Pathology of Rheumatic Fever 2009

of 54
Transcript of Pathology of Rheumatic Fever 2009
-
8/14/2019 Pathology of Rheumatic Fever 2009
1/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
2/54
Rheumatic feverRheumatic fever
-
8/14/2019 Pathology of Rheumatic Fever 2009
3/54
RHEUMATIC FEVERIs immunologically mediated, multisysteminflammatory disease that occurs a few weeksfollowing an episode of group A hemolyticstreptococcal pharyngitis.-both sexes are equally affected between 5-
15 years
-
8/14/2019 Pathology of Rheumatic Fever 2009
4/54
The incidence and mortality rate of RF have declinedremarkably in many parts of the world over the past30 years, owing to improved socioeconomic conditions,and an unexplained decrease in the virulence of group
A streptococci. Nevertheless, in developing countries,and in many crowded, economically depressed urbanareas in the Western world, RF remains an importantpublic health problem.
-
8/14/2019 Pathology of Rheumatic Fever 2009
5/54
AETIOLOGYPredisposing factors:
1-Hereditarypredisposition
2-Cold climate, low socio-economic standards
overcrowding andmalnutritionrecurrent streptococcaltonsillitis
Exciting cause: abnormalimmune reaction.
-
8/14/2019 Pathology of Rheumatic Fever 2009
6/54
uresofacuterheumatic
-
8/14/2019 Pathology of Rheumatic Fever 2009
7/54
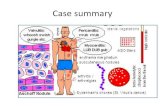
PATHOGENESIS -Group A strep pharyngeal infection precedes clinicalmanifestations of ARF by 2 - 6 weeks
-Antibodies made against group A strep cross-react
with human tissue because of molecular mimicry. heartvalve and brain share common antigenic sequences withGAS bacteria starting the formation of allergic granuloma.
-Only a minority of infected patients develop RF, suggesting
the role of genetic susceptibility
-
8/14/2019 Pathology of Rheumatic Fever 2009
8/54
PathogenesisMost important antigenic proteins in externallayer of cell wall M, T
and R proteins
-
8/14/2019 Pathology of Rheumatic Fever 2009
9/54
TISSUE REACTION
Characteristic lesion known as Aschoffs body.
Central area of necrosis.
Collection of chronic inflammatory cells withoccasional Aschoff giant cells.
Fate: Fibrosis.
-
8/14/2019 Pathology of Rheumatic Fever 2009
10/54
Normal myocarduim Aschoffbodies
-
8/14/2019 Pathology of Rheumatic Fever 2009
11/54
Aschoff body
-
8/14/2019 Pathology of Rheumatic Fever 2009
12/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
13/54
Clinical diagnosis:
The clinical diagnosis of acute rheumatic fever is madewhen two major or one major and two minor criteria -Jones Criteria, are met.The major clinical manifestations include - Carditis ,Erythema marginatum ,Migratory large joint arthritis ,
Sydenham chorea (a neurologic disorder with involuntarypurposeless, rapid movements),Subcutaneous nodules.
The minor manifestations include - arthralgia ; fever ;certain laboratory tests indicative of an inflammatoryprocess (Eg: , positive test for C-reactive protein,leukocytosis) and electrocardiographic changes
-
8/14/2019 Pathology of Rheumatic Fever 2009
14/54
Major manifestations Minor manifestations
Carditis Fever
Arthritis Arthralgia
Sydenhams chorea laboratory tests indicative of aninflammatory process
Erythema marginatum electrocardiographic changes
Subcutaneous nodules
Guidelines for the diagnosis of initial attack of rheumatic fevrer
Jones Criteria
-
8/14/2019 Pathology of Rheumatic Fever 2009
15/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
16/54
Subcutaneous nodules are rarely seen and whenpresent, they are usually associated with severecarditis. They are painless, firm, movable, measuringaround 0.5 to 2 cm. They are usually located overextensor surfaces of the joints, particularly knees,
wrists and elbows
-
8/14/2019 Pathology of Rheumatic Fever 2009
17/54
Erythema marginatumon the trunk, showingerythematous lesions with pale centers and roundedor serpiginous margins
-
8/14/2019 Pathology of Rheumatic Fever 2009
18/54
Acute rheumatic feverThe predominant clinical manifestations are those of carditis andarthritis
acute carditis: (pancarditis)includePericarditis ,myocarditis,endocarditis:During the acute stage, The myocarditis may cause cardiac dilationthat may evolve to functional mitral valve insufficiency or even heart
failure.but with chronic disease, endocarditis with permanent valvelesions are most serious and dangerous. The patholigical change of thevalve lead to its stenosis and or regurgitation.
Arthritis It typically begins with migratory arthritis accompanied byfever in which one large joint after another becomes painful and swollenfor a period of days and then subsides spontaneously, leaving no residual
disability.
-
8/14/2019 Pathology of Rheumatic Fever 2009
19/54
PATHOLOGYRheumatic carditis: Pancarditis1-Rheumatic Endocarditis
2-Rheumatic Myocarditis
3-Rheumatic pericarditis.
-
8/14/2019 Pathology of Rheumatic Fever 2009
20/54
RHEUMATIC ENDOCARDITIS
Valvular endocarditis: affects the valvular
endocardium especially arotic and mitral valve
Mural endocarditis: affects the mural endocardiumof the posterior wall of the left atruim
-
8/14/2019 Pathology of Rheumatic Fever 2009
21/54
Acute Rheumatic Valvulitis
Multipleepisodes of acute Rheumatic fever.Inflammation of the cardiac cusps with the formation of Aschoffs
nodules with edema results in swelling of the leaflets of the cusps,friction of their free borders.injury of the endotheliumthrombosis(vegetations(
-Acute phase subsides then fibrosis alters leaflet and cusp
structureresults in leaflet or cuspal thickening along valvularmargins of closure, commissural fusion and shortening, and thickeningand fusion of the tendinous cords..
Valves affected. Most often mitral valve alone .Then most oftenmitral and aortic together .Lastly aortic alone
-
8/14/2019 Pathology of Rheumatic Fever 2009
22/54
AcuteRheumaticValvulitisValve cusps are swollenand red
- Vegetations arefound near the freemargin of cusps( small, beaded, paleand adherent)
Mitral valve vegetations
http://www.pathology.vcu.edu/education/cardio/images/2e-d.jpg -
8/14/2019 Pathology of Rheumatic Fever 2009
23/54
Mitral valve vegetationsRF
Vegetation fibrin
-
8/14/2019 Pathology of Rheumatic Fever 2009
24/54
Vegetation, fibrin,platelets
-
8/14/2019 Pathology of Rheumatic Fever 2009
25/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
26/54
RHEUMATIC MYOCARDITIS
Aschoff's bodies are seen in interstitial tissue ofthe myocardium and associated with interstitialedema and mild inflammation, sometimes
with muscle fiber necrosis.
- The condition is usually mild, but mayproduce left ventricular failure.
Rheumatic
-
8/14/2019 Pathology of Rheumatic Fever 2009
27/54
Rheumaticmyocarditis
Aschoff giant
-
8/14/2019 Pathology of Rheumatic Fever 2009
28/54
Aschoff giantcells
-
8/14/2019 Pathology of Rheumatic Fever 2009
29/54
RHEUMATIC PERICARDITISRheumatic fever is the commonest cause of sero-fibrinous pericarditis mainly at the heart base,
the pericardial sac is filled with serous fluidand fibrin is deposited on both visceral andparietal pericardium. Pericarditis heals byorganization (fibrosis) which can result in
Adhesions between the visceral and parietalpericardium. Separation of which producesbread and butter appearance.
Aschoffs' bodies may be seen.
-
8/14/2019 Pathology of Rheumatic Fever 2009
30/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
31/54
Serofibrinous pricarditis,
Serofibrinous pericarditis
-
8/14/2019 Pathology of Rheumatic Fever 2009
32/54
Serofibrinous pericarditis,
-
8/14/2019 Pathology of Rheumatic Fever 2009
33/54
Serofibrinous pericarditis,
Serofibrinous pricarditis fibrin
-
8/14/2019 Pathology of Rheumatic Fever 2009
34/54
Serofibrinous pricarditis, fibrinthreads
-
8/14/2019 Pathology of Rheumatic Fever 2009
35/54
Pericarditis, fibrin at the
-
8/14/2019 Pathology of Rheumatic Fever 2009
36/54
COMPLICATIONS OF RF
-Valvular lesions.
- Infective endocarditis
Heart failure
-
8/14/2019 Pathology of Rheumatic Fever 2009
37/54
Valvular damageHealing of acute valvular lesion by fibrosis with fusion
of the cusps result in inability of the valve to openproperly.
Stenosis
Healing of acute valvular lesion by fibrosis withcontraction of the cusps result in inability of the
valve to close properly.incompetence
-
8/14/2019 Pathology of Rheumatic Fever 2009
38/54
Stenotic mitral valve
seen from left atrium.Both commissures arefused; the cusps areseverely thickened.
-
8/14/2019 Pathology of Rheumatic Fever 2009
39/54
This view of the atrioventricular valves shows marked stenosis ofthe mitral valve, and less severe involvement of the tricuspidvalve..
Thickened mitral valve, fibrotic chordae tendinae
http://www.pathology.vcu.edu/education/cardio/images/2f-a.jpg -
8/14/2019 Pathology of Rheumatic Fever 2009
40/54
Thickened mitral valve, fibrotic chordae tendinae
-
8/14/2019 Pathology of Rheumatic Fever 2009
41/54
Effect of MitralStenosis
On Heart
-Left atrium hypertrophiesand dilates and its pressure
increase. It leads topulmonary venoushypertension and oedema
-increased pulmonary
arterial pressure andpulmonary vascularresistance . Right ventricledilates from pressureoverload .. Right heart
failure develop
-
8/14/2019 Pathology of Rheumatic Fever 2009
42/54
Effect of Mitral Stenosis
On Heart
-Atrial fibrillation and thrombosis may occur.-Left ventricles protected by stenotic mitralvalve
-LV usually normal in size and contour
-
-
8/14/2019 Pathology of Rheumatic Fever 2009
43/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
44/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
45/54
Valvular damageMitral incompetance-may occur alone or associated
with mitral stenosis.
- Blood accumulates in the leftside of the heart hypertrophythen dilatation of both the leftventricle and atrium and then left
side heart failure.
http://en.wikipedia.org/wiki/File:Mitral_Regurgitation_scheme1.png -
8/14/2019 Pathology of Rheumatic Fever 2009
46/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
47/54
Aortic Regurgitation
-the leaflets of thevalve do not fittogether properly lead
to left ventriculardilatation and failure
-
8/14/2019 Pathology of Rheumatic Fever 2009
48/54
Valvular damageAortic Stenosis-Fusion, thickening of the cusps leading to concentric left ventricularhypertrophy. Inadequate coronary perfusion lead to syncope and angina.Eventually. Left ventricular failure develop.
-
8/14/2019 Pathology of Rheumatic Fever 2009
49/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
50/54
INFECTIVE ENDOCARDITIS
-Infection of the endocardium (esp. heart valves) by amicrobiological agent, with the formation ofvegetations of fibrin, inflammatory cells, & bacteria
or other organisms.-Vegetations located most commonly on heart valves,
esp. aortic & mitral.
-Vegetation may produce emboli that produce infarctsin brain, kidney, myocardium, & other organs
-
8/14/2019 Pathology of Rheumatic Fever 2009
51/54
Vegetation of infective endocarditis
-
8/14/2019 Pathology of Rheumatic Fever 2009
52/54
Heart failure
Heart failure (HF) is a condition in whichthe heart is unable to provide the bodywith enough blood and nutrients to meetits metabolic needs. Heart failure is
usually caused by failure of the heart tofunction efficiently as a pump-It may be acute or chronic.-Chronic may be right or left sided or
total heart failure.
-Blood backs up causing congestion of neck veins and swelling ofextremities and internal organs
-
8/14/2019 Pathology of Rheumatic Fever 2009
53/54
-
8/14/2019 Pathology of Rheumatic Fever 2009
54/54