Pathology of the Larynx
140
1 Pathology of the Larynx Nikolay Popnikolov M.D., Ph.D. Fellow, UTMB Dept. of Pathology January 2002
Transcript of Pathology of the Larynx

1
Pathology of the Larynx
Nikolay Popnikolov M.D., Ph.D.Fellow, UTMB Dept. of Pathology
January 2002

2
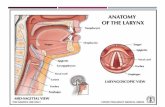
Normal Anatomy and Histology

3
Normal Anatomy and Histology

4
Normal Anatomy and Histology

5
Normal Anatomy and Histology

6
Normal Anatomy and Histology

7
Normal Anatomy and Histology

8
Laryngeal Epithelium

9
Goblet Cells and Columnar Mucinous Cells

10
Squamous Epithelium

11
Seromucinous Glands

12
Duct from Seromucinous Glands

13
Seromucinous Glands

14
Oncocytic Transformation of Seromucinous Epithelium

15
Vocal Process of the Arythenoid Cartilage

16
Chondroid Metaplasia

17
Non-neoplastic Lesions of the Larynx

18
Tuberculosis

19
Granulomatous Inflammation

20
Fungal Infections
HistolplasmosisCoccidiomycosisCryptococcosisBlastomycosisAspergilosisCandidiasis

21
Other Granulomatous Diseases
LeprosyTertiary SyphilisSarcoidosisCrohn’s diseaseWegener’s granulomatosis

22
Acute Epiglottitis
Haemophylus influenzae type BReddened, markedly edematous supraglottic structures Edema with marked infiltrate of neutrophyls with or without microabscess formation

23
Diphtheria

24
Diphtheria

25
Vocal Cord Nodules
Usually bilateralAnterior or middle third of true vocal cord Any age group Related to chronic voice abuseHoarseness or voice changes

26
Vocal Cord Polyps
Usually single Middle third of true vocal cord, but may originate from the ventricular area Any age group Sessile, raspberry-like, pedunculated Related to chronic voice abuse, infection, ETOH, smoking, hypothyroidismHoarseness or voice changes

27
Vocal Cord Polyp

28
Edematous-Myxoid Type
Submucosal accumulation of pale blue to pink material admixed with sparsely cellular and variably vascularized stroma

29
Vascular-Hyaline Type
Dilated submucosal vascular spaces and deposition of dense eosinophilic fibrin-like material

30
Vocal Cord Polyp: Fibrous Type
Moderately cellular submucosal proliferation of uniform oval to spindle-shaped cells with varying amount of fibrous tissue deposition

31
Laryngocele
Abnormal dilatation of the saccule (appendix of the ventricle) containing air and maintaining an open communication with laryngeal lumenMen >womenBilateral - 25%Hoarseness, lateral neck mass, dyspnea, dysphagia, laryngopyocele (pain)

32
Laryngocele: Types
Internal:laryngocele confined to the intrinsic larynx External:dilated sac projects upward and laterally Combined

33
Laryngocele: Etiology
Acquired:increased intralaryngeal pressure (glassblowers, musicians, weight lifters) CongenitalSCC in 15% of cases

34
Laryngocele
Smooth -surfaced, sac-like structure usually filled with air

35
Laryngocele
Respiratory epithelial-lined (ciliated, columnar) cyst with a fibrous wallSquamous metaplasiaOncocytic metaplasia

36
Laryngocele: Differential Diagnosis
Branchial cleft cystOncocytic papillary cystadenomaLaryngeal cysts

37
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx)
Benign, tumor-like condition, occurring most commonly along the posterior aspect of one or both vocal cordsMen>Women, usually adultsHoarseness, dysphagia, sore throat, dysphonia, difficulty breathing, choking, painEtiology: vocal abuse, acid regurgitation, postintubation trauma

38
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx)
Ulcerated, polypoid, nodular, or fungating mass with a beefy red to tan-white appearance, up to 3 cm in diameter

39
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx)
Ulcerated lesion with associated fibrinoid necrosis, granulation tissue, acute and chronic inflammation

40
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx)
Giant cells, vascular proliferation, and spindle cells

41
Contact Ulcers of the Larynx: Differential Diagnosis
Infectious diseasesSCCSpindle cell carcinomaVascular neoplasms: lobular capillary hemangioma, angiosarcoma, Kaposi’s sarcoma

42
Laryngeal Amyloidosis
Extracellular accumulation of fibrillar proteinsSystemic or localizedPrimary or secondaryMen > women, in the 5th and 6th decades Polypoid mass (glottis and supraglottis) or diffuse mucosal swelling (subglottis)Hoarseness

43
Laryngeal Amyloidosis
Extracellular, eosinophilic, amorphous material deposited randomly throughout submucosa; depositions around or within the walls Disappearance of the seromucous glands, Mixed chronic inflammatory infiltrate

44
Laryngeal Amyloidosis
Congo red: apple-green birefringence under polarized light

45
Subglottic Stenosis
Congenital or acquiredRare; acquired > congenitalProgressive respiratory difficulty, stridor, dyspnea, air hunger, hoarseness, abnormal cry, aphonia, dysphagiaEtiology: trauma, neoplasms, infectious or autoimmune diseases, idiopathic

46
Subglottic Stenosis
Narrowing of the endolaryngeal diameter with mucosal or submucosal mass or bulgingHistologic picture depends on the causeIdiopathic stenosis: submucosal fibrous proliferation with associated non-specific chronic inflammationDifferential diagnosis: infectious diseases, Wegener’s granulomatosis, collagen vascular diseases, neoplasms

47
Idiopathic Subglottic Stenosis

48
Terminology of Epithelial Changes
Leukoplakia:white lesion on a mucosal membrane (clinical)Erythroplakia:red lesion on a mucosal membrane (clinical)Hyperplasia:thickening of epithelial surface as a result of an absolute increase in the number of cells.Pseudoepitheliomatous hyperplasia:exuberant reactive or reparative overgrowth of squamous epithelium with no cytologic evidence of malignancy.

49
Terminology of Epithelial Changes
Keratosis:presence of keratin on an epithelial surfaceParakeratosis:presence of nuclei in the keratin layerDyskeratosis:abnormal keratinization of epithelial cellsUlceration:erosion or loss of surface epitheliumMetaplasia:change from one histologic tissue type to another

50
Terminology of Epithelial Changes
Koilocytosis:cytoplasmic vacuolization suggestive of viral (HPV) effectDysplasia or atypia:abnormal maturation and cellular aberrationsCarcinoma in situ:full thickness epithelial dysplastic change with an intact basement membrane.Superficially (microscopically) invasive SCC:SCC in which there is violation of the basement membrane with invasion into the underlying stroma.

51
Hyperplastic Epithelial Changes
Reactive or reparative benign process, reflecting the epithelial response to a stimulus or an injuryMen > womenOccurs anywhere, but mainly along the true vocal cordsHoarsenessEtiology: smoking, ETOH, voice abuse, chronic inflammation

52
Hyperplastic Epithelial Changes
Flat, papillary, or verrucoid lesion with a white (leukoplakic) or red (erythroplakic) appearanceSmall or diffuseThickening of epithelial surface as a result of an absolute increase in the number of cellsPresence of superficial keratin layer (keratosis) or nuclei in the superficial keratin layer (parakeratosis)

53
Hyperplastic Epithelial Changes
Presence of keratohyaline granules in the granulosa cell layerPresence of koilocytosisPresence of cytologic atypiaPresence of dyskeratosisDifferential diagnosis: contact ulcer, verruca vulgaris, verrucous carcinoma, well-differentiated ”conventional” SCC

54
Keratosis with Epithelial Hyperplasia w/o Dysplasia

55
Laryngeal Leukoplakia with a Papillary or Verrucoid Appearance

56
Laryngeal Leukoplakia with a Papillary or Verrucoid Appearance

57
Dysplastic Epithelial Changes
Men > womenOccurs anywhere, but mainly along the anterior portion of the true vocal cords, 25% bilateralHoarsenessEtiology: smoking, ETOH, chronic inflammation, voice abuse, Vit A deficiency, environmental exposure

58
Dysplastic Epithelial Changes
Localized, circumscribed flat or papillary area with white, red or gray appearanceCytologic alterations: hyperchromasia, increase of nuclear/cytoplasmic ratio, mitoses, crowding of cells with loss of cellular polarityBegins in basal or parabasal areas

59
Dysplastic Epithelial Changes: Grading
Mild:lower 1/3 of the thickness of epithelium Moderate:lower 2/3 of the thickness of epithelium Severe:from 2/3 to almost complete thickness

60
Dysplastic Epithelial Changes
Normal maturation of the superficial layers of the epitheliumIntact basement membraneMay be associated with keratosis or dyskeratosis, or other hyperplastic changesFull-thickness dysplasia (carcinoma in situ) is not a prerequisite prior to the development of an invasive CADifferential diagnosis: reactive epithelial changes, infectious disease, SCC

61
Flat Keratosis with Epithelial Hyperplasia and Mild Dysplasia

62
Keratosis with Moderate Dysplasia

63
Severe Dysplasia without Keratosis

64
Benign Neoplasms of the Larynx

65
Laryngeal Papilloma
Benign, exophytic neoplastic growth composed of branching fronds of squamous epithelium with fibrovascular coresThe most common benign laryngeal neoplasmNo sex predilectionChanges in phonation, dyspnea, cough, dysphagia, stridorHPV types 6 and 11

66
Laryngeal Papilloma
Juvenile type:multiple lesions with extensive growth and rapid recurrence, may remit spontaneously or persist into old ageAdult type:more often single, recurs less often, less likely to spread

67
Exophytic, warty, friable, tan-white to red growths

68
Papillary fronds of multilayered benign squamous epithelium containing fibrovascular coresLittle or no keratin production

69
Laryngeal Papilloma
Absence of stromal invasionCertain degree of cellular atypiaKoilocytic changes

70
Laryngeal Granular Cell Tumor
Men > womenHoarsenessAlong the posterior aspect of true vocal cord ( but also in supraglotic and infraglotic areas)

71
Granular Cell Tumor
Solitary, polypoid, sessile, papillary, or cystic lesion, measuring up to 3.0 cm in diameter

72
Granular Cell Tumor
Poorly circumscribed subepithelial lesion with syncytial, trabecular, or nested growth patternRound to polygonal cells with round to vesicular nuclei and coarsely granular cytoplasm. Poorly defined cell borders.Variable degree of cellular pleomorphismAbsence of mitoses or necroses

73
S-100 Protein Immunostain

74
Pseudoepitheliomatous hyperplasia

75
Granular Cell Tumor
Cytoplasmic granules:PAS/d +, Alcian blue pH 2.5 +, trichrome + (red)Angulate bodies: needle shaped, PAS + bodies in the interstitial cells Tumor cells:S-100+, NSE + Interstitial cells with angulate bodies:S-100 - and myelin protein +EM:membrane bound autophagic vacuoles containing mitochondria, RER, myelin, axon-like structures

76
Malignant Granular Cell Tumor
Rare ( 1% of all GCT)Do not occur in newbornsSize > 4 cmIncreased cellularity, pleomorphism, necrosis, prominent nucleoli, spindle shaped cells and > 2 mitoses/10 HPFMetastasize via lymphatics and blood vessels

77
Chordoma
UncommonMales > femalesDyspnea, strydor, and hoarsenessMay originates from epiglottis, cricoid, arytenoid, or thyroid cartilages May arise in Reinke’s spaceLobulated, firm to hard, blue-gray, submucosal mass, usually < 1 cm

78
Chordoma
Lobulated, normally looking chondrocytesAbsence of pleomorphism, binucleated chondrocytes, or mitotic activity

79
Rhabdomyoma
Benign tumor of striated muscleAdult type:less commonMales > females; > 40 y/oHoarseness, dyspneaWell-defined, lobulated, red-brown mass, up to 5 cm in diameter

80
Rhabdomyoma: Adult Type
Large polygonal to round cells with abundant deeply eosinophylic cyroplasm and one or two periphery placed vesicular nucleiNucleoli, cytoplasmic vacuolizationCross-striationAbsent mitosesAbundant cytoplasmic glycogen (diastase sensitive PAS positive)Desmin +, Myoglobin +

81
Rhabdomyoma: Fetal Type
Very rareMale children < 3 y/oPosterior auricular subcutaneous tissue > nasopharynx, parotis, neckSolitary, well to moderately circumscribed nodule, 1-8 cm in size, gray to pink mucoid appearance

82
Rhabdomyoma: Fetal Type
Spindle cells and immature muscle fibers with in a myxoid stromaCross-striation rarely discernible. Mature muscle fibers can be seen in the peripheryAbsence of mitoses, necrosis, and significant pleomorphism

83
Malignant Laryngeal Neoplasms

84
In Situ Squamous Cell Carcinoma
Males > females6th – 7th decadesMost often involves anterior portion of true vocal cordHoarsenessMay coexist with invasive SCCMay be isolated or multifocalCircumscribed or diffuse lesion with a white, red, or gray color and smooth or granular appearance

85
In Situ Squamous Cell Carcinoma
Dysplastic process involves the entire thickness of the epitheliumLoss of cellular maturation and polarityIncrease of nuclear/cytoplaslic ratioNormal and abnormal mitosesKeratosis and dyskeratosisExtension into adjacent seromucinous glands

86
Microinvasive or Superficially Invasive Squamous Cell Carcinoma
Nests of malignant cells that have penetrated the basement membrane and invaded superficially into the submucosaCapable of metastasizingDevelopment from carcinoma in situ or from epithelium with no evidence of CIS

87
Invasive Squamous Cell Carcinoma
2.5% of all cancers in men0.5% of all cancers in women95% of all laryngeal carcinomasEtiology: ETOH (supraglottic), tobacco (glottic), asbestos, nickel, wood, isopropyl alcohol, radiationDD: reactive epithelial changes, pseudoepitheliomatous hyperplasia

88
Invasive Squamous Cell Carcinoma

89
Supraglottic Squamous Cell Carcinoma
25–40% of laryngeal SCCEpiglottis (base), false vocal cordsChanges in the quality of voice, dysphagia, odonophagia, hoarseness, hemoptisis, dyspneaMarginal carcinomas (suprahyoid epiglottis, aryepiglottic folds); remain quiescent for longer period and present at more advanced stage

90
Supraglottic Squamous Cell Carcinoma
Ulcerated, flat, exophytic, or papillaryTend to be nonkeratinizingIn situ componentMitoses and necrosis

91
Supraglottic Squamous Cell Carcinoma
Large, tan-white neoplasm in the right supraglottis, extending upward toward epiglottis

92
Supraglottic Squamous Cell Carcinoma

93
Glottic SCC
Early: irregular area of mucosal thickeningAdvanced: exophytic, fungatic, endophytic, ulcerated massMore commonly keratinizing, well to moderately differentiatedIn situ componentInvasive component predominantly infiltrative

94
Glottic SCC

95
Glottic SCC

96
Glottic SCC

97
Subglottic Squamous Cell Carcinoma
5% of all laryngeal tumorsTend to remain clinically quiescent, presenting with advanced stageAirway obstruction (dyspnea, stridor) and vocal cord fixation (voice changes)Large exophytic, fungating, ulcerating, or endophyticTend to be keratinizing moderately to poorly differentiatedIn situ component is less commonInvasive pattern is predominantly infiltrative

98
Subglottic SCC

99
Subglottic Squamous Cell Carcinoma
Overall 5-year survival rate < 40%Spread: Into thyroarytenoid muscle (vocal cord fixation) Anteriorly: through cricothyroid membrane into thyroid gland superiorly: glottis and supraglottis inferiorly: trachea posteriorly: below the cricoid cartilage and into the esophagusLymphatic drainage: upper and lower jugular chains, perlaryngeal and paratracheal nodesStomal recurrent tumor

100
Transglottic SCC
Involves both glottic and supraglottic structuresRepresents advanced tumorNodal metastases and extranodal spreadOverall 5-year survival rate < 40%

101
Transglottic SCC

102
Spindle Cell (Squamous) Carcinoma (SCSC)
Foci of conventional SCC associated with malignant spindle cell stromal componentSynonyms: carcinosarcoma, pleomorphic carcinoma, metaplastic carcinoma, collision tumor, pseudosarcoma, Lane tumorMen (85%), 6th –8th decadesTrue vocal cords > false vocal cords and supraglottis > oral cavity > skin > tonsil and pharynxSymptoms vary according to siteNo specific etiology

103
Spindle Cell (Squamous) Carcinoma (SCSC)

104
Spindle Cell (Squamous) Carcinoma (SCSC)
Spindle cell component with variable degree of pleomorphism, mitosesFascicular, storiform, or palisading patterns; may be associated with myxomatous stroma

105
Spindle Cell (Squamous) Carcinoma (SCSC)
Spindle cells are cytokeratin-positive, but negativity does not exclude the diagnosis

106
Heterologous Elements

107
Spindle Cell (Squamous) Carcinoma (SCSC)
Differential diagnosis: Reactive (fibroblastic) proliferationMalignant fibrous histiocytomaFibrosarcomaMalignant melanoma

108
Spindle Cell (Squamous) Carcinoma (SCSC)
Controversial histogenesis. Epithelial derivation is support by:Association with conventional SCC ICH: cytokeratin + Cartilage or bone component have not been reported in metastasesMetastases may include conventional or/and spindle cell componentPoor prognosis (metastases in lymph nodes and lungs)

109
Verrucous Carcinoma
Highly differentiated variant of SCC with focally destructive, but not metastatic capabilities1-3% of all laryngeal carcinomasMen > women, 6th – 7th decadesOral cavity > nasal fossa > sinonasal tract, nasopharynxLarynx: hoarsenessIn the larynx most common in the glottic areaPotential etiologic factors: tobacco, viruses

110
Verrucous Carcinoma
Tan or white, warty, fungating, or exophytic, firm to hard mass, attached by a broad baseSquamous cell proliferation: uniform cells without dysplastic features and mitoses marked surface keratinization broad or bulbous rete pegs with pushing, NOT infiltrative marginDysplastic features limited and confined to basal soneMixed chronic immflammarory cell infiltrate

111
Verrucous Carcinoma
Tan or white, warty, fungating, or exophytic, firm to hard mass, attached by a broad base

112
Verrucous Carcinoma

113
Verrucous Carcinoma
Squamous cell proliferation: uniform cells without dysplastic features and mitoses marked surface keratinization broad or bulbous rete pegs with pushing, NOT infiltrative marginDysplastic features limited and confined to basal zoneMixed chronic inflammatory cell infiltrate

114
Verrucous Carcinoma
Differential diagnosis:Keratotic squamous papillomaReactive keratosis and epithelial hyperplasiaPseudoepitheliomatous hyperplasiaVerruca vulgarisKeratoacantoma“Conventional” SCC

115
Verrucous Carcinoma
Metastasis in regional lymph nodes are rare, and distant metastases do not occurExcellent prognosis after complete surgical removalAnaplastic transformation may result in distant metastasesAdequate biopsy material with a good epithelial-stromal interface is critical for the interpretationCervical adenopathy- reactive changes

116
Basaloid Squamous Cell Carcinoma
An invasive neoplasm, composed of basaloid cells UncommonMen > women, 6th – 7th decadesHypopharynx (pyriform sinus), larynx (supraglottis), and tongueHoarseness, dysphagia, pain, neck massEtiology: ETOH, tabaccoCell of origin: unclear

117
Basaloid Squamous Cell Carcinoma
Firm to hard, tan-white mass, often with associated central necrosisPatterns: solid, lobular, cell nests, cribriform, cords, trabeculae, gland-like, or cysticComedonecrosisIntercellular deposition of a hyaline or mucohyalin materialFocal squamous differentiation or association with SCC, SCCIS, squamous dysplasia, or spindle cell component

118
Basaloid Squamous Cell Carcinoma
Infiltrating tumor originating from the surface epithelium with solid growth pattern and comedonecrosis

119
Basaloid Squamous Cell Carcinoma
Small, closely apposed cells with hyperchromatic nuclei, scanty cytoplasm, marked mitotic activity, large cells or pleomorphism can be seen

120
Basaloid SCC with Focal Keratinization

121
Basaloid Squamous Cell Carcinoma
Histochemistry:PAS+ and Alcian blue + material in the cystic spacesIHC:
cytokeratin (+), EMA (+), CEA (+), S-100 (+); chromogranin (-), synaptophysin (-), muscle-specific actin (-)EM:basaloid component: desmosomes, rare tonofilaments cystic spaces: stellate granules or replicated basal lamina

122
Basaloid SCC: Differential Diagnosis
Adenoid cystic carcinomaNeuroendocrine carcinomaAdenosquamous carcinomaSpindle cell carcinoma

123
Basaloid Squamous Cell Carcinoma
Multifocal, deeply invasive, metastatic Metastases: lymph nodes, lung, bone, skin, brainMetastases include both basaloid and squamous componentsRapidly fatal

124
Adenosquamous Carcinoma
Malignant high grade epithelial neoplasm with histologic features of adenocarcinoma and SCCUncommonMen > women, 6th – 7th decadesLarynx, hypopharynx, oral cavity, sinonasal cavityHoarseness, dysphagia, pain, neck mass, nasal obstructionEtiology: not clear (ETOH, tobacco)Cell of origin: unclear; possible a single totipotential cell from surface epithelium or seromucous glands

125
Adenosquamous Carcinoma
Exophytic or submucosal, friable, edematous or granular mass with or without surface ulcerationsSCC component:Well to poorly differentiated, associated in situ carcinoma or invasive SCCIndividual cell keratinization, intercellular bridges, keratin pearl formation, dyskeratosisAdenocarcinoma component:In the submucosa, glandular differentiation, Both components can be admixedCellular pleomorphism, mitoses, necrosis, perineural invasion

126
Adenosquamous Carcinoma

127
Adenosquamous Carcinoma
Histochemistry: PAS/d (+) and mucicarnine (+) intraluminal materialIHC: cytokeratin (+)Behaves very aggressively, irrespective of the size of neoplasm Early lymph node metastases, lung, liverPoor prognosis: 5-year survival rate of

128
Neuroendocrine Carcinoma: Classification
Carcinoid(well differentiated)Atypical carcinoid(moderately differentiated)Small (“oat”) cell carcinoma(poorly differentiated)

129
Neuroendocrine Carcinoma
Submucosal nodular or polypoid mass with tan-white appearance and up to 4 cm in diameterSurface ulceration may present in moderately or well-differentiated neuroendocrine carcinoma

130
Carcinoid
Organoid or trabecular growth pattern with fibtovascular stromaGlands or squamous differentiation can be seenAbsence of surface ulceration

131
Carcinoid
Uniform cells with centrally located round nuclei, vesicular chromatin, and eosinophilic cytoplasmAbsence of pleomorphism, mitoses, necrosesLow nuclear:cytoplasmic ratio

132
Carcinoid
Histochemistry:PAS/d + mucin, argyrophiliaIHC:Cytokeratin +, Chromogranin +, NSE +, synaptophysin +EM:neurosecretory granules, cellular junctional complexes

133
Atypical Carcinoid
Organoid, trabecular, cribriform, or solid gowth patternMild to marked cellular pleomorphismNucleoli may be prominentMitoses and focal necrosis Variable nuclear:cytoplasmic ratio
Surface ulceration andlymphovascular and perineural invasion

134
Small Cell Carcinoma
Solid nests, sheets, or ribbons, with absence of fibrovascular stromaSurface ulcerationLymphovascular and perineural invasionGlandular or squamous differentiation is rarely seen

135
Small Cell Carcinoma
Marked cellular pleomorphism, ‘crush’ artifacts, necrosis, hyperchromatic oval to spindle nuclei, abundant mitosesHigh nuclear:cytoplasmic ratioIHC: cytokeratin, chromogranin, synaptophysin, NSE positiveEM: rare neurosecretory granules

136
Chondrosarcoma
RareMales >Females, 4th - 7th decadesCricoid > thyroid cartilage > arytenoidSmooth, lobulated, hard submucosal mass larger than 2 cm

137
Chondrosarcoma (high grade)
Lobulated hypercellular tumor with hyperchromatic, pleomorphic nuclei and prominent nucleoliBinucleate or multinucleated cellsMitoses: usually
uncommon

138
Synovial Sarcoma

139
Synovial Sarcoma

140
Synovial Sarcoma