Patient blood transfusion management: discharge hemoglobin level as a surrogate marker for red blood...
7
ORIGINAL ARTICLE Patient blood transfusion management: discharge hemoglobin level as a surrogate marker for red blood cell utilization appropriatenessJason Edwards, Chris Morrison, Maleeha Mohiuddin, Vladislav Tchatalbachev, Charmi Patel, Vicki L. Schwickerath, Jay E. Menitove, and Gurmukh Singh BACKGROUND: Blood transfusion management strate- gies minimize transfusion-associated risks, enhance outcomes, and reduce costs. We explored an associa- tion of discharge hemoglobin (Hb) with pretransfusion Hb, transfusion indications, and red blood cell (RBC) transfusions. We stipulate that patients with discharge Hb concentrations greater than 10.0 g/dL, or even 9.0 g/dL, received excessive RBC transfusions. STUDY DESIGN AND METHODS: We examined aggregate data from five hospitals and for one of the hospitals, the focus hospital, we reviewed patient records for a period of 6 months. Data analyses included number of RBC units transfused and Hb values before transfusion, after transfusion, and at discharge. RESULTS: In aggregate, 27% to 47% patients had dis- charge Hb levels greater than 10.0 g/dL. At the focus hospital, 27% had a discharge Hb level greater than 10 g/dL and 50.3% had a discharge Hb level greater than 9.0 g/dL. At the focus hospital, the mean Hb trigger for transfusion was a Hb level of 7.3 g/dL; the mean posttransfusion Hb level was 9.3 g/dL and mean discharge Hb level was 9.2 g/dL. Overall, 76% of the transfusions were of an even number of RBC units. CONCLUSION: In aggregate, overutilization exceeded 20%. At the focus hospital, approximately one-quarter of patients receiving transfusions had a Hb concentra- tion greater than 10.0 g/dL at discharge. Transfused patients’ discharge Hb concentration represents an effective indicator for retrospective monitoring of trans- fusion appropriateness. In light of the large number of patients receiving even number transfusions, reviewing Hb levels after transfusion of each RBC unit could reduce unnecessary transfusions. Retrospective review of discharge Hb data focuses providers on transfusion outcomes and affords an educational opportunity for blood utilization management. P atient blood transfusion management (PBM) recognizes the complex interplay between improving patient outcomes and reducing transfusion costs that have outpaced inflation- ary factors. 1-6 PBM involves evidence-based practices for managing anemia, hemostasis, and blood loss and improving outcomes. 7 Despite advances in proper blood management, nearly a quarter of the red blood cell (RBC) transfusions, in various studies, appear to be excessive. 8-11 There is increasing recognition of adverse events associ- ated with blood transfusions. 12-19 In this regard, we sought to determine community practices in a midwestern metropolitan area and investi- gate specific transfusion practices at an inner-city, safety net teaching hospital at which many transfusion decisions are made by physicians in training. Traditionally, conservation of valuable blood and blood product resources is important to avoid or mini- mize periods of inadequate blood supply. From 1999 to 2004, blood use in the United States increased by 16%, whereas blood use in the United Kingdom declined by 8%. 10,20 Current per-capita blood use in the United States is 15% higher than in Europe and 44% higher than in Canada suggesting possible overutilization within the United States. 21 Interest in patient outcome results, current health care reforms’ attention to outcome-based medical ABBREVIATIONS: GI = gastrointestinal; PBM = patient blood transfusion management. From the Department of Pathology, Truman Medical Center, University of Missouri Kansas City School of Medicine, and the Community Blood Center of Kansas City, Kansas City, Missouri. Address reprint requests to: Gurmukh Singh, Clinical Pathology, Truman Medical Center, 2301 Holmes St, Kansas City, MO 64108; e-mail: [email protected]. Received for publication September 26, 2011; revision received January 12, 2012, and accepted January 21, 2012. doi: 10.1111/j.1537-2995.2012.03591.x TRANSFUSION **;**:**-**. Volume **, ** ** TRANSFUSION 1
-
Upload
jason-edwards -
Category
Documents
-
view
212 -
download
0
Transcript of Patient blood transfusion management: discharge hemoglobin level as a surrogate marker for red blood...

O R I G I N A L A R T I C L E
Patient blood transfusion management: dischargehemoglobin level as a surrogate marker for red blood cell
utilization appropriateness_3591 1..7
Jason Edwards, Chris Morrison, Maleeha Mohiuddin, Vladislav Tchatalbachev, Charmi Patel,
Vicki L. Schwickerath, Jay E. Menitove, and Gurmukh Singh
BACKGROUND: Blood transfusion management strate-gies minimize transfusion-associated risks, enhanceoutcomes, and reduce costs. We explored an associa-tion of discharge hemoglobin (Hb) with pretransfusionHb, transfusion indications, and red blood cell (RBC)transfusions. We stipulate that patients with dischargeHb concentrations greater than 10.0 g/dL, or even9.0 g/dL, received excessive RBC transfusions.STUDY DESIGN AND METHODS: We examinedaggregate data from five hospitals and for one of thehospitals, the focus hospital, we reviewed patientrecords for a period of 6 months. Data analysesincluded number of RBC units transfused and Hbvalues before transfusion, after transfusion, and atdischarge.RESULTS: In aggregate, 27% to 47% patients had dis-charge Hb levels greater than 10.0 g/dL. At the focushospital, 27% had a discharge Hb level greater than10 g/dL and 50.3% had a discharge Hb level greaterthan 9.0 g/dL. At the focus hospital, the mean Hbtrigger for transfusion was a Hb level of 7.3 g/dL; themean posttransfusion Hb level was 9.3 g/dL and meandischarge Hb level was 9.2 g/dL. Overall, 76% of thetransfusions were of an even number of RBC units.CONCLUSION: In aggregate, overutilization exceeded20%. At the focus hospital, approximately one-quarterof patients receiving transfusions had a Hb concentra-tion greater than 10.0 g/dL at discharge. Transfusedpatients’ discharge Hb concentration represents aneffective indicator for retrospective monitoring of trans-fusion appropriateness. In light of the large number ofpatients receiving even number transfusions, reviewingHb levels after transfusion of each RBC unit couldreduce unnecessary transfusions. Retrospective reviewof discharge Hb data focuses providers on transfusionoutcomes and affords an educational opportunity forblood utilization management.
Patient blood transfusion management (PBM)recognizes the complex interplay betweenimproving patient outcomes and reducingtransfusion costs that have outpaced inflation-
ary factors.1-6 PBM involves evidence-based practices formanaging anemia, hemostasis, and blood loss andimproving outcomes.7 Despite advances in proper bloodmanagement, nearly a quarter of the red blood cell (RBC)transfusions, in various studies, appear to be excessive.8-11
There is increasing recognition of adverse events associ-ated with blood transfusions.12-19
In this regard, we sought to determine communitypractices in a midwestern metropolitan area and investi-gate specific transfusion practices at an inner-city, safetynet teaching hospital at which many transfusion decisionsare made by physicians in training.
Traditionally, conservation of valuable blood andblood product resources is important to avoid or mini-mize periods of inadequate blood supply. From 1999 to2004, blood use in the United States increased by 16%,whereas blood use in the United Kingdom declined by8%.10,20 Current per-capita blood use in the United States is15% higher than in Europe and 44% higher than in Canadasuggesting possible overutilization within the UnitedStates.21 Interest in patient outcome results, currenthealth care reforms’ attention to outcome-based medical
ABBREVIATIONS: GI = gastrointestinal; PBM = patient blood
transfusion management.
From the Department of Pathology, Truman Medical Center,
University of Missouri Kansas City School of Medicine, and the
Community Blood Center of Kansas City, Kansas City, Missouri.
Address reprint requests to: Gurmukh Singh, Clinical
Pathology, Truman Medical Center, 2301 Holmes St, Kansas City,
MO 64108; e-mail: [email protected].
Received for publication September 26, 2011; revision
received January 12, 2012, and accepted January 21, 2012.
doi: 10.1111/j.1537-2995.2012.03591.x
TRANSFUSION **;**:**-**.
Volume **, ** ** TRANSFUSION 1

decision-making, adverse transfusion-associated events,and proper resource utilization highlight the importanceof evaluating proper transfusion practices.
Currently, the blood supply appears adequate withonly limited instances of spot shortages. In part, thisreflects the decline of elective surgical procedures duringthe Great Recession and, in part, reflects adaptation ofhospital-based blood conservation programs. However,this trend may reverse as the population ages.22
The PBM programs highlight multiple observational,cohort studies showing higher morbidity and mortalityin patients transfused at Hb levels greater than 8.0 to9.0 g/dL and two prospective, randomized controlledtrials documenting better outcomes in patients assignedto restrictive transfusion strategy groups, that is, transfu-sion threshold hemoglobin (Hb) concentrations less than7.0 to 8.0 g/dL.2,4,5,23,24
Moreover, wide variability in blood utilization forseemingly similar surgical procedures suggests a subjec-tive rather than evidence-based approach to blood trans-fusion ordering practices. For example, in a study byBennett-Guerrero and colleagues23 blood transfusionrates among hospitals ranged from 7.8% to 92.8% inpatients undergoing coronary artery bypass surgery. Casemix explained only 20.1% of the variation among hospitalsin RBC usage. Even though the investigators did notobserve differences in outcomes that could be attributedto variations in transfusion practices, it is obvious thathigher use of blood transfusions provides no additionalbenefit and contributes to higher costs and unnecessaryexposure to transfusions risks. In a randomized controlledtrial of transfusion requirements after cardiac surgery,Hajjar and colleagues4 demonstrated that transfusingeven a single RBC unit was associated with a significantlyincreased risk of serious postoperative morbidity andmortality. RBC transfusion was independently associatedwith a 1.2-fold increased risk of death at 30 days for eachunit transfused.
It is assumed that average posttransfusion Hbincrease is 1.0 g/dL per unit and that posttransfusionlevels greater than 10.0 g/dL suggests either that the pre-transfusion Hb level was above current threshold sug-gested by TRICC and FOCUS studies or that the patientwas transfused with an excessive number of RBC units.2,24
As such, a Hb level at discharge (discharge Hb) greaterthan 10.0 g/dL, or even 9.0 g/dL, in a transfused patientserves as a surrogate marker for excessive transfusion.
This study sought to determine the prevalence of dis-charge Hb of greater than 10.0 g/dL in patients receivingRBC transfusions at hospitals served by the CommunityBlood Center of Greater Kansas City (Kansas City, MO). Inaddition, a focused analysis of transfusion practices at aninner city, safety net, teaching hospital sought to investi-gate the characteristics of transfusion practices amongmedical specialty groups. Combined, we postulated that
we could predict the potential transfusion utilizationimpact of PBM programs and identify specific processimprovement opportunities.
MATERIALS AND METHODS
The community-based aspect of the study involved solici-tation to all hospitals served by the Community BloodCenter of Greater Kansas City, to provide the last Hb testresults, before discharge, for all patients receiving transfu-sion at their institution during a defined time period andfive hospitals responded, with variations in the extent ofdata provided. The transfusion services identified patientsby hospital service. Data analysis consisted of displayingRBC-transfused patients with “discharge” Hb levelsgreater than 10.0 g/dL as a percentage of RBC recipients.The patient-focused study occurred at a single tertiarycare, safety net, inner city, 283-bed teaching hospital witha Level I trauma center that uses only leukoreduced RBCs.
We evaluated patient records retrospectively and cat-egorized them into subspecialty groups based on patientdiagnoses and the specialty managing the patients’ care.Data obtained from patient records of those receiving ablood transfusion over a 6-month period included pre-transfusion Hb, number of units transfused, posttransfu-sion Hb, and discharge Hb (the last recorded Hb value).Patients were grouped by the medical specialty orderingthe RBC transfusions.
We performed statistical analyses using one-wayanalysis of variance with SNK post hoc analysis usingcomputer software (Prism, GraphPad, La Jolla, CA). Weconsidered values significant when p values were lessthan 0.05.
The suggested trigger point for RBC transfusion at thefocus hospital was a Hb level of 8.0 g/dL or lower. Exclu-sions included patients with active bleeding if the Hb wasexpected to drop below the suggested trigger point orpatients with comorbidities such as cardiovascular dis-eases, sepsis, and respiratory insufficiency. There are nocitywide guidelines for the use of RBCs although hospitalsutilize a Hb level of 8.0 g/dL as an acceptable trigger. Thepatient-focused study received approval from the TrumanMedical Center and University of Missouri–Kansas CityInstitutional Review Board.
RESULTS
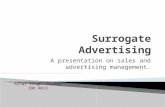
The participating hospitals ranged in bed size from 146 to504 and included records from 250 to 1881 patients perhospital. Discharge Hb levels greater than 10.0 g/dLoccurred among 27% to 47% of transfused patients(Fig. 1). This occurred in 36% to 61% of patients treated onthe family practice service, 30% to 52% on the medicalservice, 38% to 52% of those treated by nephrologists, 16%to 50% of oncology inpatients, and 13% to 52% of ortho-pedic surgery patients.
EDWARDS ET AL.
2 TRANSFUSION Volume **, ** **

For the single focus hospital subjected to detailedstudy, we obtained 475 patient records from adultpatients, 429 of which underwent analysis. We excludedrecords of 46 subjects that lacked complete information(predominately pretransfusion and/or discharge Hblevels). To determine transfusion trends throughout spe-cialties and patient groups, mean Hb value was deter-mined at several time points (Table 1). Although severalfactors influence a physician’s decision to initiate RBCtransfusion, pretransfusion Hb is the major quantifiablefactor. The mean pretransfusion Hb level was 7.3 g/dL forall groups combined. The distribution of pretransfusionHb at the focus hospital is given in Fig. 2. PretransfusionHb in trauma patients was significantly greater (p < 0.05)compared to all other specialties individually. Likewise,surgery patients had significantly (p < 0.05) greater pre-transfusion Hb levels when compared to inpatient inter-nal medicine, oncology, and obstetrics/gynecology.
A general trend between pretransfusion Hb and dis-charge Hb exists in all groups, with the exception ofsurgery and trauma (Fig. 3A). Unlike all other groups,trauma patients actually had slightly higher pretransfu-sion Hb values than discharge Hb values, presumablyreflecting the temporal relationship of injury and resusci-tation. Specifically a significant (p < 0.05) and strong cor-relation exists between pretransfusion Hb and dischargeHb (r2 = 0.72; Fig. 3B). We found no significant correlationbetween the number of units transfused and dischargeHb (data not shown). Furthermore, no significant differ-ence was observed when measuring units transfusedin patients grouped into low (<8.0 g/dL), intermediate(8.0-10.0 g/dL), or high (>10.0 g/dL) discharge Hb (datanot shown). Of note, a Hb concentration greater than
10.0 g/dL at discharge occurred in 27%of patients (Figs. 4 and 5). Discharge Hbwas greater than 9.0 g/dL in 50.3% ofpatients. The mean posttransfusion Hbwas 9.3 g/dL and the mean Hb at dis-charge was 9.2 g/dL. The distribution ofdischarge Hb is shown in Fig. 5. We didnot collect the data on time intervalbetween last transfusion and dischargebut there does not appear to be a mean-ingful change from posttransfusion todischarge Hb levels. In patients withpretransfusion Hb levels above 7.0 g/dL(within 1.0 g/dL of the trigger point) wefound that 82% were transfused with 2or more units of RBCs. In 76% of trans-fusions, the number of RBC units trans-fused comprised an even number(Fig. 6).
When comparing “elective” transfu-sions and those due to acute bleeding,the discharge Hb was above 10 g/dL in
27.8% of elective cases and in 32.7% of patients withacute bleeding. The elective cases included patients withunspecified chronic anemia, renal disease, and miscella-neous internal medicine patients. The group of patientswith acute bleeding included trauma, surgery, and gas-trointestinal (GI) bleed. It should be noted that if surgeryand trauma are examined separately, only 22.7% of thepatients had a discharge Hb level greater than 10 g/dL. Asshown in Fig. 4 nearly 50% of the GI bleed patients had adischarge Hb level of greater than 10.0 g/dL.
DISCUSSION
The notion of designating a discharge Hb level of greaterthan 10.0 g/dL, in a hospitalized patient who receivedtransfusions, as an indication of excessive transfusionseems to be a reasonable one, given that posttransfusionHb levels above 9.0 g/dL have not been shown to be asso-ciated with additional benefit. In response to a needexpressed in the literature, we are proposing that a dis-charge Hb level of greater than 10.0 g/dL should beincluded in the factors taken into account for a properPBM.8 One could propose an even more stringent targetby considering a discharge Hb level of greater than9.0 g/dL as an indication of overtransfusion.
We note that discharge Hb levels greater than10.0 g/dL ranged from 27% to 47% among transfusedpatients. This suggests at least one RBC transfusion wouldhave been avoided by following transfusion guidelinesconsistent with the TRICC and FOCUS studies.2,24
The mean pretransfusion Hb level was 7.3 g/dL forpatients receiving treatment at the focus hospital. Wefound a significant correlation between pretransfusion
Fig. 1. Percentage of transfused patients with “final” Hb level of greater than
10.0 g/dL by service. Final = latest Hb level before discharge; FP = family practice;
Med = medicine; Neph = nephrology; Onc = oncology; Ortho = orthopedic surgery.
PBM AND DISCHARGE Hb
Volume **, ** ** TRANSFUSION 3

TAB
LE
1.D
ata
fro
mfo
cus
ho
spit
alo
nly
Spe
cial
tyA
dmit
Hb
leve
l(g/
dL)
Pre
tran
sfus
ion
Hb
leve
l(g/
dL)
RB
Cun
itstr
ansf
used
Pos
ttran
sfus
ion
Hb
leve
l(g/
dL)
Dis
char
geH
ble
vel(
g/dL
)F
emal
eM
ale
Age
(yea
rs)
Ren
al8.
7�
2.8
7.0
�1.
62.
6�
2.0
9.0
�1.
09.
1�
1.5
1713
53.2
Mis
cella
neou
s9.
6�
2.4
7.4
�1.
02.
1�
0.8
9.3
�1.
49.
7�
1.7
1112
57.2
GI
8.7
�2.
57.
1�
1.4
2.9
�1.
89.
5�
1.4
9.7
�1.
432
4156
.2S
ickl
ece
ll9.
8�
3.7
6.8
�0.
72.
8�
2.1
9.6
�1.
99.
5�
2.1
53
58.4
Sur
gery
10.5
�1.
98.
1�
1.6
3.1
�2.
39.
8�
1.2
9.4
�1.
326
1753
.4In
patie
ntin
tern
alm
edic
ine
8.3
�2.
56.
7�
1.4
2.4
�1.
29.
5�
1.4
9.4
�1.
346
4751
.0Tr
aum
a11
.8�
2.3
9.7
�2.
93.
3�
2.3
10.3
�2.
09.
3�
1.8
630
33.9
Obs
tetr
ics/
gyne
colo
gy8.
2�
3.0
6.9
�2.
22.
4�
1.3
9.0
�1.
28.
8�
1.1
520
36.6
Onc
olog
y7.
9�
2.2
6.9
�1.
62.
8�
2.7
8.8
�1.
38.
8�
1.1
1818
60.9
Sep
sis
9.7
�3.
76.
8�
0.7
2.8
�2.
19.
6�
1.9
9.5
�2.
05
258
.4
Tota
l8.
9�
2.7
7.3
�1.
92.
7�
2.7
9.3
�1.
59.
2�
1.5
232
197
49.0
Fig. 2. Distribution of pretransfusion Hb at the focus hospital.
A
B
Fig. 3. (A) Data from focus hospital only. Mean pretransfusion
Hb ( ) and discharge Hb (�) levels among patient groups.
The mean pretransfusion Hb level was greater than discharge
Hb level in trauma. (B) Data from focus hospital only. When
all patient groups are combined, a strong and significant
relationship exists between pretransfusion Hb level and
discharge Hb level. IM = inpatient internal medicine;
Misc. = miscellaneous; Ob/Gyn = obstetrics/gynecology.
EDWARDS ET AL.
4 TRANSFUSION Volume **, ** **

and discharge Hb (Fig. 3B) similar to a recently reportedstudy by others, except trauma (Fig. 3A).25 The guidelineswere followed and each patient received a mean of 2 to 3RBC units (Table 1). Interestingly, 82% of patients who had
pretransfusion Hb levels above 7.0 g/dL received 2 or moreunits of RBCs. We found that an even number of RBCswas transfused in 76% of the instances. Thus, 2 or 4 unitsare being ordered and/or transfused where 1 or 3 units,respectively, may have been sufficient. It bears pointing outthat not that many years ago, single-unit RBC transfusionswere considered inappropriate and triggered a review. Therationale, then, was that if a patient needed an RBC trans-fusion, at least 2 units should be administered to provide ameaningful increase in oxygen-carrying capacity.
Although several factors, including comorbidities,length of stay, treatments given, transfusion, and underly-ing morbidities, contribute to a patient’s Hb at discharge,we attribute a discharge Hb level of greater than 10.0 g/dLas being indicative, in part, of overly aggressive transfu-sion practices. Interestingly, our finding that 27% to 47% oftransfused patients had discharge Hb levels greater than10.0 g/dL is relatively similar to the 34% reported inpatients undergoing elective orthopedic surgery.26 Amongthe group of actively bleeding patients (trauma, surgery,and GI), all had high pretransfusion Hb levels but only GIpatients had discharge Hb levels of greater than 10.0 g/dLin appreciably large numbers. It may be that in traumaand surgery patients, the treating physician could morereadily observe the extent of bleeding and blood loss,whereas in GI bleeds the blood loss being hidden fromobservation may have prompted the clinician to err on theside of “safety” by overestimating the amount of blood lossand thus “overtransfusing.” We noted that the number ofRBC units transfused did not correlate with high dischargeHb; however, the relationship between pretransfusion Hblevels and discharge Hb levels suggests that providers maybe initiating transfusions when the Hb level has not fallenbelow the optimum trigger point. Thus, “overtransfusion”may be more accurately called premature initiation oftransfusion in patients who may not have needed trans-fusion. Providers generally did not check Hb and/or Hctafter each transfusion and usually ordered RBC units ineven numbers, which probably resulted in more RBCtransfusions than may have been warranted.
The rate of overtransfusion, that is, discharge Hb levelof greater than 10 g/dL in patients with elective transfu-sions was 27.8%. This rate is not meaningfully differentfrom the overall overtransfusion rate of 27% at the focushospital. If GI bleed patients are excluded, the rate of over-transfusion in acutely bleeding patients due to traumaand surgery was appreciably lower at 22.7%. The over-transfusion in elective cases, that is, transfusion forchronic anemia, may be due to the desire to top off thepatient and prolong the interval between transfusions.
Our study was not designed to correlate Hb level toclinical outcomes; rather, it was designed to identifyopportunities for improvement and gain an understand-ing of current practices. Data addressing acute versuschronic transfusion situations were not collected.
Fig. 4. Data from focus hospital only. Group data indicating
total cases, total cases with discharge Hb levels of greater than
10.0 g/dL (�), and percent discharged with Hb levels greater
than 10.0 g/dL ( ). GI, Misc., and sepsis had the three highest
proportions of cases with discharge Hb levels above 10.0 g/dL.
IM = inpatient internal medicine; Misc. = miscellaneous;
Ob/Gyn = obstetrics/gynecology.
Fig. 5. Distribution of discharge Hb level at the focus hospital.
Fig. 6. Distribution of the number of RBC units transfused at
the focus hospital.
PBM AND DISCHARGE Hb
Volume **, ** ** TRANSFUSION 5

We infer that implementation of RBC transfusionguidelines based on a Hb “trigger” of 7.0 g/dL will result insignificant transfusion utilization declines. Current RBCutilization excess may approach 10% to 20% (midpointrange of 27% to 47%, 50% effectiveness). We suggest thatimplementing strategies correlating pretransfusion Hbdata with transfusion orders, coupled with increasing thefrequency of single-unit transfusion episodes will achievethe projected 10% to 20% RBC utilization savings.
ACKNOWLEDGMENTS
The authors are grateful to Ms Shay Weber for her kind coopera-
tion in data collection. We are also grateful for the support from
Sarah Morrison Fellowship, University of Missouri–Kansas City
School of Medicine.
REFERENCES
1. Marik PE, Corwin HL. Efficacy of red blood cell transfusion
in the critically ill: a systematic review of the literature. Crit
Care Med 2008;36:2667-74.
2. Hebert PC, Wells G, Blajchman MA, Marshall MJ, Martin C,
Pagliarello G, Tweeddale M, Schweitzer I, Yetisir E. A multi-
center, randomized, controlled clinical trial of transfusion
requirements in critical care. Transfusion Requirements in
Critical Care Investigators, Canadian Critical Care Trials
Group. N Engl J Med 1999;340:409-17.
3. Carson JL, Noveck H, Berlin JA, Gould SA. Mortality and
morbidity in patients with very low postoperative Hb levels
who decline blood transfusion. Transfusion 2002;42:812-8.
4. Hajjar LA, Vincent J, Galas FR, Nakamura RE, Silva CM,
Santos MH, Fukushima J, Kalil Filho R, Sierra DB, Lopes
NH, Mauad T, Roquim AC, Sundin MR, Leão WC, Almeida
JP, Pomerantzeff PM, Dallan LO, Jatene FB, Stolf NA, Auler
JO Jr. Transfusion requirements after cardiac surgery. The
TRACS Randomized Controlled Trial. JAMA 2010;304:1559-
67.
5. Bracey AW, Radovancevic R, Riggs SA, Houston S, Cozart
H, Vaughn WK, Radovancevic B, McAllister HA Jr, Cooley
DA. Lowering the hemoglobin threshold for transfusion in
coronary artery bypass procedures: effect on patient
outcome. Transfusion 1999;39:1070-7.
6. Walters JH, Ness PM. Patient blood management: a
growing challenge and opportunity. Transfusion 2011;51:
902-3.
7. Klein H. WHA Resolution 63.12–Overview of WHO Secre-
tariat Report and WHA Resolution. Presentation to Fortieth
Meeting Advisory Committee on Blood Safety and Avail-
ability, Department of Health and Human Services. June 7,
2011. Bethesda, Maryland.
8. Barr PJ, Donnelly M, Cardwell CR, Parker M, Morris K,
Bailie KEM. The appropriateness of red blood cell use and
the extent of overtransfusion: right decision? Right
amount? Transfusion 2011;51:1684-94.
9. O’Brien KL, Champeaux AL, Sundell ZE, Short MW, Roth
BJ. Transfusion medicine knowledge in Postgraduate Year 1
residents. Transfusion 2010;50:1649-53.
10. Wallis JP, Wells AW, Chapman CE. Changing indications
for red cell transfusion from 2000 to 2004 in the North of
England. Transfus Med 2006;16:411-7.
11. Drüeke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall
IC, Tsakiris D, Burger HU, Scherhag A; CREATE Investiga-
tors. Normalization of hemoglobin level in patients with
chronic kidney disease and anemia. N Engl J Med 2006;
355:2071-84.
12. FDA/CBER. Fatalities reported to FDA following blood
collection and transfusion. Annual summary for fiscal
year 2007. 2008. [cited 2012 Feb 29]. Available from:
URL: http://www.fda.gov/BiologicsBloodVaccines/
SafetyAvailability/ReportaProblem/TransfusionDonation
Fatalities/ucm118316.htm
13. Toy P, Popovsky MA, Abraham E, Ambruso DR, Holness
LG, Kopko PM, McFarland JG, Nathens AB, Silliman CC,
Stroncek D; National Heart, Lung and Blood Institute
Working Group on TRALI. Transfusion-related acute
lung injury: definition and review. Crit Care Med 2005;33:
721-6.
14. Silliman CC, Ambruso DR, Boshkov LK. Transfusion-
related acute lung injury. Blood 2005;105:2266-73.
15. Vamvakas EC, Blajchman MA. Transfusion-related
mortality: the ongoing risks of allogeneic blood transfusion
and the available strategies for their prevention. Blood
2009;113:3406-17.
16. Heddle NM, Klama LN, Griffith L, Roberts R, Shukla G,
Kelton JG. A prospective study to identify the risk factors
associated with acute reactions to platelet and red cell
transfusions. Transfusion 1993;33:794-7.
17. Linden JV, Pisciotto PT. Transfusion-associated graft-
versus-host disease and blood irradiation. Transfus Med
Rev 1992;6:116.
18. Hillyer CD, Blumberg N, Glynn SA, Ness PM; NHLBI
Working Group in Transfusion Recipient Epidemiology and
Outcomes Research. Transfusion recipient epidemiology
and outcomes research: possibilities for the future. Trans-
fusion 2008;48:1530-7.
19. Hendrickson JE, Hillyer CD. Noninfectious serious hazards
of transfusion. Anesth Analg 2009;108:759-69.
20. Yazer M, Triulzi D. Messages from national blood data col-
lection reports. Transfusion 2007;47:366-8.
21. MacPherson J, Mahoney CB, Katz L, Haarmann J, Bianco
C. Contribution of blood to hospital revenue in the United
States. Transfusion 2007;47:114S-6S.
22. Drackley A, Newbold KB, Paez A, Heddle N. Forecasting
Ontario’s blood supply and demand. Transfusion. 2012;52:
366-74.
23. Bennett-Guerrero E, Zhao Y, O’Brien SM, Ferguson TB Jr,
Peterson ED, Gammie JS, Song HK. Variation in use of
blood transfusion in coronary artery bypass graft surgery.
JAMA 2010;304:1568-75.
EDWARDS ET AL.
6 TRANSFUSION Volume **, ** **

24. Carson JL, Terrin ML, Magaziner J, Noveck H, Sanders DW,
Chaitman BR, Rhoads GG, Nemo G, Dragert K, Beaupre L,
Hildebrand K, Macaulay W, Lewis C, Cook DR, Dobbin G,
Zakriya KJ, Apple FS, Horney RA, Magaziner J; FOCUS
Investigators. Liberal or restrictive transfusion in high-risk
patients after hip surgery. N Engl J Med 2011;365:2453-62.
25. Boucher BA, Hannon TJ. Blood management: a primer for
clinicians. Pharmacotherapy. 2007;27:1394-411.
26. Vuille-Lessard E, Boudreault D, Girard F, Ruel M, Chagnon
M, Hardy JF. Red blood cell transfusion practice in elective
orthopedic surgery: a multicenter cohort study. Transfu-
sion 2010;50:2117-24.
PBM AND DISCHARGE Hb
Volume **, ** ** TRANSFUSION 7