Polynomial inequalities Objective –To Solve polynomial inequalities.

Pathways to Oral Health
Inequalities
Georgios TsakosDept. of Epidemiology and Public Health, UCL
Budapest
30th September 2016
Dental Public HealthW: www.ucl.ac.uk/dphT: @UCL_DentalPH
Outline
Explaining oral health inequalities: pathways
Materialist
Behaviours
Psychosocial factors
Life course approach
Do they actually explain inequalities? Evidence from
general and oral health
Implications for action
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
The shape of oral health inequalities: social gradient
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
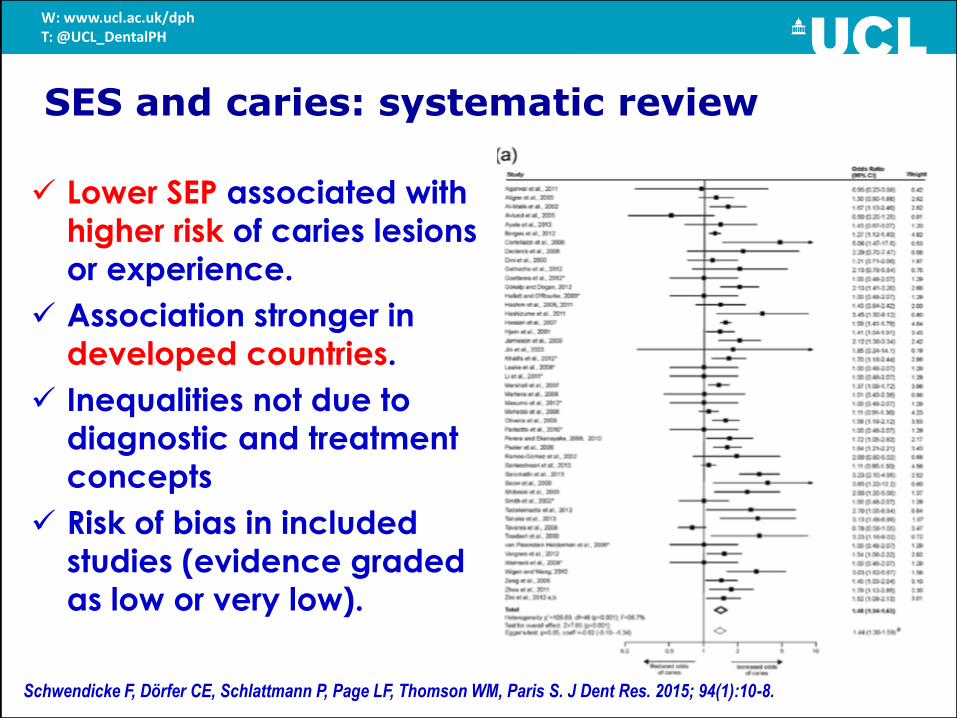
SES and caries: systematic review
Lower SEP associated with
higher risk of caries lesions
or experience.
Association stronger in
developed countries.
Inequalities not due to
diagnostic and treatment
concepts
Risk of bias in included
studies (evidence graded
as low or very low).
Schwendicke F, Dörfer CE, Schlattmann P, Page LF, Thomson WM, Paris S. J Dent Res. 2015; 94(1):10-8.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
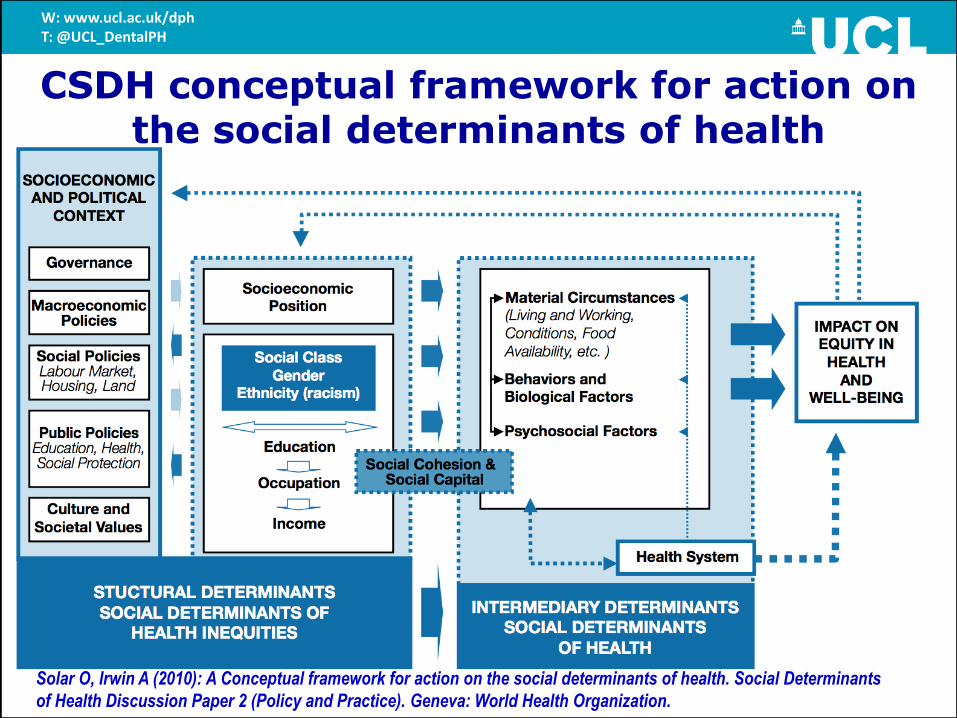
CSDH conceptual framework for action on the social determinants of health
Solar O, Irwin A (2010): A Conceptual framework for action on the social determinants of health. Social Determinants
of Health Discussion Paper 2 (Policy and Practice). Geneva: World Health Organization.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Explanations for health inequalities
Materialist
Cultural/behavioural
Psycho-social
Life course
1. Bartley M (2004): Health Inequality: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press.
2. Newton JT, Bower EJ. Community Dent Oral Epidemiol 2005; 33(1): 25-34.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Materialist pathways
Emphasizes the role of the external environment
Income / wealth and what it enables: access to goods
and services; protection from exposures to material
(physical) risk factors such as:
Poor housing;
Diet of low nutritional value;
Physical hazards at work;
Hazardous outside environments;
Pollution;
Barriers to accessing public services.
Does not sufficiently explain the social gradient in
health.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Bartley M (2004): Health Inequality: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press.

Income-related inequalities in dental service utilization, Europeans aged 50+ yrs
-20
0
20
40
60
80
Listl S. J Dent Res, 2011 * non-significant
*
*
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Cultural/behavioural pathways
• Health inequalities as a result of differences in risky
health behaviours (mainly diet, oral hygiene,
smoking, alcohol consumption, and physical
activity) between socio-economic groups
• Suggests that people from lower socioeconomic
backgrounds are more likely to engage in health
compromising behaviours than people from higher
socioeconomic backgrounds, leading to higher
levels of disease
• Due to differences in beliefs, norms and values
influenced by education and social class
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Bartley M (2004): Health Inequality: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press.

Inequalities in health behaviours
Higher socio-economic position is related to:
Lower probability of smoking.
Higher probability of healthy diet.
Higher probability of physical exercise.
Better weight control.
Lower probability of alcohol overconsumption.
Higher probability to participate in screening.
All these affect health
Lantz, House, Lepkowski, Williams, Mero, Chen (1998). JAMA; 279(21):1703-8.
Pill, Peters, Robling (1995). J Epidemiol Community Health; 49(1): 28-32.
Steptoe and Wardle (1999). Psychology and Health; 14: 391-402.
Wardle and Griffith (2001). Epidemiology and Community Health; 55(3): 185-190.
Wardle, Mccaffery, Nadel, Atkin (2004). Social Science and Medicine; 59(2): 249-261.
Wardle, Robb, Johnson, Griffith, Brunner, Power, Tovée (2004). Health Psychology; 23(3): 275-282.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Do health behaviours “explain” health inequalities?
American Changing Lives survey (n=3617): nationally
representative sample, longitudinal study.
All-cause mortality showed clear SES gradient (age –
sex – race - urbanicity adjusted).
When health risk behaviours (cigarette smoking,
alcohol drinking, sedentary lifestyle, relative body
weight) were considered, the SES gradient persisted.
“Socioeconomic differences in mortality are due to a
wider array of factors and, therefore, would persist even
with improved health behaviours among the
disadvantaged”
Lantz, House, Lepkowski, Williams, Mero, Chen (1998). JAMA; 279(21):1703-8.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Health Inequalities and Behaviours
How much of the social gradient in health can be
explained by health-related behaviours?
• “Health behaviours attenuated the association
of SES with mortality by 75%
in Whitehall II but only by
19% in GAZEL”• They are likely to be major
contributors of health
inequalities only in contexts
with a marked social
characterisation of health
behaviours
Stringhini S, Dugravot A, Shipley M, Goldberg M, Zins M, Kivimäki M, Marmot M, Sabia S, Singh-Manoux A. PLoS
Med 2011; 8(2): e1000419.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Broadbent JM, Zeng J, Foster Page LA, Baker SR, Ramrakha S, Thomson WM. J Dent Res. 2016; 95(7): 808-813.
SEP to oral health… through Behaviours
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

0
0.5
1
1.5
2
2.5
Education = 12 yrs Education < 12 yrs
Od
ds
rati
o fo
r per
ceiv
ed p
oo
r ora
l hea
lth
adjusted for confounders
adjusted also for behaviours
Do health behaviours “explain” oral health inequalities?
Sabbah, Tsakos, Sheiham, Watt (2009). Soc Sci Med; 68(2): 298-303.
US adults (NHANES III)
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Do health behaviours “explain” oral health inequalities?
Representative sample of 9th and 11th grade students
across Pennsylvania
Lower SES associated with higher prevalence of DMFT
and higher prevalence of severe caries
Lower SES associated with worse behavioural patterns
“Disparities in caries experience, however, cannot be
accounted for by SES-associated differences in
brushing, flossing, sealant use, fluoride exposure, or
recency of use of dental services”
Polk DE, Weyant RJ, Manz MC. Community Dent Oral Epidemiol 2010; 38(1):1-9.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Health Behaviours and Inequalities
Corresponding to the social gradient in health, the
social gradients for health behaviours are ubiquitous.
“Poor people behave poorly”1.
People in the lower social grades are more likely to
engage in a wide range of risk related behaviours
and less likely to practice health promoting ones.
Behavioural risk factors cluster cross-sectionally and
accumulate longitudinally.
But the health behaviours gradient is not sufficient to
fully explain the health gradient
1. Lynch J (1997). Soc Sci Med; 44 (6):809-819.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Psycho-social pathways
• Social inequality influences health through
perceptions of control and social standing, namely, a
person’s position in society relative to others.
• People of lower SEP are hypothesized to experience
higher levels of psychosocial stress
• Due to having less control over their lives, lower levels
of social support and less job security
Bartley M (2004): Health Inequality: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Does social capital explain social inequalities in inequalities?
• Systematic review:
• Social capital associated with socioeconomic
inequalities in health
• Some studies showed that “social capital has a
stronger positive effect on health for people with a
lower socioeconomic status”
• Evidence for both a buffer and a dependency effect
Uphoff E, Pickett K, Cabieses B, Small N, Wright J. Int J Equity Health 2013; 12(1):54.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
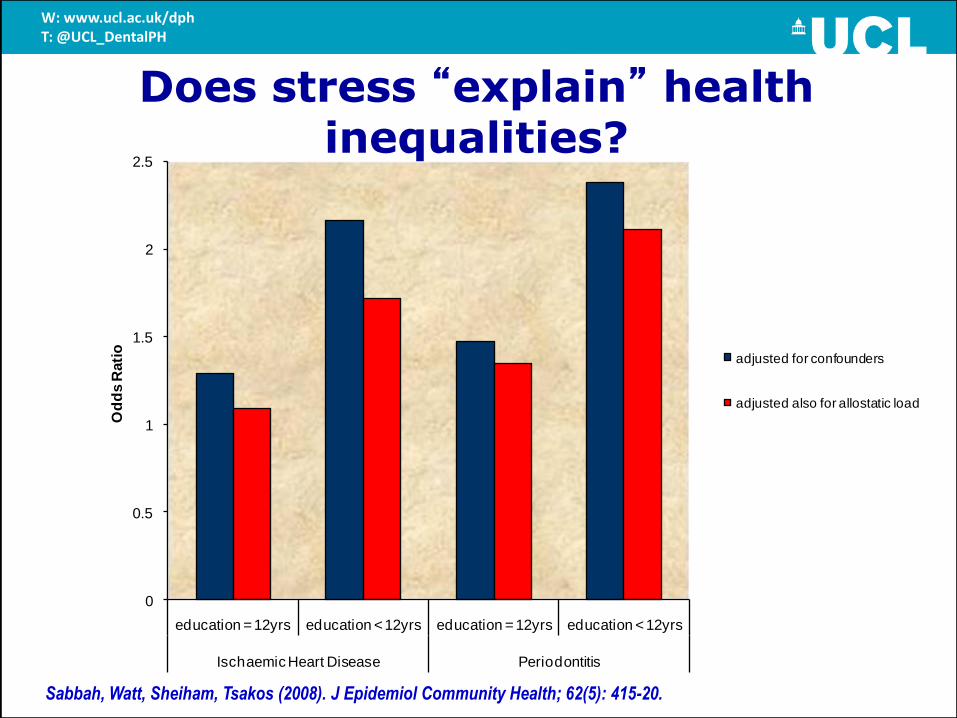
Does stress “explain” health inequalities?
0
0.5
1
1.5
2
2.5
education = 12yrs education < 12yrs education = 12yrs education < 12yrs
Ischaemic Heart Disease Periodontitis
Od
ds R
ati
o
adjusted for confounders
adjusted also for allostatic load
Sabbah, Watt, Sheiham, Tsakos (2008). J Epidemiol Community Health; 62(5): 415-20.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
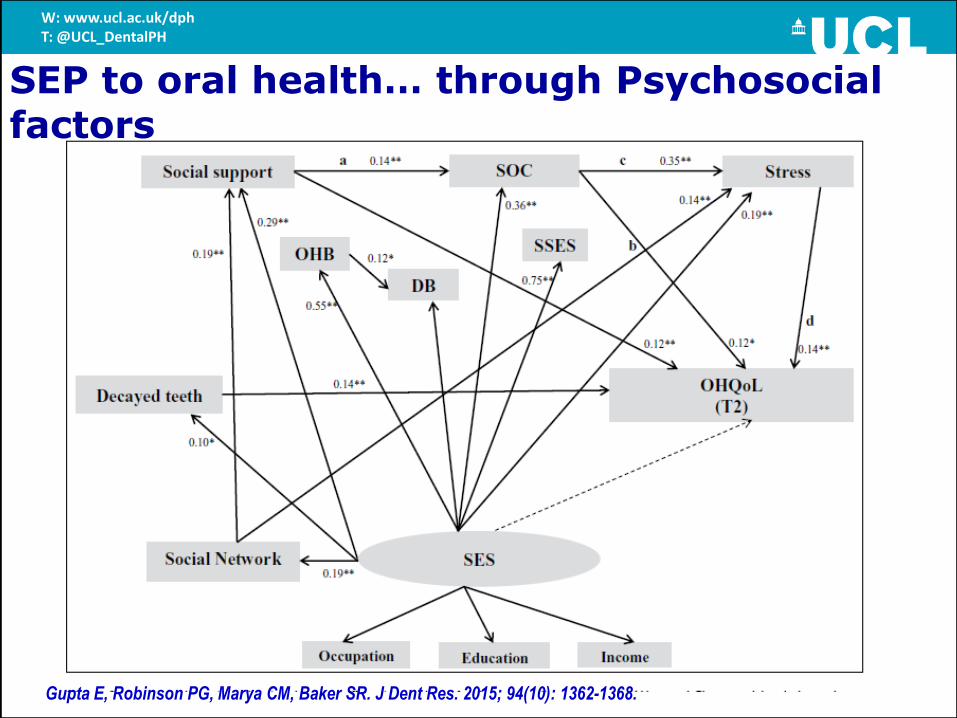
Gupta E, Robinson PG, Marya CM, Baker SR. J Dent Res. 2015; 94(10): 1362-1368.
SEP to oral health… through Psychosocial factors
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Life course model
• Health status at any given age is the result not only of
current conditions but also of prior living conditions
(starting before birth)
• Health inequality is a result of inequalities in the
accumulation of material, social, psychological, and
biological advantages and disadvantages over the
life course of individuals
• Health and social circumstances influence each
other over time.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Bartley M (2004): Health Inequality: An Introduction to Theories, Concepts and Methods. Cambridge: Polity Press.

Adler NE, Stewart J, Cohen S, Cullen M, Diez Roux A, Dow W, Evans G, Kawachi I, Marmot M (2007): Reaching for a
Healthier Life: Facts on Socioeconomic Status and Health in the U.S. The John D. and Catherine T. MacArthur Foundation
Research Network on Socioeconomic Status and Health.
http://www.macses.ucsf.edu/downloads/Reaching_for_a_Healthier_Life.pdf
The Dynamic Relationship Between Health and Socioeconomic status
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Strategic Review of Health Inequalities in England:
The Marmot Review – Fair Society Healthy Lives
Inequalities across the life course –emphasis on younger ages
W: www.ucl.ac.uk/dphT: @UCL_DentalPcH

W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Fiscal Measures
National &/or local policy initiatives
Legislation/Regulation
Healthy Settings- HPS
Community Development
Training other professional groups
Media Campaigns
School dental
health education
Chair side dental
health education
Clinical Prevention
‘Upstream’
Healthy Public Policy
‘Downstream’
Health Education &
Clinical Prevention
Upstream - downstream interventions
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Watt RG. Community Dentistry Oral Epidemiology 2007; 35: 1-11.

Oral Health Promotion - Childsmile
Childsmile: national programme designed to improve
oral health of children in Scotland and reduce
inequalities in dental health and access to services 1.
Childsmile Core: Every child provided with a Dental Pack
(toothbrush, tube of 1000ppm F-toothpaste and
information leaflet) on at least six occasions by the age of
5 yrs.
Childsmile Practice: referral by health visitor straight to a
dental practice or to a Dental Health Support Worker
Childsmile Nursery and Childsmile School: F varnish for
children aged 3+ yrs living in the most deprived areas.
Initial outcomes: reductions in dental caries of 3-year-
olds across SEP groups in Scotland2.
1. http://www.child-smile.org.uk/
2. McMahon AD, Blair Y, McCall DR, Macpherson LM. BMC Oral Health 2011; 11:29.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
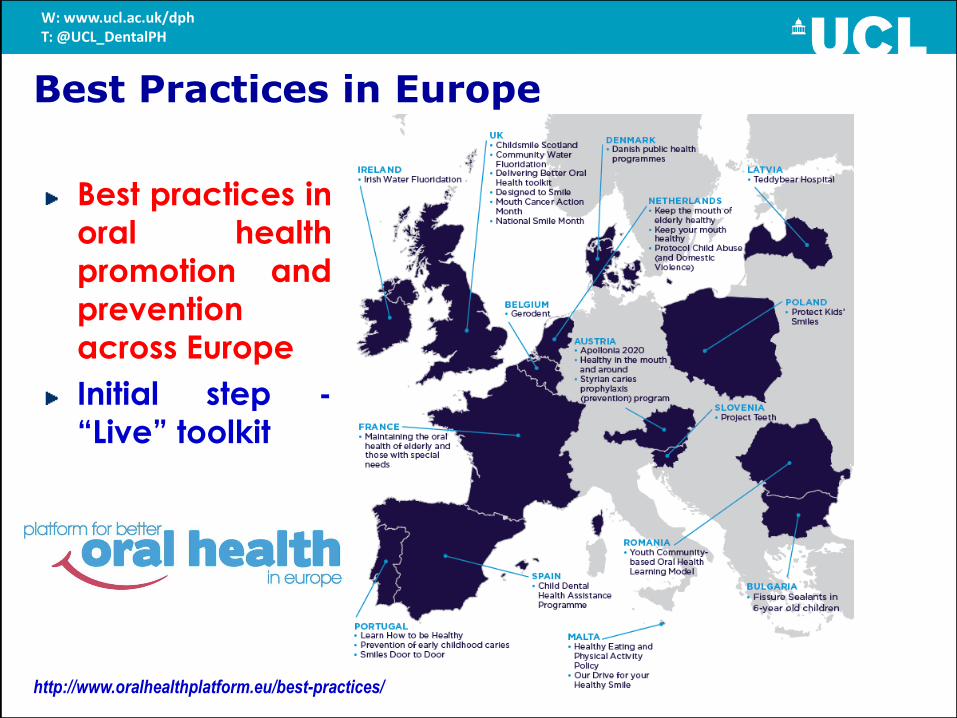
http://www.oralhealthplatform.eu/best-practices/
Best Practices in Europe
Best practices in
oral health
promotion and
prevention
across Europe
Initial step -
“Live” toolkit
W: www.ucl.ac.uk/dphT: @UCL_DentalPH
Intervention in one municipality of Japan
Creation of 'salons' (or community centers) to
boost social participation as a way of preventing long-
term disability in senior citizens
Participation in the centre associated with 2.52 times
higher odds for reporting excellent or very good self-
rated health.
“Investing in community infrastructure to boost
the social participation of communities may help
promote healthy ageing ”.
Community Psychosocial Interventions
and Oral Health Inequalities
Ichida Y, Hirai H, Kondo K, Kawachi I, Takeda T, Endo H. Soc Sci Med 2013; 94:83-90.
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

German population, aged 14-79 years
Modelling caries increments and costs over 10 years
Caries increment: 82.27 million teeth at 20% tax on SSBs;
83.02 million teeth without sugar tax.
Reduction especially in younger (rather than older)
individuals and those with low income.
Treatment costs savings: 8 billion Euros.
Additional tax revenue: 38 billion Euros.
“…a 20% sales tax on SSBs is likely to reduce caries
increment, especially in young low-income males,
thereby also reducing inequalities in caries”.
Sugar tax and Oral Health Inequalities
Schwendicke F, Thomson WM, Broadbent JM, Stolpe M. J Dent Res 2016 (in press).
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Summary
Emphasis on potential explanations (pathways) in order
to understand and address inequalities
Different pathways – not one simple or complete
explanation
Social gradient also for health behaviours – it does not
fully “explain” the social gradient (inequalities) in oral health
Interventions should focus on wider social determinants
(“causes of the causes”) – “upstream” emphasis
Common Risk Factor Approach – integration of oral
health into general health
To change behaviours, we need to change the
environment
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

What good does it do to treat people's illnesses ...
… and then send them back to the conditions
that made them sick? (Marmot)
W: www.ucl.ac.uk/dphT: @UCL_DentalPH

Thank you for your attention
www.ucl.ac.uk/dph
www.icohirp.com
MSc Dental Public Health
www.ucl.ac.uk/mscdph
Dental Public HealthW: www.ucl.ac.uk/dphT: @UCL_DentalPH
@UCL_DentalPH
UCL Department of Dental Public Health