Passy-Muir Fall 2015 Newsletter- Team Issue #2
12
\ |,i Vanderbilt University Medical Center ' Q. H \\ F. 1| D Johns Hopkins Hospital . - t--;§_| -pl: .._.. ‘~. -._.= I J 3‘ » J1 _____' - - §_ -— ‘F '2?‘ F.,.:'- 3 i-in it ii 1.. “R ‘E 6 ‘!'.'-\- 5 Passy-i\/luir, inc. I Fall2015 1 “IQ ’ A 9% I<;‘,,. ‘. J ;’ 4» '",4-,-_-. ifs .3, ‘fig '::‘r;.. $~'=_“*:1¢~$""’ '‘ ".":» ;t!1§.»' ‘r$1¢- “£11. __ 53 3}: gfi _\r':£| 2* ‘In ‘ 'I| ‘ \ I _...— ' TEAM ISSUE #2 Starting a Trach Team Ventilator Play Group Benefits of Rounds Toby Program Gets Updated Millions of Voices, ONE \/AL\/E“ @q,44#@i@17b®
-
Upload
passy-muir-inc -
Category
Documents
-
view
217 -
download
1
description
Â
Transcript of Passy-Muir Fall 2015 Newsletter- Team Issue #2

\|,i
Vanderbilt UniversityMedical Center
' Q.H
\\
F. 1|D
Johns HopkinsHospital
. - t--;§_|-pl: .._..
‘~. -._.= I
J
3‘»
J1_____' - - §_ -—
‘F
'2?‘
F.,.:'- 3 i-in
it ii
1..
“R
‘E
6‘!'.'-\-
5
Passy-i\/luir, inc. I Fall2015
1
“IQ’ A9%I<;‘,,.‘.
J;’4»
'",4-,-_-.ifs.3, ‘fig'::‘r;..$~'=_“*:1¢~$""’'‘".":»;t!1§.»'
‘r$1¢-“£11.__ 533}:gfi
_\r':£|
2*
‘In
‘ 'I|‘ \I
_...— '
TEAMISSUE #2
Starting a Trach Team
Ventilator Play Group
Benefits of Rounds
Toby Program Gets Updated
Millions of Voices, ONE \/AL\/E“ @q,44#@i@17b®

Clinical Expert Interview: Starting a Tracheostomy Team
Carmin Bartow, MS, CCC-SLP, BCS-SVanderbilt University Medical CenterCarmin is a licensed and certified speech-language pathologist who is Board Certified inSwallowing and Swallowing Disorders. She is currently employed at Vanderbilt UniversityMedical Center specializing in dysphagia management, trach/vent intervention, and inswallowing disorders in the head and neck cancer population. In addition to her clinicalresponsibilities, she facilitates a head and neck cancer support group and enjoys presentingand teaching at Vanderbilt as well as at state and national conferences. Carmin has authoredan ASHA publication titled “Tracheostomy Tubes in Adults; Management of Communicationand Swallowing impairments.” She teaches Dysphagia as an adjunct professor at TennesseeState University and is an Educational Consultant for Passy-lvluir, Inc.
1. What made you decide that a team approachfor the management ofpatients with tracheostomy (I ,was necessary at Vanderbilt University Medical Results revealed that names needed moreCenter (VUMC)?The short answer: I saw inconsistencies with trachmanagement throughout the hospital and I knew wecould do better. Our speech pathology staff evaluatesand treats tracheostomized patients in all areas of our800 bed hospital including the Emergency Department,step-down units and in eight different lCUs. We werecontinually noticing differing tracheostomy practicepatterns across VUI\/IC depending on the area, unit,or service in which the patient was placed. Nursingknowledge and skills in managing patients with trachtubes varied. In addition, there was a lack of standard-ization forsizing ofthetrach tube, trach care, cuff deflation,use of the Passy-Muir® Valves, referrals for swallowingassessments, downsizing, and decannulation. With theseinconsistencies, it became apparent that tracheostomymanagement needed improvement.I knew that tracheostomy teams existed in manyinstitutions to better manage patients with trach tubes.I began to wonder whether a trach team would befeasible at VUMC. Initially, I had concerns that a trachteam wouldn’t work in a hospital the size of Vanderbilt —too many trachs (approx 600 per year), too many ICUs,too many staff members to train and too many differentservices to include. I was also concerned I wouldencounter resistance and thought that someone otherthan a speech-language pathologist would need to takethe initiative and lead in this endeavor. For quite sometime, I waited for an MD to have the big “ah-ha” momentand magically fix the problem. But as you can imagine, thatdidn’t happen and as time passed, the problems continued.
education and mentoring withtracheostomy management. ”
I kept the trach team idea in the back of my mind andeventually decided to survey staff about trach issues.In particular, I wanted to determine nursing comfortand skill level in managing patients with tracheostomytubes. Results revealed that nurses needed moreeducation and mentoring with tracheostomy management.These results along with the inconsistencies observedby the SLPs were the impetus to begin researchingtracheostomy teams. I read numerous articles anddiscovered the many benefits of establishing trach teams:increased use of the Passy-Muir Valve, reduced length ofstay, quicker decannulation and cost savings. I watchedthe Passy-I\/luir webinar about tracheostomy teams andlearned important steps and components of trach teamdevelopment. In addition, I called hospitals that hadsuccessful trach teams in place and took copious notesabout what worked and what didn’t. The informationI gathered led me to believe that a trach team couldcertainly benefit both patients and staff and had potentialto be a reality at VUMC.
PMV® 2001(Purple Colorw)

E 2. What steps did you take toVANDERMLT develop your team?u ~ IV E R s | TYMEDICALCENTER
One of the first steps I took was togain allies. I needed support andsomeoneto championthisendeavor.I started discussions with a Head
and Neck Surgeon who was immediately interestedand agreeable to continued meetings and discussionsabout a trach team initiative. We began monthly meetingsand gradually invited other staff to get involved. Forapproximately two years a group consisting of anOtolaryngologist, Speech Language Pathologist, CaseManager, and Director of Peri-Operative Services metto develop our version of a tracheostomy team. Wedeveloped documents, procedures, team goals, tasks,financial goals and plans, etc. These documents andplans were ultimately presented to administration inanticipation of implementing the VUMC trach team.
The Vanderbilt University Medical Center Trach Consult Service.From L to R: Nina Collins, MSN, RN, ACNP-BC; Oscar Guillamondegui, MD(Trauma); Alexander Gelbard, MD (Otolaryngology): and Carmin Bartow,CCC-SLP, M.S. BCS-S. Not pictured: Clint Leonard, MSN, RN
" ‘ll
Q.
-1
A Passy-Muir Valve and swallowing assessment is automatically orderedfor all new trach patients at Vanderbilt University Medical Center
3. Did you meet any obstacles?Yes! Our first attempt at the creation of a tracheostomyteam was unsuccessful for many reasons. Administrationwas interested, but the budget didn’t allow for any newhires at the time. There was some resistance from otherservices who performed tracheotomies since they werenot involved in the planning meetings. Lastly, our mainadvocate accepted a chair position at another institution.Unfortunately, with budget limitations, resistance fromother services, and no champion to advocate for us,interest dwindled and the initial trach team initiative waslaid to rest.
It was certainly disappointing but I knew that we hadgiven it a valiant effort and thought it was time to moveon. But... those pesky little trach problems persisted!Every time I encountered a size 8 trach that had not beendownsized in a timely manner, a cuff that had not beendeflated, or a patient that should have had a Passy-Muirassessment much earlier, I felt the need to get backon the horse and try again. So after a few months offrustration, I started over. This time, I sought to includeadditional professionals from other services. I found anew champion who was a Trauma MD and we graduallystarted a new version of the VUMC Trach Team. TAKE2! We included a Registered Nurse (RN) who wasextremely knowledgeable in tracheostomy tubes, aNurse Practitioner (NP) who had experience in trachmanagement and education, and an Otolaryngologistwith a special interest in management of complex airways.We also had consultants from Patient Education,Respiratory Therapy and Case Management. This newteam proved to be the multi-disciplinary group to makethings happen!
?
Clinical Expert Interview (continued)
4. After you rallied the troops a second time,describe specific actions your team has taken toimprove patient care.
I am happy to say that the VUMC Trach Consult Serviceexists! It was a long road, nearly 3 years in the making,but well worth the time and effort. l’d like to share some ofthe improvements in practice patterns and proceduresas a result of the implementation of the Trach ConsultService:
~ Tracheotomies are performed within 24 hours of request
~ Designated NP for the Trach Consult Service whorounds on patients daily. Patients are seen routinelyon post-op day two and five and throughout theirhospitalization as needed
' Standardized care throughout VUMC for trach sizing,cuff deflation, downsizing, and decannulation
~ Development of an outpatient Trach Clinic. If a patientis discharged with a trach, he/she is automaticallyscheduled in the Trach Clinic for follow up
~ Creation and implementation of new VUMC trache-ostomy protocols, policies, order set and patienteducation hand-outs
~ Passy-Muir® Valves and swallowing assessments arepart of the order set for all new trachs, so patients aretalking and eating much sooner
v On-going staff education
VUMC has a credo which states “We provide excellencein healthcare, research and education. We treat othersas we wish to be treated. We continuously evaluate andimprove our performance.” I believe that with implemen-tation of the Trach Consult Service we are adhering to ourcredo and meeting our goal of excellence in patient care.
PMV® O07(Aqua Colorw)
Speech-language pathologist Carmin Bartow places a PMV® 2001on a patient at VUMC
5. Would you say there is one key element tomaking your team successful?
Yes, a major focus for us has been education. To ensurethe success of the VUMC Trach Consult Service, weneeded to enhance staff knowledge and skills regardingthe management of tracheostomy tubes. Tracheostomyeducation is now an integral part of what we do.
We have created an education document entitled“Nursing Management of Tracheostomy.” This step-by-step document outlining the nursing role in managing apatient with a tracheostomy tube has been distributedto all nurses in all units. We have created a webinar whichcan be assigned for nursing annual competencies.We are on the monthly agenda to provide tracheostomyeducation during new nurse orientation and ICUorientation. We provide educational booths and lecturesat unit board meetings and safety fairs.
Included in all of ourtracheostomy education presentationsand documents is information about the Passy-MuirValve. Details about use, need for complete cuff deflation,care, cleaning, placement, removal, and troubleshootingare included. It is our goal that this education be on-goingacross the institution.

/\ 1,
/
‘L‘”\?
Since the implementation of the Trach Consult Service,the management, standardization and care of thepatient with a tracheostomy tube has greatly improved.I believe this has enhanced patient quality of life as well,due to better trach care, quicker referrals for Passy-Muir®Valves and swallowing assessments, and more timelydecannulation. My message to clinicians who feel thata trach team may benefit their patients is to findcolleagues and a champion with similar goals in mindand don’t give up!
Carmin Bartow, MS, CCC-SLP presents a tracheostomy lecture which is acomponent of the Critical Care Track during the Nurse Residency Programfor new nurses
|,_.__
~_m0"‘ ,-»
Educational materials utilized for tracheostomy education during the SafetyFair at Vanderbilt University Medical Center
.-l;-
Upcoming EventsAmerican College of Chest Physicians
CHEST Conference 2015 zoomOctober 25 — 28, 2015, Montreal, Canada
American Association for Respiratory Care
November 7 - 10, 2015, Tampa, Florida 5°‘-'"'"AARC 61st International Congress
American Speech-Language-Hearingmo,” Association _704 ASHA 2015 Convention
November 12 - 14, 2015, Denver, Colorado
Vibra Hospital of RichmondTraining Session
November 12, 2015, Richmond, Virginia
East Tennessee State UniversityDepartment of Communicative Disorders
ConferenceNovember 20 — 21, 2015, Johnson City, Tennessee
South Carolina Speech Language HearingAssociation Annual Convention
February 25 - 26, 2016, Columbia, South Carolina
Anne Arundel Medical Center ConferenceApril 21, 2016, Annapolis, Maryland

w
The Cutest Hour at LeBonheur
F’,
By Julie A. Kobak, MA, CCC-SLP, Vice President of Clinical Education, Passy-Muir, Inc.
Toby Tracheasaurus“is a favorite therapy tool ofpediatric therapists. We oftenhear stories about how childrenare introduced to the Passy-MuirValve through interactive play withToby, the toy dinosaur who hashis own tracheostomy and valve.Recently we learned that Toby isquite popular in a group therapysession for children with trache-ostomies and on ventilators.
The team at LeBonheur Children’s Hospitalpulled out all the stops to make this special playgroup happen. I recently spoke to Amy Claire Petro,the speech-language pathologist who initiated thisprogram with child life specialist Molly Pearce, twonurses, Hillary Arnold and Virginia Burbank, and aphysician, Dr. Stephanie Storgion. Amy Claire startedher story by telling me why the team at her hospital feltthis group was needed. The majority of the children whohave tracheostomies and are mechanically ventilatedhave spent the first year or more of their lives in thehospital, often confined to just one single hospital room.When these children are discharged home, they quicklyexperience “sensory overload” from the stimulation ofnew environments. Amy Claire said, “Some childrenhave been so overwhelmed by new sounds and sightswhen leaving the hospital that they don’t even make itpast the car ride home and have to turn around.” Sheknew that they had to find a way to get these patientsout of their rooms to experience new environments andto socialize with other children prior to discharge into thebigger world.
“Some children have heen sooverwhelmed by new sounds and sights
when leaving the hospital that theydon’t even malee itpast the car ride
home and have to tarn around.”
L
Clinicians at LeBonheur Children's Hospital facilitate a play group forchildren on ventilators. Standing (L to R): Tandra Robinson, RN, MollyPearce, CCLS. Stephanie Storgion. MD; Seated (L to R): Laurie Braswell,OTR/L, Mary Holland Morris, CCLS. patient Jaylen, Amy Claire Petro MS,CCC-SLP, Sheri Sills, RT.
But getting three or more children with trachs and ventsin the same room at the same time is no easy matter.According to Amy Claire, it took a couple of years towork out all of the logistics. The first challenge was toidentify a physical space in the hospital large enoughto work with up to five ventilator children and theircaregivers and equipment, and to install the appropriatenumber of oxygen and suction outlets. The secondchallenge was to coordinate the staff so that there wasa therapist for every child in the group who would beresponsible for attending to suctioning and all otherrespiratory needs. Multiple disciplines share thisresponsibility, including nurses, respiratory therapists,occupational therapists, speech pathologists, physicaltherapists and child life specialists. One nurse comesin on her day off as a volunteer to assist with ventilatormanagement.

'-SI-
May Swain (patient) is held by Molly Pearce CCLS as she makes musicwith Kahlilah Brooks, MT-BC Board Certified Music Therapist.
A young patient, Cody Lewis, plays with occupational therapist,Laurie Braswell OTR/ L.
Mya Swain and Cody Lewis meet tor the first time as they play with TobyTracheasaurus“. Cody uses the PMV® 2000, clear speaking valve, in-linewith his ventilator.
\@.. .r_
, laExample of books and art suppliesused during story time and play activities.
The play group now meets every week on Thursdayafternoon. During fun activities, the therapists co-treatand address specific therapy tasks while the childrenexperience social time with their peers. For example,while the children are painting, the physical therapistworks on positioning and the occupational therapistaddresses sensory and fine motor goals. During story-time, the speech pathologist focuses on Passy-Muir®Valve wear-time, vocalizations and attention to tasks.Amy Claire said it is a great opportunity for the childrento tackle social skills that are often difficult for them,such as turn-taking and learning to accept “no.”
The children are not the only ones who benefit fromthe group. All of the staff receive great joy watching thechildren play and interact. According to Amy Claire,“Doctors will just stop by because they are having arough day and need a happy moment.” The parentsand caregivers are very pleased with the group. Forone family with two young children diagnosed withmyotubular myopathy, this therapy group was the firsttime the two brothers were able to meet!
The play group has been so successful that plans arein the works to add another “outing” for the children onWednesdays called “ChiIdren’s Chapel.” Many of thefamilies look forward to taking their children to churchservices when they go home, so an activity like thiscan prepare them for what most of us take for granted.We look forward to hearing more about the children’sadventures at LeBonheur!
LefiheurChildrerfs Hospital
nu"-I1 I'1" |l. P..
. ll 'I \'_
v "'__—.g,_
_ \’_ -1‘ -.
I '1-b I _0 I
II‘ . "1' r
<1‘V
.ér,“(‘*=s»_l.‘T‘B1F-4‘.':.;'
A‘if:-s.<,. 1
Multidisciplinary Tracheostomy Program RoundsBy Vinciya Pandian, PhD, ACNP; Therese Cole, MA, CCC-SLP; Kathryn Mattare, BS, RRT; Amanda Owen, RN, BSN, CWCN;Carol Maragos, MSN, CRNP Johns Hopkins Hospital
BackgroundThe Johns Hopkins Multidisciplinary TracheostomyProgram was established in 2006 to improve patient careby promoting safety, decreasing complication rates, anddecreasing intensive care unit and hospital lengths ofstay.‘ The Johns Hopkins Multidisciplinary TracheostomyTeam (JH-MDTT), is composed of credentialed operators(otolaryngology head and neck surgeons, traumasurgeons, and interventional pulmonologists), anesthesi-ologists, registered nurses, respiratory therapists,and speech-language pathologists. The program hasbeen functioning successfully under the direction of atracheostomy nurse practitioner and a medical director.A review of data between 2004 and 2008 revealed thatthe program was successful in decreasing airwaybleeding rates, decreasing physiological disturbancessuch as hypoxia and loss of airway during the placementof a tracheostomy tube, and improving efficiency of careas measured by the number of days to tracheostomy.1»2
Doctor Arora and colleagues from the United Kingdomfound that weekly tracheostomy multidisciplinary teamward rounds helped to improve compliance with nursingcare standards and decreased duration of cannulationfiSimilarly, biweekly multidisciplinary team rounds bythe Tracheostomy Review and Management Service(TRAMS) in Melbourne, Australia, resulted in a decreasein length of stay and duration of cannulation, andimprovement in communication.4
Despite the evidence, it was only recently that theJH-MDTT realized the effectiveness of multidisciplinarytracheostomy rounds. After discussions with DoctorArora and observations of TRAMS in action duringthe Global Tracheostomy Collaborative initiative kickoffmeeting in the United Kingdom and Australia in 2014, itsvalue was appreciated. As a result, the Johns HopkinsMultidisciplinary Tracheostomy Program implementedweekly multidisciplinarytracheostomy rounds in Februaryof 2015.
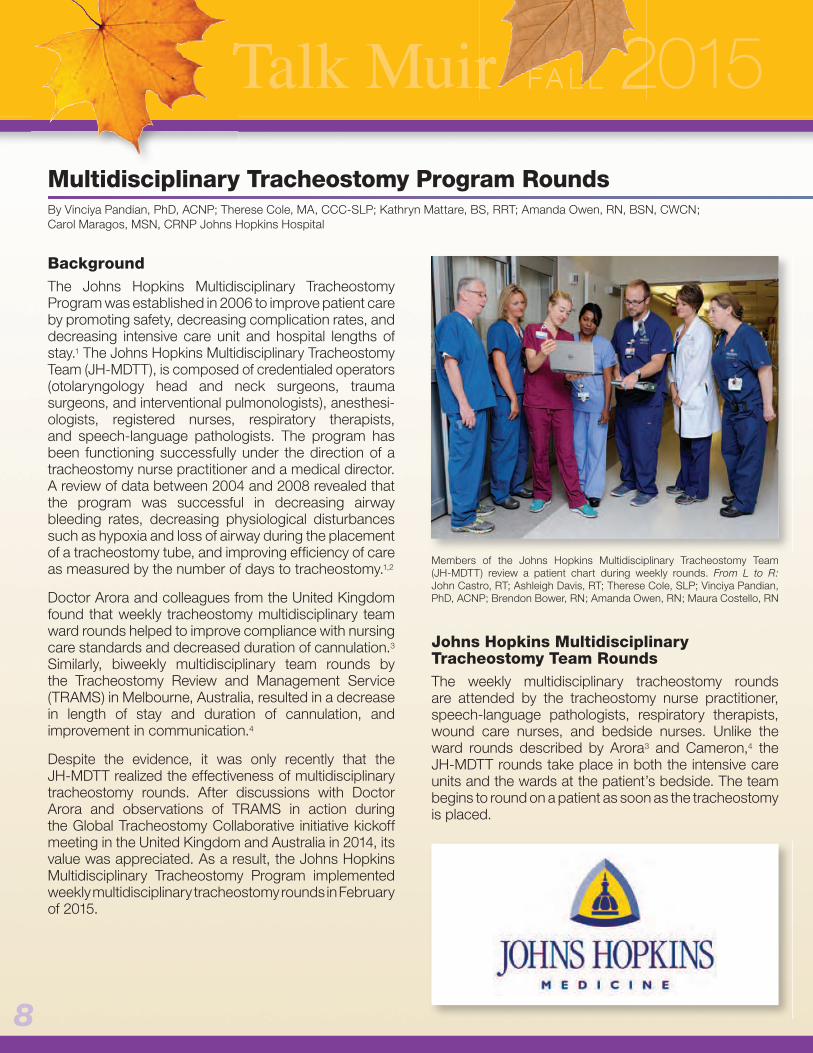
Members of the Johns Hopkins Multidisciplinary Tracheostomy Team(JH-MDTT) review a patient chart during weekly rounds. From L to R:John Castro, RT; Ashleigh Davis, RT; Therese Cole, SLP; Vinciya Pandian,PhD, ACNP; Brendon Bower, RN; Amanda Owen, RN; Maura Costello, RN
Johns Hopkins MultidisciplinaryTracheostomy Team RoundsThe weekly multidisciplinary tracheostomy roundsare attended by the tracheostomy nurse practitioner,speech-language pathologists, respiratory therapists,wound care nurses, and bedside nurses. Unlike theward rounds described by Arorag and Cameron,4 theJH-MDTT rounds take place in both the intensive careunits and the wards at the patient’s bedside. The teambegins to round on a patient as soon as the tracheostomyis placed.
JOHNS HOPKINS

A list of all patients with a tracheostomy is generated bythe electronic medical record system on the morningof the rounds. It provides information on where thepatients are located within the massive 1000-bedhospital, along with the names and contact informationof the nurses who are caring for those patients. This listserves as a guide for the team to plan their rounds in anefficient manner. The JH-MDTT rounds on approximately25 to 45 patients per week every Friday between 10:00am and noon. Occasionally, the rounds may extend pastnoon, depending on the number of patients to be seen.The tracheostomy nurse practitioner and the respiratorycoordinator round on every patient, but the dedicatedspeech-language pathologist, respiratory therapist,wound care nurse, and bedside nurse join in only whentheir patients are discussed.
Rounding GoalsThe rounding discussion focuses on stoma wound care,communication, swallowing, management of respiratorysecretions and tracheostomy tube cuff pressure,tracheostomy tube changes, and goals for decannulation.
Historically, stoma wound care was provided onlywhen nurses identified an issue and contacted thetracheostomy nurse practitioner or wound care nurses.With the weekly rounds, the stoma wounds are nowevaluated regularly, and recommendations are madefor both prophylactic management and promotion ofwound healing.
Goals of Tracheostomy Rounds
\|_oao1;r>oo|\>-
. Stoma wound care. Communication. Swallowing
Secretion Management. Cuff pressure management
Tracheostomy tube changes. Decannulation planning
2%.“
g I
Members of the Johns Hopkins Multidisciplinary Tracheostomy Team(JH-MDTT) review a patient chart during weekly rounds. From L to R:John Castro, RT; Ashleigh Davis, RT; Therese Cole, SLP; Vinciya Pandian,PhD, ACNP; Brendon Bower, RN; Amanda Owen, RN; Maura Costello, RN
Tracheostomy patients were being evaluated for speechonly if the primary team requested a consult. Often,the request could be delayed because of other urgentpriorities for the medical staff. The weekly rounds havehelped us to identify patients who are attempting tocommunicate. For patients still on the ventilator, it allowsus to initiate cuff deflation and in-line Passy-Muir® Valveuse earlier. When patients cannot tolerate cuff deflation,talking tracheostomy tubes are used to facilitate speech.
Modified barium swallow (MBS) studies are typicallyperformed for all patients with a tracheostomy. As aresult of the rounds, we have identified the need toperform a bedside fiberoptic endoscopic exam ofswallowing (FEES) instead of waiting for a convenienttime for MBS or transporting a critically ill patient for theMBS. FEES is usually done with or without a Passy-Muir®Valve. We are able to successfully perform the FEEStoward the end of rounds because all of the critical teammembers are available to provide assistance.

T YMultidisciplinary Tracheostom Program Rounds (continued)
Patients with a tracheostomy tube may have copioussecretions or dry thick secretions. During rounds,bedside nurses have made efforts to identify patternsof suctioning needs and retrospectively review theconsistency of patient secretions. This information enablesthe JH-MDTT to make specific recommendations forMucomyst or a scopolamine patch. These treatmentoptions were usually offered as a last resort, but noware considered early in the plan of care.
Communication with the respiratory therapists duringrounds regarding the tracheostomy tube enables earlyidentification of tracheomalacia or the need for earlytracheostomy tube change if cuff pressures areincreased. It also facilitates identification of appropriatesizes of tracheostomy tube for ventilation and speech.When indicated, tracheostomy tubes are downsizedto facilitate increased airway patency around thetracheostomy tube for use of a Passy-Muir® Valve forspeech. These rounds also help us to evaluate theappropriateness for timely decannulation.
Although this article provides an editorial about theestablishment of the JH-MDTT rounds, we are currentlycollecting outcome data to provide a more objectiveevaluation of this endeavor.
Acknowledgements:Kate Holden, SLP; Dana Kilonsky, SLP; Colleen McElroy,SLP; Michele Singer, SLP; Jillian Dinkheller, SLP; NicoleLangton, SLP; Kelly Heffron, Wound Care Nurse; Jac-queline Stokes, Respiratory Therapy Educator; Respira-tory Therapists and Nurses at Johns Hopkins Hospital;Claire Levine, Johns Hopkins Scientific Editor1. Pandian V, Miller CR, Mirski MA, Schiavi AJ, Morad AH, Vaswani RS,
Kalmar CL, Feller-Kopman DJ, Haut ER, Yarmus LB, Bhatti NI.Multidisciplinary team approach in the management of tracheostomypatients. Otolaryngol Head Neck Surg 2012;147(4):684-691.
2. Mirski MA, Pandian V, Bhatti N, Haut E, Feller-Kopman D, Morad A,HaiderA, Schiavi A, Efron D, Yarmus L, Stevens KA, Miller CA, PapangelouA, Vaswani R, Kalmar C, Gupta S, Intihar P, Mack S, Rushing AP,Chi A, Roberts VJ, Ulatowski J. Safety, efficiency, and cost-effectivenessof a multidisciplinary percutaneous tracheostomy program. Crit Care Med2012;40(6):1827-1834.
3. Arora A, Hettige R, lfeacho S, Narula A. Driving standards in tracheostomycare: a preliminary communication of the St. Mary’s ENT-led multidisci-plinary team approach. Clinical Otolaryngol 2008; 33(6): 596-9
4. Cameron TS, McKinstry A, Burt SK, Howard ME, Bellomo R, Brown DJ,Ross JM, Sweeney JM, O’Donoghue FJ. Outcomes of patients withspinal cord injury before and after introduction of an interdisciplinarytracheostomy team. Critical Care Resusc.11(1):14-9.
S ETI-I DATEA ||.29& 0,2016>V/
3rd International TracheostomySymposium
GTC 2016 North American KickoffJohns Hopkins University School of Medicine
Turner Building, 720 Rutland Ave.Baltimore, MD
WWW.GLOABLTRACH.ORG
@ Int otionol Q
T’ pififimy l°‘1I!S.i‘9‘1‘ilN3_--—

_ _ _
Clinicians attending Passy-Muir’snational seminars may have caught aglimpse of some exciting revisions to theToby Tracheasaurus“ pediatric program.
T0b‘lr,§ The enhancements include new dinosaur“°“°“““ cartoon characters, new therapeutic activity
cards, and a clinically improved TobyTracheasaurus” Coloring & Activity Bookthat is sure to appeal to tracheostomizedchildren, their caregivers and clinicians.
Tr
Each Toby Tracheasaurus“ pediatric program kitcomes with a draw-string backpack containing a TobyTracheasaurus” Plush Toy, the Toby Tracheasaurusl“Coloring & Activity Book with crayons, and a Toby Tote“with an assortment of therapeutic toys.
Featuring a pediatrictracheostomytube and Passy-Muir®Valve for the purpose of demonstration and education,the Toby Tracheasaurusl“ Plush Toy provides therapistswith a lighthearted method to introduce children totracheostomyandthe Passy-Muir®Valve,whilefacilitatingvocalization and enhancing therapeutic activities.
The cartoon dinosaur-themed Toby Totel“ containsclinician approved therapy toys, specifically selectedto help children practice oral exhalation, promote playtherapy, and reward children for therapeutic achievements.Used in conjunction with the Toby Tracheasaurus“Coloring & Activity Book, which features an assortmentof therapeutic and fun activities, the new TobyTracheasaurus“ materials are designed to help childrenvoice and exhale orally when using a Passy-Muir® Valve.Many of the therapeutic activities referred to in the bookmay be performed under supervision with toys from theToby Tote as well as toys readily available at most stores.
J »,. 4'
I
P s New Tracheasaurus Spotted at Passy-Muir Seminars-———Tr
T Y Trache ..8: Frienazaums
Wmi~Wu&
7//I \\ F»
'11‘*2 .1‘
I'llThe new Toby Tracheasaurus“ program
features pediatric, educational and therapeutic materials
We at Passy-Muir believe that communication is theessence of the human spirit; it is essential to individualrights and dignity. Tracheostomized children should beprovided with the same opportunities as others to allowthem to develop communication skills. It is our sinceresthope that the Toby Tracheasaurus” program will providemany hours of rewarding activity and will be enjoyed bychildren and their families.
To find out more about ourToby Tracheasaurus“! pediatricprogram, or to download copies of Toby coloring andactivity sheets, be sure to visit us at:www. passy-muir.com/products_edu_ped

TRACHTOOLS™
Speech & Resources App
TALBi€5::LJNl$lUIR
l\l\er1'<wit CONSULTANTS!Sheila Clark, DHEd, CCC-SLPSheila has been a speech language pathologist for 25 years and has worked with both pediatricand adult patients in a variety of settings. She earned a doctorate in health education in 2008 andenjoys educating healthcare professionals on the use of a holistic approach to clinical care. She hasworked closely with multiple disciplines to become an advanced practitioner in the specialty areas ofdysphagia, neurological disorders, critical care, and the management of patients with tracheostomyand mechanical ventilation.
Sara Grzina, MHS, CCC-SLPSara earned her Master’s Degree from University of Missouri — Columbia in 2010 and hasgained more than 5 years of pediatric clinical experience working with children in NICU, acutecare and outpatient settings, with specialized training evaluating and treating children withtracheostomies and swallowing disorders. Sara is currently a Speech-Language Pathologist atMercy Kids in St. Charles, MO and Cardinal Glennon Children's Medical Center in St. Louis, MO.
INTRODUCING
A NEW user-friendly app for iPhone and iPad designed to facilitatepatient communication, provide valuable information regardingtracheostomy and foster patient participation in care.
FEATURES:Pre-recorded responses & phrases enable communication ata touch of a buttonUser-defined male or female voice
I Child voice optionI Easy to use features & navigationI Links to useful resources for both patient & clinician
I‘gm: Patient videos
FREE download for a limited time at the app store or www.passy-muir.com/app
Talk-Muir is published by Passy-Muir, Inc. for clinicians and for tracheostomy and ventilator-depen- Passy-Muir, Inc.dent patients, their caregivers and medical professionals in an effort to educate, support research, PMB 273and provide ' Interesting news and stories ' Resources and clinical guidelines ~ Information about new 4521 Campus Driveeducational opportunities 0 Upcoming events. Irvine, CA 92612
Dam A Muir Contributions and comments are welcome.Inventor
PPO 21 0 © 2015 Passy-Muir, Inc. All rights reserved.