Can a management pathway for chronic cough in children improve ...

Pathway for dispensingto children
A reference guide for ABDO members
Association of British Dispensing Opticians
Pathway for dispensing to children
Without reservation the importance andsignificance of dispensing accuratelyfitting spectacles to children is widelyrecognised as a key function in thedevelopment of eyesight and visualcapability. The intention of this guide is tooffer a more comprehensive pathway toensure the highest standards of dispensingare achieved on every occasion.
The key elements required to achieve thisobjective, when dispensing an opticalappliance, are prescription interpretation,spectacle frames, spectacle lenses, facialmeasurements, verification and the fittingof the appliance. When referring to a‘dispense’ for a patient, these keyelements cannot be considered inisolation.
A registered dispensing optician’s oroptometrist’s responsibilities whendispensing a pair of spectacles can besummarised as follows:
• Receiving a prescription from aprescriber or from the patient
• Analysing the prescription, ensuringthat the prescription is unambiguous,interpreting its contents anddiscussing the prescription with thepatient/parent
• Providing advice on the suitability ofspectacle lenses that would fulfill therequirements of the prescription
• Providing advice on the suitability ofspectacle frames that would beappropriate for both the requiredlenses and the patient’s needs
• The optician should always remain thedominant force regarding the frameand lens selection, rather than theparent(s) or the child, to ensure theresultant spectacles meet the requiredstandard - in some instances the wishesof the parent(s) or the child may needto be skilfully moderated by theoptician to reach an acceptablecompromise
• Taking facial, frame and other opticalmeasurements as appropriate
• Processing an order for new spectaclesand/or other optical appliances
• Being responsible for the accuracy (torelevant standards) of the completedspectacles and/or appliance
• Fitting and adjusting the spectaclesand/or appliance
• Providing advice on the use of thespectacles and/or appliance
• Providing an ongoing aftercare servicefor the spectacles and/or appliance
GOC registrants have a duty of care toensure that dispensing to children iscarried out in person, or if the function isto be conducted by an individual who isa non-registrant, the optometrist ordispensing optician should ensure thatthe said individual has appropriateknowledge to undertake this task undersupervision. Should the latter beapplicable, the professional shouldmaintain a level of vigilance and havemeans to intervene at any point duringthe dispensing process.
In addition to the outlined definition,ABDO is of the strong opinion that manyof the caveats listed should be expandedupon to ensure higher levels of individualcare for patients are carried out.
For example, compromise on frameselection is potentially ambiguous as thenecessity for perfection of frame fit is ofparamount importance. Whilst colourpreference is acceptable, compromiseon the fitting is not.
Eye HealthFor the purposes ofthis document,effort has beenmade toconcentratefully on thehighlyimportantaspect ofspectacledispensing. It isessential however thatthe dispensing optician recognises theneed to be fully knowledgeable andunderstand comprehensively eye healthconditions and disorders that lead to theneed for spectacle provision.
In order to place high importance on thedispensing process, it is essential the child(where of the age) and a parentunderstand the need to wear spectacles.
Therefore it is very important that prior tothe commencement of dispensing,discussion of experience to date andunderstanding of the importance ofspectacle wear takes place to avoiduncertainty for those concerned.
Page 2

Support mechanism The biggest fear for many parents is theprospect of potential harm, pain, injury orother disabling situations to their child. Sowhen there is a realisation that there is adeviation from perfection, the feelingsexhibited can be both troubling anddeeply worrying. For the parents there is awhole host of negative and positivefeelings, arguably more negative.
From the perspective of the practisingdispensing optician, experience and skillin communicating bad news with patientsis part of their competency requirements.Often this can occur when a parentattends for the first time and is informedthat their child requires spectaclecorrection
It is vitally important that the practitioner isconscious of the psychological impactthat this may cause. In situations like thisthere must be a great deal ofcompassion and understandingdemonstrated. Providing acomprehensive explanation of what isinvolved during the provision ofspectacles, as well as outlining ongoingcare elements, will ensure that a degreeof trust is established by both the childand parent towards the practitioner.
The difficulties lie with the parents:how they can cope and what theycan do to help?
Some of the negative thoughts exhibited byparents might include:
• Will they be different? Historically stigmas attached to spectaclewear by parents when they were youngcan be considered a negative - nowadaysthe frames and appeal to spectacle wearis very different
• Surely it’s not forever?
• How long will they need to wear them?
• Whose fault is this, mine, my partners?
• Why my child?
• What is wrong with their eyes?
and in some very extreme cases:
• Will they go blind?
On the basis that many fail to compute andretain disturbing news, none of the questionslisted should be deemed as a difficult or sillyquestion by any practitioner. The practitionermust become the counsellor, the shoulder tolean on and the person parents intrust tomake the problem manageable for their child.
Conveying bad news to anyone isundoubtedly an unenvious task for anyonebut it needs to be done in a professionalmanner with the utmost sensitivity. Throughoutthe discussion, the balance between avoidingpessimism, providing hope, and being realisticneeds to be maintained.

Page 4
Dispensing to a child is a highly skilled andcomplex competency that requires asignificant degree of patience on thepractitioner’s part to achieve the desiredresults. Unlike dispensing to an adult, it islikely that the child will visit the practicemore frequently between eyeexaminations for various spectacle repairs.Again by outlining the professional servicesprovided during initial and ongoingdiscussions, many unfortunate situationswhere the spectacle performance andeye development is hindered due toill-fitting spectacles will almost certainly beavoided. Care must be taken to educatethe child and parent as to what is correctin terms of fitting and comfort. Should therebe a deviation from what is deemedcorrect, there should be immediateprovision made by the parent to have analteration carried out.
Process The following information proposesa framework or approach that maybe adopted to ensure thatchildren are fitted with the bestspectacles at an acceptablecost to their parents. Thisprocess is intended to beapplicable andpragmatic inpractice.
The intention is to suggest a process whichensures the parent is informed about:
• The best eyewear solution for their child
• Their NHS entitlement
• Other relevant alternatives
Sometimes a dispensing optician oroptometrist can forget that they aredealing with people, it’s not just about theeyewear; hence it should always beremembered that a person has to wearthe results of the dispensing beingundertaken. Put simply it’s worth askingevery time, “Would I wear thosespectacles?” or, “Would I let myson/daughter wear those?” or even,“Am I proud of that job?”
Lens selection
The choice of lenses involves considerationof several factors including but not limited tothe following:
Price The NHS will make a contribution via thevoucher scheme towards the costs ofchildren’s eyewear. While the currentvoucher values are set at a level of aroundhalf the normal retail prices for basic hardresin (CR39) lenses, most practitionersaccept the voucher as a means ofpayment for the spectacles. It isconceivable that the perception held by somany that spectacles for children are ‘free’is often a barrier to successful spectaclefitting. Additionally the voucher can beused as part payment towards frames andlenses of superior quality that may offerfurther benefits after taking into accountindividual needs and requirements.
Lens material The best lens option for a high myopicpatient is entirely different to the best lensesfor a hypermetropic patient, yet manychildren, regardless of prescription, arewearing conventional CR39 lenses whetherit’s stock or surfaced. Furthermore, we haveto consider that these lenses are being wornby children who can at times be careless,enjoy some rough and tumble and less likelyto clean and care for their spectacles thanadults, therefore additional lens surfacetreatments can be highly desirable.
It is conceivable that children are highly
likely to spend time on smart phones, handheld devices, computers etc and as a resultconsideration should be given to the use ofMAR coatings to improve clarity, reduceglare and enhance visual performance.
CR39 hard resin is the standard ophthalmiclens material in the UK today. This is becauseit offers a good balance of clarity, durability,lightness of weight, scratch-resistance andlow price.
Trivex (PNX, Trilogy) is thinner, lighter andsubstantially more impact resistant than CR39with equally good optical properties, UVabsorption and chemical stability. IdeallyTrivex should be considered as the first choicetougher option for most children with low tomedium prescriptions and for sports eyewear.
Polycarbonate is an extremely high impactmaterial often used for children’s spectacles.Together with Trivex it should be consideredat the very least for dispensing to children,but in particular for sports eyewear and forthose with a history of spectacle breakages.
Glass lenses should never be dispensed tochildren.
Increasing the index Children with higher powered prescriptionsmay appreciate thinner, lighter lenses just asadults do. It is the responsibility of thedispensing optician to ensure that a lens witha higher refractive index will in fact be thinnerand/or lighter than a lower index material ona case by case basis.

Page 6
In general, it could be assumed that a lensmaterial of refractive index 1.74 is the highestindex available hence it will be the thinnestoption. However, experience tells us that on asmall diameter, due to 1.74 requiring a thickercentre substance, it could be that 1.6 Index isas thin or thinner and offers more durabilitywith better optics.
Additionally pending circumstances,surfaced CR39 might be an acceptablealternative. Whilst there are no specificguidelines on when to opt for stock orsurfaced, the practioner through experiencegained will make clinical judgements basedon previous experience and understandingof additional parameters includingprescription, pupillary distance and framemeasurements.
Single vision fitting position The vertical optical centres for children havebeen typically placed on the horizontalcentre line (HCL), with the horizontal opticalcentres measured with a rule. To achieve themaximum potential of any optical correction,the eyecare professional will measure thepupil position in both meridians beforeordering the appropriate spectacles andcompensate the vertical optical centre forpantoscopic tilt.
In the case of an anisometropic child this isextremely important to reduce unintentionalprismatic effects in primary gaze position. Ifwe are trying to correct an anisometropicamblyopia then we need to eliminate these
effects to give the child maximumopportunity to adjust to, cope with andultimately show an improvement in vision.
In the absence of vertical centrationspecifications the prescription laboratorywill put the centres on HCL. There has beendebate that raising the optical centreabove HCL in hypermetropic cases willgreatly increase lens thickness, when in factthe difference is usually very small.
As an example take the case of anaverage anisometrope aged five:
• Right eye +3.00DS, Left eye +8.00DS • Metal frame eyesize 44mm,
bridge size 19mm • Monocular PDs Right eye 26.5mm,
Left eye 26.5mm
Placing the optical centres on HCL andusing an automated system we can showthe calculated surfaced right lens thicknesson HCL would be 5.5mm:

With the optical centre placed 2.5mmabove HCL the calculated surfaced rightlens thickness on HCL would be 6.2mm, just0.7mm difference:
For this child the unintentional prismaticeffect in primary gaze has been reducedby 1.25 prism dioptres. This will help thistypical child adjust to the spectacles morequickly and increases the chances ofovercoming amblyopia.
How to measure children accurately canbe difficult as they tend to move about.This can be carried out efficiently by theeye care professional using conventionalmethods or a modern digital centrationterminal.
Clearly determining the correct process tofollow will be down to the practitioner toassess but decisions will be dependent onseveral factors including engagement,capacity and interest. Using a transparent
ruler is not admitting defeat but acting inthe best interests of the child to achievethe desired results.
Bifocal fitting position In some paediatric cases a bifocal isrequired and how this is set is quiteimportant considering the use factors.Generally the bifocal will be set higher thannormal, often in line or slightly below pupilcentre to encourage use. Quite often thebifocal can be introduced at a very earlyage where the vertical depth of the framemay be 20mm-25mm. It is accepted thatleaving about 10mm of vertical distance asa minimum from bifocal top edge to toprim would be sufficient.
Very rarely nowadays E-line bifocals aredispensed to children. It is more likely to bea large D segment or occasionally Rsegments. Both have a much bettercosmetic appearance, are less thick andcertainly reduce weight.
Progressive Power Lenses (PPLs) Children who require a reading additioncould potentially benefit from progressivepower lenses. If a child has had congenitalcataracts removed then it may beappropriate to fit PPLs as they mature andwill give them more scope for studies.Again you should consider a frame withsufficient depth as they may need fullreading addition of potentially +3.00dioptres and compact designs may limit

their needs for an intermediate zonedmodern active lifestyle.
Coatings, tints and surface treatments Scratch resistant coatings are obviously ofbenefit to most children. Anti-reflectioncoatings offer similar advantages tochildren as they do for adults and could beincreasingly advantageous for youngpeople who play videogames, spend theirvirtual lives online and watch many hours ofTV. In terms of durability AR coated lensesare more scratch resistant than uncoatedlenses, but softer than a hard coat only.
Tinting for clinical purposes has to be dealtwith on a case by case basis. Tinting fortherapeutic purposes (dyslexia, etc.) arebeyond the scope of this guide thereforefurther specialised advice should besought. Fixed-tint sunglasses, with UV block,should be encouraged but as separateeyewear.
UV The cumulative damaging effects of UVexposure is well documented and nowreadily accepted as part of outdoorlifestyles and skin care. However, UVprotection for our eyes is mostly limited tosunglasses where we are required by EUregulations to ensure complete protection.The UV absorption of clear lenses hasreceived less attention. It is said that morethan half of our total lifetime UV exposureoccurs before we are 18 years old so
children are more in need of UV protectionthan adults. Most optical plastics are eithernaturally UV absorbing or have UV inhibitorsadded (to reduce yellowing), even basicCR39 offers 50 per cent UV absorption up to380nm. It follows, therefore, that a spectaclewearing child’s eyes are better, if notcompletely, protected from UV whencompared to their emmetropic friends.
Plastic photochromic lenses provide 100 percent UV protection all of the time, evenwhen un-activated. They are almost clearindoors and at night, effective sunglasses inbright daylight and good value for moneycompared to buying a separate pair ofsunglasses. Material options and coatingsare as extensive as for clear lenses. So inpurely practical terms, photochromics haveseveral good points but they are stillassociated with older spectacle wearersand some say they look undesirable whenpartially activated.
Page 8
There has been a trend in recent times fora skull fitting style. In specific circumstancesthis can be practically successful andconsideration should be given particularlyin cases when accommodating hearingaids or trochlear implants.
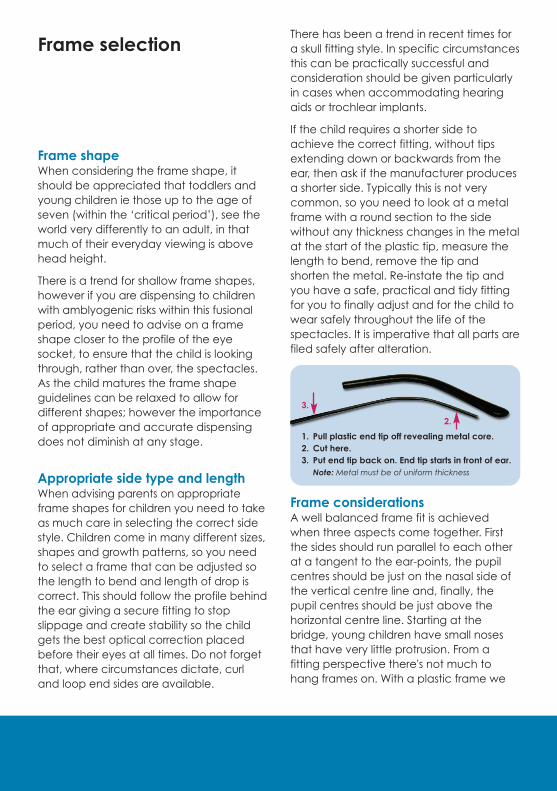
If the child requires a shorter side toachieve the correct fitting, without tipsextending down or backwards from theear, then ask if the manufacturer producesa shorter side. Typically this is not verycommon, so you need to look at a metalframe with a round section to the sidewithout any thickness changes in the metalat the start of the plastic tip, measure thelength to bend, remove the tip andshorten the metal. Re-instate the tip andyou have a safe, practical and tidy fittingfor you to finally adjust and for the child towear safely throughout the life of thespectacles. It is imperative that all parts arefiled safely after alteration.
Frame considerations A well balanced frame fit is achievedwhen three aspects come together. Firstthe sides should run parallel to each otherat a tangent to the ear-points, the pupilcentres should be just on the nasal side ofthe vertical centre line and, finally, thepupil centres should be just above thehorizontal centre line. Starting at thebridge, young children have small nosesthat have very little protrusion. From afitting perspective there's not much tohang frames on. With a plastic frame we
Frame selection
Frame shape When considering the frame shape, itshould be appreciated that toddlers andyoung children ie those up to the age ofseven (within the ‘critical period’), see theworld very differently to an adult, in thatmuch of their everyday viewing is abovehead height.
There is a trend for shallow frame shapes,however if you are dispensing to childrenwith amblyogenic risks within this fusionalperiod, you need to advise on a frameshape closer to the profile of the eyesocket, to ensure that the child is lookingthrough, rather than over, the spectacles.As the child matures the frame shapeguidelines can be relaxed to allow fordifferent shapes; however the importanceof appropriate and accurate dispensingdoes not diminish at any stage.
Appropriate side type and length When advising parents on appropriateframe shapes for children you need to takeas much care in selecting the correct sidestyle. Children come in many different sizes,shapes and growth patterns, so you needto select a frame that can be adjusted sothe length to bend and length of drop iscorrect. This should follow the profile behindthe ear giving a secure fitting to stopslippage and create stability so the childgets the best optical correction placedbefore their eyes at all times. Do not forgetthat, where circumstances dictate, curland loop end sides are available.
1. Pull plastic end tip off revealing metal core.2. Cut here.3. Put end tip back on. End tip starts in front of ear.Note: Metal must be of uniform thickness
2.
3.

need to pay attention to the bridge forthere is little that can be done to rectify apoor fit. With metal frames and adjustabletoggle pads we have much more scopefirstly to adjust the supplied pads andsecondly to replace with alternative padsof different sizes and materials.
The single biggest issue here is thatspectacles tend to slide down little noses,so we need to ensure that the frame willstay put, securely and comfortably. Alsoworth considering at this point is to makesure the eyelashes will be clear of the backsurface of the lenses. Working out from thebridge we now examine where the eyes sitwithin the eye rims ensuring that they lookbalanced and level. On occasion childrenwill have asymmetrical facialcharacteristics and level won't be possible,if necessary allow for this asymmetry in thefit. In most cases small amounts ofasymmetry can be corrected byadjustment at the temples/front joints butsome fashion frames have very thick andpractically un-adjustable temples.
Be aware of this before it becomes aproblem considering both splay angle andpantoscopic angle.
With no regard for the dictates of fashionhere are some observations on frames:
Plastic: Frames offer more substance tohide thicker lenses. In many cases pads onarms are being fitted as standard whichoffers further appeal.
Metal: Metal frames with toggle pads areeasier to adjust. A ‘twinned pad’ bridge (iea strap bridge) will spread impact if theframe is crushed against the child’s face inthe case of a fall.
Supras: Often suitable for stock minuslenses, surfaced plus lenses to ensurelongevity and appropriate edge thickness.
Rimless: Opportunity to specify parametersof lens shape; with an appropriate frameand lens material can lead to successfuloutcomes.
Special Facial Characteristics SFCFinally, should there be a situationwhere stock frames are proving less thansatisfactory in terms of fitting due to facialcharacteristics, there should always beconsideration given to supplying acustom-made frame or modifying/adaptinga stock frame.
By doing so there will be no doubt that theintroduction of individualisation will ensurethat the child will be wearing properly fittedspectacles specific to their needs.Nowadays this function is very rarely carriedout; however it is essential that thepaediatrics practitioner retains the necessaryskills should this be a suitable and practical.
Knowledge of specialist labs wheremodification/adapting frames is commonpractice or frame suppliers who offeralternatives styles to cater for deviations fromperceived normal would be highly desirable.
In cases such as dispensing Down’ssyndrome children, it is anticipated thatmany stock frames will be inappropriate dueto incorrect elements of design, particularlyaround the bridge of the nose. Clearlyordering in specific frames or modifying stockframes to take into account individualitywould result in a more appropriate wellfitted pair of spectacles.
On such occasion, the practitioner may bein a position to claim further NHS funding onthe basis that they can justify why a stockframe was inappropriate, explain whymodifications were necessary and whatmodifications were carried out. Recordkeeping in such circumstances is imperativefor auditing purposes.
Page 10

Final deliberations by the practitioner
Once the finalalterations have beenmade to the spectacleson the child’s face, thereshould be a final checkby the practitioner toensure they are satisfiedtheir work is fit andproper and as a resultthey are more thanhappy for the child toleave the practicewearing the spectacles.It is imperative that thechild is present and thespectacles are not givenout to a parent at thispoint, it would beunprofessional in everysense to allow spectaclesto be released without afinal fitting.
The following list covers points that should always bechecked before any child leaves the practice:
1. Are the spectacles fitting appropriately taking intoaccount the ‘fitting triangle’ ie length to bend, length ofdrop, inward angle of drop?
2. Are the lenses in line with expectation regardingthickness, powers, centration (vertically and horizontally)and material? - conduct an overall quality check andwhere appropriate a visual check to ensure visualexperience meets visual expectations
3. Have you highlighted the fitting process and results tothe parents to avoid any doubt as to what is anacceptable wearing position?
4. Have you made clear the provision for repairs andcleaning process?
5. Would you be happy to wear the spectacles and finallybut almost certainly the most important factor... is thechild happy?
Whilst many will have their own views and thoughts on howdispensing to children should be carried out, there will beunanimous agreement that not a single pair of spectaclescan leave a practice without the above checklist beingadhered to. The regulatory body, profession andprofessionals in the UK have a duty to eliminate the poorand often shambolic levels of care and eyewear given tochildren. Working to and applying specific elements withinthis guide into an operational routine will go some way toraising standards of care and fulfilling a commitment toprovide best possible eye care solutions to children.

Page 12

Top ten tips
Be enthusiastic, become engaged and demonstrate a genuineinterest in the child’s development through spectacle wear.
Develop a relationship built on trust, professionalism and desireto do the best you can for the child.
Educate the child and parents on spectacle wear - putting on,taking off, cleaning process and wearing schedules ie all thetime, concentrated work, classroom etc, use language thechild can understand and consider having little props at handto make them feel more comfortable eg teddies withspectacles.
Offer insight into appropriate lens choice explainingadvantages and benefits - build realistic expectation of finishedproduct (particularly hypermetropic patients) to avoiddisappointment on collection.
Guide on frame selection based on the fitting triangle ie lengthof drop, length to bend and inward angle of drop, as well aspantoscopic tilt and frame size - never sacrifice visualperformance and comfort in preference of cosmetic appeal.Let the child see how good they look and be sure to tell them.
12
3
4
5

Page 14
Be sensitive to emotions, particularly for those wearingspectacles for the first time - the child needs time to feelpositive about the imminent changes in their life andunderstand why they need to wear spectacles.
Ensure that all elements of the dispensing process are carriedout in person or are supervised accordingly - be mindful thatall of the following points are necessary to complete adispense and cannot be considered in isolation: prescriptioninterpretation, spectacle frames, spectacle lenses, facialmeasurements, verification and the fitting of the appliance.
Ensure the fitting of spectacles is done in such a way thatyou are proud and satisfied that no further amendments arenecessary unless an accident occurs where further attentionis required.
Always consider the importance and inclusion of verticalcentration measurements in addition to horizontal centration.
Most importantly... ensure the child is happy to wear their spectacles and youare happy to let them leave your practice.
6
7
8
910
Association of British Dispensing Opticians199 Gloucester Terrace, London W2 6LDTelephone 020 7298 5100 Email [email protected] www.abdo.org.uk
www.twitter.com/MembershipAbdo Jun
e 2
017