Patient Pathways...New Zealand Out-of-Hospital STEMI Pathway: Lower North Island Area Notify the...
46
Patient Pathways Horowhenua Territory Central South District Version 3, July 2019
Transcript of Patient Pathways...New Zealand Out-of-Hospital STEMI Pathway: Lower North Island Area Notify the...

Patient PathwaysHorowhenua TerritoryCentral South District
Version 3, July 2019


CENTRAL SOUTH PATIENT PATHWAYS | 1
ContentsNew Zealand Out-of-Hospital STEMI Pathway: Lower North Island Area 4
Acute stroke destination policy: Lower North Island 9
Spinal cord injury destination policy 13
Major Trauma destination policy: Lower North Island Area 19
Falls prevention pathway 23
POAC patient referral pathway 26
Raukawa Whanau Ora – Māori Health Provider Referral Pathway 29
STAR 4 Ward Community Admission 32
Horowhenua smoking cessation referral pathway 33
Safe to talk – He pai ki te kōrero 35
Caring Caller referrals 36
St John Medical Alarm referrals 39
Telehealth Services 42
Produced by: National Patient Pathways Team Version number: 3 Date issued: July 2019

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS2

CENTRAL SOUTH PATIENT PATHWAYS | 3Version: 3Date issued: July 2019
Central South Patient PathwaysDear clinicians,
Contained within this folder are the patient pathways available within your district. Please make yourself familiar with each pathway and its supporting information.
Referral pathways for low acuity patients (also known as Safe and Well) are important in ensuring that we are delivering the right care at the right time. Due to an ageing and bulging population and an increase in chronic illness, the vast majority (81%) of our patients are classified as minor or moderate (status 3 and 4) and thus developing efficient and effective ways of managing patients in the community (where appropriate) is crucial.
Patient pathways are also vital in ensuring we provide appropriate care for high acuity patients with major trauma, spinal cord injury and other life-threatening conditions.
If you have questions relating to any pathways, or wish to suggest a new pathway, please speak with your line manager and/or Territory Manager.
Thank you for everything you do for our patients.
Yours sincerely,
Steve Yanko
District Operations Manager Central South District Central Region
Johnny Mulheron
Clinical Practice Manager Central Region
Kris Gagliardi
National Patient Pathways Manager

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS4
New Zealand Out-of-Hospital STEMI Pathway: Lower North Island Area
Notify the dispatcher of “code STEMI” if air transport is being considered1
Transmit 12 lead ECG to the Clinical Desk
� Enter the patient’s surname, NHI number and a call-back cell phone number in the ECG
Complete fibrinolytic therapy/PCI checklist
Is the patient in or south of the Otaki Area?
Commence transport to Wellington Regional Hospital ASAP
� If helicopter transport is required, confirm activation of the helicopter crew and helicopter meeting point with the dispatcher
� Minimise time on scene and transport expediently
� Phone the on-call doctor for St John via the Clinical Desk ASAP to confirm hospital destination and advise patient’s details and the ETA3
If the destination is Wellington Regional Hospital, transmit 12 lead ECG to Wellington Regional Hospital
(CR15)
Notify receiving hospital personnel en route
Administer fibrinolytic therapy ASAP if all answers to the fibrinolytic therapy/
PCI checklist questions are “no” 2
Phone the on-call doctor for St John via the Clinical Desk to discuss hospital
destination and begin transport to designated hospital ASAP
Notes:
� 1 The dispatcher will notify personnel on the Air Desk, who will then phone ambulance personnel at the scene and advise of helicopter availability and estimated flight time to Wellington Regional Hospital.
� 2 Personnel must seek clinical advice prior to administering fibrinolytic therapy if any of the answers to the checklist questions are “yes” or “uncertain”.
� 3 The on-call doctor for St John will liaise with the on-call cardiologist at Wellington Regional Hospital. The on-call cardiologist will activate the catheter lab.
YES NO
Fibrinolytic therapy pathwayPrimary PCI pathway

CENTRAL SOUTH PATIENT PATHWAYS | 5Version: 3Date issued: July 2019
New Zealand Out-of-Hospital STEMI Pathway: Lower North IslandAdditional information
Introduction � This pathway is for the use of personnel in the out-of-hospital setting (for example St John and primary
care personnel), when treating patients with ST elevation myocardial infarction (STEMI) in the Lower North Island of New Zealand and should be read in conjunction with the Ambulance Sector Clinical Procedures and Guidelines (CPGs).
� The goal of this pathway is to ensure that patients with STEMI receive prompt reperfusion therapy and that there is a consistent approach to determining which reperfusion therapy patients receive.
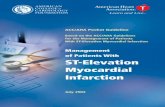
Guideline summary � Primary percutaneous coronary intervention (primary PCI) is the preferred reperfusion strategy provided
the patient is in or south of the Otaki Area as per appendix one.
� Fibrinolytic therapy should be administered as soon as possible (unless contraindicated) if the patient is north of the Otaki Area as per appendix one.
� Patients receiving fibrinolytic therapy will be transported to a hospital with the facilities for immediate PCI from the scene whenever it is feasible and safe to do so, provided the patient is eligible for rescue PCI in the event of failed reperfusion.
Pathway steps
1 Notify the dispatcher of “code STEMI” if helicopter transport is being considered
� Personnel must call the dispatcher by radio and notify “code STEMI” if helicopter transport is being considered. The dispatcher must be informed of:
– The hospital the patient is likely to be transported to and
– The cell phone number for Air Desk personnel to call.
� The dispatcher must immediately notify Air Desk personnel of the incident. Air Desk personnel will phone personnel at the scene to advise helicopter availability and the estimated flight time to Wellington Regional Hospital.
� Ambulance personnel will use this information to determine the transport time to Wellington Regional Hospital prior to phoning the on-call doctor for St John.
2 Transmit 12 lead ECG � If it is clear the patient has STEMI, the 12 lead ECG must be transmitted to the Clinical Desk whenever
possible.
� Ensure the patient’s surname, NHI (if known) and a call-back cell phone number are entered into the 12 lead ECG before transmission.
New
Zea
land
Out
-of-
Hos
pita
l STE
MI P
athw
ay: L
ower
Nor
th Is
land

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS6
� Significant time should not be spent attempting to troubleshoot failed ECG transmission. If the ECG cannot be transmitted after brief troubleshooting, personnel must proceed to the next step in the chosen reperfusion pathway.
3 Complete fibrinolytic therapy/PCI checklist � Personnel must complete the fibrinolytic therapy/PCI checklist prior to proceeding with the chosen
reperfusion pathway.
� Personnel must seek clinical advice from the on-call doctor via the Clinical Desk on 0800 111 HELP (0800 111 4357) prior to the administration of fibrinolytic therapy if the answer to any of the checklist questions is “yes” or “uncertain”.
4 Follow appropriate reperfusion pathway (primary PCI or fibrinolytic therapy)
Primary PCI pathway � Ambulance personnel should commence transport to Wellington Regional Hospital ASAP (while phoning
the on-call doctor for St John) if the patient is in or south of the Otaki Area as per appendix one.
� Ambulance personnel will phone the on-call doctor for St John via the Clinical Desk on 0800 111 HELP (0800 111 4357) ASAP (preferably before leaving the scene) to confirm hospital destination and advise them of the patient’s details, including:
– Surname, age and NHI (if known).
– Time of symptom onset.
– 12 lead ECG findings.
– Summary of the patient’s overall condition.
– Expected time of arrival.
– Ensure there is explicit discussion if the answer to any of the checklist questions is “yes” or “uncertain”.
� The on-call doctor for St John will liaise with the on-call cardiologist at Wellington Regional Hospital. The on-call cardiologist at Wellington Regional Hospital will activate cardiac catheter lab personnel.
� Personnel will transmit the 12 lead ECG to Wellington Regional Hospital (CR15).
� En route to hospital, personnel transporting the patient will phone the on-call cardiologist at Wellington Regional Hospital on 04 385 5999 approximately 30 minutes prior to arrival to re-confirm the expected time of arrival and where in the hospital the patient is expected (for example, the catheter lab or emergency department).
� If the patient is expected in the emergency department, personnel transporting the patient must phone emergency department personnel on 04 385 5813 to advise that a patient with STEMI on the primary PCI pathway is inbound.
� The patient should be transferred directly to the cardiac catheter lab on the ambulance stretcher, provided cardiac catheter lab staff are ready.
Fibrinolytic therapy pathway � If the patient is north of the Otaki Area, personnel will administer fibrinolytic therapy if all the answers
to the checklist questions are “no”. Personnel must seek clinical advice prior to administering fibrinolytic therapy if any of the answers to the checklist questions are “yes” or “uncertain”.
� The patient must be transported to a medical facility with personnel able to administer fibrinolytic therapy if there will be a significant delay in the arrival of ambulance or PRIME personnel able to do this.

CENTRAL SOUTH PATIENT PATHWAYS | 7Version: 3Date issued: July 2019
� If the patient is being transported to a medical facility for fibrinolytic therapy:
– Staging should be activated via the dispatcher ASAP and preferably before leaving the scene.
– Personnel in the receiving medical facility must be notified ASAP (and preferably before leaving the scene) that staging has been activated.
� If staging is occurring at a medical centre:
– The patient should remain in the ambulance if possible.
– The patient should remain on the ambulance stretcher if taken into the medical centre if possible.
� Following the administration of fibrinolytic therapy, personnel will phone the on-call doctor for St John via the Clinical Desk to discuss hospital destination and inform them of the patient’s details as above. The on-call doctor will liaise with receiving hospital specialists and advise ambulance personnel of the destination hospital.
� If the destination is Wellington Regional Hospital, personnel will transmit the 12 lead ECG to Wellington Regional Hospital (CR15).
� En route to hospital personnel transporting the patient will phone receiving hospital personnel approximately 30 minutes prior to arrival to provide an update on the patient’s condition and re-confirm the expected time of arrival:
– If the destination is Wellington Regional Hospital, personnel will phone the Ward 6 South coordinator on 021 504 746 and proceed to Ward 6 South.
– If the destination is Nelson Hospital, personnel will phone the on call-cardiologist at Nelson Hospital on 0800 CARDIAC (0800 227 3422) and confirm where in the hospital the patient is expected.
New
Zea
land
Out
-of-
Hos
pita
l STE
MI P
athw
ay: L
ower
Nor
th Is
land

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS8
Appendix one: Approximate PPCI and fibrinolytic therapy catchment areas
Wellington
Palmerston North
Whanganui
Featherston
Napier
Wairoa
Hastings
Otaki
Foxton
Primary PCI zone
Fibrinolytic therapy zone
Levin

CENTRAL SOUTH PATIENT PATHWAYS | 9Version: 3Date issued: July 2019
Acute stroke destination flowchart: Lower North Island
New Zealand Out-of-Hospital Acute Stroke Policy: Lower North Island Area | 2017Page 2 of 6
Acute Stroke Destination Flowchart: Lower North Island Area
Does the patient have signs or symptoms of an acute stroke?
Can the patient be transported to a stroke hospital within four hours of the onset of symptoms?
Transport to the most appropriate stroke hospital:
� Hawke’s Bay Regional Hospital. � Whanganui Hospital. � Palmerston North Hospital. � Wairarapa Hospital. � Hutt Hospital. � Wellington Regional Hospital.
Stroke is unlikely, treat appropriately without
using this policy.
Transport to the most appropriate hospital.
NO
NO
Notify hospital personnel ASAP and provide the following information as a minimum:
� FAST results and � Time of symptom onset and � NHI number (if known).
On arrival at hospital:
� Leave the patient on the ambulance stretcher during handover.
� Convey the patient to the CT scanner (accompanied by hospital personnel) if requested to do so, provided this will not cause an undue delay.
YES
YES
Acu
te s
trok
e de
stin
atio
n po
licy:
Low
er N
orth
Isla
nd

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS10
New Zealand Out-of-Hospital Acute Stroke Policy: Lower North Island Area | 2017Page 3 of 6
Acute Stroke Destination Policy: Lower North Island Area Additional information
Introduction � This policy is for the use of personnel in the out-of-hospital setting (for example ambulance and primary
care personnel), when determining the transport destination for patients with an acute stroke and should be read in conjunction with the New Zealand Ambulance Sector Clinical Procedures and Guidelines.
� The goal of this policy is to optimise outcomes for patients with acute ischaemic stroke by minimising the time to administration of fibrinolytic therapy when this is indicated.
� All patients with signs or symptoms of stroke who can reach a stroke hospital within four hours of the onset of symptoms may be eligible for fibrinolytic therapy and should be transported directly to a stroke hospital without delay whenever it is feasible and safe to do so.
� Although this policy has primarily been designed for the out-of-hospital setting, the principles within it could be used by personnel in the in-hospital setting.
� This policy does not apply to patients with trauma. Patients with acute trauma and signs or symptoms of an acute stroke should be treated using the New Zealand Major Trauma Policy.
Stroke hospitals � The term ‘stroke hospital’ is used to describe a hospital that has the appropriate facilities and personnel to
assess patients with an acute stroke and provide fibrinolytic therapy.
� The role of receiving personnel in stroke hospitals is to rapidly assess patients for their suitability to receive fibrinolytic therapy and to initiate fibrinolytic therapy without delay when it is indicated.
� The following hospitals are designated as stroke hospitals: – Hawke’s Bay Regional Hospital. – Whanganui Hospital. – Palmerston North Hospital. – Wairarapa Hospital. – Hutt Hospital. – Wellington Regional Hospital.
� Wellington Regional Hospital is the tertiary stroke hospital.
Determining the most appropriate stroke hospital � A patient with an acute stroke who can be transported to a stroke hospital within four hours of the onset
of symptoms should usually be transported to the nearest stroke hospital.
� However, clinical judgement should be used and if the patient is located an approximately equal transport time between Wellington Regional Hospital and another stroke hospital, the patient should usually be transported to Wellington Regional Hospital which is a tertiary stroke hospital. This is because tertiary stroke hospitals have additional personnel and facilities to manage patients with an acute stroke.
Acute stroke destination policy: Lower North IslandAdditional information

CENTRAL SOUTH PATIENT PATHWAYS | 11Version: 3Date issued: July 2019
New Zealand Out-of-Hospital Acute Stroke Policy: Lower North Island Area | 2017Page 4 of 6
� A patient with signs or symptoms of an acute stroke who cannot be transported to a stroke hospital within four hours of the onset of symptoms is unlikely to be eligible to receive fibrinolytic therapy and should be transported to the most appropriate hospital (which may not be a stroke hospital), taking into account:
– The patient’s anticipated clinical needs and – The location of the incident and – Where the patient lives.
Patient assessment and treatment � Ambulance personnel will use the Ambulance Sector Clinical Procedures and Guidelines.
� Clinical assessment of the patient must include an assessment for new onset of unilateral weakness and new onset of impaired speech. The FAST test is recommended:
– Face: ask the patient to smile and look for unilateral facial weakness. – Arm: ask the patient to raise both arms and close their eyes. Look for unilateral arm weakness or
unilateral drift. – Speech: ask the patient to repeat a sentence and listen for slurring of words. Ask the patient to name
several common objects and observe for difficulty naming objects. – Time: note the time of the onset of symptoms.
� The time of the onset of symptoms is the time at which the patient was last known to be symptom free. If the patient has woken with the signs or symptoms, then the time of the onset of symptoms is the time the patient was last known to be awake and symptom free.
� Examination for leg weakness is not part of the FAST assessment, however observing the patient walking (provided this is feasible and safe) may detect leg weakness or poor coordination. Poor coordination may result from a stroke within the cerebellum.
� Hypoglycaemia can cause signs and symptoms that mimic a stroke and these may persist for many hours following treatment. If the patient is hypoglycaemic or has received treatment for hypoglycaemia, the patient should not be treated using this policy.
� Seizures can cause signs and symptoms that mimic a stroke, particularly during the postictal phase and these may persist for many hours following the seizure. If the patient has had a seizure the patient should not be treated using this policy.
� IV access should be obtained, noting that: – Bilateral IV access is preferred provided this does not cause a significant delay and – 18 and 20 gauge cannulae are sufficient and – Multiple IV attempts should be avoided.
� Hospital personnel must be notified by ambulance personnel as soon as possible and preferably before leaving the scene so that appropriate personnel can be notified of the patient’s impending arrival. The following information should be provided as a minimum:
– FAST results and – Time of symptom onset and – NHI number (if known).
� Transport under lights should occur if doing so will result in a clinically significant time saving.
Transport timeframes � Four hours from the onset of symptoms has been chosen as the ‘cut off’ time for transport to a stroke
hospital. This is because evidence suggests there is no benefit (and possibly harm) from administering fibrinolytic therapy after four and a half hours from the onset of symptoms.
� Utilising a four hour time window from the onset of symptoms to arrival in a stroke hospital allows an additional thirty minutes for hospital personnel to assess the patient and commence fibrinolytic therapy if indicated.
Acu
te s
trok
e de
stin
atio
n po
licy:
Low
er N
orth
Isla
nd

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS12
New Zealand Out-of-Hospital Acute Stroke Policy: Lower North Island Area | 2017Page 5 of 6
Transport modes � Transport to hospital should usually be by road ambulance.
� Transport to hospital by helicopter should be reserved for patients with the greatest potential to benefit from fibrinolytic therapy, utilising the following criteria:
– The patient is previously independent and without severe comorbidities and – The diagnosis is clear and – The patient has severe weakness and – The patient will clearly reach a stroke hospital within four hours of the onset of symptoms and – Helicopter transport will clearly save more than thirty minutes compared with road transport.
� Personnel requiring advice on helicopter transport should phone personnel on the Clinical Desk within the Ambulance Communications Centre on 0800 111 HELP (0800 111 4357).
On arrival at a stroke hospital � On arrival at a stroke hospital, ambulance personnel should leave the patient on the ambulance stretcher
during handover and convey the patient to the CT scanner (accompanied by hospital personnel) if requested to do so. If an undue delay occurs or is anticipated prior to conveying the patient to the CT scanner, the patient should be transferred to a hospital bed.
� Once the patient has been transferred to the CT scanner, the ambulance stretcher should be removed and ambulance personnel are not required to remain with the patient.
� Exact arrangements at each stroke hospital will vary depending on locally agreed processes between stroke hospital personnel and the ambulance service. The goal of conveying the patient to the CT scanner on the ambulance stretcher is to reduce the time to fibrinolytic therapy when indicated.
Transport post fibrinolytic therapy � In the event that ambulance personnel are required to transport a patient with an acute stroke following
fibrinolytic therapy, personnel must: – Record the patient’s GCS, blood pressure, heart rate and capillary refill time every 10 minutes. – Monitor the patient closely for signs of bleeding. – Seek clinical advice if there is any significant change in the patient’s condition.

CENTRAL SOUTH PATIENT PATHWAYS | 13Version: 3Date issued: July 2019
Spin
al c
ord
inju
ry d
esti
nati
on p
olic
y
Spinal cord injury destination policyFlowchart for prehospital personnel
Does the patient have acute spinal cord injury with signs of paraplegia
or quadriplegia?
Does the patient have signs of major trauma in addition to spinal cord
injury?
Does the patient have inadequate breathing or shock?
Is it feasible to transport the patient directly to a SCI centre* by road?
Is it feasible to fly the patient directly to a SCI centre*?
Transport the patient to the most appropriate major trauma hospital
This policy does not apply. See the District Destination Policy.
Transport the patient to the most appropriate major trauma hospital
Transport the patient directly to a SCI centre* by road
Fly the patient directly to the most appropriate SCI centre*
> Middlemore Hospital (adults)
> Christchurch Hospital (adults and children)
> Starship Children’s Hospital (children)
* Spinal Cord Impairment (SCI) centres

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS14
Spinal cord injury destination policyAdditional information
Introduction This information complements the spinal cord injury destination policy flowchart for prehospital personnel and should be read in conjunction with it. This policy describes the process for prehospital personnel to determine which hospital patients with spinal cord injury should be transported to.
One of the main principles within the National Spinal Cord Impairment Action Plan is that patients with spinal cord impairment (SCI) following trauma should be treated in a designated SCI centre as soon as possible after their injury. Patient outcomes are optimised when surgery (if indicated) to decompress the spinal cord is performed urgently and this is usually only feasible when patients are transported directly to a designated SCI centre. From a prehospital perspective this means that:
> Patients with spinal cord injury and no other signs of major trauma will be transported directly from the scene to a SCI centre, whenever this is feasible. This means that even in a metropolitan setting that is close to another major hospital, patients will be transported directly to a SCI centre even if that SCI centre is a significant distance away.
> Patients with other signs of major trauma in addition to spinal cord injury will be transported to the most appropriate major trauma hospital and then secondarily referred to a SCI centre when clinically appropriate.
Patients not covered by this policy > Patients with non-traumatic spinal cord impairment are not covered by this policy. They will be
transported to the most appropriate hospital and then secondarily referred to a SCI centre when clinically appropriate.
> Inter-hospital referrals and inter-hospital transfers are not covered by this policy.
Defining spinal cord injury in the prehospital setting > For the purposes of this policy, signs of spinal cord injury require the patient to have signs of paralysis
with either paraplegia or quadriplegia.
> Altered sensation and/or weakness (without paralysis) are not sufficient because it is relatively common for patients in the prehospital setting to have these symptoms in the absence of spinal cord injury. Transporting such patients directly to a SCI centre risks large numbers of patients being inappropriately transported to a SCI centre that do not require it.
Mechanism of injury > The decision to transport a patient directly to a SCI centre is not affected by the mechanism of injury.
> However, if the mechanism involves high velocity (for example a high speed road crash) and another major trauma hospital is significantly closer to the scene than a SCI centre, it is vital to exclude other signs of major trauma prior to making a decision to transport the patient directly to a SCI centre.
Other signs of major trauma in addition to spinal cord injury > The patient must be transported to the most appropriate major trauma hospital (and then secondarily
referred to a SCI centre when clinically appropriate) if there are any signs of major trauma in addition to that of spinal cord injury.
> Personnel must seek clinical advice if they are uncertain.

CENTRAL SOUTH PATIENT PATHWAYS | 15Version: 3Date issued: July 2019
Spin
al c
ord
inju
ry d
esti
nati
on p
olic
y
> All of the SCI centres are within hospitals that are also designated as major trauma hospitals and thus patients with additional injuries will receive appropriate treatment at the SCI centres.
> See the major trauma destination policy for further details.
The adequacy of breathing > If breathing is clinically inadequate the patient must be transported to the most appropriate major
trauma hospital and then secondarily referred to a SCI centre when clinically appropriate.
> Clinically inadequate breathing is uncommon in the prehospital setting following spinal cord injury and usually only occurs with a high cervical cord injury.
> Most patients with diaphragmatic breathing following spinal cord injury have clinically adequate breathing but an inadequate cough. In this setting the patient should be transported directly to a SCI centre provided this is feasible, the patient has adequate oxygenation with supplemental oxygen and their breathing is not deteriorating.
Shock > If shock is present the patient should be transported to the most appropriate major trauma hospital
(and then secondarily referred to a SCI centre when clinically appropriate) because the patient should be presumed to have hypovolaemic shock until proven otherwise.
> Loss of sympathetic outflow from the spinal cord following spinal cord injury can cause shock and in this setting the patient is usually vasodilated below the site of injury. It is appropriate to consider transporting the patient directly to a SCI centre if personnel are confident the patient has spinal shock (particularly if the mechanism of injury involved low velocity) and the patient is clearly not deteriorating, but personnel must seek clinical advice in this setting.
Transport to a SCI centre by road > It is usually only feasible to transport a patient directly to a SCI centre by road when the patient is injured
in, or around the fringes of, the Auckland district and the Canterbury district.
> In the Auckland district:
– adults should be transported to Middlemore Hospital unless there is a compelling clinical reason to transport them to Auckland City Hospital instead.
– children should be transported to Starship Hospital unless there is a compelling clinical reason to transport them to Middlemore Hospital instead.
> On the fringes of the Auckland district (for example the southern area of Northland and the northern area of Waikato and Hauraki), if helicopter transport is not indicated (or is not available), it is preferable to transport the patient directly to a SCI centre by road, rather than transporting to Whangarei Hospital or Waikato Hospital. This is because a secondary transfer incurs a clinically significant delay that may worsen the patient’s outcome.
> In the Canterbury district the only hospital suitable for patients with major trauma is Christchurch Hospital and all patients should be transported there directly.
Transport to a SCI centre by helicopter > If it is not feasible to transport a patient directly to a SCI centre by road, the patient should be transported
directly to a SCI centre by helicopter, provided a helicopter is available and it is feasible to do so. This will occur even if another major hospital is substantially closer. In many metropolitan areas of New Zealand this will involve the patient being driven to a helicopter base (or rendezvous point) that may be very close to (or onsite at), a major hospital and then flying the patient directly to a SCI centre, without the patient entering that major hospital. Provided a helicopter is available and it is feasible to fly to the SCI centre, this is preferable to the patient being transported to that major hospital and then secondarily transferred. This is because such a secondary transfer incurs a clinically significant delay that may worsen the patient’s outcome.

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS16
> If the flight involves the patient ‘overflying’ another major trauma hospital, it is essential that helicopter personnel re-evaluate the patient prior to flight, in order to ensure that there are no other signs of major trauma in addition to spinal cord injury. Personnel must have a very low threshold for seeking clinical advice if they are uncertain.
> If a helicopter is not available within a suitable time frame, or it is not feasible (for example due to weather) to fly to a SCI centre, the patient will be transported to the most appropriate major trauma hospital and then secondarily referred to a SCI centre when clinically appropriate. A ‘suitable time frame’ cannot be tightly defined and requires clinical judgement. If a helicopter is not immediately available personnel should seek clinical advice regarding the options for transport and the destination.
> Refueling may be required en route to a SCI centre. This is preferable to flying to another major trauma hospital and the patient being secondarily transferred.
> It is not usually feasible to transport a patient by fixed wing aircraft. In very unusual circumstances a fixed wing aircraft may be used, but in this setting personnel must seek clinical advice.
> The patient must be removed from extrication devices (such as a spine board, scoop stretcher or combi-carrier) and transported directly on the stretcher, unless the total time on the extrication device is going to be less than thirty minutes.
> Additional care must be taken to ensure the patient is kept warm.
> Urinary catheterisation is not required.
Seeking clinical advice > Personnel requiring advice will contact the doctor on call for the ambulance service via the Clinical Desk
within the Ambulance Clinical Control Centre.
> In the event that further advice is required, the doctor on call for the ambulance service will contact the on call spinal consultant within the appropriate SCI centre.
Communication with receiving hospital staff > No specific additional communication is required with receiving hospital staff other than the usual
notification process for a patient with major trauma, however this notification should occur with as much advance warning as possible.
SCI centre catchment areas and transport destination > New Zealand has three designated SCI centres and each has an associated catchment area. They are:
– Middlemore Hospital for adults (15 years or older) from the upper two thirds of the North Island (orange area on the map on page 9).
– Christchurch Hospital for adults (15 years or older) from the lower third of the North Island (yellow area on the map on page 9) and all of the South Island.
– Starship Hospital for children (younger than 15 years) from all areas of New Zealand.
> Patients will be preferably transported to the catchment area SCI centre, provided it is feasible to do so. This means that some patients will be flown to a SCI centre that is not the closest SCI centre to the scene, particularly when the scene is in the upper part of the area marked in yellow on the map. This is preferable to always flying to the closest SCI because it is important to balance the patient load between the SCI centres and this reduces secondary inter-hospital transfers.
> It will not always be feasible to fly the patient to the catchment area SCI centre. In particular, it is not always feasible to fly an adult from the lower third of the North Island to Christchurch Hospital and it is rarely feasible to fly a child from the South Island directly to Starship Hospital. Thus, for the purposes of prehospital decision making, the patient will be transported to the most appropriate SCI centre and then referred (if required) to the catchment area SCI centre.

CENTRAL SOUTH PATIENT PATHWAYS | 17Version: 3Date issued: July 2019
Spin
al c
ord
inju
ry d
esti
nati
on p
olic
y
The following will be taken into account when determining which SCI centre the patient is transported to:
– the catchment area boundaries and the location of the scene
– the location and availability of helicopters
– the weather
– where the patient lives.
> Examples:
– An adult in the orange area will usually be flown to Middlemore Hospital.
– An adult in the yellow area will usually be flown to Christchurch Hospital.
– An adult in the South Island will usually be flown to Christchurch Hospital.
– A child in the North Island will usually be flown to Starship Hospital.
– A child in the South Island will usually be flown to Christchurch Hospital and then secondarily referred to Starship Hospital when clinically appropriate. This is because Christchurch Hospital is a SCI centre with the staff and facilities to provide urgent decompressive surgery if required.
> Personnel must seek clinical advice if they are uncertain which SCI centre the patient should be transported to.

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS18
Spinal cord injury destination policyCatchment area boundaries
Key
Middlemore Hospital
Christchurch Hospital
Starship Hospital (all of NZ)

CENTRAL SOUTH PATIENT PATHWAYS | 19Version: 3Date issued: July 2019
Major Trauma Destination Policy | Lower North Island Area | 2017Page 2 of 5
Major Trauma Destination FlowchartLower North Island Area
Closest appropriate medical facility. Activate
staging if this is not a major trauma hospital
Wellington Regional HospitalPalmerston North Hospital
Hawkes Bay Regional HospitalWhanganui Hospital
Consider:Wellington Regional Hospital
Palmerston North HospitalHawkes Bay Regional Hospital
Whanganui Hospital
Starship Hospital (children)Christchurch Hospital (adults)
Are any of the following present?
• Manageable airway obstruction• Respiratory distress• Shock• Motor score less than or equal to five
• Penetrating trauma to the neck or torso• Crush injury to the neck or torso• Flail chest• Penetrating trauma to a limb with arterial injury• More than one long bone fracture• Crushed, amputated, mangled or pulseless limb• Clinically obvious pelvic fracture• Burns involving the airway• Burns >20% of body surface area
• Paraplegia or quadriplegia*
Wellington Regional Hospital
YES
YES
YES
Are any of the following present?
• Intubated and ventilated for severe TBI• Lateralising neurological signs• Clinically obvious penetrating brain injury• Complex multi-system trauma
NO
Is a life threatening problem present requiring immediate medical intervention?
YES
NO
Are additional risk factors present?
Most appropriate medical facility
NO
NO
YES
Note:* Refer to the Spinal Cord Injury Destination Policy.
YES Maj
or tr
aum
a de
stin
atio
n po
licy
Major Trauma Destination Policy: Lower North Island Area

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS20
Major Trauma Destination Policy: Lower North Island AreaAdditional Information
Introduction > This policy is for the use of personnel in the out-of-hospital setting, when determining the transport
destination for patients with major trauma within the Lower North Island Area of New Zealand.
> It should be read in conjunction with the Major Trauma Destination Flowchart for the Lower North Island Area, the New Zealand Out-of-Hospital Major Trauma Triage Policy, the National Major Trauma Network Staging Guidelines and the New Zealand Spinal Cord Injury Destination Policy.
> The goal of the policies is to ensure that patients with major trauma are transported directly to the most appropriate major trauma hospital, whenever it is feasible and safe to do so.
Major trauma hospitals > The following hospitals are designated to receive patients with major trauma:
– Hawkes Bay Regional Hospital.
– Whanganui Hospital.
– Palmerston North Hospital.
– Wellington Regional Hospital.
> Wellington Regional Hospital is the tertiary major trauma hospital.
Determining the most appropriate major trauma hospital > The flowchart describes the preferred major trauma hospital/s, based on the best descriptor of the
patient’s clinical condition.
> The patient should be transported to the preferred major trauma hospital as described in the flowchart, whenever it is feasible and safe to do so.
> If it is not feasible or safe to transport the patient to the preferred major trauma hospital or more than one major trauma hospital is listed as an option, the patient should be transported to the most appropriate major trauma hospital. This will usually be the nearest major trauma hospital, but it may be appropriate to transport the patient to another major trauma hospital if that hospital has the most appropriate facilities to meet the patient’s needs.
> Personnel will determine the most appropriate major trauma hospital taking into account all of the following:
– The nature of the patient’s known injuries.
– The patient’s anticipated clinical needs.
– The facilities at the major trauma hospitals it is feasible and safe to transport to.
– The location of the incident.
– The transport modes available and the effect of weather on helicopter transport.
– The transport times to the major trauma hospitals it is feasible and safe to transport to.
– The other patients being transported from the scene, particularly if the number of patients is significant.

CENTRAL SOUTH PATIENT PATHWAYS | 21Version: 3Date issued: July 2019
Maj
or T
raum
a D
esti
nati
on P
olic
y
> Personnel should have a low threshold for seeking clinical advice if:
– The transport time to the chosen major trauma hospital is significantly longer (this is not defined and requires clinical judgement) than the transport time to the nearest major trauma hospital or
– Transport to the chosen major trauma hospital will involve bypassing (or over flying) another major trauma hospital.
Life threatening problems requiring immediate medical intervention
> The patient should be transported to the closest appropriate medical facility if they have a life threatening problem requiring immediate medical intervention that cannot be provided by personnel at the scene.
> Clinical judgement is required when determining that the medical facility is appropriate, but the medical facility must have the personnel and facilities to provide the required medical intervention.
> Personnel must activate staging via Control/Comms if the medical facility is not a major trauma hospital, preferably before leaving the scene.
> Personnel in the receiving medical facility must be notified as soon as possible of the intent to stage at the medical facility, preferably before leaving the scene.
Severe traumatic brain injury (TBI) likely to require urgent neurosurgery
> Most patients with severe TBI do not require urgent neurosurgery. However, patients with a high probability of requiring urgent neurosurgery will usually benefit from being transported to a major trauma hospital with neurosurgical facilities.
> A patient with severe TBI and any of the following clinical features should be transported to Wellington Regional Hospital whenever it is feasible and safe to do so:
– Has been intubated and ventilated or
– Has lateralising neurological signs (for example unilateral pupil dilatation or unilateral weakness) or
– Has a clinically obvious penetrating brain injury.
> Personnel should have a low threshold for seeking clinical advice if transport to Wellington Regional Hospital will involve bypassing (or over flying) another major trauma hospital, particularly if the patient is not intubated and ventilated.
Complex multi-system trauma > Patients with complex multi-system trauma will usually benefit from transport to a tertiary major trauma
hospital. This is because tertiary major trauma hospitals have additional facilities and personnel to manage patients with complex multi-system trauma.
> Complex multi-system trauma cannot be tightly defined and clinical judgement is required, but includes patients with major trauma involving very severe injuries to more than one body region.
> It is preferable to transport a patient with complex multi-system trauma to Wellington Regional Hospital provided the transport time is not significantly longer (this is not defined and requires clinical judgement) than the transport time to the closest major trauma hospital. However, the nature of the geography of the Lower North Island is such that patients with complex multi-system trauma will usually be transported to the nearest major trauma hospital.

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS22
Burns > Patients with burns greater than 20% of body surface area should usually be transported to the nearest
major trauma hospital and then be subsequently referred to a Burn Centre. This is because some patients will be referred to Middlemore Hospital (the National Burn Centre).
> However, it is preferable to transport patients with burns greater than 20% of body surface area to Wellington Regional Hospital, provided the transport time is not significantly longer (this is not defined and requires clinical judgement) than the transport time to the closest major trauma hospital.
> Patients with burns greater than 20% of body surface area are transported to Wellington Regional Hospital and not to Hutt Hospital. This is because Wellington Regional Hospital is a major trauma hospital and Hutt Hospital is not.
> Burns less than or equal to 20% of body surface area and burns involving the face (without airway burns), hands or genitals may require treatment in a Burn Centre, but in the absence of major trauma these are not time critical and the patient should usually be transported to the most appropriate hospital and be subsequently referred if required.
Major trauma hospitals outside the Lower North Island Area > It may be occasionally appropriate for the patient to be flown to a major trauma hospital outside the
Lower North Island Area. For example, in the northern aspect of the Lower North Island it may be appropriate for the patient to be flown to Waikato Hospital, particularly if the patient:
– Has been intubated and ventilated for severe TBI or
– Has lateralising neurological signs (for example unilateral pupil dilatation or unilateral weakness) or
– Has a clinically obvious penetrating brain injury or
– Has complex multi-system trauma.
> Personnel should have a low threshold for seeking clinical advice if a patient is being flown outside the Lower North Island Area.

CENTRAL SOUTH PATIENT PATHWAYS | 23Version: 3Date issued: July 2019
Falls
pre
vent
ion
path
way
Falls prevention pathway: Flowchart
Falls prevention pathway | January 2019 | page 1 of 1
Falls prevention pathway
Patient has fallen (including slip, trip or stumble), does not meet any of the exclusion criteria and:
Once the ePRF has been submitted, the referral will be sent to the Falls Prevention Service via the Referrals Coordinator.
Ask the patient for permission to refer them to the Falls Prevention Service.
This includes consent to send all relevant medical history.
Notify the patient that they will be contacted via phone to arrange the appropriate falls prevention service.
Complete ePRF including telephone number and GP practice details. Please write as much
additional info as possible including if the patient can leave the house unassisted, past falls, trip hazards, social history, use of walking aids etc.
Note in ePRF that patient does not consent to falls
referral
In disposition notes, write referral@falls
> Lives independently in their own home or retirement village and
> Is aged 65 years or over and
> Does not require transport to hospital (note: patients transported toUrgent Care Clinics and GP practices can still be referred).

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS24
Falls prevention pathwayFalls prevention pathwayFalls are the most common cause of injury in New Zealand. People over the age of 65 have a one in three chance of falling, and one in five of those will suffer serious injury.
The falls prevention pathway is an opportunity to refer patients that have fallen, or are at risk of falling. The referral is to link these patients with local services that can work with them to increase their strength and balance, and help prevent future falls.
Who should be referred?Anybody who:
> has fallen (including a slip, trip or stumble) or
> is at risk of falling and
> lives independently in their own home or retirement village (rest home patients are excluded) and
> is aged 65 years or older and
> is not being transported to hospital.
Who should not be referred?For the referral to be accepted, the patient must be able to participate in an exercise programme. For this reason, there will be some patients who are not appropriate to refer despite meeting the eligibility criteria.
Do not refer patients who:> Have cognitive impairment e.g. dementia
> Are palliative
> Are wheelchair bound or amputees – this is because the programme requires the person to be able tostand up and participate
> Have any degenerative type conditions like Multiple Sclerosis (MS) or Motor Neurone Disease (MND)where the patient will struggle to participate in an exercise programme
> Have fallen as a result of a stroke, where the patient has ongoing support needs
> Are significantly visually impaired/blind
> Are of an advanced age – use your clinical judgement around whether you think the patient wouldactually benefit from being referred e.g. a 99 year old, mostly bed bound, unable to mobiliseindependently, multiple co-morbidities would not be appropriate for a falls referral
If you are concerned about your patient being a falls risk but they are not appropriate for the falls prevention pathway, please contact the GP/Nurse to discuss further options.
Why only non-transported patients?The pathway has been set up to refer non-transported patients because the receiving hospital should make the referral for any patient that has fallen and is transported. However:
> Patients being transported to a GP practice or an Urgent Care Clinic can still be referred.
> Patients who have not fallen can also be referred if you believe they are at risk of falls. For example, apatient who cannot get out of their chair without using their arms, has had recent falls or avoids activitiesdue to a fear of falling.

CENTRAL SOUTH PATIENT PATHWAYS | 25Version: 3Date issued: July 2019
Falls
pre
vent
ion
path
way
How to make a referralType referral@falls in the Disposition Notes on ePRF.
What happens following a referral to the falls prevention programme?The referral will be sent to the Referrals Coordinator who will determine what level of support the patient requires. This will depend largely on the detail recorded by the crew in the ePRF. The referral will then be sent to the most appropriate service to action.
If the patient can leave the house unassisted: They will be referred to a local community Strength and Balance class. These are exercise based community classes run by qualified physiotherapists with an emphasis on improving the patient’s strength and balance. These classes usually run for 12 weeks and provide a great social element for those people who might otherwise be isolated.
If the patient can’t leave the house unassisted: They will be referred to the In-Home Strength and Balance programme, which is carried out in the patient’s own home by a physiotherapist. The patient will undertake a strength and balance exercise programme that is designed specifically for them, and will be followed up with further home visits and phone support. Equipment and referrals to relevant agencies can also be provided if required.
N.B. There may be a small charge to the patient to participate in the community programmes, but the service will discuss this on initial contact with them.
Important information in the ePRF > Because initial contact between the Falls Prevention Service and the patient is by phone, please make sure you
include a phone number.
> It is also important that you include as much additional information as possible in the disposition section ofePRF including social history, family support, previous falls, trip hazards, use of walking aids, etc.
> Please include the patients GP details as well, so if the falls referral is declined they can still be referred to theGP for a follow up. GP details should be recorded in the disposition section of the ePRF.
Referring other members of the household > When assessing an elderly patient who has fallen, there may be another member of the household (e.g.
patient’s spouse) who has recently fallen or is at risk of falls (e.g. very frail, uses a walking aid, has reducedmobility). It is appropriate to refer other members of the household who may benefit from referral.
> When referring other members of the household, complete a second ePRF by selecting “Add Patient” in thePatient Information section of ePRF. Select “ACC” case type to ensure the patient does not receive a bill.
> Type “referral@falls” in the disposition notes to trigger a referral.
> An ePRF for someone who is not the primary patient can be less detailed, but should include a telephonenumber and relevant background information related to the patient’s falls risk, as described above.
Other informationBefore considering leaving a patient who has fallen at home, it is important that the patient is safe to stay at home as per the CPGs. The falls referral pathway must not be used to determine whether transport to a medical facility is required.
Referrals should always be primarily for patients requiring falls prevention support and not medical support. For example, if a patient is at risk of having falls due to dizziness, hypotension or cognitive deterioration then they should be encouraged to see their GP. The GP may then subsequently refer to the falls prevention service if it is appropriate.

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS26
Exclusion criteria
> Less than 16 years of age
> The patient is not clinically safe to be managed in the community
> GCS less than 15 (unless this is normal for the patient)
> Ineligible for NZ funded health services
> Asthma (adult or child) requiring repeated bronchodilators without improvement
POAC patient referral pathway
Assess and treat patient as per CPGs
Patient requires urgent clinical review and staff believe the patient
can be safely and appropriately managed at a POAC facility
Is the patient status 3 or 4? Do they meet the inclusion criteria and are
unlikely to be referred on to hospital?
If the patient consents to transport to a POAC facility then call the
appropriate clinic to discuss the patient and book an appointment if
possible/necessary.Ask to speak to the POAC champion.
> Patient given ACS advice sheet with ‘POAC’ written at top of form
> Advise patient to contact registered GP or POAC facility within 12 hours of St John assessment and present the ambulance ACS sheet on arrival
Inclusion criteria
> Aged 16 years or older
> Patient is eligible to access funded New Zealand health care services
Specified conditions
> Cellulitis
> Deep vein thrombosis (DVT)
> COPD
> Gastroenteritis
> Asthma
> Lower Respiratory Tract Infection
> Urinary retention (requiring acute catheterisation or a blocked catheter)
> Non-specifically unwell
> Iron deficiency anaemia
Transport patient to POAC facility (see next page). Handover to clinical
personnel on arrival
Patient is not eligible for POACEnsure ‘POAC’ is recorded in the Disposition Notes of ePRF
Assessed as safe to self transport

CENTRAL SOUTH PATIENT PATHWAYS | 27Version: 3Date issued: July 2019
POAC facilitiesTe Waiora Community Health 10 Ladys Mile Foxton 4814 Triage Nurse: 06 363 8001 (ambulance only)
Masonic Medical Centre 685 Queen Street East, Horowhenua Levin 5510 PH: 06 368 8068
Horowhenua Community Practice 62 Liverpool St Horowhenua Levin 5510 Triage Nurse: 06 368 8539 (ambulance only) PH: 06 368 8065
Cambridge Street Medical 127 Cambridge St Horowhenua Levin 5510 PH: 06 367 0423
Otaki Medical Centre 2 Aotaki St Otaki 5512 PH: 06 364 8555
POA
C pa
tien
t ref
erra
l pat
hway

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS28
POAC patient referral pathwayWhat is POAC? Primary Options for Acute Care (POAC) is a coordination service which aims to give general practice teams and community health services the resources to manage patients with a variety of acute conditions in the community rather than send them to hospital.
Under POAC, these patients may be transported or referred to a POAC accredited facility at no additional cost for the consultation. The POAC service is funded by Mid Central District Health Board and enables ambulance staff to determine the most effective and efficient way to meet the patient’s healthcare needs.
Referring patients to a POAC accredited practice If appropriate, transporting the patient to their own GP should be considered in the first instance. GP practices will only accept currently enrolled patients. If there is no availability or it is outside the GP’s hours, then consider referring the patient to an alternative POAC facility e.g. City Doctors
Staff must phone first and ask to speak to the POAC champion to be accepted, this will likely be a practice nurse. If this is not possible ask to speak to a doctor or nurse before transporting them. It may be requested that the patient is transported to ED if they do not think it is safe or appropriate for the patient to be treated in the community or there is a capacity issue.
The following must be explained to the patient and/or caregivers prior to transport:
> Ambulance personnel are recommending that the patient is transported or referred to their GP or an urgent care clinic, rather than being transported to a hospital ED.
> The patient is still responsible for the bill associated with this ambulance callout (unless it is covered by ACC).
> Any bill from the GP or clinic for this visit will be paid for them under a special funding arrangement.
> If during this visit, they are referred to hospital by the doctor and they require further transport by ambulance, the bill for the extra ambulance transfer will also be paid for them.
Referring patients for self-transport to their GP Where the patient meets referral criteria and has their own transport to safely make their own way to their GP, they may transport themselves and still have their treatment at the GP or clinic paid for by POAC.
If a patient is seen overnight POAC funding will apply if the patient presents within 12 hours to see a GP.
Please indicate on the ePRF that POAC has been initiated and advise the patient they must take the ACS form and any supporting paperwork with them eg. an ECG.

CENTRAL SOUTH PATIENT PATHWAYS | 29Version: 3Date issued: July 2019
Raukawa Whanau Ora – Māori Health Provider Referral PathwayRaukawa Whanau Ora Health Services is a kaupapa Māori Iwi Health Provider. Raukawa Whānau Ora was formed with the vision to maximise our contribution to the survival and wellbeing of Māori as a people through the design and delivery of kaupapa based services. The services are specifically for Māori but do not exclude non-Māori who wish to use them.
Raukawa Whānau Ora focus on delivering holistic services from pepe (baby) through to kaumatua (elder) working collaboratively with other providers (internally & externally) providing accessible, quality health care for the whole whanau, utilising Whanau Ora concept (empowering whanau to take responsibility for their own wellbeing). The area covered is from Te Horo in the South to Manawatu/Palmerston North and Bulls in the North. This includes all outskirts of these areas.
Raukawa Whanau Ora Health Services offers the following services: Whanau /Tamariki Ora Well Child Service
> Well child growth and development checks (0–5) as per the National Well child Schedule, vision and ear assessments and immunisations; and includes assessment of other members of the whanau (family) if requested.
Mother & Pepe Support / Toa Haputanga
> Antenatal and postnatal support, advocacy and advice from conception to 5 years for Young / New Mothers and Parents.
Immunisation Service
> Immunisations as per the National schedule for nga Tamariki aged 3 months to 11 years and adults 45 years and older. FREE influenza vaccinations for those 65 years and over or those under 65 who have chronic disease/disorder such as asthma. Home or clinic.
Whakapiki Hauora
> Adult Mental Health Service – Support for those 17 years and over who have mental health diagnosis
Alcohol & Drug Support (AOD)
> Community support for those of any age affected by alcohol and/or drugs.
Child Adolescent & Family Support
> Community support for 0–17 year olds and their whanau, who have a mental health diagnosis and/or ongoing behavioural challenges.
Day Activities
> Group activities to promote socialisation for individuals 17 years and over who have a mental health diagnosis. Transport provided.
Cervical Screening
> Free clinics and/or home visits.
Māo
ri H
ealt
h Pr
ovid
er R
efer
ral P
athw
ay

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS30
Disease State Management
> For adults with diabetes, heart and respiratory disease states. To assist them and/or their whanau to independently manage the disease state(s) over a 12-month period.
Māori Disability Support Service
> To assist those with disabilities particularly kaumatua (50 years and over) to access Needs Assessment Service Coordinator (Supportlinks). Includes advocacy and liaison.
Cancer Control Coordinator
> Support improved access to services along the continuum of care for clients and their whanau affected by cancer.
Long Term Conditions
> Clinical nursing assessment in homes or within community clinics for clients aged 17 years and older who are suspected of, or diagnosis as having respiratory (breathing) problems.
Who should be referred?Raukawa Whanau Ora Health Services will accept referrals from anyone who identifies Māori, has Māori whanau or would like a Māori philosophy service delivery and suffers from a health issue or health related social issue requiring follow-up.
How to make a referral > Gain consent from the patient/whanau for referral.
> Complete ePRF – clearly stating what the patient’s needs are and/or which service is required.
> Type referral@maorihealth in the Disposition section of ePRF.
> Advise the patient that someone from Raukawa Whanau Ora Health Services will contact them.
What will happen following referral? On receipt of the referral the patient/whanau (family) will be contacted by one of the kaimahi (worker) within the service to arrange a time and date to visit to discuss a care action plan.

CENTRAL SOUTH PATIENT PATHWAYS | 31Version: 3Date issued: July 2019
Assess patient
Complete ePRF – clearly stating what the patient’s needs are and/or which service is required.
Ambulance personnel offer this referral pathway to the patient/client and their whanau.
Explain pathway and gain consent from the patient/whānau referral.
Then do the following:
1. Complete ePRF
2. Type referral@maorihealth in the Disposition section of ePRF
3. Advise the patient that someone from Raukawa Whānau Ora Health Services will contact them
Māo
ri H
ealt
h Pr
ovid
er R
efer
ral P
athw
ay
Raukawa Whanau Ora – Māori Health Provider Referral Pathway

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS32
STAR 4 Ward Community Admission Specialist treatment, assessment and rehabilitation (STAR) 4 Ward is a 20-bed hospital located at the Horowhenua Health Centre in Levin. It has 24-hour nursing and medical officer cover with a geriatrician round twice a week. Most of the admissions come from Palmerston North hospital, however, appropriate community admissions are also accepted to avoid unnecessary ED presentations.
Who can be referred? Status 3 & 4 patients with:
> Chest infection
> UTI
> Cellulitis
> Multiple falls / unsafe mobility
> Frailty / multiple co-morbidities- unsafe to leave at home
> Acute or chronic functional or cognitive decline-unsafe to leave at home
> Palliative / terminal care
> Complex pain
> Suspected spinal / pubic rami fractures
> Poly pharmacy, medical conditions that needs reviewing within a ward environment.
X ray and Med lab facilities (blood tests) are available Mon-Friday 9-3:30pm. IV antibiotics, diuretics and fluids are also available.
Who can NOT be referred: > New fracture that requires orthopaedic input
> Acute respiratory illness
> On renal dialysis programme
> Restlessness, agitation or behaviour requiring 1:1 observation, restraint or a secure environment
> Mental health illness / crises
> Sub-specialty (e.g. gastroenterology, CCU) or shared secondary care services needed (e.g. medical and surgical/ orthopaedic)
> Urgent transfusion needs.
How to refer a patientSTAR 4 will discuss new community admissions between 8.30am and 3.00pm.
Please ring STAR 4 on 06 366 0063 or 027 680 1391 to discuss the potential admission with medical officers Dr Martie Gray, Dr Sherry Martin or charge nurse Diane Hague.
Note: if the patient is well known to STAR 4 and has recently been discharged they will consider this on a case by case basis during the hours after 3pm, early evening and weekends.
If STAR 4 does not have capacity on the day and the patient has good family support it may be possible for STAR 4 to arrange admission when a bed is available.

CENTRAL SOUTH PATIENT PATHWAYS | 33Version: 3Date issued: July 2019
Horowhenua smoking cessation referral pathwayKey factsTobacco is the leading cause of preventable morbidity in New Zealand, accounting for around 5,000 deaths every year. Of this total, 350 people die as a result of second-hand smoke. Smoking contributes significantly to cardiovascular disease, cancer and COPD and adversely affects child health through its direct effects during pregnancy and indirect effects in childhood (e.g. causing respiratory tract infections and asthma).
Who should be referred? Any patient who:
> Smokes and
> Is not being transported and
> Has consented to a referral.
How to make the referralType referral@smoking in the disposition notes and ensure these details are in the ePRF:
> Full name
> Telephone number they can be reached at
> Current address if possible
> If the patient is pregnant, and if so, EDD
> Primary ethnicity.
If the patient declines your offer of cessation support, document this in the ePRF.
What will happen following referral? The client will be contacted within one week by a Quit Coach, who will then discuss with them which local service they would prefer to work with.
Services can provide: > 1:1 face time with a Quit Coach who can help the client to develop a plan and goals specific to them
> Telephone catch ups
> Family and group appointments
> Nicotine Replacement Therapy (NRT) e.g. gum, lozenges and patches as well as information about other smoking cessation medications such as Zyban and Champix
> Follow ups as required
> Rewards for reaching goals e.g. vouchers
> Most importantly, non-judgmental ongoing support for their journey to become smoke free.
Hor
owhe
nua
smok
ing
cess
atio
n re
ferr
al p
athw
ay

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS34
What can I say to help encourage a referral?Ambulance personnel should use the MoH ABC tool when referring:
A: Ask – “Are you currently smoking?”
B: Brief advice – “We are working with our local stop smoking service, can we refer you for some support to quit?”
C: Cessation support – refer as above
Using the ePRF “current smoker” tick box is an easy way to start this conversation, as though you are gathering routine information such as a patient’s name or D.O.B. If the patient states that they smoke, let them know that St John are working with the local stop smoking service and ask if they would like to be referred for FREE support to quit.
You could also use a script such as:
“To give you the best chance of success I can refer you to a local team who can offer you free face to face support and products. Are you happy for me to refer you?”
Offer a brief explanation of what will happen following referral and most importantly remain non-judgemental.
It is important to remember that not everyone is ready to quit and it is up to the individual. However, by asking the patient about quitting, you are planting a seed which may lead to a successful referral in the future.
Advice for other people who smoke in the householdThe service is happy to work with whānau and friends. If there is someone else in the household who is interested in quitting as well, make sure your patient mentions that when they are contacted. The more people who are involved, the better the outcome for everyone.
For more information about becoming Smokefree call:
Te Ohu Auahi Mutunga (TOAM) – (06) 357 3426

CENTRAL SOUTH PATIENT PATHWAYS | 35Version: 3Date issued: July 2019
Safe to talk – He pai ki te kōreroSafe to talk is a 24/7 sexual harm information and support helpline that is available nationwide.
Safe to talk has been set up as part of the Government’s commitment to better support people affected by sexual harm in any way and prevent sexual harm by ensuring more people get the help they need at the right time.
The service provides free, confidential information and support to people affected by sexual harm. People who contact the helpline can remain anonymous and say as much or as little as they would like.
Sexual harm is a descriptor for a number of sexual behaviours that are engaged in without consent and involve elements of force, coercion and/or power by one person over another for the purpose of sexual gratification and control. This can include both contact and non-contact behaviour, including ‘online’ computer-assisted sexual harm.
How can patients access the helpline? > Freephone: 0800 044 334 > Text: 4334 > Website/online chat: www.safetotalk.nz > Email: [email protected]
What will Safe to talk offer? > Specialists trained in sexual harm support
> Accessible information
> Crisis counselling and support
> Advice about local service providers
Please Note:
If you have discussed this service with your patient please write “Safe to talk services offered” in the disposition section of ePRF.
Safe
to ta
lk –
He
pai k
i te
kōre
ro

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS36
Caring Caller referrals
Please note: St John Caring Caller is not suitable for patients with severe mental health issues. Caring Callers provide a friendship service only and are not trained counsellors.
Assess and treat patient as per CPGs
Is today’s problem primarily due to
loneliness or social isolation?
Seek patient’s permission to refer them to St John
Caring Caller
Note in ePRF that patient does not wish
to be contacted
> Inform patient they will be contacted by a member of the Caring Caller team to discuss arrangements
> Document referral plan in ePRF
Subject: e.g. Caring Caller referral
Member number of submission
Description: Full name, age, special
considerations for referral, e.g. loneliness,
family support etc.
Patient/ Customer call-back number
Submission type: Patient/ Customer Services Request
Job number of attending incident

CENTRAL SOUTH PATIENT PATHWAYS | 37Version: 3Date issued: July 2019
Cari
ng C
alle
r ref
erra
ls
Caring Caller referrals fact sheetSometimes living alone or being house-bound means that people miss out on daily human contact, someone to chat to, laugh with and share news with. People become lonely and isolated as friends and family move on or have passed away, or physical disabilities prevent them from getting out and about.
It is often said that loneliness is a silent and unnoticed epidemic that runs through our communities. Recognising that loneliness is a real issue in our communities, St John established the Caring Caller service. This is a free telephone friendship service that aims to reduce the loneliness experienced by some people, by providing them with contact and companionship via telephone on a regular basis.
This is not a help line; it is a free friendship service both parties enjoy. Many clients and Callers report genuine telephone friendships forming, some lasting many years.
The philosophy of the St John Caring Caller service is to: > provide high quality, client-focused, telephone friendship on a regular basis using caring volunteers who
are friendly, reliable, and good listeners
> respect and appreciate the value and worth of the volunteers who so freely give their time to assist St John and their local community through our service
> seek further support or assistance using other agencies when it is discovered that one of our clients needs help, and that these needs are beyond what our service is able to provide.
The benefits of the Caring Caller serviceBoth parties benefit from this new friendship. For the Caring Caller, it is very rewarding to be helping someone in need, even if that means just talking to them. For the client, it is a break from the social isolation, a new-found friend, regular contact, and knowledge that someone ‘out there’ cares about them.
The service plays an active role, we believe, in helping many people remain in their own homes rather than going into residential care. In times of crisis, the regular phone call can be extremely reassuring for some of the clients. They know that if they fail to answer the telephone the Caring Caller will become concerned. The Caller will then advise Caring Caller management, and a family member, a neighbour, or someone from St John will be asked check on them. In some cases an ambulance may be dispatched if necessary.
Matching clients with a Caring CallerWhen people join the Caring Caller service as clients we ask several questions to ascertain their interests and preferences. Such things as when they would like to be called, what hobbies they have and so forth. We then use this information to match the client with an appropriate Caring Caller.
Telephone conversationsCaring Callers usually call the client 2-3 times per week, for an approximate duration of 5-15 minutes (although some pairs chat a lot longer than this once they get to know each other). A range of things are discussed – anything from what they have been doing, family, TV programmes, weather, news items to what’s happening in the community. Caring Callers do not offer professional help but may suggest the client goes to their doctor, solicitor etc.

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS38
AnonymityCaring Callers are volunteers, carefully selected for their kindness and care for people. They are all ages and from all walks of life, and all enjoy the company of others. They also go through training to make sure they understand their role and know what to do if any issues arise.
There is a high level of anonymity imposed by the service. Caring Callers are only provided with the first name, age, telephone number, and a short personal profile of their client. When the Caring Caller telephones the client, it is the policy of the service that they do not disclose their surname, address, or telephone number to the client. This prevents the Caring Caller from ever being inadvertently harassed by their client, who is in most cases quite lonely throughout the day. As it is the Caring Caller who has the client’s telephone number, and not vice versa, the Caring Caller can mentally prepare him or herself before they ring the client. This allows the Caring Caller to make sure they are available for the whole of the agreed time and they are being an active listener.
Policy on meeting or visiting a clientThe Caring Caller service is a telephone friendship service only. There is a no-meeting and no-visiting policy.
Neither Caller nor client is given the personal details of each other. Their personal information is held in a secure database. When joining the service both Callers and clients are made aware of the no-meeting and no-visiting policy and that they are not to share this level of information.
There is a complaints process in place to manage any concerns raised by either clients or Callers.
How to refer someone to the St John Caring Caller serviceTo refer someone to the Caring Caller service, use the On-Scene Feedback App on the ePRF tablet. Under ‘Subject’, advise service required (Caring Caller). In ‘Description’, advise patient’s full name, age, address and any special considerations, e.g. loneliness, family support, etc. Ensure the patient’s phone number is recorded.

CENTRAL SOUTH PATIENT PATHWAYS | 39Version: 3Date issued: July 2019
St John Medical Alarm referrals
Assess and treat patient as per CPGs
Patient meets clinical indications for a St John
medical alarm?
Patient currently has a medical alarm with St John
or another provider?
Patient consents to medical alarm referral
Not eligible to be referred
> Inform patient they will be contacted by a member of the St John Medical Alarms team to discuss arrangements
> Document referral plan in ePRF
Subject: e.g. medical alarm referral
Member number of submission
Description: Full name, age, special
considerations for referral, e.g. loneliness,
family support etc.
Patient/ Customer call-back number
Submission type: Patient/ Customer Services Request
Job number of attending incident
St Jo
hn M
edic
al A
larm
refe
rral
s

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS40
St John Medical Alarm referralsIntroductionSt John Medical Alarms are designed to allow the elderly and people with disabilities to live independently for longer. In an emergency, when help is delayed, there is a higher risk of mortality, longer stays in hospital and potentially avoidable on-going medical care. A St John medical alarm allows our patients to contact emergency assistance and receive help quickly.
A St John Medical alarm can be worn when in the garden as well as in the home and there is a wide range of alarms available. Because there is a cost associated with a medical alarm, St John offers a free no obligation trial for up to one month to allow patients to see if a medical alarm is right for them. Some patients may also be eligible for medical alarm funding through the Ministry of Social Development, ACC or other agencies.
As well as increasing the client’s chances of quickly receiving emergency help at home when they need it, the cost of a medical alarm covers the ambulance call out fee.
Why a St John Medical Alarm?The St John medical alarm philosophy is “independent living – providing families with peace of mind”. Medical alarms help the elderly and people with disabilities maintain a high quality of life for longer, allowing them to feel safer in the home with more confidence to perform daily activities and reduced anxiety for the client and their family alike.
Clinical indications for a St John Medical AlarmThe St John medical alarm is ideal for anybody living at home with an increased risk of falling or requiring emergency medical assistance. Potential candidates include, but are not limited to:
> elderly patients, particularly those who are frail and/or live alone
> people with a physical disability
> people with impaired vision, balance or hearing
> people with multiple co-morbidities (medical problems)
> people who are on multiple medications
> people whose home has obstacles (e.g. stairs) that may pose a falls risk.
What is a St John Medical Alarm and how does it work?The St John Medical Alarm is a 2 piece set (base and pendant) that is continuously monitored by St John. If at any stage a medical alarm client suddenly feels unwell, falls, or otherwise requires emergency medical assistance, they push the button on the medical alarms pendant and St John will automatically call the client back through the loud-speaker on the alarms base.
From here St John will assess the client’s condition and arrange the most appropriate assistance. This could include an ambulance, a paramedic in an alternative vehicle (e.g. Sierra unit), another emergency service or expert advice. Where appropriate, a preferred carer or a family member may be notified.
Ethical practice and our medical alarm serviceIt is crucial that we maintain a professional image with our patients at all times. When discussing the option of a medical alarm with a patient, it is important we do not devalue other medical alarm providers or encourage the patient to switch providers to St John.

CENTRAL SOUTH PATIENT PATHWAYS | 41Version: 3Date issued: July 2019
St Jo
hn M
edic
al A
larm
refe
rral
s
Other key principles > Never give the patient false or misleading information about the product.
> If you don’t have the answer, be honest and refer the patient’s question to the St John Medical Alarms team.
> Do not be pushy - your patient has the right to say no to a medical alarm referral. Respect their decision and document this accordingly.
How to refer someone for a St John Medical Alarm To refer someone for a medical alarm, use the On-Scene Feedback App on the ePRF tablet. Under ‘Subject’, advise service required (medical alarm). In ‘Description’, advise patient’s full name, age, address and reason for referral e.g. falls, lives alone. Ensure the patient’s phone number is recorded.
Inform the patient that a St John medical alarms representative will contact them to organise a no obligation consultation and a free trial.
Want to know more?If you have any questions, or would like any more information, feel free to email [email protected].

Version: 3Date issued: July 2019
| CENTRAL SOUTH PATIENT PATHWAYS42
Telehealth ServicesThese services are free of charge to users and available 24/7, 365 days a year. Please consider passing the following information on to your patient if you feel they would benefit from some extra support.
Alcohol Drug HelplineIf you have a patient who is concerned about their drinking or drug taking, Alcohol Drug Helpline can help. They provide friendly, non-judgmental, professional help and advice. Family/whanau and friends can also phone if they are concerned about someone close to them. All calls are free and confidential. Call 0800 787 797 or text 8681, 24 hours a day, 7 days a week, to speak with a trained counsellor.
1737, Need To Talk?1737 is New Zealand’s national mental health & addictions helpline number. This service is completely free for patients who are:
> Feeling anxious or needing someone to talk to
> Feeling down or a bit overwhelmed
> Feeling out-of-sorts or depressed
The patient can call or text 1737 for 24/7 access to a trained counsellor who can offer behavioural support, and referrals to other services for ongoing help.
HealthlineHealthline is staffed by experienced registered nurses who provide health information and recommend appropriate care for callers with symptoms.
Call 0800 611 116
Elder Abuse Response Service (EARS)Available to patients who are worried they are victims of elder abuse and want to speak with someone confidentially. Calls are answered by registered nurses, who will help connect them with their local elder abuse specialist service provider. Family/whanau or friends who are concerned about someone can also phone for advice and support. Phone 0800 32 668 65
Gambling HelplineGambling Helpline is a 24 hour, freephone helpline for those worried about gambling or the gambling of others. Patients can call to receive immediate support, to be referred to another gambling support organisation, or for information services for problem gambling. Gambling Helpline is the helpline associated with the Government’s Choice Not Chance campaign to end harmful gambling. Phone 0800 654 655 or free text on 8006.

CENTRAL SOUTH PATIENT PATHWAYS | 43Version: 3Date issued: July 2019
Tele
heal
th S
ervi
ces
Poisons LinePlease note: For St John personnel, this line should only be used to identify a poison and what effects/signs and symptoms it might have. All clinical advice should be obtained through the Clinical Support Officer on the Clinical Desk.
The National Poisons Centre provides advice to members of the public and health care professionals about acute poisoning situations. This can involve: medicines, chemicals, hazardous creatures (e.g. spiders, snakes, jellyfish), plants and fungi.
The NPC gives advice on what to do in situations of poisoning or where poisoning might occur. This includes:
> if someone has swallowed, inhaled or injected a substance
> if someone has got a substance in their eye(s) or on their skin
> if someone has been bitten or stung by a hazardous creature
> advice on preventing poisonings in the home
> general first aid advice for poisonings.
Call 0800 POISON (0800 764 766)