Paternal sex chromosome aneuploidy as a possible origin of ... · Sex chromosome aneuploidy as a...
4
Paternal sex chromosome aneuploidy as a possible origin of Turner syndrome in monozygotic twins O.Martinez-Pasarell 1 , C.Templado 1 , E.Vicens-Calvet 2 , J.Egozcue 3 and C.Nogues 3,4 1 Dept de Biologia Cel.lular i Fisiologia, Unitat de Biologia, Facultat de Medicina, Universitat Autonoma de Barcelona, 2 Servei de Pediatria, Hospital Universitari Materno-Infantil Vall d'Hebron, Barcelona and 3 Dept de Biologia Cellular i Fisiologia, Unitat de Biologia Cellular, Facultat de Ciencies, Universitat Autonoma de Barcelona, 08193 Bellaterra, Barcelona, Spain 4 To whom correspondence should be addressed The meiotic or mitotic origin of most cases of Turner syndrome remains unknown, due to the difficulty in detecting hidden mosaicisms and to the lack of meiotic segregation studies. We have had the opportunity to study one pair of monozygotic twins concordant for Turner syndrome of paternal origin. The paternal origin of the single X chromosome was determined by polymerase chain reaction (PCR) amplification. No mosaicism was detected for the X or Y chromosome. In this case, a meiotic error during gametogenesis would be a likely origin of X monosomy. To determine if meiotic errors are more frequent in the father of these monozygotic twins con¬ cordant for Turner syndrome of paternal origin, molecular studies in spermatozoa were conducted to analyse sex chromosome numerical abnormalities. A total of 12 520 sperm nuclei from the twins' father and 85 338 sperm nuclei from eight normal donors were analysed using three-colour fluorescent in-situ hybridization. There were significant differences between the twins' father and control donors for XY disomy (0.22 versus 0.11%, P< 0.001) and total sex chromosome disomy (0.38 versus 0.21%, P < 0.001). These results could indicate an increased tendency to meiotic sex chromosome non-disjunction in the father of the Turner twins. Key words: aneuploidy/spermatozoa/Turner syndrome/twins Introduction Turner syndrome is one of the most common sex chromosome abnormalities, affecting an estimated 1-2% of all clinically recognized pregnancies (Jacobs, 1992). Experimental evidence from restriction fragment length polymorphisms (RFLP) has demonstrated that 70-80% of 45,X cases are paternal in origin (Hassold et al., 1992; Lorda-Sanchez et al, 1992; Chu etal., 1994). The loss of a sex chromosome could occur as a result of non-disjunction or anaphase lag at either a meiotic division during gametogenesis, or an early cleavage division of a normal zygote. Some authors have suggested that most 45,X liveborns arise from a mitotic error in an early zygote and are actually cryptic mosaics for a normal cell line in some critical organ or tissue (Hook and Warburton, 1983; Held etal., 1992). However, the presence of X and Y cryptic mosaicism found in 45,X patients seems not to be so frequent (Lorda-Sanchez et al., 1992; Jacobs et al., 1997). So far, the meiotic or mitotic origin of most 45,X cases remains unknown due to the difficulty to detect hidden mosaicisms and to the lack of meiotic segregation studies. Monozygotic twinning in Turner syndrome is not frequent, although it has been reported previously (for review, see Machin, 1996). Usually, the twin pairs are discordant for Turner syndrome; in that case, the origin of the syndrome can be traced to a postzygotic malsegregation of chromosomes, resulting in sex chromosome mosaicism. On the other hand, the origin of monozygotic twins concordant for Turner syndrome is more likely to result from a meiotic error during gametogenesis. In this paper, we present a case of monozygotic twins concordant for Turner syndrome and paternal in origin (loss of the paternal sex chromosome). In order to study the possible meiotic or mitotic origin of the X monosomy in these monozygotic twins we have carried out a sex chromosome aneuploidy analysis in the spermatozoa from their father, to find out if there is an increase in the rate of sex chromosome disomy/nullisomy. The analysis of paternal gametes may help to elucidate the mechanisms involved in the origin of Turner syndrome. Case report Clinical report The twins, two 13-year-old girls, were born after 38 weeks of a normal pregnancy. They were monochorionic and diamniotic. At birth, the father was 35 years old and the mother 33 years old. The mother had had two previous pregnancies: a miscarriage at 3 months and a healthy girl. At 4.5 years of age, the twins were referred for clinical and laboratory analyses and follow-up. At that time, physical examination revealed that both twins had short stature, triangular face, low set ears, widely spaced nipples, micrognathia, short neck without pterygium, shield-like thorax, cubitus valgus and IQ (WISCH) of 98 and 72 respectively. No cardiovascular or renal abnormalities were detected. Standard cytogenetic studies of 50 metaphases from peripheral blood showed in each case only a 45,X cell population, CASE REPORT
Transcript of Paternal sex chromosome aneuploidy as a possible origin of ... · Sex chromosome aneuploidy as a...

Paternal sex chromosome aneuploidy as a possible origin of Turner syndrome in monozygotic twins
O.Martinez-Pasarell1, C.Templado1, E.Vicens-Calvet2, J.Egozcue 3 and C.Nogues 3 , 4
1Dept de Biologia Cel.lular i Fisiologia, Unitat de Biologia, Facultat de Medicina, Universitat Autonoma de Barcelona, 2Servei de Pediatria, Hospital Universitari Materno-Infantil Vall d'Hebron, Barcelona and 3 Dept de Biologia Cellular i Fisiologia, Unitat de Biologia Cellular, Facultat de Ciencies, Universitat Autonoma de Barcelona, 08193 Bellaterra, Barcelona, Spain 4To whom correspondence should be addressed
The meiotic or mitotic origin of most cases of Turner syndrome remains unknown, due to the difficulty in detecting hidden mosaicisms and to the lack of meiotic segregation studies. We have had the opportunity to study one pair of monozygotic twins concordant for Turner syndrome of paternal origin. The paternal origin of the single X chromosome was determined by polymerase chain reaction (PCR) amplification. No mosaicism was detected for the X or Y chromosome. In this case, a meiotic error during gametogenesis would be a likely origin of X monosomy. To determine if meiotic errors are more frequent in the father of these monozygotic twins con¬ cordant for Turner syndrome of paternal origin, molecular studies in spermatozoa were conducted to analyse sex chromosome numerical abnormalities. A total of 12 520 sperm nuclei from the twins' father and 85 338 sperm nuclei from eight normal donors were analysed using three-colour fluorescent in-situ hybridization. There were significant differences between the twins' father and control donors for XY disomy (0.22 versus 0.11%, P< 0.001) and total sex chromosome disomy (0.38 versus 0.21%, P < 0.001). These results could indicate an increased tendency to meiotic sex chromosome non-disjunction in the father of the Turner twins.
Key words: aneuploidy/spermatozoa/Turner syndrome/twins
Introduction
Turner syndrome is one of the most common sex chromosome abnormalities, affecting an estimated 1-2% of all clinically recognized pregnancies (Jacobs, 1992). Experimental evidence from restriction fragment length polymorphisms (RFLP) has demonstrated that 70-80% of 45,X cases are paternal in origin (Hassold et al., 1992; Lorda-Sanchez et al, 1992; Chu etal., 1994). The loss of a sex chromosome could occur as a result of non-disjunction or anaphase lag at either a meiotic division
during gametogenesis, or an early cleavage division of a normal zygote. Some authors have suggested that most 45,X liveborns arise from a mitotic error in an early zygote and are actually cryptic mosaics for a normal cell line in some critical organ or tissue (Hook and Warburton, 1983; Held etal., 1992). However, the presence of X and Y cryptic mosaicism found in 45,X patients seems not to be so frequent (Lorda-Sanchez et al., 1992; Jacobs et al., 1997). So far, the meiotic or mitotic origin of most 45,X cases remains unknown due to the difficulty to detect hidden mosaicisms and to the lack of meiotic segregation studies.
Monozygotic twinning in Turner syndrome is not frequent, although it has been reported previously (for review, see Machin, 1996). Usually, the twin pairs are discordant for Turner syndrome; in that case, the origin of the syndrome can be traced to a postzygotic malsegregation of chromosomes, resulting in sex chromosome mosaicism. On the other hand, the origin of monozygotic twins concordant for Turner syndrome is more likely to result from a meiotic error during gametogenesis.
In this paper, we present a case of monozygotic twins concordant for Turner syndrome and paternal in origin (loss of the paternal sex chromosome). In order to study the possible meiotic or mitotic origin of the X monosomy in these monozygotic twins we have carried out a sex chromosome aneuploidy analysis in the spermatozoa from their father, to find out if there is an increase in the rate of sex chromosome disomy/nullisomy. The analysis of paternal gametes may help to elucidate the mechanisms involved in the origin of Turner syndrome.
Case report
Clinical report The twins, two 13-year-old girls, were born after 38 weeks of a normal pregnancy. They were monochorionic and diamniotic. At birth, the father was 35 years old and the mother 33 years old. The mother had had two previous pregnancies: a miscarriage at 3 months and a healthy girl.
At 4.5 years of age, the twins were referred for clinical and laboratory analyses and follow-up. At that time, physical examination revealed that both twins had short stature, triangular face, low set ears, widely spaced nipples, micrognathia, short neck without pterygium, shield-like thorax, cubitus valgus and IQ (WISCH) of 98 and 72 respectively. No cardiovascular or renal abnormalities were detected. Standard cytogenetic studies of 50 metaphases from peripheral blood showed in each case only a 45,X cell population,
CASE REPORT

DXS 1 2 8 3 E
OYS 1! D M D 4 9 DXS 1283E AR p3mS2l 1 i 1 i 1 i 1 Hind III
A DNA/ DXS 52 Hind lfl+
i 1 EGO Fll
q?6 • DXS 52
a . X chromosome
pBR3£2/ SRY/DYS II DYZ3/1R5 DYZ1/[R5 Hind III i 1 i ! i
pi 1.3 SRY
ql l . l j ™ DY73
DYZ1
b . Y chromosome
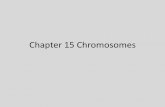
Figure 1. Location of the primers studied for X ( a ) a n d Y ( b ) chromosome and gel electrophoresis analysis of polymerase chain reaction (PCR) amplified products from the Turner twins (TS) and their parents (F: father, M: mother).
and homozygosity tests demonstrated that both twins were identical for the 15 blood markers analysed, making the probability of monozygosity >99.95%.
All blood and semen donors involved in this study gave their informed consent prior to the study, which was approved by our institutional ethics committee.
Molecular studies DNA extraction from peripheral blood of the Turner twins and their parents was carried out using a standard salt procedure (Miller et al., 1988). It was not possible to obtain permission to study fibroblasts or other somatic tissues. The parental origin of the single sex chromosome was determined by PCR amplification of five X chromosome microsatellites (Figure 1a): DMD49 (Clemens et al., 1991), DYS II (Feener etal., 1991), DXS1283E (Yen and Lin, 1994), AR (Mahtani and Willard, 1993) and DXS52 (Richards etal., 1991). DNA amplification was performed in a final reaction volume of 50 ml containing 1% of standard PCR buffer (Ecogen), 250 mmol/l of dNTPs (Perkin Elmer), 1.5 mmol/l MgCl 2 , 0.8 mmol/l of each primer (Research Genetics Inc.), 0.5 IU Taq polymerase (Ecogen) and 0.4-1 mg of DNA. Samples were processed in a Perkin Elmer thermal cycler from 24 to 30 cycles. Specific PCR conditions for each primer are described in Table I. Samples were run on a 6% acrylamide:bisacrylamide (19:1) gel at 12 mA for 13-16 h; the gel
Table I. Characteristics of X and Y chromosome primers and conditions of PCR amplification
Primer No. of Size (bp) Heterozygosity Annealing alleles temperature (°C)
X chromosome DMD49 19 227-257 93.3 62 DYS II 8 214-228 82.0 55 DXS1283E 12 145-167 88.0 58 AR 11 195-225 90.2 58 DXS52 14 700-3000 80.4 55
Y chromosome SRY 360 55 DYZ3 170 55 DYZ1 236 60 Chromosome 19 IR5 276 55/60
was then stained with ethidium bromide. DXS52 polymorphism was characterized on a 1% agarose gel owing to its size (700-3000 pb). Electrophoresis was carried out at 100 V for 1 h.
Three Y chromosome-specific segments (Kocova et al., 1995) were amplified by PCR to detect possible Y hidden mosaicism (Figure 1b). Internal controls were simultaneously amplified with SRY (DYS
2736

Sex chromosome aneuploidy as a possible origin of Turner monozygotic twins
Table II. Frequency of sex chromosome numerical abnormalities observed in spermatozoa of control donors and in the twin's father
Donors (age) No. of spermatozoa XX (%) YY (%) XY (%) Total disomy (%) Nullisomy (%) Diploidy (%)
Control donors C1 (22) 11 058 0.07 0.10 0.09 0.26 0.43 0.28 C2 (22) 10 347 0.03 0.04 0.10 0.17 0.16 a 0.37 b
C3 (31) 10 152 0.05 0.07 0.13 0.25 0.25 0.20 C4 (33) 11 620 0.04 0.04 0.10 0.18 0.23 0.16 C5 (45) 10 390 0.04 0.06 0.11 0.21 0.40 0.24 C6 (49) 10 786 0.05 0.06 0.08 0.19 0.38 0 . 4 1 b
C7 (49) 10 945 0.03 0.05 0.06 0.14 0.37 0.15 C8 (55) 10 040 0.04 0.07 0.18 0.29 0.34 0.19 Mean ± SD 85 338 0.04 ± 0.01 0.06 ± 0.02 0.11 ± 0.04 0.21 ± 0.05 0.32 ± 0.09 0.25 ± 0.10 Twin's father 12 520 0.06 0.10 0.22 c 0.38 d 0 .51 e 0.24
a C2 nullisomy frequency is significantly different from C1, C5, C6 and C7; P < 0.01. b C 2 and C6 diploidy frequencies are significantly different from C4, C7 and C8; P < 0.01. c - eSignificantly higher than control donor mean: c , d P < 0.0015; e P < 0.01.
II located in Xp), DYZ1 and DYZ3 (IR5 located in chromosome 19) (Seino et al., 1990).
Three-colour FISH in spermatozoa Semen samples were obtained from eight healthy control men (from 22 to 55 years of age) and the Turner twins' father (48 years old). Six control donors were of proven fertility. The semen samples were processed for three-colour fluorescent in-situ hybridization (FISH) analysis of spermatozoa as previously described (Vidal et al., 1993).
We applied three-colour FISH with DNA centromeric probes for chromosomes X (Spectrum green, Vysis Inc.), Y (Spectrum orange, Vysis Inc.) and 6 (1:1 mix of Spectrum green and Spectrum orange, Vysis Inc.). FISH incubation and detection were performed according to manufacturer's instructions. Chromosome 6 provided an internal control to characterize diploid and disomic cells, as well as non-hybridized cells.
Slides were analysed under an Olympus AX70 epifluorescence microscope equipped with a FITC/Texas Red/DAPI triple-band pass filter and single-band pass filter for DAPI, Texas Red and FITC.
Scoring criteria Sperm nuclei were scored only ifthey were intact and non-overlapped. Two spots of the same colour were scored as two copies of the corresponding chromosome when they were comparable in brightness and size and were separated from each other by a distance longer than the diameter ofeach signal. All ambiguous signals were examined by at least one additional independent observer.
Statistical analysis To determine if there were any significant differences in disomy and diploidy frequencies among the donors, we used a two-tailed Fisher's exact test. The Bonferroni procedure was applied to adjust for multiple comparisons. A Spearman correlation test was employed to study the relationship between the control donor's age and the aneuploidy frequencies.
Results
All five markers for the X chromosome were informative and showed that the twins only inherited one allele from their mother. No Y amplification was detected (Figure 1). X chromo¬ some and chromosome 19 fragments were simultaneously amplified with Y chromosome specific fragments as internal controls to avoid false-negative results.
We analysed 85 338 sperm nuclei from control donors
(~10 000 per donor), and 12 520 from the father of the Turner monozygotic twins by three-colour FISH. Hybridization and decondensation efficiency were in each case higher than 98%. Disomy, diploidy and nullisomy rates obtained in sperm nuclei for control donors and the twins' father are shown in Table II. Interdonor heterogeneity was found for control donors in diploidy and nullisomy frequencies. However, there was no correlation between donor ages and disomy rates.
There were significant differences between the twins' father and control donors for XY disomy (0.22 versus 0.11%; P < 0.001), and total sex chromosome disomy (0.38 versus 0.21%; P < 0.001) and sex chromosome nullisomy (0.51 versus 0.32%; P < 0.01).
Discussion The twins reported in this study were monochorionic, diamniotic and monozygotic (with a probability >99.95%) and both displayed the full Turner phenotype. We have established, by PCR amplification, five X chromosome poly¬ morphisms, indicating that the origin of the syndrome for these twins was paternal (loss of the paternal sex chromosome).
These observations suggest that the error leading to X-monosomy occurred before the twinning event, either during early embryo cleavage or paternal spermatogenesis. A mitotic error in an early embryo would produce two mosaic embryos (probably 45,X/46,XX), although the production of two non-mosaic 45,X embryos, in which the normal cell line would only contribute to extra-embryonic tissues, could not be rejected. On the other hand, a meiotic error during paternal spermatogenesis would lead to two non-mosaic 45,X embryos both concordant for Turner syndrome. The possibility of sex chromosome mosaicism has been ruled out in peripheral blood for these twins. Unfortunately, it has not been possible to analyse the placenta or the fibroblasts and we cannot absolutely exclude mosaicism.
The study carried out in the spermatozoa of their father and eight control donors has shown several differences in the sex chromosome aneuploidy rates. The frequencies of XY (0.22%) and total sex chromosome disomy (0.37%) from the twins' father were significantly increased compared with those obtained in our control donors. These data suggest an increase
2737

of meiotic errors in the segregation of sex chromosomes. The observed excess of XY spermatozoa has to be the result of non-disjunction during meiosis I, that would produce an excess of XY and nullisomic versus normal spermatozoa for sex chromosomes.
Thus, it seems that in these monozygotic twins, Turner syndrome would have originated through a meiotic error during paternal spermatogenesis. At any rate, this sex chromosome aneuploidy increase in the twins' father compared to control donors is moderate and we cannot exclude that it also could be attributed to individual variations in sperm aneuploidy described by several authors (reviewed by Downie etal., 1997; Egozcue et al., 1997). However, recently, a moderate increase for chromosome 21 disomy has also been found in the spermatozoa of fathers of Down's syndrome children (Blanco et al., 1998). Further studies of larger series of Turner syndrome patients will be needed to elucidate the origin of non-mosaic Turner syndrome.
Acknowledgements We gratefully acknowledge Dr D. Gallardo (Banc de Sang, Hospital de la Vall d'Hebron de Barcelona) for performing the homozygosity test. This work received financial support from Direccion General de Enserianza Superior, Ministerio de Educacion y Cultura (DGICYT, project no. PB95-0655) and the Generalitat de Catalunya (CIRIT, 1997 SGR 00030).
Lorda-Sanchez, I., Binkert, F., Maechler, M. et al. (1992) Molecular study of 45,X conceptuses: correlation with clinical findings. Am. J. Med. Genet., 42, 487-490.
Machin, G.A. (1996) Some causes of genotypic and phenotypic discordance in monozygotic twin pairs. Am. J. Med. Genet., 61, 216-228.
Mahtani, M.M. and Willard, H.J. (1993) A polymorphic X-linked tetranucleotide repeat locus displaying a high rate of new mutation: implications for mechanisms of mutation at short tandem repeat loci. Hum. Mol. Genet., 2, 431-437.
Miller, S.A., Dykes, D.D. and Polesky, H.F. (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res., 16, 1215.
Richards, B., Heiling, R., Oberle,I . et al. (1991) Rapid PCR analysis of the St14 (DXS52) VNTR. Nucleic Acids Res., 19, 1994.
Seino, S., Seino, M. and Bell, G.I. (1990) Human insulin receptor gene. Partial sequence and amplification of exons by polymerase chain reaction. Diabetes, 39, 123-128.
Vidal, F., Moragas, M., Catala, V. et al. (1993) Sephadex filtration and human serum albumin gradients do not select spermatozoa by sex chromosome: a fluorescent in-situ hybridization study. Hum. Reprod., 8, 1740-1743.
Yen, P. and Lin, H. (1994) Dinucleotide repeat polymorphism at the DXS1283E locus. Hum. Mol. Genet., 3, 388.
Received on April 12, 1999; accepted on August 17, 1999
References Blanco, J., Gabau, E., Gomez, D. et al. (1998) Chromosome 21 disomy in
the spermatozoa of the fathers of children with trisomy 21 in a population with a high prevalence of Down's syndrome. Increased incidence in cases of paternal origin. Am. J. Hum. Genet., 63, 1067-1072.
Chu, C.E., Donaldson, M.C.D., Kelnar, C.J.H. et al. (1994) Possible role of imprinting in the Turner phenotype. J. Med. Genet., 31, 840-842.
Clemens, P.R., Fenwick, R.G., Chamberlain, J.S. etal. (1991) Carrier detection and prenatal diagnosis in Duchenne and Becker muscular dystrophy families, using dinucleotide repeat polymorphisms. Am. J. Hum. Genet., 49, 951-960.
Downie, S.D., Flaherty, S.P. and Matthews, C.D. (1997) Detection of chromosomes and estimation of aneuploidy in human spermatozoa using fluorescence in-situ hybridization. Mol. Hum. Reprod., 3, 585-598.
Egozcue, J., Blanco, J. and Vidal, F. (1997) Chromosome studies in human sperm nuclei using fluorescence in-situ hybridization (FISH). Hum. Reprod., Update, 3, 441-452.
Feener, C.A., Boyce, F.M. and Kunkel, L.M. (1991) Rapid detection of CA polymorphisms in cloned DNA: application to the 5 'region of the dystrophin gene. Am. J. Hum. Genet., 48, 621-627.
Hassold, T., Pettay, D., Robinson, A. et al. (1992) Molecular studies of parental origin and mosaicism in 45,X conceptuses. Hum. Genet., 89, 647-652.
Held, K.R., Kerber, S., Kaminsky, E. et al. (1992) Mosaicism in Turner syndrome: does survival in early pregnancy depend on the presence of two sex chromosomes? Hum. Genet., 88, 288-294.
Hook, E.B. and Warburton, D. (1983) The distribution of chromosomal genotypes associated with Turner' s syndrome: livebirth prevalence rates and evidence for diminished fetal mortality and severity in genotypes associated with structural Y abnormalities or mosaicism. Hum. Genet., 64, 24-27.
Jacobs, P.A. (1992) The chromosome complement of human gametes. In Milligan SR (ed.), Oxford Reviews of Reproductive Biology, vol. 14. Oxford University Press, New York, pp 47-72.
Jacobs, P. A., Dalton, P., James, R. etal. (1997) Turner syndrome: a cytogenetic and molecular study. Ann. Hum. Genet., 61, 471-483.
Kocova, M., Siegel, S.F., Wenger, S.L. etal. (1995) Detection of Y chromosome sequences in a 45,X/46XXq- patient by southern blot analysis of PCR amplified DNA and fluorescent in situ hybridization (FISH). Am. J. Med. Genet., 55, 483-488.
2738