
Paper for indian journal of population education
24
Yade Lal Tekhre and Alka Sharma CONTRACEPTION USE AMONG MALES IN HIMACHAL PRADESH (Research Paper for Indian Journal of Population Education) Introduction: The development of safe, effective and reversible contraceptive methods for men is an important goal in expanding the choices available to couples to regulate their fertility. The advent of an effective and reversible systemic male contraceptive method should provide a valuable alternative to the limited options of the condom, vasectomy and withdrawal that are currently available to men. The 1994 International Conference on Population and Development (ICPD) Programme of Action states that “the aim of family planning programmes must be to enable couples and individuals to decide freely and responsibly the number and spacing of their children and to have the information and means to do so and to ensure informed choice and make available a full range of safe and effective methods (United Nations, 1995). The shortcomings of currently available methods are a major barrier to the greater involvement of men in family planning. Increasing the choice of methods, which include those available to men, should go a long way in responding to the diverse individual contraceptive needs of couples. A regional workshop on Gender, Sexuality and Reproductive Health in Asia and Pacific held in January 1996 in the Philippines, found that in 12 countries of the region, all of which had low levels of male contraceptive use, little research had yet been done to find out the root of this problem. This fact reflects that there has been little real concern for reaching men and promoting more gender-balanced use of contraceptives. Despite great progress over the last several decades, more than 120 million women worldwide want to prevent pregnancy, but they and their partners are not using contraception; reasons for unmet need are many: services and supplies are not yet available everywhere or choices are limited; fear of social disapproval or partner’s opposition pose formidable barriers; worries of side effects and health concerns hold some people back; others lack
-
Upload
yade-tekhre -
Category
Data & Analytics
-
view
39 -
download
2
Transcript of Paper for indian journal of population education

Yade Lal Tekhre and Alka Sharma
CONTRACEPTION USE AMONG MALES IN HIMACHAL PRADESH(Research Paper for Indian Journal of Population Education)
Introduction: The development of safe, effective and reversible contraceptive methods for men is an important goal in expanding the choices available to couples to regulate their fertility. The advent of an effective and reversible systemic male contraceptive method should provide a valuable alternative to the limited options of the condom, vasectomy and withdrawal that are currently available to men. The 1994 International Conference on Population and Development (ICPD) Programme of Action states that “the aim of family planning programmes must be to enable couples and individuals to decide freely and responsibly the number and spacing of their children and to have the information and means to do so and to ensure informed choice and make available a full range of safe and effective methods (United Nations, 1995). The shortcomings of currently available methods are a major barrier to the greater involvement of men in family planning. Increasing the choice of methods, which include those available to men, should go a long way in responding to the diverse individual contraceptive needs of couples.
A regional workshop on Gender, Sexuality and Reproductive Health in Asia and Pacific held in January 1996 in the Philippines, found that in 12 countries of the region, all of which had low levels of male contraceptive use, little research had yet been done to find out the root of this problem. This fact reflects that there has been little real concern for reaching men and promoting more gender-balanced use of contraceptives. Despite great progress over the last several decades, more than 120 million women worldwide want to prevent pregnancy, but they and their partners are not using contraception; reasons for unmet need are many: services and supplies are not yet available everywhere or choices are limited; fear of social disapproval or partner’s opposition pose formidable barriers; worries of side effects and health concerns hold some people back; others lack knowledge about contraceptive options and their use, these pe0ple need help now.
Methodology: The main purpose of this study was to explore the problem of acceptance of male contraceptives to recommend appropriate interventions towards increasing acceptance of male contraceptive usages.
Study area: Keeping in view of the high prevalence of male contraceptive acceptance in the country, the State of Himachal Pradesh was selected; further, the District Kullu was selected for the high acceptance of NSV as compared to other districts. In Kullu district, two Primary Health Centres were selected based on high and low prevalence of male contraceptive acceptance, as representative of rural area and from urban area two wards of district Kullu head quarter were selected for the study.
Study population: Married male whose wives were in reproductive age group were selected for gathering primary data. To collect qualitative information, focus group discussions [FGD] were conducted in each Primary Health Centres and urban wards.
Sampling Procedure: For the broad coverage and actual representation, multistage-sampling procedure was followed. A total of one hundred seventy four married male from two PHC (head

quarter and non-headquarter village) were interviewed randomly. From the district head quarter, two wards were selected randomly and from each ward, twenty-five respondents were interviewed, fifty-one respondents were from both the wards. Two focus group discussions in each PHC were conducted. Similarly, one FGD in each sampled ward were conducted. 225 married male whose wives were in reproductive age group were randomly interviewed from rural and urban area. Fifty-one were from urban and 174 respondents were from rural segment.
Data collection Tools and Techniques: Quantitative data were collected through the semi-structured pre-tested schedule; containing open-ended, close-ended and multiple response type of questions were incorporated. To collect qualitative information, six Focus Group Discussions (FGDs) were organized in both the sampling unit (rural and urban). Data were analysed in SPSS packages. Complementarily, these tables were edited and re framed in MS-Word. The qualitative data through focus group discussion were analysed by the investigators manually.
General Objective
To study the determinants and major barriers of contraceptive usages in men and to suggest an intervention package which will enhance contraceptive acceptance in men.
Specific Objectives
To study the factor that determines the contraceptive usages in married men, whose wives are in the reproductive age group.
To study the range of options available to men in contraceptive usage
To identify the factors which influence male support to their spouses for use of contraceptive.
Background characteristics of the respondents: The table mentioned below shows that majorities (90%) of respondents were from 25-49 years of age group and 97.8% of them were literate, 40.4 % were cultivator; about one-fifth of them were in government job and business, respectively. The respondents were belongs to both the residence - urban (22.7%) and rural (77.3%). Majority of them were Hindu (92 %), whereas 6.7% were Buddhist, 0.4 % and 0.9 % were Sikh and Christians, respectively. Furthermore, 10.2% of them belong to Schedule Castes, 7.6 % were Scheduled Tribes, 2.2 % were Other Backward Castes and 80% belongs to general caste. 63.1% of the respondents were from nuclear family, 32.4% were from joint family while rests 4.4 % were from extended family.

Figure 1: Distribution of respondents according to age
Table 1: Socio-Demographic profile of the Respondents
Age groupResidence
TotalRural Urban
20-24 7 (3.1) 1 (0.4) 8 (3.6) 25-29 34 (15.1) 6 (2.7) 40 (17.8) 30-34 43 (19.1) 7 (3.1) 50 (22.2) 35-39 36 (16.0) 11 (4.9) 47 (20.9) 40-44 27 (12.0) 16 (7.1) 43 (19.1) 45-49 18 (8.0) 6 (2.7) 24 (10.7) 50-54 6 (2.7) 3 (1.3) 9 (4.0) 55 + 3 (1.3) 1 (0.4) 4 (1.8) Total 174 (77.3) 51 (22.7) 225 (100.0)
Level of Education
Illiterate 4 (1.8) 1 (0.4) 5 (2.2) Literate 11 (4.9) 2 (0.9) 13 (5.8) Primary 29 (12.9) 4 (1.8) 33 (14.7) Middle 43 (19.1) 8 (3.6) 51 (22.7) H. Secondary 72 (32.0) 22 (9.8) 94 (41.8) Graduate 12 (5.3) 10 (4.4) 22 (9.8) PG & above 3 (1.3) 4 (1.8) 7 (3.1) Total 174 (77.3) 51 (22.7) 225 (100.0)
Occupation Cultivator 84 (37.3) 7 (3.1) 91 (40.4) Labourers 10 (4.4) 1 (0.4) 11 (4.9) Private Job 15 (6.7) 6 (2.7) 21 (9.3) Govt. Job 31 (13.8) 20 (8.9) 51 (22.7) Not Working 4 (1.8) 1 (0.4) 5 (2.2) Business 30 (13.3) 16 (7.1) 46 (20.4) Total 174 (77.3) 51 (22.7) 225 (100.0)
1.8%
4%
10.7%
19.1%
20.9%22.2%
17.8%
3.6%
Distribution of Respodent according to Age Group 20-24
25-29
30-34
35-39
40-44
45-49
50-54
55 +

Caste SC 18 (8.0) 5 (2.2) 23 (10.2) ST 14 (6.2) 3 (1.3) 17 (7.6) OBC 2 (0.9) 3 (1.3) 5 (2.2) Others 140 (62.2) 40 (17.8) 180 (80.0) Total 174 (77.3) 51 (22.7) 225 (100.0)
Religion Hindu 159 (70.7) 48 (21.3) 207 (92.0) Sikh 1 (0.4) -- 1 (0.4) Christian 1 (0.4) 1 (0.4) 2 (0.9) Buddhist 13 (5.8) 2 (0.9) 15 (6.7) Total 174 (77.3) 51 (22.7) 225 (100.0)
Family Type
Nuclear 112 (49.8) 30 (13.3) 142 (63.1) Joint 55 (24.4) 18 (8.0) 73 (32.4) Extended 7 (3.1) 3 (1.3) 10 (4.4) Total 174 (77.3) 51 (22.7) 225 (100.0)
Figures within parenthesis represent percentage. Table 2: Distribution of the respondents according to Age at which they come to know
about various Family Planning Methods
Age group
Family Planning MethodsCondom Oral Pills Cu-T Vasectomy Tubectomy Withdrawal Safe Periodn % n % n % n % n % n % n %
10-14 17 7.6 3 1.3 2 .9 11 4.9 10 4.415-19 115 51.1 68 30.2 38 16.9 93 41.3 94 41.8 6 2.7 5 2.220-24 61 27.1 100 44.4 87 38.7 65 28.9 58 25.8 49 21.8 45 20.025-29 19 8.4 22 9.8 36 16.0 22 9.8 33 14.7 17 7.6 18 8.030-34 5 2.2 10 4.4 6 2.7 2 .9 5 2.2 3 1.3 2 .935-39 2 .9 4 1.8 11 4.9 3 1.3 5 2.240-44 2 .9 1 .4 1 .445 + 6 2.7 16 7.1 45 20.0 28 12.4 19 8.4 150 66.7 155 68.9Total 225 100.0 225 100.0 225 100.0 225 100.0 225 100.0 225 100.0 225 100.0
Large variations were found between different age groups with regard to knowledge of various family planning methods. Condom was known to 50.1 per cent of the sample respondents in the age group of 15-19 years and 27.1 per cent in the age group of 20-24 years. Oral Pills was known by 44.4 per cent, Cu-T by 38.7 per cent, vasectomy by 28.9 per cent, Tubectomy by 25.8 per cent, withdrawal by 21.8 per cent and safe period by 20 per cent in the age group of 20-24 years. Withdrawal and safe period were known at later age after 45 years of age by 66.7 per cent and 68.9 per cent respectively. Surprisingly, in case of Cu-T, vasectomy, tubectomy and oral pill, it was known after 45 years of age by 20 per cent, 12.4 per cent, 8.4 per cent and 7.1 per cent respectively. Below 14 years of age 7.6 per cent were known about condom, followed by 4.9 per cents for vasectomy, 4.4 per cent for tubectomy and 1.3 per cent were known for oral pill.
Contraceptive needs of couples vary according to their background, purpose of contraception and age of users. The purpose of contraception for individual couples varies from postponing childbearing, spacing of births, limiting of family size and to avoid unwanted pregnancy. In this chapter attention have been paid to find out the determinants of various family planning

techniques. Each family planning methods were taken in to consideration for detailed investigations related to its behavioural aspects, clinical aspects and social aspects. Meanwhile, views, perceptions, and appropriateness of various contraceptives methods were also gathered and discussed appropriately.
Table 3: Distribution of respondents who ever used family planning methods according to their educational background (N=225)
MethodsEver used
Educational level of respondentsTotalBelow
PrimaryPrimary Middle
Higher Secondary
Graduate & Above
Condom9(6.5)
{50.0}18(13.0)
{54.5}30(21.7)
{58.8}58(42){61.7}
23(16.7){79.3}
138(100){61.3}
Oral Pill1(1.9){5.6}
10(19.2){30.3}
13(25.0){25.5}
24(46.2){25.5}
4(7.7){13.8}
52(100){23.1}
Cu-T -3(10.0)
{9.1}8(26.7){15.7}
10(33.3){10.6}
9(30.0){31.0}
30(100){13.3}
Vasectomy3(11.5){16.7}
5(19.2){15.2}
10(38.5){19.6}
7(26.9){7.4}
1(3.8){3.4}
26(100){11.6}
Tubectomy9(9.8)
{50.0}15(16.3)
{45.5}25(27.2)
{49.0}34(37.0)
{36.2}9(9.8)
{31.0}92(100){40.9}
Withdrawal 2(5.6)
{11.1}3(8.3){9.1}
7(19.4){13.7}
19(52.8){20.2}
5(13.9){17.2}
36(100){16.0}
Safe period 1(2.5){5.6}
1(2.5){3.0}
6(15.0){11.8}
26(65.0){27.7}
6(15.0){20.7}
40(100){17.8}
Total18(100){8.0}
33(100){14.7}
51(100){22.7}
94(100){41.8}
29(100){12.9}
225(100)
The above table clearly indicates that condom was used by most of the respondents (61.3%) as compared to other all methods mentioned in the Table. In further classifications according to their educational level 42 per cent were higher secondary, 21 per cent middle and 16.7 per cent were graduate and above. The trend of condom use within the educational level was quite high 79.3 per cent among graduate and above. Subsequently this pattern was followed by higher secondary 16.7 per cent, middle 58.8 per cent, Primary 54.5 per cent and below primary 50 per cent. This distribution indicates higher rate of ‘condom use as the education’ level increases. But, this linear trend is not found in case of any other method in the table. In case of Cu-T insertions the highest (31 per cent) graduate and above respondents availed the facility within their educational group. This educational group is also using Tubectomy in equal percentage (31 percentages).

Table 4: Views and perceptions of the respondents regarding Side-effect, reliability and appropriateness of the various family planning methods (N=225)
Views and perceptions
Type of family planning methods
CondomOral Pill
Cu-TVasec-tomy
Tubec-tomy
With-drawal
Safe-period
Side-effect exists 9(4.0) 79(35.1 74(32.9) 71(31.6) 75(33.3) 7(3.1) 4(1.8)
Reliability of method
181(80.4) 177(78.7) 162(72.0)183(81.3
)189(84.0) 38(16.9) 40(17.8)
Appropriate method for spacing
213(94.7) 200(88.9) 174(77.3) - - 88(39.1) 78(34.7)
In view of the respondents, about one-third felt that oral pill, Cu-T, vasectomy and tubectomy methods were having side-effects (35.1%, 32.9%, 31.6% and 33.3 per cent respectively). Only 4 per cent of them highlights about its existence in case of condom. 80.4 per cent respondents realize that condom is a reliable method. Similarly 78.7 per cent respondents for oral pills, 72 per cent for Cu-T, 81.3 per cent for vasectomy and 84 per cent for tubectomy realize about its reliability. In case of withdrawal and safe period, a very few (16.9% and 17.8%) were agreed towards its trustworthiness. Similarly, the highest (94.7%) were agreed for condom, 88.9 per cent for oral pills and 77.3 per cent for Cu-T, about appropriate method for spacing. Though, just 39 per cent and 34.7 per cent were also advocated for appropriateness as a spacing method.
The above analysis clearly indicates that nearly one-third of respondents viewed and conscious that tubectomy, oral pill, cu-T and vasectomy methods were not free from side-effects, but on the reliability of these methods, all these methods accepted as ‘reliable’. More than this, condom oral pill land Cu-T were also perceived as appropriate for spacing by large number of people. Noticeably, natural methods does not perceived much reliable and appropriate by the respondents.

Table 5: Views regarding Side-effect of various family planning methods according to the residents of respondents (N=225)
Family planning methods
Views regarding Side-effect of the methods
Locality Total Rural Urban
Condom
Side-effect existsWithin the locality
7(77.8){4.0}
2(22.2){3.9}
9(100){4.0}
No side-effectsWithin the locality
167(77.3){96.0}
49(22.7){96.1}
216(100){96.0}
Oral Pills
Side-effect existsWithin the locality
62(78.5){35.6}
17(21.5){33.3}
79(100){35.1}
No side-effectsWithin the locality
112(76.7){64.4}
34(23.3){66.7}
146(100){64.9}
Cu-T
Side-effect existsWithin the locality
58(78.4){33.3}
16(21.6){31.4}
74(100){32.9}
No side-effectsWithin the locality
116(76.8){66.7}
35(23.2){68.6}
151(100){67.1}
Vasectomy
Side-effect existsWithin the locality
59(83.1){33.9}
12(16.9){23.5}
71(100){31.6}
No side-effectsWithin the locality
115(74.7){66.1}
39(25.3){76.5}
154(100){68.4}
Tubectomy
Side-effect existsWithin the locality
58(77.3){33.3}
17(22.7){33.3}
75(100){33.3}
No side-effectsWithin the locality
116(77.3){66.7}
34(22.7){66.7}
150(100){66.7}
Withdrawal
Side-effect existsWithin the locality
6(85.1){3.4}
1(14.3){2.0}
7(100){3.1}
No side-effectsWithin the locality
168(77.1){96.6}
50(22.9){98.0}
218(100){96.9}
Safe period
Side-effect existsWithin the locality
3(75.0){1.7}
1(25.0){2.0}
4(100){1.8}
No side-effectsWithin the locality
171(77.4){98.3}
50(22.6){98.0}
221(100){98.2}
Total 174(77.3) 51(22.7) 225(100)
The above table indicates the level of side-effects between varieties of family planning methods according to residence of the respondents as well ‘within the locality’. Interestingly, it was found that almost in all the methods, there was no much difference in their views on ‘no side-effects’ based on residence. Only in case of vasectomy, about 10 per cent urban respondents were more advance in their opinion. Even though, regardless of the residence 35.1 per cent respondents for condom, 32.9 per cent for cu-T, 31.6 per cent for vasectomy and 33.3 per cent respondents for tubectomy informed that these methods were not free from side-effects in their view point.
In case of condom, only 4 per cent respondents communicate this method has some amount of side-effects. It can derive that rural and urban segment were almost in the same view for existence of side-effects.

Table 6: Perception regarding reliability of the various family planning methods according to locality of residence (N=225)
Family planning Methods
Perception regarding reliability of the methods
Locality Total Rural Urban
CondomUnreliable
Within type of locality33(75.0){19.0}
11(25.0){21.6}
44(100){19.6}
Reliable Within type of locality
141(77.9){81.0}
40(22.1){78.4}
181(100){80.4}
Oral PillsUnreliable
Within type of locality37(77.1){21.3}
11(22.9){21.6}
48(100){21.3}
Reliable Within type of locality
137(77.4){78.7}
40(22.6){78.4}
177(100){78.7}
Cu-TUnreliable
Within type of locality55(87.3){31.6}
8(12.7){15.7}
63(100){28.0}
Reliable Within type of locality
119(73.5){68.4}
43(26.5){84.3}
162(100){72.0}
VasectomyUnreliable
Within type of locality35(83.3){20.1}
7(16.7){13.7}
42(100){18.7}
Reliable Within type of locality
139(76.0){79.9}
44(24.0){86.3}
183(100){81.3}
TubectomyUnreliable
Within type of locality32(88.9){18.4}
4(11.1){7.8}
36(100){16.0}
Reliable Within type of locality
142(75.1){81.6}
47(24.9){92.2}
189(100){84.0}
Withdrawal Unreliable
Within type of locality146(78.1)
{83.9}41(21.9){80.4}
187(100){83.1}
Reliable Within type of locality
28(73.7){16.1}
10(26.3){19.6}
38(100){16.9}
Safe periodUnreliable
Within type of locality147(79.5)
{84.5}38(20.5){74.5}
185(100){82.2}
Reliable Within type of locality
27(67.5){15.5}
13(32.5){25.5}
40(100){17.8}
Total 174(77.3) 51(22.7) 225(100)
The above table indicates the perception regarding ‘reliability’ of various family planning methods according to rural and urban residence. It was found that tubectomy was perceived to be reliable by 84 per cent, vasectomy by 81.8 per cent, condom by 80.4 per cent and Cu-T by 72 per cent. On the other hand, withdrawal and safe period methods perceived to be reliable by 16.9 per cent and 17.8 per cent respectively. In case of rural and urban distribution, there was a wide gap of about 16 per cent between rural and urban folk for Cu-T. 84.3 per cent urban and 68.4 per cent rural respondents expressed about its reliability. Similarly, for the method of Tubectomy 92.2 urban and 81.6 per cent rural respondents realize its reliability, there was a narrow gap for the method of oral pills, withdrawal and condom as compare to other methods on the viewpoint of ‘reliability’. The findings of the table indicates, further scope for awareness campaigns and advocacy, good quality reproductive health services and sensitive counseling and clarifications of doubts or misconceptions at the grassroots level to the target group of family planning methods.
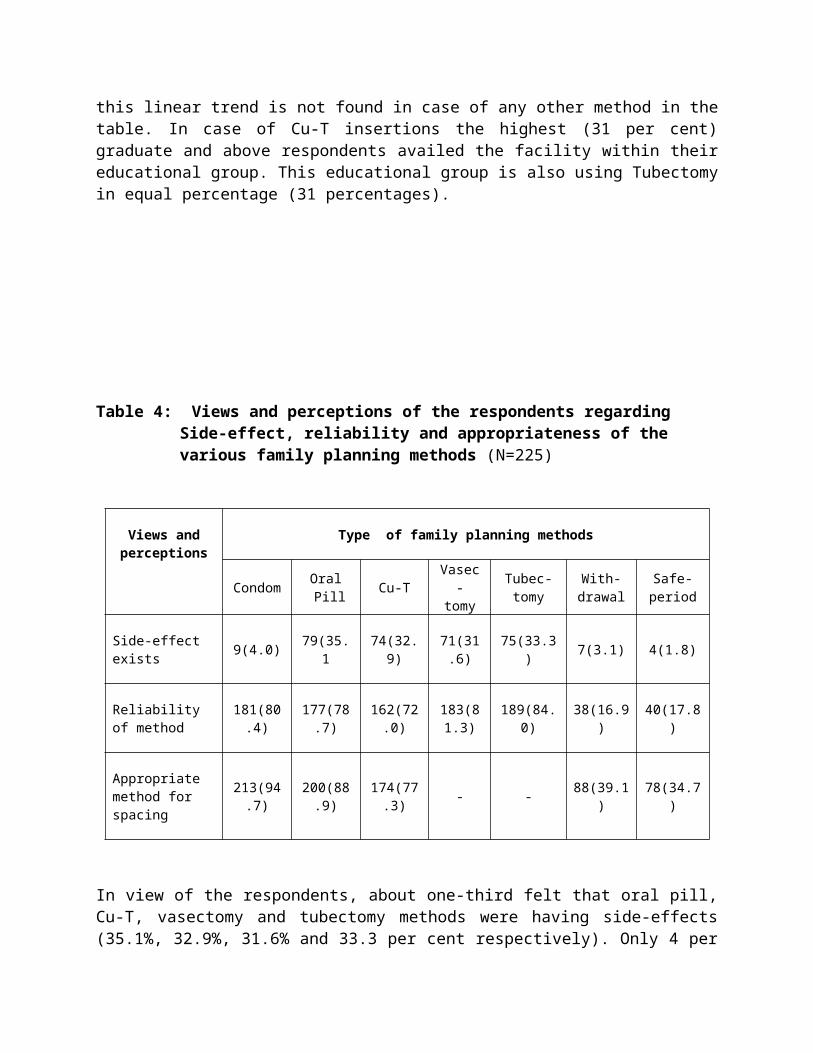
Table 7: Perception regarding appropriateness of various family planning methods for spacing according to residence of the respondents
(N=225)
Family planning Methods
Perception regarding appropriateness
Locality Total
Rural Urban
Condom
Not appropriate Within type of locality
9(75.0){5.2}
3(25.0){5.9}
12(100){5.3)
Appropriate Within type of locality
165(77.5){94.8}
48(22.5){94.1}
213(100){94.7}
Oral Pills
Not appropriate Within type of locality
18(72.0){10.3}
7(28.0){13.7}
25(100){11.1}
Appropriate Within type of locality
156(78.0){89.7}
44(22.0){86.3}
200)100){88.9}
Cu-T
Not appropriate Within type of locality
41(80.4){23.6}
10(19.6){19.6}
51(100){22.7}
Appropriate Within type of locality
133(76.4){76.4}
41(23.6){80.4}
174(100){77.3}
Withdrawal
Not appropriate Within type of locality
115(83.9){66.1}
22(16.1){43.1}
137(100){60.9}
Appropriate Within type of locality
59(67.0){33.9}
29(33.0){56.9}
88(100){39.1}
Safe period
Not appropriate Within type of locality
119(81){68.4}
28(19.0){54.9}
147(100){65.3}
Appropriate Within type of locality
55(70.5){31.6}
23(29.5){45.1}
78(100){34.7}
Total 174(77.3) 51(22.7) 225(100)
Based on locality (rural and urban residence) of respondents, perception regarding appropriateness of various family planning methods, the above Table indicates that a large number of respondents within the rural residents, 94.8 per cent for condom, 89.7 per cent for oral pills, and 76.4 per cent for Cu-T, perceived these methods were appropriate. But in case of withdrawal and safe period this percentage was 33.9 and 31.6 respectively.
If we compare with rural and urban set-up, in case of Cu-T, withdrawal and safe period the urban respondents were found more advance for its appropriateness. But this is not true in case of condom and oral pills as spacing method, either rural were keeping equal or little high perception for appropriateness.

Table 8: Perception regarding side-effects of various family planning methods for spacing according to their current age
(N=225)
Family planning methods
Views regarding Side-effect of the methods
Current ageTotal Below 30 31-40 41+
CondomNo side-effects
Within the current age60(27.8){90.0}
92(42.6){96.8}
64(29.6){100}
216(100){96.0}
Side-effect existsWithin the current age
6(66.7){9.1}
3(33.3){3.2}
- 9(100){4.0}
Oral PillsNo side-effects
Within the current age45(30.8){68.2}
60(41.1){63.2}
41(28.1){64.1}
146(100){64.9}
Side-effect existsWithin the current age
21(26.6){31.8}
35(44.3){36.8}
23(29.1){35.9}
79(100){35.1}
Cu-TNo side-effects
Within the current age48(31.8){72.7}
58(38.4){61.1}
45(29.8){70.3}
151(100){67.1}
Side-effect existsWithin the current age
18(24.3){27.3}
37(50.0){38.9}
19(25.7){29.7}
74(100){32.9}
VasectomyNo side-effects
Within the current age49(31.8){74.2}
63(40.9){66.3}
42(27.3){65.6}
154(100){68.4}
Side-effect existsWithin the current age
17(23.9){25.8}
32(45.1){33.7}
22(31.0){34.4}
71(100){31.6}
TubectomyNo side-effects
Within the current age49(32.7){74.2}
61(40.7){64.2}
40(26.7){62.5}
150(100){66.7}
Side-effect existsWithin the current age
17(22.7){25.8}
34(45.3){35.8}
24(32.0){37.5}
75(100){33.3}
Withdrawal No side-effects
Within the current age63(28.9){95.5}
91(41.7){95.8}
64(29.4){100}
218(100){96.9}
Side-effect existsWithin the current age
3(42.9){4.5}
4(57.1){4.2}
- 7(100){3.1}
Safe periodNo side-effects
Within the current age64(29.0){97.0}
93(42.1){97.9}
64(29.0){100}
221(100){98.2}
Side-effect existsWithin the current age
2(50.0){3.0}
2(50.0){2.1}
- 4(100){1.8}
Total Within the current age
66(100){29.9}
95(100){42.2}
64(100){28.4}
225{100}
The above table describes the views regarding side-effects of the contraception method according to distribution of current age of the respondents. It was noted that regardless of age groups, 96 per cent respondent for condom, 68.4 per cent for vasectomy, 67.1 per cent for Cu-T, 66.7 per cent for tubectomy and 64.9 per cent respondents for oral pills, highlighted that these methods were not having any side-effects. As compared to other two age groups, below 30 years of age group viewed that condom (9.1 per cent), withdrawal (4.5 per cent) and safe period (3 per cent) perceive ‘side-effects exists’. Similarly the age group of 31 to 40 was found highest (36.8 per cent, for oral pills and 38.9 per cent for Cu-T) towards existence of side-effects. On the other side the age group above 41 years were found towering as compare to other counterparts (34.4 per cent for vasectomy and 37.5 per cent for tubectomy method) for the same concurrence. It is, therefore, conclude that the percentage within the age groups varied from method to method, the distributions of percentage were almost constant or having narrow gaps between the classified groups.

Major Recommendations:
Family counseling systems has to be introduced to remove misconceptions and to increase inter-spousal understanding regarding use of contraceptives; as the major barriers while adopting vasectomy was ‘wives didn’t allow for vasectomy.
Based on findings, a comprehensive interventional package with the help of various stakeholders has to be introduced at village level. Regular monitoring and evaluation should also be ascertained.
Networking with other organisations like NGO, self-help group, schoolteacher, PRIs and ISM personnel must be strengthened for promotion of male contraceptives.
Vasectomy adopter’s forum should be established in each village/locality for advocacy/promotion/removing misconception about vasectomy. Adopters must be provide an opportunity to become a member of village health committees.
Knowledge about performance of NSV must be imparted to the health worker/officials through exclusive IPC training, so they can percolate to their clients.
Merits and surgical procedure of NSV should be shown in electronic media especially on television (live telecast) for better understanding and doctors who are conducting NSV, should be provided enough opportunity to interact with community.
Action/operational research including interventional activities must be initiated through local self-government and PRIs for strengthening male contraception.
Insurance for vasectomy adopters should be introduced, as misconceptions related to vasectomy and status of male perceive as a prime earner.

References
1. DELBANCO, T.L. and DALEY, I. Trough the patient’s eyes: Strategies toward more successful contraception. Obstetrics and Gynecology 88(3 Suppl.): S41-47.Sep.1996.
2. DIXON-MULLER,R. Population policy and women’s rights: Transforming reproductive choice. Westport, Connecticut, Praeger, 1993. 300p.
3. ENTWISLE, B., RINDFUSS, R.R., GUILKEY, D.K., CHAMRATRITHIRONG, A., CURRAN, S.R., and SAWANGDEE. Y. Community and contraceptive choice in rural Thailand: A case study of Nang Rong. Demography 33(1) 1-11, Feb.1996.
4. Family Planning: A Global Handbook for providers: A WHO Family Planning cornerstone, Department of Reproductive Health and Research: Johns Hopkins Bloomberg School of Public Health Center for Communication Programs INFO Project, 2008.
5. JEJEEBHOY, S.I. The importance of social science research in protecting adolescents’ sexual and reproductive choice. Medicine and Law.18(2-3):255-275.
6. KAKAR V.N. Communication in Family Planning; India’s Experience; National Institute of Health and Family Welfare, Munirka, New Delhi. 1987.
7. KIM, Y.M., KOLS. A., and MUCHEKE, S. Informed choice and decision-making in family planning counselling in Kenya. International Family Planning Perspectives 24(1):4-11, 42. Mar.1998.
8. SHEPARD, B. Feminist ethical perspectives in the international family planning field. Presented at the 116th Annual Meeting of the American Public Health Association, Boston, Nov.13-17, 1988. 10p. (Unpublished)
9. STASH, S. Reasons for unmet need in Nepal: An attempt to pick up where fertility surveys leave off. Ann Arbor, Michigan, University of Michigan, Population Studies Center, 1995. 44p. (Unpublished)
10. UNITED NATIONS, Programme of Action of the International Conference on Population and Development, Cairo, UN, 1995, 115p.
11. BOSVELD, W. Explaining between-country variation in fertility: The theoretical link between individual behaviour and social context. Amsterdam, Postdoctorale Onderzoekersopleiding Demografie, Aug.1998. (Nethur-Demography Paper No.41)17p.

Authors:
Dr. Yade Lal Tekhre, Former Professor, Department of Social Sciences, National Institute of Health and Family Welfare, Munirka, New Delhi-110 067, India email: [email protected]
Dr. Alka Sharma, Professor and Head, Department of Sociology and Coordinator, Women’s Development and Research Centre, Banasthali Vidhyapeeth, Rajasthan-304022 Email: [email protected] and [email protected]



















