Paranasal-sinuses-2008-.pptx
70
Paranasal sinuses By: Atheer Al-Sabri Khalil Al- Saffar
-
Upload
heba-s-radaideh -
Category
Documents
-
view
3 -
download
0
Transcript of Paranasal-sinuses-2008-.pptx
Slide 1
Paranasal sinusesBy: Atheer Al-Sabri Khalil Al-Saffar Eman Dhaif
Pseudo stratified columnar ciliated epithelium3
A coronal cross section diagram of the skullSuperior meatusMiddle MeatusEthmoid sinuses
A coronal cross section diagram of the skullFrontal sinusesFronto-nasal duct
Sphenoid sinusesBody of the sphenoid bone
Sphenoethmoidal recess
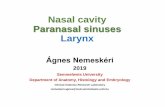
Sagittal CT image showing the sphenoid sinus (SpS) with sinus ostium (*) and arrow demonstrating the sphenoethmoidal recess (SER). (PE: posterior ethmois sinus)
Maxillary sinusesA coronal cross section diagram of the skullSemilunar hiatusZygomatic recessAlveolar recessInfraorbital recessHeating and humidification
Reduction of cranial weight
Voice resonation
Evolutionary unwanted space
FucntionImaging themaxillary sinusPeriapical radiographHighest detail/ resolution
Only floor can be viewed
Periapical radiographZygomatic proccessNasal fossaSeptumPeriapical radiographSoft radiolucent neurovascular canals
These are bony nodules, that appear to be well defined and blend at certain points, homogenous and showing trabeculation.
Waters viewOccipitomental radiograph Head tilted back 37 degrees
X-ray tubeX-ray receptor or film
Frontal sinusesMaxillary sinusZygomatic boneSuperior maxillary borderZygomatic archLateral cephalometricSuperimposition of the left and right sides.
The structures closer to the image receptor appear less magnified.
Not used as a diagnositic tool.
Lateral cephalometricSphenoid sinusEthmoid sinusMaxillary sinusFloor of the orbitPterygomandibular fissureZygomatic body and processHard palate
This is lateral skull radiograph of the mucous retention in the maxillary sinus Panoramic radiographFull continous border
Super imposition of the zygoma
Compare the left and right sinuses for abnormalities.
Usually asymmetrical
Infraorbital canalZygomatic bodyComputed tomographySlit like beam of rays.
Receptor encircles the patient
Produces images which resembles slices of the patient.
Contraindications: Acute inflammatory swelling
CT Scan a large mass was seen in the Maxillary SinusMagnetic resonance imagingRapidly changing magnetic fields.
Physical and biochemical properties of the tissue examined.
Differentiating between inflammatory and tumor tissue.
Right maxillary mucocele eroding superior wall of the sinus causing eye proptosis and cheek swelling.CT versus MRIADVANTAGES OF CT
Better bony detail
Less expensive
More readily available.
Dental artifacts
Patient comfortADVANTAGES OF MRI
Superior soft tissue discrimination
Multiplanar
No radiation
Vascular anatomy
Intrinsic diseases of the maxillary sinusMucositis Definition: increase in thickness of lining mucosa 10 to 15 times due to infection or allergic process.Clinical features:Asymptomatic unrecognized by patient and are discovered only incidentally on a radiograph.
Radiographic findings:Thickened mucosa is detectable in the radiogrph as a noncorticated band notice more radiopaque than air filled sinus .
Locally thickened mucosa is seen as a noncorticated, radiopaque band that follows the contour of the sinus floor.Sinusitis Definition: Generalize inflammation of paranasal sinus mucosa due to allergen, bacteria, or viral and there Is classification that divide sinusitis into three subtypes based on the time :-Clinical features Can cause clear nasal discharge or pharyngeal drainage and the patient may complain of pain and tenderness to pressure or swelling over the involved sinus associated with fever, chills, malaise and elevated leukocyte. The pain may also referred to the premolar and molar teeth on the affected side. No external sign occur. Chronic sinusitis associated with anatomic derangements that inhibit the outeflow of mucus and also associated with allergic, asthma, cyctic fibrosis and dental infection. Acute sinusitis: Chronic sinusitis:Thickening of sinus mucosa and accumulation of secretions that reduce air content of the sinus that cause increase radiopacity. the most common radiopaque patterns that occur in the Waters view are localized mucosal thickening along sinus floor and generalized thickening of the mucosal lining around the entire wall of the sinus. Radiographic feature
Sinusitis results in generalised thickening of the mucosa, which makes the internal structure of the maxillary sinus more radiopaque. Figure A: Internal radiopacity. Figure B: Normal sinus.Definition: Blockage of the secretory ducts of seromucous gland in the sinus mucosa.The retention pseudocyst rarely cause any sign or symptoms, some clinical features show nasal obstruction and postnasal discharge.
Pseudocyst may occur bilaterally. Occasionally more than one pseudocysts may form in sinus and some may form on the lateral walls.
Retention pseudocyst Radiographic features Clinical features
This is lateral skull radiograph of the mucous retention psuedocyst in the maxillary sinus Polyps Definition: The thickened mucous membrane of a chronically inflamed sinus frequently forms into irregular folds.Clinical features:
Cause displacement or destruction of bone and can cause destruction of the medial wall of the orbit.Radiographic features:Polyp usually occurs with a thickened mucous membrane lining.
This is CT, Coronal image with arrow pointing to maxillary sinus polyp. Often on imaging a polyp and mucus retention cyst cannot be differentiated, but is usually of little clinical consequence.Antrolith Definition:Antroliths occur within the maxillary sinus and result of deposition of mineral salts such as calcium phosphate, calcium carbonate, and magnesium around a nidus.Clinical features:
The smaller antrolith are asymptomatic and usually are discovered as incidental findings on the radiographic examination and the patient associated sinusitis, blood stained nasal discharge, nasal obstruction, or facial pain.Radiographic features:
Antrolith are well defined and may have a smooth or irregular shape.
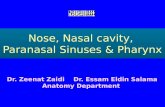
A lateral maxillary occlusal film that reveals the presence of a radiopaque antrolith. Note that the antrolith is positioned above the sinus floor.MucoceleDefinition : Mucocele is an expanding, destructive lesion that result from blocked sinus ostium.Clinical features:
Fullness in the cheek and the area may swell and it may cause loosening of the posterior teeth in the area and also can cause diplopia.
Radiographic features:
About 90% of mucoceles occur in the ethmoidal and frontal sinus and rare in the maxillary and sphenoid sinuses and the shape of sinus change into more circular shape as the mucocele enlarges.
This is maxillary sinus on the right side is completely obliterated by a mucocele and these mucoclel cystic like multiloculated mass and also This mucoclele extends fills the upper nasal cavity on the right and displacing the orbital contents.Benign neoplasms of the paranasal sinuses Epithelial papilloma Osteoma Epithelial papilloma Definition: The epithelial papilloma is rare neoplasm of respiratory epithelium that occur in the nasal cavity and paranasal sinuses. It occur manly in the men.Clinical features :
Unilateral nasal obstruction, nasal discharge, pain and the patient may have complained of recurring sinusitis for years. The epithelial papilloma relatively rare and has 10% incidence of associated carcinoma.Radiographic features:
Its appears as an isolated polyp in the nose or sinus. This neoplasm appears as a homogenous radiopaque mass of soft tissue density.
A recurrent right maxillary sinus inverted papilloma. The entire mass in the maxillary sinus is homogeneous by CT scan.
MRI scan of the same patient demonstrating the delineation between retained secretions and inverted papilloma. However, the MRI does not define the site of attachmentOsteoma Definition: Osteoma is the most common of the mesenchymal neoplasm in paranasal sinuses.Clinical features:It is almost twice as common in the males as females and more common in the second, third and fourth decades. Most are slow growing and asymptomatic and when symptoms occur they are result of obstruction of the sinus. Those growing in maxillary sinus may extend into nose and cause nasal obstruction or swelling of the side of the nose. Radiographic features:Usually lobulated or rounded and has sharply defined margin and the internal aspect is homogenous and extremely radiopaque.
A lateral cephalometric skull projection shows a frontal sinus osteoma as a well-defiend, uniformly radiopaque mass (arrow).
Malignant neoplasms of the paranasal sinuses
Squamous cell carcinoma PseudotumorSquamous cell carcinoma Definition: Squamous cell carcinoma from metaplastic epithelium of the sinus mucosal lining.Clinical features:
Facial pain or swelling, nasal obstruction and lesion in the oral cavity. The mean age of the patient is 60 years (range 25 to 89 years) and also lymph nodes are involved in about 10% of cases. the symptoms are present for about 5 months before diagnosis.Radiographic features:
Most carcinomas occur in the maxillary sinuses but involvement of the frontal and sphenoid sinuses is also common and the internal aspect of the maxillary sinus has radiopaque appearance.
Pseudotumor Definition: Pseudotumor is descriptive name for a group of related diseases of fungal origin that occur in the paranasal sinuses. Clinical features:
The symptoms may not be very specific and may be cause erosion of the walls of the involved sinus. Altered nerve function resulting from involvement of the nerve or occlusion of blood vessels by the mass has also been reported.Radiographic features:
The radiographic findings in pseduotumor include masses that cause erosion of bony walls of the involved sinuses.
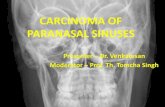
71-year-old man with inflammatory pseudotumor and malignant transformation of left maxillary sinus. Patient had left gingival pain for 6 months. Axial (A) and coronal (B) CT scans show soft-tissue lesion (M inB) in left maxillary sinus. Associated massive bony destructions are evident. Radiologic primary diagnosis was malignant lesion with bony destruction. Wide excision was performed. Pathologic results indicated inflammatory pseudotumor with malignant transformation.
ABExtrinsic inflammatory diseasesInflammatory odontogenic diseaseClinical features:
Diffusion of inflammatory exudate
Usually resolves in days or weeks
Radiographic features:
Homogeneous radiopaque
Follows the contour of the floor
PeriostitisExudate from dental inflammatory lesions.
Can strip and elevate the periosteal lining of the cortical bone of the floor of the maxillary antrum.Radiographic Features Thin radiopaque line, or it may be very thick or, rarely, laminated(similar to onion skin).
The halo-like appearnace of bone (arrow) surrounding the palatal root of the first molar is the result of periosteal new bone formationOdontogenic cystsMost common group of extrinsic lesions that encroach on the maxillary sinusesRadicular cysts
Dentigerous cysts
Odontogenic keratocystRadiographic features:
Curved or oval shape defined by a corticated border.
The cyst may displace the floor of the maxillary antrum. In some cases the cyst may enlarge to the point that it has encroached on almost the entire sinus
Internal structure:
Homogeneous and radiopaque.
Most common perioral radiolucencyAssociated with the crown of an unerupted tooth (in this instance, the upper right 8).Has a well defined, corticated margin (arrows).Dentigerous cyst
Radicular cystPeriapical lucency, corticated margin, > 1.5cm
Arise from epithelial rests in the perodontal ligament as a consequence of inflammation.
Odontogenic keratocyst containing a third molar tooth inthe maxillary antrum.TraumaDENTAL STRUCTURES DISPLACED INTO THE SINUS
Definition
Tooth roots may be fractured as a result of various formsof trauma, including iatrogenic causes.
Fractured roots may be forced into the sinus during extractionClinical Features
No specific features may be visible if the root was displaced into the sinus recently: However, the dentist may note the absence of the root fragment on examining the extracted tooth and be unable to locate it anywhere .
Asking the patient to hold his or her nose while attempting to breathe out through it will cause bubbles to appear within the blood contained within the fresh extraction socket.
The dental fragment usually has no effect on surrounding structures; however, sinusitis may result.Radiographic Features
Location of the Roots or teeth in the sinus are associated with premolars and molars because the sinus is often in close proximity to the roots.
More often they are located near floor of the sinus because of gravity .
Sometimes the displaced structure may be submucosal, between the osseous wall of the sinus and the periosteum.
Retained root into antrum
Coronal view shows the palatal root lodged into the ostium of the maxillary sinus.FIBROUS DYSPLASIAMay arise in
Maxillary boneSphenoid boneFrontal boneEthmoid boneTemporal bone
Clinical Features
Facial asymmetry.Nasal obstruction.Proptosis.Pituitary gland compression.Impingement on cranial nerves.Sinus obliteration.Lesion may displace the roots of teeth and cause teeth to separate or migrate. More common in children and young adults
Radiographic Features
The posterior maxilla is the most common location. Usually not well defined, tending to blend into the surrounding bone.The normal radiolucent maxillary antrum may be partially or totally replaced by the increased radiopacity of this lesion .The degree of radiopacity depends on its stage of development and the relative amounts of bone present.The radiopaque areas have the characteristic "ground glass"appearance on extraoral radiographs or an "orange peel" appearance on intraoral views.
Fibrous dysplasiaMonostotic form more common in the craniofacial regionGround glass change with areas of sclerosis (arrows)More ill-defined border compared to ossifying fibromaThank you