Pathological fractures
54
Pathological Fractures
-
Upload
raunak-milton -
Category
Healthcare
-
view
101 -
download
0
Transcript of Pathological fractures
Pathological Fractures
• Pathologic fractures occur in abnormal bone. • Weakened bone predisposes the patient for
failure during normal activity or after minor trauma.
Systemic- non neoplastic
Correctable• Renal osteodystrophy• Hyperparathyroidism• Osteomalacia• Disuse osteoporosis
Uncorrectable• Osteogenesis imperfecta • Polyostotic fibrous dysplasia• Postmenopausal
osteoporosis• Paget disease• Osteopetrosis
• Weak bones predisposed to fractures.• Poor callus formation.• Slow healing.
• Common metastatic cancers-– Breast– Lung– Prostate– thyroid– kidney
• Common sites of metastasis-– Spine– Pelvis– Ribs– Skull– proximal femur– Proximal humerus.
History
• Degree of trauma• Presence of prodromal pain- dull aching to
intense pain.• Exacerbated by weight bearing.• Previously diagnosed or treated cancer,• h/o radiation Rx• Weight loss, fever, night sweats, fatigue.
Factors suggesting path #
• Spontaneous fracture• Fractures after minor trauma• Pain at the site before the fracture• Multiple recent fractures• Unusual # patterns• Patient older than 45 years.• History of malignancy.
Examination
• Palpation of mass• Identification of obvious deformity• Neurovascular examination.• Evaluation of possible primary sites(Breast,
prostate, lung, thyroid)• Lymphadenopathy.
Lab
• CBC• ESR• Electrolytes• BUN• Serum glucose• Liver function tests
• Total protein• Albumin• Calcium, phosphorus,
and alkaline phosphatase.
• Anemia, hypercalcemia, increased ALP- widespread metastasis.
• Serum and urine electrophoresis- multiple myeloma
• Microsopic hematuria- RCC• TFT, CEA, CA-125, PSA.
• N-telopeptide and C-telopeptide are markers of bone collagen breakdown measured in serum and urine.– Confirm increased destruction caused by bone
metastasis– Measure the overall extent of bone involvement– Assess the response of the bone to
bisphosphonate treatment
Demers LM, Costa L, Lipton A. Biochemical markers and skeletal metastases. ClinOrthop Relat Res. 2003;(415):S138–S147.
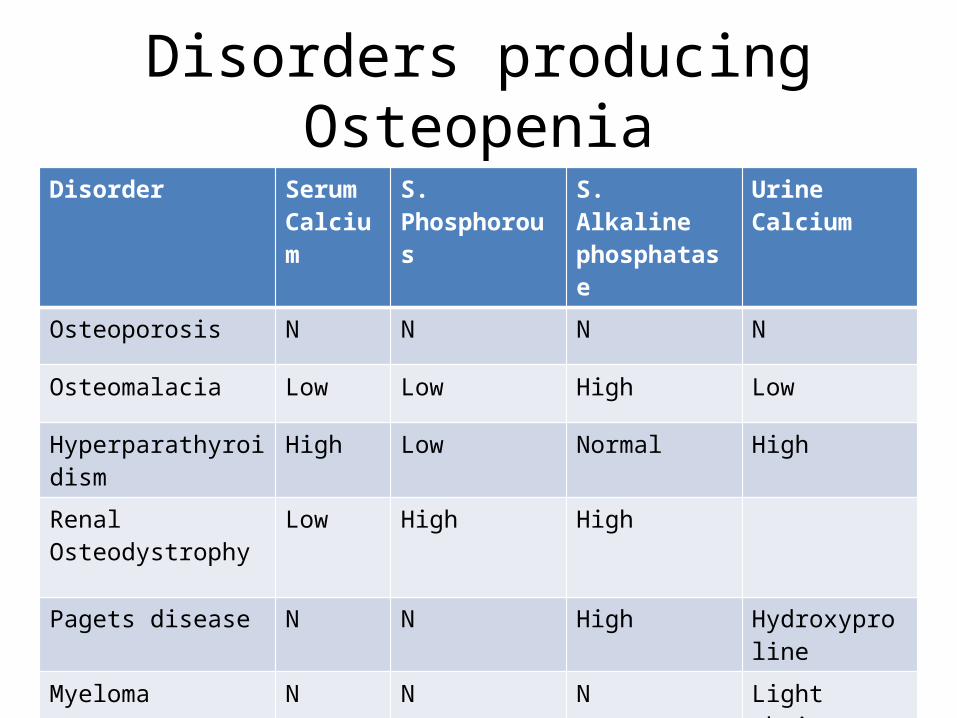
Disorders producing OsteopeniaDisorder Serum
CalciumS. Phosphorous S. Alkaline
phosphataseUrine Calcium
Osteoporosis N N N N
Osteomalacia Low Low High Low
Hyperparathyroidism High Low Normal High
Renal Osteodystrophy Low High High
Pagets disease N N High Hydroxyproline
Myeloma N N N Light chains
Associated Medical Problems
• Limitation of ADL due to pain/pathological fractures.
• Neurological deficits/ paralysis in spinal fractures.
• Prolonged recumbency predisposes to hypercalcemia.
• Anemia• Hypercalcemia of malignancy- poor prognosis.
Hypercalcemia- Clinical features
• Neurologic- Headache, confusion, irritability, blurred vision.
• GI- Anorexia, Nausea, Vomiting, Weight loss. Constipation, abdominal pain.
• MSK- Fatigue, Weakness, joint and bone pain, unsteady gait.
• Urinary- Nocturia, polydipsia, polyuria.
• Level of hypercalcemia does not always correlate with the severity of the metastasis.
• Vigorous volume repletion- treat the tumor directly/ bisphosphonates to reduce osteoclastic activity.
• All biochemical parameters should be corrected prior to surgery.
Ennekings questions
• Where is the lesion?– Epiphysis/Metaphysis/ Diaphysis– Cortex/ Medullary canal– Long bone/ Flat bone
• What is the lesion doing to the bone?– Osteolysis- Total/ Diffuse/ Minimal
• What is the bone doing to the lesion?– Well defined reactive rim- benign/slow growing– Intact but abundant periosteal reaction-
Aggressive– Periosteal reaction that cannot keep up with
tumor- Malignant
• Clues to tissue type within the lesion-– Calcification-Bone infarct/ Cartilage tumor– Ossification-Osteosarcoma/ Osteoblastoma– Ground glass appearance- Fibrous dysplasia
• Entire bone to imaged.• Pain in the distal sites can have proximal
source.

• Osteopenia- indicates inadequate bone(osteoporosis) or inadequately mineralised bone(osteomalacia)
– Looser lines-compression side radiolucent lines– Calcification of small vessels– Phalangeal periosteal reaction
• s/o osteomalacia or hyperparathyroidism
• Osteoporosis-– Thinning of cortices– Loss of normal trabecular pattern
• Permeative or moth eaten pattern of cortical destruction is highly suggestive of malignancy.
• >40 yrs- Metastatic carcinoma, myeloma, lymphoma.
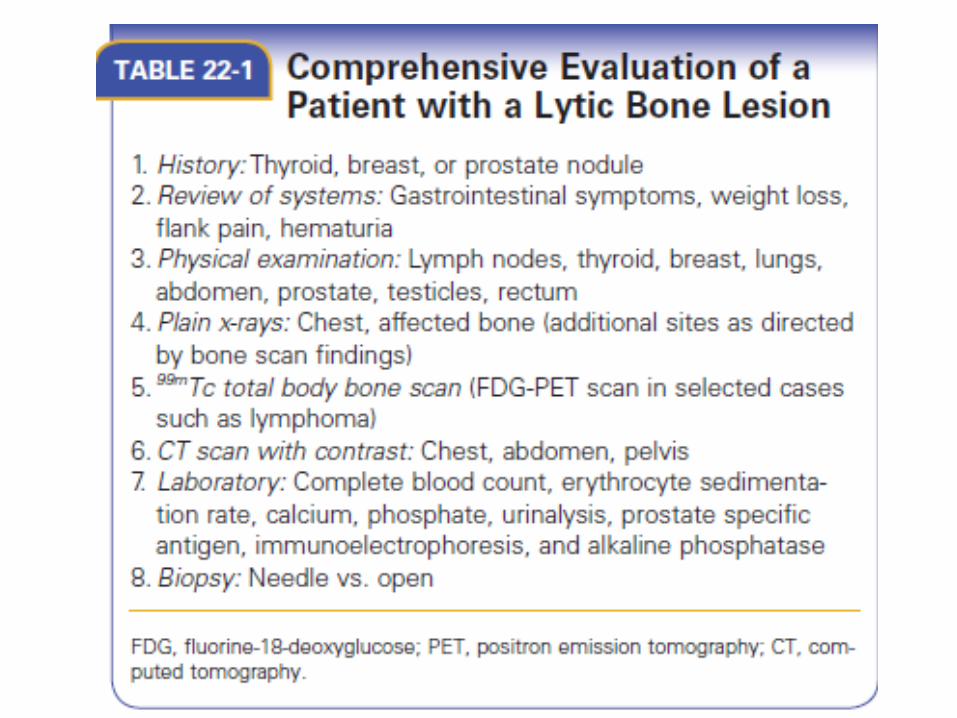
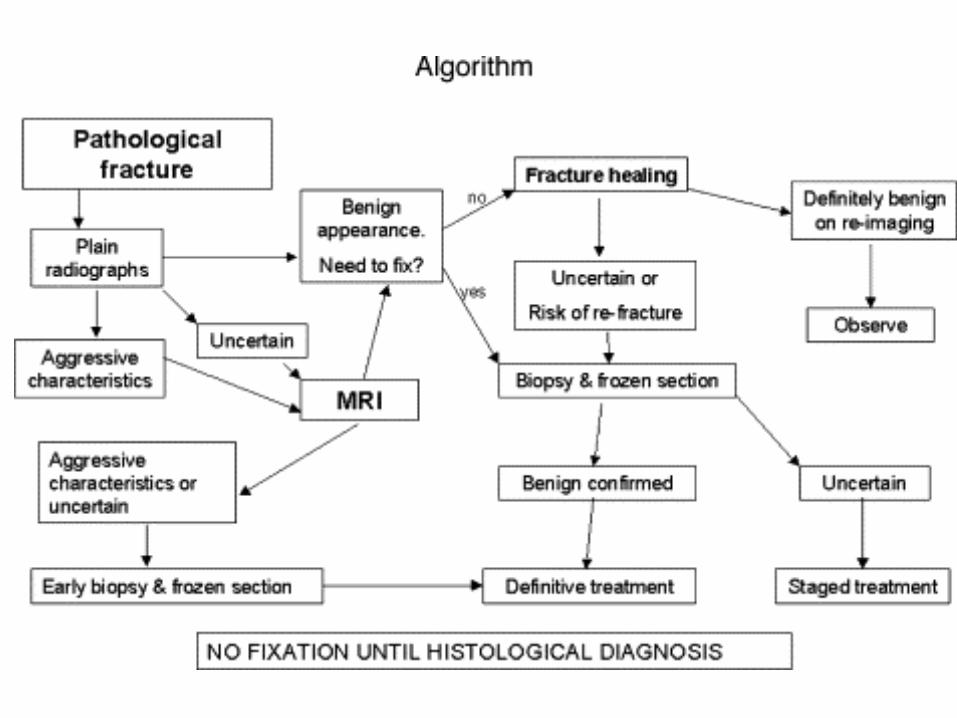
Performing biopsy for lytic lesions
• Solitary bone lesion in a patient with or without history should be done.
• Needle biopsy is definitive when differentiating carcinoma from sarcoma with adequate immunohistochemistry.
• When there is pathologic fracture through the lytic lesion, bleeding can occur due to early fracture callus.
• Thus these fractures should be stabilised first and then biopsy undertaken.
• Biopsy should be obtained from a site near but unaffected by fracture.
• Site should be as small as possible, longitudnally in line with the extremity.
• Tissues involved in post- biopsy hematoma must be considered as contaminated.
• Cultures for all biopsy to rule out infections that may mimic tumors on x rays.
• If definitive diagnosis present on frozen sections intraop then ideal to fix the fractures, otherwise wait for permanent sections.
Impending pathological fractures
• Known skeletal mets usually treated by radiation/chemotherapy +/- prophylactic fixation.
• Radiological assesment of lesion and patient symptoms necessary to calculate the risk.
• Mirels developed a scoring system based on pain, location, size of the lesion,radiographic appearance.

Mirel’s CriteriaVariable 1 2 3
Site Upper extremity Lower extremity Peritrochanteric
Pain Mild Moderate Severe
Lesion Blastic Mixed Lytic
Size <1/3rd diameter 1/3rd-2/3rd >2/3rd
• Lesions with score of less than 7 can be irradiated safely, >8 require prophylactic fixation.
• Patients treated prophylactically have:– Shorter hospitalization – More immediate pain relief– Faster and less complicated surgery– Less blood loss– Quicker return to premorbid function– Improved survival– Fewer hardware complications
• Fracture risk is greatest during patient positioning, prepration and draping.
• Decision making includes:– Life expectancy of the patient– Patient comorbidities– Extent of the disease– Tumor histology– Anticipated future oncologic treatments– Degree of pain
Management considerations
• Treatment of local bone lesion-• Surgical stabilisation +/- resection: large lytic
lesion at risk of fractures/pathologic fractures.• Radiation: Adjuvant local treatment for entire
operative field. • Functional bracing• Bisphosphonates: inhibit osteoclast mediated
bone resorption.
• Perioperative antibiotics• Thromboembolic prophylaxis• Nutrition: Serum prealbumin• Post operative pulmonary exercises• Early mobilisation.
Bracing
• Indicated in-– Limited life expectancies– Severe comorbidities– Small lesions– Radiosensitive tumors
• Humerus shaft, forearm, tibia• Weight bearing should be limited.
Operative treatment
• Intramedullary device or modular prosthesis provides better stability.
• Bone cement-– Increases the strength of fixation– Should not be used to replace segment of bone
• Goal should be to stabilize as much of the bone as possible.
Options
• Proximal, total humeral endoprosthesis.• Humerus shaft- locked intramedullary nails,
intercalary allograft.• Distal humerus- flexible intramedullary nail,
bicondylar fixation, resection with modular distal femur reconstruction.
• Radius/ Ulna- Flexible rods, rigid plate fixation,radial head resection, curettage.

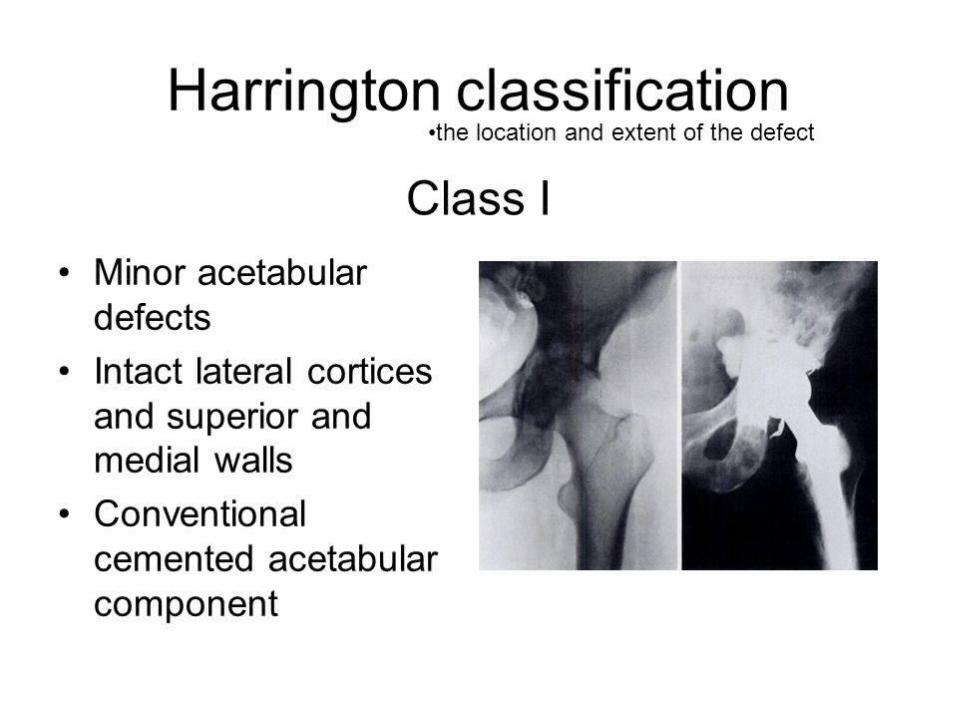
Periacetabular lesions
• Harrington classification:• Class I lesion- – Minor defects, with maintenance of lateral cortex,
superior wall, medial wall.– Treated with conventional cemented acetabular
component.• Class II- – Major acetabular defect with deficient medial wall and
superior dome.– Antiprotrusion device/ medial mesh

• Class III– Massive defects with deficient lateral cortex and
superior bone.– No substantial peripheral rim for fixation of metal
component.– Acetabular cage with long screw fixation into
remaining pubis,illium or ischium.– Bone cement to provide stability and steinmann
pins to anchor the construct.
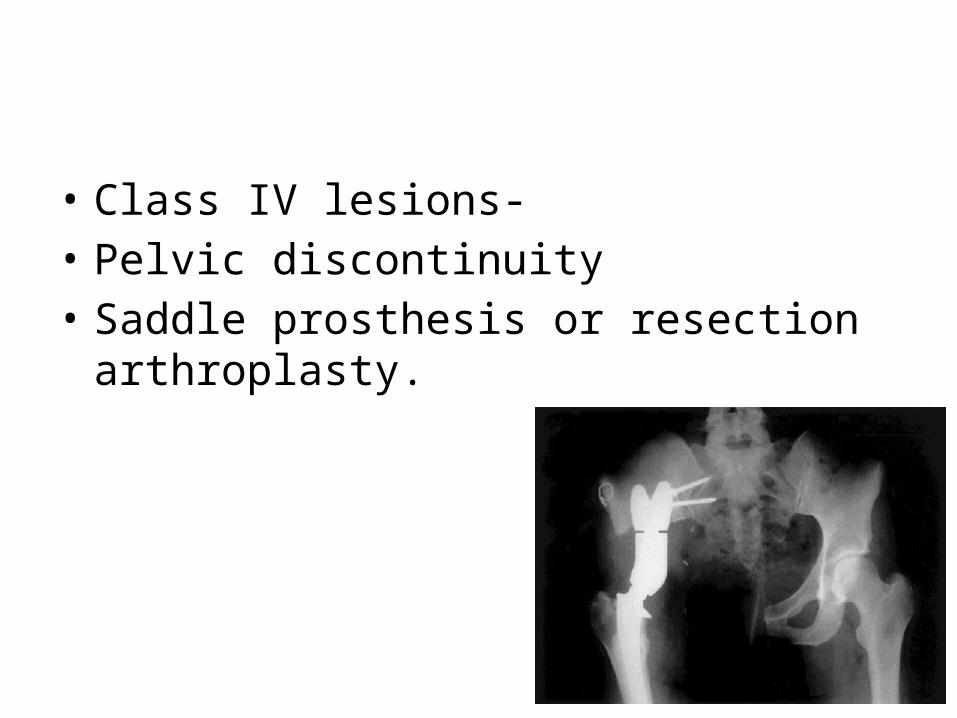
• Class IV lesions- • Pelvic discontinuity• Saddle prosthesis or resection arthroplasty.
Proximal femur
• Painful lytic lesions should be stabilised-– High risk of fracture– Ease of surgery
• Stabilize as much of proximal femur to avoid future implant failure- since lytic process is continous.
Femur neck
• Cemented prosthesis procedure of choice.• Curette all tumour tissue before putting the
implant.• Use a long stem component for adjacent
lesions- cement to be injected in a fairly liquid state after canal prepration.
Intertrochanteric region
• High failure rate of DHS.• Intramedullary device or prosthetic
replacement.• A cephalomedullary device has an added
function of protecting the femoral neck.• Cemented calcar replacing prosthesis used for
more extensive lesions.

Subtrochanteric region
• Statically locked nail +/- bone cement.• Failed internal fixation/ extensive destruction-
modular proximal femur device.• Increased risk of dislocation and abductor
weakness with megaprosthesis.• Bipolar head is used to provide additional
stability if acetabulum is not involved.• Largest diameter nail used for diaphysis.
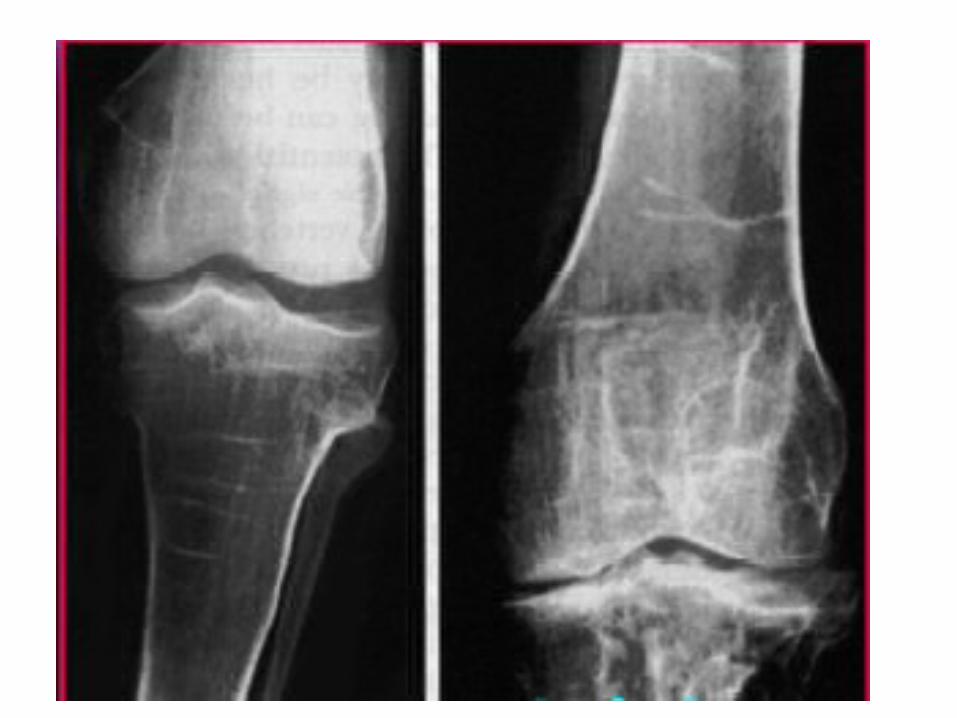
Distal femur
• Difficult to treat due to poor bone stock and communition.
• Lateral locking plate with cement or modular distal femur prosthesis.
• For extensive destruction modular prosthesis is the optimum choice as it allows resection en bloc.
• Retrograde nail- does not stabilize neck, seeding.
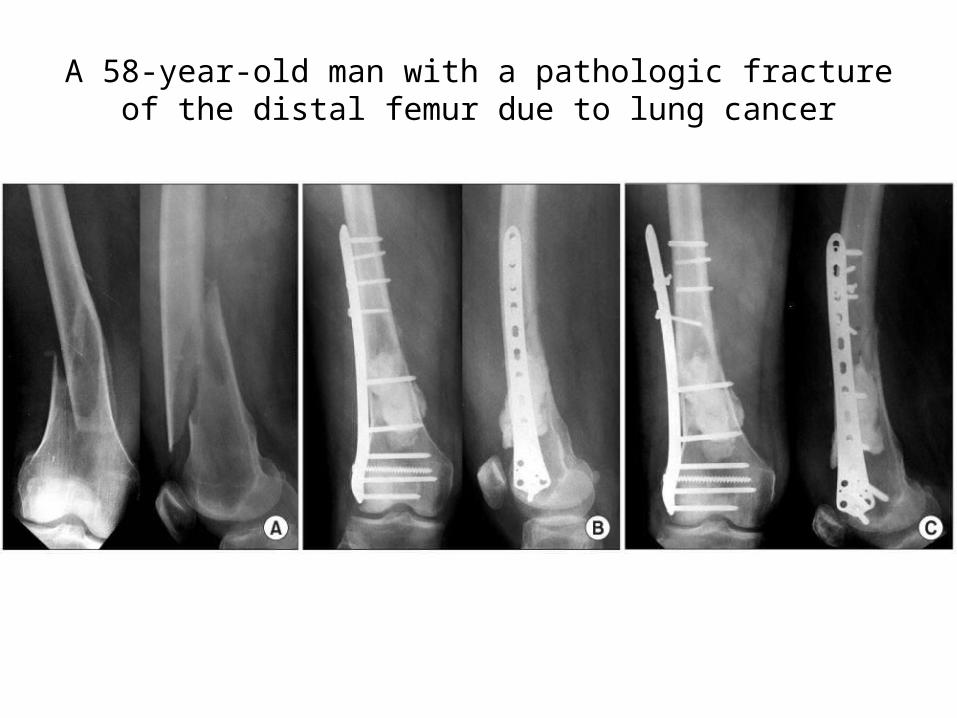
A 58-year-old man with a pathologic fracture of the distal femur due to lung cancer
Tibia
• Proximal tibia- locking plate with cement• Diaphysis- Intramedullary nail.
Spine
• Any cancer patient with back pain- consider mets.
• Any patient treated for osteoporotic compression fracture should undergo a biopsy when not responding to treatment or when there is excessive destruction of bone.
• CT guided biopsy.
• X ray- Loss of pedicle on the AP view.• MRI– Complete replacement of the vertebral segment– Multiple vertebral body lesions– Pedicle involvement– Intact intervertebral disk
• Bone marrow biopsy.
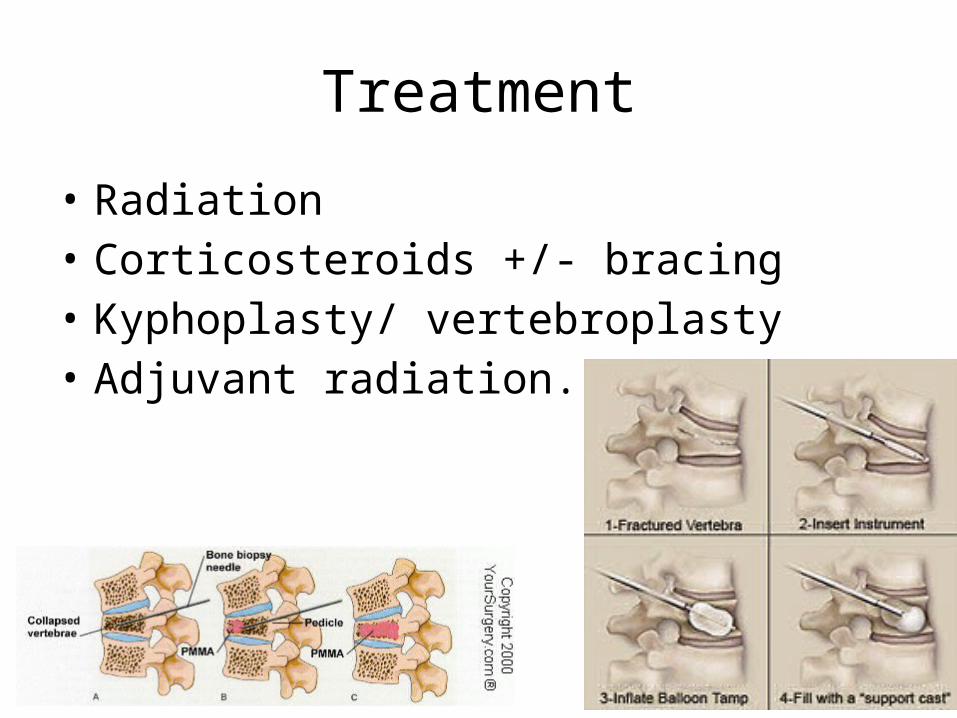
Treatment
• Radiation• Corticosteroids +/- bracing• Kyphoplasty/ vertebroplasty• Adjuvant radiation.
Indications of surgery
• Progression of disease after radiation• Neurologic compromise caused by bony
impingement• Radioresistant tumor within the spinal canal• Impending fracture• Spinal instability caused by a pathologic
fracture• Progressive deformity.