
PANDEMIC INFLUENZA: FOCUS ON LOCAL PREPAREDNESS
74
PANDEMIC INFLUENZA: FOCUS ON LOCAL PREPAREDNESS David J. Weber, MD, MPH Professor of Medicine, Pediatrics, and Epidemiology Associate Chief of Staff Medical Director, Hospital Epidemiology and Occupational Health University of North Carolina at Chapel Hill
-
Upload
helen-powers -
Category
Documents
-
view
21 -
download
1
description
PANDEMIC INFLUENZA: FOCUS ON LOCAL PREPAREDNESS. David J. Weber, MD, MPH Professor of Medicine, Pediatrics, and Epidemiology Associate Chief of Staff Medical Director, Hospital Epidemiology and Occupational Health University of North Carolina at Chapel Hill. Structure of the Influenza Virus. - PowerPoint PPT Presentation
Transcript of PANDEMIC INFLUENZA: FOCUS ON LOCAL PREPAREDNESS

PANDEMIC INFLUENZA:FOCUS ON LOCAL PREPAREDNESS
David J. Weber, MD, MPHProfessor of Medicine, Pediatrics, and Epidemiology
Associate Chief of StaffMedical Director, Hospital Epidemiology and Occupational Health
University of North Carolina at Chapel Hill

Structure of the Influenza Virus
Polymerase (P) Proteins
Hemagglutinin (HA)16 types in influenza A
Neuraminidase (NA)9 types in influenza A
M2M2
Nucleoprotein (NP)ssRNA–highly mutable
8 segments-allowsreassortment during
double infection
M1M1
Adapted from: Hayden FG et al. Clin Virol. 1997:911-42.

INFLUENZA: BIOLOGY & IMPACT
Single-stranded, enveloped, RNA virus (orthomyxoviridae): Causes respiratory tract disease (pneumonia) Sudden onset More severe pneumonia during pregnancy No carrier state but inapparent disease may occur
Influenza A Potentially severe illness; epidemic and pandemics Rapidly changing Hemagluttinin (HA) 16 types; neuraminidase (NA) 9 types
Influenza B Usually less severe illness; may cause epidemics More uniform
Influenza C Usually mild or asymptomatic illness

ENVIRONMENTAL SURVIVALOF INFLUENZA A
0%
20%
40%
60%
80%
100%
0 10 20 30 40 50 60
Minutes
Survival on hands Survival on surfaces
Efficacy of antisepticsAlcohol 60% gel, >99.99% reduction in 20 secEthanol 75%, >99.99% reduction in 20 sec Sattar SA, Tetro JA., 2006

Deaths25,000 - 72,000
Hospitalizations114,000 - 257,500
Infections and illnesses50 - 60 million
Physician visits~ 25 million
Thompson WW et al. JAMA. 2003;289:179-86. Couch RB. Ann Intern Med. 2000;133:992-8. Patriarca PA. JAMA. 1999;282:75-7. ACIP. MMWR. 2004;53(RR06):1-40.
Influenza Disease Burden to U.S. Societyin an Average Year
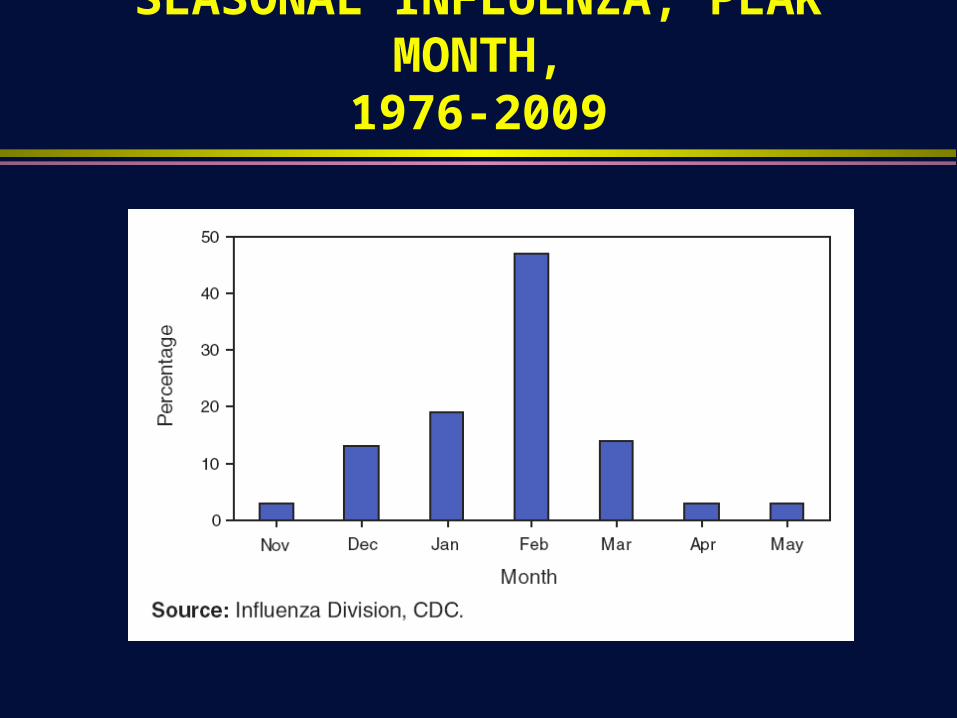
SEASONAL INFLUENZA, PEAK MONTH,1976-2009

Antigenic Drift

Antigenic Shift

Hampson AW, Mackenzie JS. MJA 2006;185:S39-43

De Clercq E. Nature Rev 2006;5:1015-25

INFLUENA PANDEMICS IN THE 20th CENTURY
Years VirusUS Mortality Greatest Risk
Spread from Asia to US
1918-1919“Spanish”
Type A H1N1
500,000 Young, healthy adults
Unknown
1957-58“Asian”
Type A H2N2
70,000 Infants, elderly
4-5 mo
1968-69“Hong Kong”
Type A H3N2
34,000 Infants, elderly
2-3 mo
HHS Pandemic Influenza Plan, October 2005


C DCC EN TE RS FOR D ISE A S E C ON TRO L
A ND P RE V EN TION
U .S. L ife Expectancy 1900-1960
30
1900 1905 1910 1915 1920 1925 1930
Year
Lif
e E
xpec
tan
cy
1935 1940 1945 1950 1955 1960
38
46
54
62
70

NY Times, 30 April 2009

INFLUENZA AND PNUEMONIA MORTALITY, US, 1911-17 VS 1918

PANDEMIC INFLUENZA PLANNING CHALLENGES
Pandemic strain unknown The ability of the virus to rapidly spread worldwide Simultaneous outbreaks throughout the US, limiting the ability of any
jurisdiction to provide assistance to other areas People may be asymptomatic while infectious Long duration (>2 years) and multiple waves Enormous demands on the healthcare system
Need for surge capacity: Medications, ventilators, beds, personnel Personnel: Exhaustion, concerns about infection
Maintaining social distancing Providing adequate antivirals including distribution/allocation Vaccine development and distribution/allocation

PANDEMIC INFLUENZA PLANNING ASSUMPTIONS
Most likely pandemic strain H5N1 (ongoing epidemic since 1999) Pandemic likely to start in Asia and then spread to US
Mitigation strategies will limit epidemic: Social distancing, antivirals, vaccines
Pandemic will be characterized by distinctive waves Susceptibility to the pandemic influenza virus will be universal
Highest infection rate among school-aged children (~40%) Highest morbidity and mortality among the elderly
Asymptomatic persons may transmit infection Antivirals likely in to be in short supply Vaccine will be not be available for >6 months Number of hospitalizations and deaths will depend on virulence

Stochasic model - Germann TC, et al. PNAS 206;103:5935-5940

MODELING AN INFLUENZA PANDEMIC:CONCLUSIONS
Social distancing (travel restrictions, closing schools) Travel restrictions with >99% efficacy required to increase time
between exports to the order of weeks Delays epidemic and decreases peak Limited effect on total number ill, hospitalized, or dead
Antivirals Likely to decrease total number infected Requires early therapy or long-term prophylaxis for efficacy Adequate stockpile and distribution key
Vaccines Must be available early in epidemic Most effective if provided to children with leftover vaccine going to
middle aged adults

PANDEMIC INFLUENZA PLANNING ASSUMPTIONS
Most likely pandemic strain H5N1 (ongoing epidemic since 1999) (-) Pandemic likely to start in Asia and then spread to US (-)
Mitigation strategies will limited epidemic: Social distancing, antivirals, vaccines (-)
Pandemic will be characterized by distinctive waves (-) Susceptibility to the pandemic influenza virus will be universal
Highest infection rate among school-aged children (~40%) (-) Highest morbidity and mortality among the elderly (-)
Asymptomatic persons may transmit infection (+) Antivirals likely in to be in short supply (-) Vaccine will be not be available for >6 months (+) Pandemic influenza strain likely have increased virulence (-)

WHO INFLUENZA PANDEMIC ALERT,11 JUNE 2009 (alert raised to phase 6)

ESTIMATES OF NOVEL H1N1 IMPACT
Seasonal Influenza Novel Influenza
Attack Rate 10-20% 30-50%
Symptomatic 50-60 million 60-120 million
Hospitalizations 114,000 – 257,000 Up to 1.8 million
ICU care Up to 300,000
Deaths 25,000 – 72,000 30,000 to 90,000
President’s Council of Advisors on Science and Technology, 7 Aug 2009

NOVEL INFLUENZA H1N1, 2009CURRENT EPIDEMIOLOGY
Unique strain: Includes genetic components of human, avian, and swine origin
Worldwide outbreak Efficient human-to-human transmission documented Susceptible to antivirals (oseltamivir and zanamivir) but oseltamivir
resistance described Median age, US = 12 (highest infection incidence, 5-24 years) Older individuals may have cross-reacting antibodies (i.e., partial
protection) Risk factors:
Obesity (BMI >30) and morbid obesity (BMI >40) a newly described risk for severe illness
Pregnant women: Death rate 4-6x higher than general public

Gather D. J Clin Virol 2009;45:174-178

Emergence of Quadruple-Reassortant H1N1/09
Garten et al., Science, 2009; 325:198

IMPACT OF NOVEL H1N1
Worldwide (WHO, 8 January) 12,799 confirmed deaths; 208 countries/territories reported activity
US (CDC, April to 14 November) 47 (range, 34-67) million cases 213,000 (range, 154,000-303,000) hospitalizations 9,820 (range, 7,070-13,930) deaths
North Carolina (NC Health Dept., 13 October) 81 deaths {since April 2009}
UNC Hospitals (Hospital Epipidemiology, 4 January) 115 hospitalizations, 5 deaths

H1N1 EPIDEMIOLOGY, US
Hospitalization rate (US, 15 April to 24 July, 2009) Cases: 43,771 Hospitalizations: 5,011 (11.4%) Deaths: 302 (0.69%)
Secondary attack rate Acute respiratory illness: 18% to 19%
Definition: >2; fever, cough, sore throat, rhinorrhea Influenza-like illness: 8% to 12%
Definition: Fever plus cough or sore throat Generation time
Acute respiratory illness: 2.0-3.1 days Influenza-like illness: 2.4-3.1 days

International EpidemiologyInternational Co-circulation of 2009 H1N1 and Seasonal
Influenza(As of 4 January 2010)

NOVEL H1N1,OUTBREAK CURVE, MEXICO,11 MARCH – 29 MAY
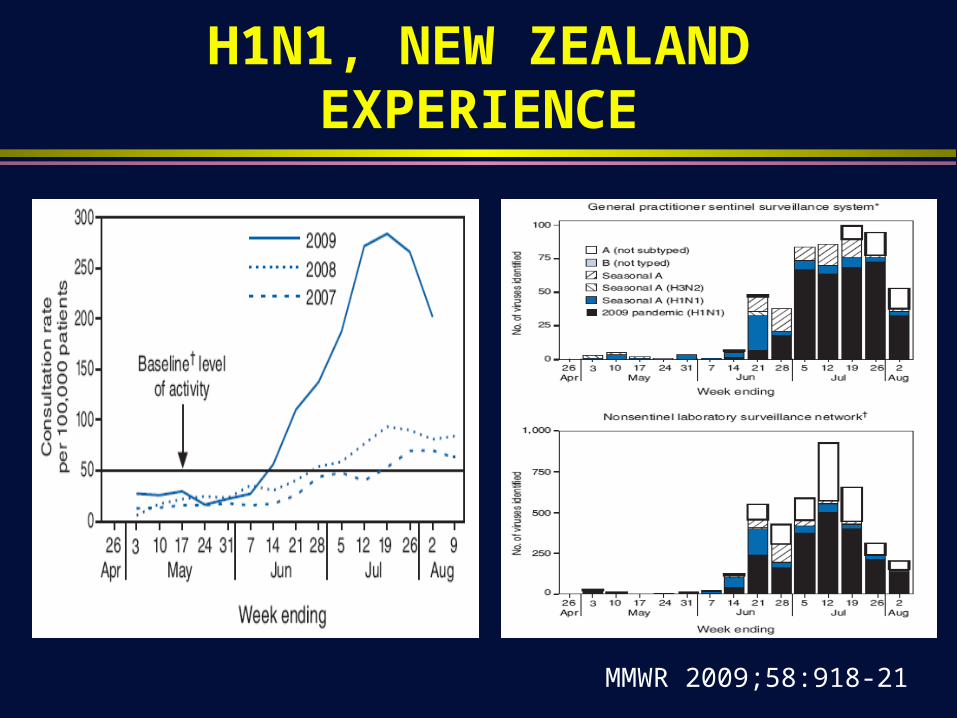
H1N1, NEW ZEALAND EXPERIENCE
MMWR 2009;58:918-21


ILI REPORTED BY US OUTPATIENT ILINet

INFLUENZA ACTIVITY, US, BY VIRAL TYPE

H1N1 SURVEILLANCE, CDC,30 AUGUST TO 2 JANUARY

H1N1 SURVEILLANCE, UNC
H1N1 Outcomes Count
Hospitalizations 115
Deaths 5

NOVEL INFLUENZA H1N1, 2009:SYMPTOMS
Cough 98% Subject fever 96% Fatigue 89% Headache 82% Nausea 55% Stomach ache 50% Diarrhea 48% Shortness of breath 48% Joint pain 46%
Max temperature 39.0 oC (102.2 oF)
Temperature range 37.2-40.0 39.0 oC (99.0-104.0 oF)
95% reported subjective fever PLUS cough or sore throat
MMWR. NYC. 2009;58(dispatch;1-3

H1N1 CASES RATE, US,BY AGE GROUP
15 April to 24 July, CDC

WARNING SIGNS FOR WHEN A PERSON SHOULD SEEK MEDICAL CARE
Children Fast breathing or trouble
breathing Bluish or gray skin color Not drinking enough fluids Severe or persistent vomiting Not waking up or not interacting Being so irritable that the child
does not want to be held Flu-like symptoms that improve
but then return with fever and worse cough
Adults Difficulty breathing or shortness
of breath Pain or pressure in the chest or
abdomen Sudden dizziness Confusion Severe or persistent vomiting Flu-like symptoms that improve
but then return with fever and worse cough

PERSONS AT HIGH RISK OF COMPLICATIONS FROM H1N1 INFLUENZA
Age < 2 years Age >65 years Pregnant women Immunosuppression: HIV infection, chemotherapy Persons with metabolic disorders: Diabetes, chronic renal failure, chronic
liver failure, sickle cell anemia Persons with cardiovascular disorders: Congestive heart failure (not
hypertension) Persons with compromised respiratory function: Cognitive dysfunction,
spinal cord injuries, seizure disorders, other neuromuscular disorders Persons with respiratory disorders: Asthma

Acute Febrile Respiratory Illness of <7 days Duration With Fever AND >1 Of The Following● Cough
● Sore throat
Vomiting and diarrhea do NOT exclude the diagnosis of influenza H1N1Fever defined as subjective fever or temperature >37.8 oC or 100 oF
Place surgical mask on patient immediatelyIsolate as soon as possible (private room if possible)
Use Droplet Precautions (surgical mask)For cough inducing procedures (bronchoscopy, intubation) use an N95 respirator
plus eye protection (face shield or goggles)
Obtain NP swab for influenza PCRAdditional clinical evaluation as indicated
Algorithm for Evaluation of UNC Health Care Patients With Possible Novel H1N1 Influenza
* Persons considered at high risk for complications: children less than 2 years old, persons aged 65 years or older, pregnant women, persons younger than 19 years of age who are receiving long-term aspirin therapy, and persons of any age with certain chronic medical or immunosuppressive conditions
(chronic pulmonary {including asthma}, cardiovascular {except hypertension}, renal, hepatic, hematological {including sickle cell disease}, metabolic disorders {including diabetes}; disorders that can compromise respiratory tract function or increase the risk of aspiration {e.g., cognitive dysfunction,
seizure disorders}; and immunosuppression {e.g., HIV}.
Influenza (H1N1) is susceptible to oseltamivir and zanamivir but resistant to amantadine/rimantadine
Only high risk persons should be considered for post-exposure prophylaxis and therapy. Early treatment is an alternative to chemoprophylaxis after a suspected exposure.
23 September 2009 Updates at http://intranet.unchealthcare.org/intranet_news/empnews/flu
YesNo
No influenza testing recommendedAdditional evaluation and follow-up
as clinically indicated
Do patient’s symptoms indicate need for hospitalization ORIs the patient in a high risk group for complications of influenza* or from an extended care facility
Yes
Hospitalizedbegin empiric therapy with oseltamivir
Use Droplet PrecautionsFor cough inducing procedures use an N95 respirator
plus eye protection (face shield or goggles)
DischargedConsider empiric therapy (zanamivir preferred) only if patient at “high
risk” for complications of influenzaAntivirals most effective if inititiated <48 after onset of symptoms
Patient should stay home until 24 hours afebrile off antipyreticsUse proper hand and respiratory hygiene
Call or seek emergency medical care, if warranted
No
DischargePatient should stay home until 24 afebrile off antipyretics
Use proper hand and respiratory hygieneCall or seek emergency medical care, if warranted
If zanamivir contra-indicated (by age or hx of asthma) use oseltamivir
Additional evaluation and follow-up as clinically indicated
Obtain influenza test only if clinically indicated

CDC2 Oct

SYMPTOMS OFHOSPITALIZED PATIENTS
Fever 93%Cough 83%
Shortness of breath 54%Fatigue/weakness 40%
Chills 37%Myalgias 36%
Rhinorrhea 36%Sore throat 31%Headache 31%Vomiting 29%Wheezing 24%Diarrhea 24%

H1N1 HOSPITALIZATION RATE(per 100,000), BY AGE GROUP

AGE GROUPS OF HOSPITALIZED PATIENTS: SEASONAL VERSUS NOVEL INFLUENZA
MMWR 2009;58(RR-10)

MMWR 2009:58;749
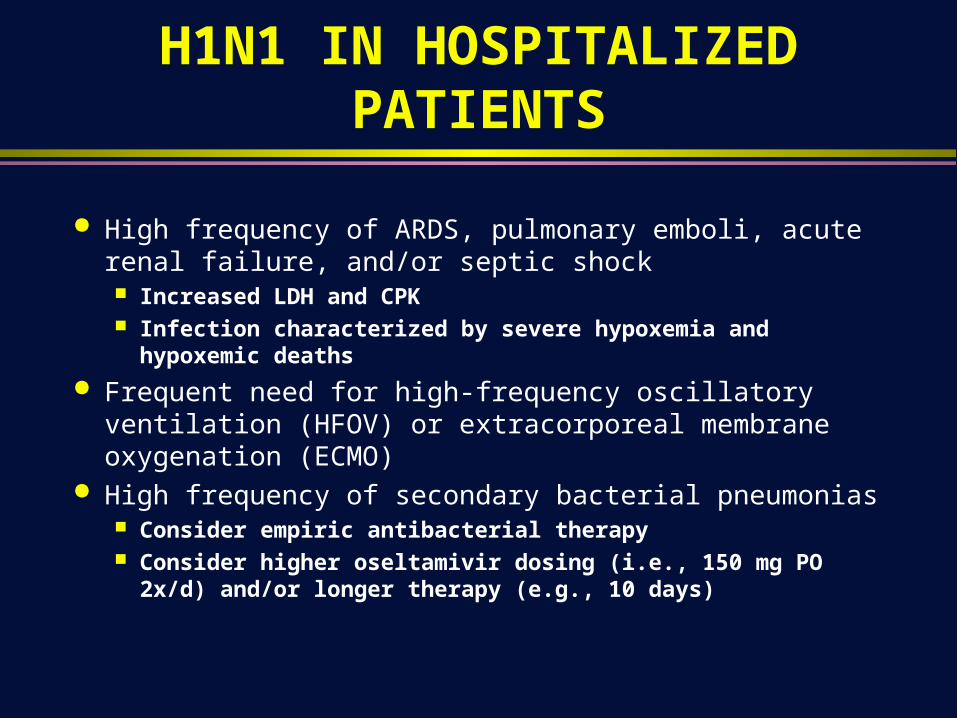
H1N1 IN HOSPITALIZED PATIENTS
High frequency of ARDS, pulmonary emboli, acute renal failure, and/or septic shock Increased LDH and CPK Infection characterized by severe hypoxemia and hypoxemic deaths
Frequent need for high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO)
High frequency of secondary bacterial pneumonias Consider empiric antibacterial therapy Consider higher oseltamivir dosing (i.e., 150 mg PO 2x/d) and/or
longer therapy (e.g., 10 days)
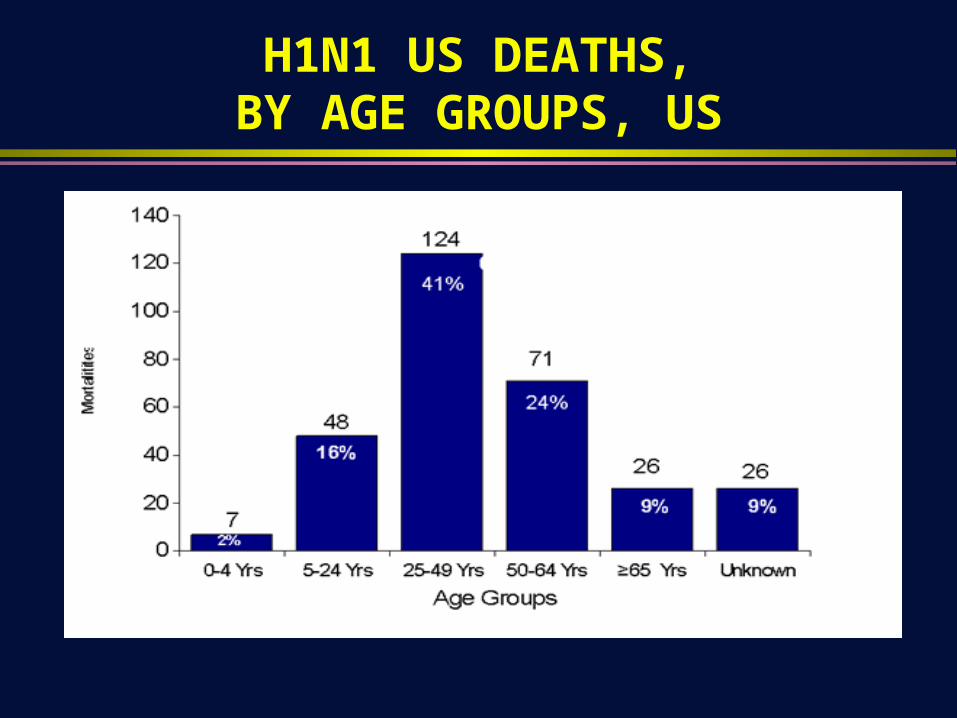
H1N1 US DEATHS,BY AGE GROUPS, US

H1N1 US ILLNESS AND DEATHS,BY AGE GROUPS, MEXICO
Chowell G, et al. NEJM 2009;361:674-9


MMWR 2009;58: 941-47

SECONDARY BACTERIAL INFECTIONSIN PATIENTS WITH H1N1
Examination of 77 H1N1 cases by autopsy
22 of the 77 cases had evidence of bacterial superinfection S. pneumoniae 10 S. pyogenes 6 S. aureus 7 H. influenzae 1 Multiple pathogens 4
MMWR 2009;58:1071

ANTIVIRAL THERAPY
Consider for possible cases of novel influenza at high risk for complications
Treatment of hospitalized patients and patients at high risk for influenza complications should be prioritized
Provide therapy as soon as possible (target <48 hours) Recommended duration is 5 days Use same doses as recommended for seasonal influenza Novel influenza
Zanamivir alone, OR Oseltamivir PLUS amantadine or rimantadine (if seasonal flu possible)


TREATMENT ANDPOST-EXPOSURE PROPHYLAXIS
Treatment (oseltamivir) PEP (oseltamivir)
Adults 75-mg capsules 2x/d x 5 days 75-mg capsule 1x/d x 10 days
Child >12 mo <15 kg 15-23 23-40 >40
30-mg 2x/d x 5 days45-mg 2x/d x 5 days60-mg 2x/d x 5 days75-mg 2x/d x 5 days
30-mg 1x/d x 5 days45-mg 1x/d x 5 days60-mg 1x/d x 5 days75-mg 1x/d x 5 days
Treatment (oseltamivir) PEP (oseltamivir)
Adults 2 5-mg inhalations (10 mg) 2x/d
2 5-mg inhalations (10 mg) 1x/d
Children 2 5-mg inhalations (10 mg) 2x/d(age >7 years)
2 5-mg inhalations (10 mg) 1x/d(age >5 years)

INFLUENZA: PROPHYLAXIS AND THERAPIES
Oseltamivir (Tamiflu)*: Influenza A & B Treatment: 75 mg PO 2x/day x 5d** Post-exposure prophylaxis: 75 mg PO 1x/day x 10 days Seasonal prophylaxis: 75 mg PO 1x/day x 4-8 weeks
Zanamivir (Relenza)*: Influenza A & B Treatment: 10 mg (2 nasal inhalations 2x/d x 5d) Post-exposure prophylaxis: 10 mg (2 nasal inhalations 1x/d x 10d) Seasonal prophylaxis: 10 gm (2 nasal inhalations 1x/day x 4-8 weeks)
Ramantidine*: Influenza A*** Treatment: 100 mg PO 2x/d (adult); 100 mg PO 1x/d (>65, elderly in ECF) Prophylaxis: 100 mg PO 2x/d (adult); 100 mg PO 1x/d (elderly in ECF)
*Should begin therapy within 2 days of onset of illness Reduce dose if creatinine clearance <30mL/min**, or <10mL/min***

ANTIVIRAL RESISTENCE
CDC data (Since 1 October 2008) Resistance in seasonal H1N1 (N=1,148)
Oseltamivir 99.6%, zanamivir 0%, adamantanes 0.5% Resistance in seasonal H3N2 (N=261)
Oseltamivir 0%, zanamivir 0%, adamantanes 100% Novel H1N1 (N=1,678)
Oseltamivir 0.6%, zanamivir 0%, adamantanes 100%
Reports of resistance 2 immunocompromised patients, Seattle (MMWR 2009;58:893) 2 linked cases (normal hosts) in NC

COMBINATION THERAPY WITH OSELTAMIVIR, AMANTADINE, AND RIBAVIRIN ON H5N1
Smee DF, et al. AAC 2009;53:2120-2128

surveillance
select strains
prepare reassortants
standardize antigen
assign potency
review/license
formulate/test/package
vaccinate
WHO/CDC)
WHO/CDC/FDA
CDC/FDA
FDA
FDA
FDA
manufacturers
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
clinic
Vaccine Development

Effective of VaccineUsing Different DeliveryStrategies
Medlock J, Galvani AP.Science 2009;325:1705

H1N1 VACCINE
Made in a similar fashion to seasonal influenza vaccine Egg based production Single dose syringes and inhaled vaccine are thimerosal free Multi-dose vials have miniscule amount of thimerosal (no human harm
demonstrated from thimerosal per IOM report) No adjuvant Risk of Guillain-Barre = 1 additional case per 1,000,000 vaccinated
Both inactivated and live-attenuated vaccines will be available Licensed by FDA 15 September 2009: CSL Limited, MedImmune LLC,
Novartis Vaccines and Diagnostic Limited, and Sanofi Pasteur Inc. Available for clinical use in early to mid-October
Requires one dose in adults, 2 doses in children: Robust immune response produced in healthy adults in 8-10 days (15ug dose 96.7%):
Vaccine provided free by Federal Government

H1N1 VACCINE: TITER >1:40
Zhu F-C, et al. NEJM 2009;361

EFFICACY OF INACTIVATED VS ATTENTUATED SEASONAL INFLUENZA VACCINE
Monto AS, et al. NEJM 2009;361:1260-7

EFFICACY OF INFLUENZA VACCINE PRODUCED MAMMALIAN CELL CULTURE
J Infect Dis 2009;200:841-8

TARGET GROUPS FOR H1N1 VACCINE
Initial Pregnant women People who live with or care for infants younger than 6 months of age Healthcare and emergency medical personnel Anyone from 6 months through 24 years of age Anyone from 25 through 64 years of age with certain chronic medical
conditions or a weakened immune system As more vaccine become available, these groups should also be
vaccinated Healthy 25 through 64 year olds Adults 65 years and older
Children through 9 years of age should get 2 doses of vaccine about a month apart
CDC. 2 October 2009

H1N1 VACCINES FOR USE IN THE US, 6 OCTOBER, 2009

FDA APPROVED 2009 H1N1 VACCINES: CONTRA-INDICATIONS & WARNINGS
Inactivated vaccines (contra-indications) Anaphylaxis to a previous dose of influenza vaccine Hypersensitivity to eggs or chicken proteins Hypersensitivity to gelatin (Sanofi), formaldehyge (Sanofi), polymyxin
(Novartis, CSL), neomycin (Novartis, CSL), nonylphenol ethoxylate (Novartis)
Inactivated vaccines (warnings) Guillain-Barre syndrome within 6 weeks of a previous dose of
influenza vaccine Immunocompromised persons may have a diminished immune
response

FDA APPROVED 2009 H1N1 VACCINES: CONTRA-INDICATIONS & WARNINGS
Live attenuated vaccine (contra-indications) Anaphylaxis to a previous dose of influenza vaccine Hypersensitivity to eggs, chicken protein, gelatin, gentamicin, or
arginine Live attenuated vaccine (warnings and precautions)
Do not administer to persons with asthma or children <5 years of age with recurrent wheezing
Guillain-Barre syndrome within 6 weeks of a previous dose of influenza vaccine
Pregnant women Immunocompromised persons Persons at high risk of complications from influenza

NOVEL INFLUENZA H1N1, 2009INFORMATION NOT AVAILABLE
Will seasonal H3N2 influenza virus disapper Number of persons who will develop disease in Fall/Winter Duration of viral shedding Modes of transmission: Droplet (presumed), airborne?, contact? Ability to develop an accurate rapid diagnostic test Efficacy of H1N1 vaccine Likelihood of antiviral resistance developing Efficacy of IV neuraminidase inhibitors Morbidity* (Hospitalization rate) Mortality*
* Current data subject to ascertainment bias

CDC GUIDELINES: CONTROVERSIES
Duration of furlough for ill healthcare workers Initially 7 days from onset of illness or afebrile x 24 hours Afebrile x 24 hours off antipyretics
Respiratory protection N95 respirator Surgical mask
Vaccine Live attenuated Inactivated

SURGICAL MASK VS N95 FOR PREVENTING INFLUENZA AMONG HCWs
Randomized clinical trials, 2008-2009 influenza season Location = Ontario tertiary care hospitals 446 nurses enrolled
Outcome = Laboratory confirmed influenza (PCR, serology)Loeb M, et al. JAMA 2009;302:E1

UNC HOSPITAL PREPAREDNESS:ISSUES
Critical issues Surge capacity Maintaining adequate
staffing Provision of essential
services/supplies
Additional issues Surveillance Diagnosis Protecting personnel Occupational health Stockpiling antiviral agents Triage of limited
supplies/beds Security

UNC HOSPITAL PREPAREDNESS:PROVIDING ESSENTIAL SERVICES
Explicit statement by University/Hospital that all employees are expected to provide service Requirement that illness be documented if unable to work
Food supplies: Ability to use UNC University supplies (>6 weeks) Water: Infrastructure to support supply via trucks Electrical: University generator
UNC Hospitals highest priority Additional capacity planned
Medical gases: 1 week supply; additional supply to be added Beds
Outpatient: Plans to use medical student training area Inpatient: Plans to use unlicensed beds (e.g., PACU, 24 hour hold
area)

UNC HOSPITAL PREPAREDNESS:SURGE CAPACITY - STAFFING
Supplementation of staff Use of allied faculty (e.g., Schools of Nursing, Public Health,
Pharmacy)(e.g., Nursing = ~20 faculty, ~200 students) Use of medical/nursing students Use of retired medical personnel and volunteers Use of UNC University staff (e.g., security, housekeeping, etc.) Assumption of malpractice costs & provision of worker’s
compensation (in case of acquisition of illness) Day care under consideration
Plan for flexible shifting of personnel to meet demand

Many many thanks to all persons who aided in development of our highly communicablerespiratory plan and have contributed to ourresponse to swine influenza


















