
Pap maneg
25
Management Of Abnormal Pap Test, When To Refer For Colposcopy Ahmed Mousa MBBS, M.Sc, FRCSC, FACOG Assistance Professor and Consultant of Gynecology Oncology King Abdulaziz University
-
Upload
basalama-ali -
Category
Education
-
view
147 -
download
0
Transcript of Pap maneg
Management Of Abnormal Pap Test, When To Refer For
ColposcopyAhmed Mousa MBBS, M.Sc, FRCSC, FACOG
Assistance Professor and Consultant of Gynecology Oncology
King Abdulaziz University

∗ The importance of cervical cancer screening ∗ The modality of screening∗ The advantages and the disadvantages of each
modality.∗ The interpretation of cytological abnormalities.∗ The management of of abnormal result.
Objectives
∗ Is the fourth most common cancer affecting women worldwide
∗ 528,000 cases estimated in 2012∗ 85% occur in developing countries
∗ 266,000 estimated death from cervical cancer ∗ account for 7.5% of all female cancer related death ∗ 87% of cervical cancer death occur in developing
countries.
GLOBOCAN 2012 (IARC)
Cervical Cancer
∗ Human Papillomavirus is the etiological risk factor ∗ Is the most common sexually transmitted disease with a
79% estimated life time risk of cervical infection. (CDC Fact sheet 2013)
∗ HPV DNA detected in 99.7% cervical carcinoma. (Walboomers, J.M., et al.)
Cervical Cancer Etiology
∗ HPV are classified based on their oncogenic characteristics into ∗ High risk type (oncogenic)
∗ HVP 16 & 18 account for 73% of cervical cancer cases.∗ HPV 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68 account
for the remaining cases
∗ Low risk type
Cervical Cancer Etiology

Woodman et al. Nature Reviews Cancer 7, 11–22 (January 2007) | doi:10.1038/nrc2050
HPV-mediated progression of cervical cancer
10 -13years 90% clear the infection within 2 years
∗ Pap test∗ Conventional ∗ Liquid based cytology
∗ HPV∗ Primary ∗ Reflex ∗ Co-testing
Screening for cervical cancer
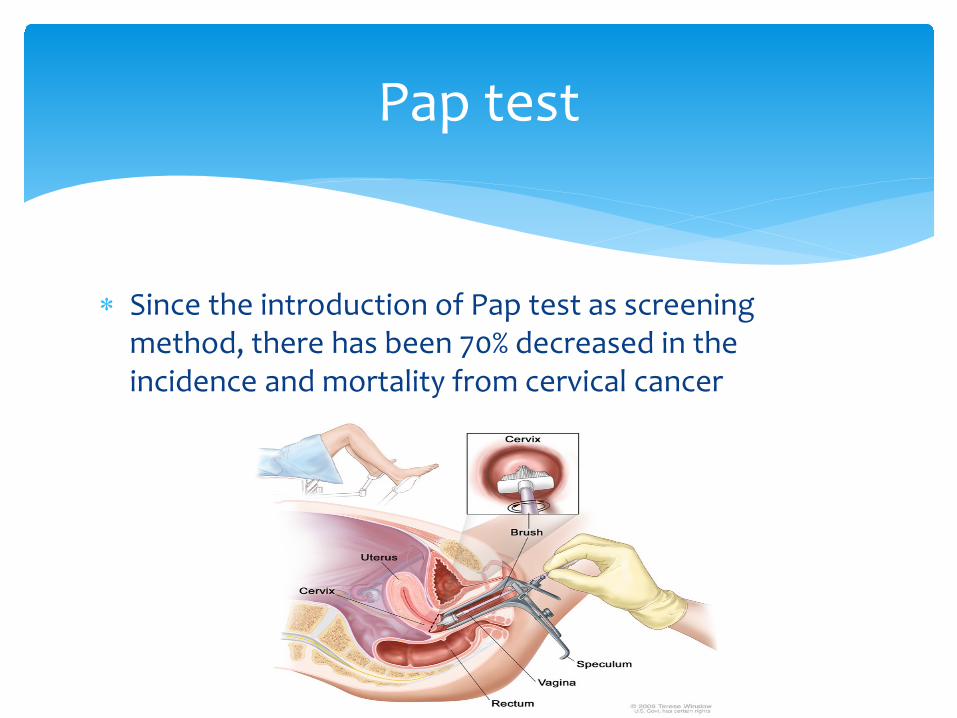
∗ Since the introduction of Pap test as screening method, there has been 70% decreased in the incidence and mortality from cervical cancer
Pap test
∗ Conventional vs liquid based cytology ∗ Both have similar sensitivity and specificity for detection
high grade and low grade intraepithelial lesion ∗ conventional pap smear is more specific than LBC for
ASCUS∗ LBC reduces unsatisfactory pap test in subgroup of
patients with obscured blood and inflammatory cells.∗ LBC cytology offer the advantage of performing HPV
test
Pap test
Whitlock EP et al, Arbyn M et al, Davey E et all
∗ Overall the sensitivity of Pap test range between 50-70%
∗ Reasons for failure ∗ Failure to screen∗ Failure to detect abnormality in the first Pap test ∗ Failure to follow up abnormal Pap test
Pap test
Leyden et all, 2005
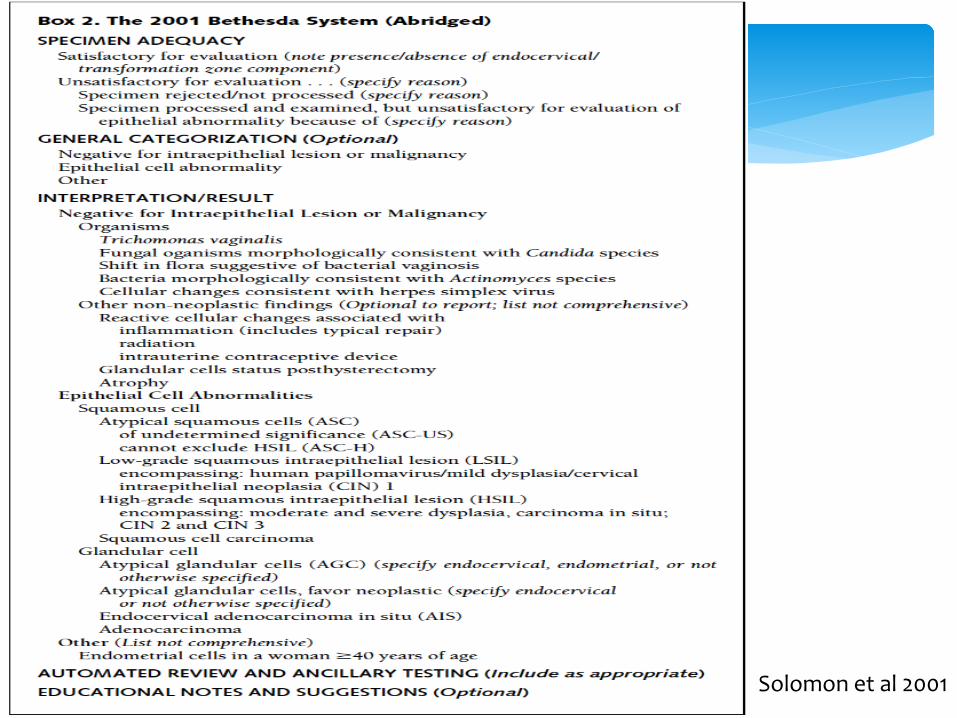
Solomon et al 2001
∗ hrHPV vs Pap test∗ Primary hrHPV or in combination with cytology is more
sensitive than pap test in the detection of HSIL and cancer.
∗ Use of hrHPV alone or in combination with cytology reduce the incidence of HSIL (RR:0.34 for primary and RR: 0.30 for cotetsting) and invasive cervical cancer (RR:0.44) compared to Pap test.
∗ Improved detection of ADK
HPV
∗ Role of genotyping ∗ HVP 16 and 18
∗ Cumulative incidence of HSIL over 3 years 21-26%
∗ Other types ∗ Cumulative incidence of HSIL over 3 years 5-6.5 %
HPV
∗ <21 ∗ No screening
∗ 21-29∗ Cytology alone every 3 years
∗ 30-65∗ HPV co-testing every 5 years ∗ Or cytology every 3 years
∗ >65∗ No screening unless
∗ Inadequate screening ∗ History of CIN 2/3, cervical ca
∗ Following Hysterectomy ∗ No screening following benign disease ∗ Screen if history of CIN 2/3, cervical cancer
Screening Per ASCCP 2012

Recently updated guideline for cervical cancer
Warner K. Huh , Kevin A. Ault , David Chelmow , Diane D. Davey , Robert A. Goulart , Francisco A.R. Garcia , Walte...
Use of primary high-risk human papillomavirus testing for cervical cancer screening: Interim clinical guidance
Gynecologic Oncology, Volume 136, Issue 2, 2015, 178 - 182
http://dx.doi.org/10.1016/j.ygyno.2014.12.022
∗ Defined as∗ Scanty cellularity ∗ Obscured by blood or inflammatory cells ∗ Or could not be processed for any reasons
Pap test should be repeated in 2-4 months∗ OR
∗ HPV negative repeat pap or HPV in 3 years ∗ HPV positive
∗ Colposcopy ∗ Or genotyping
∗ HPV 16/18 colpo∗ Other types
∗ Pap test ∗ Abnormal colop∗ Normal routine screen
Unsatisfactory

∗ HPV status ∗ Unknown
∗ Offer HPV test
∗ Positive ∗ Cytology and HPV at 1 year
∗ Negative routine screening
NILM but absent EC/TZ

∗ The most common abnormality (2.8%) ∗ Risk
∗ 7 % underlying CIN II∗ 3% underlying CIN III∗ 0.1% underlying invasive cancer
∗ 25% associated with HPV∗ HPV +
∗ 18% underlying CIN II∗ 7% underlying CIN III∗ 0.4% underlying invasive cancer
∗ HPV –∗ 1.5% underlying HSIL
∗ Options ∗ Repeat Pap test in one year
∗ ASCUS or more colpo∗ Normal routine screen
∗ Preform HPV (Reflex test)∗ Positive colpo∗ Negative routine screen
ASCUS
∗ Incidence 0.17%∗ Risk ∗ CIN II: 35%∗ CIN III: 18%∗ Invasive cancer: 2.6 %
∗ Patient must be referred to colposcopy ∗ Do not perform HPV ( 67% of patients are positive)
ASC-H
∗ Incidence 1 %∗ Risk
∗ CIN II:16%∗ CIN III: 5.2%∗ Invasive cancer :0.16%
∗ HPV + in 88%∗ HPV +
∗ CIN II: 19%∗ CIN III: 6%
∗ HPV negative∗ CIN II: 5%∗ CIN III : 2%
∗ Two options ∗ Colposcopy ∗ HPV
∗ Positive colposcopy ∗ Negative
∗ Repeat both test in one year ∗ If any abnormal colposcopy ∗ Normal routine screening
LSIL
∗ Incidence 0.21%∗ Risk ∗ CIN II: 70% ∗ CIN III: 47% ∗ Invasive cancer: 7%
∗ HPV positivity: 75%∗ Even those with negative test the risk of CIN II/III
>30% and invasive cancer 6% ∗ Refer to colposcopy
HSIL
∗ Incidence 0.1-2%∗ AGC
∗ Endocervical∗ Endometrial ∗ NOS
∗ 10% endometrial ca∗ AGC-favor neoplasia
∗ Endocervical∗ ADK 5%∗ AIS 2.5
∗ Endometrial ∗ Endometrial ca: 27% ∗ CAH: 22%
∗ NOS∗ AIS∗ Adenocarcinoma
∗ Finding is benign in 60-70%∗ Approximately 50% associated with squamous abnormality
AGC
∗ AGC-endometrial ∗ Perform endometrial biopsy and ECC∗ If negative refer to colposcopy
∗ AGC- other category∗ Colposcopy ∗ ECC∗ And endometrial biopsy if age > 35 and at risk of endometrial
ca∗ AIS
∗ Colposcopy ∗ If no lesion identified cold knife biopsy
AGC
Thank you


















