Paranasal Sinus Cancer
38
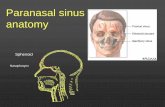
Paranasal sinus cancer Definition Paranasal sinus cancer is a disease in which cancer (malignant) cells are found in the tissues of the paranasal sinuses—the four hollow pockets of bone surrounding the nasal cavity. Description The paranasal sinuses, which are arranged symmetrically around the nasal cavity, include the: frontal sinuses (in the forehead, directly above the nose) ethmoidal sinuses (on each side of the nasal cavity, just behind the upper part of the nose) maxillary sinuses (on each side of the nasal cavity, in the upper region of the cheek bones) sphenoidal sinuses (behind the ethmoidal sinuses, in the center of the skull) The paranasal sinuses, which normally contain air, are lined by mucous membranes that moisten the air entering the nose. Because they contain air, the sinuses allow the voice to echo and resonate. Because the paranasal sinus area lies in an anatomically complex region, tumors in the paranasal sinuses can invade a variety of structures—such as the orbit (the bony cavity protecting the eyeball), the brain, the optic nerves, and the carotid arteries— even before symptoms appear. The pharynx (throat) is divided into three sections: the nasopharynx, oropharynx, and laryngopharynx. The nasopharynx is the area behind (posterior to) the nose. The oropharynx is the area posterior to the mouth. The laryngopharynx opens into the larynx and esophagus. Usually, cancers of the paranasal sinuses originate in the lining of
-
Upload
silvia-aslami -
Category
Documents
-
view
227 -
download
0
description
stase THT
Transcript of Paranasal Sinus Cancer

Paranasal sinus cancer
Definition
Paranasal sinus cancer is a disease in which cancer (malignant) cells are found in the tissues of the paranasal sinuses—the four hollow pockets of bone surrounding the nasal cavity.
Description
The paranasal sinuses, which are arranged symmetrically around the nasal cavity, include the:
frontal sinuses (in the forehead, directly above the nose)
ethmoidal sinuses (on each side of the nasal cavity, just behind the upper part of the nose)
maxillary sinuses (on each side of the nasal cavity, in the upper region of the cheek bones)
sphenoidal sinuses (behind the ethmoidal sinuses, in the center of the skull)
The paranasal sinuses, which normally contain air, are lined by mucous membranes that moisten the air entering the nose. Because they contain air, the sinuses allow the voice to echo and resonate.
Because the paranasal sinus area lies in an anatomically complex region, tumors in the paranasal sinuses can invade a variety of structures—such as the orbit (the bony cavity protecting the eyeball), the brain, the optic nerves, and the carotid arteries— even before symptoms appear.
The pharynx (throat) is divided into three sections: the nasopharynx, oropharynx, and laryngopharynx. The nasopharynx is the area behind (posterior to) the nose. The oropharynx is the area posterior to the mouth. The laryngopharynx opens into the larynx and esophagus. Usually, cancers of the paranasal sinuses originate in the lining of the nasopharynx or oropharynx. In rare cases, melanomas—a type of cancer arising from dark pigment-producing cells called melanocytes—may appear in the naso-or oropharynx. There is also an area of specialized sensory epithelium (surface layer of cells) through which the terminal branches of the olfactory nerve enter the roof of the nasal cavity, which gives rise to a very rare malignant neoplasm (growth) known as an esthesioneuroblastoma, or olfactory neuroblastoma .
Infrequently, a cancer may arise from the muscles or the soft tissues of the paranasal sinus region; these lesions are called sarcomas . Occasionally, lesions called midline granulomas (a granular-type tumor usually from lymphoid or epithelioid cells) occur; these lesions arise in the nose or paranasal sinuses and spread to surrounding tissues. Also rare are slow-growing cancers called inverting papillomas (papillae are tiny, nipple-like protuberances).

Demographics
Malignant growths of the paranasal sinuses are uncommon in the general population. Paranasal sinus cancer represents 3% of all cancers in the upper aerodigestive tract (air and food passages) and less than 1% of all malignancies in the body. The incidence of paranasal sinus cancer is about one case per 100, 000 people per year in the United States. Only about 200 new cases a year are diagnosed in the United States. The disease is more common in Asia Minor and China than in Western countries. The incidence of maxillary sinus cancer is highest in the South African Bantus and in Japan.
Paranasal sinus tumors occur about two to three times more frequently in men than women, and diagnosis usually occurs between the ages of 50 and 70. Cancers of the maxillary sinus are the most common of the paranasal sinus cancers, occurring in about 80% of individuals. Tumors of the ethmoidal sinuses are less common (about 20%), and tumors of the sphenoidal and frontal sinuses are rarest (less than 1%).
Squamous cell carcinoma (cancer that originates from squamous keratinocytes in the epidermis, the top layer of the skin) is the most frequent type of malignant tumor in the paranasal sinuses (about 80%). Adenocarcinomas (cancer that begins in cells that line certain internal organs and that have glandular, or secretory, properties) constitute 15%, and the remaining 5% are composed of all other types.
Causes and symptoms
Although the causes of paranasal sinus cancer are not known, several occupational groups have been found to have an increased risk of developing these tumors. These groups include leather and textile workers, nickel refiners, woodworkers, and manufacturers of isopropyl alcohol, chromium, and radium. Also, snuff and thorium dioxide (a radiological contrast agent) have been associated with an increased incidence of paranasal sinus cancer. It is unclear whether these factors cause cancer by direct carcinogenesis (cancer production) or by altering the normal nasal epithelial physiology.
Nickel workers primarily develop squamous cell carcinomas, which usually arise in the nasal cavity. Woodworkers, however, usually develop adenocarcinomas that usually arise in the ethmoidal sinuses. The incidence of adenocarinomas in these workers is 1, 000 times higher than that of the general population. Tobacco and alcohol use have not been demonstrated conclusively as a causative factor in the development of paranasal sinus tumors. However, viral agents, especially the human papilloma virus (HPV), may also play a causative role.
In patients with cancer of the head and neck, the immune system is often not functioning properly. Malignant cells are not recognized as foreign, or when recognized, the immune system does not effectively destroy cancer cells. Causes of the failure of the immune system include severe malnutrition, substances in the tumor that deactivate the immune system, or a genetic predisposition.

The symptoms of paranasal sinus cancer vary with the type, location, and stage of cancer present. Symptoms typical of early lesions often resemble those of an upper respiratory tract infection and include nasal obstruction, facial pain, and thin, watery nasal discharge (rhinorrhea), which can at times be blood-tinged. The key factor that differentiates the symptoms of an upper respiratory infection from a malignant lesion, however, is the duration of the symptoms. An upper respiratory infection generally clears up or improves dramatically in several weeks with appropriate medical care, but symptoms associated with a malignancy persist.
The most common symptoms of paranasal sinus cancer include:
persistently blocked nose
feeling of recurrent "sinus infections"
bleeding without apparent cause from the nose or the paranasal sinuses
progressive pain and swelling of the upper region of the face or around the eyes
closing up of one eye, blurred vision, or visual loss
persistent pain in the forehead, the front of the skull, or over the cheekbones
swelling in the roof of the mouth
loosening of teeth, poorly fitting dentures, or bleeding from upper teeth sockets
Tumors in the nasal cavity and paranasal sinuses metastasize (spread) to the cervical lymph nodes (lymph nodes in the neck) in about 15% of individuals.
Diagnosis
There are several steps in establishing a diagnosis of paranasal sinus cancer. The first step is a thorough medical history, followed by a physical examination. The physical examination may reveal a lesion in the nose or a submucosal (below the mucous membrane) mass arising in an adjacent sinus.
After the history and physical examination, a series of tests are performed to determine the precise nature of the suspicious growth and the extent of its spread. These tests may include:
Biopsy (the removal of a sample of tissue that appears to be suspicious) is performed after a lesion is identified. The tissue is studied under the pathologist's microscope.

Computed tomography (CT) scan, which is a series of detailed pictures with thin cross-sectional slices taken radiologically through the body and interpreted with a computer.
Nasoscopy, which utilizes an instrument called the nasoscope for examining the nasal cavity and the paranasal sinuses.
Magnetic resonance imaging study (MRI), an imaging study that consists of detailed pictures, but instead of using x rays, a powerful magnet is used to polarize electrons inside the body to obtain images, which are then interpreted by a computer.
Posterior rhinoscopy, in which the nasopharynx and the rear portion of the nose are examined using a light and a special mirror.
Although endoscopic techniques (visualizing the nasal cavity with an endoscope—a tube-like device to which an optical system is attached) have greatly improved the ability to examine the nasal cavities and the paranasal sinuses, radiographic studies are also necessary in completing the evaluation. The most important radiographic studies include CT and MRI scans, usually used in combination. The MRI scan has become the most essential radiographic test for accurate delineation of pretreatment tumor extent, and also for following up patients after treatment.
However, each scanning technique has its own advantages and limitations. The CT scan is preferred in evaluating the bony structures in the paranasal sinus area. The MRI better assesses soft-tissue differences, enabling not only the differentiation of tumor from inflammatory changes in the nose and sinuses, but also the determination of involvement of the soft tissues in, for example, the orbit, the brain, and the optic nerve.
Obtaining a biopsy is crucial to diagnosis. Endoscopic sinus surgery is widely used for obtaining tissue for biopsy. Combining endoscopic surgery with CT imaging, however, allows the surgeon access into small recesses of the nose and sinuses and along the base of the skull, making biopsy not only more accurate but also safer for the patient.
Treatment team
Patients with paranasal sinus cancer are usually treated by a team of specialists using a multifaceted approach. Each patient receives a treatment plan that is tailored to fit his or her requirements, specifically the patient's overall constitution, grade, and stage of disease. Usually, however, the treatment team includes:
an otorhinolaryngologist (ear, nose, and throat specialist)
an oncologist (cancer specialist)
a radiotherapist (x-ray treatment specialist)

If extensive surgery is required, a plastic and reconstructive surgeon may also serve as part of the treatment team.
Clinical staging, treatments, and prognosis
Paranasal sinus cancer staging involves carefully establishing the degree of cancer spread. If the cancer has spread, it is also necessary to establish the extent of spread and organ involvement.
Cancer grading is a microscopic issue; the pathologist determines the degree of aggressiveness of the cancer. The term well-differentiated means less aggressive; the terms moderately differentiated, intermediately aggressive, and poorly differentiated mean more aggressive.
Both grading and staging help the physician establish the prognosis (degree of seriousness of the disease) and likely outcome.
Staging
Staging may involve additional imaging tests such as CT scan of the brain, abdominal ultrasound, bone scan, or chest x ray . Although no clear-cut staging protocol exists for the relatively uncommon cancers of the paranasal sinuses, the following practical staging exists for cancer of the maxillary sinuses, the most common cancer of this area:
Stage I: The cancer is confined to the maxillary sinus, with no bony erosion or spread to the lymph nodes.
Stage II: The cancer has begun to destroy the surrounding bones but without spread to the lymph nodes.
Stage III: The cancer has spread no further than the bones around the sinus and to one node on the same side of the neck, and is no greater than 3 cm (1.1 in) in size, or has spread to the cheek, the rear portion of the sinus, the eye socket, or the ethmoidal sinus (spread to lymph nodes on the same side of the neck may or may not be present).
Stage IV: The cancer has spread to the eye, other sinuses, or tissues adjacent to the sinuses (spread to lymph nodes on the same side of the neck may or may not be present). The cancer may have spread within the sinus itself or to surrounding tissues, to lymph nodes in the neck on one or both sides, to any node larger than 6 cm (2.3 in), or to other parts of the body. Recurrent maxillary sinus cancer—either in the same location or in a different one after primary treatment has been completed—is also in this category.
Treatment options
The major treatment options for paranasal sinus cancer include:

Surgery. May be necessary for the removal of a section of the nasal cavity or the paranasal sinus at any stage of the disease. Also, some lymph node dissection may be required in the neck, depending upon the staging and grading. May be combined with radiotherapy at any stage, depending on the type of cancer and its location.
Radiotherapy. Also called radiation therapy , radiotherapy is sometimes used alone in stage I and II disease, or in combination with surgery in any stage of the disease. In the early stages of paranasal sinus cancer, radiotherapy is considered the alternative local therapy to surgery. Radiotherapy involves the use of high energy, penetrative rays to destroy cancer cells in the zone treated. Radiation therapy is also employed for palliation (control of symptoms) in patients with advanced cancer. Teletherapy (external radiation) is administered via a machine remote from the body while internal radiation (brachytherapy) is given by implanting a radioactive source into the cancerous tissues. Patients may or may not require both types of radiation. Radiotherapy usually takes just five to ten minutes per day, five days a week for about six weeks, depending upon the type of radiation used.
Chemotherapy . Usually reserved for stage III and IV disease. Besides local therapy, the best attempt to control cancer cells circulating in the body is by using systemic therapy (therapy that affects the entire body) in the form of injections or oral medications. This form of treatment, called chemotherapy, is given in cycles (each drug or combination of drugs is usually administered every three to four weeks). Chemotherapy may also be used in combination with surgery, radiotherapy, or both.
At the forefront of research into head and neck cancer, molecular biology and gene therapy are providing new insights into the basic mechanisms of cancer genesis and treatment. The detection of various oncogenes (genes that can induce tumor formation) in head and neck cancer is also progressing rapidly. Gene therapy trials, still in their infancy as of 2001, are also introducing genetic material to help the immune system recognize cancer cells.
ALTERNATIVE AND COMPLEMENTARY TREATMENTS.
Alternative and complementary therapies may also be used at any stage of the disease. Alternative treatments are treatments used instead of conventional treatments. Complementary therapies are used in addition to conventional treatments. Although not specifically used in treating paranasal sinus cancer, there is much anecdotal (non-scientific) evidence for a number of alternative cancer therapies. Some insurance plans cover complementary therapies, such as acupuncture.
The safest and most accepted of these complementary therapies include:
acupuncture
biofeedback
diet that includes fresh fruit, vegetables, and whole grains

massage
meditation, prayer, or creative visualization
vitamins (especially antioxidants A, E, and C), minerals, and herbs
The National Center for Alternative and Complementary and Alternative Medicine, part of the National Institutes of Health, discusses some alternative and complementary cancer treatments on its web site <http://www.nccam.nih.gov>.
Prognosis
The high mortality rate and poor prognosis association with paranasal sinus cancer is related to late diagnosis. Most lesions (75%) are at an advanced stage at the time of definitive diagnosis. Surgical treatment alone may be sufficient for stage I or II lesions if adequate surgical margins are obtained. However, for advanced tumors, combined therapy with radical surgical excision and postoperative radiotherapy has been demonstrated to improve the five-year survival rate.
The primary cause of death is failure of local control. Most paranasal sinus cancers grow rapidly and invade nearby tissues but are slow to spread to distant sites. Thus, patients with advanced disease usually die from a local recurrence of their tumor, even after aggressive treatment.
Coping with cancer treatment
Cancer treatments such as radiotherapy and chemotherapy not only destroy cancer cells but also damage healthy tissue. The effects of radiation depend upon the dose of radiation, the size of the area radiated, and the number and size of each fraction. When doses are fractionated, the total dose of radiation therapy is divided into several smaller, equal doses delivered over a period of several days.
The most common side effect of radiotherapy is extreme fatigue . Although rest is encouraged, most radiotherapists advise patients to move around as much as possible. Another common side effect is radiation dermatitis— the skin covering the radiated area becomes red, dry, itchy, and may show signs of scaling. This skin problem is associated only with teletherapy (external radiation therapy).
Radiation also may cause nausea and vomiting , diarrhea , and urinary discomfort. There may also be a decrease in white blood cells, which are needed to fight infection. Usually the radiotherapist can suggest the drugs and diet necessary to alleviate these problems.

Chemotherapy drugs may cause a wide spectrum of side effects. The severity of these symptoms vary with each drug and with each individual. Some of the most common side effects of chemotherapy include:
diarrhea
hair loss (alopecia )
hearing loss
skin rashes
tingling and numbness in the fingers and toes
vomiting
Most of these side effects are treatable, temporary, and recede after therapy ends. However, the attitude of the patient is very important during cancer therapy. The better psychologically prepared the patient is for treatment, the better the chances of experiencing decreased side effects.
If extensive surgery is required, reconstruction and rehabilitation by specialized physicians can improve the patient's quality of life.
Clinical trials
As of 2001, 35 clinical trials involving paranasal sinus cancer were operating in the United States. Clinical trials can be located at the web site <http://www.clinicaltrials.gov>, a service of the National Institutes of Health and the National Library of Medicine.
Some of the new drugs under investigation for advanced, recurrent, or metastatic head and neck cancer—either alone, in combination, with concurrent radiotherapy, or with standard chemotherapy drugs such as fluorouracil (5-FU), paclitaxel , or cisplatin —include:
A10 and AS2-1 (antineoplastons)
Dimesna (chemoprotective agent)
Fenretinide (retinoid, or vitamin A derivative)
Filgrastim (G-CSF or granulocyte colony-stimulating factor; increases white blood cells)
Flavopiridol (cyclin-dependent kinase [Cdk] inhibitor; kinases plays a role in cell cycle regulation and tumor formation)

Gemcitabine (antimetabolite)
ONYX-015 (genetically engineered cold virus)
C225/cetuximab (monoclonal antibody)
Oxaliplatin (platinum compound; chemotherapeutic agent)
SU5416 (angiogenesis inhibitor)
Prevention
The causes of paranasal sinus cancer are unknown. However, avoiding environmental risk factors such as heavy smoking or drinking, or inhaling wood dust or other toxic substances (such as isopropyl alcohol, chromium, or radium) on a regular basis may decrease the chances of developing this form of cancer.
Special concerns
Although surgical treatment of squamous cell carcinoma of the head and neck offers the best chance for cure in many patients, the results of the surgery have often been extremely disfiguring and functionally debilitating. The changes in facial appearance and loss of ability to speak, swallow, and breathe normally can be devastating, both physically and psychologically.
If the anticipated surgical defect is large, often a reconstructive team will harvest tissue from a distant site in the body to use as a graft while the oncology team is removing the cancer. Initially, reconstructive teams were more concerned with simply closing the surgical defect and re-establishing a more natural form. Increasingly, the focus has been to re-establish normal function.
Resources
BOOKS
Abeloff, Martin D., James O. Armitage, Allen S. Licter, and John E. Niederhuber. "Paranasal Sinuses and Nose." In Clinical Oncology, 2nd ed. New York: Churchill Living stone, 2000: 1297-1299.
Harrison, Louis B., Roy B. Sessions, and Waun Ki Hong, eds. Head and Neck Cancer: A Multidiscplinary Approach. Philadelphia: Lippincott Williams & Wilkins, 1999.
Schantz S. P., L. B. Harrison, and A. A. Forastiere. "Tumors of the Nasal Cavity and Paranasal Sinuses, Nasal Pharynx, Oral Cavity, and Oropharynx." In Cancer: Principles and Practice of Oncology, 5th ed. DeVita, V. T. Jr, S. Hellman, and S.A. Rosenberg, eds. Philadelphia: Lippincott-Raven Publishers, 1997: 741-801.

PERIODICALS
Lee, Misa M., et al. "Multimodality Therapy in Advanced Paranasal Sinus Carcinoma: Superior Long-Term Results." Cancer Journal from Scientific American 5 (August 1999): 219-223.
Khuri, Fadlo et al. "A Controlled Trial of Intratumor ONYX-015, a Selectively Replicating Adenovirus, in Combination with Cisplatin and 5-Fluorouracil in Patients With Recurrent Head and Neck Cancer." Nature Medicine. 6 (August 2000): 879-885.
ORGANIZATIONS
American Cancer Society, 1599 Clifton Road, NE, Atlanta, GA 30329-4251. <http://www.cancer.org> Phone: 1-800-ACS-2345.
National Cancer Institute. Public Inquiries Office, Building 31, Room 10A03, 31 Center Drive, MSC 2580, Bethesda, MD 20892-2580. <http://www.nci.nih.gov>. Phone: 1-800-4-CANCER.
National Center for Complementary and Alternative Medicine (NCCAM), NCCAM Clearinghouse, P.O. Box 8218, Silver Springs, MD 20907-8218, <http://www.nccam.nih.gov> Phone: 1-888-644-6226.
OTHER
<http://www.clinicaltrials.gov> (List of clinical trials)
Cancernet (List of organizations and web sites offering information and services for cancer patients and their families)<http://www.cancernet.nci,nih.gov/cancerlinks.html>
<cancersource.com> (Cancer resources for patients and families)
Genevieve Slomski, Ph.D.

Sinonasal malignant neoplasms are rare tumors that constitute about 3% of tumors in the upper respiratory tract. Only a fraction arises at the nasal cavity.[1] Due to the contiguity of the nasal cavities with the paranasal sinuses, identifying the specific site of origin of large sinonasal tumors is often difficult. Henceforth, malignant tumors of the nasal cavities are often grouped with those in the paranasal sinuses. Their proximity to vital structures such as the brain, optic nerves, and internal carotid artery pose significant challenges for their treatment and may be the source of significant morbidity to the patients. Malignant tumors of the sinonasal tract are derived from diverse histologic elements within the nasal cavity. They include the following:
Epithelial
Squamous cell carcinoma
Transitional cell carcinoma
Adenocarcinoma
Adenoid cystic carcinoma
Melanoma
Olfactory neuroblastoma
Undifferentiated carcinoma
Nonepithelial
Soft-tissue sarcoma
Rhabdomyosarcoma
Leiomyosarcoma
Fibrosarcoma
Liposarcoma
Angiosarcoma
Myxosarcoma
Hemangiopericytoma
Connective tissue sarcoma
Chondrosarcoma
Osteosarcoma
Synovial sarcoma
Lymphoreticular tumors

Lymphoma
Plasmacytoma
Giant cell tumor
Metastatic carcinoma
Epidemiology
Frequency
The annual incidence of nasal tumors in the United States is estimated to be less than 1 in 100,000 people per year. These tumors occur most commonly in whites, and the incidence in males is twice that of females.[2] Epithelial tumors most commonly present in the fifth and sixth decades of age.
Although tumors of the nasal cavities are equally divided between benign and malignant types, most tumors of the paranasal sinuses are malignant. Approximately 55% of sinonasal tumors originate from the maxillary sinuses, 35% from the nasal cavities, 9% from the ethmoid sinuses, and the remainder from the frontal and sphenoid sinuses. Squamous cell carcinoma is the most common malignant histologic type (approximately 70-80%) followed by adenoid cystic carcinoma and adenocarcinoma (approximately 10% each).[3]
Etiology
Exposures to industrial fumes, wood dust, nickel refining, and leather tanning have all been implicated in the carcinogenesis of various types of sinonasal malignant tumors. In particular, wood dust and leather tanning exposures are well associated with increased risk for adenocarcinoma.[4] Other etiologic agents have been reported including mineral oils, chromium and chromium compounds, isopropyl oils, lacquer paint, soldering and welding, and radium dial painting. Tobacco smoking is not considered to be a significant etiologic factor; however, recent studies demonstrated a higher incidence of nasal cancers in cigarette smokers.[2, 5]
Presentation
Tumors of the sinonasal tract commonly present with symptoms that are identical to those caused by inflammatory sinus disease, such as nasal obstruction, nasal discharge, epistaxis, headache, facial pain, and nasal discharge. Tumors of nasal cavities, however, tend to be diagnosed earlier than those of the paranasal sinuses because of the earlier presentation of obstructive symptoms and epistaxis.
To further complicate this issue, 9-12% of patients are frequently asymptomatic.[6] These factors contribute to a delay in diagnoses, and, hence, an advanced stage of disease at the time of diagnosis. Patients with unilateral sinonasal symptoms or those that are associated with unilateral facial swelling,

diplopia or blurred vision, unilateral proptosis, and cranial neuropathies should raise a high index of suspicion for sinonasal cancer and warrant urgent evaluation.
Regional and distant metastases are infrequent even in the presence of advanced stage tumors. The incidence of cervical metastases on initial presentation varies from 1-26%, with most large series reporting less than 10%. Distant metastasis on initial presentation is even less common, with most series presenting an incidence of less than 7%.[1] The presence of regional or distant metastases is a poor prognostic sign.
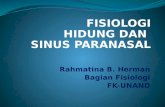
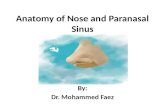
A thorough head and neck examination, cranial nerve assessment, and a nasal endoscopy should be performed in all patients. Physical examination may reveal proptosis, extraocular muscle impairment, mass effect of the cheek, gingival or gingivobuccal sulcus, (eg, ill-fitting dentures) and loose dentition. Numbness or hyperesthesia of the infraorbital (V2) branch of the maxillary nerve strongly suggests malignant invasion (as in the images below).
A nasal cavity tumor has eroded through the hard p
A nasal cavity tumor has eroded through the hard palate and is causing difficulty with fitting a denture.
A nasal tumor that has eroded through the nasal bo
A nasal tumor that has eroded through the nasal bone and causing deformity of the nasal bridge.
Relevant Anatomy
By examining the close relationships of the nasal cavities to the oral cavity, paranasal sinuses, orbit, nasopharynx, pterygomaxillary fissure and pterygopalatine fossa, infratemporal fossa, skull base, and intracranial fossa, one can better understand the myriad signs and symptoms caused by sinonasal tumors.
Local tumor invasion can breach the boundaries of the nasal cavity invading and destroying structures and/or following preformed pathways. The paired nasal cavities are separated by the nasal septum. Their lateral walls comprise the medial wall of the maxillary sinus and the inferior, middle, and superior turbinates. Lateral extension of tumor can infiltrate the maxillary sinus, ethmoid air cells, or even the orbit (through the lamina papyracea). Eventually, orbital involvement manifests as ocular pain, fullness of the eyelid, unilateral epiphora, diplopia, extraocular muscle limitation/diplopia, or proptosis. The floor of the nasal cavity corresponds to the hard palate of the oral cavity; thus, caudal extension of the tumor can present as palatal fullness, pain, and ulceration.
The roof of the nasal cavities is formed by the cribriform plate, which separates the dura of the anterior cranial fossa from the nasal cavity. The cribriform plate, as implied by its name, has multiple openings to

accommodate the passage of olfactory filaments. Tumor can spread to the anterior cranial fossa using these openings or by perineural spread. Violation of this barrier during surgery is likely to produce a cerebrospinal fluid (CSF) leak, increasing the risk for meningitis and intracranial abscess. The nasal cavities open externally via the nares and communicate posteriorly with the nasopharynx via the choanae. The eustachian tubes open into the nasopharynx just behind the infero-lateral aspect of the choanae. Tumor extension into the nasopharynx may cause eustachian tube obstruction and secondary serous otitis media that manifests as hearing loss.
Except in the nasal vestibule, the nasal cavity is lined with pseudostratified columnar ciliated epithelium. The nasal vestibule, which corresponds to the ala of the nose, is lined with squamous epithelium containing vibrissae and sweat and sebaceous glands. A small part of the superior portion of the nasal cavity (bound by the superior turbinate laterally and the nasal septum medially) is lined by olfactory epithelium.
The pterygopalatine and infratemporal fossae are important anatomical considerations, as they are densely populated by the mastication muscles, various sensory and motor nerves, and by the blood vessels that supply the nasal cavity, oral cavity, maxillary teeth, pharynx, and ICAs. Tumor extension into these areas can cause a myriad of symptoms, such as the following:
1. Trismus (involvement of the pterygoid muscles or motor branches of the mandibular division of the trigeminal nerve)
2. Facial hypesthesia (involvement of the infraorbital nerve or other sensory branches from the maxillary and mandibular divisions of the trigeminal nerve)
3. Pain in the maxillary dentition (involvement of the anterior, middle, or posterior superior alveolar nerve branches of the maxillary division of the trigeminal nerve)
4. Severe epistaxis (involvement of the terminal branches of the internal maxillary artery)
The pterygopalatine and infratemporal fossae are also potential routes for intracranial tumor spread, via direct extension or hematogenous spread.
Imaging Studies

Imaging is essential to stage the tumor locally and to rule out the presence of metastases. Computer tomography (CT) scan and magnetic resonance imaging (MRI) have replaced plain radiograms because of the fine anatomical detail provided by these imaging modalities. Each has its own advantages and limitations, but in most cases they are considered complimentary.
CT scan is superior for the evaluation of the bony architecture of the sinonasal tract and skull base. It helps to assess bony erosion or remodeling in critical areas such as the orbital walls, cribriform plate, fovea ethmoidalis, pterygoid plates, pterygopalatine fossa, and the walls of the sinuses. The use of contrast also reveals tumor vascularity and its relationship to the carotid artery. Disadvantages of CT include its inability to differentiate tumor borders from the surrounding soft tissue and the need for ionizing radiation.
MRI is the best modality for defining soft tissue detail. It can differentiate adjacent tumor from soft tissue (eg, gadolinium enhances tumor diffusely to an intermediate degree, whereas inflamed mucosa enhances more intensely in a peripheral fashion), differentiate tumor from secretions in an opacified sinus, demonstrate perineural spread (especially adenoid cystic carcinoma), and demonstrate invasion of the dura, orbit, or brain parenchymal, as seen in the images below.
Coronal MRI T1 with contrast showing an esthesione
Coronal MRI T1 with contrast showing an esthesioneuroblastoma of the right nasal cavity eroding the skull base and invading the brain. The maxillary sinus is filled with edematous mucosa.
Axial MRI T1 with contrast of the same patient in
Axial MRI T1 with contrast of the same patient in Image 4 showing mucus in the right sphenoid sinus due to obstruction of the tumor.
Axial MRI T1 with contrast showing tumor in the le
Axial MRI T1 with contrast showing tumor in the left maxillary sinus with perineural spread in to the left vidian canal.
Other advantages of MRI include the fact that it is less affected by the artifact effect associated with dental fillings and that it requires no exposure to ionizing radiation. MRI, however, is more expensive than CT scan and takes longer to perform, making it more prone to motion artifact. In addition, some patients cannot tolerate the procedure due to claustrophobia. Despite the proliferation of “open MRI centers,” it should be recognized that, at this time, this modality offers an inferior resolution that is invariably inadequate to evaluate tumors of the sinonasal tract. Apparent Diffusion Coefficient (ADC) mapping shows potential as an additional MRI tool to effectively differentiate benign/inflammatory lesions from malignant tumors in the sinonasal area.[7]

Angiography with carotid flow study is not routinely performed and is only reserved for surgical candidates presenting with tumors that surround the carotid artery or when sacrifice of the vessel is anticipated to obtain clear margins.[8] Balloon occlusion test of the ICA, used with SPECT, Xenon CT scan, or transcranial Doppler, offers a reasonable estimate of the risk of ischemic brain infarction if the internal carotid artery is sacrificed. These tests however, cannot predict ischemia at marginal (“watershed”) areas or embolic phenomena.
Metastatic workup should be performed should an extensive resection be considered in a patient with advanced stages, especially those with tumors that have invaded the soft tissues of the face and in tumors with a propensity for hematogenous metastasis, such as sarcomas. This may include CT scans of the neck, chest, and abdomen and bone scan. This extensive work up is necessary should an extensive resection be considered. A CT fused with positron emission tomography (PET/CT) is increasingly being used to evaluate for metastases and for surveillance.
Diagnostic Procedures
Biopsy of the lesion is commonly performed using a rods lens endoscope in the office under topical or local anesthesia. Alternatively, the sampling can be performed in the more controlled environment of an operating room when a deep biopsy is required of if profuse bleeding is anticipated.
Histologic Findings
Below is a brief description of the common types of nasal cavity tumors.
Benign Tumors of Epithelial Origin
Inverted papillomas
Papillomas of the nasal cavity may be classified in 3 distinct categories: inverted, fungiform, and cylindrical. Fungiform papillomas arise from the nasal septum, whereas inverted and cylindrical papillomas typically arise from the lateral nasal wall. Although benign in nature, they can extend beyond their site of origin and destroy bone and recur when incompletely excised. Malignant degeneration can occur in 5-20% of inverted papillomas. They are most commonly diagnosed in white males during the fifth to the seventh decade (mean 50 years).
Complete resection has been the criterion standard for the treatment of these lesions. Traditionally, a lateral rhinotomy with a medial maxillectomy were recommended; however, endoscopic approaches have slowly become the standard treatment. One challenge for the planning of its surgical excision is that the lesion tends to be more extensive than clinical examination suggest. In addition, 12-30% of inverted papillomas are multicentric.[9] Excision with negative margins may be difficult and incomplete

removal invariably leads to recurrence. In most series using traditional approaches, the recurrence rate is 10-30%.
Refinements in endoscopic techniques have lead to a paradigm shift for the resection of inverted papilloma. Endoscopic resection offers the advantage of avoiding incisions and in most patients can be performed as ambulatory surgery. The extent of the procedure is customized accordingly to the extent of the disease, including total ethmoidectomies, wide maxillary antrostomies, sphenoidotomies, frontal recess exploration, and turbinate resection, if required. Once all visible papillomas are removed, any residual tumors are eliminated by drilling over its site of origin. In experienced hands, endoscopic resection has a recurrence rate that is equal to that of traditional techniques.[10, 11] Outcomes using endoscopic techniques compare favorably with that of open approaches.
Long-term endoscopic surveillance and frequent follow-up are crucial, regardless of the surgical technique. Recurrence is usually discovered 12-20 months after surgery but has been reported as late as 30-56 months.[10] In selected cases, endoscopic management is a useful approach with favorable outcomes and less morbidity when compared with more aggressive surgical approaches.[12]
Malignant Tumors of Epithelial Origin
Squamous cell carcinoma
Squamous cell carcinoma (SCC) is the most common malignant tumor in the sinonasal tract and is mostly found in white men in their fifth and sixth decade.[1] It most commonly arises from the lateral nasal wall followed by the nasal septum.[13] Its prognosis is related to extent and location. Those that arise from the nasal vestibule or anterior nasal septum appear to have a poorer prognosis due to its ability to infiltrate the local soft tissues of the face, such as the columella, nasal floor, or upper lip that are associated with a higher risk of regional spread to the neck nodes.[14] Histologic variants such as verrucous carcinoma, basaloid SCC, or carcinosarcoma have been described. However, the extent of disease is a more important prognostic factor than the degree of differentiation.
Treatment of SCC and most other sinonasal malignancies is based on the stage of the disease. In general, early lesions (T1-T2) are treated by either surgery or radiation therapy. Advanced diseases (T3-T4) are treated with multi-modal therapy (surgical extirpation followed by postoperative radiation or chemo-radiation therapy).[13] Elective treatment of the neck is not indicated unless clinically palpable or radiologically evident nodes exist. Nonetheless, elective treatment should be considered if the tumor extends to the soft tissues of the face or infratemporal fossa. Local recurrences occur in 30-40% of cases, while systemic metastasis occurs in 10% of patients. The 3-year and 5-year survival rates of patients with SCC of the nasal cavity were 86% and 69%, respectively.[15]
Adenocarcinoma

Adenocarcinomas (AC) make up 4-8% of all sinonasal tumors. They arise most commonly from the ethmoid sinuses and nasal cavities. Adenocarcinomas have a strong epidemiological association with hardwood dust, which partly explains the preponderance in male patients (75-90%). For reasons that are not well defined, adenocarcinomas are more prevalent in Europe (especially intestinal type), where they comprise the vast majority of paranasal malignancies.
Patterns of tumor growth and histologic differentiation have a broad relationship to their prognosis. Three basic growth forms exist: papillary, sessile, and alveolar mucoid. Papillary tumors are usually most localized and associated with the best prognosis. Sessile tumors have broad surfaces and a greater invasive propensity, resulting in a worse prognosis than the papillary type. Alveolar mucoid type, characterized by abundant mucin in which nests of individual cells reside, is the most aggressive type.
Adenocarcinomas are also divided into low-grade and high-grade according to their histological characteristics. Low-grade tumors are well differentiated with minimal mitotic activity, rarely presenting with perineural invasion or distant metastases. Their tendency is to recur locally. High-grade adenocarcinomas are poorly differentiated with nuclear pleomorphisms, and high number of mitotic activities. Up to one-third of these patients have distant metastases at initial presentation. In one study of 50 cases of sinonasal tract AC (excluding ACC and mucoepidermoid carcinoma), 78% of the 23 patients diagnosed with low-grade ethmoid AC survived with no evidence of disease at a mean follow-up of 6.3 years. Conversely, only 7% of the 27 patients with high-grade lesions had no evidence of disease; 68% of them died of disease within 3 years of initial treatment.[16]
One study evaluated the outcome and prognosis of 44 patients treated for sinonasal adenocarcinoma with endoscopic resection followed by radiotherapy. After 5-year follow-up, the overall survival rate was 63%, the disease-specific survival rate was 82%, and the recurrence-free survival rate was 60%. These results add support to the assertion that endoscopic resection is a valid treatment option to the open resection technique.[17]
The treatment of choice for local control is surgical excision. Postoperative radiotherapy is recommended for patients with positive margins and those with high-grade or advanced staged tumors. Local recurrences are more likely in patients with intracranial involvement. The 5-year disease-specific survival after surgery and postoperative radiation therapy is 55% for T1 and T2, 28% for T3, and 25% for T4 lesions.[18]
The use of topical 5-fluorouracil after surgical resection has been reported with good results.[19, 20] Knegt et al reported a 5-year disease-free survival of 96%, 86%, and 74% at 2, 5, and 10 years on 62 patients treated between 1976 and 1997. Almeyda reported an 86% 5-year disease-free survival on 25 patients. More studies are needed to evaluate the merits of this modality.

Adenoid cystic carcinoma
Adenoid cystic carcinoma is the most common minor salivary gland tumor in the sinonasal tract, accounting for 14-20% of all the adenoid cystic carcinomas arising in the head and neck. Within the sinonasal tract, the maxillary sinus is the most common site of origin followed by the nasal cavities.[21, 22] It is slightly more common among women, and most patients are between 30 and 70 years of age. Lymphatic regional metastases are extremely rare.
Three histological subtypes have been described: cribriform, tubular, and solid. Cribriform pattern is the most common subtype and has the classic "swiss cheese" appearance, whereby the cells are arranged in nests separated by round or oval spaces.[21] The tubular variety has the best prognosis, while the solid type exhibit the worst.
Szanto et al in 1984 describes 3 grades based on the proportion of the above subtypes.[23] Grade I tumors are those comprising of tubular and cribriform patterns without any solid component. Grade II is composed of mostly cribriform pattern having less than 30% solid cellular architecture. Grade III is a tumor with a predominantly solid pattern. Grade I tumors have the best prognosis and grade III tumors the worst. Grade III tumors tend to be larger, recur frequently, and have a higher incidence of perineural invasion.
Adenoid cystic carcinomas are characterized by early spread to neurovascular structures, submucosal spread, and advanced stage at the time of diagnoses. Perineural spread, a hallmark of the disease, typically involve the maxillary, mandibular, and vidian nerves. It can spread retrograde intracranially via the foramen rotundum (V2), foramen ovale (V3), and the vidian or pterygoid canal. It can also spread anterograde from the gasserian ganglion to the infratemporal and pterygopalatine fossa.
Surgical excision and postoperative radiotherapy is the usual treatment of choice for adenoid cystic carcinoma of the sinonasal tract. Getting clear surgical margins is often difficult because of the intricate anatomy of the nasal cavity and skull base; therefore, microscopic disease (positive margins) is present in up to 60% of patients.[22] Postoperative radiotherapy is strongly recommended for positive surgical margins, and for tumors of high-grade and advanced stage. Fast-neutron radiation therapy seems to yield better results than radiation using photons or electrons, resulting in better locoregional control for unresectable or recurrent ACC of the parotid gland. However, the use of this therapy is not widespread due to limited availability. In addition, this advantage does not seem to be as significant for ACC of the sinonasal tract.
Prognostic factors for ACC include tumor site, skull base invasion, stage, histopathologic type, histologic grade, and extent of tumor. The overall 5-year survival rates range from 50-86%.[21, 22] The overall

recurrence rate is 51%-65%. Distant hematogenous spread occurs in 26-40% of cases and determines overall survival.[21] Some developed distant metastases, despite local control at the primary site. Lungs, liver, and bones are the most frequent target organs. The appearance of distant metastases is not necessarily associated with a rapidly fulminating clinical decline. More than 20% of patients with distant metastasis can survive 5 years or longer.[24]
Recurrence may occur 10-20 years after the initial treatment and, hence, long-term follow-up is mandatory. Unlike SCC, survival cures of patients with ACC continue to decline after 5 years.
Sinonasal undifferentiated carcinoma
Sinonasal undifferentiated carcinoma (SNUC) is a rare, aggressive malignancy first described by Frierson et al in 1986.[25] It is characterized by rapid growth, a propensity for early locoregional recurrences, and distant metastases. Men with a median age of approximately 50 years are most commonly affected. The tumor usually arises in the nasal cavities and the great majority of patients present with locally advanced tumors, including involvement of the orbit or anterior cranial fossa.
Histologically, SNUC is made up of small to medium sized pleomorphic cells with a high nuclear-cytoplasmic ratio and high number of mitoses. It is part of the differential diagnosis of other small cell carcinomas such as esthesioneuroblastoma, lymphoma, rhabdomyosarcoma, and melanoma.
Distinguishing these tumors often require electron microscopy or immunohistochemistry. SNUC stains positive for cytokeratin 7, 8, and 19 and neuron-specific enolase.[26] Another important differential diagnosis is nasopharyngeal undifferentiated carcinoma. These 2 entities can be differentiated based on their immunohistochemistry and the presence of Epstein-Barr virus in the tumor tissue (absent in SNUC). Making the distinction is important, as the treatment and prognosis differ significantly. SNUC has a poorer prognosis with a median survival reported to be 18 months.[27]
The overall outcome for SNUC remains poor. An aggressive multimodality approach including surgery (for resectable disease), radiation, and platinum-based chemotherapy offers the best chance for locoregional control and cure. The optimal sequence of multimodality treatment remains unresolved. In patients with unresectable disease, chemoradiation (if performance status permits) or radiation alone can give good palliation.[26] The risk of loco-regional recurrence after treatment is 20-30%, while the risk of distant dissemination is approximately 25-30%.[28]
Olfactory neuroblastoma

Esthesioneuroblastoma (ENB), also known as olfactory neuroblastoma, is a rare tumor arising from the olfactory epithelium in the superior nasal vault. It represents 7-10% of sinonasal malignancies and has a bimodal frequency at 10-20 and 50-60 years of age, with a similar gender distribution.[13]
Microscopically, the tumor is made up of round cells that are characteristically arranged into rosettes, pseudorosettes, or sheets and clusters. It expresses neuroendocrine markers such as neuron-specific enolase (NSE), chromogranin, and synaptophysin, which help to differentiate it from other small cell carcinomas. Hyams described 4 grades of differentiation based on several features such as growth, architecture, mitotic activity, nuclear pleomorphism, etc.[29] Histologic grade of esthesioneuroblastoma seems to correlate with prognosis and impacts its treatment.
The prognosis is mostly related to the extent of disease and resectability on initial presentation. Several staging systems have been described to characterize the extent of ENB. The Kadish staging system was first described in 1976 and remains the most commonly used system. Nonetheless, the UCLA staging by Dulguerov and Calcaterra seems to provide better prognostication since factors such as orbital or extradural invasion are considered separately from intracranial intradural invasion.[30]
Kadish staging system
Stage A tumors are confined to the nasal cavity.
Stage B tumors in the nasal cavity show extension into the paranasal sinuses.
Stage C tumors extend into the orbit, base of skull, cranial cavity or present with cervical or distant metastasis.
UCLA staging system
T1 tumors involve the nasal cavity, paranasal sinuses, or both (excluding sphenoid), sparing the most superior ethmoidal air cells.
T2 tumors involve the nasal cavity, paranasal sinuses, or both (including the sphenoid), with extension to or erosion of the cribriform plate.
T3 tumors extend into the orbit or protrude into the anterior cranial fossa.
T4 tumors involve the brain.
Surgical excision is the treatment of choice. Among the various surgical approaches, an anterior skull base resection (via craniofacial, or endoscopic or endoscopic-assisted approach) is considered the criterion standard. It allows for good oncologic resection with tumor-free margins. Recent improvements in endonasal endoscopic techniques, both extirpative and reconstructive, have allowed their use for the resection of ENB.[31, 32]

Although the extent of resection remains unchanged, the endonasal endoscopic approach spares the patient of the potential sequelae and side effects associated with a traditional craniofacial resection. The addition of postoperative radiation therapy has improved the therapeutic results.[33] The 5-year disease-free survival for all stages is 65% after combined surgery with radiotherapy.
In a large series of 50 patients reported by University of Virginia, the disease-free survival was 86.5% and 82.6% at 5 and 15 years, respectively. Their protocol differs in that they advocate preoperative radiation for Kadish Stage A or B and in that they add neoadjuvant chemotherapy for Kadish Stage C. In their series, 12 patients developed locoregional recurrence; while 5 patients developed distant metastases. The mean time to recurrence was 6 years; thus, the authors stressed the importance of long-term follow-up.[34]
Mucosal melanoma
Melanoma of the head and neck is, in general, a rapidly lethal neoplasm. Although 20% of all melanomas originate in the head and neck, less than 1% arises from the sinonasal tract. They are most commonly found in the nasal cavity followed by the maxillary sinus and oral cavity.[1] Within the nasal cavity, it is often found on the nasal septum or inferior turbinate and spreads submucosally with little erosion of adjacent cartilage and bone. Their pigmentation and clinical appearance varies considerably, ranging from normal pigmentation to being heavily pigmented, and they can be polypoid, exophytic, or ulcerated. The immunostains most commonly used to confirm the diagnosis are S-100 and HMB-45.[35]
Most mucosal melanomas manifest with disease confined to the primary site; however, they are commonly at an "advanced" staged due to their depth of invasion. The possibility of regional or distant metastases must be considered in all cases. One third of all patients have neck metastases, and their presence strongly suggests distant spread. More than half the patients have a local recurrence and often show distant metastases thereafter.[35] Distant metastases are usually rapidly fatal, although some patients achieve long-term control with aggressive salvage surgery for local recurrence.
Survival is primary impacted by advanced T stage and the presence of regional metastases.[36] Other prognostic factors include site (nasal septum has a better prognosis than maxillary sinus and lateral nasal wall), volume, and thickness.[35] However, the overall prognosis and survival rates are poor. The median survival is 19-21 months, and the overall 5-year survival is about 22%.[35, 37] Most patients succumb to the disease within the first 36 months.[37]
Surgical resection with clear margins is the treatment of choice. Currently, no effective therapy for sinonasal mucosal melanoma exists, and the prognosis remains grim regardless of treatment modality. The incidence of local recurrence is high, even with fresh frozen section to ensure complete excision. The aim of radiotherapy is to improve locoregional control,[38] but some studies have failed to show

any improvement in local control or overall survival.[35, 37] Nevertheless, both surgery alone and surgery combined with postoperative irradiation are superior to radiation therapy alone.[35] Adjuvant therapies such as systemic interferons and vaccines are under investigations.
Malignant Nonepithelial Tumors
Although the metastatic potential and oncologic outcome of sarcomas arising in the sinonasal tract is variable among the different histologic types, the local behavior of sarcomas is similar. Sarcomas infiltrate and advance further than what the naked eye or imaging can appreciate. This often leads to an inadequate resection and subsequently to a local recurrence. Wide excision is necessary to improve the local control, but this may be difficult to achieve due to the proximity of vital structures to the sinonasal.
Neurogenic sarcomas
Neurogenic sarcomas are rare in the head and neck and are most commonly associated with neurofibromatosis. They are locally aggressive and frequently present with distant metastases. Surgical resection is the mainstay treatment with radiation and chemotherapy reserved for incomplete removal, inoperable cases, or recurrences.[39] The 5-year survival rate is around 60%. Those associated with neurofibromatosis have the poorest prognosis, with a 5-year survival rate around 30%.[39]
Rhabdomyosarcoma
Rhabdomyosarcomas involve the head and neck region in 35-45% of cases. The sinonasal tract is involved in 10% of cases, affecting the head and neck.[40] Histologically, they are classified into 5 major categories: embryonal (most common), alveolar, botryoid embryonal, spindle cell embryonal, and anaplastic. The embryonal and alveolar varieties are more common in children and young adults, while the anaplastic type is more common in adults. Rhabdomyosarcomas in adults have a less favorable outcome, with a 5-year survival rate of only 35%.[41]
Rhabdomyosarcomas of the sinonasal tract are classified as nonorbital parameningeal and behave more aggressively than those arising in other locations. Systemic and regional metastases are common. Treatment includes a multimodality approach involving a combination of chemotherapy, radiation, and surgery.[42]
For early superficial nonorbital lesions, wide excision is recommended, provided that function and cosmesis can be preserved. This is often difficult because of the anatomic constraints in the head and neck region. The Intergroup Rhabdomyosarcoma Studies IV showed that aggressive surgical management is not necessary. A successful treatment for the large majority of patients with localized parameningeal sarcoma can be achieved with intensive chemotherapy and radiation.[43] Conversely,

adults are usually treated by wide surgical excision. Radiation is recommended for positive margins or inoperable or recurrent disease. Chemotherapy only has a palliative role.
Fibrosarcoma
Fibrosarcoma is a tumor arising from fibroblast and has a spectrum that ranges from low-grade to higher-grade tumors. Radiation and trauma have been implicated as possible etiologic factors. The treatment of choice is wide surgical excision for previously untreated tumors. Radiation is recommended for involved margins or recurrent or inoperable tumors.
Chondrosarcoma
Chondrosarcomas are slow-growing tumors that arise from cartilaginous structures. Approximately 5-10% are located in the head and neck, mostly in the maxilla and mandible. These tumors are graded from I to III on the basis of the rate of mitoses, cellularity, and nuclear size. The size of the tumor and grading correlate with the local aggressiveness, rate of metastasis, and ultimate survival. Surgical removal with wide margins is the treatment of choice. Gross total removal with postoperative radiation is recommended for those involving vital structures and for those exhibiting a high histological grade.
Hemangiopericytoma
Hemangiopericytomas are rare perivascular tumors with variable malignant potential. They arise from the pericytes of Zimmerman in the walls of capillaries. Vascular pericytes are of mesenchymal origin that spiral around capillaries and postcapillary venules. They are believed to be capable of differentiating into smooth muscle cells. They possess contractile properties and are able to modify the lumen of blood vessels to regulate blood flow.
Hemangiopericytoma invade locally and metastasize in 10-15% of cases. Sixteen percent are found in the head and neck, with about 50 reported cases arising in the sinonasal tract.[44] The primary treatment is surgical excision. Life-long follow-up is required to evaluate local recurrence and late metastases.
Lymphoma
Lymphoma of the sinonasal tract accounts for 5.8-8% of the extranodal lymphomas in the head and neck area. Although rare, they are still the most common nonepithelial malignant tumors of the nose. It is a disease of the very young or the aging adult. With advances in immunochemistry, they are classified according to the cell of origin into B-cell, T cell, or NK-T cell lymphomas.[45]

The T/NK-cell lymphoma T-cell lymphomas are typically found in the nasal cavity and are more common in Asian and South American countries. Patients present at a younger age. These lymphomas have an aggressive, angioinvasive growth pattern that result in necrosis and bony erosion. It has been termed in the past as midline lethal granuloma, which is a progressive, destructive lesions affecting the midline of the face. With advancement in immunohistochemistry, they have been determined to be of T-cell or natural killer (NK) origin. T/NK-T-cell sinonasal lymphomas are associated with Epstein-Barr virus infection. It is postulated that once EBV infection occur, the NK /T cell are activated and recruited to the nasal mucosa. A single clone of T or NK cell, influenced by other possible molecular accidents, continues to proliferate and ultimately leads to NK/T cell lymphoma.
By contrast, B-cell lymphomas are typically located in the paranasal sinuses and have a slight predominance in Western countries. They are believed to arise from sinonasal mucosa–associated lymphoid tissue (MALT) that resides in the subepithelium. MALT contains specialized clusters of lymphocytes next to mucosal surfaces. It is characterized by a chronic inflammatory infiltrate.
Clinically, NK/T-cell lymphomas can be distinguished from B-cell lymphomas by location (as mentioned above) and appearance. NK/T-cell lymphomas often cause severe destruction of the nasal septum and midline facial structures. They are characterized by unrelenting ulceration and necrosis. The tumor cells frequently infiltrate and destroy blood vessels, causing ischemic necrosis. Conversely, B-cell lymphomas tend to surround, but not invade, blood vessels. Extensive necrosis and ulceration are extremely rare.
The treatment includes radiation therapy for localized lesions and chemotherapy for systemic involvement or to prevent systemic recurrence. A good response is achieved with local radiotherapy alone, often with complete tumor regression. However, the incidence of metastasis and local recurrence is high (up to 49%). With the addition of chemotherapy, such as cyclophosphamide, hydroxydaunomycin, Oncovin, and prednisone (CHOP), a reduction in recurrence and metastasis and improved survival rates are observed. Patients treated with chemotherapy alone have a higher risk of local recurrence. Bone marrow transplant in a few patients that were refractory to the combined treatment yielded mixed results. For high-grade aggressive lymphomas, the central nervous system is at risk for tumor involvement. The current recommendation is to radiate the CNS only if disease involvement is documented by lumbar puncture and MRI, not prophylactic ally.
The 5-year overall survival rate for all subtypes is 52%. A younger age, early stage of disease, and the use of combination chemoradiotherapy correlate with a better prognosis. Although univariate analyses demonstrate that T-cell lymphomas are associated with a lower cure rate, a higher relapse rate, and a worse overall survival rate, tumor immunophenotype is not an independent prognostic factor based on multivariate analyses.
Extramedullary plasmacytoma

Extramedullary plasmacytoma refers to a malignant plasma celltumor growing outside the bone marrow. They involve the head and neck region in 80-90% of the cases, and around 40% of them arise in the sinonasal tract. They are more common in the sixth to seventh decades. Extramedullary plasmacytomas tend to spread locally, and can be found in the cervical nodes in less than 25% of the cases. Most of these lesions respond to radiation therapy in doses of 4000-5000 cGy administered over 4-5 weeks.
Metastatic Tumors
Metastatic tumors to the sinonasal tract produce symptoms similar to those of primary tumors. The most common sources are the kidneys, breasts, and lungs. Maxillary sinus is the most frequent site affected by metastases followed by ethmoid, frontal, and sphenoid sinus in descending order. Their treatment is palliative, using radiation, surgery, or chemotherapy to relieve obstructive and compressive symptoms or pain.
Staging
Staging of nasal cavity and paranasal sinus carcinomas is not as well established as for other head and neck tumors. For cancer of the nasal cavity and the ethmoid sinus, the American Joint Committee on Cancer (AJCC) has designated a staging system using the TNM classification.[46] This staging system differentiates resectable (T4a) from unresectable (T4b) tumors by recognizing recent surgical advances and limitations, as follows:
TX: Primary tumor cannot be assessed
T0: No evidence of primary tumor
Tis: Carcinoma in situ
T1: Tumor restricted to any one subsite, with or without bony invasion
T2: Tumor invading two subsites in a single region or extending to involve an adjacent region within the nasoethmoidal complex, with or without bony invasion
T3: Tumor extends to invade the medial wall or floor of the orbit, maxillary sinus, palate, or cribriform plate
T4a: Tumor invades any of the following: anterior orbital contents, skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid or frontal sinuses
T4b: Tumor invades any of the following: orbital apex, dura, brain, middle cranial fossa, cranial nerves other than (V2), nasopharynx, or clivus
The AJCC also recommends a different system for soft-tissue sarcomas. This system includes a histologic grading system that differs from the system used for epithelial tumors. Grading is considered the most

significant prognostic factor in patients with mesenchymal tumors and is based on the number of mitoses, degree of cellularity, amount of stroma, degree of maturation, nuclear pleomorphism, and presence or absence of necrosis.
Medical Therapy
Surgery is the mainstay of treatment for most sinonasal tumors. Radiation as the sole modality of treatment is recommended for unresectable cases, poor surgical candidates, or for lymphoreticular tumors. Combination therapy of surgery and adjuvant radiotherapy with or without chemotherapy is given in situations with an advanced tumor (T3 and T4), positive surgical margins, perineural spread, perivascular invasion, cervical lymphatic metastasis, and in recurrent tumors. Chemotherapy may also have a palliative role for cytoreduction.
Radiation therapy
Radiation may be used as a single modality, as an adjunct to surgery, or as palliative therapy. It is the primary treatment for lymphoreticular tumors and in patients who are poor surgical candidates, refuse surgical treatment, or have tumors that are deemed inoperable. As an adjunct to surgery, it can be given preoperatively or postoperatively with similar oncological results. Preoperative radiation is given in cases of bulky tumor to help decrease the tumor volume that would have resulted in severe cosmetic and functional morbidity with resection. We favor giving radiation therapy after surgery, as a smaller volume of tumor cells exist, the margins of the non-radiated tumor can be better defined during surgery, and the postoperative wound healing is more predictable.
Chemotherapy
The role of chemotherapy for the treatment of tumors of the sinonasal tract is usually adjunctive to radiotherapy (radiosensitizer) or palliative, using its cytoreductive effect to relieve pain, obstruction, or to debulk a massive external lesion. It is increasingly being given concurrently with radiation and used in patients at high risk of recurrence, such as those with positive margins after resection, perineural spread, or extracapsular spread in regional metastases.