Paper Patologia

of 14
-
Upload
maria-jose-vega-pardo -
Category
Documents
-
view
227 -
download
0
Transcript of Paper Patologia
-
7/23/2019 Paper Patologia
1/14
Muscle Tension Dysphonia in Vietnamese FemaleTeachers
*,Duong Duy Nguyen,Dianna T. Kenny,Ninh Duy Tran, andkJonathan R. Livesey,*xThai Nguyen city, Vietnam, andyzkSydney, Australia
Summary:There has been no published research on muscle tension dysphonia (MTD) in speakers who use a tonallanguage. Using a sample of 47 Northern Vietnamese female primary school teachers with MTD, we aimed to discover
whether professional voice users of tonal languages presented with the same symptoms of MTD as speakers of nontonallanguages and whether they presented with additional symptoms as a result of speaking a tonal language. The vocalcharacteristics were assessed by use of a questionnaire and expert perceptual evaluation. Laryngeal features were as-
sessed by photolaryngoscopy. The results showed that MTD was associated with a larger number of vocal symptoms
than previously reported. However, the participants did not have the same vocal symptoms reported in English speakers,
for example, hard glottal attack, pitch breaks, unusual speech rate, and glottal fry. Factor analysis of the vocal symptoms
revealed three factors: vocal fatigue/hyperfunction, physical discomfort, and voice quality, all of which demon-
strated high reliability. The major laryngeal characteristic was a glottal gap. The glottal shapes observed included:
44.7% had an incomplete closure, 29.8% a posterior gap, 12.8% an hourglass-shaped gap, 8.5% a spindle-shaped
gap, and 4.3% had complete glottal closure. The findings implied a potential contribution of linguistic-specific factorsand teaching-related factors to the presentation of this voice disorder in this group of teachers.
Key Words:Muscle tension dysphoniaTeaching voiceGlottal gap.
INTRODUCTIONMuscle tension dysphonia (MTD) is a voice disorder in the ab-
sence of current organic laryngeal pathology, without obvious
psychogenic and neurologic etiology.1 It is characterized by
a generalized increase in muscle tension in the larynx and paral-
aryngeal areas associated with vocal abuse.2,3 The syndrome is
seen commonly in young and middle-aged people with exten-
sive voice use in stressful situations.4 The laryngeal features
of MTD include a posterior glottal gap4 and supraglottic hyper-functional activities, that is, anteroposterior (AP) contraction
and lateral ventricular fold adduction.3 Voice therapy is the ma-
jor method of treatment because the disorder results from func-
tional problems related to improper use of the laryngeal musclesin phonation rather than a structural change in the larynx.3
The etiology of the increased laryngeal muscle tension is
multifactorial.5 However, the above definition excludes some
voice disorders of other etiologies that share clinical features
with MTD. The first is dysphonia in relation to psychological
phenomena, which also has considerable supraglottic activities6
and in many situations it is difficult to differentiate it from MTD
without referring to its etiology. Morrison and Rammage2
maintain that a diagnosis of psychogenic dysphonia should
only be given to muscle misuse disorders that have a clear pri-
mary psychoemotional etiology defined using standard psychi-
atric evaluations. Sapir7 suggests that psychogenic dysphonia
should be suspected when three criteria are satisfied: symptom
incongruity (ie, the dysphonia is physiologically incongruent
with the existing disease, internally inconsistent, and incongru-
ent with other speech and language findings); symptom revers-
ibility (ie, the voice completely returns to normal state with
short-term voice therapy or psychotherapy); and symptom psy-
chogenicity (ie, the dysphonia occurs in logical linkage at thetime of onset,course, and severity to an identifiable psycholog-
ical stimulus).7 The second is laryngeal focal dystonia, that is,
adductor spasmodic dysphonia, which is characterized by ac-
tion-induced, task-specific hyperadduction of the vocal folds.1
Various techniques have been suggested to differentiate this
neurogenic condition from MTD, for example, acoustic voice
analyses.8 Additionally, there is also an increased muscle ten-
sion known as secondary MTD as an attempt to compensate
for a glottal incompetence in an organic voice disorder such as
vocal fold paralysis. In this condition, the characteristics of the
dysphonia and the choice of treatment methods are substan-
tially influenced by the primary organic pathology rather than
the disordered muscle tension and the diagnosis of MTD is nor-
mally not given even in mucosal pathologies occurring as a con-
sequence of vocal hyperfunction as in the case of vocal nodules.
Despite its wide recognition and description, no published
study has investigated clinical characteristics of MTD in a pop-
ulation of tonal language speakers, for example, Vietnamese. It
is possible that phonation differences between tonal and non-
tonal languages are related to the different uses of the larynx
in languages, which may affect the characteristics of this voice
disorder in each type of language. In tonal languages, there are
specific phonological features that are not usually present or are
not linguistically significant in nontonal languages. This typi-
cally results from the cross-linguistic use of the glottis associ-
ated with the various states of the vocal folds.9 In tonal
languages, the glottis is configured for different phonation types
Accepted for publication September 6, 2007.Presented at the Voice Foundations 36th Annual Symposium: Care of the Professional
Voice, May 29June 3, 2007, The Westin Philadelphia, Philadelphia, Pennsylvania, USA.From the *Department of Otolaryngology, Thai Nguyen General Central Hospital, Thai
Nguyen city, Vietnam; yFaculty of Health Sciences, The University of Sydney, Sydney,Australia;zFaculty of Health Sciences and the Australian Centre for Research in MusicPerformance, The University of Sydney, Sydney, Australia;xDepartment of Otolaryngol-ogy, Thai Nguyen Medical College, Thai Nguyen University, Thai Nguyen city, Vietnam;and the kVoice Connection at the North Shore Medical Centre and the Voice Clinics at theSt. Vincents Hospital, Sydney, Australia.
Address correspondence and reprint requests to Duong Duy Nguyen, Department ofOtolaryngology, Thai Nguyen General Central Hospital, Luong Ngoc Quyen Street,Thai Nguyen city, Vietnam. E-mail:[email protected]
Journal of Voice, Vol. 23, No. 2, pp. 195-2080892-1997/$36.00 2009 The Voice Foundationdoi:10.1016/j.jvoice.2007.09.003
mailto:[email protected]:[email protected] -
7/23/2019 Paper Patologia
2/14
such as laryngealization and breathiness.9 In Vietnamese, for
example, laryngealization is produced in the broken tone and
the dropped tone as a contrastive cue and breathiness is associ-
ated with the falling tone as a tonal enhancement feature. 10
Tonal languages also use pitch variation to convey lexical infor-
mation. In Vietnamese, pitch variation creates six tonal distinc-
tions, including one level tone, two falling tones, one rising
tone, and two concave tones. Additionally, there may also besupraglottic involvement in lexical tone production, which
has not been well understood. It is not yet known whether there
is a relationship between phonological characteristics in a tonal
language and the probability of acquiring a functional voice dis-
order and if so, whether its clinical manifestations differ be-
tween tonal and nontonal language speakers. Examining
characteristics of MTD in tonal language speakers would help
clarify this problem and give insight into whether linguistic-
specific factors play any role in this voice disorder, which
would form the basis for understanding the interaction between
linguistic-specific and pathology-specific factors.
Because the physiological basis for lexical tones are the la-
ryngeal muscles,11 functional problems associated with MTDmay affect tone production, causing tone misperception. This
can be reflected by two aspects. Firstly, linguistic phonation
types may not be properly produced in speakers with MTD.
For example, laryngealization is produced with a tightly ad-
ducted posterior glottis so that the vocal folds only vibrate in
the anterior parts.9 Meanwhile, MTD is believed to have
a posterior glottal gap due to the excessive contraction of the
posterior cricoarytenoid muscle during phonation.12 This phe-
nomenon clearly interferes with laryngealization. In Vietnam-
ese, the broken tone phonated without laryngealization willbe heard as the rising tone. Secondly, abnormal laryngeal mus-
cle tension may restrict pitch variation, which affects the reali-
zation of lexical contrasts in tonal languages. This is possible
because previous studies on both nontonal and tonal language
speakers have found evidence of pitch problems in MTD sub-
jects. For example,Morrison et al reported pitch breaks and in-
appropriate pitch.13 Koufman and Blalock3 found reduction in
vocal rangeand pitch lock. In Vietnamese speakers, Nguyen
and Kenny14 found that tone height was decreased in high tones,
and pitch movement were affected in the falling tone and rising
tone in those who had MTD. Understanding the characteristics
of MTD in tonal language speakers would help explain mech-
anisms of tone production in this disorder.
MTD is oftenseen in professional voice users, such as teachers
because of their high vocal demands.Teachers are at high riskofdeveloping voice disorders in general15 and MTD in particular.16
However, to date no study has investigated MTD in school
teachers. This voice disorder can negatively affect their job per-
formance, threaten their career, and result in financial difficulties
due to job absence and medical care. Furthermore, teachers who
use a tonal language may have difficulties in tone phonation if
they suffer from MTD. This may affect tone perception by lis-
teners, impairing the intelligibility of speech conveyed to stu-
dents. Therefore, data on the characteristics of this voice
disorder in teachers would be useful for early diagnosis and man-
agement of voice disorders in this population, given that MTD
may be an antecedent of vocal fold lesions,13 which require
more complicated protocols and longer treatment time.
The aims of the present study were to (1) assess vocal symp-
toms of MTD in Northern Vietnamese primary school teachers
and compare them with those reported previously in nontonal
language speakers and (2) examine laryngeal symptoms of
MTD in Northern Vietnamese primary school teachers.
METHODS
Participants
Participants were recruited from 14 primary schools in the city
of Thai Nguyen (Thai Nguyen province, Northern Vietnam,
76 km North of Hanoi) using school-based survey and screen-
ing examination with the permission of the head of the Depart-
ment of Education and Training. In total, 500 teachers were
surveyed and 416 returned survey questionnaires. Based on
the results of school-based surveys, teachers who reported voice
symptoms were invited to undertake a laryngeal examination.
Teachers with voice problems were reluctant to go to hospitalto attend voice and laryngeal examination, citing the complex
administrative procedures in hospitals and reluctance to leave
their students as disincentives to hospital attendance. Therefore,
schools arranged a time in the working day where examinations
could be conducted in the medical room in the school. Exami-
nations were carried out in the first hour of the teaching day
(89 AM) to obtain data before potential changes in the vocal ap-
paratus related to teaching during the day. On the day of the ex-
amination, an otolaryngologist performed a perceptual voice
assessment and laryngeal examination on all teachers with
voice problems. Those who were diagnosed with MTD com-
pleted a data collection questionnaire (described below) about
their vocal symptoms and other details related to MTD as rele-
vant to the aims of this study. Those diagnosed with other voice
disorders were consulted about further examination and treat-
ment but were not included in the present study.
Forty-seven primary school teachers were diagnosed with
MTD during the period from September 2005 to July 2006.
The mean age of the participants was 42.8 years (SD 8.6),ranging from 22 to 54 years. All participants were female.
Mean duration of occupation of the participants was 22.5 years
(SD8.7), ranging from 1 to 33 years. On average, participantstaught 5.98 hours per day (ranging from 3 to 8 hours per day), 5
days per week.
Diagnostic criteria included a problem with the voice, for ex-ample, hoarseness; no organic lesions on the vocal folds; signs
of vocal hyperfunction, for example, supraglottic constrictionand increased external laryngeal muscle tonicity; normal hear-
ing; and nonsmoker.
Teachers with organic lesions of the vocal folds, for example,
laryngitis, vocal nodules, polyps, and Reinkes edema were ex-
cluded. The study also excluded teachers who had a history of
psychological problems preceding the onset of dysphonia, signs
of psychological problems at the time of study, spasmodic
dysphonia, acute respiratory tract infection, rheumatoid arthritis,history of neck or chest trauma, and history of laryngeal surgery.
Journal of Voice, Vol. 23, No. 2, 2009196
-
7/23/2019 Paper Patologia
3/14
Data collection
Questionnaire. The questionnaire contained 37 short answer
and multiple-choice questions on personal and occupational de-
tails, voice usage, voice care, history of voice problems, and cur-
rent voice problems(Appendix1). Participants indicated whether
or not they encountered voice problems and other uncomfortable
signs in thethroat,neck, chest, andbreathing associatedwith pho-
nation. Participants also gave an overall self-rating of their voiceusing a five-point equal-appearing interval (EAI) scale: 1 very
good, 2 good, 3 fair, 4 bad, and 5 very bad. They
werealso asked to rateeachof the symptoms they had: 1 slight,
2 mild, 3 moderate, and 4 severe. Participants were of-
fered support to complete the questionnaire if needed.
Voice assessment and laryngeal examination. The
voice and laryngeal examinations for the MTD participants
were parts of the screening examination mentioned above andthe results were recorded on an assessment form (Appendix
2). The examiner evaluated the voices of the participants for
symptoms in pitch, intensity, voice quality, and tone phonation.
He also gave an overall rating score for the severity of dyspho-nia in each participant using a six-point EAI scale with 0 being
normal and 5 severe.
Participants then underwent a laryngoscopy and neck exami-
nation. Instruments included a 90 rigid telescope (Hawk Opti-
cal Electronic Instruments Co., Ltd., Zhejiang, China) with
a light fountain (OLYMPUS CLV-S30, Shirakawa Olympus
Co., Ltd. Fukushima, Japan). A digital video camera (OLYM-
PUS OTV-S6) was connected to the telescope. The output of
the camera was connected to a video capture board that was in-
put to a laptop computer, which was used to take digital images
of the larynx during examination. These instruments were con-
sidered suitable for examination at schools, where more compli-
cated procedures such as transnasal flexible strobolaryngoscopywas not suitable. During the procedure, participants were seated
in a comfortable posture to avoid overall muscle tension that
may cause involuntary tension or gag reflex. Two sprays of Xy-
locaine 10% solution were applied into the posterior mouth cav-
ity. The use of local anesthetic was considered necessary to
avoid excessive gag reflex. This was not expected to affect hy-
perfunctional behaviors of participants because previous re-
search has found no significant interference oflocal anesthetic
with laryngeal movement during laryngoscopy.17 The examiner
used a small strip of gauze to hold the participants protruded
tongue and inserted the telescope to the intended position in
the posterior mouth cavity. The participant was required to pro-
duce a stably sustained /i/ sound for at least 5 seconds. An assis-tant helped the examiner with taking the photographs.
After the procedure, the examiner made ratings of the laryn-geal findings using the assessment form. The larynx was as-
sessed at the glottic and supraglottic levels. At the glottic
level, glottal shape, vocal folds, and the arytenoid cartilages
were assessed. The vocal fold was examined for smoothness
andstraightness of thevibrating edge andmucosa (color, edema,
and mucus); the arytenoids were evaluatedfor symmetry, mobil-
ity, and mucosa. At the supraglottic level, the degree of AP con-
traction and ventricular foldadduction(lateral contraction) were
assessed. The AP contraction was rated from absence to vo-
cal fold obscured. The lateral contraction was also rated from
absence to vocal fold obscured. Tonicity of the external la-
ryngeal muscles and the vertical position of the larynx during
phonation were also evaluated.
Statistical methods
Data were managed withMicrosoft Accessand transferred to thestatistics softwareSPSSversion 12.0 for Windows for analyses.
The observed phenomena were described in terms of frequency
of occurrences. Pearsons correlationcoefficient was used forcor-
relationanalyses. Chi-squaretests wereused to examine the asso-
ciation betweencategorical variables. Exploratory factoranalysis
(principal component analysis) was performed on the self-
reported vocal symptoms in the questionnaire data. The aim
was to extract the most significant clusters of symptoms that rep-
resented possible underlying pathophysiological phenomena.
Theappropriateness of factor analysis to the datawas checked us-
ing the Kaiser-Meyer-Olkin (KMO) measure of sampling ade-
quacy and the Bartletts test of sphericity. KMO values below
0.5 were considered unacceptable. Values between 0.5 and 0.7are acceptable, and measures >0.70.8 are excellent.1820 The
KMO measure was calculated for the whole sample and sepa-
rately for individual variables. The extracted factors were exam-
ined with regard to their eigenvalue andpercentage of variance
explained. Based on Kaisers criterion,21 only factors with an ei-
genvalue greater than 1 were retained. Variables in the factors
with high eigenvalues (1) were examined for their implicationswith respect to the characteristic clusters of symptoms that the
factors represented. Both orthogonal (varimax method) and obli-
que rotations (direct oblimin method) were run and the results of
theoblique rotation were checked for correlation between fac-
tors.18 The results of the oblique rotation showed correlations be-
tween a number of extracted factors, therefore, the orthogonal
rotation was discarded and the oblique rotation was used. Using
the direct oblimin method, the recommended delta value of
zero was setto avoid too high or toolow correlations betweenfac-
tors.18 The postrotation extracted factors were usedto explainthe
data. Only variables with a factor loading greater than 0.3 were
retained. The reliability of the factors extracted from the factor
analysis was assessed using Cronbachs alpha. In all statistical
calculations, the significance level selected was 0.05.
RESULTS
Demographic and vocal use characteristics
All 47 teachers with MTD returned the data collection question-naire. However, questionnaires from six participants were not
used because they did not provide required information, for ex-
ample, occupational details or current voice symptoms. There-
fore, questionnaire data were available for 41 participants.
Among these, 37 were general primary school teachers, three
were music teachers, and one was an art teacher.Sixteen (39%) very frequently used a loud voice in teaching
and 25 (61%) used a loud voice sometimes during teaching.
None replied never used loud voice in teaching. Most of the
participants (85.4%) shouted or screamed occasionally, three
Duong Duy Nguyen, et al MTD in Teacher 197
-
7/23/2019 Paper Patologia
4/14
(7.3%) frequently shouted or screamed, and three reported that
they never shouted. Most of the participants also reported having
to speak over background noise (73.2%); eight (19.5%) fre-
quently talked over noise; only three (7.3%) never talked over
noise. In singing and speaking, 33 participants (80.5%) some-
times used the wrong register and only eight (19.5%) reported
never using the wrong register. The use of the wrong register in
these participants was related to their intention to increase the at-tractiveness and authority of their voices. Most (87.8%) claimed
that they did not have any knowledge about how to use their voi-
ces properly. None had received formal voice training.
Teachers were asked whether they rested their voices after
teaching and during upper respiratory tract infections. After
teaching, 70.7% of the participants never rested their voices,
24.4% had voice rest only occasionally, and only 4.9% fre-
quently had voice rest. During upper respiratory tract infection
(eg, rhinopharyngitis), 51.2% of the participants still used their
voices extensively; 48.8% sometimes rested their voices; and
none rested their voices completely during upper respiratory
tract infection. Likewise, no participant rested her voice when
she had a voice problem. Most participants (75.6%) reporteda normal or comfortable psychological state during teaching.
Negative psychological states were reported in 24.4%, includ-
ing worried (14.6%) and tense (9.8%). None ever had required
treatment or consultation for a psychological problem.
Most of the participants were aware of the conditions that
triggered their vocal difficulties. These included extensive
voice use (n 17, 41.5%), rhinopharyngitis (n13, 31.7%),and shouting (n2, 4.9%). Six participants (14.6%) couldnot identify a precedent and three participants (7.3%) did not
respond to this question.
Subjective vocal symptomsTable 1presents subjective vocal complaints in the 41 partici-
pants. There were a large number of vocal symptoms associated
with this voice disorder and most of them occurred at a rela-tively high frequency. Although hoarseness was predominant,
there were also symptoms of various negative changes in the
voice, for example, changes in vocal pitch, signs of an uncom-
fortable phonation (eg, voice gets tired quickly), and symptomsof physical discomfort, for example, throat pain in talking, in-
creased throat mucus, neck and chest discomfort, neck tension,
and throat constriction. Symptoms were seen at different sever-
ity levels but the higher frequency of symptoms fell into themild and moderate levels. This is further reflected by the
mean scores of the symptoms in which the highest was only
2.07 for hoarseness. All but one participant had two or more
symptoms.
The duration of symptoms varied, with a mean of 40.36
months (SD36.8). The shortest duration of constantly pres-ent dysphonia in these participants was 3 months and the lon-
gest was almost 10 years. Intermittent symptoms were not
included in the duration of voice problem.
Factor analysis and reliability analysis of the self-re-
ported vocal symptoms. From the initial 19 items, the
item complete voice loss was discarded as no participant re-
ported this symptom; 18 items were subjected to factor and re-
liability analysis. Cronbachs alpha for the total scale of 18
items was 0.909. Item-total correlations (0.4080.733) and al-
pha if item deleted statistics indicated that all items contributed
equally to the scale, hence none was deleted. Although the sam-
ple size was relatively small for factor analysis, KMO measure
of sampling adequacy for the sample was 0.79. The KMO range
TABLE 1.
Self-Reported Vocal Symptoms (Multiple-Response Data)
Symptoms n %
Severity Self-Rating Score
Mean Score SD1 2 3 4
Hoarseness 35 85.4 6 12 13 4 2.07 1.21
Voice gets tired quickly 29 70.7 2 9 15 3 1.88 1.38
Out of breath in talking 29 70.7 4 12 10 3 1.71 1.33
Throat clearing 27 65.9 7 11 4 5 1.49 1.38
High notes difficulties 26 63.4 1 7 14 4 1.78 1.49
Increased vocal effort 26 63.4 4 6 14 2 1.61 1.41
Weak voice 26 63.4 4 7 13 2 1.59 1.40
Pitch change 24 58.5 6 9 7 2 1.29 1.31Throat pain in talking 23 56.1 4 5 12 2 1.41 1.43
Voice deteriorates at end of day 23 56.1 1 7 11 4 1.56 1.52
Increased throat mucus 19 46.3 7 5 4 3 1.00 1.32
Neck-chest discomfort 19 46.3 10 4 4 1 0.83 1.12
Throat constriction 17 41.5 8 4 3 2 0.80 1.19
Neck tension 15 36.6 2 7 5 1 0.85 1.24
Decreased pitch range 13 31.7 1 7 5 0 0.73 1.14
Low notes difficulties 10 24.4 1 2 7 0 0.63 1.18
Loss of voice at times 7 17.1 1 3 3 0 0.39 0.92
Tone phonation difficulties 4 9.8 0 0 4 0 0.29 0.90
Complete voice loss 0 0 0 0 0 0 0
Journal of Voice, Vol. 23, No. 2, 2009198
-
7/23/2019 Paper Patologia
5/14
for all variables (0.720.88) indicated adequate sample size for
all the variables. Bartletts test of sphericity was highly signif-
icant, also confirming that the data were suitable for factor anal-
ysis (c2384.65,df153, P< 0.001).Using factor analysis with oblique rotation (direct oblimin),
three factors explaining the largest amount of variance were ex-
tracted (Table 2). The three factors, labeled to describe the clus-
tering of variables, were as follows:
(1) Factor 1: Vocal fatigue/hyperfunction explained the
largest amount of variance (39.8%) and also contained
the highest number of variables. Cronbachs alpha for
this factor was 0.894. Item-total correlations ranged
from 0.437 to 0.761.
(2) Factor 2: Physical discomfort contained three items
and explained 9.8% of the variance. Cronbachs alpha
for this factor was 0.839. Item-total correlations ranged
from 0.64 to 0.763.
(3) Factor 3: Voice quality explained 9.3% of the vari-
ance. Cronbachs alpha was 0.84. Item-total correlations
ranged from 0.472 to 0.723.
Factors1 and 2 (r0.31) and factors 1 and 3 (r0.423) werecorrelated, confirming the need for oblique rotation.
Examiner-reported vocal symptoms. In 47 participants
with MTD, the examiner reported strained voice in 45 partici-pants (95.7%), breathiness in 43 (91.5%), and roughness in
23 (48.9%). Symptoms such as pitch breaks, glottal fry, hard
glottal attack, and voice loss were not reported.
Laryngoscopic findings
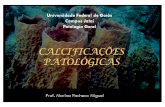
Glottal shapes. Table 3shows the glottal shape patterns ob-
served. The posterior glottal gap was defined as a triangle-shaped
gap in the posterior glottis between the two arytenoid cartilages
and posterior membranous vocal folds (Figure 1). This definition
excluded the cases in which there was a gap between the two ar-
ytenoids but no gap between the posterior vocal folds. The in-
complete glottal closure indicated the cases in which the twovocal folds did not completely close the glottis during the closed
phase (Figure 2). The spindle-shaped gap was a special case of
the incomplete closure in which the two vocal folds did not com-
pletely approach, leaving a glottal gap in the shape of a spindle
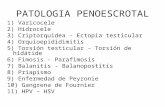
(Figure 3). An hourglass gap was defined as a glottal gap in
which there were both anterior and posterior glottal chinks,
with a small contact at approximately the middle of the membra-
nous vocal folds in the absence of mucosal lesions (Figure 4).
Supraglottic findings. Thirty-five participants had an AP
contraction: 20 had a score of 1, 10 had a score of 2, four had
a score of 3, and one had a score of 4. None had a full AP con-
traction. Eleven participants had a lateral contraction amongwhom nine had a score of 1 and two had a score of 2.
Vocal fold and arytenoid mucosa. The status of mucosa
was assessed for each vocal fold. The degree of visible mucosal
changes was minor and comparable between the two vocal
folds. The rating scores for the vocal fold smoothness ranged
from 1 to 3 on the six-point EAI rating scale. For both vocal
folds, the smoothness score was 1 for most of the rated vocal
folds. Only one participant had a score of 3 for vocal fold
TABLE 2.Characteristics of the Three Factors in Vocal Symptoms (a Cronbachs Alpha)
Vocal Symptoms
Factor 1 Factor 2 Factor 3
Loading aif item deleted Loading aif item deleted Loading aif item deleted
Voice deteriorates at end of day 0.832 0.886
Increased vocal effort 0.783 0.876
Voice gets tired quickly 0.743 0.883
Weak voice 0.681 0.879
Out of breath in talking 0.644 0.883
High notes difficulties 0.608 0.880 0.324 0.811
Neck tension 0.593 0.884
Loss of voice at times 0.575 0.894
Throat pain in talking 0.447 0.885 0.387 0.820
Increased throat mucus 0.323 0.893
Throat constriction 0.885 0.718Tone phonation difficulties 0.790 0.842Neck-chest discomfort 0.780 0.744Low notes difficulties 0.849 0.800
Decreased pitch range 0.842 0.813
Pitch change 0.724 0.834
Throat clearing 0.426 0.886 0.564 0.808
Hoarseness 0.530 0.835
Variance explained (%) 39.8 9.8 9.3
a 0.894 0.839 0.840
Duong Duy Nguyen, et al MTD in Teacher 199
-
7/23/2019 Paper Patologia
6/14
smoothness bilaterally. Similarly, the straightness scores also
ranged from 1 to 3 and most of the participants had a score of
1. Pearsons correlation coefficients between smoothness and
straightness scores for the left and right vocal folds were 0.72
and 0.74, respectively (P< 0.01). This finding indicated that
the straightness of the vocal fold medial edge depended largely
on the status of the vocal fold mucosa.Table 4 shows the findings on the vocal fold mucosa. In-
creased mucus secretion was found in 34% and 36.2% of the
participants for the left and right vocal folds, respectively. Mu-
cus was often present either on the superior surface of the vocal
folds or at the middle of the medial vibrating edge where it
could be mistaken as vocal nodule. By having the participant
do a slight throat clearing, the mucus was removed but returned
shortly afterward. Additionally, mild to moderate thickness,
edema, and erythema of the vocal folds were also observed.
The arytenoid mucosa was also examined including the inter-
arytenoid space. Signs of inflammation, including edema and
erythema, were noted in 30 participants (63.8%). The interary-
tenoid space showed erythema lesion in 19 participants(40.4%). The main characteristic of arytenoid mucosal inflam-
mation was uneven distribution; the lesions did not diffuse all
over the surface of the arytenoids but concentrated in clusters,
mostly in the areas near the upper esophageal sphincter and
the aryepiglottic fold.
Neck. The suprahyoid muscles increased tonicity in 31 partic-
ipants (66%) and laryngeal vertical position was found to rise in
29 participants (61.7%). There was a strong correlation between
increased suprahyoid muscle tension and elevated larynx height
during phonation (c239.1,P < 0.001).
DISCUSSION
Vocal characteristics of MTD in Vietnamese teachersThis study found that the Vietnamese teachers with MTD had
more vocal symptoms than previously reported in nontonal lan-
guage speakers.3,13 The symptoms covered various aspects of
dysfunction in the phonation system, for example, problems in
the larynx (eg, hoarseness), lack of effective coordination be-
tween phonation and breathing support (eg, out of breath in
talking), disorders in the related musculoskeletal system (eg,
neck chest discomfort), functional sensorimotor problems ofthe vocal tract (eg, throat constriction and throat pain in talk-
ing), and the possible coexistence of cofactors (eg, increased
throat mucus). Symptoms reliably fitted three factors: vocal fa-
tigue/hyperfunction, physical discomfort, and voice quality, rep-
resenting three major areas of dysfunction in this voice disorder.
However, a number of vocal symptoms of MTD reported in
TABLE 3.
Glottal Shape Findings
Categories
n by Age
n %2229 3039 4049 5054
Incomplete 2 3 14 2 21 44.7
Posterior gap 2 4 7 1 14 29.8
Hourglass 1 1 3 1 6 12.8
Spindle 0 0 3 1 4 8.5
Complete 0 0 1 1 2 4.3
Total 5 8 28 6 47 100
FIGURE 1. Posterior glottal gap.
FIGURE 2. Incomplete glottal closure.
FIGURE 3. Spindle-shaped glottal gap.
Journal of Voice, Vol. 23, No. 2, 2009200
-
7/23/2019 Paper Patologia
7/14
previous studies were not observed in this study, for example,
hard glottal attack, stridency, pitch breaks, and glottal fry (exceptfor the creaky voice associated with the linguistic laryngealiza-
tion in the broken tone and the dropped tone).Differences in linguistic characteristics between Vietnamese
and nontonal languages may have contributed to the findings.
This possibility might explain for the absence of some symp-
toms of MTD reported in previous studies. It is not known
howlinguisticfeatures affect vocalquality in voicedisorders be-
cause the cross-linguistic manifestation of voice disorders hasnotbeen well investigated. However, thedifferent uses of thelar-
ynx by tonal and nontonal languages suggest that there may be
an association between the linguistic background and the vocal
output in a voice disorder. When the larynx is used for creating
tonal contrasts, the laryngeal features pertinent to the phonolog-
ical characteristics of the tonal language may interact with those
generated by the voice disorder. The actual mechanism of inter-
action is not yet understood and should be studied in future re-
search. In Vietnamese, such an interaction may exist given
that the larynx performs two linguistically significant phenom-
ena, that is, pitch variation at word level and nonmodal phona-
tion types (ie, laryngealization and breathiness). These are
distinctive features of the language, which may result in certaindifferences in the symptomatology of MTD as compared with
nontonal language speakers. In nontonal languages, pitch varia-
tion and phonation types are not lexically significant. Therefore,
the pattern of interaction between linguistic factors and voice
disorders, if any, may be different from that in tonal languages.
For example, interactionmay exist between vocaltract activities
and voice disorders rather than between linguistically relevantlaryngeal features and voice disorders. The interaction pattern
may even be different between nontonal languages because of
differences in articulatory characteristics. This leads to the
fact that differences in dysphonic symptoms because of linguis-
tic differences may occur not only between tonal and nontonal
language speakers but also between nontonal languagespeakers. For example, Lorch and Whurr22 investigated the per-
ceptual characteristics of spasmodic dysphonia in a number of
French participants. They applied the same diagnostic criteria
for this voice disorder as those used in studies on English partic-
ipants. They did not find pitch breaks, a symptom normally
found in English spasmodic dysphonia patients. In contrast,
some symptoms not considered important in English speakers
were found to be prominent, for example, harshness and breath-
iness. Clearly, the linguistic-specific effects of laryngeal and vo-
caltract features onvoice disordersneed to be taken into account
and should be investigated further.
The higher number of MTD symptoms in this study than pre-
viously reported might be attributed to a well-recognized prob-
lem in the teaching voice in general, that is, voice problems in
teachers often involve a high number of symptoms23 regardless
of the underlying diagnosis. This perhaps results from the im-
pact of various factors on their voices such as vocal skills, pos-
ture, physical and psychological conditions, and teaching
environment24,25. However, the effect of factors related to sea-
sons and the stage of the school year are not well understood. In
the first authors experience, teachers suffer from more voice
problems in the transitional periods between autumn and winter
and between winter and spring, probably due to low humidity
and episodes of viral infection in the upper respiratory tract.
Additionally, teachers tend to have more problems with theirvoices toward the end of a school year, particularly those related
to vocal fatigue. Because this study spanned a period from Sep-
tember 2005 (autumn and commencement of school year in
Vietnam) to July 2006 (summer, two months after the school
year), these factors may have played some role in adding
more vocal symptoms into the vocal profile of MTD in these
Vietnamese teachers. Future research designed to assess the
effect of these factors on the teaching voice is needed.
The findings may have been compromised by testing errors
due to the use of subjective measures (questionnaires and exam-
iners perceptual voice assessment) that obscured actual
FIGURE 4. Hourglass glottal gap.
TABLE 4.
Mucosal Findings
Findings and
Rating Scores
n
Left Vocal Fold Right Vocal Fold
Mucus
1 14 15
2 2 2
Total 16/47 17/47
Thickness
1 9 9
2 1 1Total 10/47 10/47
Edema
1 7 7
2 3 3
3 1 1
Total 11/47 11/47
Erythema
1 6 5
3 1 1
Total 7/47 6/47
Duong Duy Nguyen, et al MTD in Teacher 201
-
7/23/2019 Paper Patologia
8/14
physiological differences in the symptoms of MTD between
this and previous reports. Higher frequency of self-reported
symptoms might have resulted from the possibility that some
participants included intermittent symptoms. Other factors af-
fecting subjective self-report include possible misunderstand-
ing of the description of some of the vocal symptoms in the
questionnaire and variability in teachers awareness of and sen-
sitivity to their vocal symptoms. Although the result of factoranalysis in the present study was encouraging, the sample
size was small and replication with a larger group is needed.
Laryngeal characteristics of MTD in VietnameseteachersWe did not find any differences in laryngeal characteristics of
MTD compared with previous studies, suggesting that, the laryn-
geal symptoms observed were not specific to this tonal language.
The major symptoms found were glottal gaps and supraglottic
constriction, which have been documented in nontonal language
speakers.2,3 These findings appeared not to support the involve-
ment of the phonological characteristics of Vietnamese in themanifestation of MTD. Probably, linguistic factors in this tonal
language, for example, phonation types, may contribute to
some differences in vocal symptoms but they might not necessar-
ily result in a distinctive laryngeal feature in this voice disorder.
This might stem from twopossibilities. Firstly, the tonal language
speakers who have MTD might voluntarily reduce the magnitude
of lexically significant phenomena in an attempt to adapt to the
changed laryngeal muscle tension or vocal tract discomfort asso-
ciated with MTD. For example, they might reduce pitch move-
ment or laryngealization to avoid vocal fatigue. As a result,
those linguistic phenomenacould not affectthe laryngeal features
in this voice disorder. However, the linguistic content in the re-
stricted tones might not be sufficiently contrastive and would re-
sult in tone misperception.
Secondly, the differences in vocal symptoms without any dif-
ference in laryngeal findings compared with previous studies
might also result from the fact that MTD is an unexplained voice
disorder in which the laryngeal appearance may not precisely re-
flect the underlying vocal function and control mechanism. It has
been known that MTD is characterized by anincongruity be-
tween vocal symptoms and laryngeal findings,3 which is related
to the fact that many of its symptoms are behaviorally induced
and behaviorally modifiable.1 Furthermore, the laryngeal find-
ings in MTD are not specific: they may also be seen in some peo-
ple whose voice is not dysphonic. For example, Linville
26
foundthat both young and elderly female speakers showed a high inci-
dence of glottal gaps. The patterns of glottal gaps seen in young
women were posterior gap and incomplete closure. In elderly
women, the common patterns were anterior gap and spindle-
shaped gap. Sama et al27 found that vocally healthy people
also possessed many features of MTD, for example, incomplete
vocal fold adduction, AP contraction, and ventricular fold con-
traction. The incongruity between vocal and laryngeal symptoms
of MTD, and the nonspecificity of its laryngeal symptoms sug-
gest that, regardless of the language used, laryngeal findings
alone may not constitute a diagnosis of MTD.
A number of methodological limitations should be noted.
First, the laryngoscopic findings in this study were collected us-
ing a fiberoptic right-angled rigid laryngoscope at a school set-
ting. Whether the findings can be generalized to a larger MTD
population or whether they are comparable with previous re-
ports on MTD using transnasal flexible fiberopticlaryngoscopy
needs to be validated. Sodersten and Lindestad28 reported that
the estimated degree of incomplete glottal closure was signifi-cantly higher during rigid telescopy than during flexible laryn-
goscopy especially in soft phonation. Their results might have
resulted from the fact that a rigid telescope tends to better mag-
nify the details in the observed field than the flexible laryngo-
scope. Second, although the purpose of the study was to
examine how MTD presented in tonal language speakers, the
study did not use tone-specific speech samples for examination
because it only used rigid laryngoscopy, which precluded the
use of connected speech samples. Additionally, the setting of
the study did not allow more complex laryngeal examination
to be performed. Although the use of the /i/ sound facilitated la-
ryngeal examination, it was not a suitable stimulus to find the
potential glottal configuration specific to this tonal language.As a result, the findings did not allow a conclusive statement
to be made on the potential role of linguistic-specific factors
in the manifestation of this voice disorder. Laryngeal movement
during various vocal tasks should be examined in future studies
of MTD in tonal language speakers. Acoustic and physiological
investigation of tone production in normal and dysphonic voi-
ces should also be conducted and laryngeal findings should
be interpreted based on data from those measurements. Find-
ings from such studies might reveal useful information for un-
derstanding the laryngeal function during lexical tone
phonation in normal and pathological states of the larynx.
CONCLUSIONOur study provided preliminary data about MTD in primary
school teachers who used a tone language and identified a range
of vocal symptoms in teachers with a specified voice disorder.
The vocal symptoms of MTD identified in this study may rep-
resent a wide range of disorders in the phonatory system. The
major groups of symptoms included hyperfunction, vocal fa-
tigue, impaired voice quality, and physical dysfunction. Be-
cause of the multidimensional nature of MTD, in diagnosis of
this voice disorder particularly in teachers, it is necessary to
look for all voice symptoms rather than focus on voice quality.
The higher number of vocal symptoms overall and the absence
of particular vocal symptoms found in previous MTD studies innontonal language speakers suggest that symptom presentation
of MTD may be influenced by linguistic factors. Nevertheless,
the symptom configuration of MTD of the tonal languageper se
needs to be separated from effects on the voice of teaching.
Abnormal glottal closure in the absence of structural lesions
of the vocal folds was the major laryngeal characteristic in these
participants. Five types of glottal closure were observed. How-
ever, the design of the study did not allow confirmation of an
association between the use of a tonal language and the specific
pattern of glottal shape and other laryngeal features in this voice
disorder. This issue should be examined in future research.
Journal of Voice, Vol. 23, No. 2, 2009202
-
7/23/2019 Paper Patologia
9/14
Acknowledgment
The authors thank the school teachers who participated in this
study and the Education and Training Department of Thai
Nguyen City, Vietnam for supporting this study. We also thank
the two anonymous reviewers for their helpful comments on themanuscript.
REFERENCES1. Verdolini K, Rosen C, Branski R.Classification Manual for Voice Disor-
dersI. Mahwah, NJ: Lawrence Erlbaum Associates; 2006.
2. Morrison MD, Rammage LA. Muscle misuse voice disorders: description
and classification.Acta Otolaryngol. 1993;113:428-434.
3. Koufman JA, Blalock PD. Functional voice disorders. Otolaryngol Clin
North Am. 1991;24:1059-1073.
4. Morrison MD, Rammage LA, Belisle GM, Pullan CB, Nichol H. Muscular
tension dysphonia. J Otolaryngol. 1983;12:302-306.
5. Altman KW, Atkinson C, Lazarus C. Current and emerging concepts in
muscle tension dysphonia: a 30-month review. J Voice. 2005;19:261-267.
6. Rammage L, Morrison M, Nichol H.Management of the Voice and Its Dis-
orders. San Diego, CA: Singular-Thomson Learning; 2001.
7. Sapir S. Psychogenic spasmodic dysphonia: a case study with expert opin-
ions.J Voice. 1995;9:270-281.8. Sapienza CM, WaltonS, MurryT. Adductorspasmodic dysphonia and mus-
cular tension dysphonia: acoustic analysis of sustained phonation and read-
ing.J Voice. 2000;14:502-520.
9. Ladefoged P. The features of the larynx.J Phonetics. 1973;1:73-83.
10. Nguyen LV, Edmondson JA. Tones and voice quality in modern Northern
Vietnamese: instrumental case studies. Mon-Khmer Stud. 1998;28:1-18.
11. Ohala J. Production of tone. In: Fromkin V, ed. Tone: A Linguistic Survey.
New York, NY: Academic Press; 1978:5-39.
12. Belisle GM, Morrison MD. Anatomic correlation for muscle tension
dysphonia.J Otolaryngol. 1983;12:319-321.
13. Morrison M, Nichol H, Rammage L. Diagnostic criteria in functional
dysphonia. Laryngoscope. 1986;94:1-8.
14. Nguyen DD, Kenny DT. Impact of muscle tension dysphonia on tone
height, contour and fundamental frequency movements in Vietnamese
tones. Presented at: The 5th Asia-Pacific Conference on Speech, Language
and Hearing; July 913, 2007; Brisbane, Australia.
15. Smith E, Lemke J, Taylor M, Kirchner HL, Hoffman H. Frequency of voice
problemsamong teachers and other occupations.J Voice. 1998;12:480-488.
16. Mathieson L. The Voice and Its Disorders. London: Whurr Publishers;
2001.
17. Peppard RC, Bless DM. The use of topical anesthetic in videostroboscopic
examination of the larynx. J Voice. 1991;5:57-63.
18. Field A. Discovering Statistics Using SPSS. London: Sage Publications;
2005.
19. Kaiser HF. An index of factorial simplicity.Psychometrika. 1974;39:31-36.
20. Hutcheson GD, Sofroniou N.The Multivariate Social Scientist: Introduc-
tory Statistics Using Generalized Linear Models. London: Sage Publica-
tions; 1999.
21. Kaiser HF. The application of electronic computers to factor analysis.Educ
Psychol Meas. 1960;20:141-151.
22. Lorch M, Whurr R. Cross-linguistic study of vocal pathology: perceptual
features of spasmodic dysphonia in French-speaking subjects. J Multiling
Commun Disord. 2003;1:35-52.
23. Smith E, Gray SD, Dove H, Kirchner L, Heras H. Frequency and effects of
teachers voice problems. J Voice. 1997;11:81-87.
24. Kooijman PG, de Jong FI, Oudes MJ, Huinck W, van Acht H, Graamans K.
Muscular tension and body posture in relation to voice handicap and voicequality in teachers with persistent voice complaints.Folia Phoniatr Logop.
2005;57:134-147.
25. Kooijman PGC, de Jong FICRS, Thomas G, Huinck W, Donders R,
Graamans K, Schutte HK.Riskfactors forvoice problems inteachers. Folia
Phoniatr Logop. 2006;58:159-174.
26. Linville SE. Glottal gap configurations in two age groups of women.
J Speech Hear Res. 1992;35:1209-1215.
27. Sama A, Carding PN, Price S, Kelly P, Wilson JA. The clinical features of
functional dysphonia. Laryngoscope. 2001;111:458-463.
28. Sodersten M, Lindestad PA. A comparison of vocal fold closure in rigid
telescopic and flexible fiberoptic laryngostroboscopy. Acta Otolaryngol.
1992;112:144-150.
Duong Duy Nguyen, et al MTD in Teacher 203
-
7/23/2019 Paper Patologia
10/14
Appendix 1
QUESTIONNAIREEvaluation and management of voice disorders
Please fill in this questionnaire with your best knowledge. Information you provide in this questionnaire will be kept
confidential and will be used only for the purpose of this study.
PART 1: PERSONAL DETAILS1. Full name (Print):.....................................................................Sex (circle): Male/Female
2. Date of birth:............................. Ethnic group:...........................Contact number:........................................................
3. Name of school: ...........................................................................................................................................................
PART 2: OCCUPATIONAL DETAILS
4. What type of school are you teaching (e.g. primary or secondary)? ............................................................................
5. How long have you been teaching (years and months)? ..............................................................................................
6. What subjects are you teaching? ..................................................................................................................................7. How many days per week are you teaching?................................................................................................................
8. On average, how many hours do you teach per day? ...................................................................................................
9. Are you involved in any other vocal activities and what are they? ..............................................................................
10. Your current psychological state in teaching:
Comfortable Stressed Worried
PART 3: YOUR VOCAL USE11. Do you speak loudly in teaching?
Never Sometimes Frequent
12. Do you speak over background noise?
Never Sometimes Frequent
13. Do you ever shout or scream during teaching?
Never Sometimes Frequent
14. Have you ever spoken or sung in your wrong register?
Never Sometimes Frequent
15. Do you often clear your throat?
Never Sometimes Frequent
16. Do you plan any voice rest after teaching?
Never Sometimes Frequent
17. Do you seek voice rest during flu/pharyngitis/upper respiratory tract infections?
Never Sometimes Frequent
18. You think that when you are teaching, you should speak:
With normal voice Louder As loud as you can
19. Do you know how to use your voice efficiently?.........................................................................................................
20. When you have a voice problem, do you stay at home or still go to work? .................................................................
PART 4: VOCAL HISTORY
21. Have you ever had any voice problem in the past? ......................................................................................................
If yes, list the symptoms you have had:..........................................................................................................................................................................................................................................................................................................................................
Journal of Voice, Vol. 23, No. 2, 2009204
-
7/23/2019 Paper Patologia
11/14
22. Did you seek treatment for those problems?
Yes Methods of treatment:..................................................................................................
Your voice after treatment Normal Improved The same Worsened
No
PART 5: YOUR CURRENT VOICE
23. In your opinion, your current voice is (circle the most appropriate):
1. Very good 2. Good 3. Fair 4. Bad 5. Very bad24. Do you have any problem with your voice currently?
No
Yes Which symptoms of the following do you currently have?
(Mark x in the appropriate boxes to indicate the symptoms you have, and give your rating for the severity of each
of those symptoms: 1 = Slight; 2 = Mild; 3 = Moderate; 4 = Severe. For the symptom you do not have, please leave
the box blank):
SeveritySymptoms1 2 3 4
Hoarseness
Complete voice loss
Loss of voice at times
Pitch change
Reduced pitch rangeDifficulties with high notes
Difficulties with low notes
Weak voice
Voice gets tired quickly
Voice deteriorates at the end of a teaching day
Difficulties in tone phonation
Running out of breath in talking
Increased vocal effort
Neck tension
Throat pain in talking
Feel like a lump in the throat
Increased mucus in throat
Throat-clearing
Discomfort in neck/chest
25. If you have other symptoms not mentioned above, please list them here ....................................................................
....................................................................................................................................................................................................
26. How long have you had the current voice problem?....................................................................................................
27. In what situation did you have the current voice problem:
After rhinopharyngitis After a period of intensive voice use After loud speaking Not sure
Other:...........................................................................................................................................................
28. Which of the following are the causes of your voice problem (check the appropriate boxes):
Intensive voice use Loud speaking No vocal training
Frequent shouting Pharyngitis Other respiratory tract infections
Speaking over noise Not sure Other causes:.....................................
29. Have you had treatment for the current voice problems?
Yes Methods of treatment:............................................................................................................
Your voice after treatment Normal Improved The same Worsened
No
Duong Duy Nguyen, et al MTD in Teacher 205
-
7/23/2019 Paper Patologia
12/14
PART 6: IMPACT OF VOICE PROBLEMS
30. With your current voice problem, what tone is the most difficult for you to phonate:.................................................31. With your current voice problem, do you phonate one tone to be another?
0. No 1. Rarely 2. Sometimes 3. Frequently 4. Constantly
What tone to be what tone:
32. The degree of difficulties the listeners have when listening to your voice:
0. No 1. Very little 2. Moderate 3. Much 4. Very much33. Do you have to repeat what you have just said to the audience?
0. No 1. Very little 2. Moderate 3. Much 4. Very much34. How does your voice problem affect your job performance?
0. No 1. Very little 2. Moderate 3. Much 4. Very much35. When you have voice problem, you think that teaching is:
0. The same 1. Slightly difficult 2. Rather difficult 3. Difficult 4. Very difficult
36. How does your voice problem affect your daily conversation?
0. No 1. Very little 2. Moderate 3. Much 4. Very much37. In general, how does your voice problem affect your life?
0. No 1. Very little 2. Moderate 3. Much 4. Very much
Date..............
Signature:.
END OF QUESTIONNAIRE
Journal of Voice, Vol. 23, No. 2, 2009206
-
7/23/2019 Paper Patologia
13/14
Appendix 2
LARYNGOSCOPIC FORM
I. Personal details
- Full name:..................................................................D.O.B.:.....................M/F. Ethnic group:....................................
- Occupation:.......................... Address: ..........................................................................................................................- Contact number:....................................Hospital code:.................................Study code:..............................................
II. History
ENT:
Voice problems:
Allergy Smoking Alcohol Reflux Other
III. Larynx and voice assessment
1. Perceptual assessment
Pitch: Average High Low
Intensity: Average Loud Soft
Normal Rough Breathy
Strained Pitch breaks Phonation breaks
Creaky Diplophonia Tremor
Voice quality:
Other qualities:.........................................................................................
Tone phonation: Normal Difficulties in (circle):
T1 T2 T3 T4 T5 T5s T6 T6s
Remarks:.......................................................................................................................
Phonation type: Breathiness (T2, T4): Yes No Tones:.................................
Laryngealization (T3, T6): Yes No Tones:.................................
0 1 2 3 4 5Voice rating:
Normal Severe dysphonia
2. Glottal shape (circle the most appropriate one)
Remarks:..........................................................................................................................................................................
3. Supraglottic activities (circle the best number)
A-P contraction0 1 2 3 4 5
Absence Slight Vocal fold obscured
Lateral contraction
0 1 2 3 4 5
Absence Slight Vocal fold obscured
Duong Duy Nguyen, et al MTD in Teacher 207
-
7/23/2019 Paper Patologia
14/14
4. Vocal fold medial edge smoothnessLeft 0 1 2 3 4 5
Smooth Rough
Right 0 1 2 3 4 5 Smooth Rough
Remarks:..........................................................................................................................................................................
5. Vocal fold medial edge straightness
Left 0 1 2 3 4 5 Straight Irregular
Right 0 1 2 3 4 5 Straight Irregular
Remarks:..........................................................................................................................................................................
6. Vocal fold mucosa (circle the best number)
Findings Left vocal fold Right vocal fold
Edema
No Severe
0 1 2 3 4 5
No Severe
0 1 2 3 4 5
Erythema 0 1 2 3 4 5 0 1 2 3 4 5
Thickening 0 1 2 3 4 5 0 1 2 3 4 5
Mucus 0 1 2 3 4 5 0 1 2 3 4 5
Dilation 0 1 2 3 4 5 0 1 2 3 4 5
Sulcus 0 1 2 3 4 5 0 1 2 3 4 5Contact ulcers 0 1 2 3 4 5 0 1 2 3 4 5
Plaque 0 1 2 3 4 5 0 1 2 3 4 5
Nodules
Polyps
Other
7. Arytenoids
Mucosa: Normal Edema Erythema Ulcer
Symmetry: Yes No Palsy (circle) Left -- Right
Vocal processes: Normal Thickened Ulcer
Interarytenoid space: Normal Erythema Ulcer
Remarks: .........................................................................................................................................................................
8. Lower pharynx and piriform sinuses
Normal Edema Erythema Mucus
Remarks:..........................................................................................................................................................................
IV. Neck
1. Larynx height in phonation
Elevated Unchanged
2. Supra- and infra-hyoid muscular tone
High Average Low
Date:
Examiner:
Journal of Voice, Vol. 23, No. 2, 2009208