
PATHOPHYSIOLOGY OF HEART FAILURE - …c.ymcdn.com/sites/ OF HEART FAILURE Sara ... due to decreased...
22
7/20/2016 1 PATHOPHYSIOLOGY OF HEART FAILURE Sara Paul DNP, FNP, FAHA, CHFN, FHFSA HF Pathophysiology 1. Initiating Cause/Event 2. Neurohormonal Activation 3. Immune Activation 4. Physiologic Alterations (remodeling) • Systolic vs. diastolic dysfunction 5. Hemodynamic Changes • Right vs. left-sided HF 6. Symptom Development Initiating Causes/Events • Ischemic heart disease/CAD • Hypertension • Valvular disease • Genetic abnormalities, hypertrophic cardiomyopathies • Congenital heart abnormalities/defects • Peripartum cardiomyoathy • Amyloidosis/sarcoidosis • Infections (e.g., viral myocarditis, Chagas’ disease) • Metabolic disorders (hyperthyroidism, diabetes) • Toxins (e.g., alcohol or cytotoxic drugs) • Prolonged arrhythmias • Idiopathic cardiomyopathy
Transcript of PATHOPHYSIOLOGY OF HEART FAILURE - …c.ymcdn.com/sites/ OF HEART FAILURE Sara ... due to decreased...

7/20/2016
1
PATHOPHYSIOLOGY OF
HEART FAILURE
Sara Paul DNP, FNP, FAHA, CHFN, FHFSA
HF Pathophysiology
1. Initiating Cause/Event
2. Neurohormonal Activation
3. Immune Activation
4. Physiologic Alterations (remodeling)
• Systolic vs. diastolic dysfunction
5. Hemodynamic Changes
• Right vs. left-sided HF
6. Symptom Development
Initiating Causes/Events
• Ischemic heart disease/CAD
• Hypertension
• Valvular disease
• Genetic abnormalities, hypertrophic cardiomyopathies
• Congenital heart abnormalities/defects
• Peripartum cardiomyoathy
• Amyloidosis/sarcoidosis
• Infections (e.g., viral myocarditis, Chagas’ disease)
• Metabolic disorders (hyperthyroidism, diabetes)
• Toxins (e.g., alcohol or cytotoxic drugs)
• Prolonged arrhythmias
• Idiopathic cardiomyopathy

7/20/2016
2
Neurohormones in Heart Failure
• Norepinephrine
• Renin
• Angiotensin II
• Aldosterone
• Vasopressin
• Endothelin
• ANP, BNP
• Cytokines
• Nitric oxide
CNS sympathetic outflow
Disease progression
Cardiac sympathetic
activity
1-receptors
2-receptors
1-receptors
Vasoconstriction
Sodium retention
Myocardial toxicity
Increased arrhythmias
Sympathetic
activity to kidneys
+ peripheral vasculature
Activation
of RAS1- 1-
Compensatory Mechanisms:
Sympathetic Activation in Heart Failure
RAAS Activation

7/20/2016
3
NE
UR
OH
OR
MO
NE
S
Natriuretic Neurohormones
• Natriuretic Peptides: Three known types
• Atrial Natriuretic Peptide (ANP)
• Predominantly found in the atria
• Diuretic and vasodilatory properties
• Brain Natriuretic Peptide (hBNP)
• Predominantly found in the cardiac ventricles
• Diuretic and vasodilatory properties
• C-type Natriuretic Peptide (CNP)
• Predominantly found in the central nervous system
• Limited natriuretic and vasodilatory properties

7/20/2016
4
Hemodynamic
(balanced vasodilation)
• veins
• arteries
• coronary arteries
Neurohormonal
aldosterone
norepinephrine
Renal
diuresis & natriuresis
Pharmacological Actions of hBNP
Abraham WT and Schrier RW, 1994 INHIBITED BY NEPRILYSN
BN
P C
on
cen
trat
ion
(pg
/mL
)
186 ± 22
791 ± 165
2013 ± 266
HF Severity
Mild
n = 27
Moderate
n = 34
Severe
n = 36
0
500
1000
1500
2000
2500
BNP Concentration
and Degree of HF Severity
Dao Q et al. J Am Coll Cardiol. 2001;37:379.
Antidiuretic Hormone (ADH) –
Vasopressin
• Activation of carotid sinus & aortic arch
baroreceptors due to low C.O. leads to ADH
release &
• stimulation of thirst
• promotes water retention
• leads to decreased plasma sodium concentration
(hyponatremia)
• increases SVR (hence, BP & afterload)

7/20/2016
5
Decreased systemic blood pressure
Central baroreceptors
Stimulation of hypothalamus, which produces
vasopressin for release by pituitary gland
Release of vasopressin by pituitary glandVasoconstriction
Increased systemic blood pressure
Vasopressin
*Note: water retention with extreme activation of this system
Endothelium-Derived
Vasoactive Substances
- Produced by a thin lining of cells within the arteries and veins called the endothelium
Endothelium-derived relaxing factors (EDRF) –Vasodilators:
• Nitric Oxide (NO) – diminished in African Americans
• Bradykinin (increased with ACE inhibitors)
• Prostacyclin – increases renal perfusion; blocked by NSAIDs
Endothelium-derived constricting factors (EDCF) – Vasoconstrictors:
• Endothelin I
Alterations in endothelium-dependent vasodilation --
Role of nitric oxideArtery Vein
Endothelial
Cells
Smooth muscle
Cells
Connective
tissue
Epithelial
Cells
Valve

7/20/2016
6
The story of nitric oxide and endothelin . . . .
• Increased endothelin OR decreased nitric oxide OR both
contribute to poor exercise tolerance in HF patients by
diminishing pulmonary and peripheral vasodilation
Immune Activation
Immune Activation in HF
• What are cytokines?
• Low molecular weight protein molecules released by most
cell types in response to a variety of stimuli, such as
cardiac injury
• Myocardial cells are capable of synthesizing pro-
inflammatory cytokines
• Can be produced in the absence of immune system
activation
• Negative inotropes, cause muscle breakdown/wasting
• Elevated levels associated with cardiac cachexia & worse
clinical outcomes

7/20/2016
7
Cytokines
• TNF-α
• Inflammatory cytokine found in myocardium,
skeletal muscle & circulation
• Promotes LV remodeling, negative inotrope
• Promotes skeletal muscle wasting &
apoptosis
• Found in high levels in cachectic patients
Cytokines
• Interleukins
• Interleukin-1 has neg inotropic effects
• Interleukin-6 - Patients with higher IL-6
levels have worse NYHA class & poor LV
function
“Cytokine Hypothesis” for HF
• At high concentrations in lab animals, HF phenotype develops--
• LV enlargement
• LV remodeling
• LV dysfunction
• Pulmonary edema
• Cytokines don’t cause HF, but contribute to progression of HF.

7/20/2016
8
TNF Overexpression in the heart: ABC = 24 week old transgenic mice (note LV dilatation)
DEF = age matched control mouse
Deleterious Effects of Inflammatory
Mediators in HF
• LV dysfunction
• LV enlargement & remodeling
• Pulmonary edema
• Cardiomyopathy
• Endothelial dysfunction
• Anorexia and cachexia
• Skeletal muscle wasting
• Disruption of collagen weave
• Fibrosis
NYHA Class as related to Cytokine Level
10
0
2
4
6
8
Normal I II III IV
NYHA Functional Class
Seta Y, Shan K, Bozkurt B et al. J Cardiac Failure 1996; 2:243-49

7/20/2016
9
Renin-Angiotensin-Aldosterone
Endothelin
Norepinephrine
Vasopressin
Natriuretic Peptides
Nitric Oxide
Bradykinins
Vasoconstriction
Sodium/Fluid Retention
Chronic Cardiac Stress Tissue Remodeling/Fibrosis
Vasodilation
Natriuresis/Diuresis
Cardiac Stress
Remodeling
Opposition of Neurohormonal Forces
in Heart Failure
Endogenous vasoconstrictors overpower
endogenous vasodilators. This is especially true
during exercise!
Endothelin
Aldosterone
Angiotensin II
Vasopressin
Norepinephrine
NO
ANP
BNP
Harmful
Helpful
Neurohormone Wars
The Dark Side
Angiotensin IIAldosteroneNorepinephrineVasopressinEndothelinCytokines
BNP
ANP
NO
Bradykinin
The Force

7/20/2016
10
Physiologic Alterations

7/20/2016
11
Normal
collagen struts
between myocytes
Disruption of
collagen struts due
to ischemia

7/20/2016
12
Remodeling of collagen weave in hypertrophy
Matrix metalloproteinases
(MMPs) are enzymes that
degrade collagen
“Slippage” of myocytes
Cardiac Myocyte
7/20/2016
13
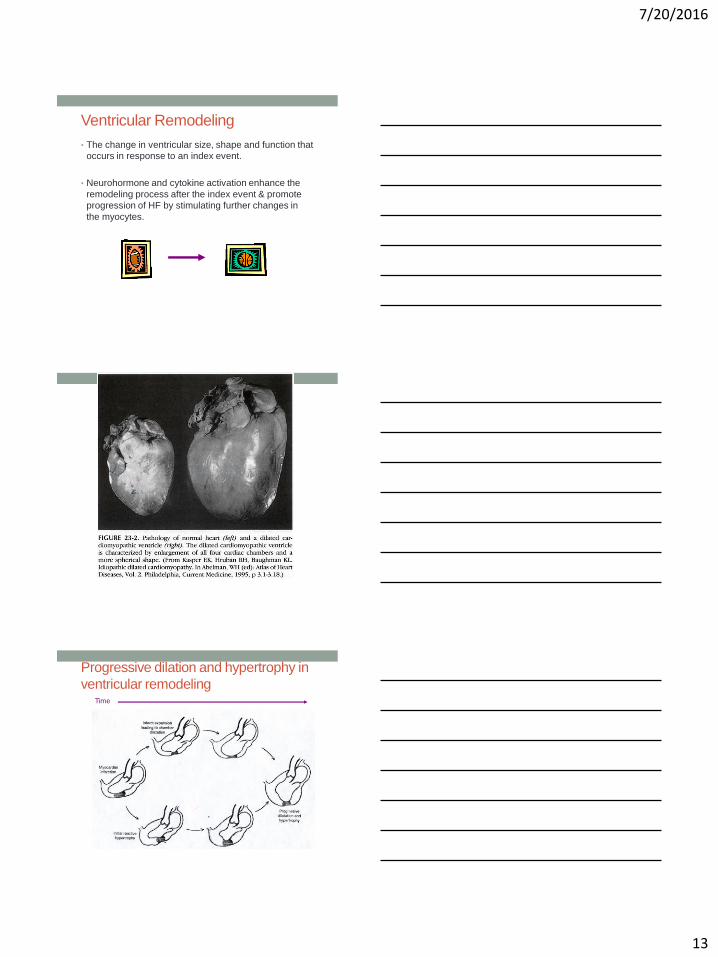
Ventricular Remodeling
• The change in ventricular size, shape and function that
occurs in response to an index event.
• Neurohormone and cytokine activation enhance the
remodeling process after the index event & promote
progression of HF by stimulating further changes in
the myocytes.
Progressive dilation and hypertrophy in
ventricular remodelingTime

7/20/2016
14
Remodeling:
Myocardial thinning and hypertrophy
Pulmonary Vasculature

7/20/2016
15
Updated WHO Clinical Classification of
Pulmonary HTN (Dana Point, 2008)• 5 Main groups
1. Pulmonary arterial hypertension (PAH)
2. Pulmonary hypertension owing to left heart disease
3. Pulmonary hypertension owing to lung diseases and/or
hypoxia
4. Chronic thromboembolic pulmonary hypertension (CTEPH)
5. Pulmonary hypertension with unclear multifactorial
mechanisms
Simonneau et al. Updated Clinical Classification of Pulmonary Hypertension. JACC 2009, 54(1); S43-S54.
2. Pulmonary hypertension due to
left heart disease• Pulmonary venous hypertension
• Systolic dysfunction
• Diastolic dysfunction
• Valvular disease
• The most common
cause of pulmonary
hypertension
Pulmonary
Artery
Pulmonary
Veins

7/20/2016
16
Now let’s bring the kidneys into the
picture…..
How are the kidneys affected in
heart failure???
Traditional Assumption:
Renal dysfunction is secondary to renal hypoperfusion
due to decreased cardiac output with heart failure
NEW HYPOTHESIS:
Renal dysfunction in patients with heart failure is more
strongly associated with venous congestion than with
reduced cardiac output

7/20/2016
17
Cardiorenal syndrome
Arterial blood flow
Venous blood flow
> 0.3 mg or 25% increase in creatinine
Hemodynamic Changes
Pathophysiology: Symptoms vs
Disease Progression
What produces progression?
Neurohormonal abnormalities
• Activation of renin-angiotensin system (RAS) andsympathetic nervous system (SNS)
• Cytokines, endothelin, vasopressin, others, etc.
What produces symptoms?
Hemodynamic abnormalities
— Changes in cardiac function and peripheral hemodynamics
Cohn JN. N Engl J Med. 1996;335:490–498.

7/20/2016
18
Cardiac Performance• Preload
• End diastolic ventricular stretch (pressure)
• Determined by venous return (ventricular filling)
• Afterload
• Arterial pressure the ventricle must pump against; aortic
pressure for LV, pulmonary pressure for RV
• Increased by norepi, angiotensin II, vasopressin
Frank-Starling Curve
2-7 mmHg
25/9 mmHg
10mmHg
25/9 (14)
90-140/5-12

7/20/2016
19
Pulmonary Hypertension or Left Heart Failure
Right Heart
Failure
Venous
CongestionWorsening
Renal Function
Right heart failure: mitral stenosis
Valve stenosis
affecting right heart muscle
Some terminology:
LV Ejection Fraction• The percentage of blood volume ejected from the left
ventricle with each heartbeat.
• Normal = 60%
• Is a measurement of the strength of contraction

7/20/2016
20
2 Types of heart failure
Filling Dysfunction (HFpEF)
• Heart failure symptoms with EF 40%
• Hypertrophic CMP, HTN, Ischemia, Age
• Impaired relaxation
Contractile Dysfunction (HFrEF)
• Depressed contractility EF 40%
• CAD, Valve disease, Ischemic and Idiopathic
CMP
• Impaired contractility
Definition of Heart FailureClassification Ejection
Fraction
Description
I. Heart Failure with
Reduced Ejection Fraction
(HFrEF)
≤40% Also referred to as systolic HF. Randomized clinical trials have
mainly enrolled patients with HFrEF and it is only in these patients
that efficacious therapies have been demonstrated to date.
II. Heart Failure with
Preserved Ejection
Fraction (HFpEF)
≥50% Also referred to as diastolic HF. Several different criteria have been
used to further define HFpEF. The diagnosis of HFpEF is
challenging because it is largely one of excluding other potential
noncardiac causes of symptoms suggestive of HF. To date,
efficacious therapies have not been identified.
a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their
characteristics, treatment patterns, and outcomes appear similar to
those of patient with HFpEF.
b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF
previously had HFrEF. These patients with improvement or recovery
in EF may be clinically distinct from those with persistently
preserved or reduced EF. Further research is needed to better
characterize these patients.
HFrEF HFpEF

7/20/2016
21
Symptom Development
Symptoms are the “Tip of the Iceberg”
in Heart Failure
Dyspnea
FatigueEdema
Orthopnea
Neurohormonal
Activation
Volume
Overload
Pressure
Overload
LV Remodeling
Fibrosis
Cytokines
Vasoconstriction
Index Event
Left Ventricular Remodeling
Neurohormonal Activation
Reduced Myocardial Function
Volume Overload & Elevated LV Filling Pressure
SymptomsDyspnea
Fatigue
Edema
Orthopnea/PND
Cough
Water is pushed out into interstitial space

7/20/2016
22
Definition of Heart Failure:
Old and New
Old definition
State in which the heart is unable to pump enough blood to meet the metabolic demands of the body
New definition
Complex clinical syndrome that results from structural and functional changes in the heart that all occur in the milieu of neurohormonal activationand cytokine release
A clinical syndrome or condition rather than a disease; the end result of a variety of diseases.
Summary
• Initiating Cause/Event
• Neurohormonal Activation
• Immune Activation
• Physiologic Alterations (remodeling)
• Systolic vs. diastolic dysfunction
• Hemodynamic Changes
• Right vs. left-sided HF
• Symptom Development


















