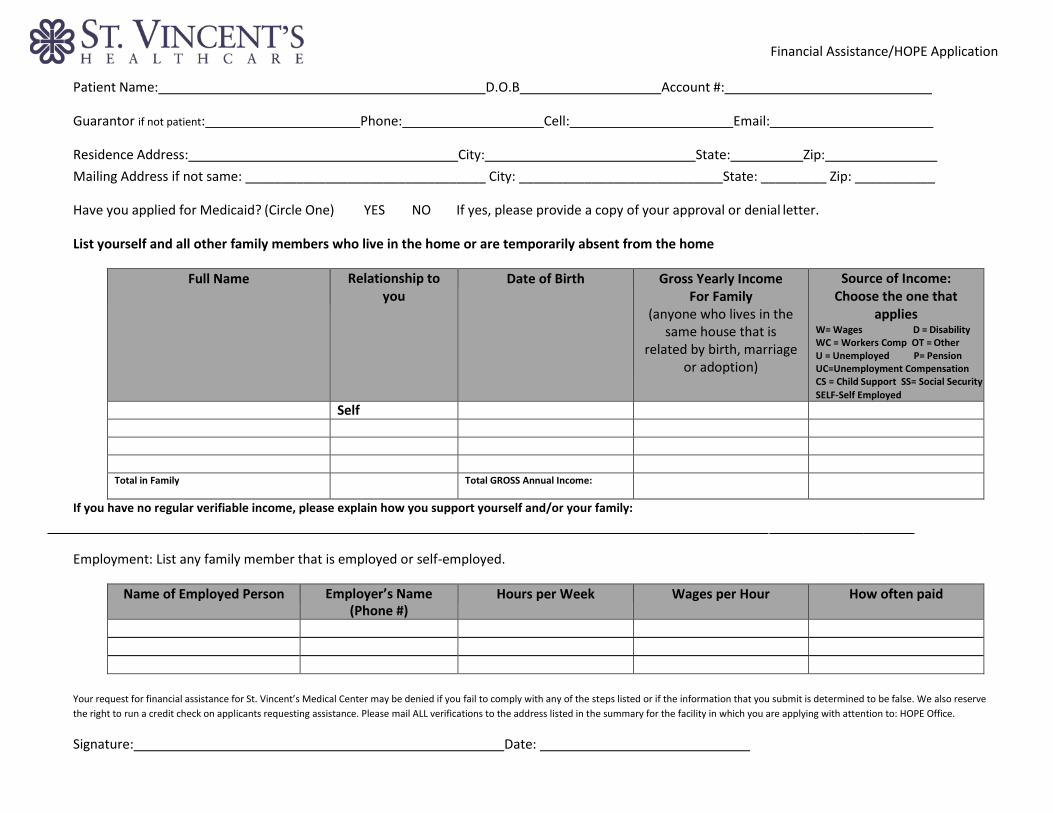
Financial Assistance/HOPE Application
Patient Name: D.O.B Account #:
Guarantor if not patient: Phone: Cell: Email:
Residence Address: City: State: Zip:
Mailing Address if not same: _________________________________ City: ____________________________State: _________ Zip: ___________
Have you applied for Medicaid? (Circle One) YES NO If yes, please provide a copy of your approval or denial letter.
List yourself and all other family members who live in the home or are temporarily absent from the home
Full Name
Relationship to you
Date of Birth Gross Yearly Income For Family
(anyone who lives in the same house that is
related by birth, marriage or adoption)
Source of Income: Choose the one that
applies W= Wages D = Disability WC = Workers Comp OT = Other U = Unemployed P= Pension UC=Unemployment Compensation CS = Child Support SS= Social Security
SELF-Self Employed
Self
Total in Family Total GROSS Annual Income:
If you have no regular verifiable income, please explain how you support yourself and/or your family:
Employment: List any family member that is employed or self-employed.
Name of Employed Person Employer’s Name (Phone #)
Hours per Week Wages per Hour How often paid
Your request for financial assistance for St. Vincent’s Medical Center may be denied if you fail to comply with any of the steps listed or if the information that you submit is determined to be false. We also reserve
the right to run a credit check on applicants requesting assistance. Please mail ALL verifications to the address listed in the summary for the facility in which you are applying with attention to: HOPE Office.
Signature: Date:
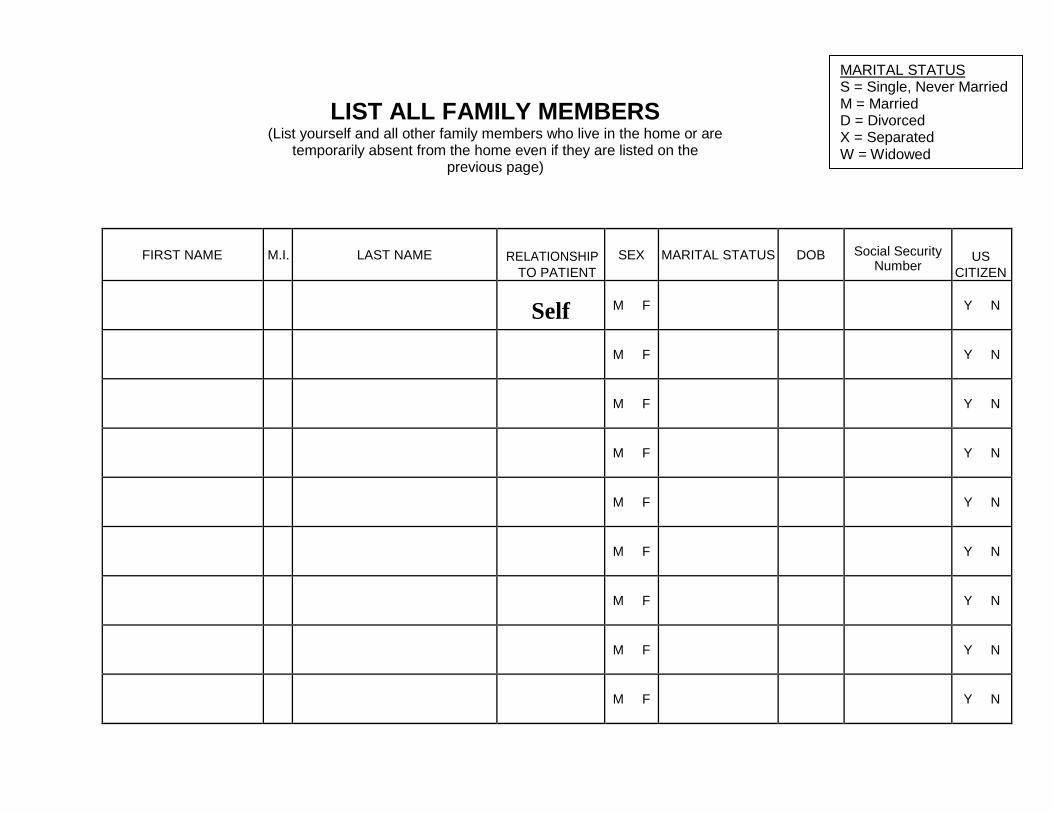
FIRST NAME
M.I.
LAST NAME
RELATIONSHIP
TO PATIENT
SEX
MARITAL STATUS
DOB
Social Security
Number
US
CITIZEN
Self
M F
Y N
M F
Y N
M F
Y N
M F
Y N
M F
Y N
M F
Y N
M F
Y N
M F
Y N
M F
Y N
MARITAL STATUS S = Single, Never Married M = Married D = Divorced X = Separated W = Widowed
LIST ALL FAMILY MEMBERS (List yourself and all other family members who live in the home or are
temporarily absent from the home even if they are listed on the previous page)
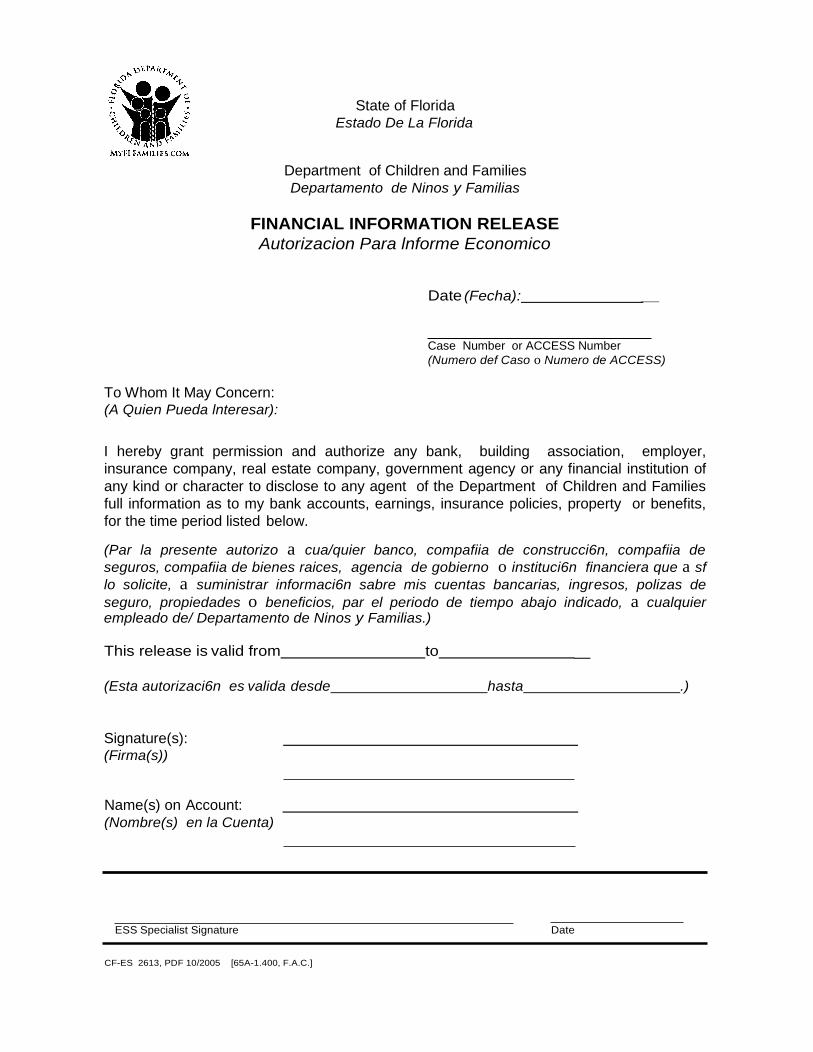
State of Florida Estado De La Florida
Department of Children and Families
Departamento de Ninos y Familias
FINANCIAL INFORMATION RELEASE
Autorizacion Para lnforme Economico
Date (Fecha): _
Case Number or ACCESS Number
(Numero def Caso o Numero de ACCESS)
To Whom It May Concern: (A Quien Pueda lnteresar):
I hereby grant permission and authorize any bank, building association, employer,
insurance company, real estate company, government agency or any financial institution of
any kind or character to disclose to any agent of the Department of Children and Families
full information as to my bank accounts, earnings, insurance policies, property or benefits,
for the time period listed below.
(Par la presente autorizo a cua/quier banco, compafiia de construcci6n, compafiia de
seguros, compafiia de bienes raices, agencia de gobierno o instituci6n financiera que a sf
lo solicite, a suministrar informaci6n sabre mis cuentas bancarias, ingresos, polizas de
seguro, propiedades o beneficios, par el periodo de tiempo abajo indicado, a cualquier empleado de/ Departamento de Ninos y Familias.)
This release is valid from to _
(Esta autorizaci6n es valida desde hasta .)
Signature(s): (Firma(s))
Name(s) on Account:
(Nombre(s) en la Cuenta)
ESS Specialist Signature Date
CF-ES 2613, PDF 10/2005 [65A-1.400, F.A.C.]
St. Vincent’s HealthCare
P.O. Box 45167
Jacksonville, FL 32232
Date:
Designated Representative
I, understand that by submitting my signature I am
(Patient Name)
authorizing the Georgia Division of Family and Children Services (DFCS) to release information to
St. Vincent's Health System and their representatives. This release is made to St. Vincent's
Health System and Care Coverage, a division of R1 and shall be used solely to fulfill their
obligation in assisting me with my Medicaid application. Information to be released is limited to:
Status of application (approved, denied, enrolled or pending)
Reason for closure or denial
Scheduled interview dates and time
Verifications requested and dates due
Patient Signature Financial Counselor’s Name and Phone #
Medical Record Number
Case Number
APPOINTMENT OF A DESIGNATED REPRESENTATIVE
Customer’s Name
Completed by Customer
I would like for to act on my behalf in determining my Name of Representative
eligibility for public assistance from the Department of Children and Families.
Signature of Customer Date
Completed by Representative
I understand that by accepting this appointment, I am responsible to provide or assist in providing information needed to establish this person’s eligibility for assistance. I understand that I may be prosecuted for perjury and/or fraud if I withhold information or intentionally provide false information.
Signature of Representative Date
Relationship to Customer Street Address
City State
Phone Number
Self-Appointment by Representative
I am acting for in providing information to establish eligibility for assistance because he/she is unable to act on his/her own behalf. I will provide information to the best of my knowledge. I understand that if I withhold information or if I intentionally provide false information, I may be prosecuted for perjury and/or fraud. I agree to immediately report any change in their situation of which I become aware.
Signature of Representative Date
Relationship to Customer Street Address
City State
Phone Number
CF-AA 2505, PDF 03/2008

HIPAA AUTHORIZATION FORM
AUTHORIZATION FOR USE OR DISCLOSURE OF PROTECTED HEALTH INFORMATION
Patient Name:
Patient Birth Date:
I, [Name of Patient] hereby authorize any physician, hospital, nursing facility, clinic, treatment center,
therapist, or other health care professional or provider who has treated me to disclose any and all of
my protected health information to Care Coverage, a division of R1, to assist me in applying for health
insurance coverage. I authorize Care Coverage to use and disclose my protected health information to
provide me this assistance.
The protected health information that is covered by this authorization includes (a) all my diagnostic
and treatment records, including any and all records related to my diagnosis or treatment of drug or
alcohol abuse, mental illness, or human immunodeficiency virus (HIV); and (b) all records related to
payment for my health care items or services.
This authorization shall be in force and effect for one year.
I understand that I may revoke this authorization at any time by sending written notice of revocation to
R1 Care Coverage at 26533 Evergreen Rd., Suite #700, Southfield, Michigan 48076. I understand that a revocation is not effective to the extent that Care Coverage or any health care provider has already relied upon my authorization for the use or disclosure of my protected health information.
I understand that information used or disclosed pursuant to this authorization may be disclosed by the
recipient and may no longer be protected by federal or state law.
My health care provider(s) will not condition my treatment on whether I provide authorization for the
requested use or disclosure.
Signature of Patient
Date
1
AUTHORIZATION OF PATIENT REPRESENTATION AND RELEASE OF INFORMATION
FROM: (PATIENT’S NAME) _____________________________________________
I hereby designate Care Coverage a service of R1 RCM Inc., its agents and employees (“Care Coverage a service of R1 RCM”)
to act on my behalf solely for the purpose of obtaining or modifying health care coverage for me and/or members of my
household before any health care provider, financial institution, life insurance company, place of employment, county/state
Department of Human Services, the Social Security Administration (and any legal counsel I may engage to represent me in a
Social Security Administration case), mental health institution and the Veterans Administration.
I expressly consent to the disclosure and release of the following information to Care Coverage a service of R1 RCM by any of
the person(s) and/or organization(s) named above:
1) Medical records, including psychiatric /mental health reports, reports relating to drug, alcohol, and HIV/AIDS;
2) Financial information, including bank statements, life insurance policies, and employment/payroll documentation;
and
3) Other documents and information pertaining to me and/or members of my household that may be relevant to health
care coverage.
I authorize Care Coverage a service of R1 RCM to take any and all steps to obtain a) health care coverage for me and/or members
of my family and b) the documentation needed to secure such coverage. I understand that Care Coverage a service of R1 RCM
makes no guarantees or warranties that it will be able to secure health insurance/Medicaid/Medicare coverage for me, and I
understand that even if coverage is secured, I will remain responsible for any and all unpaid balances for health care services
rendered.
I further authorize Care Coverage a service of R1 RCM to disclose and/or release information they receive from any of the
person(s) and/or organization(s) named above solely for the purpose of modifying or obtaining healthcare coverage for me and/or
members of my household.
I have had full opportunity to read and understand the contents of this authorization, and I confirm that the contents are consistent
with my direction to the person(s) and/or organization(s) named above and to Care Coverage a service of R1 RCM. I understand
that by signing this authorization, I am confirming such person(s) and/or organization(s) may disclose and/or release my
information to Care Coverage a service of R1 RCM and that Care Coverage a service of R1 RCM may in turn disclose such
information for the limited purpose of modifying or obtaining health care coverage.
The authorizations will be in effect until health care coverage is approved, a final determination is made that I am not eligible for
any health care coverage, or I withdraw the authorizations contained in this document by providing written notice to Care
Coverage a service of R1 RCM.
______________________________ ____________
Patient Name (print) Signature Date
______________________________ _________________________________ _____________
Authorizing Person if other than Patient Signature Date
_____________________________________________________________
Street Address
_____________________ _____ _______________ ________________________
City State Zip Phone
________________________________ _____________________________________
Hospital / Admit Date Witness Signature (if patient unable to sign)
________________________________
R1 RCM, Inc. Representative
2
INSTRUCTIONS: Please provide two additional contacts that R1 RCM Inc. can speak to on your behalf regarding your health
insurance/Medicaid/Medicare case:
AUTHORIZATION TO DISCUSS HEALTH CARE COVERAGE
I hereby authorize R1 RCM Inc. to use or disclose information related to my health care coverage with the
individuals listed below. This authorization will be in effect until health care coverage is approved, a final
determination is made that I am not eligible for any health care coverage, or I withdraw this authorization by
providing written notice to R1 RCM Inc.
Name: ________________________
Relationship to Patient: ____________________________
Phone: _____________________________
Name: ________________________
Relationship to Patient: _____________________________
Phone: ____________________________
______________________________ ____________
Patient Name (print) Signature Date
______________________________ _________________________________ _____________
Authorizing Person if other than Patient Signature Date
_____________________________________________________________
Street Address
_____________________ _____ _______________ ________________________
City State Zip Phone
________________________________ _____________________________________
Hospital / Admit Date Witness Signature (if Patient unable to sign)
________________________________
R1 RCM, Inc. Representative

FINANCIAL ASSISTANCE AGREEMENT
Please read before signing. Initial the small line at the beginning of each paragraph.
All information obtained will be utilized by our Patient Accounts staff to help resolve your financial
obligation to St. Vincent’s HealthCare. All questions asked and information requested will be utilized to
determine eligibility for potential funding sources such as Medicaid, HCRA, etc. and remain confidential. I
CERTIFY I am uninsured or underinsured and the information I have provided is true and accurate to the best
of my knowledge. I will make application for ANY and ALL ASSISTANCE which may be available through
federal, state, local government and private sources to help pay this hospital bill and will take all action
necessary to obtain assistance from the above sources.
I understand that if I do not cooperate with St. Vincent’s HealthCare (Herein known as SVHC) within 45
days from the date of service in requesting ANY additional information, my application may be denied for
possible financial assistance. I hereby designate SVHC’s Patient Accounts Department as my representative to
act on my behalf and assist in the application process and/or appeal of my application for any medical
assistance program.
I authorize a representative from SVHC Patient Accounts to file an application which includes my
electronic signature, receive any and all information from the Department of Children and Families regarding
the status, disposition, eligibility or denial of my application for medical assistance and to file a Fair Hearing
Appeal against the Department of Children and Families if a disagreement arises with the disposition of the
application. I also grant permission for a Patient Accounts representative to assist in obtaining a certified
copy of a birth or death certificate for myself or a member of my immediate family in order to continue the
application process. A copy of the designation of representative shall remain in effect for one (1) year or until
otherwise advised by the SVHC Accounts Department or myself. I acknowledge receipt of Rights and
Responsibilities, if applicable.
I will ASSIGN to SVHC ALL FUNDS received from the above sources, which are provided to help with
the HOSPITAL BILL. I, on my own behalf, and for my immediate family member(s), authorized
representative(s), physician(s), counselor(s) (including clergy) and attorney(s), agree to hold and maintain in
strict confidence any written communications and/or oral discussions between me and SVHC, regarding
matters relating to services provided to me by SVHC.
I understand that the information which I submit is subject to verification by SVHC,
including credit reporting agencies, and subject to review by FEDERAL and/or STATE AGENCIES
and others as required. I AUTHORIZE my employer to release to SVHC proof of my income. I
UNDERSTAND that if any information I have given proves to be untrue, SVHC will re-evaluate my
financial status and take whatever action becomes appropriate.
I hereby certify that the above information is true and correct to the best of my knowledge. In
accordance with s.817.50 F.S., providing false information to defraud a hospital for goods and services is a
misdemeanor in the second (2nd) degree. St. Vincent’s HealthCare can require income tax information or
investigate wages with employer to validate eligibility.
Patient Signature: _ Date:
Guarantor if other than patient:
Hospital Representative:
Date:
Date:

RMS Admin
Rectangle

Affidavit of Support
I, ___________________________, declare that I am presently unemployed and
have received $_________ income for the past ________ months/years, from
__________ to __________.
I currently live at ____________________________________________________.
My food and living expenses are provided by ______________________________
who is my _____________________.
_______________________ ________ ______________________ ________
St. Vincent’s Medical Center PO Box 2982
Jacksonville, FL
(Patient Name)
(Start Date) (Ending Date)
(Address)
(Provider Name)
(Relationship to Patient)
(Patient Signature) (Provider Signature) (Date) (Date)

HOPE PROGRAM
HOMELESS ATTESTATION FORM
Patient Name: ______________________________ DOB: _______________________________
Last 4 of SSN: _______________ SSN Verified (Y/N): ____________
___ I am currently a homeless individual and am allowed to receive mail at the following
address:
_____________________________________________________________________________
_____________________________________________________________________________
___ I receive food stamps in the amount of $________________ per month.
___ I am unemployed and have had no income for the last _____ months.
PATIENT
I hereby attest that my response to the applicable preceding statement is true, complete and
accurate. By signing this Attestation, you certify that you have read this Attestation or that it
has been read to you and applied a valid, legal signature.
_______________________________ _____________ __________________________
Patient Signature Date Phone Number
Homeowner/Leasee
Please have the homeowner/leasee of the home where you are allowed to receive mail
complete this section:
I _____________________________ attest that _______________________ is currently
homeless and is allowed to receive mail at my home address listed above.
_______________________________ _____________ __________________________
Resident Signature Date Phone Number