Patient Preparation and Coronary CTA Techniques
47
Patient preparation and coronary CTA techniques Gregory Kicska, M.D. Ph.D. University of Washington, Thoracic Imaging
Transcript of Patient Preparation and Coronary CTA Techniques

Patient preparation and coronary CTA techniques
Gregory Kicska, M.D. Ph.D.University of Washington, Thoracic Imaging

Overview
1. Patient preparation2. Scanning techniques

Patient preparation
Preparation related to any contrast CT examination
Preparation specific to coronary CTA

Exclude contraindications
Patient safety
Study quality

Contrast
renal insufficiency
allergy (anaphylaxis)
Radiation
pregnancy
radiation dose/age
Claustrophobia
Medically unstable
Contraindications: patient saftey

Contrast
renal insufficiencycreatinine measurement before intravenous contrast mediainjection are summarized in Table 4. Most centers employ aserum creatinine threshold of 1.5 mg/dl for detection ofpatients at high risk for contrast-induced nephrotoxicity.However, considerable derangement of renal function canbe masked by a normal appearing serum creatinine report.Hence, the current recommendation is to screen high-riskpatients with estimated glomerular filtration rate (GFR).Derangement of GFR can occur in a patient due toundetected chronic renal disease though the creatininemeasurements are normal. The Modification of Diet inRenal Disease (MDRD) study group equation is anaccurate method for GFR estimation from serum creatinine[27]:
GFR !186" serum creatinine# $% 1:154" age# $ % 0:203" k
For women, k=0.742; for men, k=1Multiply by 1.210 if African-AmericanThe risk of contrast-induced nephrotoxicity based on
estimated GFR is summarized in Table 5. Recently, somevendors are investigating rapid strip-test-based methods forquick measurement of serum creatinine when patients arrivefor contrast-enhanced radiological studies [28]. Such methodsto estimate serum creatinine can enable efficient detection ofpatients at risk for contrast-induced nephrotoxicity.
Metformin therapy and the risk of lactic acidosis
When patients taking metformin receive iodinated contrastmedia, they are at risk for lactic acidosis. If renaldysfunction occurs due to iodinated contrast media, anaccumulation of metformin can occur and cause lacticacidosis. According to the American College of Radiology(ACR) guidelines, metformin should be discontinued at thetime of an examination or procedure using intravascularcontrast media, withheld for 48 h after the procedure, andreinstated only after renal function has been re-evaluatedand found to be normal [3]. However, the examination mayproceed even if the patient took a dose of metformin on themorning of the examination.
Administration of contrast media to pregnant patients andnursing mothers
When given in usual clinical doses, iodinated contrastmedia cross the human placenta and enter the fetus [3]. Noadequate and well-controlled teratogenic studies of theeffects of these agents in pregnant women have beenperformed. While it is not possible to conclude thatiodinated contrast media present a definite risk to the fetus,there is insufficient evidence to conclude that they pose norisk. The ACR recommends that iodinated contrast mediamay be given to pregnant patients only when [3]:
– the diagnostic information requested using contrast-enhanced study cannot be obtained via other means(such as ultrasound)
– the information needed affects the care of the patientand fetus during the pregnancy
– it is not prudent to wait to obtain this information untilafter the patient is no longer pregnant
Less than 1% of iodinated contrast media is excreted intobreast milk, out of which only 1% is absorbed by theinfant’s gut. According to ACR recommendations, it is safefor the mother and infant to continue breast-feeding afterreceiving contrast media [3]. However, if the motherremains concerned about any potential ill effects to theinfant, she may abstain from breast-feeding for 24 h [3].
Conclusion
Prompt recognition and treatment are invaluable inblunting an adverse response of a patient to contrastmedia, and may prevent a reaction from becoming severeor even life-threatening. Proper patient evaluation andprocedure selection, and adequate prophylactic measurescan prevent some adverse reactions. Knowledge, training,and preparation are crucial for appropriate and effectivetherapy in the event of an adverse reaction. Radiologistsand their staff need to review the treatment algorithmsregularly so that each can accomplish his or her roleefficiently.
Table 4 Indications for serum creatinine measurement beforeintravenous administration of iodinated contrast media
History of kidney diseaseFamily history of renal failureDiabetes treated with insulin or other medications prescribed by aphysicianMyelomaCollagen vascular diseaseMedications: metformin, non-steroidal anti-inflammatory drugs,aminoglycosides
Table 5 Risk of contrast induced nephrotoxicity based on estimatedglomerular filtration rate (GFR)
GFR (ml/min/1.73 m2)
Risk of contrast inducednephrotoxicity
Intravenous iodinatedcontrast media
60 Negligible Safe30–60 Moderate Use only if clinically
essential prophylaxisrequired
<30 High Contraindicated
214
Contraindications: patient saftey

Contrast
renal insufficiency
creatinine measurement before intravenous contrast mediainjection are summarized in Table 4. Most centers employ aserum creatinine threshold of 1.5 mg/dl for detection ofpatients at high risk for contrast-induced nephrotoxicity.However, considerable derangement of renal function canbe masked by a normal appearing serum creatinine report.Hence, the current recommendation is to screen high-riskpatients with estimated glomerular filtration rate (GFR).Derangement of GFR can occur in a patient due toundetected chronic renal disease though the creatininemeasurements are normal. The Modification of Diet inRenal Disease (MDRD) study group equation is anaccurate method for GFR estimation from serum creatinine[27]:
GFR !186" serum creatinine# $% 1:154" age# $ % 0:203" k
For women, k=0.742; for men, k=1Multiply by 1.210 if African-AmericanThe risk of contrast-induced nephrotoxicity based on
estimated GFR is summarized in Table 5. Recently, somevendors are investigating rapid strip-test-based methods forquick measurement of serum creatinine when patients arrivefor contrast-enhanced radiological studies [28]. Such methodsto estimate serum creatinine can enable efficient detection ofpatients at risk for contrast-induced nephrotoxicity.
Metformin therapy and the risk of lactic acidosis
When patients taking metformin receive iodinated contrastmedia, they are at risk for lactic acidosis. If renaldysfunction occurs due to iodinated contrast media, anaccumulation of metformin can occur and cause lacticacidosis. According to the American College of Radiology(ACR) guidelines, metformin should be discontinued at thetime of an examination or procedure using intravascularcontrast media, withheld for 48 h after the procedure, andreinstated only after renal function has been re-evaluatedand found to be normal [3]. However, the examination mayproceed even if the patient took a dose of metformin on themorning of the examination.
Administration of contrast media to pregnant patients andnursing mothers
When given in usual clinical doses, iodinated contrastmedia cross the human placenta and enter the fetus [3]. Noadequate and well-controlled teratogenic studies of theeffects of these agents in pregnant women have beenperformed. While it is not possible to conclude thatiodinated contrast media present a definite risk to the fetus,there is insufficient evidence to conclude that they pose norisk. The ACR recommends that iodinated contrast mediamay be given to pregnant patients only when [3]:
– the diagnostic information requested using contrast-enhanced study cannot be obtained via other means(such as ultrasound)
– the information needed affects the care of the patientand fetus during the pregnancy
– it is not prudent to wait to obtain this information untilafter the patient is no longer pregnant
Less than 1% of iodinated contrast media is excreted intobreast milk, out of which only 1% is absorbed by theinfant’s gut. According to ACR recommendations, it is safefor the mother and infant to continue breast-feeding afterreceiving contrast media [3]. However, if the motherremains concerned about any potential ill effects to theinfant, she may abstain from breast-feeding for 24 h [3].
Conclusion
Prompt recognition and treatment are invaluable inblunting an adverse response of a patient to contrastmedia, and may prevent a reaction from becoming severeor even life-threatening. Proper patient evaluation andprocedure selection, and adequate prophylactic measurescan prevent some adverse reactions. Knowledge, training,and preparation are crucial for appropriate and effectivetherapy in the event of an adverse reaction. Radiologistsand their staff need to review the treatment algorithmsregularly so that each can accomplish his or her roleefficiently.
Table 4 Indications for serum creatinine measurement beforeintravenous administration of iodinated contrast media
History of kidney diseaseFamily history of renal failureDiabetes treated with insulin or other medications prescribed by aphysicianMyelomaCollagen vascular diseaseMedications: metformin, non-steroidal anti-inflammatory drugs,aminoglycosides
Table 5 Risk of contrast induced nephrotoxicity based on estimatedglomerular filtration rate (GFR)
GFR (ml/min/1.73 m2)
Risk of contrast inducednephrotoxicity
Intravenous iodinatedcontrast media
60 Negligible Safe30–60 Moderate Use only if clinically
essential prophylaxisrequired
<30 High Contraindicated
214Contraindications: patient saftey

Radiation
pregnancy
radiation dose/age
Contraindications: patient saftey

Claustrophobia
Diazapam 5 mg oral*
Medically unstable
*Dose adjustment needed specific conditions
Contraindications: patient saftey

Contraindications: study qualityMotion
Breath hold
Gating
Artifact
Inability to raise arms
Metal
Obesity

Contraindications: study qualityMotion
Breath hold (7-12 sec @ 64 slice)
270 ms acquisition dual source

Contraindications: study qualityMotion
Gating
atrial fibrillation or frequent PVCs

Contraindications: study quality Artifact
Inability to raise arms
Metal
Obesity

The ideal patient
HR < 65, sinus
Calm
Thin
Large veins
Pearl diver (able to hold breath)
Able to follow commands

No caffeine (24 hrs)No viagra (24 hrs)No “energy supplement” (24 hrs)No food (4 hrs)No liquid (1 hr)
Preparation: 24-1 hr pre-exam

Cardiac medications should not be suspended!
Preparation: 24-1 hr pre-exam

Non-anaphylactic contrast reaction•50 mg prednisone @ 13,7,1 hrs before exam
•oral Benadryl 1 hour before exam
Preparation: 24-1 hr pre-exam

•IV access•18 - 20 gauge needle•Right arm
Preparation: 1 hr pre-exam

Satisfactory IV accessContraindications excluded / mitigated
Preparation: 1 hr pre-exam
Proceed to HR control

Satisfactory IV accessContraindications excluded / mitigated
Preparation: 1 hr pre-exam
Proceed to HR control

Contraindications Metoprolol allergy
Bronchospastic disease (asthma)Aortic valve disease
Worsening heart failureHeart block
Oral metoprolol (50 mg tabs)50-100 mgWait 90 minutes, check BP/HRConsider additional 50 mg
IV metoprolol (5 mg)Give 5 mg IVPWait 20 minutes, check BP/HRConsider additional 5 mg x 2
Preparation: 1 hr pre-exam

Preparation: 1 hr pre-exam

Preparation: 1 hr pre-exam
Beta blocker contraindication? Consider oral Verapamil

HR < 65 bpm
Preparation: 1 hr pre-exam
Proceed to Ca++ score

Center heart in scanner
Examination: patient positioning

Center heart in scanner
Examination: patient positioning
= Lowest noise

Center heart in scanner
Examination: patient positioning
= Lowest noise

Ca++ score coverage
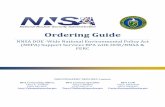
Examination: Ca++ score

Examination: Ca++ scoreVoxels are 3 x 1.3 x 1.3 mmnon-overlapping
Threshold of 130 H.U.
Agatston volumemass score

> 400-1000 - high risk of stenosis= 0 - CAD unlikely
Ca++ Score Sensitivity Specificity
>1
>100
>1000
92% 75%
73% 90%
30% 98%
Predicting Stenosis
Low false negative
No false positiveLow sensitivity on CTA
Examination: Ca++ score

Examination: Ca++ score0 < Agatston score < 400-1000
Proceed to CTA planning

Retrospective, dose modulation
Retrospectiveno modulation
Retrospectivewith modulation
Prospective
Old - HR 92, BP 110/60, Weight 260 lbs,Temp 37
New - HR 80, BP 98/60
Examination: gating

Retrospective, dose modulation
Retrospectiveno modulation
Retrospectivewith modulation
Prospective
Old - HR 92, BP 110/60, Weight 260 lbs,Temp 37
New - HR 80, BP 98/60
Prospective RetrospectiveModulation
Rate < 70no functionno calciumAge < 40
Rate > 70functioncalcium
Age > 40
RetrospectiveNo modulation
A-fib

Ca++ score coverage
Examination: CTA coverage
Top slice with CA
Bottom slice with CA
Coronary CTA coverage (retrospective)

Ca++ score coverage
Examination: CTA coverage
Top slice with CA
Bottom slice with CA
Coronary CTA coverage (prospective)

Set kVp and MAS.
Automatic exposure control
set desired held soon in its standard deviation
set upper and lower limits to avoid spikes in current due to hardware
Weight table
Examination: dose

Examination: dose

Examination: dose
Participate in dose related QA

80 ml5 ml/s
40 ml4 ml/s
50 ml4 ml/s
100%60%
100%40%
Examination: contrast

ContraindicationsHead trauma/bleedSystolic BP < 100Nitrate AllergyPhosphodiesterase inhibitors
AdverseHeadaches - 50%
Examination: nitroglycerin

4 minutesExamination: nitroglycerin

4 minutes elapsed
Proceed to CTA scanning
Examination: nitroglycerin

Examination: scanning

Examination: reconstruction
Main reconstruction for 3D station
Thin section (0.625 mm) axial cardiac kernal< 32cm FOV50% overlap

Examination: reconstruction
Additional reconstruction for 2D station
•Axial 2.5 mm, lung kernel, lung FOV•Axial 2.5 mm, body kernel, body FOV•Coronal/sagittal, body kernel

Conclusions
• Exclude contraindications related to patient safety or exam quality• ensure proper patient preparation for contrast exam• control heart rate with beta blocker• calcium scoring is used to plan CTA or terminate exam• scanner gating is one of the most effective ways to reduce dose• utilize automatic exposure control when possible

Thank you