Pathways to Collaboration: Integrating Community- … · Pathways to Collaboration: Integrating...
53
Pathways to Collaboration: Integrating Community- Based Organizations and New Health Home Programs June 20, 2013 Malinda Ellwood Center for Health Law and Policy Innovation of Harvard Law School & Liz Brosnan, Christie’s Place, San Diego CA Download the slides & materials at www.HIVHealthReform.org
Transcript of Pathways to Collaboration: Integrating Community- … · Pathways to Collaboration: Integrating...
Pathways to Collaboration: Integrating Community-Based Organizations and
New Health Home Programs
June 20, 2013
Malinda Ellwood Center for Health Law and Policy Innovation of Harvard Law School
&
Liz Brosnan, Christie’s Place, San Diego CA
Download the slides & materials at www.HIVHealthReform.org
Webinar Instructions
– All attendees are in listen-only mode
– Everyone can ask questions at any time using the chat feature
– This webinar has too many attendees for questions to be submitted over the phone.
• During Q & A segment, the moderators will read questions that have been submitted
• If you are having audio or webinar trouble, go to HIVHealthReform.org for troubleshooting help
Raise your Hand, Use the Question Feature to Ask Questions, or email questions
• You can also email questions to [email protected]
This webinar is brought to you by HIVHealthReform.org
• New hub to share information on health reform for people with HIV and health care and social service providers
• This webinar is part of a monthly series
• Features a blog, email newsletters, and resources for understanding and implementing health care reform
• Founding partners: AIDS Foundation of Chicago, The Center for Health Law and Policy Innovation of Harvard Law School, Treatment Access Expansion Project, Project Inform
• Contributors: AIDS United, HIV Medicine Association, HIV Prevention Justice Alliance, NASTAD, San Francisco AIDS Foundation
• Made possible by MAC AIDS Fund
Join us for a follow-up conference call!
Monday, July 1 at 12 p.m. ET
866-740-1260, Access Code: 3902556
You do not need to register in advance!
• Opportunity to talk with our presenters peers about ACA implementation
• Part of an informal discussion series we host after each webinar
Opportunities for Integrating CBOs into Patient Centered
Medical Homes and Medicaid Health Homes
(Overview)
June 20, 1013 Malinda Ellwood, JD
Health Law and Policy Clinical Fellow Center for Health Law and Policy Innovation (CHLPI)
of Harvard Law School Treatment Access Expansion Project (TAEP)
Download the slides & materials at www.HIVHealthReform.org
Overview: Patient Centered Medical Homes
(PCMH)
Review: What does the ACA do?
1) Insurance Reforms – Ends discriminatory insurance practices
– Making insurance more affordable/accessible
• Expands access to Medicaid and private insurance and requires core set of Essential Health Benefits (EHB)
2) Encourages new coordinated care delivery models – Our focus today: Health Homes
– Other initiatives, e.g. dual-eligible projects and others supported by the Center for Medicare & Medicaid Innovation (CMMI)

Delivery Reform: Need for Coordinated, Whole-Person Care
• Current fee-for-service system leads to fragmentation across many providers
• Tendency not to pay for care coordination and case management services
• Incentive to see many patients = not enough time with each patient individually
• Often insufficient cultural competence and health navigation
• Increasing emphasis on reduced costs (less use of ER services, etc.)
Existing system not ideal for chronic disease management
One solution- Patient-Centered Medical Home (PCMH)
Coordination and integration of whole person care • Physician arranges care with subspecialists and consultants, oversees and
coordinates the team
• Use electronic health records; patient registries; care coordinator services
• Comprehensive care including preventive and end-of-life care
Enhanced access • Flexible scheduling system; easy access to members of the team
Quality and safety
• Decision support based on updated practice guidelines
Payment • Quality-based, shared savings; reimbursement for care coordination;
account for complexity and severity of illness
Taken from “Joint Principles of Patient-Centered Medical Homes, American Academy of Family Physicians; the American
Academy of Pediatrics; the American College of Physicians; and the American Osteopathic Association.
PCMH Certification
• Standards often focus on primary care providers (medical)
• But, standards for accreditation may include services that CBOs can provide
Market CBO skills sets and services as necessary and complimentary to making PCMHs work
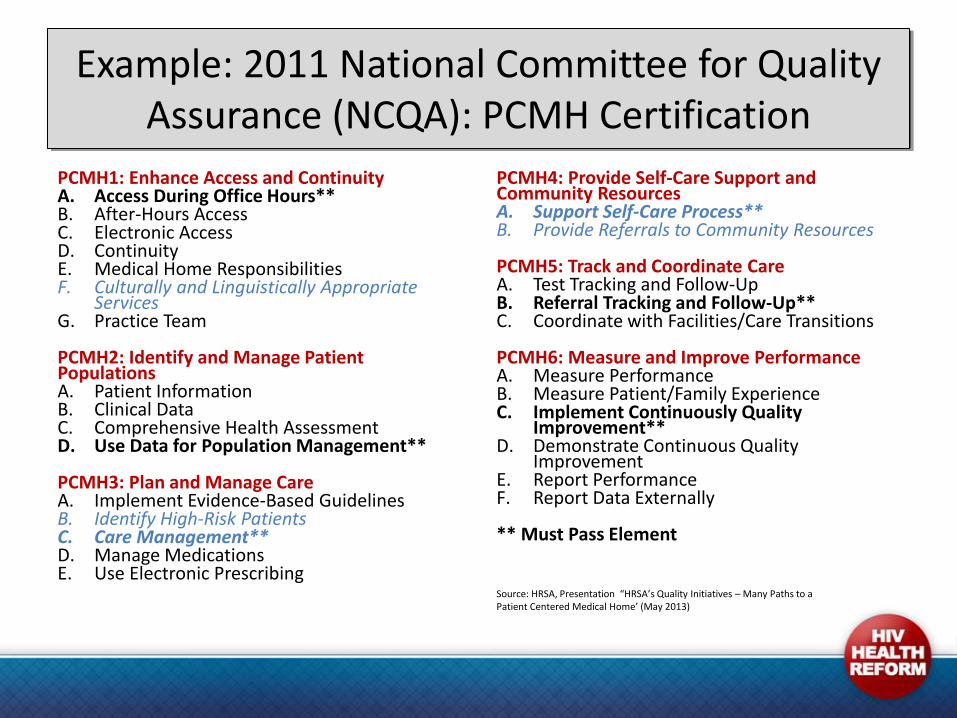
Example: 2011 National Committee for Quality Assurance (NCQA): PCMH Certification
PCMH1: Enhance Access and Continuity A. Access During Office Hours** B. After-Hours Access C. Electronic Access D. Continuity E. Medical Home Responsibilities F. Culturally and Linguistically Appropriate
Services G. Practice Team PCMH2: Identify and Manage Patient Populations A. Patient Information B. Clinical Data C. Comprehensive Health Assessment D. Use Data for Population Management**
PCMH3: Plan and Manage Care A. Implement Evidence-Based Guidelines B. Identify High-Risk Patients C. Care Management** D. Manage Medications E. Use Electronic Prescribing
PCMH4: Provide Self-Care Support and Community Resources A. Support Self-Care Process** B. Provide Referrals to Community Resources
PCMH5: Track and Coordinate Care A. Test Tracking and Follow-Up B. Referral Tracking and Follow-Up** C. Coordinate with Facilities/Care Transitions PCMH6: Measure and Improve Performance A. Measure Performance B. Measure Patient/Family Experience C. Implement Continuously Quality
Improvement** D. Demonstrate Continuous Quality
Improvement E. Report Performance F. Report Data Externally ** Must Pass Element
Source: HRSA, Presentation “HRSA’s Quality Initiatives – Many Paths to a Patient Centered Medical Home’ (May 2013)
Ongoing PCMH/Care Coordination Opportunities
• Many different health home initiatives are ongoing
– For example: HRSA initiative targets FQHCs with the goal of helping them to become certified as PCMHs, for more info, visit: http://bphc.hrsa.gov/policiesregulations/policies/pal201101.html
• Medicaid Health Homes
Medicaid Health Homes for
Chronic Disease Management
The Medicaid Health Home Option
• New state Medicaid option under the ACA: implement health homes for individuals with chronic conditions • States must file a State Plan Amendment (SPA) and must provide
public notice
• Builds on PCMH models to focus specifically on people living
with chronic conditions • Emphasis on integrating primary and behavioral health care
• Development of health homes can help states:
- Improve care for people with chronic conditions - Restrain growth in Medicaid costs
Financial Benefits to States
• 90% federal matching funding for health home services for the first two years
• States are also eligible for up to $500,000 in planning funds to explore the feasibility of creating health homes
Which Medicaid Beneficiaries Are Eligible for Medicaid Health Home Services?
Medicaid Beneficiaries who:
• Have two or more chronic conditions, or
• Have one chronic condition and are at risk for a second, or
• Have one serious and persistent mental health condition
Chronic conditions listed in the ACA:
• mental health, substance abuse, asthma, diabetes, heart disease, and being over weight
• HIV specifically designated as an eligible condition
What services are included in the Medicaid Health Home Option?
All Medicaid Health Homes must include six core services (with an emphasis on use of Health Information Technology (HIT):
• Comprehensive care management
• Care coordination
• Health promotion
• Comprehensive transitional care/follow-up
• Patient & family support
• Referral to community & social support services
But, individual states decide what each of those services actually involves.
• As with PCMH standards, many could involve skills/services that CBOs specialize in
Each state has the flexibility to decide from among these options (can choose to include all three, and/or set additional certification criteria):
A Designated provider
– May be a physician, clinical/group practice, rural health clinic, community health center, community mental health center, home health agency, pediatrician, OB/GYN, or other provider
A team of health professionals operating w/ a desig. provider
– May include physicians, nurse care coordinators, nutritionists, social workers, behavioral health professionals, or others
– Can be free-standing, virtual, hospital-based, or a community mental health center or another appropriate setting
Health team
– Must include medical specialists, nurses, pharmacists, nutritionists, dieticians, social workers, behavioral health providers, chiropractic, licensed complementary and alternative practitioners
• Any of these designations could include an opportunity for CBOs to subcontract with designated Medicaid Health Homes, even if the CBO is not the actual health home
Who can be designated as a Medicaid health home?
Design of Payment Methods
Payment methodologies:
– Monthly management care fee (most states)
• Can vary based on the severity of a person’s condition or the capabilities of health home provider
– Fee-for-service
– State may propose alternative approach
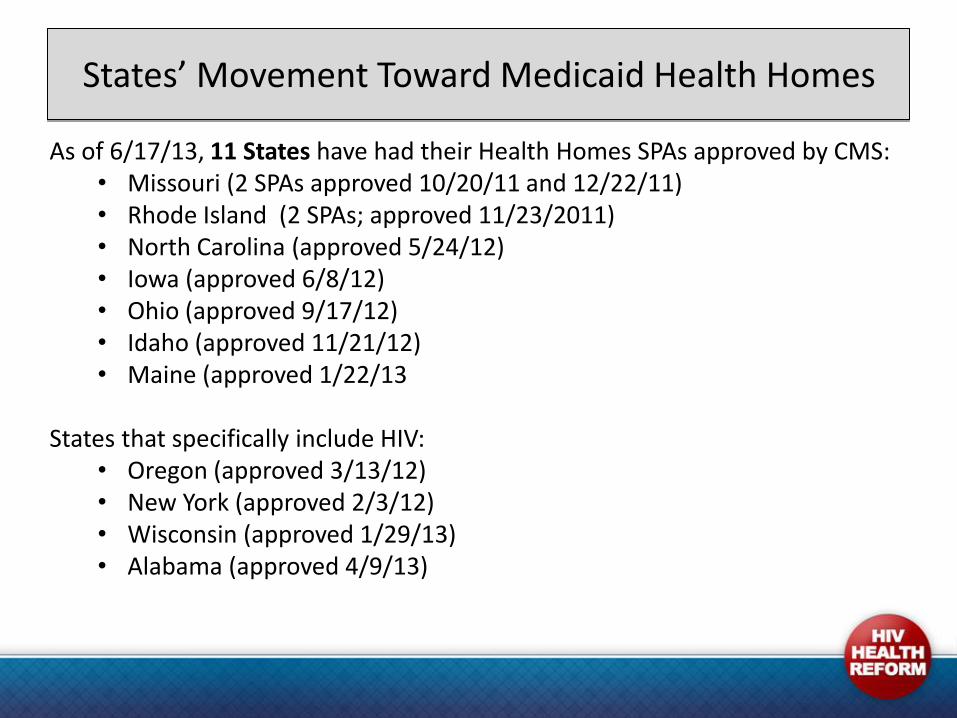
States’ Movement Toward Medicaid Health Homes
As of 6/17/13, 11 States have had their Health Homes SPAs approved by CMS: • Missouri (2 SPAs approved 10/20/11 and 12/22/11) • Rhode Island (2 SPAs; approved 11/23/2011) • North Carolina (approved 5/24/12) • Iowa (approved 6/8/12) • Ohio (approved 9/17/12) • Idaho (approved 11/21/12) • Maine (approved 1/22/13
States that specifically include HIV: • Oregon (approved 3/13/12) • New York (approved 2/3/12) • Wisconsin (approved 1/29/13) • Alabama (approved 4/9/13)
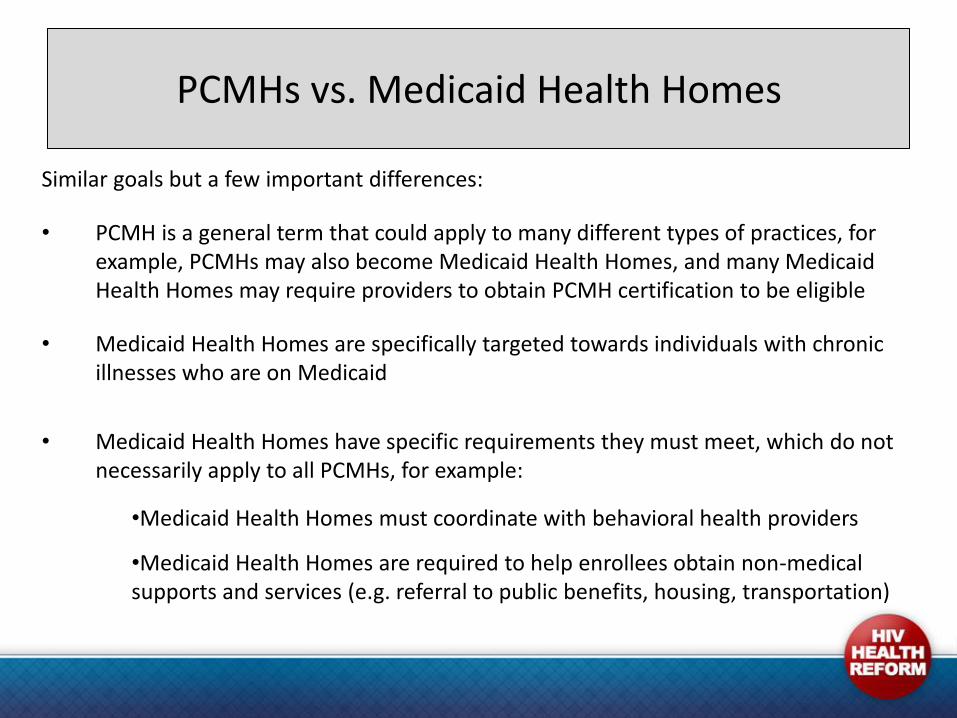
PCMHs vs. Medicaid Health Homes
Similar goals but a few important differences:
• PCMH is a general term that could apply to many different types of practices, for example, PCMHs may also become Medicaid Health Homes, and many Medicaid Health Homes may require providers to obtain PCMH certification to be eligible
• Medicaid Health Homes are specifically targeted towards individuals with chronic illnesses who are on Medicaid
• Medicaid Health Homes have specific requirements they must meet, which do not necessarily apply to all PCMHs, for example:
•Medicaid Health Homes must coordinate with behavioral health providers
•Medicaid Health Homes are required to help enrollees obtain non-medical supports and services (e.g. referral to public benefits, housing, transportation)
Opportunities for CBOs
Integrating CBOs into Medicaid Health Homes
• Medicaid Health Homes emphasize connection to community, and whole-person needs (including social supports)
– Also need to make use of existing care coordination infrastructure (e.g. Wisconsin SPA refers specifically to ASOs)
• CBOs can become an MHH, or member of provider teams
• CBOs can subcontract to provide specific core services and/or to generally make the Medicaid Health Home more successful:
– e.g., CBOs have expertise and experience in cultural competence, adherence and retention in care, care coordination, non-medical case management, obtaining community resources, connection to family members, patient trust, etc.
Ongoing Challenges
• Emphasis tends to be on clinical/primary care sites rather than CBOs. Requirement is only to refer to non-medical support services.
• No requirement that PCMHs or Medicaid Health Homes contract with CBOs (but, you can advocate that your state incorporate these)
• Reimbursement levels are not high = less motivation/ability to subcontract
• States may have Health Information Technology (HIT) requirements that can be expensive for CBOs
Next Steps for CBOs
• If not already doing so, reach out to medical clinics (FQHCs, etc.) and begin to build relationships – Demonstrate/communicate your expertise in reaching and assisting
hard to reach clients with complex care needs
– Use PCMH/MHH language to describe your services
• Quantitative + Qualitative Data Collection: identify health outcome criteria and track them – and cost reductions if possible – for all clients – Use data to argue for cost-effectiveness and inclusion in health
homes and other coordinated care opportunities
Be on the Lookout for Other Care Coordination Opportunities
• ACA coordinated care opportunities:
– E.g. dual eligibles projects through the Centers for Medicare & Medicaid Innovation (CMMI); Accountable Care Organizations (ACOs); Managed Care Organizations (MCOs)
– These could represent additional opportunities for CBOs to form partnerships
Resources on PCMHs and Medicaid Health Homes
Patient Centered Medical Homes: – NCQA PCMH certification programs: http://is.gd/YNn7XH –Agency For Healthcare Quality and Research (AHRQ), PCMH Research Center: http://is.gd/Uruphe
Medicaid Health Homes
Resources from the Centers for Medicare and Medicaid Services (CMS):
– Overview: http://is.gd/FHIUtu
– Medicaid Health Home Information Resource Center: http://is.gd/13je87
Resources on Medicaid Health Homes from Families USA:
– Medicaid Health Homes: Challenges and Opportunities for Advocates: http://is.gd/Wgangi
– Medicaid Health Homes: Designing Consumer Friendly Health Homes: http://is.gd/8fKwLn
– Medicaid Health Homes: Holding Health Homes Accountable: Quality & Payment Measures http://is.gd/y5fPGD
Health Homes/Delivery System Reform:
– Families USA, Health system reform generally: http://www.familiesusa.org/health-system-reform/
– National Academy for State Health Policy (NASHP), Medical Home Resource Center: http://is.gd/E7WHrR
– Center for Medicare and Medicaid Innovation (CMMI): http://innovation.cms.gov/
– CARE Act Target Center – medical home resource center https://careacttarget.org/mhrc
Health Reform and HIV: HIVHealthReform.org: http://www.hivhealthreform.org/
Treatment Access Expansion Project (TAEP): www.taepusa.org
Be on the Look-Out for Other Care Coordination Opportunities
Malinda Ellwood, JD
Health Law and Policy Clinical Fellow
Remaining Relevant in the New Reality
A Case Example of CBOs Pioneering Partnerships With
Patient-Centered Medical Homes
June 20, 2013
Download the slides & materials at www.HIVHealthReform.org
Who We Are
Christie’s Place is a leading nonprofit community
based organization in San Diego County
that provides culturally competent and
comprehensive HIV/AIDS education, support,
and advocacy.
Our mission is to empower women, children,
and families whose lives have been impacted
by HIV/AIDS to take charge of their health and
wellness.
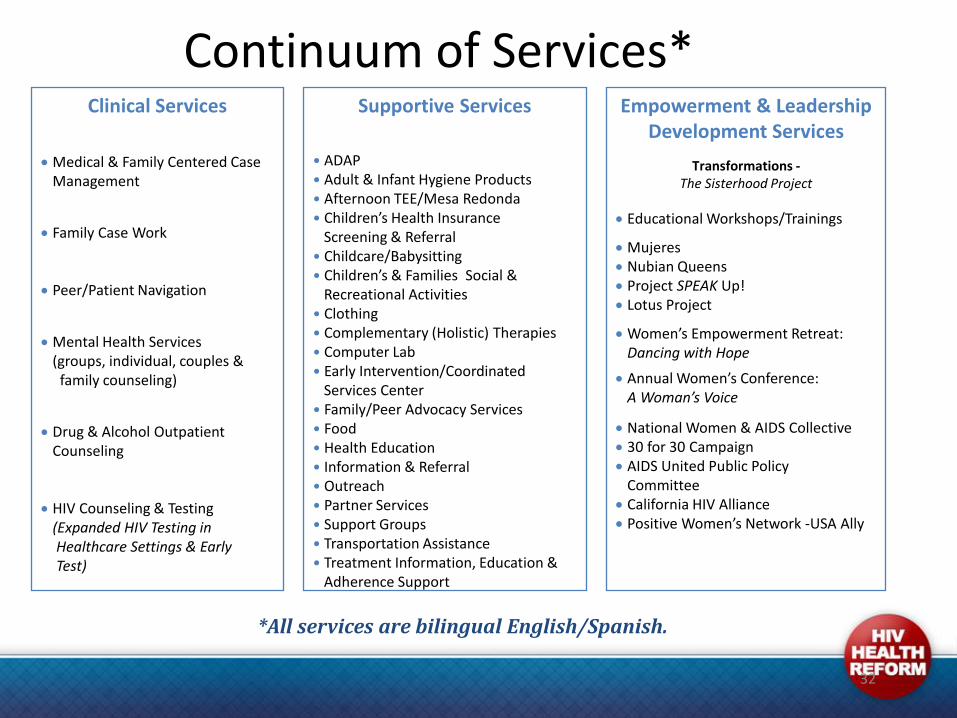
Continuum of Services* Clinical Services
Medical & Family Centered Case Management
Family Case Work Peer/Patient Navigation
Mental Health Services (groups, individual, couples & family counseling)
Drug & Alcohol Outpatient Counseling HIV Counseling & Testing (Expanded HIV Testing in Healthcare Settings & Early Test)
Supportive Services
• ADAP • Adult & Infant Hygiene Products • Afternoon TEE/Mesa Redonda • Children’s Health Insurance Screening & Referral • Childcare/Babysitting • Children’s & Families Social & Recreational Activities • Clothing • Complementary (Holistic) Therapies • Computer Lab • Early Intervention/Coordinated Services Center • Family/Peer Advocacy Services • Food • Health Education • Information & Referral • Outreach • Partner Services • Support Groups • Transportation Assistance • Treatment Information, Education & Adherence Support
*All services are bilingual English/Spanish.
Empowerment & Leadership Development Services
Transformations - The Sisterhood Project
Educational Workshops/Trainings
Mujeres Nubian Queens Project SPEAK Up! Lotus Project
Women’s Empowerment Retreat: Dancing with Hope
Annual Women’s Conference: A Woman’s Voice
National Women & AIDS Collective 30 for 30 Campaign AIDS United Public Policy Committee California HIV Alliance Positive Women’s Network -USA Ally
32
Darwinism
If you don’t evolve, you become extinct.
A Matter of Relevance & Sustainability
• Strategic positioning (and repositioning) has always been a constant
• Not only does the landscape change, community & client needs change
– Need for greater cultural (& gender) responsiveness
– Need for for health systems navigation
– Need to integrate whole person care
– Need for better care coordination
• Reform = Opportunities
CBOs & the Affordable Care Act
Navigating the New Reality
• National HIV/AIDS Strategy (NHAS) • Goals:
• Reduce HIV incidence
• Increase access to care for people living with HIV and optimize health outcomes
• Reduce HIV-related disparities
• Affordable Care Act • Investments in community health centers
• Insurance reforms
• Medicaid expansion
• Medical homes (NCQA 2011 PCMH Standards)
• Patient navigation & care coordination
• Future of Ryan White
Understanding the Landscape
• Must know the “speak” – learn the language • Coordinated Care methodology
• Medical homes
• NCQA Standards and Guidelines for Patient-Centered Medical Homes (PCMH 2011)
• accreditation includes services CBOs provide, we help to make this work
• Organizational readiness • Assess – what services are (or could be)
reimbursable?
• Relationships with medical clinics?
• Develop plan with tactics to position your
organization
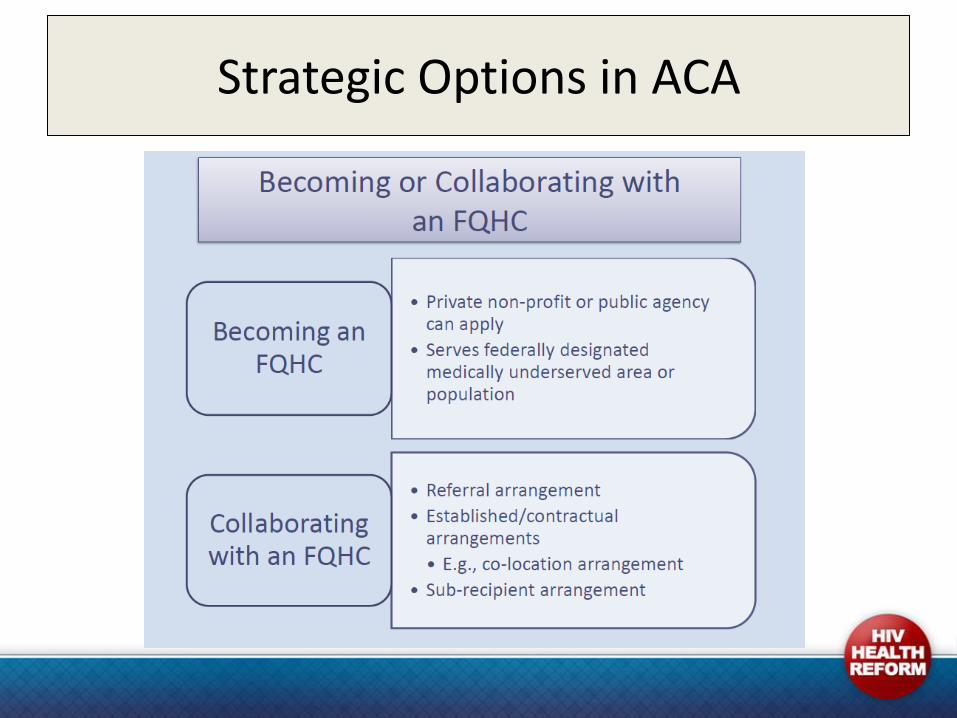
Strategic Options in ACA
Our Response: Strategic Alliances
• Why choose this option? ACA, funding, positioning in community, diversification of services
• Staying true to our mission and expertise – Understanding and articulating what we bring to the table – the “value
added”/ROI for clinical partners
• Developed/developing strategic alliances with clinical partners – Co-location with primary care
• Peer navigation • Behavioral health • Medical case management
– Part of clinic health teams – Whole person care
• Patient and family support • Social support services
• Strengthening medical home models
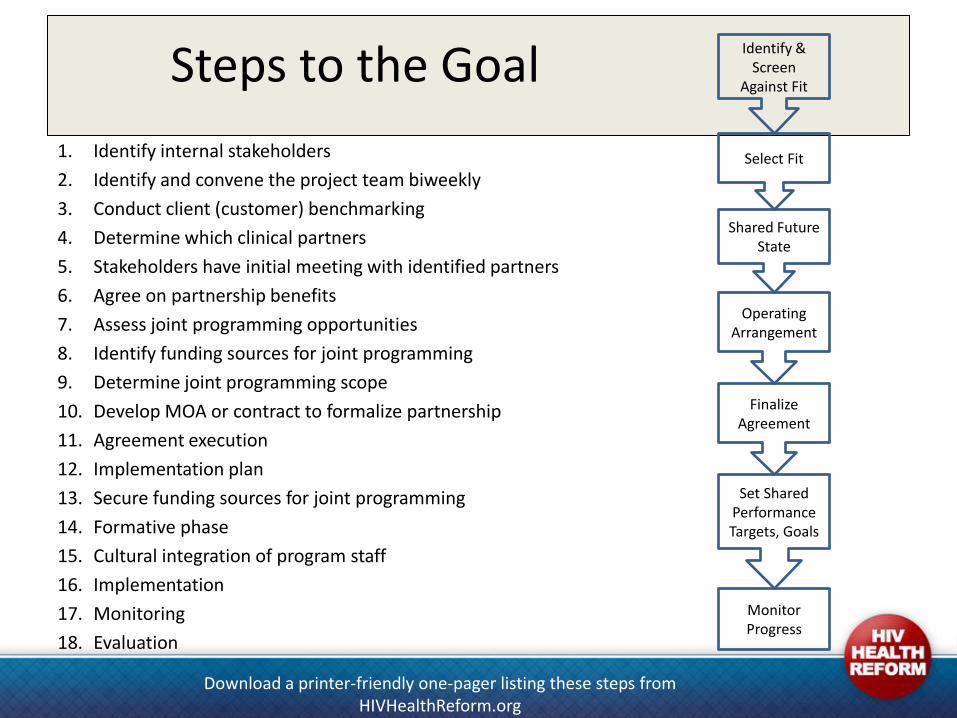
Steps to the Goal
1. Identify internal stakeholders
2. Identify and convene the project team biweekly
3. Conduct client (customer) benchmarking
4. Determine which clinical partners
5. Stakeholders have initial meeting with identified partners
6. Agree on partnership benefits
7. Assess joint programming opportunities
8. Identify funding sources for joint programming
9. Determine joint programming scope
10. Develop MOA or contract to formalize partnership
11. Agreement execution
12. Implementation plan
13. Secure funding sources for joint programming
14. Formative phase
15. Cultural integration of program staff
16. Implementation
17. Monitoring
18. Evaluation
Identify & Screen
Against Fit
Select Fit
Shared Future State
Operating Arrangement
Finalize Agreement
Set Shared Performance Targets, Goals
Monitor Progress
Download a printer-friendly one-pager listing these steps from HIVHealthReform.org
Outcome
Access to Care & Retention in Care Initiatives
Case Example: CHANGE for Women
• Innovative, responsive & relevant approach
• Addresses 2nd & 3rd goals of NHAS & positions for ACA
• Network of Care Model: a system-wide care coordination approach – Involves multiple collaborating organizations
– Pursue balanced and coordinated array of strategies to address access to care
• Partners include: – University of California, San Diego (UCSD) Antiviral Research Center
– UCSD Mother, Child, and Adolescent Program
– UCSD Owen Clinic
– North County Health Services
– County of San Diego HIV, STD & Hepatitis Branch
– The San Diego LGBT Community Center
– Vista Community Clinic
– Casa Cornelia Law Center
– American Friends Services Committee: US Mexico Border Project
– Cardea Services (evaluation)
Strengthening Medical Homes
• Patient/consumer education - 4 E’s: education, eligibility, enrollment, engagement – Navigation and support around understanding and enrolling in
Medicaid expansion and marketplace insurance opportunities
• Expanded linkages to community/social supports
• Co-location of services and integration with provider teams = enhanced culturally appropriate & person-centered care; comprehensive care management; care coordination
• Patient & family support; provision of social service support (i.e. transportation, food , childcare)
• Created and expanded Peer Navigator model at clinical partner sites and through a mobile, home-based approach
• Medical Home via My Chart – Increase self-efficacy by training HIV+ women to access and utilize their
electronic medical records
– Increase communication with healthcare providers
• Center of Excellence in Women’s HIV Care & Research – UCSD Owen/Fem-Owen Clinic Medical Home
– Enhanced coordination of medical and behavioral healthcare (integrated model)
• “I Am More Than My Status” social marketing campaign
Strengthening Medical Homes (continued)
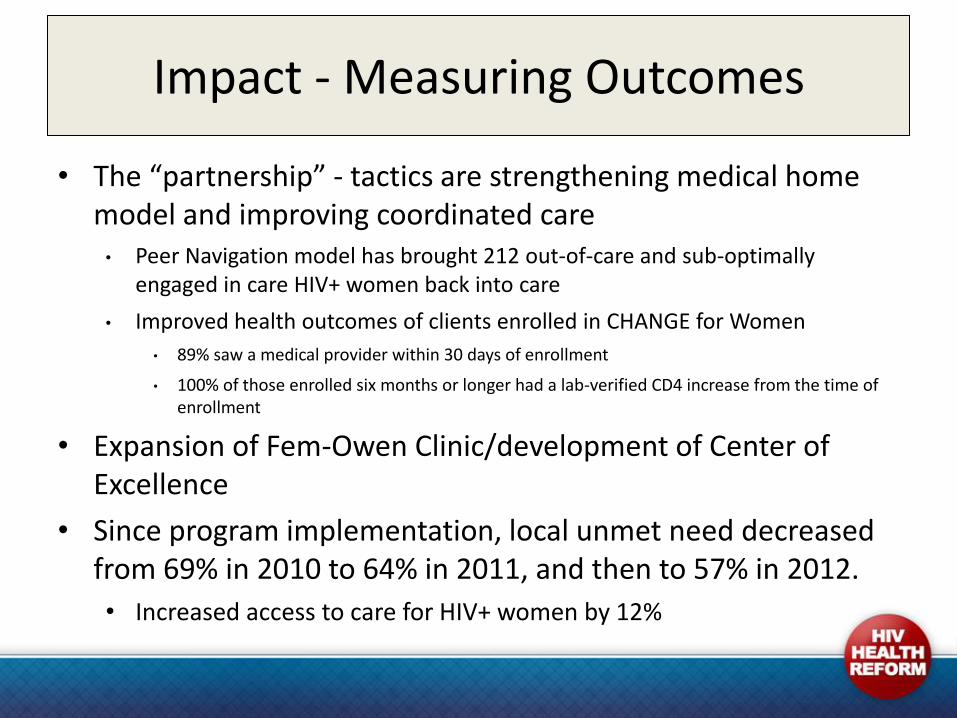
Impact - Measuring Outcomes
• The “partnership” - tactics are strengthening medical home model and improving coordinated care • Peer Navigation model has brought 212 out-of-care and sub-optimally
engaged in care HIV+ women back into care
• Improved health outcomes of clients enrolled in CHANGE for Women
• 89% saw a medical provider within 30 days of enrollment
• 100% of those enrolled six months or longer had a lab-verified CD4 increase from the time of enrollment
• Expansion of Fem-Owen Clinic/development of Center of Excellence
• Since program implementation, local unmet need decreased from 69% in 2010 to 64% in 2011, and then to 57% in 2012.
• Increased access to care for HIV+ women by 12%
Next Steps
• Working with State partners on how to certify/credential Peer Navigation
—can this become a reimbursed service?
• Electronic Health Record technology
• Public and commercial third party insurance reimbursement for behavioral health services
• Becoming providers on the Health Exchange/Marketplace plans
• Reimbursement through sub-recipient agreements
Lessons Learned
• Relevance, positioning, sustainability
• Never underestimate the value of relationship capital
• Readiness planning is a must – Take time for strategic thinking . . . be proactive, forecast and don’t do it in
a bubble
• Know the data, the drivers and the deliverables required
• Be willing to take smart, calculated risks
• Must constantly evolve the way you do business – “evolve or become extinct”
• Power of advocacy and policy
Acknowledgements
• AIDS United
• MAC AIDS Fund
• Johnson & Johnson
• Alliance Healthcare Foundation
• Macy’s Foundation & Passport Fund
• Janssen Therapeutics LINCC Initiative
• Kaiser Permanente Foundation Hospitals, Southern CA Region
• Qualcomm Foundation
• San Diego HIV Funding Collaborative
• The California Wellness Foundation
• UCLA/Johnson & Johnson Health Care Executive Program
Strengthening the Health and Resilience of Women and Families Impacted by HIV/AIDS
49
For More Information
Elizabeth (Liz) Brosnan Executive Director, Christie’s Place
[email protected] (619) 702-4186 x210 www.christiesplace.org
Chair, National Women & AIDS Collective www.nwac-us.org - Upcoming TA Webinars!!
“The vast majority of local organizations are pure service providers. It has
become clear that if all organizations on the local and state level do not reserve a portion of their agenda for advocacy, coalition building, and public policy, they are no longer doing right by their constituents.”
-Pablo Eisenberg, National Center for Responsive Philanthropy
Join us for a follow-up conference call!
Thursday, May 23 at 3 p.m. ET
(866) 206-0240 passcode 437543#
You do not need to register in advance!
• Opportunity to talk with Julia and your peers about ACA implementation
• Part of an informal discussion series we have hosted after webinar
What’s next?
• Download & share the presentation and webinar recording (available in a few days)
• We need your feedback! When you sign off, take the quick, five-question survey about the webinar
• Watch for the announcement on the next webinar
Questions?
• Ask your questions using the webinar chat feature.
• Or email them to [email protected]
• If we don’t get to your question it will be logged and we’ll do our best to follow up!