THE UTERINE CORPUS Emad Raddaoui, MD, FCAP, FASC Hala Kfoury, FRCPA, KSUF 1.
Upload
randolf-mitchell-murphyCategory
view
224download
4
PARAPROTEINEMIAS
Sheikha

ProfessorAnwar SheikhaAnwar Sheikha
MD, FRCP, FRCPath., FCAP, FRCPA, FRCPI, FACP
Senior Consultant Clinical & Lab. Hematologist
Clinical Professor of HematologyUniversity of Mississippi Medical Center, Jackson,
Mississippi
Professor of Hematology, University of Salahaddin, Erbil, Kurdistan,
IRAQ

Sheikha
PARAPROTEINEMIAS

Sheikha
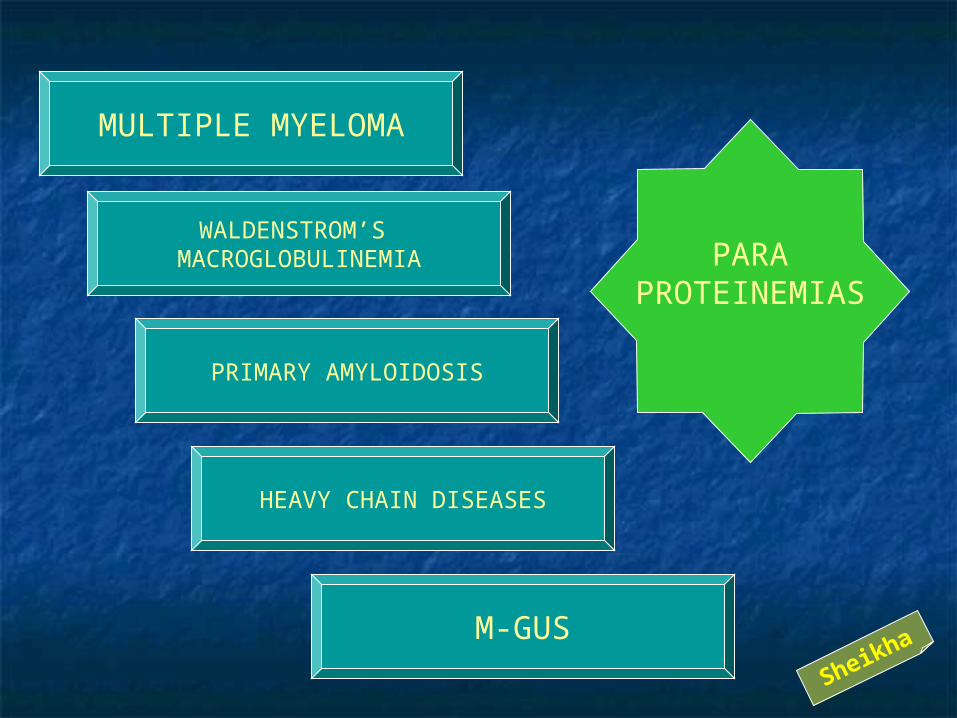
MULTIPLE MYELOMA
WALDENSTROM’S MACROGLOBULINEMIA
PRIMARY AMYLOIDOSIS
HEAVY CHAIN DISEASES
M-GUS
PARAPROTEINEMIAS
Sheikha
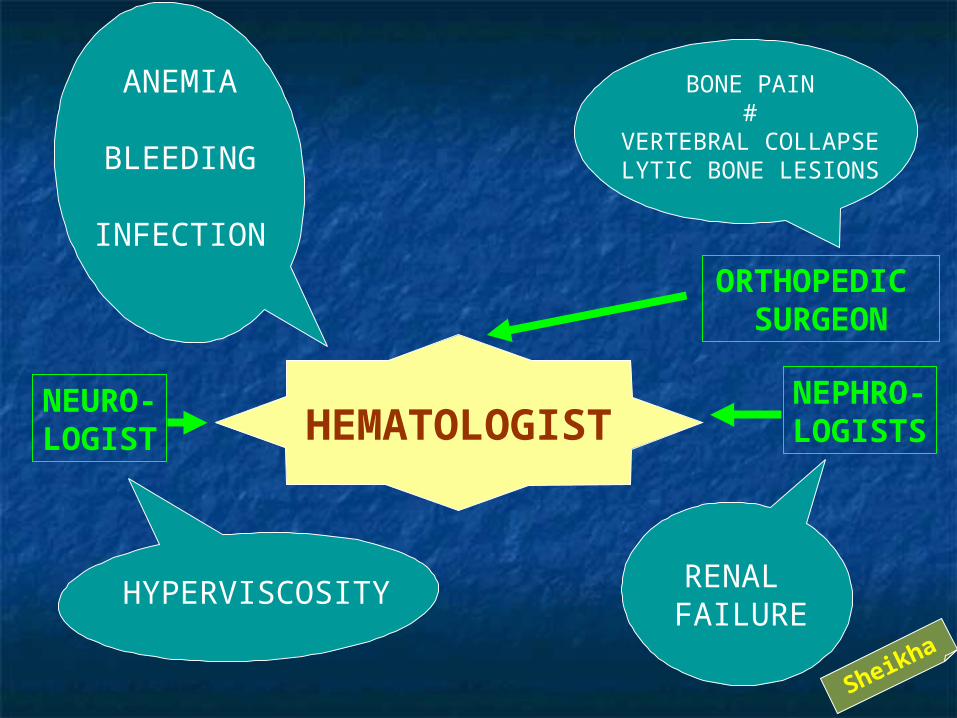
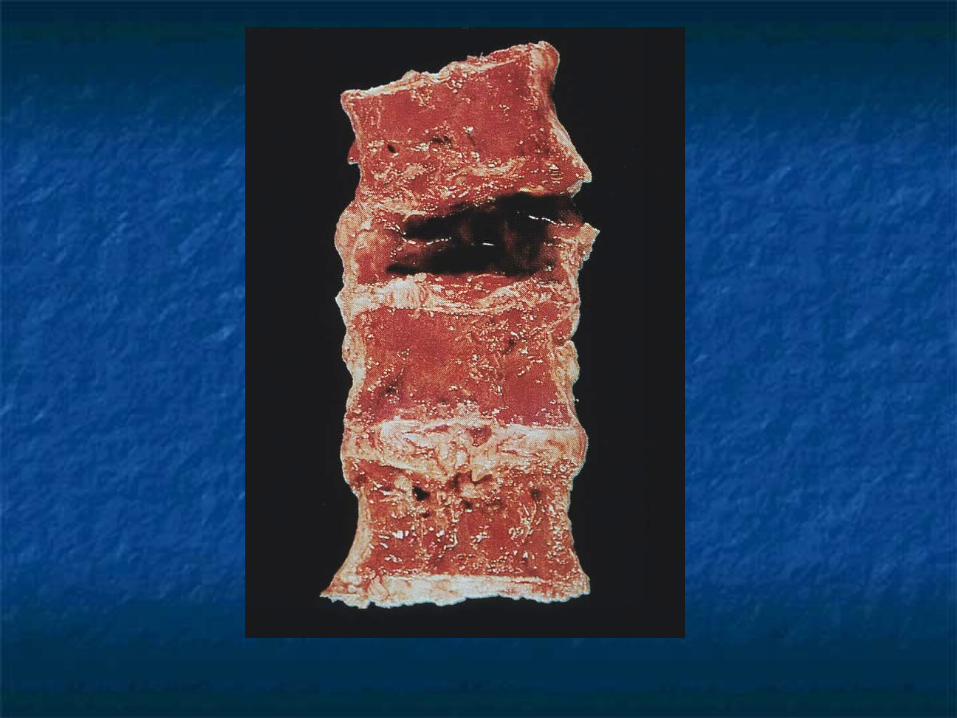
BONE PAIN#
VERTEBRAL COLLAPSELYTIC BONE LESIONS
ANEMIA
BLEEDING
INFECTION
HYPERVISCOSITY RENAL FAILURE
NEPHRO-LOGISTS
NEURO-LOGIST
ORTHOPEDIC SURGEON
HEMATOLOGIST
Sheikha

MULTIPLEMYELOMAMULTIPLEMYELOMA
1% of All Cancers 2% of All Cancer Deaths
Average Age ~ 65 Black: White = 2:1

PARAPROTEINPRODUCTION
OSTEOLYTICBONE LESIONS
BONE MARROWINFILTRATION
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

BONE MARROWINFILTRATION
PANCYTOPENIA
↓ PLATELET
↓ WBC ANEMIA
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

BONE MARROWINFILTRATION
PANCYTOPENIA
↓ PLATELET
↓ WBC ANEMIA
BLEEDING
INFECTION
IMMUNESUPPRESSION MULTIPLE
MYELOMA
MULTIPLEMYELOMA
Sheikha

BONE MARROWINFILTRATION
PANCYTOPENIA↓ WBC
INFECTION
IMMUNESUPPRESSION
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Chemotherapy myelosuppression
Steroid immunosuppression
Sheikha

OSTEOLYTICBONE LESIONS
BONE PAIN
VERTEBRALCOLLAPSE
BONE
#
↑ Ca++ RENAL FAILURE
ANEMIAMULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha
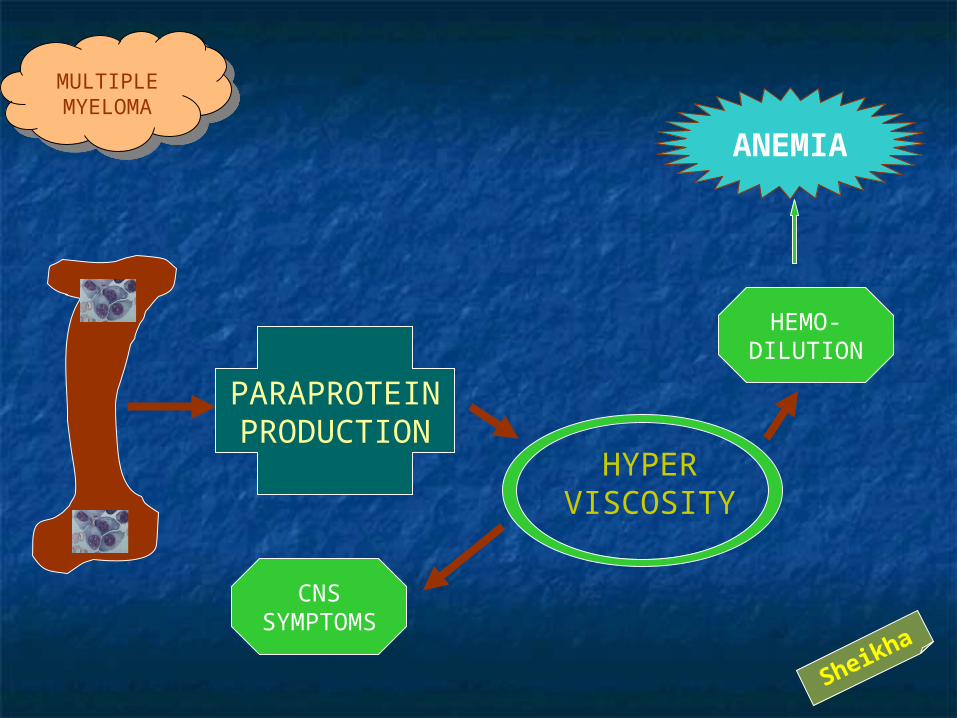
PARAPROTEINPRODUCTION
ANEMIA
HYPERVISCOSITY
CNSSYMPTOMS
HEMO-DILUTION
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

PARAPROTEINPRODUCTION
BLEEDING
INTERFERENCEWITH CLOTTING
FACTORS
COATING OFPLATELETS
ANEMIA
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha
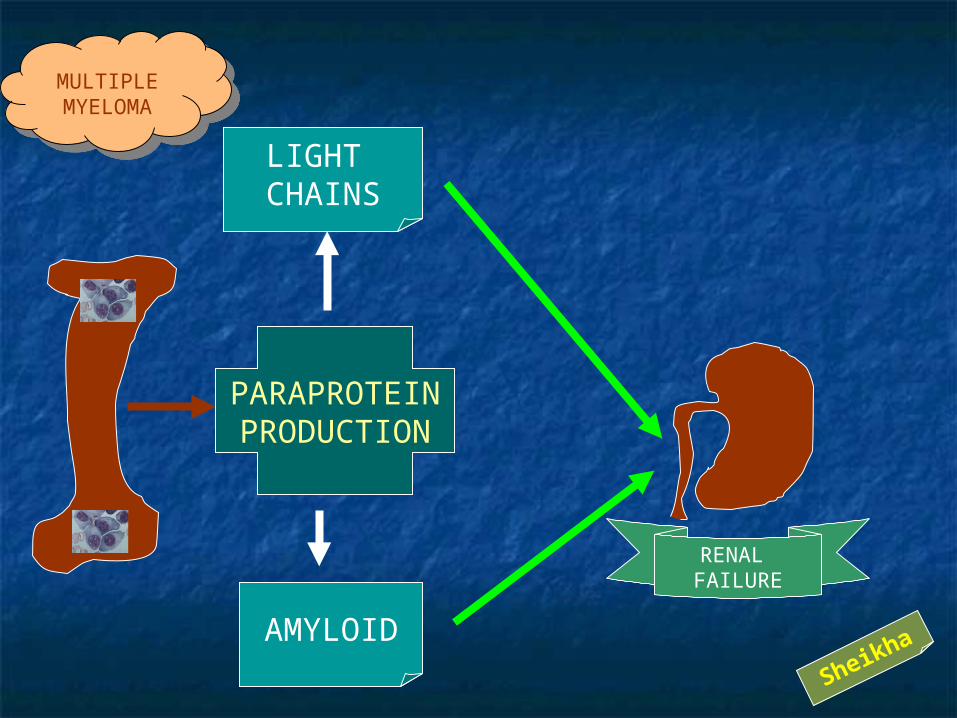
PARAPROTEINPRODUCTION
RENAL FAILURE
AMYLOID
LIGHT CHAINS
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

RENAL FAILURE
AMYLOID
LIGHT CHAINS
?RENALFAILUREINFECTION PYELONEPHRITIS
↑ Ca++
MULTIPLEMYELOMA
MULTIPLEMYELOMA Sheikha
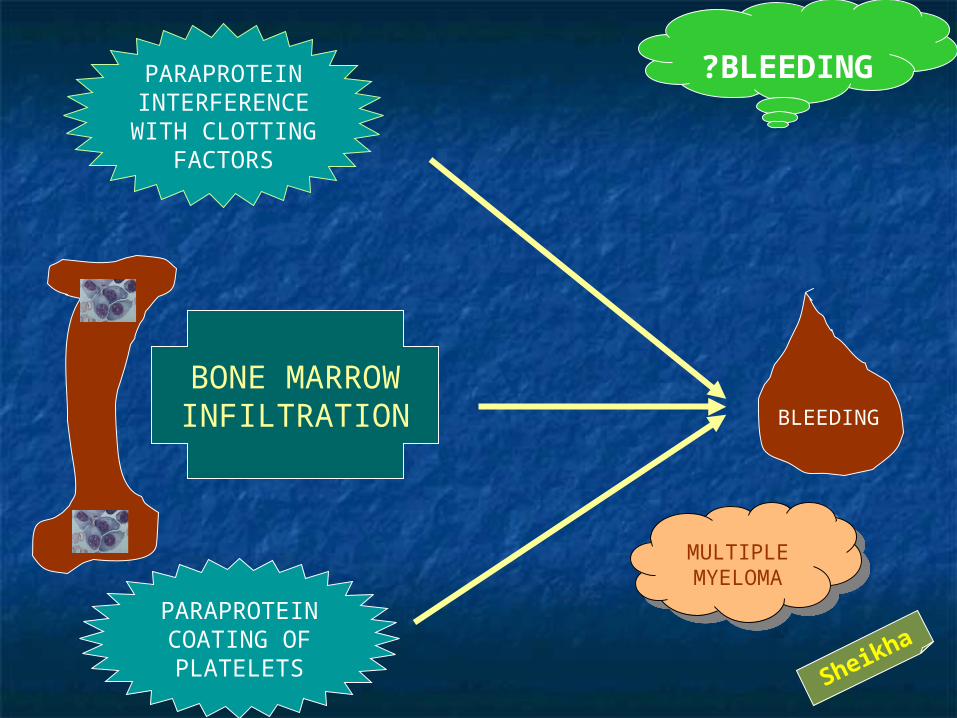
PARAPROTEININTERFERENCEWITH CLOTTING
FACTORS
PARAPROTEINCOATING OFPLATELETS
?BLEEDING
BONE MARROWINFILTRATION BLEEDING
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

RENAL FAILURE
?ANEMIA
BONE MARROWINFILTRATION
BLEEDING
HEMO-DILUTION
MULTIPLEMYELOMA
MULTIPLEMYELOMA
Sheikha

PARAPROTEINPRODUCTION
OSTEOLYTICBONE LESIONS
BONE MARROWINFILTRATION
MULTIPLEMYELOMA
MULTIPLEMYELOMAANEMIA
BLEEDINGINFECTION
RENALFAILURE
HYPER-VISCOSITY
↑ Ca++
BONE PAIN,# & VERT.COLLAPSE
Sheikha

Sheikha
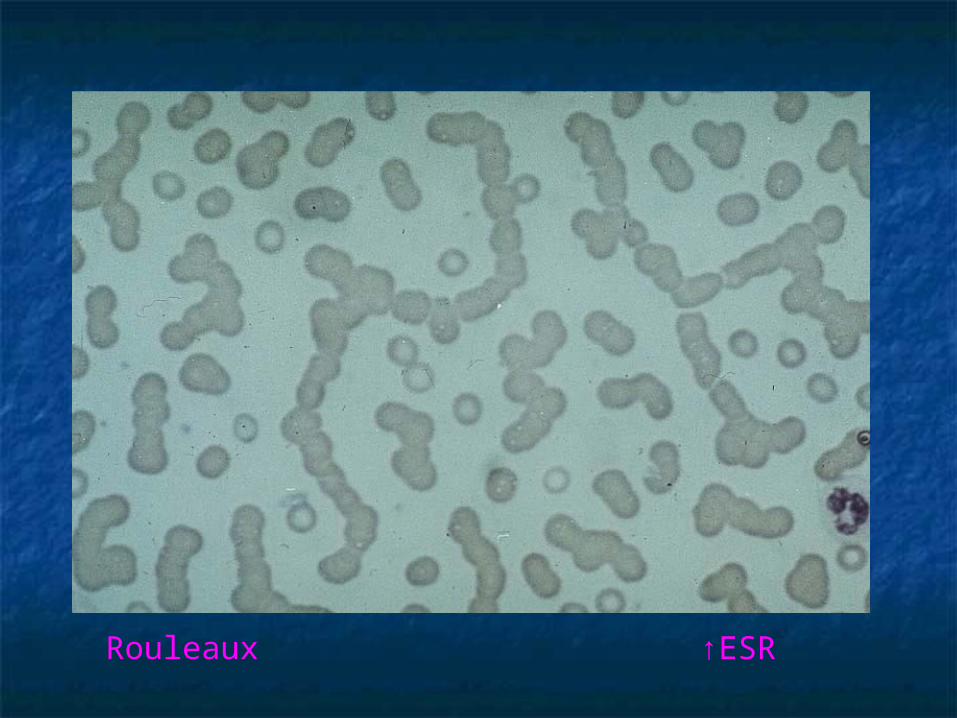
Rouleaux ↑ESR
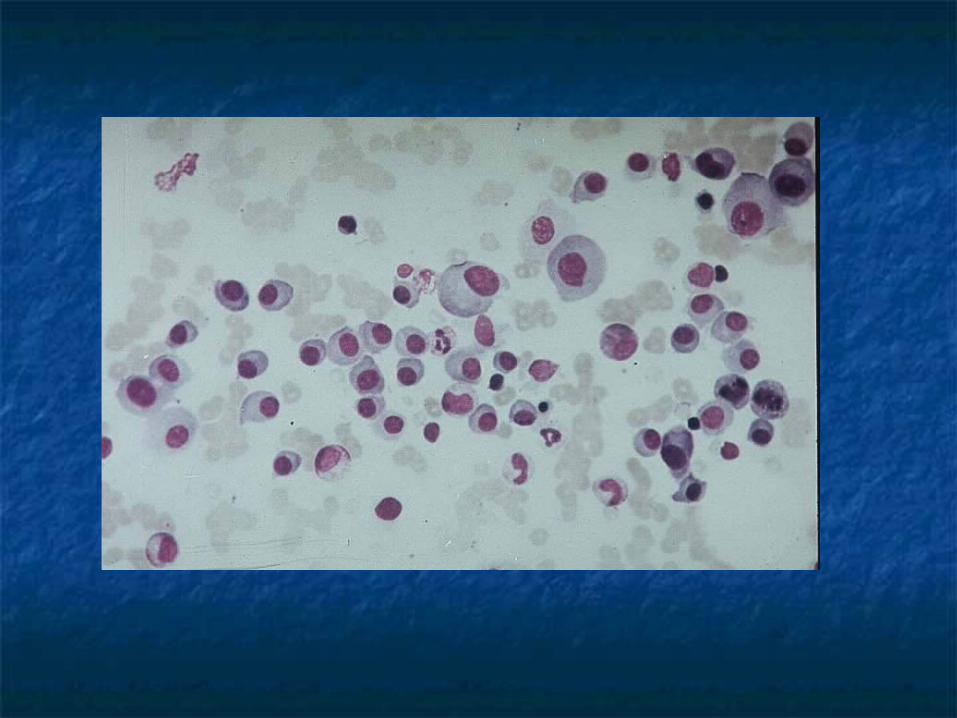
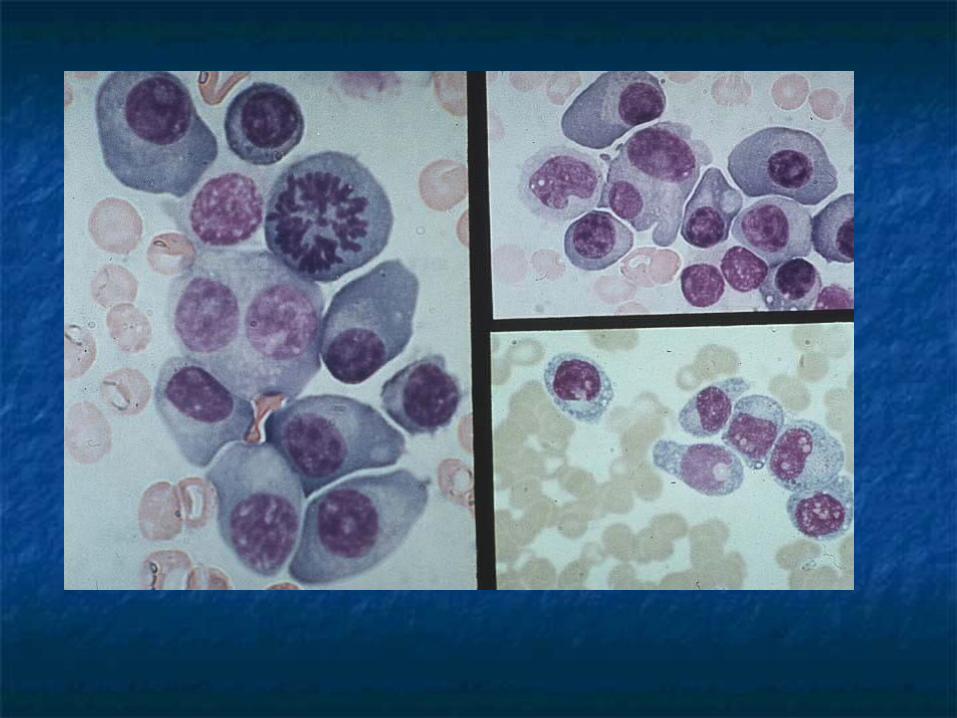

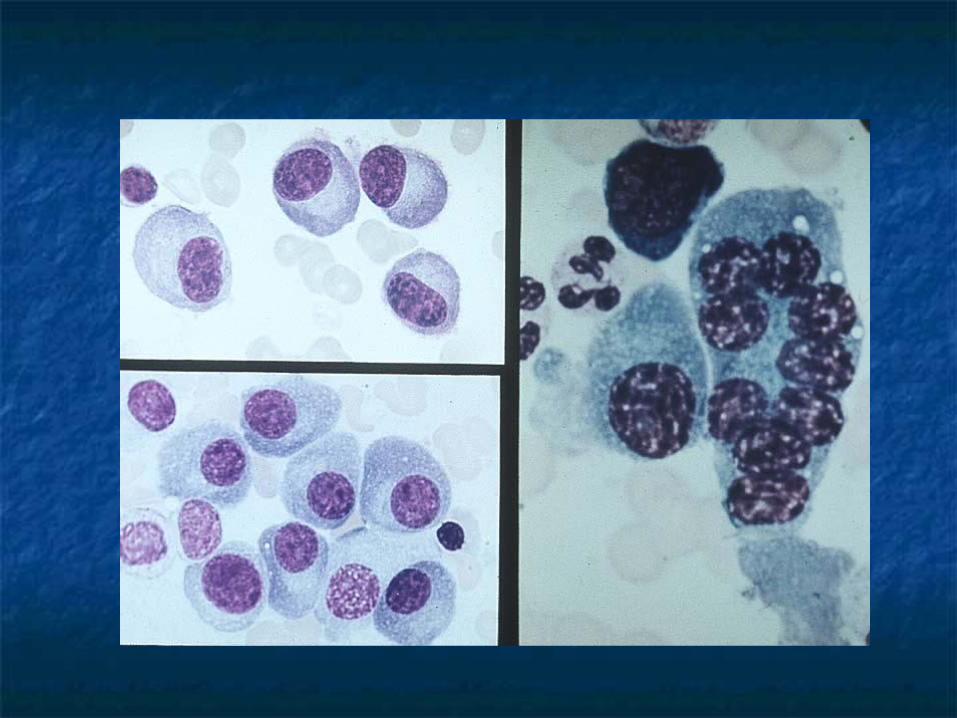
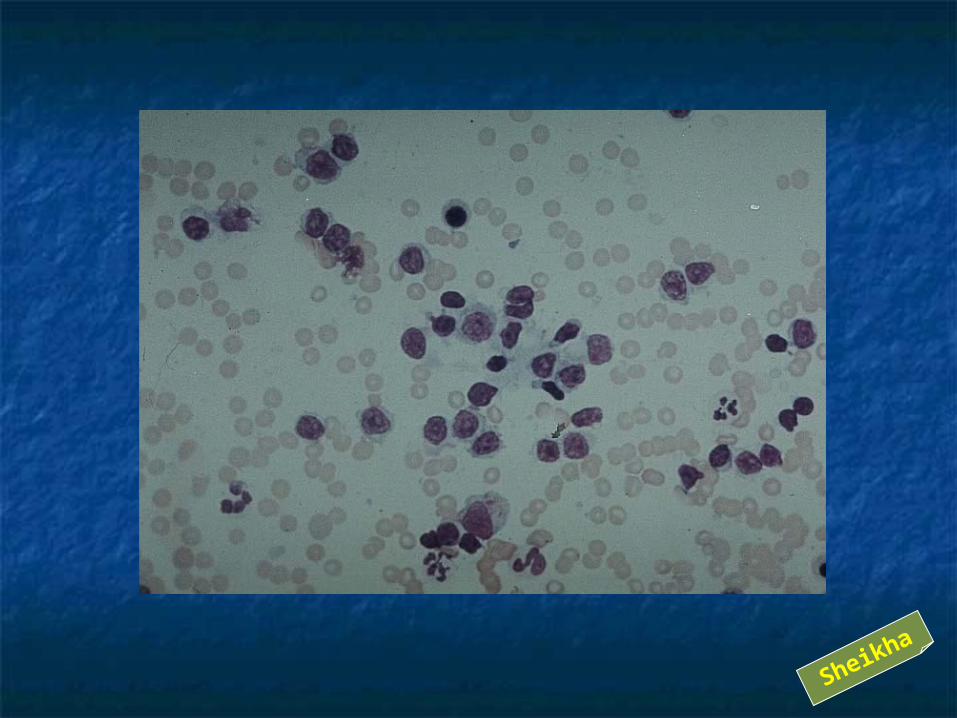
The cytoplasm of Myeloma Cells contains abundant Endoplasmic Reticulum (ER) , which may contain retained, condensed or crystallised cytoplasmic Ig producinga variety of morphologically distinctive findings, including:
Multiple pale bluish-white, grape-like accumulation Mott or Morula Cells
Cherry-red refractive round bodies Russell Bodies
Vermilion staining glycogen-rich IgA Flame Cells
Overstuffed fibrils Gaucher-like cells; thesaurocytes
&
Crystalline Rods
THESE CHANGES ARE NOT PATHOGNOMONIC FOR MM SINCE THEY MAY BE FOUND IN REACTIVE PLASMA CELLS


MULTIPLE MYELOMA
IgG>50%
IgA25%
LightChain20%
IgDrare
Non-Secretory
Bi-clonal
?IgM
Sheikha

NORAMAL

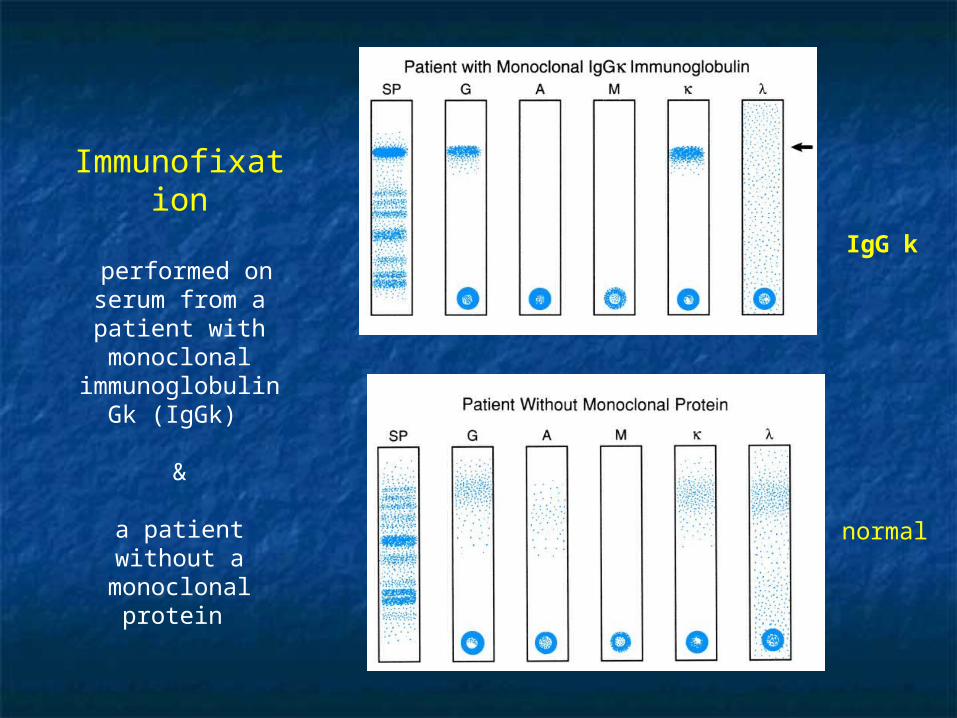
Immunofixation
performed on serum from a patient with monoclonal
immunoglobulin Gk (IgGk)
&
a patient without a monoclonal
protein
normal
IgG k




Sheikha

Sheikha

PLASMA CELLS OSTEOCLASTS
OAF(IL-1/ TNF)
PDGF/ IL-6
BMSC“Bone Marrow Stromal Cells”
IL- 6
Sheikha
Sheikha
صدامحرس
الجمهوري
Sheikha

Sheikha

PC
Osteoclasts
Sheikha

Interleukin-6-mediated myeloma cell growth
BMSC: bone marrow stromal cell IL: interleukin NF: nuclear factor TGF: transforming growth factor
MM rely on contact with BM Stromal Cells “BMSC”Adhesive interaction between MM cells & BMSC induce cells to secrete IL-6which then acts a paracrine growth factor promoting survival of MM cells &
inhibiting apoptosis

OAF
IL-1 β
TGF- β
OtherCytokines
Osteoclast Activation
Osteoblast Suppression
OSTEO-LYTICBONE
LESIONS




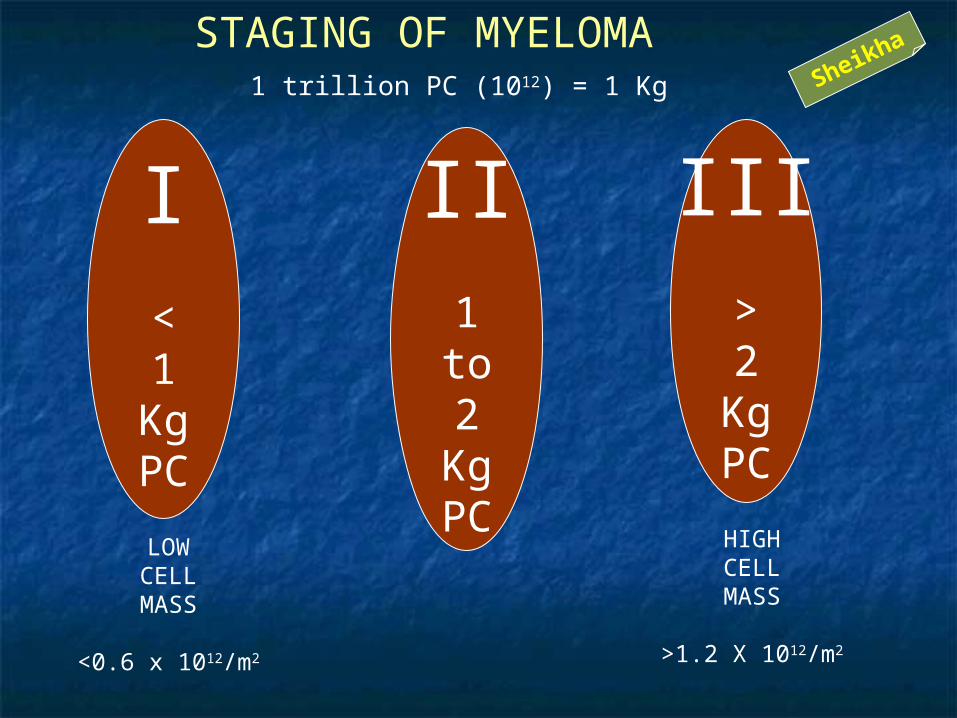
I<1
KgPC
II1to2
KgPC
III>2
KgPC
1 trillion PC (1012) = 1 Kg
LOWCELLMASS
<0.6 x 1012/m2
HIGHCELLMASS
>1.2 X 1012/m2
STAGING OF MYELOMASheikha

Stage II Overall data
minimally abnormal as shown
for stage I and no Single value
abnormal as defined
For stage III
Stage IAll of the following:
Hemoglobin value >10 g/dL
Serum calcium value normal(<12 mg/dL)
On roentgenogram, normal bone structure (scale) or solitary bone plasmacytoma only
Low monoclonal component production rates
IgG value <50 g/L
IgA value <30 g/L
Urine light chain monoclonal component onelectrophoresis <4 g/24 h
Durie-Salmon Myeloma Staging System
Stage IIIone or more of the following:
Hemoglobin value <8.5 g/L
Serum Ca value >12 mg/dL
Advanced lytic bone lesions (scale 3)
High monoclonal component production rates
IgG value >70 g/L
IgA value >50 g/L
Urine light chain monoclonal component on electrophoresis >12 g/24 h
Subclassification:
a: Relatively normal renal function (serum creatinine value <2.0 mg/dL)
b: Abnormal renal function (serum creatinine >2.0 mg/dL)
Sheikha

Stage II Overall data
minimally abnormal as shown
for stage I and no Single value
abnormal as defined
For stage III
Stage IAll of the following:
Hemoglobin value >10 g/dL
Serum calcium value normal(<12 mg/dL)
On roentgenogram, normal bone structure (scale) or solitary bone plasmacytoma only
Low monoclonal component production rates
IgG value <5 g/dL
IgA value <3 g/dL
Urine light chain monoclonal component onelectrophoresis <4 g/24 h
Durie-Salmon Myeloma Staging System
Stage IIIone or more of the following:
Hemoglobin value <8.5 g/L
Serum Ca value >12 mg/dL
Advanced lytic bone lesions (scale 3)
High monoclonal component production rates
IgG value >7 g/dL
IgA value >5 g/dL
Urine light chain monoclonal component on electrophoresis >12 g/24 h
Subclassification:a: Relatively normal renal function (serum creatinine value <2.0 mg/dL)
b: Abnormal renal function (serum creatinine >2.0 mg/dL)
<1
KgPC
1to2
KgPC
>2
KgPC
Sheikha

Criteria for Diagnosis of Multiple Myeloma
Major criteria
1. Plasmacytomas on tissue biopsy
2. Bone marrow plasmacytosis (>30% plasma cells)
3. Monoclonal immunoglobulin spike on serum electrophoresis: IgG >35 g/L or IgA >20 g/L; or light-chain excretion >1.0 g/d on 24-h urine protein electrophoresis
Minor criteria
a. Bone marrow plasmacytosis (10-30% plasma cells)
b. Monoclonal immunoglobulin spike present but of lesser magnitude than in 3
c. Lytic bone lesions
d. Normal IgM <0.50 g/L, IgA <1.00 g/L, or IgG <6.00 g/L
Any of the following sets of criteria will confirm the diagnosis:
Any two major criteria
Major criterion 1 plus minor criterion b, c, or d
Major criterion 3 plus minor criterion a or c
Minor criteria a, b, and c or a, b, and dSheikha

g/L mg/dLIgM 0.5 – 1.5 50 - 150
IgA 1.5 – 5.0 150 - 500
IgG 5.0 – 15.0 500-1500
Normal Ig Values
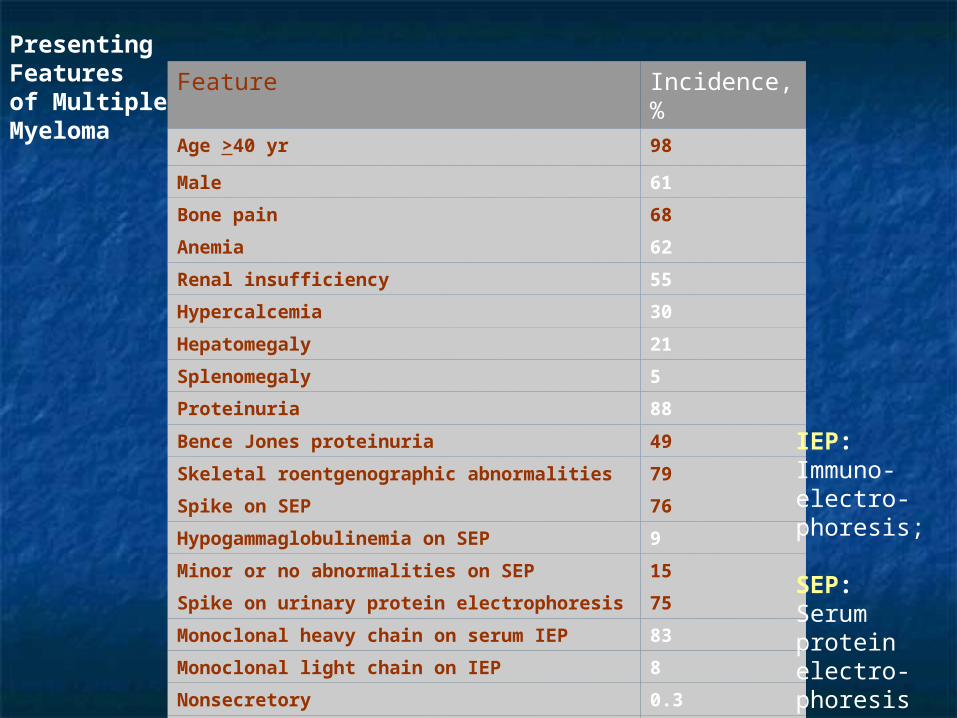
Feature Incidence, %Age >40 yr 98
Male 61
Bone pain 68
Anemia 62
Renal insufficiency 55
Hypercalcemia 30
Hepatomegaly 21
Splenomegaly 5
Proteinuria 88
Bence Jones proteinuria 49
Skeletal roentgenographic abnormalities 79
Spike on SEP 76
Hypogammaglobulinemia on SEP 9
Minor or no abnormalities on SEP 15
Spike on urinary protein electrophoresis 75
Monoclonal heavy chain on serum IEP 83
Monoclonal light chain on IEP 8
Nonsecretory 0.3
Amyloidosis 7
Presenting Features of Multiple Myeloma
IEP:Immuno-electro-phoresis;
SEP: Serumprotein electro-phoresis

Frequency of Different Types of Monoclonal Proteins Produced By Plasma Cell Tumors
Monoclonal Protein Frequency, %
IgG 52
IgA 21
IgD 2
IgE <0.01
IgM (Waldenström's) 12
Light chain only 11
Heavy chain only <1
2 or more 0.5
None detected 1
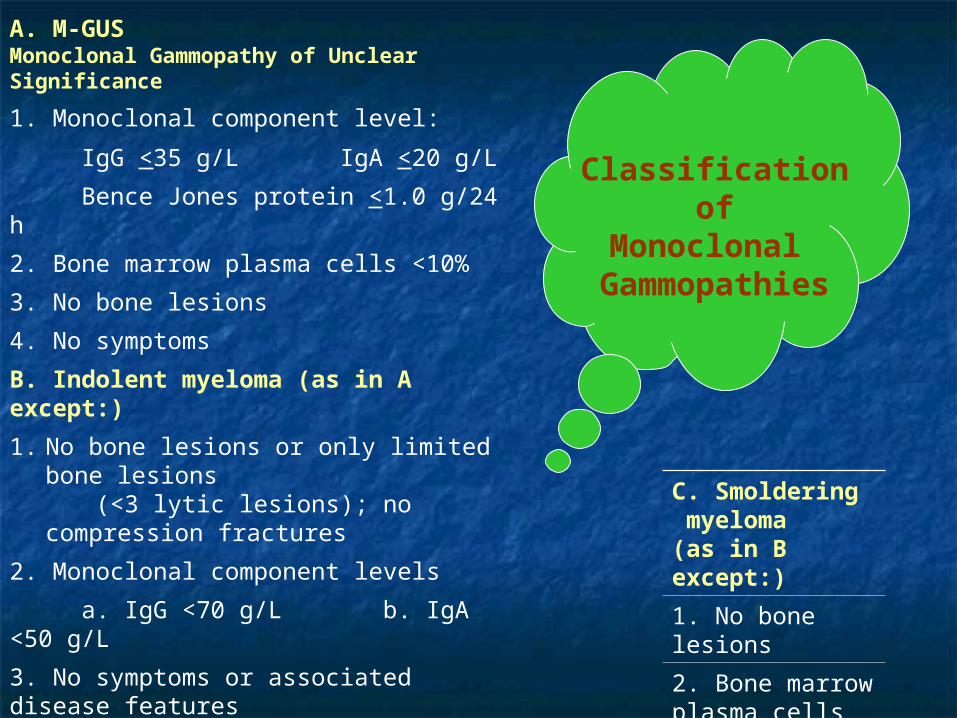
A. M-GUSMonoclonal Gammopathy of Unclear Significance
1. Monoclonal component level:
IgG <35 g/L IgA <20 g/L
Bence Jones protein <1.0 g/24 h
2. Bone marrow plasma cells <10%
3. No bone lesions
4. No symptoms
B. Indolent myeloma (as in A except:)
1. No bone lesions or only limited bone lesions (<3 lytic lesions); no compression fractures
2. Monoclonal component levels
a. IgG <70 g/L b. IgA <50 g/L
3. No symptoms or associated disease features
a. Performance status >70%
b. Hemoglobin >10 g/dL
c. Serum calcium normal
d. Serum creatinine <2.0 mg/dL
e. No infections
C. Smoldering myeloma (as in B except:)
1. No bone lesions
2. Bone marrow plasma cells <30%
Classification of
Monoclonal Gammopathies
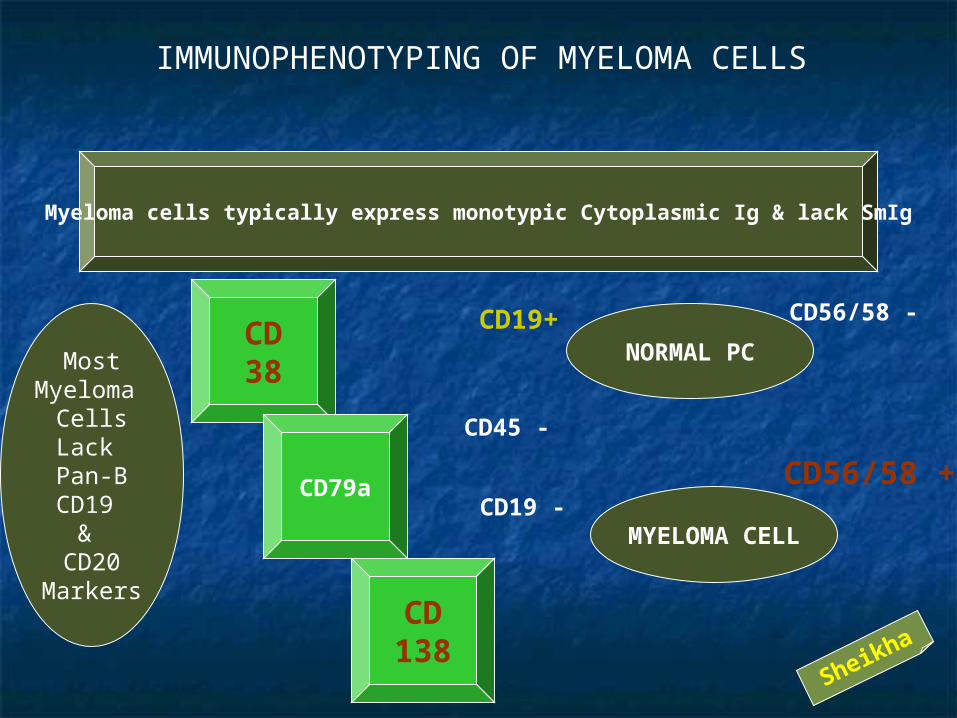
IMMUNOPHENOTYPING OF MYELOMA CELLS
Sheikha
Myeloma cells typically express monotypic Cytoplasmic Ig & lack SmIg
MostMyeloma
CellsLack Pan-BCD19
& CD20
Markers
CD38
CD79a
NORMAL PC
MYELOMA CELL
CD19+
CD19 -
CD56/58 -
CD56/58 +
CD138
CD45 -
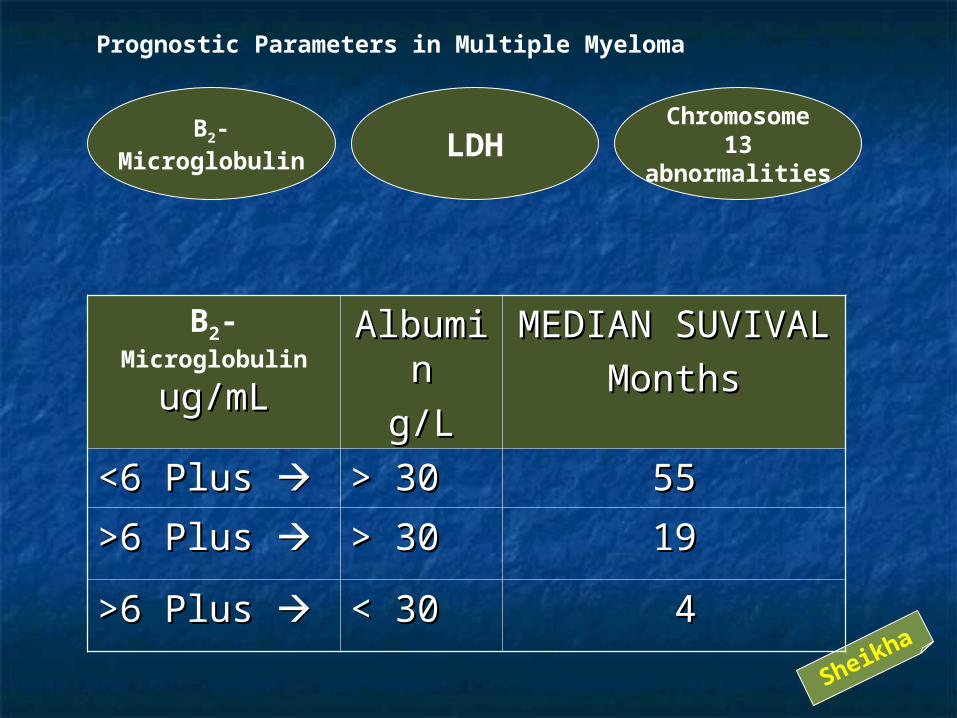
Prognostic Parameters in Multiple Myeloma
Sheikha
Β2-Microglobulin LDH
Chromosome13
abnormalities
Β2- Microglobulin
ug/mLug/mLAlbumiAlbumi
nn
g/Lg/L
MEDIAN SUVIVALMEDIAN SUVIVAL
MonthsMonths
<6 Plus <6 Plus > 30> 30 5555
>6 Plus >6 Plus > 30> 30 1919
>6 Plus >6 Plus < 30< 30 44

MANAGEMENT OF
MULTPLE MYELOMA
Sheikha

MPVAD
Quicker ResponseBetter control of symptoms
Less Myelotoxic & more convenient before autologous Transplant
Good after MP relapse
4 day infusion iscumbersome & need
central Line
M2PROTOCOL
AggressiveAlkylating
Combination
Better reservedfor relapse after
autotransplantfailure & otherSpecial cases
STANDARDREGIMEN
NO OTHERREGIMEN
PRODUCED BETTER OS
OS > 3YRSSheikha
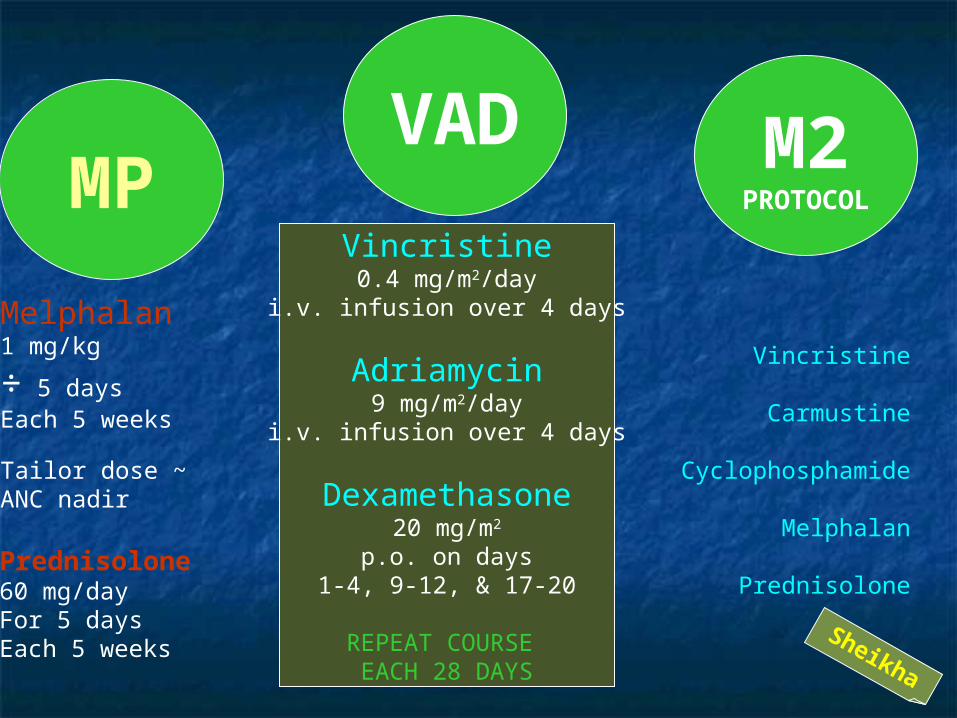
MPVAD
Melphalan1 mg/kg
÷ 5 days Each 5 weeks
Tailor dose ~ ANC nadir
Prednisolone60 mg/dayFor 5 daysEach 5 weeks
Vincristine0.4 mg/m2/day
i.v. infusion over 4 days
Adriamycin9 mg/m2/day
i.v. infusion over 4 days
Dexamethasone20 mg/m2
p.o. on days1-4, 9-12, & 17-20
REPEAT COURSE EACH 28 DAYS
M2PROTOCOL
Vincristine
Carmustine
Cyclophosphamide
Melphalan
Prednisolone
Sheikha

Thalidomide
Begin at200 mg p.o. daily
Increase by200 mg every
2 weeksfor a goal
of 800 mg
p.o.daily
Constipation Neuropathy Somnolence
Thalidomideis
NOTMyelotoxic
Sheikha

Thalidomide
potential mechanisms of antimyeloma activity: (a) Direct effects (b) antiadhesive action (a)(c) GF inhibition (d) antiangiogenesis (a)(e) immunomodulation
bFGF: basic fibroblast growth factor TNF: tumor necrosis factor ICAM: intracellular adhesion molecule IFN: interferon IL: interleukin VEGF: vascular endothelial growth factor
Thalidomide
Begin at 200 mg p.o. daily
Increase by 200 mg every 2 weeks for a goal of 800 mg p.o. daily
Angio-genesis

Thalidomide

Dexamethasone
Described as the single most effective agent in Myeloma
Effective efficacy comparable to VAD in Primary Refractory Myeloma
Not Myelosuppressive and suits patients with severe marrow compromise
In Frail & Elderly patients start with a lower dose
Dexamethasone20 mg/m2 p.o. on days
1-4, 9-12, & 17-20
REPEAT COURSE EACH 28 to 42 DAYS
Sheikha
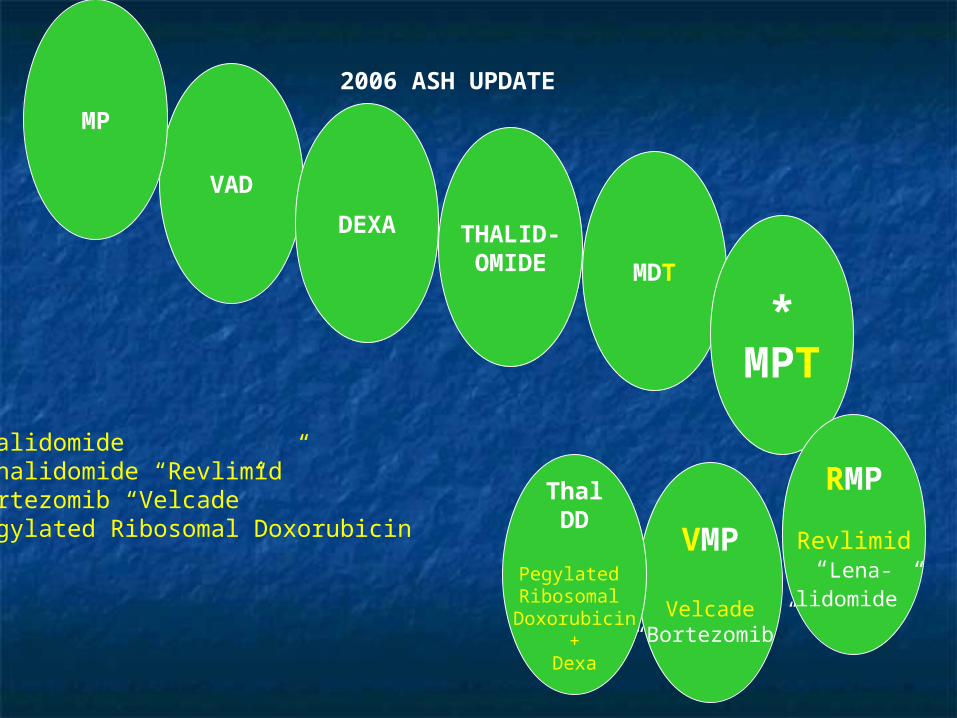
2006 ASH UPDATE
VAD
MP
DEXA THALID-OMIDE MDT
*MPT
VMP
Velcade“Bortezomib”
RMP
Revlimid“Lena-
lidomide”
ThalDD
Pegylated Ribosomal Doxorubicin
+Dexa
ThalidomideLenalidomide “Revlimid”Bortezomib “Velcade”Pegylated Ribosomal Doxorubicin


French randomized trial of conventional versus high-dose therapy


BONEMARROW
or
PERIPHERALSTEM CELL
TRANSPLANTATION
HIGH DOSE CHEMOTHERAPY
“VAD”
AutologousTransplant
ALLOGENEICTRANSPLANT
Ideal for YoungPatients with
HistocompatibleDonor Sibling
Sheikha

PBSCT, peripheral blood stem cell transplantation
Stem Cell Transplantation as Up-Front versus Rescue Treatment
Measure PBSCT Early PBSCT Late
Estimated median overall survival 64.6 mo 64.0 mo
Median event-free survival 39.0 mo 13.0 mo
Quality-adjusted time without symptoms or toxicity 27.8 mo 22.3 mo


ADJUVANT TREATMENTS IN MULTIPLE MYELOMA
BIS-PHOSPHONATES
PAMIDRONATEZOLEDRONATE
EPO
RADIATION
HEMO-DIALYSIS
INTERFERON
Pneumovax
Inhibit Bone Resorption
Reduces Bone #
Suppresses Hypercalcemia
Convenient 1 injection/monthSheikha


DC: dendritic cell IL: interleukin IMIDS: immunomodulatory drugs MM: multiple myeloma VEGF: vascular endothelial growth factor
Novel treatment approaches to Myeloma from the bench to the bedside

THANK YOU

Thalidomide:
potential mechanisms of antimyeloma activity. (a)Direct effects; (b) antiadhesive action;
(b)(c) growth factor inhibition; (d) antiangiogenesis; (c)(e) immunomodulation. bFGF, basic fibroblast growth factor;
(d)ICAM, intracellular adhesion molecule; IFN, (e)interferon; IL, interleukin; TNF, tumor necrosis factor;
(f)VEGF, vascular endothelial growth factor
Angio-genesis

AMYLOIDOSIS
Sheikha

PRIMARYAMYLOIDOSIS
Sheikha

Primary Amyloidosis
PC neoplasm that secretes an abnormal Ig,Which deposits in various tissues & forms a
β-pleated sheet structure that binds Congo Red dye with characteristic birefringence
RareAdult
Disease
80% of Patients have Monoclonal Ig
20% haveMyeloma
15% ofMyeloma have or develop
10
Amyloidosis
GUT
Mal-Absorp-
tion
CHFHMG
N.S.
CRF
Macroglossia
NERVESSensorimotorneuropathy
Loss of Sphinctercontrol
DiagnosticBiopsy Sites
Abd. s.c. fat-padBone Marrow
Rectum
Sheikha

Primary Amyloidosis
Deposition in organs ORGANOMEGALY
BLEEDINGIncreased vessel fragility
Coagulation factors binding
Amyloid is a fibrillary protein that causes organ failure
ALPrimary or
Ig- light chainAmyloidosis
(~ Myeloma)
AASecondary
~ inflammation
AFFamilial
β2 Micro-
globulin
~ Dialysis
Sheikha










SOP
Sheikha

SOP
SolitaryOsseous
Plasmacytoma
Sheikha

SOP
5% of PC neoplams
No other Lytic lesions should be detectedMarrow away from the lesion should not have plasmacytosis
Site depends on marrow activity
In order of frequency sites are:Vertebrae Ribs Skull Pelvis Femur Clavicle Scapula
35%CURED
55%MM
>10 years
10%Local Recurrennce
orAnother SOP
Treatment
RTIf Paraprotein +veit should disappear
after treatment
Sheikha

Sheikha

Sheikha

Sheikha
Sheikha
EXTRA-OSSEOUSPLASMACYTOMA
Sheikha

EOP
ExtraOsseous
Plasmacytoma
Sheikha

BMSC, bone marrow stromal cell ECM, extracellular matrix ICAM, intracellular adhesion molecule IL, interleukin
LFA, lymphocyte function-associated antigen MM, multiple myeloma VCAM, vascular cell adhesion molecule
VLA, very late antigen
Role of
adhesion molecules
in disease
pathogenesis

EOPEXTRA
OSSEOUSEXTRA
MEDULLARY
5% of PC neoplasmsNo Lytic lesions or marrow plasmacytomaMedian Age: 55 yearsM/F ratio: 2:1
80%UPPER
RESPIRATORY TRACT
OropharynxNasopharynx
SinusesLarynx GIT
BLADDER CNS BREAST THYROID
TESTIS
PAROTIDL. N.SKIN
15 – 20% may have PARAPROTEINEMIATreatment RT15%MM
25%Recurrence
Sheikha

WALDENSTOROM’SMACROGLOBULINEMIA
Sheikha

Sheikha

Sheikha
Sheikha



M-GUS
MONOCLONAL GAMMOPATHYOF UNDETERMINATE SIGNIFICANCE
BENIGN MONOCLONAL GAMMOPATHY
Sheikha

Sheikha

HCD
HEAVYCHAIN
DISEASES
Sheikha

HCD
αμ γ
Sheikha

HCD
γGamma
HCD
αAlphaHCD
μmuHCD
A variant
of
LPCLymphoma
A variant
ofExtranodal
Margianl Zone
MALTLymphoma
A variant
of
CLL
Sheikha

αHeavy Chain Disease
IPSIDImmunoproliferative Small Intestinal Disaese
Mediterranean Lymphoma
~ H. pyloriSheikha



POEMSSYNDROME
POLYNEUROPATHY(Sensorimotor Demyelination)
SKIN CHANGES(Hyperpigmentation;
Hypertrichosis)MONOCLONAL GAMMOPATHY
ENDOCRINOPATHY(Diabetes;
Gynecomastia;Testicular Atrophy;
Impotence)
ORGANOMEGALY(Hepato-
Splenomegaly)
OSTEOSCLEROTICMYELOMA
Marrow infiltrated by PC & bone trabeculae thickenedRare:1 to 2% of PC dyscrasias Median Age: 50 years

HIWA HEMATOLOGY HOSPITAL




THANKS


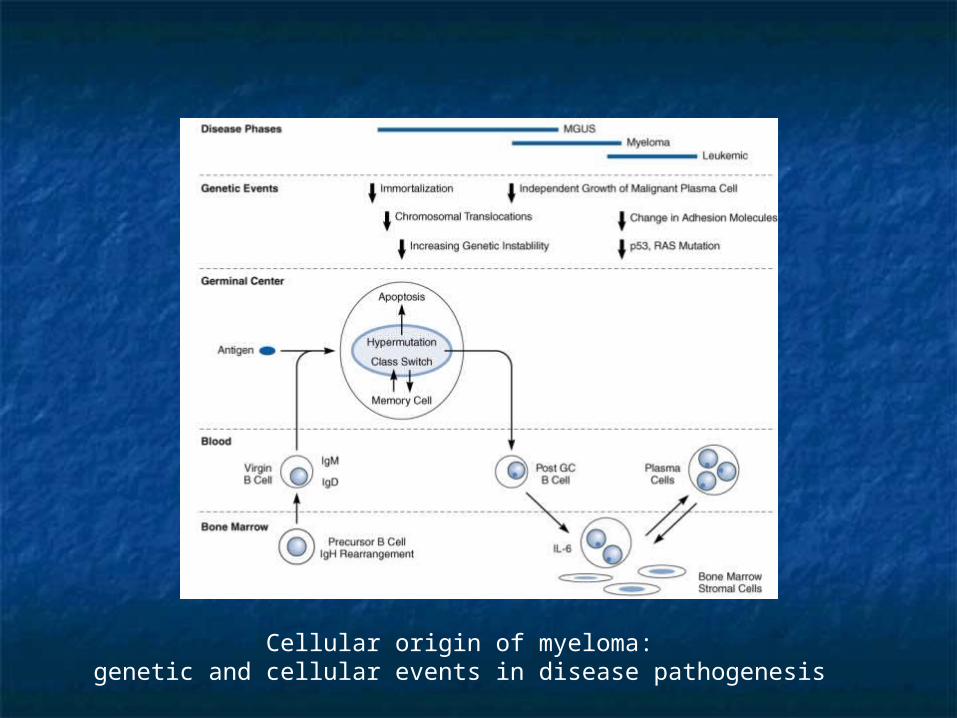
Cellular origin of myeloma: genetic and cellular events in disease pathogenesis

Interleukin-6-mediated myeloma cell growth. BMSC, bone marrow stromal cell; IL, interleukin;
NF, nuclear factor; TGF, transforming growth factor

Apoptosis signaling cascades in myeloma cells. IL, interleukin; JNK, c-jun N-terminal kinase; PYK, proline-rich tyrosine kinase; RAFTK, related adhesion focal tyrosine kinase; SAPK, stress-activated protein kinase

Interleukin-6 growth and antiapoptotic cascades in myeloma cells. MAP, mitogen-activated protein; RAFTK, related adhesion focal tyrosine kinase; SHP, Src homology protein tyrosine phosphatase

BMSC, bone marrow stromal cell ECM, extracellular matrix ICAM, intracellular adhesion molecule IL, interleukin
LFA, lymphocyte function-associated antigen MM, multiple myeloma VCAM, vascular cell adhesion molecule
VLA, very late antigen
Role of
adhesion molecules
in disease
pathogenesis










SOP
SolitaryOsseous
Plasmacytoma











None 6