Papua New Guinea National HIV and AIDS Strategy...to the National HIV and AIDS Strategy 2011–2015...
89
Papua New Guinea National HIV and AIDS Strategy 2011-2015 Monitoring and Evaluation Framework
Transcript of Papua New Guinea National HIV and AIDS Strategy...to the National HIV and AIDS Strategy 2011–2015...

Papua New Guinea
National HIV and AIDS Strategy
2 0 1 1 - 2 0 1 5
Monitoring and Evaluation Framework

Papua New Guinea National HIV and
AIDS Strategy2011-2015
Monitoring and Evaluation Framework

Published in 2010 by the National AIDS Council of Papua New Guinea © Copyright 2010, National AIDS Council of Papua New Guinea All rights reserved.
ISBN: 978-9980-948-53-3
Papua New Guinea: National HIV and AIDS Strategy: 2011-2015: Monitoring and Evaluation Framework
Design and Layout by Mairi Feeger
Printed by Moore Printing, Scratchley Road, Badili, NCD, PNG
The document was developed and written by several groups acknowledged here : National HIV and AIDS Strategy Core Group, National HIV and AIDS Strategy Technical Support Team, National HIV and AIDS Strategy Secretariat and Independent Review Group Key Stakeholders for your contributions and the National AIDS Council Secretariat for your leadership and direction.
We would also like to thank our development partners, AusAID and UN Agencies for your financial and technical support in the development and publication of the National HIV and AIDS Strategy 2011-2015.

iii
ContentsAcronyms iv
Situation analysis of the monitoring and evaluation and surveillance environment in PNG 1
The scope and goals of the National Monitoring and Evaluation Framework 8
Structures for coordination and management of strategic information 9
Flow of data and reports 11
National indicators 15
Definitions for national indicators 22
Strategic information needs not addressed through national indicators 64
Guidelines for developing program monitoring and evaluation plans based on the
National Monitoring and Evaluation Framework 67
Appendix I – Inventory of questions to be included in surveys for measuring
national indicators 68
Appendix II – Repository of additional indicators for monitoring and evaluation
of programs 72
Appendix – III Glossary 80
Contents

iv
Acronyms ADB Asian Development Bank
AIDS acquired immune deficiency syndrome
ANC antenatal care
ART antiretroviral therapy
ARV antiretroviral
AusAID Australian Agency for International Development
BSS behavioural surveillance survey
CBO community based organisation
CRIS Country Response Information System
CTX cotrimoxazole
DHS Demographic Health Survey
FBO faith based organisation
FHI Family Health International
GBV gender based violence
GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria
GoPNG Government of Papua New Guinea
HAMP Act HIV and AIDS Management and Prevention Act
HBC home based care
HCT HIV counselling and testing
HIV human immunodeficiency virus
IBBS Integrated Bio-Behavioural Survey
ICME Intelligence, Cross Cutting Issues and Monitoring and Evaluation Unit
IRG Independent Review Group
MARP more-at-risk population(s)
MCH Maternal and Child Health
M&E monitoring and evaluation
MSM men who have sex with men
NAC National AIDS Council
NACS National AIDS Council Secretariat
NASA National AIDS Spending Assessment
NDoH National Department of Health
NGO non-government organisation
NHIS National Health Information System
NHS National HIV and AIDS Strategy
NOC National M&E Oversight Committee
NRA National Research Agenda
Acronyms

v
NRI National Research Institute
NSO National Statistical Office
PA priority area
PAC Provincial AIDS Committee
PACS Provincial AIDS Committee Secretariat
PACSO PNG Alliance of Civil Society Organisations
PCP pneumocystis jiroveci pneumonia
PEP post-exposure prophylaxis
PHO Provincial Health Office
PLHIV people living with HIV and AIDS
PLLSMA Provincial and Local Level Service Monitoring Authority
PMTCT prevention of mother-to-child transmission
PNG Papua New Guinea
PNGIMR Institute of Medical Research
POC point-of-care
PPTCT prevention of parent-to-child transmission
ProMEST Provincial Monitoring Evaluation and Surveillance Teams
RAC Research Advisory Committee
RCU Research Coordination Unit
SAM service availability mapping
SO strategic objective
SPA service provision assessment
STI sexually transmitted infection
STWG Surveillance Technical Working Group
TA technical assistance
TB tuberculosis
UA universal access
UN United Nations
UNAIDS Joint United Nations Programme on HIV and AIDS
UNDP United Nations Development Programme
UNGASS UNGASS United Nations General Assembly Special Session on HIV and AIDS
USAID United States Agency for International Development
VCT voluntary counselling and testing
WHO World Health Organisation
Acronyms

1
Situation analysis of the monitoring and evaluation and surveillance environment in PNG
The national Monitoring and Evaluation (M&E) system in PNG is guided by the ‘third one’ of the ‘three ones principles’ of having one national M&E system which is linked to the National HIV and AIDS Strategy 2011–2015 (NHS). Like any fully functioning national HIV M&E system, it comprises the following 12 components:
1. Organisational structures with HIV M&E functions2. Human resources capacity for HIV M&E3. Partnerships to plan, coordinate and manage the HIV M&E system4. National, multi-sectoral HIV M&E plan5. Annual costed national HIV M&E work plan6. Advocacy and communications culture for HIV M&E7. Routine HIV program monitoring 8. Surveys and surveillance9. National and sub-national HIV databases10. Supportive supervision and data auditing11. HIV evaluation and research12. Data dissemination and use
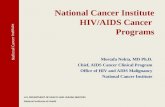
These 12 components will be integrated with each other following the three tiers depicted in Figure 1: • people,partnershipsandplanning• collecting,verifyingandanalysingdata• usingdatafordecisionmaking.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

2Situation analysis of the monitoring and evaluation and surveillance environment in PNG
Figure 1: Situation analysis of the monitoring and evaluation and surveillance environment in PNG
Costed M&E
work planM&E plan
M&E
par
tner
ships
Human capacity
for M&E
Organisational structures with M&E
M&E
adv
ocac
y,
com
mun
icatio
ns a
nd
cultu
re
Data dissemination and use
Rout
ine p
rogr
amm
e
mon
itorin
gSurveys and
surveillance
M&E datab
ase
HIV evaluation
research and
learning
Supervision and
data auditing
In the National HIV and AIDS Strategy and the accompanying NHS Implementation Framework, M&E is envisaged as an integral part of the NHS and found in many of the strategic objectives and major activity areas. M&E is also specifically addressed in Priority area 3, Systems strengthening.

3
Situational analysis: Integration of the twelve components in national monitoring and evaluation in PNGThis section conducts a situation analysis for each of the 12 components listed above that make up a functioning national HIV M&E system. The situational analysis was current at June 2010.
1. Organisational structures for HIV M&E functions
There has been a lot of progress in ensuring that all M&E functions are realigned to existing structures and that these functions are strengthened and fully implemented.
The NACS Intelligence, Cross Cutting Issues and Monitoring and Evaluation Unit (ICME) at the National AIDS Council Secretariat (NACS), the Surveillance Unit at the National Health Information System (NHIS) and the Surveillance and Monitoring and Evaluation Unit within the National STI and HIV and AIDS Program at the National Department of Health (NDoH) are the three main national structures with HIV M&E functions. At the sub-national level, Provincial Monitoring Evaluation and Surveillance Teams (ProMEST) have been established.
The NACS Research Coordination Unit (RCU) is the main coordinating body for all HIV related research in PNG. The National Research Institute (NRI) and the PNG Institute of Medical Research (PNGIMR) are the two main research institutions that design and implement many of the HIV-related surveillance and survey studies.
The main challenge is to ensure that there is regular and meaningful communication between the coordinating bodies and with all stakeholders to ensure that the comprehensive HIV and AIDS response is monitored through this structure and monitoring reports are utilised to inform programming.
2. Human resource capacity for HIV M&E
The NACS ICME and the NDoH Surveillance/NHIS units are struggling to address the planning, programming and logistical demands involved in coordinating the national M&E framework. NDoH has strived to increase its capacity to strengthen the STI, HIV and AIDS surveillance and M&E program. Staff have expertise in epidemiology, demography, statistics and mathematics. Four regional program M&E staff have been recruited to support M&E and surveillance at the sub-national level. Continuous short- and long-term capacity building of staff involved in M&E at national and sub-national levels is critical to ensure quality monitoring outcomes.
At the provincial level most Provincial AIDS Committee Secretariats (PACS) do not have positions or staff dedicated to M&E. There is a need for ongoing capacity development for all people engaged in HIV M&E, including partners in civil society. Although development partners have invested heavily in this area, a more coordinated approach to capacity development within the national M&E framework is required and needs to be a higher priority for stakeholders, especially development partners.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

4
3. Partnerships to plan, coordinate and manage the HIV M&E system
The National Monitoring and Evaluation Oversight Committee (NOC) is still in its initial stages of development. The key task for this committee is to coordinate all HIV and AIDS related M&E activities amongst all stakeholders at national and sub-national levels.
At the technical level, a Surveillance Technical Working Group (STWG) exists at NDoH which is responsible for providing coordinated technical oversight for all STI, HIV and AIDS data gathering and management requirements, guidelines, and procedures. The STWG is chaired by NDoH and comprises representatives from NDoH, NACS, NRI, Asian Development Bank (ADB), World Health Organisation (WHO), Joint United Nations Programme on HIV and AIDS (UNAIDS), United Nations Development Programme (UNDP), Family Health International (FHI), Igat Hope (an organisation of people living with HIV), PNGIMR, the University of PNG and the Australian Agency for International Development (AusAID). Currently, the STWG only deals with technical issues specific to program monitoring data for the health sector and HIV and AIDS behavioural and biological surveillance.
The key challenge for the HIV and AIDS M&E system in this area is to ensure adequate coordination at both high and technical levels and ensure provision of necessary M&E support to sub-national levels, where implementation occurs.
4. National multi-sectoral HIV M&E plan
A key achievement of the National Strategic Plan for HIV/AIDS, 2005-2010 was the development of an overarching M&E framework that formed the basis for monitoring of the HIV response.
This new national HIV M&E framework has been developed in alignment with the new National HIV Strategy, 2011-2015 and will form the basis of monitoring the national response to the epidemic over the next five years.
The main challenge for the NHS and its implementers will be to ensure that the M&E framework is target driven and realistic enough to adequately monitor the trends in HIV and its associated risk behaviours to enable a better response. Another important challenge is for the M&E plan to embrace, to the extent possible, all the reporting commitments of PNG and for the development partners to limit their reporting requirements to the national HIV M&E plan.
5. Annual costed national HIV M&E work plan
Although annual work plans have been developed they have never been successfully costed. In addition to costing a plan, the main challenge is to mobilise resources based on that plan and effectively use them for achieving M&E targets. The HIV-STI surveillance plan for 2007–2010 was costed and this facilitated resource mobilisation for its implementation.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

5
6. Advocacy and communications culture for HIV M&E
There is an increasing receptiveness to the incorporation on M&E into HIV programming. The new NHS places a strong emphasis on communication of strategic information as the basis for evidence-informed interventions in its three priority areas.
7. Routine HIV program monitoring
The ProMEST coordinating mechanism is only functioning in a small number of provinces. Those provinces that have a well functioning ProMEST are generally better at reporting HIV-related data than provinces where ProMEST is not functioning.
One of the overall challenges for routine HIV program monitoring is the existence of parallel reporting mechanisms. In addition to ProMEST and provincial surveillance systems, many implementing partners, particularly non-government organisations (NGOs) and faith based organisations (FBOs), have their own reporting systems and have not been using ProMEST monitoring tools and guidelines to report to provincial and national levels. Instead they report using other formats and frameworks, in line with the conditions set by their parent organisation or donor(s).
8. Surveys and surveillance
NDoH is responsible for national coordination of all surveillance activities for STI, HIV and AIDS. Its core mandates include:
1. Routine surveillance of STI, HIV and AIDS through case reporting. 2. Development of estimates and projections for HIV and AIDS, with the
assistance of a panel of experts. 3. Conducting annual sentinel surveys of STI clients, antenatal care (ANC) clients
and tuberculosis (TB) patients. 4. Conducting behavioural surveillance surveys (BSS).
Reports on all of these activities are available. Three rounds of BSS surveys have been conducted between 2006–2010 at various sites targeting more-at-risk populations (MARPs) such as youth, sex workers, economic enclave workers and truck drivers. NDoH works in partnership with NRI in designing and conducting behavioural and bio-behavioural surveys. The BSS component of the surveillance system has been sub-contracted to NRI. NDoH intends to initiate similar arrangements with IMR to support BSS as part of implementing comprehensive second generation surveillance. An integrated bio-behavioural survey among the general population is being planned for 2011.
The Independent Review Group’s (IRG) 2010 report noted that the HIV surveillance system in NDoH has been steadily improving. This is a result of the increase in HIV testing sites and the establishment of a sentinel surveillance system. The IRG also found that the quality of HIV surveillance reporting has improved, with a greater number of sites reporting more complete information.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

6
A significant challenge is limited surveillance of MARPs by either NDoH or other institutions which limits comprehensive programming targeting these groups. Other key challenges include the need for surveys to be gender and age sensitive and the importance of disaggregating data to assist with analysis.
9. National and sub-national HIV databases
With technical and financial support from development partners, ICME has established the National HIV and AIDS Database using the Country Response Information System (CRIS). Aligning all HIV and AIDS data from all sources is still in train. Data needs to be more widely available to all partners.
10. Supportive supervision and data auditing
NACS policy is to decentralise many M&E and surveillance functions to the provinces, including the reallocation of resources, delegation of power, infrastructure support and local capacity building. Implementing this policy faces many challenges. There are ongoing issues related to the quality management of data coming from the provinces. Specific data quality assurance and control mentoring programs for staff are required.
The NDoH Surveillance Unit, with the assistance of WHO and the United States Centres for Disease Control’s regional program, is currently piloting quality assurance and data quality improvement tools.
11. HIV evaluation and research
A prioritised National HIV/AIDS Research Agenda (2008–2013) was launched in 2008. In addition, the NACS RCU conducted a thorough and systematic review of 62 studies carried out or published in 2007 and 2008 and synthesised findings in a published report.
A national Research Advisory Committee (RAC) has been established and is functioning to ensure ethical design and implementation of HIV and AIDS research and compatibility of research with the HIV and AIDS Management and Prevention Act, 2003 (HAMP). The RAC comprises members from PNG research and academic institutions, NGOs, community based organisations (CBOs), donor organisations and NDoH, as well as representation of people living with HIV and AIDS (PLHIV).
The Independent Review Group (IRG) also contributes to ongoing M&E of PNG’s national HIV response. This is a group of inter-disciplinary international experts engaged by NACS, with funding support from AusAID and the United Nations (UN). The IRG carries out regular assessments of progress in implementing various aspects of the national response and publishes reports of its findings.
The AusAID-funded Strengthening HIV Social Research Capacity in Papua New Guinea Project is a collaboration between IMR and the National Centre in HIV Social Research at the University of New South Wales. The project is contributing to building the capacity for HIV social research in PNG. It is designed to position social research as a central component of the evidence base for effective, sustainable responses to the HIV epidemic through a cadetship program and the dissemination of findings.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

7
An important challenge is the translation of research into the day-to-day practice of service providers. Additionally, operations research is not being conducted by either service providers or researchers.
12. Data dissemination and use
While relatively good-quality data and information is being produced in PNG it is not consistently or systematically being passed on and promoted to program planners and managers. There is a demonstrated need for an agreed plan on how to regularly update policies and programs based on the regular review of available knowledge of the HIV epidemic and response in PNG.
Although there has been a lot of information generated and written about the epidemic in PNG, having program planners and policy makers use this information has been a challenge.
Situation analysis of the monitoring and evaluation and surveillance environment in PNG

8
The scope and goals of the National Monitoring and Evaluation Framework
This framework has been developed to guide STI, HIV and AIDS monitoring, evaluation and surveillance activities in PNG. The scope of this framework is the national response to STI and HIV epidemics. As such the framework measures the totality of the national response and is not designed to be an M&E framework for any one program.
The goals of the National Monitoring and Evaluation FrameworkThe goals of the framework are to:
1. direct the M&E of the NHS2. guide the development of M&E plans for programs under the NHS3. harmonise the implementation of strategic objectives and major activity areas of
the NHS related to strategic information, surveillance and M&E.
Based on the above-mentioned scope and goal, this framework:• shouldnotbeusedasastep-by-stepguidelinefordevelopingprogram-and
project-level M&E plans• willnotprovideafulllistofindicatorstobeusedinmonitoringandevaluating
different programs and projects, especially at the input and output levels• willnotreplacetheNationalResearchAgenda(NRA).
The scope and goals of the National Monitoring and Evaluation Framework

9
Structures for coordination and management of strategic information
One of the strategic priorities of the NHS is to improve strategic information systems, which includes M&E, surveillance, research and utilisation of evidence. This requires an emphasis on ensuring effective management and coordination of strategic information.
Responsibility at the national level for data collection, management and analysis is split between NACS and NDoH. NACS is responsible for strategic information for all HIV-related activities outside the health sector, whilst NDoH has responsibility in relation to strategic information for health-sector activities and surveillance of the HIV epidemic. Within NACS, the ICME is the responsible entity. At NDoH, there are two responsible units. Firstly there is the Surveillance Unit which is responsible for monitoring of HIV testing, care and treatment services and surveillance activities (including HIV case reporting, sentinel surveillance and survey-based surveillance). Secondly, the Monitoring and Evaluation and Research Unit is responsible for the surveillance system for STIs.
The NACS RCU is the main coordinating and supervisory body for all HIV-related research in PNG. The NACS RAC oversights ethical aspects of research conduct and application of the HAMP Act’s provisions in research practice. The NRI and the PNG IMR are the two main research institutions that design and implement many of the HIV-related surveillance and research studies.
The NOC has overarching responsibility for coordination of all activities related to M&E, surveillance and strategic information. The Committee is chaired by the Director of NACS and has representation from NDoH, NRI, IMR, the National Statistical Office, key government departments, the PNG Alliance of Civil Society Organisations, the Business Alliance Against HIV and AIDS, FBOs, international NGOs and the Development Partner’s Forum. The NOC reports to NAC and NACS.
There are two other national-level, multisectoral technical working groups that provide advice on the development of data collection tools, data collection activities, data management, analysis and reporting. The STWG provides technical advice on strategic information for all health sector and epidemiological surveillance activities. Its secretariat is provided by the NDoH Surveillance Unit. The Monitoring and Evaluation Technical Working Group provides technical advice on strategic information for all HIV-related activities outside the health sector. Its secretariat is provided by the ICME. Both of these technical working groups report to the NOC as well as NAC, NACS and NDoH.
NOC’s key areas of responsibility are to: 1. Coordinate and provide high-level oversight to ensure that the M&E framework
for the NHS is being effectively implemented, consistent with the aim of one national M&E system.
Structures for coordination and management of strategic information

10
2. Promote better collaboration and coordination amongst multi-sectoral agencies in regular data reporting and data use.
3. Ensure the multi-sectoral M&E and surveillance technical working groups have functional secretariats at NACS and NDoH respectively, and report on their progress and obstacles to NOC, NACS and NDoH.
4. Ensure that all stakeholders in the HIV and AIDS response who collect data based on either routine reporting of service delivery activities or other means (including research), comply with reporting deadlines, guidelines, tools and reporting lines and procedures as developed by the two technical working groups.
5. Report to NAC and all stakeholders about the situation of the HIV and AIDS epidemic and the response.
6. Mobilise financial and other resources for the development and operation of the M&E system and monitor the functionality and sustainability of the system.
7. Advocate at all policy-making levels for an evidence-informed approach in decision making and management of the HIV response.
8. Ensure that all stakeholders at national and provincial levels have been informed about reports and analyses relevant to them.
Joint ProMESTs have been established at the sub-national level. These teams consist of the Provincial Health Office (PHO), the Provincial AIDS Council Secretariat (PACS) and key program implementers and service providers within the province. Each team is mandated to collect data from all service providers and to ensure quality and completeness of data. Summarised data reports are sent to the NACS ICME each quarter.
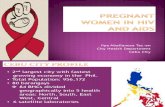
The NOC, the two national technical working groups and the ProMESTs are the key multi-sectoral committees supporting and oversighting HIV and AIDS M&E activities. The functions of these groups, NACS, NDoH and provincial level bodies in relation to data flow activities are shown in Figure 2.
Structures for coordination and management of strategic information

11
Flow of data and reports
HIV and AIDS data and reports related to M&E and strategic information in PNG originate from a wide range of activities including delivering services, conducting nation-wide studies and compiling secondary information. There is a division of labour between NACS and NDoH in managing data and information related to the HIV response. NDoH is the custodian and manager of epidemiological data and data related to providing services in health care facilities and NACS deals with data from all other sources (that is, data from non-health sector services).
Health facility services include HIV counselling and testing (HCT), treatment and care of HIV infection, STI diagnosis, care and treatment, and some prevention activities like prevention of parent-to-child transmission (PPTCT) and post-exposure prophylaxis. On the other hand, non-health sector services include social support and protection for people living with or affected by HIV, prevention interventions through awareness-raising among the general population and key populations at higher risk, and other targeted promotion and education interventions. Some service delivery, like condom provision to the general population and key populations at higher risk, may be provided by both health care facilities and non-health services.
Data flow is affected by the presence of multiple funding agencies and the operations of NGOs and FBOs which are conducting projects in multiple provinces. These organisations need to report their M&E data to provincial and in some cases national authorities as well as their funding agencies and governing NGOs or FBOs.
The national M&E framework will follow the data flow systems summarised in Figure 2.
Data flow for monitoring of services provided by health care facilitiesIn each province, the PHO is the authority receiving data based on national M&E indicators and program specific indicators. Data comes from facilities providing the following services:
1. HCT, including rapid testing, followed by laboratory confirmation or point-of-care (POC) rapid testing and use of another rapid test for confirmation. HCT is provided through voluntary counselling and testing (VCT) in stand-alone sites or other testing facilities or through provider-initiated testing and counselling in ANC clinics, STI or TB or other clinical facilities, as well as screening of all blood donors.
2. Anti-retroviral therapy (ART), including adult and paediatric regimens as well as providing anti-retroviral (ARV) drugs for prevention of mother-to-child transmission (PMTCT) and post-exposure prophylaxis.
3. Diagnosis (syndromic and aetiological) and treatment of STIs .
Flow of data and reports

12
4. Case reports of new diagnoses of HIV are sent to the PHO on a monthly basis. Unified data collection forms for each centre are provided by NDoH or the PHO to reflect the data collection needs at provincial, program or national level.
The PHO compiles provincial summaries from service providers and shares these with all stakeholders at provincial level through ProMEST. Summarised reports, based on national indicators for services 1, 2 and 4 above, are sent to the Surveillance Unit at NDoH. Data on service 3 above are sent to the Monitoring and Evaluation and Research Unit (also known as NHIS).
In some circumstances, health services may be required to send a copy of their reports directly to relevant units at NDoH. Where this occurs the Surveillance, M&E and Research Units compile provincial reports and send them to the PHO.
In summary, health service providers send data to the PHO as their first-line M&E reporting authority. In addition, some data is sent to NDoH as the second line or national authority, as a backup in situations when the reporting to PHO is not working properly. The PHO reports summarised information to provincial stakeholders through ProMEST and to NDoH. NDoH sends summary provincial and national reports to the PHO and they have to share them with stakeholders through ProMEST.
Data flow for monitoring non-health sector services In each province, the PACS is the authority receiving data based on national M&E indicators and other program-specific indicators. These data have to be sent to the PACS on a quarterly basis. Unified data collection forms for each service will be provided by the NACS ICME or the PACS to reflect data collection needs at provincial, program and national levels.
The PACS compiles provincial summaries from the service providers and share these with all stakeholders at provincial level through ProMEST. The PACS sends a summarised report, based on national indicators to ICME. ICME sends summary provincial and national reports to the PACS, which share these with stakeholders though ProMEST.
Data flow for research and study resultsAll researchers are required to send a copy of their research reports to the RCU. The RCU shares a copy of these findings with the PACS in the province(s) where the study was conducted or requests the principal investigator to share the findings.
Management of data and information at provincial and national levelsThe PACS and PHO in each province receive monitoring data from service providers throughout the province. All data and information are entered into a single database at provincial level and shared with stakeholders through ProMEST or other mechanisms
Flow of data and reports

13
suitable for that province. This database should be the basis for developing summarised reports which are sent to the national level. To standardise the structure of the database and format of the reports the CRIS should be used to develop all provincial databases. This would enhance consistency with the data held at the national level. At national level, a CRIS database is used for all data coming from the provinces, NDoH and the RCU. This National HIV and AIDS Database is the data centre for all HIV-related reports produced through service provision, surveillance and studies. This data centre is used for all national and international reporting, unless other sources of data are needed.
Flow of data and reports

14
Figure 2: HIV and AIDS data flow in PNG
National Oversight Committee
National Level
Provincial Level
Service type
Surveillance Unit NDoH
NACS1: NACS Quarterly Reporting Form for Non-Health Agencies NACS2: NACS Quarterly Reporting Form for Non-Health Agencies NHIS1: National Health Information System Monthly Report SURV1: HIV Monthly Testing Summary FormSURV2: HIV/ART Monthly Data Collection Sheet SURV3: STI Clinic Patient Record Form (this form will be kept at health facilities) SURV4: Notification Form for HIV and AIDS CasesSURV4.1: Laboratory Request Form for HIV Confirmatory Test SURV5.1: HIV Sentinel Surveillance Form for ANC/PPTCT Clinic SURV5.2: HIV Sentinel Surveillance Form for STI Clinic SURV5.3: HIV Sentinel Surveillance Form for TB Clinic
Non-Health services data
(GLA, NGOs, CBOs, FBOs, PS, and D/FAs)
DHS, BSS & IBBS other researches
National HIV and AIDS Database
ProMEST
Data Sharing /Coordination
NHIS Unit M & E Unit NACS
Reporting
Feedback
Surveillance Technical Working Group
M&E Technical Working Group
Provincial Lab
Health services data
(VCT, ANC, STI, TB clinics, Hospitals, Clinics, Health Centre,
sentinel sites, Blood Banks)
Academic, Research & Statistic Institutes
(NRI, IMR, NSO)
SURV4.1SURV4.1
SURV4
SURV4 NHIS1 NACS2
NHIS1 NACS1
SURV1 SURV5.1 SURV5.2 SURV5.3
SURV1 SURV5.1 SURV5.2 SURV5.3
SURV2
SURV4
PHO PAC
Flow of data and reports

15
National indicators
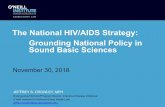
The list of national indicators (see Table 1) is limited to 39 core indicators that are essential for high-level monitoring of STI, HIV and AIDS epidemiology and PNG’s national response.
Of the 39 national indicators, most are taken from the United Nations General Assembly Special Session on HIV and AIDS (UNGASS) core indicators. Others are taken from the Universal Access indicators list and the additional recommended UNGASS indicators list (UNGASS+). Detailed information about the definitions of the national indicators is in the next section.
It should be noted that in addition to the suggested disaggregation levels for the national indicators, geographical disaggregation is also needed, usually at the level of province whenever possible.
Questions that should be included in survey questionnaires for measuring some of these indicators are presented in Appendix I – Inventory of questions to be included in surveys measuring national indicators.
In addition to the national indicators other indicators have been developed or chosen from indicators already in use at the national and international level for program monitoring purposes. These additional indicators are presented in Appendix II – Repository of indicators suggested for monitoring and evaluation of programs. These additional indicators can be used, as appropriate, by projects and programs for their own internal M&E. However, there is no requirement to report to PACS, NACS and/or NDoH on performance against these additional indicators.
National indicators

16
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
1P
erce
ntag
e of
wom
en a
nd m
en a
ged
15 to
59
with
mor
e th
an o
ne o
ngoi
ng s
exua
l par
tner
ship
at t
he p
oint
in ti
me
durin
g th
e pa
st th
ree
mon
ths
Sex
A
gePA
11 - 1.
1.4
–
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Spe
cial
pop
ulat
ion
beha
viou
ral s
urve
illan
ce
surv
ey (B
SS
)
Eve
ry th
ree
to
five
year
s
2P
erce
ntag
e of
wom
en a
nd m
en a
ged
15 to
59
with
mor
e th
an o
ne o
ngoi
ng s
exua
l par
tner
ship
at t
he p
oint
in ti
me
durin
g th
e pa
st 1
2 m
onth
sS
ex
Age
PA1
- 1.1
.4–
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Spe
cial
pop
ulat
ion
BS
S
Eve
ry th
ree
to
five
year
s
3P
erce
ntag
e of
wom
en a
nd m
en a
ged
15–5
9 w
ho h
ave
had
sexu
al in
terc
ours
e w
ith m
ore
than
one
par
tner
in th
e la
st 1
2 m
onth
sS
ex
Age
PA1
- 1.1
.4U
NG
AS
S
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Spe
cial
pop
ulat
ion
BS
S
Eve
ry th
ree
to
five
year
s
4P
erce
ntag
e of
men
and
wom
en a
ged
15 to
59
who
had
m
ore
than
one
sex
ual p
artn
er in
the
past
12
mon
ths
and
who
repo
rt th
e us
e of
a c
ondo
m d
urin
g la
st in
terc
ours
eS
ex
Age
PA1
- 1.1
.2U
NG
AS
S
Spe
cial
pop
ulat
ion
BS
S
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Eve
ry th
ree
to
five
year
s
Indi
cato
rs fo
r the
top
10 in
terv
entio
ns
1 N
HS
Prio
rity
area
1
Tabl
e 1:
Th
e lis
t of n
atio
nal i
ndic
ator
s
National indicators

17
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
5P
erce
ntag
e of
fem
ale
and
mal
e se
x w
orke
rs re
porti
ng th
e us
e of
a c
ondo
m w
ith th
eir m
ost r
ecen
t clie
ntS
ex
Age
G
ende
rPA
1 - 1
.1.6
UN
GA
SS
Spe
cial
pop
ulat
ion
BS
SE
very
two
to
thre
e ye
ars
6P
erce
ntag
e of
men
and
wom
en w
ho h
ave
parti
cipa
ted
in
trans
actio
nal s
ex in
the
last
12
mon
ths
and
who
repo
rt co
ndom
use
at l
ast t
rans
actio
nal s
exS
ex
Age
PA1
- 1.1
.7–
Spe
cial
pop
ulat
ion
BS
S
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Eve
ry tw
o to
th
ree
year
s
7P
erce
ntag
e of
men
repo
rting
con
dom
use
the
last
tim
e th
ey
had
anal
sex
with
a m
ale
partn
erA
ge
Gen
der
PA1
- 1.1
.8U
NG
AS
SS
peci
al p
opul
atio
n B
SS
Eve
ry tw
o to
th
ree
year
s
8P
erce
ntag
e of
men
and
wom
en a
ged
15 to
59
who
repo
rt co
ndom
use
dur
ing
last
tim
e of
ana
l sex
Sex
A
ge
Par
tner
sex
PA1
- 1.1
.3–
Yout
h an
d ge
nera
l po
pula
tion
surv
eyE
very
thre
e to
fiv
e ye
ars
9P
erce
ntag
e of
men
and
wom
en a
ged
15 to
59
who
repo
rt co
ndom
use
dur
ing
last
tim
e of
ana
l sex
AR
V re
gim
en ty
pePA
1 - 1
.2.2
UN
GA
SS
Pro
gram
dat
a E
stim
atio
nA
nnua
l
10P
erce
ntag
e of
pre
gnan
t wom
en w
ho w
ere
test
ed fo
r HIV
an
d re
ceiv
ed th
eir r
esul
ts -
durin
g pr
egna
ncy,
dur
ing
labo
ur
and
deliv
ery,
and
dur
ing
the
post
-par
tum
per
iod
(<72
ho
urs)
, inc
ludi
ng th
ose
with
pre
viou
sly
know
n H
IV s
tatu
s
Pre
gnan
cy s
tage
PA1
- 1.2
.3U
nive
rsal
ac
cess
(UA
)P
rogr
am d
ata
Ann
ual
11N
umbe
r of o
pera
tiona
l Fam
ily S
uppo
rt C
entre
s–
PA1
- 2.1
.3
PA3
- 2.1
.7–
Pro
gram
dat
aA
nnua
l
12P
erce
ntag
e of
wom
en a
nd m
en a
ged
15 to
59
who
rece
ived
an
HIV
test
in th
e la
st 1
2 m
onth
s an
d w
ho k
now
the
resu
ltsS
ex
Age
PA22 -
1.1.
1 PA
2 - 1
.1.2
UN
GA
SS
Yout
h an
d ge
nera
l po
pula
tion
surv
eyE
very
thre
e to
fiv
e ye
ars
2 N
HS
Prio
rity
area
2
National indicators

18
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
13P
erce
ntag
e of
mor
e-at
-ris
k po
pula
tions
that
hav
e re
ceiv
ed
an H
IV te
st in
the
last
12
mon
ths
and
know
the
resu
ltsS
ex
Age
G
ende
rPA
2 - 1
.1.3
UN
GA
SS
Spe
cial
pop
ulat
ion
BS
SE
very
two
to
thre
e ye
ars
14P
erce
ntag
e of
TB
clie
nts
who
had
an
HIV
test
resu
lt re
cord
ed in
the
TB re
gist
erS
ex
Age
TB
dia
gnos
isPA
2 - 1
.1.7
UN
GA
SS
+,
UA
Hea
lth m
anag
emen
t in
form
atio
n sy
stem
Ann
ual
15P
erce
ntag
e of
STI
clie
nts
who
had
an
HIV
test
Sex
A
ge
STI
dia
gnos
isPA
2 - 1
.1.7
–he
alth
man
agem
ent
info
rmat
ion
syst
emA
nnua
l
16P
erce
ntag
e of
adu
lts a
nd c
hild
ren
with
adv
ance
d H
IV
infe
ctio
n re
ceiv
ing
antir
etro
vira
l the
rapy
Sex
A
gePA
2 - 2
.1.1
UN
GA
SS
Pro
gram
dat
aE
stim
atio
nA
nnua
l
17P
erce
ntag
e of
est
imat
ed H
IV-p
ositi
ve in
cide
nt T
B c
ases
th
at re
ceiv
ed tr
eatm
ent f
or T
B a
nd H
IVS
ex
Age
PA2
- 2.1
.3U
NG
AS
SP
rogr
am d
ata
Est
imat
ion
Ann
ual
18P
erce
ntag
e of
adu
lts a
nd c
hild
ren
with
HIV
kno
wn
to b
e on
trea
tmen
t at 1
2/24
/36/
48 m
onth
s af
ter i
nitia
tion
of
antir
etro
vira
l the
rapy
Sex
A
gePA
2 - 2
.1.1
0U
NG
AS
S –
U
AA
RT
repo
rting
Ann
ual
19P
erce
ntag
e of
NG
Os,
FB
Os
and
CB
Os
subm
ittin
g th
eir
plan
s an
d re
ports
to th
eir P
AC
S o
r NA
CS
on
time
Age
ncy
type
S
ubm
issi
on ty
pePA
33 - 3
.1.3
–N
HS
man
agem
ent
repo
rtA
nnua
l
20P
erce
ntag
e of
tech
nica
l ass
ista
nce
depl
oyed
to s
uppo
rt th
e N
HS
impl
emen
tatio
n at
sub
-nat
iona
l lev
el c
ompa
red
to th
e to
tal T
AD
urat
ion
of T
APA
3 - 3
.1.4
–N
HS
man
agem
ent
repo
rtA
nnua
l
21P
erce
ntag
e of
pro
vinc
ial g
over
nmen
ts th
at re
port
to th
e P
rovi
ncia
l and
Loc
al L
evel
Ser
vice
Mon
itorin
g A
utho
rity
(PLS
SM
A) o
n th
eir s
peci
fic H
IV re
spon
sibi
litie
s un
der t
he
Det
erm
inat
ion
on S
ervi
ce D
eliv
ery
–PA
3 - 3
.2.3
–N
HS
man
agem
ent
repo
rtA
nnua
l
3 N
HS
Prio
rity
area
3
National indicators

19
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
22P
erce
ntag
e of
wom
en a
nd m
en w
ho a
re H
IV in
fect
ed
Age
Impa
ct o
f the
N
HS
UN
GA
SS
Ant
enat
al c
are
(AN
C)
serv
ices
IBB
S
Ann
ual f
or A
NC
da
ta a
nd e
very
th
ree
to fi
ve
year
for g
ener
al
popu
latio
n in
tegr
ated
bi
o-be
havi
oura
l su
rvey
(IB
BS
)
23P
erce
ntag
e of
mor
e-at
-ris
k po
pula
tions
who
are
HIV
in
fect
edS
ex
Age
Impa
ct o
f the
N
HS
UN
GA
SS
Spe
cial
pop
ulat
ion
IB
BS
Eve
ry tw
o to
th
ree
year
s
24D
omes
tic a
nd in
tern
atio
nal A
IDS
spe
ndin
g by
cat
egor
ies
and
finan
cing
sou
rces
–
Cro
ss-c
uttin
g ac
ross
sev
eral
st
rate
gic
obje
ctiv
es,
spec
ifica
lly:
PA3
- 2.3
.4
PA3
- 3.2
.4
UN
GA
SS
Nat
iona
l AID
S S
pend
ing
Ass
essm
ent
Eve
ry tw
o to
th
ree
year
s
25N
atio
nal C
ompo
site
Pol
icy
Inde
x (N
CP
I) (A
reas
cov
ered
: pr
even
tion,
trea
tmen
t, ca
re a
nd s
uppo
rt, h
uman
righ
ts, c
ivil
soci
ety
invo
lvem
ent,
gend
er, w
orkp
lace
pro
gram
s, s
tigm
a an
d di
scrim
inat
ion
and
M&
E)
–
Cro
ss-c
uttin
g ac
ross
man
y st
rate
gic
obje
ctiv
es,
spec
ifica
lly:
PA3
- 1.1
.1
PA3
- 1.1
.2
PA3
- 1.1
.5
UN
GA
SS
Des
k re
view
N
CP
I int
ervi
ews
Eve
ry tw
o ye
ars
26Th
e de
gree
of s
tigm
a an
d di
scrim
inat
ion
as id
entifi
ed b
y th
e P
eopl
e Li
ving
with
HIV
Stig
ma
Inde
x
–
Cro
ss-c
uttin
g ac
ross
sev
eral
st
rate
gic
obje
ctiv
es,
spec
ifica
lly:
PA1
- 2.4
.2
PA3
- 2.5
.4
–P
eopl
e Li
ving
with
HIV
S
tigm
a In
dex
inte
rvie
wE
very
thre
e ye
ars
Indi
cato
rs fo
r mon
itorin
g th
e re
spon
se e
nviro
nmen
t and
inpu
ts
National indicators

20
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
27P
erce
ntag
e of
hea
lth fa
cilit
ies
with
pos
t-exp
osur
e pr
ophy
laxi
s (P
EP
) ava
ilabl
eTy
pe o
f hea
lth
faci
lity
PA1
- 1.1
.5
PA1
- 1.3
.2U
GA
SS
+ U
AH
ealth
faci
lity
revi
ewE
very
two
to
thre
e ye
ars
28P
erce
ntag
e of
don
ated
blo
od u
nits
scr
eene
d fo
r HIV
in a
qu
ality
ass
ured
man
ner
–PA
1 - 1
.3.3
UN
GA
SS
Blo
od b
ank
revi
ewA
nnua
l
29P
erce
ntag
e of
sch
ools
that
pro
vide
d lif
e-sk
ills
base
d H
IV
educ
atio
n w
ithin
the
mos
t rec
ent a
cade
mic
yea
rLe
vel
PA1
- 2.2
.5
PA1
- 2.3
.4U
NG
AS
SS
choo
l prin
cipa
ls s
urve
yE
very
two
year
s
30P
erce
ntag
e of
mor
e-at
-ris
k po
pula
tions
reac
hed
with
HIV
pr
even
tion
prog
ram
sS
ex
Age
G
ende
r
PA1
- 1.1
.9
PA1
- 2.4
.1
PA1
- 2.4
.4
PA1
- 2.4
.5
UN
GA
SS
Spe
cial
pop
ulat
ion
BS
SE
very
two
to
thre
e ye
ars
31N
umbe
r of d
istri
ct le
vel A
RT
site
sTy
pe o
f hea
lth
faci
lity
Type
of A
RT
serv
ice
PA2
- 2.1
.2–
Pro
gram
repo
rtA
nnua
l
32P
erce
ntag
e of
hea
lth fa
cilit
ies
that
offe
r pae
diat
ric A
RT
(that
is
, pre
scrib
e an
d/or
pro
vide
clin
ical
follo
w-u
p)P
ublic
and
priv
ate
sect
or s
ites
PA2
- 2.2
.1U
AP
rogr
am re
port
Ann
ual
33P
erce
ntag
e of
infa
nts
born
to H
IV in
fect
ed w
omen
who
are
st
arte
d on
cot
rimox
azol
e pr
ophy
laxi
s w
ithin
two
mon
ths
of
birth
Sex
PA2
- 2.2
.2U
NG
AS
S +
U
AP
rogr
am re
port
Ann
ual
34P
erce
ntag
e of
hea
lth fa
cilit
ies
that
pro
vide
STI
scr
eeni
ng
and
synd
rom
ic m
anag
emen
tP
ublic
and
priv
ate
sect
or s
ites
PA2
- 2.3
.1–
Nat
iona
l Hea
lth
Info
rmat
ion
Sur
vey
Ann
ual
35P
erce
ntag
e of
AR
T se
rvic
es th
at a
re li
nked
to H
BC
and
ot
her f
amily
and
com
mun
ity s
uppo
rt se
rvic
esP
ublic
P
rivat
eFB
Os
PA2
- 2.4
.1
Glo
bal F
und
to F
ight
AID
S
Tube
rcul
osis
an
d M
alar
ia
gran
t pro
posa
l
Sur
vey
amon
g A
RT
site
sA
nnua
l
36P
erce
ntag
e of
HIV
cou
nsel
ling
and
test
ing
(HC
T) s
ervi
ces
usin
g th
e 20
09 n
atio
nal p
oint
-of-c
are
algo
rithm
Pub
lic
Priv
ate
FBO
sPA
2 - 1
.1.1
0–
Pro
gram
repo
rtA
nnua
l
Indi
cato
rs fo
r mon
itorin
g th
e na
tiona
l res
pons
e ou
tput
s
National indicators

21
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Indi
cato
r lin
kage
Dat
a co
llect
ion
met
hod/
sour
ceD
ata
colle
ctio
n fr
eque
ncy
37P
erce
ntag
e of
wom
en a
nd m
en w
ho b
oth
corr
ectly
iden
tify
way
s of
pre
vent
ing
the
sexu
al tr
ansm
issi
on o
f HIV
and
who
re
ject
maj
or m
isco
ncep
tions
abo
ut H
IV tr
ansm
issi
onS
ex
Age
PA1
- 1.1
.1
PA1
- 2.2
.1U
NG
AS
S
Yout
h an
d ge
nera
l po
pula
tion
surv
ey
Dem
ogra
phic
and
hea
lth
surv
ey
Eve
ry th
ree
to
five
year
s
38P
erce
ntag
e of
mor
e-at
-ris
k po
pula
tions
who
bot
h co
rrec
tly
iden
tify
way
s of
pre
vent
ing
the
sexu
al tr
ansm
issi
on o
f H
IV a
nd w
ho re
ject
maj
or m
isco
ncep
tions
abo
ut H
IV
trans
mis
sion
Sex
A
ge
Gen
der
PA1
- 1.1
.6
PA1
- 1.1
.8U
NG
AS
SS
peci
al p
opul
atio
n B
SS
Eve
ry tw
o to
th
ree
year
s
39P
erce
ntag
e of
you
ng w
omen
and
men
who
hav
e ha
d se
xual
inte
rcou
rse
befo
re th
e ag
e of
15
Sex
A
gePA
1 - 2
.2.9
UN
GA
SS
Yout
h su
rvey
Dem
ogra
phic
and
hea
lth
surv
eyO
ther
rela
ted
surv
eys
Eve
ry th
ree
to
five
year
s
Indi
cato
rs fo
r mon
itorin
g kn
owle
dge
and
beha
viou
rs
National indicators

22
Definitions for national indicators
Indicator 1: Percentage of women and men aged 15–59 with more than one ongoing sexual partnership at the point in time during the past three months
Concurrent sexual partnerships potentially increase the spread of HIV by creating more connected sexual networks, reducing the time until onward HIV transmission after acquisition, and eliminating the ‘protective sequencing’ provided by serial monogamy. Concurrent sexual partnerships are defined as: Overlapping sexual partnerships where sexual intercourse with one partner occurs between two acts of intercourse with another partner.
Considering the importance of concurrent, multiple, sexual partnership in HIV epidemics of a more generalised pattern, this issue has attracted a special focus in the NHS and addressing it is one of the Top 10 interventions.
To assess progress in reducing the percentage of people who have concurrent sexual partnerships.
Every three to five years.
Youth and general population surveys, Demographic and Health Survey or other household surveys among the general population. Special population surveys among MARPs.
Number of respondents aged 15–59 with more than one ongoing partnership three months before the interview. In the case that one partnership ends and another begins in the third month before the interview, this individual will not be included in the numerator as it cannot be determined whether this is actual concurrency or serial monogamy.
Number of respondents aged 15–59.
Respondents are asked whether or not they have ever had sexual intercourse. If yes, they are asked how long ago they last had sexual intercourse, and how long ago they first had sexual intercourse with that person. If the last intercourse occurred in the past three months, they are asked if they have had intercourse with any other person in the past three months, and if so, they are asked to give the time of last and first sex with that second partner.
This question is repeated for a third partner if one exists. The proportion of individuals who had more than one ongoing partnership at the exact point in time three months before the interview is calculated based on the dates of first and last intercourse with up to the last three partners in the past three months. See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Definitions for national indicators

23
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
To assess progress in reducing the percentage of people who have concurrent sexual partnerships.
Every three to five years.
Youth and general population surveys, Demographic and Health Survey or other household surveys among the general population. Special population survey among MARPs.
Number of respondents aged 15–59 with more than one ongoing partnership 12 months before the interview. In the case that one partnership ends and another begins in the 12th month before the interview, this individual will not be included in the numerator as it cannot be determined whether this is actual concurrency or serial monogamy.
Number of respondents aged 15–59.
Respondents are asked whether or not they have ever had sexual intercourse. If yes, they are asked how long ago they last had sexual intercourse, and how long ago they first had sexual intercourse with that person. If the last intercourse occurred in the past year, they are asked if they have had intercourse with any other person in the past 12 months, and if so, they are asked to give the time of last and first sex with that second partner.
This question is repeated for a third partner if one exists. The proportion of individuals who had more than one ongoing partnership at the exact point in time three months before the interview is calculated based on the dates of first and last intercourse with up to the last three partners in the past year.
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 2: Percentage of women and men aged 15–59 with more than one ongoing sexual partnership at the point in time during the past 12 months
Concurrent sexual partnerships potentially increase the spread of HIV by creating more connected sexual networks, reducing the time until onward HIV transmission after acquisition, and eliminating the ‘protective sequencing’ provided by serial monogamy. Concurrent sexual partnerships are defined as: Overlapping sexual partnerships where sexual intercourse with one partner occurs between two acts of intercourse with another partner.
Considering the importance of concurrent, multiple, sexual partnership in HIV epidemics of a more generalised pattern, this issue has attracted a special focus in the NHS and addressing it is one of the Top 10 interventions.
Definitions for national indicators

24
To assess progress in reducing the percentage of people who have multiple sexual partners.
Every three to five years.
Youth and general population surveys, Demographic and Health Survey or other household surveys among the general population. Special population survey among MARPs.
Number of respondents aged 15–59 who have had sexual intercourse with more than one partner in the last 12 months.
Number of respondents aged 15–59.
Respondents are asked whether or not they have ever had sexual intercourse and, if yes, they are asked: In the last 12 months, how many people have you had sexual intercourse with?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 3: Percentage of women and men aged 15–59 who have had sexual intercourse with more than one partner in the last 12 months
The spread of HIV largely depends upon unprotected sex among people with a high number of partners. Individuals who have multiple partners (concurrently or sequentially) have a higher risk of HIV transmission than individuals who do not link into a wider sexual network.
Considering the importance of concurrent, multiple, sexual partnership in HIV epidemics of a more generalised pattern, this issue has attracted a special focus in the NHS and addressing it is one of the Top 10 interventions. While this indicator cannot discriminate between concurrent and serial multiple sexual partnerships, it can measure the overall prevalence of multiple sexual partnerships.
Definitions for national indicators

25
To assess progress towards increasing the percentage of people with multiple sexual partners who used a condom during last intercourse.
Every three to five years.
Youth and general population surveys, Demographic and Health Survey or other household surveys among the general population. Special population survey among MARPs.
Number of respondents (aged 15–59) who reported having had more than one sexual partner in the last 12 months who also reported that a condom was used the last time they had sex.
Number of respondents (15–59) who reported having had more than one sexual partner in the last 12 months.
Respondents are asked whether or not they have ever had sexual intercourse and, if yes, they are asked: 1. In the last 12 months, how many different people have you had sexual intercourse with?
If more than one, the respondent is asked: 2. Did you or your partner use a condom the last time you had sexual intercourse?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 4: Percentage of men and women aged 15–59 who had more than one sexual partner in the past 12 months who report the use of a condom during last intercourse
The spread of HIV largely depends upon unprotected sex among people with a high number of partners. Individuals who have multiple partners (concurrently or sequentially) have a higher risk of HIV transmission than individuals who do not link into a wider sexual network.
Considering the importance of concurrent, multiple, sexual partnership in HIV epidemics of a more generalised pattern, this issue has attracted a special focus in the NHS and is one of the Top 10 interventions. Condom use is an important measure of protection against HIV, especially among people with multiple sexual partners.
Definitions for national indicators

26
To assess progress in increasing the percentage of sex workers who used a condom with their most recent client.
Every two to three years.
Special surveys for the numerator and denominator, including the FHI BSS for sex workers.
Number of respondents who reported that a condom was used with their last client.
Number of respondents who reported having commercial sex in the last 12 months.
Respondents are asked the following question: Did you use a condom with your most recent client?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Gender (man, woman, male-to-female transgender, female-to-male transgender).
Disaggregation
METHOD OF MEASUREMENT
Indicator 5: Percentage of female and male sex workers reporting the use of a condom with their most recent client
Various factors increase the risk of exposure to HIV among sex workers, including multiple, non-regular partners and more frequent sexual intercourse. However, sex workers can substantially reduce the risk of HIV transmission, both from clients and to clients, through consistent and correct condom use.
Countries with generalised epidemics may also have a concentrated sub-epidemic among sex workers, making it valuable to report on this indicator.
Definitions for national indicators

27
To assess progress in increasing the percentage of people who engage in transactional sex who used a condom at last transactional sex.
Every two to three years.
Special surveys for the numerator and denominator, including the FHI BSS for sex workers or adaptations based on the NHS definition of transactional sex.
Number of respondents who reported that a condom was used with their last transactional sex partner.
Number of respondents who reported having transactional sex in the last 12 months.
Respondents are asked the following questions:
1. Have you had sexual intercourse in the last 12 months with anybody beside your spouse in exchange for money, gifts, food, shelter or any other services? (If yes continue)
2. For the last time you had sexual intercourse in exchange for money, gifts, food, shelter or any other services, did you or your partner use a condom?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 6: Percentage of men and women who have participated in transactional sex in the last 12 months, reporting condom use at last transactional sex
Various factors increase the risk of exposure to HIV among people who engage in transactional sex. Transactional sex is defined as providing sexual services in exchange for money, goods, services or other favours. This can be a frequent practice or on an occasional basis in response to a particular need. However, those who engage in transactional sex can substantially reduce the risk of HIV transmission through consistent and correct condom use.
Countries with generalised epidemics may also have a concentrated sub-epidemic among those engaged in transactional sex, making it valuable to report on this indicator.
Definitions for national indicators

28
To assess progress in increasing the percentage of men reporting condoms use the last time they had anal sex with a male partner.
Every two to three years.
Special surveys including the FHI BSS for men who have sex with men.
Number of male respondents who reported that a condom was used the last time they had anal sex with a male partner.
Number of respondents who reported having had anal sex with a male partner in the last six months.
In a behavioural survey of a sample of men who have sex with men, respondents are asked about sexual partnerships in the preceding six months, about anal sex within those partnerships and about condom use when they last had anal sex.
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Gender (man, male-to-female transgender, female-to-male transgender).Disaggregation
METHOD OF MEASUREMENT
Indicator 7: Percentage of men reporting condom use the last time they had anal sex with a male partner
Condoms can substantially reduce the risk of the sexual transmission of HIV. Consequently, consistent and correct condom use is important for men who have sex with men because of the high risk of HIV transmission during unprotected anal sex. In addition, men who have anal sex with other men may also have female partners, who could also become infected. Condom use with their most recent male partner is considered a reliable indicator of longer-term behaviour.
Countries with generalised epidemics may also have a concentrated sub-epidemic among men who have sex with men, making it valuable to report on this indicator.
Definitions for national indicators

29
To assess progress in increasing the percentage of men and women reporting condoms use the last time they had anal sex.
Every three to five years.
Youth and general population surveys, Demographic and Health Survey or other household surveys among the general population. Special population survey among MARPs.
Number of respondents who reported that a condom was used the last time they had anal sex.
Number of respondents who reported having had anal sex with a partner in the last 12 months.
Respondents are asked:
• In the last 12 months, have you ever had anal intercourse with another person (man or woman)?
If yes, the respondent is asked:
• Did you or your partner use a condom the last time you had anal intercourse?• What was your partner’s sex?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Sex of partner (male, female).
Disaggregation
METHOD OF MEASUREMENT
Indicator 8: Percentage of men and women aged 15–59 who reported condom use during last time of anal sex
Anal sex is not only restricted to men who have sex with men; it is also practiced among heterosexual partners and it carries the same risk of HIV transmission. Condoms can substantially reduce the risk of the sexual transmission of HIV. Consequently, consistent and correct condom use is important for those having anal sex because of the relatively higher risk of HIV transmission during unprotected anal sex. Condom use with their most recent anal sex partner is considered a reliable indicator of longer-term behaviour.
Definitions for national indicators

30
Indicator 9: Percentage of HIV-positive pregnant women who receive ARV medicines to reduce the risk of mother-to-child transmission
In the absence of any preventative intervention, infants born to and breastfed by HIV-infected women have roughly a one-in-three chance of acquiring infection. This can happen during pregnancy, during labour and delivery or after delivery through breastfeeding. The risk of mother-to-child transmission can be significantly reduced through the complementary approaches of ARV regimens for the mother with or without prophylaxis to the infant, implementation of safe delivery practices and use of safer infant feeding practices.
To assess progress in increasing the percentage of HIV-positive pregnant women who receive ART to reduce mother-to-child HIV transmission.
Data should be collected continuously at the facility level and should be aggregated at least annually.
For the numerator: program monitoring tools, such as patient registers and summary reporting forms.
For the denominator: antenatal clinic surveillance surveys in combination with demographic data, or estimation models such as Spectrum.
Number of HIV-infected pregnant women who received ARV medicines to reduce the risk of mother-to-child transmission in the last 12 months.
Estimated number of HIV-infected pregnant women in the last 12 months.
Program monitoring and HIV surveillance.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
ARV regimen type:
• single-dose Nevirapine only• prophylactic regimens using a combination of two ARV drugs• prophylactic regimens using a combination of three ARV drugs
ARV for HIV-infected pregnant women eligible for treatment.
Disaggregation
METHOD OF MEASUREMENT
Definitions for national indicators

31
Indicator 10: Percentage of pregnant women who were tested for HIV and received their results—during pregnancy, during labour and delivery, and during the post-partum period (<72 hours), including those with previously known HIV status
Identification of a pregnant woman’s HIV serological status provides an entry point for other services for the PPTCT of HIV and to tailor prevention, care and treatment to her needs.
This indicator measures the percentage of pregnant women who were tested for HIV and received their results.
Data should be collected continuously at the facility level and should be aggregated at least annually.
The numerator is calculated from national program records aggregated from facility registers for ANC, labour and delivery and postpartum care. Health facility registers should record known HIV infection in pregnant women coming to ANC clinics for a new pregnancy, so that they receive services for PMTCT of HIV. All public, private and NGO health care facilities that are providing testing and counselling for pregnant women should be included.
The denominator is derived from a population estimate of the number of pregnant women giving birth in the past 12 months. This can be obtained from estimates of births from the central statistics office or from the UNPD or pregnancy registration systems with complete data.
Number of pregnant women of known HIV status.
This is compiled from: 1. the number of women of unknown HIV serological status attending ANC, labour and
delivery and postpartum services, who have been tested for HIV and know their results and
2. women with known HIV infection attending ANC for a new pregnancy in the past 12 months.
The numerator is the sum of the four categories below:a) pregnant women who have an HIV test and receive the result during ANCb) pregnant women of unknown HIV serological status attending labour and delivery who
were tested and received resultsc) women of unknown HIV serological status attending postpartum services within 72
hours of delivery who were tested and received resultsd) pregnant women with known HIV infection attending ANC for a new pregnancy.
Pregnant (and postpartum) women of unknown serological status: women who were not tested during ANC or at labour and delivery for this pregnancy or who do not have documented proof of having been tested during this pregnancy.
Pregnant women with known HIV infection: women who were tested and confirmed to be HIV-positive at any time before the current pregnancy, who are attending ANC for a new pregnancy. These women do not need to be retested if there is documented proof of their positive status, in line with national guidelines on testing pregnant women. These women do, however, need services for the PMTCT of HIV and are counted in the numerator.
Estimated number of HIV-infected pregnant women who gave birth in the past 12 months. This is a proxy measure of the number of infants born to HIV-infected women.
Program monitoring.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Pregnancy stage (ANC, labour and delivery, post partum).Disaggregation
METHOD OF MEASUREMENT
Definitions for national indicators

32
To assess the construction, quality and utilisation of Family Support Centres (FSCs) in hospitals in all provinces and their progress in providing quality, coordinated services for survivors of family and sexual violence.
Data should be collected continuously at the facility level and should be aggregated quarterly. The third quarter data will be used for measuring the indicator annually.
Program monitoring tools such as client registers and summary reporting forms.
Number of FSCs which have referred at least three clients per month in the past quarter.
Not applicable.
Number of FSCs that refer clients to their partner organisations, which include Department of Justice and Attorney General, Family and Sexual Violence Action Committees and health services.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Not applicable.Disaggregation
METHOD OF MEASUREMENT
Indicator 11: Number of operational Family Support Centres
Violence against women, including gender-based violence, is among the important vulnerability factors putting many women at higher risk of HIV infection. It also hampers access by women to prevention, treatment and care services. Increasing the availability of services for survivors of violence can help them decrease their vulnerability to HIV as well as decrease the risk of repetition of violence.
Definitions for national indicators

33
This indicator measures the percentage of people who had an HIV test in the previous 12 months and received their result.
Every three to five years.
Population-based surveys (Demographic Health Survey, AIDS Indicator Survey, Multiple Indicator Cluster Survey or other representative survey).
Number of respondents aged 15–59 who have been tested for HIV during the last 12 months and who know their result.
Number of all respondents aged 15–59.
Respondents are asked:
1. I don’t want to know the results, but have you been tested for HIV in the last 12 months?
2. If yes: I don’t want to know the results, but did you get the result of that test?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 12: Percentage of women and men aged 15–59 who received an HIV test in the last 12 months and who know the result
In order to protect themselves and to prevent infecting others, it is important for individuals to know their HIV status. Knowledge of one’s HIV status enables regular monitoring of immune status and seeking treatment at the clinically appropriate time.
Definitions for national indicators

34
This indicator measures the percentage of MARPs who had an HIV test in the previous 12 months and received their result.
Every two to three years.
Behavioural surveillance or other special surveys.
Number of MARPs aged 15–59 who have been tested for HIV during the last 12 months and who know their result.
Number of all MARPs aged 15–59.
Respondents are asked:
1. I don’t want to know the results, but have you been tested for HIV in the last 12 months?
2. If yes: I don’t want to know the results, but did you get the result of that test?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Gender (man, woman, male-to-female transgender, female-to-male transgender).
Disaggregation
METHOD OF MEASUREMENT
Indicator 13: Percentage of MARPs that have received an HIV test in the last 12 months and know the result
In order to protect themselves and to prevent infecting others, it is important for MARPs to know their HIV status. Knowledge of one’s HIV status enables regular monitoring of immune status and seeking treatment at the clinically appropriate time.
The NHS defines MARPs as groups of people that have a common HIV risk behaviour and often some other defining characteristic, such as selling sex, and that have an existing rate of HIV infection. In PNG, MARPs include: women and men involved in sex work and transactional sex, men who have sex with men, migrant workers, enclave workers, prisoners, and mobile men with money (such as public servants, police, politicians, landowners, cash crop buyers and sellers, transport sector workers and business men). The populations who are more-at-risk vary over time as the dynamics of an epidemic change. In other countries the term ‘most’ at risk populations is generally used. There is currently insufficient epidemiological data in PNG to determine which populations are ‘most’ at risk so the term ‘more’ at risk has been used.
This indicator should be calculated separately for each population group considered more-at risk, like sex workers, injecting drug users and men who have sex with men.
Countries with generalised epidemics may also have a concentrated sub-epidemic(s) among one or more MARPs, making it valuable to report on this indicator.
Definitions for national indicators

35
This indicator measures the coverage of HIV testing among TB clinic clients.
Data should be collected continuously at the facility level and should be aggregated at least annually.
Program monitoring tools, such as client registers and summary reporting forms.
Number of TB clinic clients registered during a given time period who had an HIV test result recorded in the TB register.
Total number of TB clinic clients registered during the same time period.
Data for this indicator can be collected using national program records aggregated from facility registers; either the TB register or a separate HIV counselling and testing register. Where available, data should come from the national TB control program surveillance system and should include data from TB services delivered in public and private health care facilities and prisons, as well as from TB services delivered by FBOs and NGOs.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (0–4, 5–14, 15 and above). TB status (positive, negative).
Disaggregation
METHOD OF MEASUREMENT
Indicator 14: Percentage of TB clients who had an HIV test result recorded in the TB register
TB is the leading cause of morbidity and mortality among people living with HIV in many countries. In addition, high rates of HIV co-infection are found among TB patients in settings with high HIV prevalence. In these settings, ensuring that TB patients receive HIV counselling and testing services should be a high priority. Knowledge of HIV status enables HIV-positive TB patients to access the most appropriate HIV prevention, treatment, care and support services. Trends over time will demonstrate progress towards national and international targets.
Definitions for national indicators

36
This indicator measures the coverage of HIV testing among STI clinic clients.
Data should be collected continuously at the facility level and should be aggregated at least annually.
Program monitoring tools, such as client registers and summary reporting forms.
Number of STI clinic clients registered during a given time period who had an HIV test result recorded in the STI register.
Total number of STI clinic clients registered during the same time period.
Data for this indicator can be collected using national program records aggregated from facility registers; either the STI register or a separate HIV counselling and testing register. Where available, data should come from the national STI control program surveillance system and should include data from STI services delivered in public and private health care facilities and prisons, as well as from STI services delivered by FBOs and NGOs.
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female) Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59) STI status (positive, negative)
Disaggregation
METHOD OF MEASUREMENT
Indicator 15: Percentage of STI clients who had an HIV test
STIs are a factor in facilitating HIV transmission; moreover, people having any type of STI are at a higher risk of having HIV because of the same behaviours that put them at the risk of acquiring the other STI. HCT of clients at STI clinics is a strategic targeting of people at higher risk of being infected with HIV.
Definitions for national indicators

37
This indicator measures the percentage of people with advanced HIV infection receiving ART.
Data should be collected continuously at the facility level and should be aggregated at least annually.
For the numerator: facility-based ART registers or drug supply management systems.
For the denominator: HIV prevalence estimation models such as Spectrum.
Number of adults and children with advanced HIV infection who are currently receiving ART combination therapy in accordance with the nationally approved treatment protocol at the end of the reporting period.
Estimated number of adults and children with advanced HIV infection.
Program monitoring and HIV surveillance.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (0–14, 15 and above).Disaggregation
METHOD OF MEASUREMENT
Indicator 16: Percentage of adults and children with advanced HIV infection receiving ART
As the HIV epidemic matures, increasing numbers of people are reaching advanced stages of HIV infection. ART has been shown to reduce mortality amongst those infected. ARV combination therapy should always be provided in conjunction with broader care and support services including counselling for family caregivers.
Definitions for national indicators

38
This indicator measures the percentage of HIV-positive incident TB cases that received treatment for TB and HIV.
Data should be collected continuously at the facility level and should be aggregated at least annually.
Facility ART registers and reports; program monitoring tools.
Number of adults with advanced HIV infection who received ARV combination therapy in accordance with the nationally approved treatment protocol (or WHO-UNAIDS standards) and who were started on TB treatment (in accordance with national TB program guidelines), within the reporting year.
Estimated number of incident TB cases in people living with HIV.
Program data and estimates of incident TB cases in people living with HIV.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (0–14, 15 and above).Disaggregation
METHOD OF MEASUREMENT
Indicator 17: Percentage of estimated HIV-positive incident TB cases that received treatment for TB and HIV
TB is a leading cause of morbidity and mortality in people living with HIV, including those on ART. Intensified TB case-finding and access to quality TB treatment is essential for improving the quality and quantity of life for people living with HIV. A measure of the percentage of HIV-positive TB cases that access appropriate treatment for their TB and HIV is important.
Definitions for national indicators

39
To assess progress in increasing retention of PLHIV on ART and survival.
As PLHIV start ART, monthly cohort data should be collected continuously. Data for monthly cohorts that have completed at least 12/24/36/48 months of treatment should then be aggregated, at least annually.
Program monitoring tools; cohort and group analysis forms.
Number of adults and children who are alive and still on ART at 12/24/36/48 months after initiating treatment.
The numerator requires that adult and child patients must be alive and on ART at 12/24/36/48 months after their initiation of treatment. For a comprehensive understanding of retention and survival, the following data must be collected:
1. Number of adults and children in the ART start-up groups initiating therapy at least 12/24/36/48 months prior to the end of the reporting period.
2. Number of adults and children who are alive and still on ART at 12/24/36/48 months after initiating treatment.
(refer to: http://www.unaids.org/en/HIV_data/Methodology/default.asp
The numerator does not require patients to have been on ART continuously for the 12/24/36/48-month period. Patients who may have missed one or two appointments or drug pick ups, and temporarily stopped treatment during the 12/24/36/48 months since initiating treatment but are recorded as still being on treatment at month 12/24/36/48 are included in the numerator. However, those patients who have died, stopped treatment or been lost to follow up at 12/24/36/48 months since starting treatment are not included in the numerator.
For example, for a patient who started ART in May 2011: if at any point during the period May 2011 to May 2012 the patient dies, is lost to follow-up (and does not return), or stops treatment (and does not restart), then at month 12 (May 2012), the patient is not on ART, and not included in the numerator.
Conversely, a patient who started ART in May 2011 and who missed an appointment in June 2011, but is recorded as being on ART in May 2012 (at month 12) is on ART and will be included in the numerator. What is important is that the patient who started ART in May 2011 is recorded as alive and on therapy after 12 months, regardless of what happens from May 2011 to May 2012.
ART registers and ART cohort analysis report form.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
METHOD OF MEASUREMENT
Indicator 18: Percentage of adults and children with HIV known to be on treatment at 12/24/36/48 months after initiation of ART
One of the goals of any ART program is to increase survival among PLHIV. As provision of ART is scaled-up, it is important to understand why and how many people drop out of treatment programs. These data can be used to demonstrate the effectiveness of programs and highlight obstacles to expanding and improving them.
Definitions for national indicators

40
Total number of adults and children who initiated ART who were expected to achieve 12/24/36/48-month outcomes within the reporting period, including those who have died since starting therapy, those who have stopped therapy, and those recorded as lost to follow up at month 12/24/36/48.
The denominator is the total number of adults and children in the ART start-up groups who initiated therapy at any point during the 12/24/36/48 months prior to the beginning of the reporting period, regardless of their 12/24/36/48-month outcome. For example, for the reporting period 1 January to 31 December 2011, this will include all patients who started ART during the 12-month period from 1 January to 31 December 2010. This includes all patients, both those on ART as well as those who are dead, who have stopped treatment or are lost to follow up at month 12.
At the facility level, the number of adults and children on ART at 12/24/36/48 months includes patients who have transferred in at any point from initiation of treatment to the end of the 12-month period and excludes patients who have transferred out during this same period to reflect the net current cohort at each facility. In other words, at the facility level, patients who have transferred out will not be counted either in the numerator or the denominator. Similarly, patients who have transferred in will be counted in both the numerator and denominator.
At the national level, the number of transferred-in patients should match the number of transferred-out patients. Therefore, the net current cohort (the patients whose outcomes the facility is currently responsible for recording – the number of patients in the start-up group plus any transfers in, minus any transfers out) at 12/24/36/48 months should equal the number in the start-up cohort group 12/24/36/48 months prior.
Denominator
Sex (male, female). Age (0–14, 15 and above).Disaggregation
Definitions for national indicators

41
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
To assess progress in increasing the number of NGOs, FBOs and CBOs that submit their HIV plans and reports to NACS and PACS on time.
Quarterly and annually. The third quarter data will be used for national reporting.
NACS and PACS records or files of NGOs, FBOs and CBOs submitted HIV plans, activity progress reports and program indicator reports. There will be a numerator and denominator for submissions (plans and reports) to NACS and another set for PACS.
1. Number of NGOs, FBOs and CBOs that submit their HIV plans for grants of less than the financial cap to the PACS of the province they operate in, on time.
2. Number of NGOs, FBOs and CBOs that submit their reports for their HIV grants of less than the financial cap to the PACS of the province they operate in, on time.
3. Number of NGOs, FBOs and CBOs that submit their HIV plans for grants of over the financial cap to the NACS, on time.
4. Number of NGOs, FBOs and CBOs that submit their reports for their HIV grants of over the financial cap to the NACS, on time.
Total number of NGOs, FBOs and CBOs involved in the HIV response in each province.
NACS and PACS records, files and registers of the number of NGOs, FBOs and CBOs that submit their annual plans, activity progress reports and program indicator reports on time.
Agency type (FBO/NGO). Submission type (plan/report).Disaggregation
METHOD OF MEASUREMENT
Indicator 19: Percentage of NGOs, FBOs and CBOs submitting their plans and reports to their PACS or NACS on time
Under the NHS, coordination will be strengthened to ensure all agencies align their plans with NACS and PACS and report on a specified periodic basis.
NGOs, FBOs and CBOs will continue to submit reports to their respective funding agencies and headquarters, in addition to this required reporting to PACS. Submitting plans and reports to PACS ensure one national reporting system for HIV and AIDS, which is consistent with the third principle of the three-ones principles.
The current practice is that CBOs submit their plans for grants of up to K300,000 to PACS, and plans for grants of more than K300,000 to NACS.
NACS and all PACS M&E focal points will develop and keep up-to-date a database of all NGOs, FBOs and CBOs.
Definitions for national indicators

42
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
To assess the progress in deploying more TA to the sub-national level
Annually – data should be collected continuously and should be aggregated annually.
Donors, development partners and NACS respective records, registers and reports.
The total monetary cost of TA deployed to the sub-national level to support the NHS implementation.
The total monetary cost of TA provided in the country.
PACS and NACS will require development partners that fund TA to provide an annual update on the placement of TAs (as per the disaggregation categories below).
Duration of TA (less than four weeks; four to 12 weeks; more than 12 weeks).Disaggregation
METHOD OF MEASUREMENT
Indicator 20: Percentage of technical assistance (TA) deployed to support the NHS implementation at sub-national level compared to the total TA
Since the first case of AIDS in PNG was identified in 1987, TA has steadily increased. It has increasingly become evident that a large proportion of TA is provided at the national level, with insufficient TA at the sub-national level.
One of the strategies of the NHS is to ensure a significant increase in the TA provided at the sub-national level. NACS will keep an up-to-date database of TA provided for the HIV and AIDS response so as to be in a position to measure the proportion of TA provided at national and sub-national levels.
Definitions for national indicators

43
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
To assess the extent to which provinces are implementing their HIV service responsibilities under the PLLSMA Determination on Service Delivery.
Annually.
Provincial Coordinating and Monitoring Committee reports submitted to PLLSMA by provincial governments.
Number of provincial governments that report to PLLSMA on their specific HIV responsibilities under the Determination on Service Delivery.
Total number of provinces.
Provincial government data on which agencies are providing which HIV and AIDS services and levels of funding.
Not applicable.Disaggregation
METHOD OF MEASUREMENT
Indicator 21: Percentage of provincial governments that report to PLLSMA on their specific HIV responsibilities under the Determination on Service Delivery
The Department of Provincial and Local Government Affairs (DPLGA) has, by way of an National Executive Committee Determination, delineated and assigned the service delivery functions and responsibilities for provincial and local-level governments. The Determination identifies what services each level of government is accountable for and who is responsible for funding. The HIV services to be provided by different sectors – such as health, education and community development – is also delineated. The Determination also includes development of policies and plans such as district HIV and AIDS plans.
National-level coordination and monitoring of the implementation of national policies and programs is overseen by the PLLSMA, which was established under the DPLGA. Each province has established a Provincial Coordinating and Monitoring Committee which brings together the provincial government, businesses and civil society groups to monitor progress in implementing programs and improving services. The PACS and sectors responsible for providing HIV and AIDS services under the Determination report to these Committees in regards to their provincial-level response to HIV and AIDS.
Definitions for national indicators

44
To assess progress in reducing HIV infection.
Annual.
WHO guidelines for HIV sentinel surveillance or PPTCT program data.
Number of antenatal clinic attendees tested whose HIV test results are positive.
Number of antenatal clinic attendees tested for HIV.
This indicator is calculated using data gathered from pregnant women attending antenatal clinics in HIV sentinel surveillance sites in the capital city, other urban areas and rural areas.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49).Disaggregation
METHOD OF MEASUREMENT
Indicator 22: Percentage of women and men who are HIV infected
A key goal of the NHS is to reduce transmission of HIV.
Definitions for national indicators

45
To assess progress on reducing HIV prevalence among MARPs.
Every two to three years.
Repeated biological or integrated bio-behavioural surveys among MARPs.
Number of members of the MARP who test positive for HIV.
Number of members of the MARP tested for HIV.
This indicator is calculated using data from HIV tests conducted among members of MARP groups in the primary sentinel site or sites.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49).Disaggregation
METHOD OF MEASUREMENT
Indicator 23: Percentage of MARPs who are HIV infected
MARPs typically have the highest HIV prevalence in countries with either concentrated or generalised epidemics. In many cases, prevalence among these populations can be more than double the prevalence among the general population. Reducing prevalence among MARPs is a critical measure of a national-level response to HIV.
The NHS defines MARPs as groups of people that have a common HIV risk behaviour and often some other defining characteristic, such as selling sex, and that have an existing rate of HIV infection. In PNG, MARPs include: women and men involved in sex work and transactional sex, men who have sex with men, migrant workers, enclave workers, prisoners and mobile men with money (such as public servants, police, politicians, landowners, cash crop buyers and sellers, transport sector workers and business men). The populations more-at-risk vary over time as the dynamics of an epidemic change. In other countries the term ‘most’ at risk populations is generally used. There is currently insufficient epidemiological data in PNG to determine which populations are ‘most’ at risk so the term ‘more’ at risk has been used.
This indicator should be calculated separately for each population that is considered more-at-risk.
Countries with generalised epidemics may also have a concentrated sub-epidemic among one or more MARP, making this an important indicator. If so, it would be valuable for them to calculate and report on this indicator for those populations.
Definitions for national indicators

46
To collect accurate and consistent data on how funds are spent and where those funds are sourced.
Every two to three years.
Primary tool/method: National AIDS Spending Assessment
Alternative tools/methods:
1. National Health Accounts – AIDS sub-accounts: There should not be any difference in the AIDS health spending measured by NASA or by the National Health Accounts sub-accounts. However, activities performed outside the health system might not be included in National Health Accounts.
2. Resource Flows Survey: Some activities performed outside the health system might not be included in this Resource Flows Survey. In addition, some population-related actions should be excluded from the total for AIDS.
The outputs from any of these measurement tools are to be used to complete the National Funding Matrix.
Actual expenditures classified by eight AIDS spending categories and by financing source, including public expenditure from its own sources (that is, government revenues such as taxes) and from international sources:
1. Prevention2. Care and treatment3. Orphans and vulnerable children4. Program management and administration strengthening5. Incentives for human resources6. Social protection and social services (excluding orphans and vulnerable children)7. Enabling environment and community development8. Research (excluding operations research included under program management).Three main groups of financing sources:1. Domestic public2. Domestic private3. International
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
METHOD OF MEASUREMENT
Indicator 24: Domestic and international AIDS spending by categories and financing sources
As the national response to HIV and AIDS continues to scale up, it is increasingly important to accurately track in detail how funds are spent and where the funds originate. The data are used to measure PNG’s commitment and action, which is an important component of the country’s obligations under the UNGASS Declaration of Commitment on HIV/AIDS. In addition, the data help national-level decision makers monitor the scope and effectiveness of programs. This piece of strategic information also supports the coordination role of NACS and provides the basis for resource allocation and improved strategic planning processes. When aggregated across multiple countries, the data also help the international community evaluate the status of the global response.
Not applicable.Numerator
Not applicable.Denominator
Not applicable.Disaggregation
Definitions for national indicators

47
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
To assess progress in the development and implementation of national-level HIV and AIDS policies, strategies and laws.
Every two years.
National Composite Policy Index questionnaire.
The National Composite Policy Index questionnaire is divided in two parts which cover the following areas:
Part A – to be administered to government officials:
1. Strategic plan2. Political support3. Prevention4. Treatment, care and support5. M&E.
Part B – to be administered to representatives from civil society organisations, bilateral agencies, and UN organisations:
1. Human rights2. Civil society involvement3. Prevention4. Treatment, care and support.
Some questions are asked in both Part A and Part B to ensure that the views of both the national government and non-government respondents, whether in agreement or not, are obtained.
Each section should be completed by (a) conducting a desk review of relevant documents and (b) interviewing key people most knowledgeable about the topic.
It is important to fully complete the National Composite Policy Index by checking the relevant standardised responses and providing further information in the open text boxes, where requested. This will facilitate a better understanding of the current situation, provide examples of good practice for others to learn from, and pinpoint some issues for further improvement.
METHOD OF MEASUREMENT
Indicator 25: National Composite Policy Index (areas covered: prevention, treatment, care and support, human rights, civil society involvement, gender, workplace programs, stigma and discrimination and M&E)
An effective national response to the HIV epidemic is only achievable in a supportive and conducive environment. Such an environment includes different elements ranging from over-arching issues like human rights and stakeholder participation in the national response at all levels, to more specific programming issues. Monitoring the evolving policy environment helps the stakeholders at the national level to identify the weaknesses and strengths of the supportive environment and to take remedial action as needed.
Definitions for national indicators

48
Numerator Not applicable.
Denominator Not applicable.
Not applicable.Disaggregation
National Composite Policy Index responses reflect the overall policy, strategy, legal and program implementation environment of the HIV response. The open text boxes provide an opportunity to comment on issues that are perceived as important but that are insufficiently captured in the questions (for example, important sub-national variations; the level of implementation of strategies, policies, laws or regulations; explanatory notes; comments on data sources). In general, draft strategies, policies, or laws are not considered to be ‘in existence’ so questions about whether such a document exists should be answered with a ‘no’. It is, however, useful to state that such documents are in draft form in the relevant open text box.
Definitions for national indicators

49
To measure the extent and forms of stigma and discrimination faced by people living with HIV.
Every three years.
People Living with HIV Stigma Index.
Not applicable.
Not applicable.
As detailed in the Stigma Index guidelines.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Not applicable.Disaggregation
METHOD OF MEASUREMENT
Indicator 26: The degree of stigma and discrimination as identified by the People Living with HIV Stigma Index
People living with HIV often face stigma and discrimination. Many do not know what their rights are and how they can help to change things for the better. There are a number of organisations that are campaigning against stigma and discrimination and fighting for improved rights for people living with HIV. This index aims to collect information on stigma, discrimination and the rights of people living with HIV that will help in these advocacy efforts.
Definitions for national indicators

50
This indicator measures the availability of PEP in health care facilities.
Annual for program records; every 2 to 3 years for facility survey/census.
For health-facility surveys or censuses, tools such as the Service Provision Assessment (SPA) or the Service Availability Mapping (SAM) can be used.
Number of health care facilities with PEP available for those who are at risk of HIV infection through occupational and/or non-occupational exposure to HIV.
Total number of health care facilities.
Percentage of health care facilities with PEP services available for those at risk of HIV infection through occupational and/or non-occupational exposure to HIV. Health care facilities include public and private facilities, health centres and clinics (including TB centres), as well as health care facilities that are run by FBOs or NGOs.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Type of health facility (government, FBO, NGO, private).Disaggregation
METHOD OF MEASUREMENT
Indicator 27: Percentage of health care facilities with post-exposure prophylaxis available
Post-exposure prophylaxis (PEP) reduces the probability of HIV infection after exposure to potentially HIV-infected blood or body fluids. For maximum effectiveness, PEP should be provided as soon as possible after exposure and no later than 72 hours following exposure. PEP may be provided following occupational exposure (for example, in healthcare facilities) or non-occupational exposure (such as after sexual assault).
Within the health sector, PEP should be provided as part of a comprehensive standard precautions package that reduces staff and patient exposure to infectious hazards. PEP for non-occupational exposure should be considered for sexual assault survivors, particularly in high HIV-prevalence settings.
Definitions for national indicators

51
To measure the percentage of donated blood units screened for HIV in a quality-assured manner.
Annual.
FRAME Tool (Framework for Assessment, M&E of blood transfusion services): a rapid assessment tool used by the WHO Global Database on Blood Safety.
The information relates to data from the previous 12 months (January to December). It should be available from the National Blood Transfusion Service or the officers responsible for the National Blood Program in NDoH.
The following information is required to measure this indicator:
• The total number of blood units that were donated in the country.• For each blood centre and blood screening laboratory that screens donated blood
for HIV:1. The number of units of blood donated in each blood centre/blood screening
laboratory2. The number of donated units screened in the blood centre/blood screening
laboratory3. If the blood centre/blood screening laboratory followed documented standard
operating procedures for HIV screening4. If the blood centre/blood screening laboratory participated in an External Quality
Assessment Scheme for HIV screening.
From this information, the indicator can be calculated.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
METHOD OF MEASUREMENT
Indicator 28: Percentage of donated blood units screened for HIV in a quality assured manner
Blood safety programs aim to ensure that all blood units are screened for transfusion-transmissible infections, including HIV, and that only those units that are non-reactive on screening tests are released for clinical use.
Universal (100%) screening of donated blood for HIV and other transfusion-transmissible infections cannot be achieved without mechanisms to ensure quality and continuity in screening. Interruptions to supplies of test kits and reagents, or emergency situations, can result in the use of blood for transfusion without screening for transfusion-transmissible infections. The development of systems for reliable and regular supplies of low-cost, high-quality test kits and reagents as well as effective stock management are therefore essential to ensure universal quality screening of blood units. Thus, it is crucial that all donated blood units be screened for HIV in a quality-assured manner.
The following methodologies are two key components of quality assurance in screening:
1. The use of documented and standardised procedures (standard operating procedures) for the screening of every blood unit.
2. Participation of the laboratories in an external quality assessment scheme for HIV screening in which external assessment of the laboratory’s performance is conducted using samples of known, but undisclosed, content to assess its quality system and assist in improving standards of performance.
Definitions for national indicators

52
Number of donated blood units screened for HIV in a quality assured manner. For the purposes of data collection screening in a quality assured manner is defined as screening performed in blood centres/blood screening laboratories that:
1. follow documented standard operating procedures and 2. participate in an external quality assurance scheme.
Numerator
Total number of blood units donated.
In this context, donation refers to any blood collected for the purposes of medical use. This includes all possible types of providers of blood, regardless of whether they receive remuneration or not.
Denominator
Not applicable.Disaggregation
Definitions for national indicators

53
To measure the percentage of schools providing life skills-based HIV education.
Every two years.
School survey or education program review.
Number of schools that provided life skills-based HIV education in the most recent academic year.
Number of schools surveyed.
Principals/heads of a nationally-representative sample of schools (both private and public) are briefed on the meaning of life skills-based HIV education and then asked the following question:
Within the most recent academic year, did your school provide at least 30 hours of life-skills training to each grade?
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Level (primary, secondary).Disaggregation
METHOD OF MEASUREMENT
Indicator 29: Percentage of schools that provided life skills-based HIV education within the most recent academic year
Life skills-based education is an effective methodology that uses participatory exercises to teach behaviours to young people that help them deal with the challenges and demands of everyday life. It can include decision-making and problem-solving skills, creative and critical thinking, self-awareness, communication and interpersonal relations. It can also teach young people how to cope with their emotions and causes of stress.
When adapted specifically for HIV education in schools, a life skills-based approach helps young people understand and assess the individual, social and environmental factors that raise and lower the risk of HIV transmission. When implemented effectively, it can have a positive effect on behaviours, including delay in sexual debut and reduction in the number of sexual partners.
Definitions for national indicators

54
To measure the coverage of HIV prevention programs for MARPs.
Every two to three years.
Behavioural surveillance or other special surveys.
Number of MARP respondents who replied ‘yes’ to both (all three for injecting drug users) questions.
Total number of respondents surveyed.
Respondents are asked the following questions:
1. Do you know where you can go if you want to have an HIV test?2. In the last 12 months, have you been given condoms (for example, through an
outreach service, drop-in centre or sexual health clinic)?Injecting drug users should be asked the following additional question:3. In the last 12 months, have you been given sterile needles and syringes (for example,
by an outreach worker, a peer educator or through a needle exchange program)?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Gender (man, woman, male-to-female transgender, female-to-male transgender).
Disaggregation
METHOD OF MEASUREMENT
Indicator 30: Percentage of MARPs reached with HIV prevention programs
MARPs are often difficult to reach with HIV prevention programs. However, in order to prevent the spread of HIV among these populations as well as into the general population, it is important that they access these services.
The NHS defines MARPs as groups of people that have a common HIV risk behaviour and often some other defining characteristic, such as selling sex, and that have an existing rate of HIV infection. In PNG, MARPs include: women and men involved in sex work and transactional sex, men who have sex with men, migrant workers, enclave workers, prisoners and mobile men with money (such as public servants, police, politicians, landowners, cash crop buyers and sellers, transport sector workers and business men). MARPs vary over time as the dynamics of an epidemic change. In other countries the term ‘most’ at risk populations is generally used. There is currently insufficient epidemiological data in PNG to determine which populations are ‘most’ at risk so the term ‘more’ at risk has been used.
This indicator should be calculated separately for each population that is considered more-at-risk. Countries with generalised epidemics may also have a concentrated sub-epidemic among one or more MARPs so this is an important indicator.
Definitions for national indicators

55
To measure the number of district health care facilities providing ART.
Annual for program records; every 2 to 3 years for facility survey/census.
For health facility surveys or censuses, tools such as SPA or SAM can be used.
Number of health care facilities at district level that offer ART (that is, prescribe and/or provide clinical follow up).
Not applicable.
Number of health care facilities at district level that offer ART (that is, prescribe and/or provide clinical follow up). Health care facilities include public and private facilities, health centres and clinics (including TB centres), as well as health care facilities run by FBOs or NGOs.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Type of health facility (government, FBO, NGO, private). Type of ART service (prescription, clinical follow up).Disaggregation
METHOD OF MEASUREMENT
Indicator 31: Number of district level ART sites
ART is a cornerstone of effective HIV treatment, and measuring the percentage of health care facilities that offer ART provides valuable information about ART availability. One strategy to scale-up ART services is to make ART available in more health care facilities. This may be achieved by decentralising ART services from tertiary facilities (for example, hospitals) to primary- and secondary-level health care facilities.
Definitions for national indicators

56
To improve availability of quality paediatric ART services in all ART sites.
Data will be collected routinely through the monthly ART collection forms.
Numerator: This will be collected continuously through the monthly ART data form submitted by sites. This form has variables for age groups that indicate whether the site is providing ART to children
Denominator: This will be collected in the same way as for the numerator.
Number of ART sites providing paediatric ART.
Number of ART sites providing both adult and paediatric ART services.
Routine monthly program reports.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Public and private.Disaggregation
METHOD OF MEASUREMENT
Indicator 32: Percentage of health care facilities that offer paediatric ART (that is, prescribe and provide clinical follow up)
Scale-up of paediatric ART has lagged behind ART scale up for adults. It is important that both adult and paediatric ART services are provided in all facilities that are delivering ART. Where paediatricians are not available, it is important to encourage and support health care workers trained in integrated management of adolescent and adult illness to provide paediatric ART to all eligible children.
Definitions for national indicators

57
To measure the coverage of cotrimoxazole CTX prophylaxis for HIV-exposed infants in line with international guidelines.
Annual.
Numerator: facility-based records, such as integrated maternal and child health registers, HIV-exposed infant follow-up registers, or pre-ART registers.
Denominator: ANC surveillance, Spectrum, published estimates (for example, estimates from the UNDP).
Number of infants born to HIV-infected women in the last 12 months started on CTX prophylaxis within two months of birth.
Estimated number of HIV-infected pregnant women giving birth in the last 12 months.
Data for the numerator should be aggregated from the appropriate facility registers, which could include integrated maternal and child health registers, HIV-exposed infant follow-up registers, or pre-ART registers.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male; female).Disaggregation
METHOD OF MEASUREMENT
Indicator 33: Percentage of infants born to HIV-infected women who are started on Cotrimoxazole prophylaxis within two months of birth
Cotrimoxazole (CTX) prophylaxis is a simple and cost-effective intervention to prevent pneumocystis jiroveci pneumonia (PCP) among HIV-exposed and HIV-infected infants. PCP is the leading cause of serious respiratory disease in young HIV-infected infants in resource-constrained countries, and it often occurs before HIV infection can be diagnosed. Because of the difficulties in diagnosing HIV-infection in young infants, all infants born to HIV-infected women should receive CTX prophylaxis, starting at 4 to 6 weeks after birth and continuing until HIV infection has been excluded and the infant is no longer at risk of acquiring HIV through breastfeeding.
Definitions for national indicators

58
To enhance the availability of STI screening and syndromic management.
All patients with STI symptoms and/or risk factors will be screened and data will be recorded and continuously reported to NHIS at NDOH. The data will be aggregated annually.
Numerator: collected routinely by NHIS.
Denominator: collected routinely by NHIS.
Number of all health care facilities providing STI screening and syndromic management.
Total number of health care facilities in the country.
Quarterly program data.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Private/public.Disaggregation
METHOD OF MEASUREMENT
Indicator 34: Percentage of health care facilities that provide STI screening and syndromic management
It is crucial that all health care facilities provide STI screening and syndromic management or refer all individuals with risk factors and/or STI symptoms to appropriate services. Currently, not all facilities are providing these services to patients. Given the link between HIV and STI, it is important that STI services are provided in all healthcare facilities or through referrals.
Definitions for national indicators

59
To support the continuum of prevention to care and treatment.
Data should be collected quarterly at the facility level and should be aggregated at least annually.
Numerator: This will be collected through supervisory visits and aggregated annually.
Denominator: This will be collected through quarterly reports.
Program reports.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Number of ART sites linked to HBC and family and community services.Numerator
Total number of ART sites.Denominator
Public; private; FBOs.Disaggregation
METHOD OF MEASUREMENT
Indicator 35: Percentage of ART sites that are linked to HBC and other family and community support services
Linking patients on ART to HBC and family and community support is critical to the provision of comprehensive care and support. It also helps to promote HIV treatment adherence, which in turn improves quality of life and limits the development of drug resistance. HBC and family support also help to minimise HIV-related stigma and discrimination and facilitates community access to services.
Definitions for national indicators

60
To ensure HIV prevention, care and treatment services are provided directly to HIV-positive individuals in a timely manner or through referrals to other services.
Data will be collected continuously at the facility level and will be aggregated at least annually.
Numerator: The number will be collected from the monthly HCT report form (Survey 1). The numerator is calculated from national program records, aggregated from facility rapid test log books for ANC, labour and delivery and postpartum care; STI, TB, VCT, outpatients/inpatients, blood donors etc. All public, private, FBO and NGO health care facilities and standalone services that are providing testing and counselling should be included.
Denominator: The total number of reporting sites providing HIV counselling and testing.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Number of HCT sites implementing POC – HIV confirmation testing.Numerator
Total number of HCT sites.Denominator
Public; private; FBOs.Disaggregation
Program monitoring.
METHOD OF MEASUREMENT
Indicator 36: Percentage of HCT sites using the 2009 national point-of-care algorithm
Provision to clients of their HIV test results on the same day as testing will minimise loss to follow up.
Definitions for national indicators

61
To assess progress towards universal knowledge of the essential facts about HIV transmission.
Every three to five years.
Youth survey, Demographic and Health Survey, other related surveys.
Number of respondents who gave the correct answer to all five questions.
Number of all respondents.
This indicator is constructed from responses to the following set of prompted questions:
1. Can the risk of HIV transmission be reduced by having sex with only one uninfected partner who has no other partners?
2. Can a person reduce the risk of getting HIV by using a condom every time they have sex?
3. Can a healthy-looking person have HIV?4. Can a person get HIV from mosquito bites?5. Can a person get HIV by sharing food with someone who is infected?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Numerator
Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59).Disaggregation
METHOD OF MEASUREMENT
Indicator 37: Percentage of women and men who both correctly identify ways of preventing the sexual transmission of HIV and who reject major misconceptions about HIV transmission
HIV epidemics are primarily perpetuated through sexual transmission of infection. Sound knowledge about HIV is an essential prerequisite – albeit, often an insufficient condition – for adoption of behaviours that reduce the risk of HIV transmission.
Definitions for national indicators

62
To assess progress in building knowledge of the essential facts about HIV transmission among MARPs.
Every two to three years.
Special behavioural surveys such as the FHI BSS for MARPs.
Respondents are asked the following five questions:
1. Can having sex with only one faithful, uninfected partner reduce the risk of HIV transmission?
2. Can using condoms reduce the risk of HIV transmission?3. Can a healthy-looking person have HIV?4. Can a person get HIV from mosquito bites?5. Can a person get HIV by sharing a meal with someone who is infected?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Number of MARP respondents who gave the correct answers to all five questions.Numerator
Number of MARP respondents who gave answers, including ‘don’t know’, to all five questions.Denominator
Sex (male, female). Age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59). Gender (men, women, male-to-female transgender, female-to-male transgender).
Disaggregation
METHOD OF MEASUREMENT
Indicator 38: Percentage of MARPs who both correctly identify ways of preventing the sexual transmission of HIV and who reject major misconceptions about HIV transmission
Sound knowledge about HIV and AIDS is an essential prerequisite if people are going to adopt behaviours that reduce their risk of infection.
The NHS defines MARPs as groups of people that have a common HIV risk behaviour and often some other defining characteristic, such as selling sex, and that have an existing rate of HIV infection. In PNG, MARPs include: women and men involved in sex work and transactional sex, men who have sex with men, migrant workers, enclave workers, prisoners and mobile men with money (such as public servants, police, politicians, landowners, cash crop buyers and sellers, transport sector workers, and business men). The populations who are more-at-risk vary over time as the dynamics of an epidemic change. In other countries the term ‘most’ at risk populations is generally used. There is currently insufficient epidemiological data in PNG to determine which populations are ‘most’ at risk so the term ‘more’ at risk has been used.
This indicator should be calculated separately for each population that is considered more-at-risk. Countries with generalised epidemics may also have a concentrated sub-epidemic among one or more MARPs.
Definitions for national indicators

63
To assess progress in increasing the age at which young women and men aged 15–24 first have sex.
Every three to five years.
Youth survey, Demographic and Health Survey, other related surveys.
Respondents are asked whether or not they have ever had sexual intercourse and, if yes, they are asked: How old were you when you first had sexual intercourse for the first time?
See Appendix 1 – Inventory of standardised questions to be included in surveys measuring national indicators.
PURPOSE
DATA COLLECTION FREQUENCY
MEASUREMENT TOOL
Number of respondents (aged 15–24 years) who report the age at which they first had sexual intercourse as under 15 years.Numerator
Number of all respondents aged 15–24 years.Denominator
Sex (male, female). Age (15–19, 20–24).Disaggregation
METHOD OF MEASUREMENT
Indicator 39: Percentage of young women and men who have had sexual intercourse before the age of 15
One HIV prevention strategy is to delay the age at which young people first have sex and discourage premarital sexual activity because it reduces their potential exposure to HIV. There is also evidence to suggest that first having sex at a later age reduces susceptibility to infection per act of sex, at least for women.
Definitions for national indicators

64
Strategic information needs not addressed through national indicators
The NHS has an emphasis on generating and using evidence to guide all programs. While a good deal of strategic information will be collected by the national indicators, additional evidence will be needed. Table 2 lists major activity areas from the NHS Implementation Framework where additional strategic information is needed, beyond what will be collected by the national indicators. Research topics related to these major activities will be included in a revised National Research Agenda (NRA) for the NHS 2011–2015. The first 21 activities in Table 2, which are highlighted in light green, are of a higher priority.
In addition, the NHS has placed an emphasis on the importance of operations research. This will be reflected in the NRA, including a focus on developing capacity for operations research.
(Note: in Table 2, in the column ‘NHS Strategic Objective’, I, II and III refers to NHS Priority areas 1, 2 and 3. For example, I–1.1.2 refers to Priority area 1: Prevention, and Strategic objective 1.1.2.)
I – 1.1.2
I – 1.1.4
I – 1.1.9
NHS strategic objective
NHS Implementation Framework major activity areas
Identify and address the barriers (including gender- and age-related barriers) to effective condom promotion, including working with churches, to advocate the importance of condoms as a tool for the prevention of HIV, STIs and for family planning.
Conduct social research on concurrent sexual relationships to guide programming.
Conduct regular reviews of evidence for HIV-related, high-risk behaviours to determine who are the more-at-risk populations in PNG.
I – 1.1.10 Identify and address barriers to PLHIV accessing sexual and reproductive health services.
Table 2: NHS Implementation Framework—major activity areas where additional strategic information is needed
I – 1.4.3 Expand surveillance to establish a clearer understanding of the extent that injecting drug use is practised and undertake socio-behavioural research to understand data on injecting drug use, its contexts of use and meanings, what is being used, why it is being used, and whether this is a significant mode of HIV transmission.
Strategic information needs not addressed through national indicators

65
I – 2.1.2 Review existing gender-based violence, sexual violence and related intervention programs and identify and disseminate lessons learned, with reference to the Family and Sexual Violence Action Strategy and including a clearing house on resources.
I – 2.4.1 Conduct social research to identify HIV vulnerabilities of more-at-risk populations and use this information to inform interventions.
I – 2.4.4 Develop criteria for ‘mobile men with money’ based on social and behavioural research.
I – 2.5.2 Undertake research to explore the links between sexual risk for males and females in relation to the transportation and sale of buai.
I – 3.2.3 Undertake HIV impact assessments for all current and future economic developments (for example, LNG, mines, plantations, fisheries) and develop and implement appropriate interventions for workforces and surrounding communities.
II – 2.1.1 Review and strengthen existing ART services, including an analysis of gender-linked factors affecting access and adherence.
II – 2 .1.9 Strengthen the capacity for monitoring drug resistance.
II – 2.3.1 Conduct periodic microbial resistance studies for STIs and review and implement recommended changes in national guidelines.
II – 2.3.3 Conduct research on STI health seeking behaviours to increase uptake of STI services.
II – 2.4.7 Identify the requirements of PLHIV support groups for specific populations such as women, young people, men who have sex with men, sex workers, men and sero-discordant partners, and establish groups as needed.
II – 2.4.8 Identify and document the barriers for PLHIV and their families in accessing education, training and vocational skills building.
III – 1.1.2 Undertake a comprehensive review of all ProMEST, starting with higher prevalence provinces, to identify critical gaps and weaknesses and develop appropriate actions to strengthen the effectiveness of each ProMEST.
III – 1.3.2 Revise the priority research areas of the NRA to include research on men and women’s sexuality and sexual beliefs, roles and practices.
III – 2.1.1 Trial, review and share learning from existing or pilot interventions that address gender-related vulnerabilities.
NHS strategic objective
NHS Implementation Framework major activity areas
III – 2.4.2 Review and remedy barriers to the effective utilisation of the HAMP Act.
III – 2.5.4 Trial and implement evidence-informed, gender-sensitive interventions which reduce stigma and discrimination within communities, initially in high prevalence or highly stigmatising communities, and particularly focused on addressing higher levels of stigma toward HIV positive women.
Strategic information needs not addressed through national indicators

66
I – 1.1.9 Conduct periodic size estimations of more-at-risk groups are undertaken.
I – 1.4.1 Conduct targeted social research and surveillance on penile modification practices.
I – 1.4.2 Conduct targeted social research and surveillance on tattooing, piercing and scarification practices and the contexts of their use (ethnicity, identity, as part of initiation).
I – 1.4.2 Develop evidence-informed harm reduction interventions that reduce the risks of HIV transmission for males and females associated with tattooing, piercing and scarification, particularly in cultural groups, work places and institutional environments (for example, prisons, uniformed services, schools).
I – 1.4.4 Conduct targeted social research and surveillance on vaginal drying practices and use of sexual enhancement products.
I – 2.1.6 Review, initiate and disseminate social research that examines the HIV vulnerabilities associated with specific cultural practices.
I – 2.1.6 Establish and share the learning from HIV prevention and care programs that use positive cultural practices to reduce vulnerabilities to HIV.
I – 2.5.1 Implement research-informed pilot programs to reduce drug and alcohol use are established in communities, institutions and workplaces for specific age, gender and more-at-risk groups (MSM, FSW, PLHIV).
II – 1.1.8 Pilot and review initiatives that promote increased access and uptake of HCT of men, women, transgendered and young people.
II – 2.1.10 Develop, trial and implement a range of interventions and tools to improve treatment adherence (for example, counselling services, nutrition support, treatment companions, preventing drug stock outs, use of mobile phones, pill boxes).
II – 2.4.5 Develop and implement a needs assessment tool to determine the scope of psycho-social needs of PLHIV and people affected by HIV.
II – 2.4.5 Develop and implement a needs assessment tool to determine the nutrition needs of PLHIV.
III – 1.3.1 Conduct periodic risk and vulnerability assessment surveys for different geographical as well as specific population groups and develop risk and vulnerability profiles for each of them.
III – 1.3.1 Conduct population size-estimation exercises for the groups found to have higher risks and vulnerabilities.
III – 1.3.3 Conduct periodic assessments of the capacity of research institutions and other possible partners for conducting social, socio-economic and behavioural research based on the NRA priorities and develop and implement a capacity development plan.
III – 1.3.4 Conduct an assessment across major service providers (for example, key government departments, large NGOs and FBOs) regarding their internal operational research capacity and identify TA needs.
III – 2.1.8 Commission research to review the level of participation of men and women on NAC, PACs and DACs.
NHS strategic objective
NHS Implementation Framework major activity areas
Strategic information needs not addressed through national indicators

67
Guidelines for developing program monitoring and evaluation plans based on the National Monitoring and Evaluation Framework
M&E plans for national programs like counselling and testing, care and treatment, and prevention of HIV in target groups such as students, out-of-school children or MARPs should be based on the internal logical framework of inputs, outputs and outcomes. However, to ensure the harmonisation of all M&E activities and alignment of the M&E of specific programs with the National M&E Framework, the following issues need to be considered when developing M&E plans at the program level:
1. Population impact and behavioural-level indicators at the program level should use the national indicators contained in this framework. If the program planners strongly believe they need other population impact and behavioural-level indicators, data collection for those indicators should be aligned with the data collection for the national indicators through the surveys already envisaged in this framework.
2. For output and other indicators developed as part of a program’s logical framework, national indicators and/or the additional indicators in Appendix II should be used. When using national indicators, programs should use the definitions contained in this framework. When designing any additional indicators, programs should keep be guided by the structure of definitions for the national indicators and draw on concepts contained in those definitions, as appropriate.
3. All national programs should use the data flow mechanisms provided in this framework. If there are special needs to add to or change the flow of data, this has to be approved by one of the M&E or STWG.
4. Generally speaking, national programs should not have more than 20 indicators in addition to those that apply from the list of national indicators.
The M&E and surveillance technical working groups will provide technical support to the NACS ICME and NDoH Surveillance Unit in developing M&E for non-health and health sector programs.
Guidelines for developing program monitoring and evaluation plans based on the National Monitoring and Evaluation Framework

68
Appendix I
Inventory of questions to be included in surveys for measuring national indicators
Data for measuring a significant number of the national indicators have to be collected through population or special surveys.
To be able to measure these indicators reliably over time and through different surveys, there is a clear need for a set of standardised questions for each indicator. In addition, questions for age, which is the main demographic attribute, need to be standardised to allow for comparison of results across different surveys. A list of standardised questions for national indicators that will be measured through population or special surveys is provided below. The numbers of those national indicators that will be measured by using these standardised questions have been supplied. Survey designers are encouraged to use these standardised questions in their questionnaires. For many of the indicators, the suggested questions are drawn from international guidelines.
It should be noted that not all of the questions are meant to be included in the one survey. Some of the questions are for general and youth population surveys and others are for special surveys among MARPs. Moreover, using one set of questions might mean others in this standardised list of questions are not needed. It is up to the survey design team, in consultation with the STWG, to choose the indicators they want to measure and determine which standardised questions should be used.
Use these questions for all indicators where disaggregation by age is needed
Age1. Do you know your exact birth month and year? If yes, can you tell me the
month and year of your birth? (if no answer go to the next question)2. Do you know your birth year? If yes, can you tell me your birth year?
(if no answer go to the next question)3. Do you know how old are you? Can you tell me your age?
(if no answer go to the next question)4. Can you tell me which of the following age groups you are in? Less than 15, 15–19, 20–24, 25–29, 30–34, 35–39, 40–45, 45–49, 50–54,
55–59, 60 and above (if no answer go to the next question)5. Can you tell me which of the following age groups you are in? Less than 15, 15–24, 25–59, 60 and above (if no answer leave blank)
Appendix I – Inventory of questions to be included in surveys for measuring national indicators

69
Indicator 1: Multiple concurrent sexual partnerships (in the last three months)
1. Have you ever had sexual intercourse? (If yes go to next question)2. How long ago did you last have sexual intercourse?
(if less than three months continue)3. How long ago did you first have sexual intercourse with that same person?4. Have you had sexual intercourse with any other person in the past three months?
(If yes go to next question)5. How long ago did you last have sexual intercourse with this second person?6. How long ago did you first have sexual intercourse with this second person?7. Have you had sexual intercourse with any other person in the past three months?
(If yes go to next question)8. How long ago did you last have sexual intercourse with this third person?9. How long ago did you first have sexual intercourse with this third person?
Note1: To avoid confusion by respondents in answering these questions the interviewer can use an auxiliary tool such as a graphical representation to depict the answers and check it with the interviewee. This tool will be developed by NACS.
Note 2: The series of questions only cover up to three sexual partners. While some persons might have more than three sexual partners during the previous three months, there is no need to go further than establishing three partners as the respondent has been already identified as having multiple concurrent sexual partners.
Indicator 2: Multiple concurrent sexual partnerships (for the last 12 months)
1. Have you ever had sexual intercourse? (If yes go to next question)2. How long ago did you last have sexual intercourse?
(if less than 12 months continue)3. How long ago did you first have sexual intercourse with that same person?4. Have you had intercourse with any other person in the past 12 months?
(If yes go to next question)5. How long ago did you last have sexual intercourse with this second person?6. How long ago did you first have sexual intercourse with this second person?7. Have you had intercourse with any other person in the past 12 months?
(If yes go to next question)8. How long ago did you last have sexual intercourse with this third person?9. How long ago did you first have sexual intercourse with this third person?
Note1: To avoid confusion by respondents in answering these questions the interviewer can use an auxiliary tool such as a graphical representation to depict the answers and check it with the interviewee. This tool will be developed by NACS.
Note 2: The series of questions only cover up to three sexual partners. While some persons might have more than three sexual partners during the previous three months, there is no need to go further than establishing three partners as the respondent has been already identified as having multiple concurrent sexual partners.
Appendix I – Inventory of questions to be included in surveys for measuring national indicators

70
Indicator 3: Multiple sexual partnerships (for the past 12 months)
1. Have you ever had sexual intercourse? (If yes go to next question)2. In the last 12 months, how many people have you had sexual intercourse with?
Indicator 4: Condom use in multiple sexual partnerships
1. In the last 12 months, how many people have you had sexual intercourse with? (If more than one, continue)
2. Did you or your partner use a condom the last time you had sexual intercourse?
Indicator 5: Condom use in sex workers1. Have you had sexual intercourse in the past 12 months in exchange for money,
goods or other services? (If yes continue)2. Did you use a condom with your most recent client?
Indicator 6: Condom use in persons engaged in transactional sex
1. Have you had sexual intercourse in the last 12 months with anybody beside your spouse in exchange for money, gifts, food, shelter or any other services? (If yes continue)
2. For the last time you had sexual intercourse in exchange for money, gifts, food, shelter or any other services, did you or your partner use a condom?
Indicator 7: Condom use in men who have sex with men
1. Have you had sex with another man in the past six months? (If yes continue)2. Did you or your male partner use a condom the last time you had anal sex with
another man?
Indicator 8: Condom use in anal sex1. In the last 12 months, have you ever had anal intercourse with another person
(man or woman)? (If yes continue)2. Did you or your partner use a condom the last time you had anal intercourse?3. What was your partner’s sex?
Appendix I – Inventory of questions to be included in surveys for measuring national indicators

71
Indicators 12 and 13: HIV testing1. I don’t want to know the result, but have you been tested for HIV in the last 12
months? (If yes continue)2. I don’t want to know the result, but did you get the result of that test?
Indicator 30: Reach of HIV prevention programs for MARPs
1. Have you provided sexual services to people in past 12 month in exchange for money, gifts, food, shelter or any other services? (If yes continue)
2. Do you know where you can go if you want to have an HIV test?3. In the last 12 months, have you been given condoms (for example, through an
outreach service, drop-in centre or sexual health clinic)?
OR for males only:
1. Have you had sex with another man in the past six months? (If yes continue)2. Do you know where you can go if you want to have an HIV test?3. In the last 12 months, have you been given condoms (for example, through an
outreach service, drop-in centre or sexual health clinic)?
Indicator 37 and 38: Comprehensive and correct knowledge on sexual transmission of HIV
1. Can the risk of HIV transmission be reduced by having sex with only one uninfected partner who has no other partners?
2. Can a person reduce the risk of getting HIV by using a condom every time they have sex?
3. Can a healthy-looking person have HIV?4. Can a person get HIV from mosquito bites?5. Can a person get HIV by sharing food with someone who is infected?
Indicator 39: Sexual intercourse before 15 years of age
1. Have you have ever had sexual intercourse? (If yes go to next question)2. How old were you when you had sexual intercourse for the first time?
Appendix I – Inventory of questions to be included in surveys for measuring national indicators

72
Appendix II
Repository of additional indicators for monitoring and evaluation of programs
A limited number of national indicators, (39), have been developed to collect information on progress in key areas and to collectively give a good overview of PNG’s progress in responding to the HIV epidemic (See List of national indicators). This appendix contains additional indicators, some of which were formulated during the development of this NHS and other indicators already in use at the national and international level for monitoring of particular programs (see Table 3). While the Monitoring and Evaluation Framework only requires reporting against the national indicators, the indicators contained in this appendix can be used, as appropriate, by projects and programs for their internal, more detailed M&E. (Note: in Table 3, in the column ‘Related Strategic Objective’, I, II and III refers to NHS Priority areas 1, 2 and 3. For example, I-1.1.2 refers to Priority Area 1: Prevention, and Strategic objective 1.1.2.)
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

73
Tabl
e 3:
A
dditi
onal
indi
cato
rs fo
r mon
itorin
g an
d ev
alua
tion
of p
rogr
ams
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
1P
erce
ntag
e of
HIV
pre
vent
ion
prog
ram
s th
at in
clud
e in
terv
entio
ns fo
r gen
der-
base
d an
d se
xual
vio
lenc
e–
I – 2
.1.2
––
Ann
ual
2N
umbe
r of H
IV in
terv
entio
ns th
at a
ddre
ss c
ultu
ral p
ract
ices
w
hich
incr
ease
HIV
risk
dis
aggr
egat
ed b
y se
x, lo
catio
n an
d cu
ltura
l pra
ctic
e–
I – 2
.1.6
––
Ann
ual
3P
erce
ntag
e of
HIV
pre
vent
ion
inte
rven
tions
that
can
de
mon
stra
te m
eani
ngfu
l par
ticip
atio
n of
you
ng p
eopl
eA
ge Sex
Act
ivity
type
I – 2
.2.2
––
Ann
ual
4P
erce
ntag
e of
HIV
pre
vent
ion
prog
ram
s th
at ta
rget
the
vuln
erab
ility
of c
hild
ren
to H
IV w
hich
mea
ning
fully
invo
lve
child
ren
in th
e de
sign
, del
iver
y an
d m
onito
ring
of in
terv
entio
ns–
I – 2
.3.2
––
Ann
ual
5P
erce
ntag
e of
HIV
pre
vent
ion
inte
rven
tions
that
incl
ude
drug
an
d al
coho
l har
m re
duct
ion
activ
ities
–I –
2.5
.1–
–A
nnua
l
6N
umbe
r of c
ultu
ral,
chur
ch a
nd s
ocia
l eve
nts
with
targ
eted
aw
aren
ess
prog
ram
s ad
dres
sing
mul
tiple
con
curr
ent
partn
ersh
ips
–I –
3.1
.1–
–A
nnua
l
7P
erce
ntag
e of
spo
rting
ass
ocia
tions
sig
ned
up to
the
PN
G
Dec
lara
tion
on H
IV a
nd A
IDS
Pre
vent
ion
thro
ugh
Spo
rt–
I – 3
.1.2
––
Ann
ual
8N
umbe
r of d
istri
cts
with
HIV
and
STI
pre
vent
ion
inte
rven
tions
du
ring
elec
tion
perio
ds–
I – 3
1.3
––
Year
s in
whi
ch
elec
tions
are
hel
d
Indi
cato
rs fo
r mon
itorin
g th
e re
spon
se e
nviro
nmen
t and
Inpu
ts
9P
erce
ntag
e of
hot
els,
bar
s an
d ni
ghtc
lubs
that
hav
e m
ade
mal
e an
d fe
mal
e co
ndom
s av
aila
ble
–I –
3.1
.5–
–A
nnua
l
10N
umbe
r of o
rgan
isat
ions
with
app
ropr
iate
HIV
wor
kpla
ce
polic
ies
and
stra
tegi
es–
I – 3
.2.2
––
Ann
ual
11P
erce
ntag
e of
HC
T se
rvic
es th
at e
mpl
oy P
LHIV
Em
ploy
men
t sta
tus
(vol
unte
er; p
aid)
II –
1.1.
4–
–A
nnua
l
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

74
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
12P
erce
ntag
e of
trea
tmen
t ser
vice
s th
at e
mpl
oy P
LHIV
Em
ploy
men
t sta
tus
(vol
unte
er; p
aid)
II –
2.1.
7–
–A
nnua
l
13A
nnua
l per
cent
age
chan
ge in
reso
urce
allo
catio
n to
STI
and
se
xual
hea
lth p
rogr
ams
–II
– 2.
3.2
––
Ann
ual
14P
erce
ntag
e of
HB
C a
nd c
omm
unity
sup
port
prog
ram
s th
at
empl
oy P
LHIV
Em
ploy
men
t sta
tus
(vol
unte
er; p
aid)
II –
2.4.
4–
–A
nnua
l
15N
umbe
r of s
uppo
rt gr
oups
run
by p
ositi
ve p
eopl
e–
II –
2.4.
7–
–A
nnua
l
16P
erce
ntag
e of
HB
C a
nd/o
r com
mun
ity s
uppo
rt pr
ogra
ms
whe
re m
en a
nd b
oys
are
activ
ely
invo
lved
–II
– 2.
4.10
––
Ann
ual
17N
umbe
r of u
pdat
ed ri
sk a
nd v
ulne
rabi
lity
profi
les
avai
labl
e–
III –
1.3
.1–
–A
nnua
l
18P
erce
ntag
e of
rese
arch
pro
vide
d by
Gov
ernm
ent o
f PN
G a
nd
deve
lopm
ent p
artn
ers
for r
esea
rch
that
is b
ased
on
the
NR
A–
III –
1.4
.2–
–A
nnua
l
19N
umbe
r of H
IV p
rogr
ams
addr
essi
ng g
ende
r-re
late
d vu
lner
abili
ty, r
epor
ted
in th
e N
HS
ann
ual p
lann
ing
proc
ess
Type
of p
rogr
amIII
– 2
.1.1
––
Ann
ual
20N
umbe
r of m
en’s
gro
ups
invo
lved
in H
IV a
nd A
IDS
pro
gram
sTy
pe o
f or
gani
satio
nA
ctiv
ities
III –
2.1
.3–
–A
nnua
l
21N
umbe
r of w
omen
’s g
roup
s in
volv
ed in
HIV
and
AID
S
prog
ram
sTy
pe o
f or
gani
satio
nA
ctiv
ities
III –
2.1
.4–
–A
nnua
l
22P
erce
ntag
e of
men
and
wom
en o
n H
IV-r
elat
ed c
oord
inat
ion
and
deci
sion
-mak
ing
com
mitt
ees
at n
atio
nal a
nd s
ub-n
atio
nal
leve
lsS
exIII
– 2
.1.8
––
Ann
ual
23P
erce
ntag
e of
HIV
pro
gram
s th
at d
emon
stra
te m
eani
ngfu
l in
volv
emen
t PLH
IV–
III –
2.2
.1–
–A
nnua
l
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

75
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
24P
erce
ntag
e of
PLH
IV g
roup
s th
at a
re p
art o
f a n
atio
nal
netw
ork
–III
– 2
.2.2
––
Ann
ual
25P
erce
ntag
e of
PLH
IV g
roup
s th
at m
onito
r and
repo
rt on
st
igm
a an
d di
scrim
inat
ion
and
grea
ter i
nvol
vem
ent o
f peo
ple
livin
g w
ith H
IV (G
IPA
), us
ing
the
stan
dard
inde
x–
III –
2.2
.3–
–A
nnua
l
26N
atio
nal J
oint
Coo
rdin
atin
g C
omm
ittee
(NJC
C) m
eetin
gs
occu
r on
a re
gula
r bas
is b
etw
een
key
serv
ice
deliv
ery
depa
rtmen
ts–
III –
2.3
.3
III –
3.2
.1–
–A
nnua
l
27N
umbe
r of a
rres
ts a
nd p
rose
cutio
ns fo
r sex
wor
k–
III –
2.4
.2–
–A
nnua
l
28N
umbe
r of c
ases
and
suc
cess
ful p
rose
cutio
ns u
nder
the
HA
MP
Act
–III
– 2
.5.1
––
Ann
ual
29N
HS
ann
ual p
lan
and
budg
et s
ubm
issi
ons
and
annu
al
parli
amen
tary
repo
rt co
mpl
eted
on
time
–III
– 3
.1.1
––
Ann
ual
30P
erce
ntag
e of
PA
CS
and
DA
CS
that
rece
ive
thei
r qua
rterly
di
sbur
sem
ents
and
sen
d in
qua
rterly
and
ann
ual r
epor
ts
on ti
me
–III
– 3
.12
––
Ann
ual
31N
umbe
r of N
GO
s an
d FB
Os
that
hav
e pa
rtici
pate
d in
a
colla
bora
tive
proj
ect w
ith a
noth
er N
GO
or F
BO
in th
e
last
yea
r–
III–3
.1.5
––
Ann
ual
32N
umbe
r of g
over
nmen
t dep
artm
ents
repo
rting
to N
AC
S
thro
ugh
the
NH
S p
lann
ing
and
repo
rting
cyc
le–
III –
3.1
.6–
–A
nnua
l
33N
umbe
r of m
eetin
gs b
etw
een
NA
CS
and
PA
CS
–III
– 3
.2.2
––
Ann
ual
34N
umbe
r of c
omm
uniti
es u
sing
gen
der-
sens
itive
com
mun
ity
mob
ilisa
tion
tool
s in
HIV
pla
nnin
g, im
plem
enta
tion
and
mon
itorin
g–
III –
3.3
.1–
–A
nnua
l
35P
erce
ntag
e of
HIV
com
mun
ity m
obili
satio
n pr
ogra
ms
that
can
de
mon
stra
te m
eani
ngfu
l par
ticip
atio
n of
PLH
IV–
III –
3.3
.2–
––
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

76
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
36N
umbe
r of f
acili
ties
prov
idin
g A
NC
ser
vice
s th
at a
lso
prov
ide
HIV
cou
nsel
ling
and
test
ing
for p
regn
ant w
omen
–I –
1.2
.1U
AH
ealth
faci
litie
s su
rvey
Ann
ual
37P
erce
ntag
e of
hea
lth c
are
faci
litie
s de
liver
ing
PP
TCT
serv
ices
th
at re
port
stoc
k ou
t of t
est k
its in
the
last
12
mon
ths
–I –
1.2
.4–
Hea
lth fa
cilit
ies
surv
eyA
nnua
l
38P
erce
ntag
e of
hea
lth c
are
faci
litie
s th
at m
eet m
inim
um
stan
dard
s in
uni
vers
al p
reca
utio
ns u
sing
an
infe
ctio
n co
ntro
l au
dit t
ool
–I –
1.3
.1–
Hea
lth fa
cilit
ies
surv
eyA
nnua
l
39P
erce
ntag
e of
you
ng p
eopl
e ag
ed 1
5–24
in fu
ll tim
e ed
ucat
ion
or in
com
e ge
nera
ting
Age Sex
I – 2
.2.8
–Yo
uth
surv
eyE
very
thre
e to
fiv
e ye
ars
40P
erce
ntag
e of
pro
vinc
es w
ith c
hild
pro
tect
ion
syst
em b
ased
on
the
Luka
utim
Pik
inin
i Act
–I –
2.3
.1–
–A
nnua
l
41P
erce
ntag
e of
cus
todi
al fa
cilit
ies
that
mak
e co
ndom
s an
d ot
her h
arm
redu
ctio
n re
sour
ces
acce
ssib
le to
pris
oner
s as
pa
rt of
a c
ompr
ehen
sive
har
m re
duct
ion
prog
ram
–I –
2.4
.3–
Cus
todi
al fa
cilit
ies
revi
ewE
very
two
year
s
Indi
cato
rs fo
r mon
itorin
g th
e na
tiona
l res
pons
e ou
tput
s
42P
erce
ntag
e of
eco
nom
ic e
ncla
ve s
ites
and
reso
urce
de
velo
pmen
t pro
ject
s th
at h
ave
HIV
pre
vent
ion
and
prim
ary
heal
thca
re in
terv
entio
ns–
I – 3
.2.3
––
Ann
ual
43N
umbe
r of p
ublic
-priv
ate
partn
ersh
ips
for H
IV d
isag
greg
ated
by
pro
vinc
e, s
cope
and
type
of s
ervi
ce–
I – 3
.2.4
––
Ann
ual
44P
erce
ntag
e of
HC
T se
rvic
es th
at a
re m
aint
aini
ng m
inim
um
stan
dard
s–
II –
1.1.
5–
–A
nnua
l
45P
erce
ntag
e of
HC
T se
rvic
es th
at a
re a
ccre
dite
d to
pro
vide
H
CT
for c
hild
ren
–II
– 1.
1.6
––
Ann
ual
46P
erce
ntag
e of
HC
T cl
ient
s w
ho a
re s
atis
fied
with
the
serv
ice
prov
ided
Sex
Age
II –
1.1.
8–
–A
nnua
l
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

77
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
47P
erce
ntag
e of
HC
T se
rvic
es d
istri
butin
g co
ndom
s to
all
clie
nts
–II
– 1.
1.9
––
Ann
ual
48P
erce
ntag
e of
AR
T se
rvic
es th
at h
ave
unde
rgon
e re
gula
r qu
ality
ass
uran
ce a
uditi
ng–
II –
2.1.
4–
–A
nnua
l
49P
erce
ntag
e of
AR
T se
rvic
es w
ith in
tegr
ated
/link
ed T
B, S
TI
and
gend
er-b
ased
vio
lenc
e se
rvic
es–
II –
2.1.
5–
–A
nnua
l
50N
umbe
r of A
RT
site
s pr
ovid
ing
the
min
imum
pac
kage
of
com
preh
ensi
ve c
are
–II
– 2.
1.6
––
Ann
ual
51P
erce
ntag
e of
AR
T cl
ient
s w
ho a
re s
atis
fied
with
the
serv
ice
prov
ided
Sex
Age
II –
2.1.
8–
–A
nnua
l
52P
erce
ntag
e of
hea
lth c
are
faci
litie
s pr
ovid
ing
AR
T us
ing
CD
4 m
onito
ring
in li
ne w
ith n
atio
nal g
uide
lines
or p
olic
ies,
eith
er o
n si
te o
r thr
ough
refe
rral
–II
– 2.
1.9
UN
GA
SS
+U
A–
Ann
ual
53P
erce
ntag
e of
hea
lthca
re fa
cilit
ies
that
offe
r Pae
diat
ric A
IDS
se
rvic
es w
ith s
taff
train
ed in
del
iver
ing
thes
e se
rvic
es–
II –
2.2.
3–
–A
nnua
l
54P
erce
ntag
e of
hea
lth c
are
faci
litie
s th
at p
rovi
de v
irolo
gica
l te
stin
g se
rvic
es (f
or e
xam
ple,
PC
R) f
or in
fant
dia
gnos
is o
n si
te o
r thr
ough
drie
d bl
ood
spot
s)–
II –
2.2.
4U
A–
Ann
ual
55P
erce
ntag
e of
HIV
infe
cted
chi
ldre
n ag
ed 0
to 1
4 ye
ars
who
ar
e cu
rren
tly re
ceiv
ing
AR
TS
ex
Age
II –
2.2.
5–
–A
nnua
l
56P
erce
ntag
e of
STI
clie
nts
who
are
sat
isfie
d w
ith th
e se
rvic
e pr
ovid
edS
exA
geII
– 2.
3.3
––
Ann
ual
57P
erce
ntag
e of
hea
lth c
are
faci
litie
s re
porti
ng a
dequ
ate
and
unin
terr
upte
d su
pplie
s of
STI
dru
gs–
II –
2.3.
4–
–A
nnua
l
58N
umbe
r of m
ales
and
fem
ales
trai
ned
in n
atio
nal s
tand
ards
fo
r HB
CS
exII
– 2.
4.3
––
Ann
ual
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

78
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
60C
urre
nt s
choo
l atte
ndan
ce a
mon
g or
phan
s an
d am
ong
non-
orph
ans
aged
10
to14
Sex
II –
2.4.
6U
NG
AS
S–
Eve
ry th
ree
to
five
year
61N
umbe
r of P
LHIV
acc
essi
ng in
com
e su
ppor
t ini
tiativ
esS
exA
geII
– 2.
4.8
––
Ann
ual
62P
erce
ntag
e of
PLH
IV o
rgan
isat
ions
util
isin
g in
itiat
ives
that
pr
omot
e he
alth
, dig
nity
and
pre
vent
ion
–II
– 2.
4.9
––
Ann
ual
63N
umbe
r of s
uppo
rt pr
ogra
ms
that
spe
cific
ally
targ
et th
e ne
eds
of m
ale
and
fem
ale
yout
h liv
ing
with
HIV
–II
– 2.
4.12
––
Ann
ual
64N
umbe
r of s
uppo
rt pr
ogra
ms
that
spe
cific
ally
targ
et th
e ne
eds
of P
LHIV
who
hav
e ad
ditio
nal v
ulne
rabi
litie
s (fo
r exa
mpl
e,
men
who
hav
e se
x w
ith m
en a
nd s
ex w
orke
rs)
–II
– 2.
4.13
––
Ann
ual
65N
umbe
r of b
io, b
ehav
iour
al, a
nd b
io-b
ehav
iour
al s
urve
illan
ce
stud
ies
cond
ucte
d an
nual
lyS
iteTa
rget
gro
upIII
– 1
.2.1
–S
urve
illan
ce a
nd
rese
arch
repo
rtA
nnua
l
66N
atio
nal C
ounc
il of
Wom
en a
nnua
l act
ivity
pla
n, b
udge
t al
loca
tion
and
repo
rts d
emon
stra
te a
ctiv
e en
gage
men
t with
th
e H
IV a
nd A
IDS
resp
onse
–III
– 2
.1.5
––
Ann
ual
67P
erce
ntag
e of
org
anis
atio
ns w
ith a
ppro
pria
te H
IV w
orkp
lace
po
licie
s an
d st
rate
gies
Type
of
orga
nisa
tion
III –
2.2
.4–
–A
nnua
l
68N
umbe
r of l
eade
rs w
ho p
artic
ipat
e in
HIV
and
AID
S
lead
ersh
ip s
treng
then
ing
prog
ram
sS
exS
ecto
rIII
– 2
.3.1
––
Ann
ual
69P
erce
ntag
e of
HIV
trai
ners
who
can
dem
onst
rate
com
pete
ncy
in H
IV tr
aini
ng to
nat
iona
l sta
ndar
ds–
III –
3.1
.7–
–A
nnua
l
59P
erce
ntag
e of
AR
T si
tes
that
offe
r psy
chos
ocia
l sup
port
and
nutri
tion
inte
rven
tions
–II
– 2.
4.5
––
Ann
ual
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

79
Dis
aggr
egat
ion(
s)R
elat
ed
stra
tegi
c ob
ject
ive(
s)In
dica
tor
Inte
rnat
iona
l in
dica
tor l
ist
Dat
a co
llect
ion
tool
Dat
a co
llect
ion
freq
uenc
y
71P
erce
ntag
e of
men
and
wom
en w
ho c
an id
entif
y th
e ris
ks
of H
IV tr
ansm
issi
on a
ssoc
iate
d w
ith p
enile
mod
ifica
tion
disa
ggre
gate
d by
the
type
of p
enile
mod
ifica
tion
Sex
Age
I – 1
.4.1
–Yo
uth
and
gene
ral
popu
latio
n su
rvey
Eve
ry th
ree
to
five
year
s
72P
erce
ntag
e of
men
and
wom
en w
ho c
an id
entif
y th
e ris
k of
HIV
tran
smis
sion
ass
ocia
ted
with
tatto
os, p
ierc
ing
and
scar
ifica
tion
prac
tices
, dis
aggr
egat
ed b
y pr
actic
e an
d ag
e
Sex
Age
I – 1
.4.2
–Yo
uth
and
Gen
eral
P
opul
atio
n S
urve
yE
very
thre
e to
fiv
e ye
ars
73P
erce
ntag
e of
inje
ctin
g dr
ug u
sers
who
repo
rted
usin
g st
erile
in
ject
ing
equi
pmen
t the
last
tim
e th
ey in
ject
edS
exA
geI –
1.4
.3U
NG
AS
SS
peci
al p
opul
atio
n B
SS
Eve
ry tw
o to
th
ree
year
s
74P
erce
ntag
e of
wom
en w
ho k
now
that
vag
inal
dry
ing
can
incr
ease
risk
of H
IV tr
ansm
issi
onA
geI –
1.4
.4–
Yout
h an
d G
ener
al
Pop
ulat
ion
Sur
vey
Eve
ry th
ree
to
five
year
s
75P
erce
ntag
e of
you
ng w
omen
and
men
age
d 15
to 2
4 w
ho
repo
rt th
ey c
ould
get
con
dom
s on
thei
r ow
nS
exA
ge (1
5–19
; 20–
24; 2
5–34
; 35–
49;
50–5
9)Fe
mal
e an
d m
ale
cond
oms
I – 2
.2.3
UN
GA
SS
+Yo
uth
and
Gen
eral
P
opul
atio
n S
urve
yE
very
thre
e to
fiv
e ye
ars
70P
erce
ntag
e of
wom
en a
nd m
en li
ving
with
HIV
usi
ng a
co
ndom
at l
ast s
exS
exA
geK
now
n se
ro-
disc
orda
nce
stat
us
of th
e co
uple
I – 1
.1.1
0–
Spe
cial
pop
ulat
ion
BS
SE
very
two
to
thre
e ye
ars
Indi
cato
rs fo
r mon
itorin
g th
e kn
owle
dge
and
beha
viou
rs
Appendix II – Repository of additional indicators for monitoring and evaluation of programs

80
Appendix III
Glossary
Appraisal: An assessment of the relevance, feasibility and sustainability of a development intervention prior to a decision on funding. Note: In development banks and agencies, the purpose of appraisal is to enable decision makers to decide whether the activity represents an appropriate use of resources.
Assessment: A process (which may or may not be systematic) of gathering information, analysing it and making a judgement on the basis of the information.
Baseline: Data on current status before commencement of an intervention which provides a base for measuring and comparing the effect of the intervention. The baseline may be the status of services (for example, coverage or utilisation data) or outcome-related measures such as knowledge, attitudes and behaviours.
Demographic and Health Survey (DHS): A nationally-representative household survey with a large sample size (usually between 5,000 and 30,000 households). A DHS provides data for a wide range of monitoring and impact evaluation indicators in the areas of population, health and nutrition.
Disease surveillance: The ongoing systematic collection, analysis and interpretation of data to describe diseases and their transmission in populations. These data can help predict future trends and target needed prevention and treatment programs. When data are collected from certain sites – for example, antenatal clinics – that are believed to be representative of the population as a whole or key population groups of interest, surveillance has the potential to provide early warning signs. This is called sentinel surveillance.
Evaluation: The systematic and objective assessment of the design, implementation and results of an ongoing or completed project, program or policy. The aims may include determining relevance, fulfilment of objectives, development efficiency, effectiveness, impact and sustainability. An evaluation should provide information that is credible and useful, enabling the incorporation of lessons learned into the decision-making process of both implementers and donors. Evaluation also refers to the process of determining the worth or significance of an activity, policy or program. Note: Evaluation in some instances involves the definition of appropriate standards, the examination of performance against those standards, an assessment of actual and expected results and the identification of relevant lessons.
Appendix III – Glossary

81
Facility survey: A site inventory of all elements required to deliver services, such as basic infrastructure, drugs, equipment, test kits, registers and trained staff. The units of observation are facilities of various types and levels in the health system and normally include both public and private facilities in the sample frame of sites. This type of survey may also be referred to as a service provision assessment. When a survey covers only facilities providing health services, it is usually called a ’health facility survey’.
Formative evaluation: A type of process evaluation undertaken during program implementation to furnish information that will guide program improvement. A formative evaluation focuses on collecting data on program operations so that needed changes or modifications can be made. Formative evaluations are used to provide feedback to program managers and other personnel about aspects of the program that are working and those that need to be changed.
Impact evaluation: The systematic identification of the broad, long-term effects (positive or negative, intended or unintended) that can at least in part be attributed to a particular project or program. Impact evaluation helps answer key questions for evidence-based policy and program development such as what works, what does not work and why.
Impact monitoring: In the field of public health, impact is usually monitored by measuring disease prevalence or incidence (see ‘disease surveillance’ above). With this type of monitoring, data are collected at provincial, regional and national levels.
Indicator: A quantitative or qualitative variable, or combination of variables, that provides a simple and reliable means to measure achievement in relation to a strategic objective, to reflect the changes connected to an intervention, or to help assess performance (for example, the percentage of female and male sex workers reporting the use of a condom with their most recent client). In order for indicators to be useful for monitoring and evaluating program results, it is important that they be objective, time-sensitive, and that regular data collection in relation to the indicator is practical.
Input and output monitoring: Involves the tracking of information about program inputs (that is, the different types of resources that go into a program) and program outputs (for example, program activities). Data sources for monitoring inputs and outputs usually exist in program documentation, such as activity reports, logs and client records, which offer details about the time, place and the quantity of services delivered, as well as the types of clients receiving services.
Integrated biological and behavioural surveillance measures HIV prevalence, and often STI prevalence, in a defined population at a point in time, as well as behaviours and demographic information, to provide a better understanding of the dynamics of the epidemic. When these surveys are repeated over time, trends in the epidemic can be measured.
Logical framework (Logframe): A management tool used to improve the design of interventions, most often at the project level. It involves identifying strategic elements (inputs, outputs, outcomes, impact) and their causal relationships, indicators, and assumptions or risks that may influence success and failure. It thus facilitates planning, execution and evaluation of an intervention. Related term: results-based management.
Appendix III – Glossary

82
Monitoring: The routine tracking and reporting of priority information about a program and its intended outputs and outcomes. Monitoring asks: What have we achieved?
Monitoring and evaluation: Symbiotic processes that are used to measure results. These processes include collecting, managing, analysing and interpreting data produced from a variety of sources such as regular program monitoring data, surveillance and research.
Monitoring and evaluation plan: A comprehensive planning document for all M&E activities which documents the key M&E questions to be addressed. It includes baselines, targets, assumptions, what indicators are collected, how, how often, from where and why they will be collected. The plan specifies how all data will be analysed or interpreted, and how or how often reports will be developed and distributed.
Monitoring and evaluation system: The set of planning, information gathering, synthesis, reflection and reporting processes, along with the necessary supporting conditions and capacities required for the M&E outputs, to make a valuable contribution to project decision making and learning.
Monitoring and Evaluation Framework: A matrix describing the performance questions, information gathering requirements (including indicators), reflection and review events with stakeholders, and resources and activities required to implement a functional M&E system. This matrix lists how data will be collected, when, by whom and where.
Operations research: Applies systematic research techniques to improve service delivery. This type of research and evaluation analyses only factors that are under the control of program managers, such as improving the quality of services, increasing training and supervision of staff, and adding new service components. Operations research is usually undertaken to assess the accessibility, availability, quality and sustainability of programs.
Outcome evaluation: A type of evaluation that is concerned with determining if, and to what extent, program activities or services achieved their intended outcomes. Whereas outcome monitoring is helpful and necessary in knowing whether outcomes were attained, outcome evaluation attempts to attribute observed change to the intervention tested, describe the extent or scope of program outcomes and indicate what might happen in the absence of the program. Outcome evaluation is methodologically rigorous and generally requires a comparative element in design, such as a control or comparison group.
Outcome monitoring: The tracking of indicators of desired program outcomes. Changes in outcome could be attributable to multiple factors, not just the program, so outcome monitoring does not infer causality. With national AIDS programs, outcome monitoring is typically conducted through population-based surveys to track whether desired outcomes have been reached. It may also track information directly related to program clients, such as change in knowledge, attitudes, beliefs, skills, behaviours, access to services, policies and environmental conditions.
Output indicator: An indicator that measures the quantity of products and services resulting from program activities within a given timeframe. For example, the number of individual and group client counselling sessions in the past 12 months.
Appendix III – Glossary

83
Process evaluation: A type of evaluation that focuses on program implementation, adding a dimension to information tracked in input and output monitoring. Areas commonly examined include how services are delivered, access to services and management practices. Process evaluation usually focuses on a single program and uses largely qualitative methods to describe program activities and perceptions, especially during the developmental or early implementation stage of a program. It may also include some quantitative approaches, such as surveys about client satisfaction and perceptions about needs and services. In addition, process evaluation might provide understandings about a program’s cultural, socio-political, legal, and economic contexts that affect implementation.
Process monitoring: The routine gathering of information on all aspects of project or program implementation to check on how project activities are progressing. It provides information for planning and feedback on the progress of the project to the development partners, implementers, and beneficiaries.
Program evaluation: Program evaluation is a systematic method for collecting, analysing, and using information to determine the value of and to improve programs.
Program monitoring: The process of documenting the activities of program implementation. This implies tracking HIV-related activities and services through a monitoring system where all partners submit regular, structured program reports that are externally verified.
Routine data: Are those data generated as part of the implementation of a program, activity or service. For example, every time a patient visits a hospital, the patient’s name is recorded in the hospital register. Such a register therefore contains routine data.
Second-generation surveillance: HIV surveillance that is tailored to meet the specific pattern of the epidemic in a country. It not only tracks HIV prevalence but also uses additional sources of data to increase understanding of trends of the epidemic over time. It includes biological surveillance of HIV and other STIs as well as systematic surveillance of risk behaviours.
Appendix III – Glossary