Patient Centered Medical home talk at WVU
32
West Virginia wants PCMH Level Care Paul Grundy MD, MPH IBM International Director Healthcare Transformation Trip to Denmark July 10 2009 Paul Grundy, MD, MPH, FACOEM, FACPM IBM Director Healthcare Transformation President Patient Centered Primary Care Collaborative
-
Upload
paul-grundy -
Category
Health & Medicine
-
view
1.655 -
download
4
description
To employers the cost of healthcare is now a business issue and this talk is about what one large buyer IBM did to drive transformation via broad coalition with other large employers to form the Patient Centered Medical Home movement and the covenant between buyer and provider away from the garbage we now buy episodic uncoordinated disintegrated care. In the change of convenient conversation we have worked with the Primary care providers to give us coordinated, integrated, accessible and compressive care with a set of principles know as the Patient centered medical home. A Patient Centered Medical Home (PCMH) happens when primary care healers keeping that core healing relationship with their patients step up to become specialists in Family and Community Medicine. The move is to the discipline of leading a team that delivers population health management, patent centered prevention, care that is coordination, comprehensive accessible 24/7 and integrated across a deliver system. PCMH happens when the specialists in Family and Community Medicine wake up every morning and ask the question how will my team improve the health of my community today? All over the world three huge factors are in play that is driving the concept of Patient Centered Medical Home. They are: 1) Cost and demography 2) Information technology and data (information that is actionable will equal a demand for accountability by the payer or buyer of the care) 3) Consumer demand to engage healthcare differently (at least as well as they can their bank- on line) have a question about lab results why not e-mail? But at its core it is a move toward integration of a healing relationship in primary care and population management all at the point of care with the tools to do just that.
Transcript of Patient Centered Medical home talk at WVU

West Virginia wants PCMH Level Care
Paul Grundy MD, MPHIBM International Director Healthcare
Transformation
Trip to Denmark July 10 2009
Paul Grundy, MD, MPH, FACOEM, FACPM IBM Director Healthcare TransformationPresident Patient Centered Primary Care Collaborative

Who was Who was the the Shooter’s Doctor?Shooter’s Doctor?
Away from Away from Episodes of Care - Episodes of Care - FFS FFS
Population management !!
Accountability !!

If we truly want to understand costs and where they can be reduced without compromising outcomes, we need to aggregate costs around the patient. (need a place to do that – that is PCMH)
The way care is currently organized leads to redundant administrative costs, unnecessary and expensive delays in diagnosis and treatment, and unproductive time for physicians.
A system integrator a place where data is aggregated, understood and held accountable at the level of the individual patient -- THAT IS PCMH. In fact, cost reduction will often be associated with better outcomes.
The Big Idea: How to Solve the Cost Crisis in Health Careby Robert S. Kaplan and Michael E. Porter Sept 2011 Harvard review

Just Out WellPoint End Of Pilots -- Rollout time for
PCMH!!! BCBS Mi 2670 physician (BIG study) CMS CMMI CPCi APC
2010 2011
Adults (18-64)
ER visits -6.6% -9.9%Primary care sensitive ER Visits -7.0% -11.4%Ambulatory care sensitive Hospitalizations (per 1,000) -11.1% -22.0%

The Cause? Mostly due to unregulated fee-for-service payments and an over reliance on rescue/specialty care. This is stark evidence that the U.S. health care Industry has been failing us for years “Commonly cited causes for the nation's poor performance are not to blame - it is the failure of the deliver system!!”
- Unaccountable Care Organizations* Peter A. Muennig and Sherry A. Glied Health Affairs Oct. 7, 2010
Dubuque, Iowa
WV 2011

76
88 8981
8899 97
109116
10697
134
115 113
127120
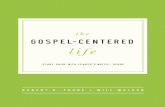
55 57 60 61 61 64 66 67 74 76 77 78 79 80 8396
0
50
100
150 1997–98 2006–07Deaths per 100,000 population*
U.S. Lags Other Countries: Mortality Amenable to Health Care
Source: Adapted from E. Nolte and M. McKee, “Variations in Amenable Mortality—Trends in 16 High-Income Nations,” Health Policy, published online Sept. 12, 2011.
The Bottom Line If the U.S. had achieved levels of amenable mortality seen in the three best-performing countries—France, Australia, and Italy—84,300 fewer people under age 75 would have died last year. Instead we focused on Rescue Care

The West Virginia Plan Strong Primary care is foundational to a high
performing healthcare system Additional resources needed to help primary care
manage populations Learned timely data is essential to success Learned must build better local healthcare systems
(public-private partnership) Physician leadership is critical Improve the quality of the care provided and cost
will come down
Sec of HHS Michael Lewis MD PhD Commissioner of Public Health, Marian Swinker, MD, MPH

WV HEALTH IMPROVEMENT INSTITUTEWV HEALTH IMPROVEMENT INSTITUTE
ADOPTION OFELECTRONIC
HEALTH RECORDS
Develop proposed mechanisms to
accelerate adoption of electronic health
records in West Virginia
MEASUREMENT
Create a forum of alignment of
measures across
stakeholders to facilitate reporting
SELF MANAGEMENT
SUPPORT
To align and improve access to resources
and best practices to improve the self-
activation capacity of all patients
EDUCATION OF THE PROVIDER
COMMUNITY
To develop a system of provider engagement to
accelerate Medicaid Transformation and
assist physician practices with migration
to AMH
PAY FORPERFORMANCE
To provide guidance on the deployment of a
P4P program as a model for the
State
QUALITYCOLLABORATIONS
To support a focused collaboration of key
stakeholders on improving quality, building on past
initiatives
Member EducationHealthy Rewards
Advanced Medical Homes
Advanced Medical HomesPay 4 Performance
Evidenced Based MedicineHealth Information Systems
Electronic Health InformationProvider Technology Incentives
OTHER RELEVANT INITIATIVESWV HIN – WVMI - OTHERS

Electronic Health RecordsElectronic Health Records
“A team approach to care…utilizing advanced information systems (including a standardized electronic health record); redesigned, more functional offices, and a whole-person orientation that focuses on quality, safety and care provided in a community context.”
129 Clinicians NCQA certified PCMH practices (ZERO Morgantown)
Advanced Medical HomeAdvanced Medical Home

Avoidable emergency room visits continue downward trend, seven percent better than market. Following evidence-based medicine continues to improve, six percentage points better than market. Medical cost trend is more than seven percentage points better than market. Diabetes is better controlled, will improve long-term health and lower medical costs.
And Today in West Virginia Medical Homes

Don’t handle your care needs in a BAD MEDICAL NEIGHBORHOOD!!
Unaccountable care, lack of organization, DO NOT GO THERE ALONE!!
Be wise when you pay for care, KNOW WHAT YOU BUY!! BEST HEART SURGERY !!!!

PopulationHealth
System Integrator
PatientExperience
The System Integrator
Creates a partnership across the medical neighborhood Drives PCMH primary care redesignOffers a utility for population health and Financial management
The Quadruple Aim = MU, PCMH & ACO Readiness, Experience of Care, Population Health, Cost
Per Capita Cost
Readiness

The Foundation for population health needs A long-term
comprehensive relationship with a Personal Physician empowered
with the right tools and linked to their care team.

The Joint Principles: Patient Centered Medical Home Personal physician - each patient has an ongoing relationship with a personal physician trained to provide first contact, and continuous and
comprehensive care Physician directed medical practice – the personal physician leads a team of
individuals at the practice level who collectively take responsibility for the ongoing care of patients
Whole person orientation – the personal physician is responsible for providing for all the patient’s health care needs or arranging care with other qualified professionals
Care is coordinated and integrated across all elements of the complex healthcare community- coordination is enabled by registries, information technology, and health information exchanges
Quality and safety are hallmarks of the medical home- Evidence-based medicine and clinical decision-support tools guide decision-making; Physicians in the practice accept accountability voluntary engagement in performance measurement and improvementEnhanced access to care is available - systems such as open scheduling, expanded hours, and new communication paths between patients, their personal physician, and practice staff are used
Payment appropriately recognizes the added value provided to patients who have a patient-centered medical home- providers and employers work together to achieve payment reform

If you scan the world for value based healthcare you will find a common element: a relationship-based team with a project manager! A comprehensivist that can command and control in an accountable system with DATA!!
So simple!So much!

Powerful Engine for transformation
Let me put this in WV
terms… Compressive vs Episodic
Integrated
Accessible
Coordinated
“Opportunities to expand access to primary care, build the health care workforce, and improve prevention and quality and attract jobs.”
Improve the care of the population while controlling costs
A “medical home” for patients, emphasizing primary care and make WV a business destination jobs .
Community networks capable of managing recipient care with local systems that improve management of chronic illness in both rural and urban settings

West Virginia Medicaid and employers –Valuebased purchasing means
holding providers accountable for both the quality and cost of care, through:
Increased transparency of cost and quality outcomes; Rewards for performance; and Payment reform. Emergency Department Collaborative Care
Management Initiative – Reduction ED Cost Accountable Communities Initiative -- align financial
incentives for those providers to work together to improve value and decrease avoidable costs.
Leveraging and/or expansion of current initiatives and federal opportunities

“Aug. 29 (Bloomberg) -- GlaxoSmithKline Plc is giving its privately insured U.S. workers PCMH level Care Via CCNC health-care network that uses primary care doctors to track patient use of specialists and hospitals.
Large Employers Partner With Medicaid CCNC
New Game Changer
Community Care North Carolina Patient-Centered Medical Home model. It provides a comprehensive, team-based model of healthcare delivery. This model drives out variability by implementing standards for all aspects of primary care services.
CCNC team ensures that care is all-inclusive and integrated with all other care provided within our system.
Each patient will be assigned to a Medical Home, led by one’s primary care physician. The patient is a part of that team as well as a nurse educator, a care coordinator, and other support staff , all linked into and supporting the patient’s health.

Reinventing Medicaid with PCMH findings are Outstanding Oklahoma's patient-centered medical home initiative has
reduced Medicaid costs $29 per patient per year from 2008 to 2010. Moreover, use of evidence-based primary care, including screening for breast and cervical cancer, increased.
The Colorado initiative expanded access to care. Before the initiative, only 20 percent of pediatricians in the state accepted Medicaid; as of 2010, 96 percent and did and at a lower cost to the state.
Vermont, inpatient care use and related per-person per-month costs decreased 21 percent and 22 percent, respectively, from July 2008 to October 2010. ER use and related per-person per-month costs decreased 31 percent and 36 percent, respectively.
Patient Centered Medical Home in Washington in State Acute care spending there was 18 percent below the national average. Inpatient stays per beneficiary were 35 percent below the national average.
Citation -- M. Takach, "Reinventing Medicaid: State Innovations to Qualify and Pay for Patient-Centered Medical Homes Show Promising Results," Health Affairs, July 2011 30(7):1325–34.
The Bottom Line in Medicaid (AS WV discovered already) PCMH starting to show an impact in access to care, quality, and cost control.

8
Source: Health2 Resources 9.30.08
Defining the Care
Publically available
information
•Patients have accurate, standardized information on physicians to help them choose a practice that will meet their needs.

21
Medical Home Model
Patientis the center
of theMedical Home
Population Health
Patient-Centered Care
Refocused Medical Training
Patient & Physician Feedback
Advanced IT Systems
Access to Care
Team-Based Healthcare
Delivery
Decision Support Tools
Model adapted from theNNMC Medical Home
Enhances beneficiary’s relationship with provider
Includes all service primary care initiatives
Guiding principles, policy Certification criteria
(AHRQ modification) Governance
(formal/informal/advisory) Metrics
(process and end-state) Permits debut of the
“comprehensivist”
Enhancing Health andthe Patient Experience

Public Health Prevention
Specialists
PCMH in Action Vermont “Blueprint” model
Community Care TeamNurse Coordinator
Social WorkersDieticians
Community Health WorkersCare Coordinators
Public Health Prevention HEALTH WELLNESS
Hospitals
PCMH
PCMH
Health IT Framework
Global Information Framework
Evaluation Framework
Operations
A Coordinated Health System
Mental health
PCMH

Vermont Financial Impact
2009 2010 2011 2012 2013Percentage of Vermont population participating 6.7% 9.8% 13.0% 20.0% 40.0%
Participating population 42,179 61,880 82,332127,04
5254,852 # Community Care Teams 2 3 4 6 13

Smarter Healthcare…36.3% drop in hospital days,32.2% drop in ER use. 9.6%, total cost 10.5%, inpatient specialty care costs are down18.9%, ancillary costs down 15.0%. outpatient specialty down
Outcomes of Implementing Patient Centered Medical Home Interventions: A Review of the Evidence from Prospective Evaluation Studies in the US, K. Grumbach & P. Grundy, November 16th 2010.



Payment reform requires more than one method, you have dials, adjust them !!! MAINE IS !!
“fee for health”“fee for outcome”“fee for process,” “fee for
belonging/membership” “fee for service” “fee for satisfaction”

OPM $39 Billion Book with Accountable CarePatient at the center
24-7 clinician phone response Provide open scheduling. Provide care management and
coordination by specially-trained team members.
Use an EHR with decision support. Use CPOE for all orders, test
tracking, and follow-up. Medication reconciliation for every
visit. Prescription drug decision support. Implement e-prescribing.
Pre-visit planning and after-visit follow-up for care management.
Offer patient self-management support.
Provide a visit summary to the patient following each visit.
Maintain a summary-of-care record for patient transitions.
Email consultations. Telephone consultations. The development of care
plans. Performance outcome measures.

CMS New Comprehensive Primary Care Initiative
Risk-stratified care management: Primary care practices will be able to proactively assess their patients to determine their needs and provide appropriate and timely preventive care.
Access and continuity: Primary care practices must be accessible to patients on a 24/7 basis
Planned care for chronic conditions and preventive care
Patient and caregiver engagement:
Coordination of care across the medical neighborhood.

Where do you train the WV Workforce? There are examples of at least a few "high performing" Health
Professional schools that support team based coordinated care delivery SELECT AND SUPPORT THESE
…Requires a Smarter Healthcare Workforce
OR ?


Recommendations WVU and WV Start the journey -- build the foundation,
the horizontal platform, a place of accountability - PCMH
WV really engage your patients find out what they need and become very patient centered
Employers in WV Stop buying from unaccountable care organizations unwilling to transform - Join us
WV - Stop sending your students to train at UCO’s. Set up WV workforce standards for education and
training based on guiding principles of PCMH Integrate Health and Sick care GIVE US LEADERSHIP ----SHOW US THE WAY