Pancreatitis
72
Acute Pancreatitis: Management Update Dr Tapan Shah, MS, DNB, MD;FACS, MACS SURGICAL GASTROENTEROLOGY AND HEPATOBILIARY SURGEON
-
Upload
tapan-shah -
Category
Health & Medicine
-
view
104 -
download
0
Transcript of Pancreatitis
Acute Pancreatitis: Management Update
Dr Tapan Shah, MS, DNB, MD;FACS, MACSSURGICAL GASTROENTEROLOGY AND
HEPATOBILIARY SURGEON

Overview of Acute Pancreatitis
85% of patients have interstitial pancreatitis; 15 (range 4 – 47%) have necrotizing pancreatitis
Among patients with necrotizing pancreatitis, 33% (range 16-47%) have infected necrosis
Approximately 10% of patients with interstitial pancreatitis experience organ failure, but in the majority it is transient
Mortality in acute pancreatitis overall, is approximately 5%: 3% in interstitial pancreatitis, 17% in necrotizing pancreatitis
In necrotizing pancreatitis, mortality 3-fold infected vs. sterile necrosis
Mortality increases with development of organ failure ~ 3% (0-8%) and with multi-system organ failure 47% (range 28-69)ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
Acute Pancreatitis:Concepts 2009
1) Volume replacement is the foundation of therapy
2) Establish severity Utilize initial laboratory data standardized modalities i.e. Ranson criteria require 48 hrs CT abnormalities correlate with severity No need for early CT to establish severity
3) Establish etiology Importance is to prevent recurrence
4) Biliary Pancreatitis
Utilize laboratory markers for diagnosis of retained CBD ERCP is only for treating patients with cholangitis

5) Do not use prophylactic antibiotics
6) CT guided aspiration is the diagnostic test for pancreatic infection & allows directed antibiotic therapy
Acute Pancreatitis:Concepts 2009

Acute Pancreatitis:Concepts 2009
(Cont)
7) Surgical intervention in patients with infected pancreatic necrosis but rarely in sterile necrosis
8) Early enteral feeding is safe, prevents leaky gut and is associated with less complications than TPN

Definition of Severe Acute Pancreatitis (SAP)
SAP is acute pancreatitis with local and/or systemic complications Local complications are:
necrotizing pancreatitis Infected necrosis Pancreatic abscess Peripancreatic fluid collection and pseudocystic lesions
Systemic complications are: Pulmonary and renal failure Shock Cardio-circulatory dysfunctions systemic sepsis coagulation disorder
Bradley EL, III. Arch Surg 1993;128:585-590

Acute Pancreatitis: Mechanisms of Intra and-Extrapancreatic Inflammation
Mediated by cytokines and other inflammatory mediators: Activation of inflammatory cells Chemo-attraction of activated inflammatory cells to the
microcirculation Activation of adhesion molecules allowing the binding of
inflammatory cells to the endothelium Migration of activated inflammatory cells into areas of
inflammationACG Practice Guidelines in Acute Pancreatitis.
Am J Gastroenterol 2006;101:2379-2400
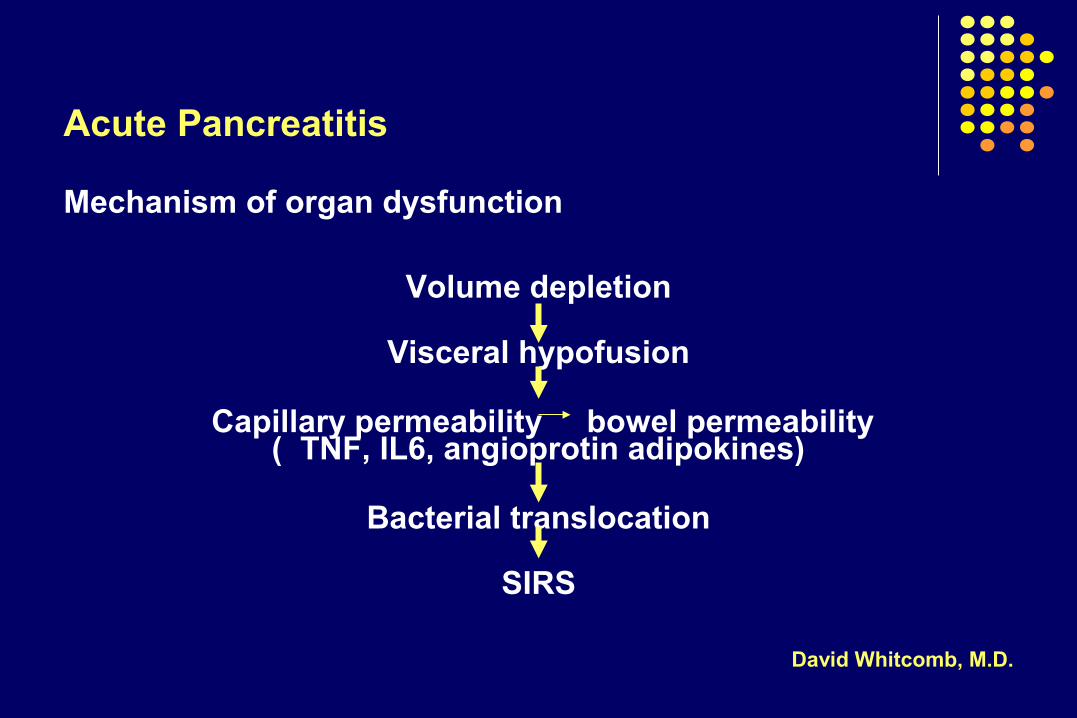
Acute Pancreatitis
Mechanism of organ dysfunction
Volume depletion
Visceral hypofusion
Capillary permeability bowel permeability( TNF, IL6, angioprotin adipokines)
Bacterial translocation
SIRS
David Whitcomb, M.D.

Causes of mortality
Acute Pancreatitis
DEATH
Early (< one week)• Systemic inflammatory
response syndrome (SIRS)
• Multiorgan failure
Late (> one week)• Multiorgan failure
• Pancreatic infections/sepsis

Systemic Inflammatory Response Syndrome (SIRS)
Defined by two or more of the following criteria:
Pulse > 90 beats/min
Respiratory rate > 20/min or PCO2 <32 mmHg
Rectal temperature <36° C or >38°C
White blood count <4,000 or >12,000/mm3
ACG Practice Guidelines in Acute Pancreatitis Am J Gastroenterol 2006;101:2379-2400
Acute Pancreatitis
Prognosis
• Bedside AssessmentUnderestimates severe disease
• Scoring SystemsRanson, Glasgow, Apache, Rabenek
• Serum MarkersTrypsinogen activation peptide (TAP)C-reactive protein (CRP)Cytokines
• Imaging criteriaFluid collections, necrosis
Prognosis in Acute Pancreatitis
Acute Pancreatitis
Early Indicators of Severity
• Tachycardia, hypotension
• Tachypnea, hypoxemia
• Hemoconcentration
• Oliguria
• Encephalopathy
Early Diagnostic Indicators in Acute Pancreatitis
Acute Pancreatitis
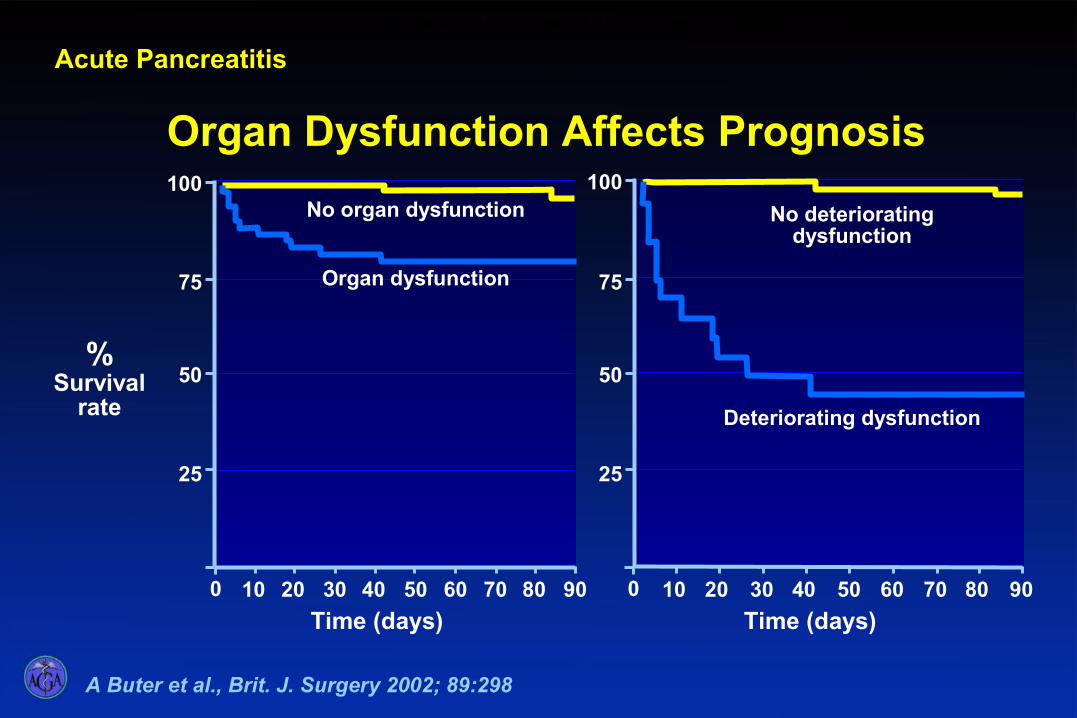
No deteriorating dysfunction
Deteriorating dysfunction
25
100
50
75
0 10 20 30 40 50 60 70 80 900
No organ dysfunction
Organ dysfunction
10 20 30 40 50 60 70 80 90
25
100
50
75
Time (days)
%Survival
rate
Time (days)
Organ Dysfunction Affects Prognosis in Acute Pancreatitis
Organ Dysfunction Affects Prognosis
A Buter et al., Brit. J. Surgery 2002; 89:298
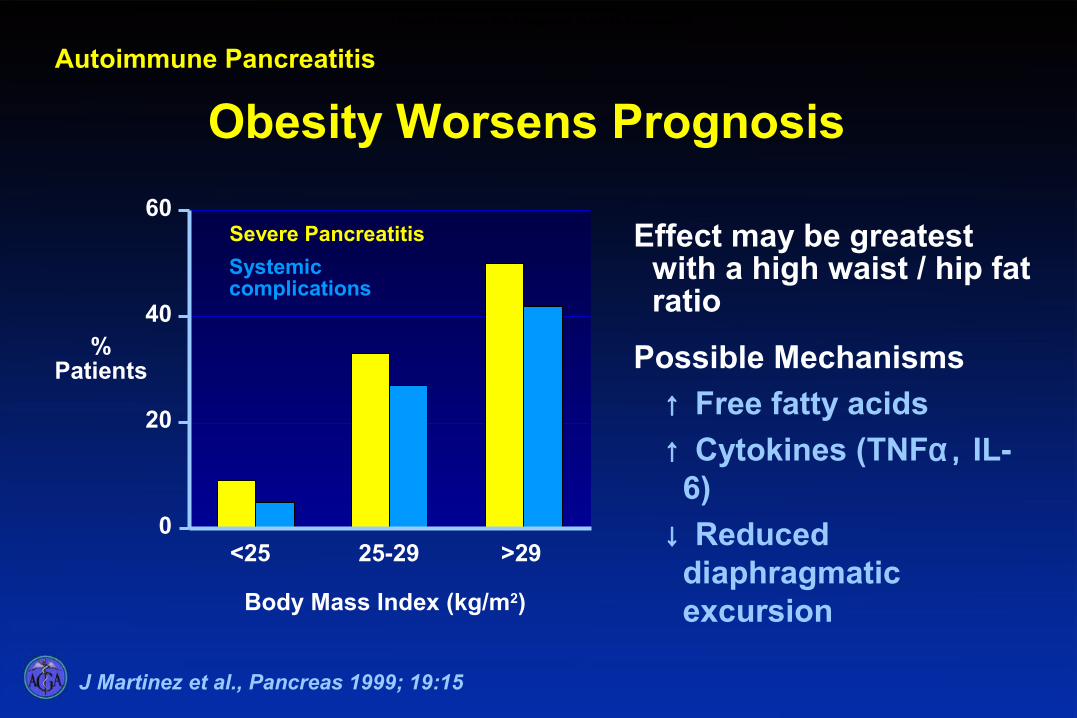
J Martinez et al., Pancreas 1999; 19:15
Effect may be greatest with a high waist / hip fat ratio
Possible Mechanisms
↑ Free fatty acids
↑ Cytokines (TNFα, IL-6)
↓ Reduced diaphragmatic excursionBody Mass Index (kg/m2)
%Patients
0
20
40
60
<25 25-29 >29
Severe Pancreatitis
Systemic complications
Obesity Worsens Prognosis
Autoimmune Pancreatitis
Obesity Worsens the Prognosis in Acute Pancreatitis

Diagnostic Guideline I: Look for Risk Factors of Severity at Admission
Older age (>55 yrs) Obesity – BMI > 30 Organ failure at admission Pleural effusion and/or infiltrates When organ failure is corrected within 48 hours,
mortality is close to 0 When organ failure persists for more than 48 h,
mortality is 36%Level of Evidence III
ACG Practice Guidelines in Acute Pancreatitis Am J Gastroenterol 2006;101:2379-2400

APACHE II score = (acute physiology score)
1. Rectal temperature (°C)2. Mean arterial pressure (mmHg)3. Heart rate (bpm)4. Respiratory rate (bpm)5. Oxygen delivery (mL/min)6. PO2 mmHg)7. Arterial pH8. Serum sodium (mmol/L9. Serum potassium (mmol/L)10. Serum creatinine (mg/dL)11. Hematocrit (%)12. White cell count (103 /mL)13. History of severe organ insufficiency
ACG Practice Guidelines in Acute Pancreatitis. Am J Gastroenterol 2006;101:2379-2400

Diagnostic Guideline II: Determination of severity by Laboratory Tests at Admission or < 48 Hours
Level of Evidence III Hematocrit ≥ 44 at admission and failure of admission hematocrit to
decrease at 24 h are the best predictors of necrotizing pancreatitis
– Absence of hemoconcentration at admission or during the first 24 h is strongly suggestive of a benign clinical course
C-reactive protein greater than 150 mg/L within the first 72 h of disease correlate with the presence of necrosis with a sensitivity and specificity that are both >80%
–The peak of c-reactive protein is generally 36 – 72 h after admission, therefore this test is not helpful at admission in assessing severity
ACG Practice Guidelines in Acute PancreatitisAm J Gastroenterol 2006;101:2379-2400

Hematocrit and Severity
Criteria Incidence of Necrosis
Admission hematocrit >44% 50%OR fails to fall over
first 24 hours
Neither present 4%
Acute Pancreatitis
Brown J, et al., Pancreas 2000; 20:367
Hematocrit and Severity of Acute Pancreatitis
Acute Pancreatitis
Computed Tomography: Indications
•Diagnosis
•Prognosis
•Detect complications
Indications for Computed Tomography (CT) in Acute Pancreatitis
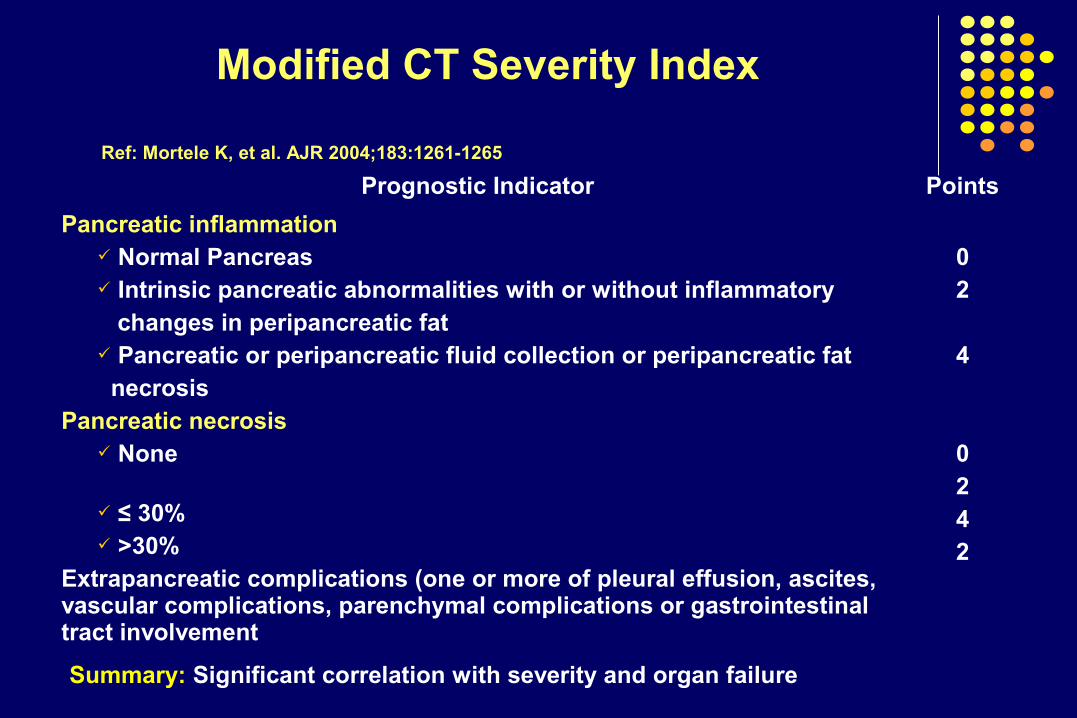
Modified CT Severity Index
Prognostic Indicator Points
Pancreatic inflammation Normal Pancreas Intrinsic pancreatic abnormalities with or without inflammatory changes in peripancreatic fat Pancreatic or peripancreatic fluid collection or peripancreatic fat necrosis
Pancreatic necrosis None ≤ 30% >30%
Extrapancreatic complications (one or more of pleural effusion, ascites, vascular complications, parenchymal complications or gastrointestinal tract involvement
02
4
0242
Summary: Significant correlation with severity and organ failure
Ref: Mortele K, et al. AJR 2004;183:1261-1265
Computed Tomography and Magnetic Resonance Imaging in the Assessment of Acute Pancreatitis
Aim: To compare the accuracy of magnetic resonance imaging with computed tomography in assessing acute pancreatitis
Method: MRI was performed with intravenous secretin and contrast medium
Results 39 patients were studied
Acute pancreatitis was assessed clinically as severe in 7 patients
Considering the Ranson score, MRI detected severe AP with 83% (58-96, 95% CI); sensitivity, 91% (68-98) specificity vs. 78% (52-93) and 86% (63-96) for CT
Magnetic resonance showed pancreatic duct leakage in 3 patients (8%)
Arvanitakis M, et al. Gastroenterology 2004;126(3):715-23
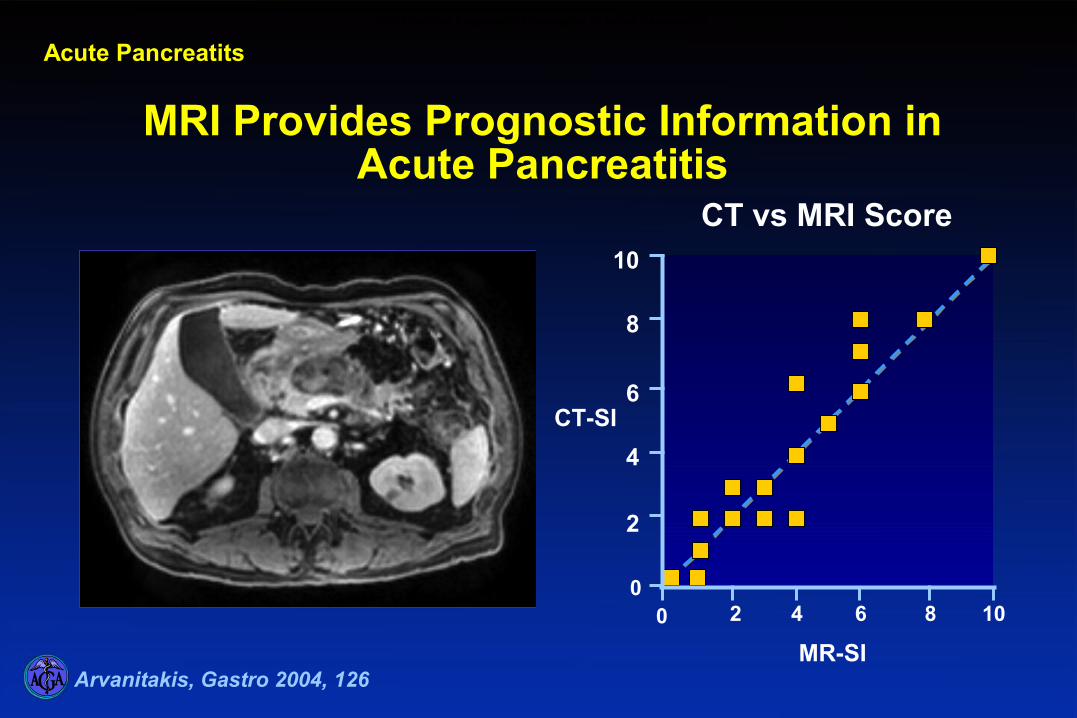
MRI Provides Prognostic Information in Acute Pancreatitis
CT vs MRI Score
MR-SI
CT-SI
2 4 6 8 10
8
10
6
4
2
Arvanitakis, Gastro 2004, 126
00
MRI Provides Prognostic Information in Acute Pancreatitis
Acute Pancreatits

Diagnostic Guideline IIIDetermination of Severity During Hospitalization
Contrast-Enhanced CT Scan
Not on admission if diagnosis is determined - A few days after admission to distinguish interstitial from
necrotizing pancreatitis when there is clinical evidence of increased severity. Level of Evidence III
To guide aspiration in patients with fluid collection to determine if infected
ACG Practice Guidelines in Acute PancreatitisAm J Gastroenterol 2006;101:2379-2400
Acute Pancreatitis
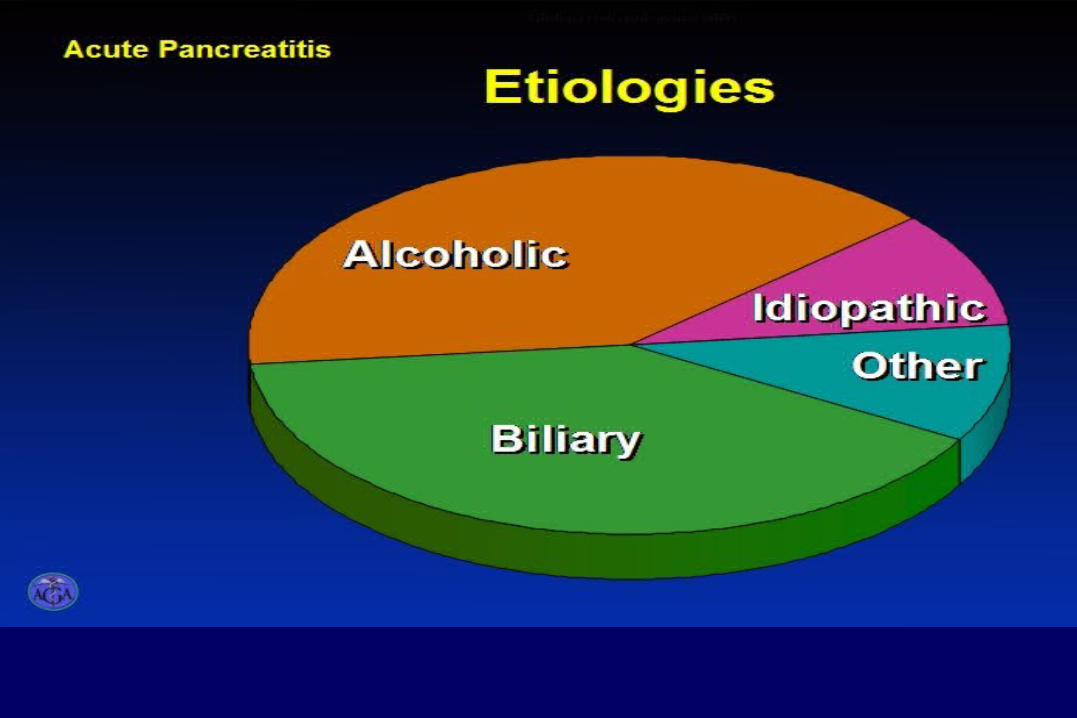
Etiologies of acute pancreatitisEtiologies
Acute Idiopathic Pancreatitis: does it really exist or is it a myth?
Background: Gallstones and alcohol abuse are the most frequent
causes (75% of patients) of acute pancreatitis
Consider hyperlipidemia, hypercalcemia and drugs
In 10% to 40%, no cause is identified
Identifying a cause in these patients is important, since the recurrence rate is high
Van Brummelen SE, et al. Scand J Gastroenterol (Suppl) 2003;(239):117-22

Microlithiasis is the Most Common Cause Acute Idiopathic Pancreatitis
Results: Microlithiasis or biliary sludge is an important cause of
acute ‘idiopathic’ pancreatitis in up to 80% of patients
Microlithiasis can be detected by trans-abdominal/endoscopic ultrasonography or polarizing light microscopy of bile
Acute pancreatitis can be prevented by performing cholecystectomy and opening the sphincter of Oddi
Adapted from: Van Brummelen SE, et al. Scand J Gastroenterol (Suppl) 2003;(239):117-22

Microlithiasis: Effect of Treatment
E Ros, Gastroenterology 1991; 101:1701SP Lee, N Engl J Med 1992, 326:589
%with
recurrent pancreatitis
0
20
40
60
80
100
Untreated Treated
Ros 91Lee 92
Microlithiasis: Effect of Treatment
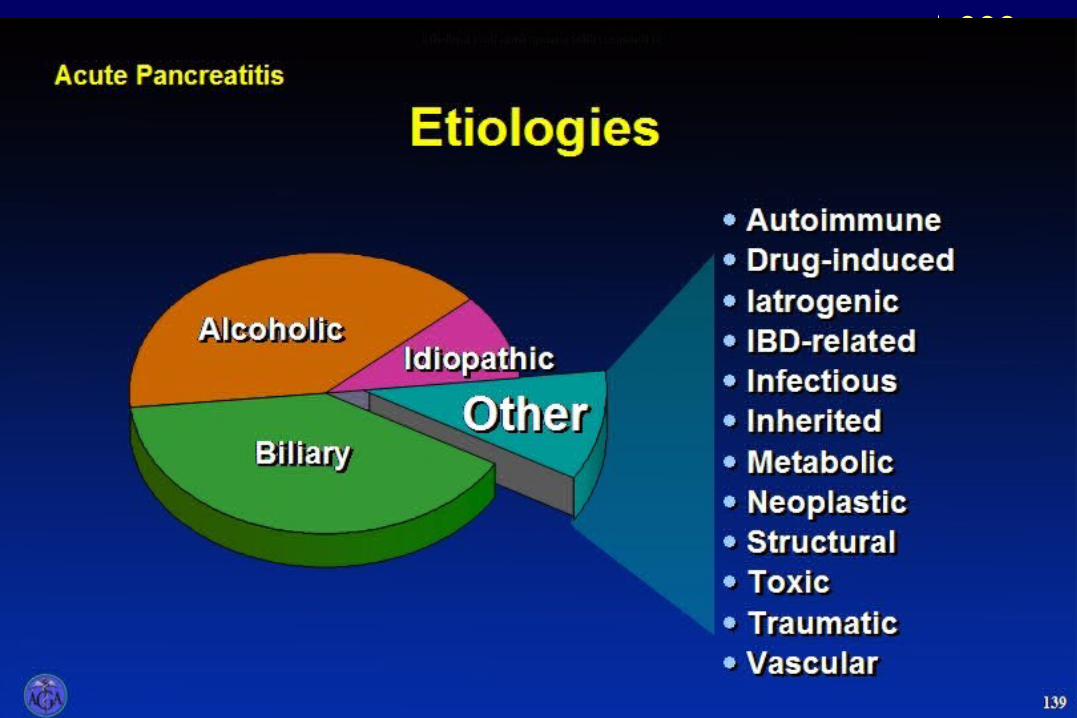
Acute PancreatitisEtiologies of acute pancreatitis expandedEtiologies

Drug-Induced Pancreatitis
1.4% to 2.0% of patients
Mechanism – hypersensitivity - early vs. toxic metabolite (usually <12 weeks)
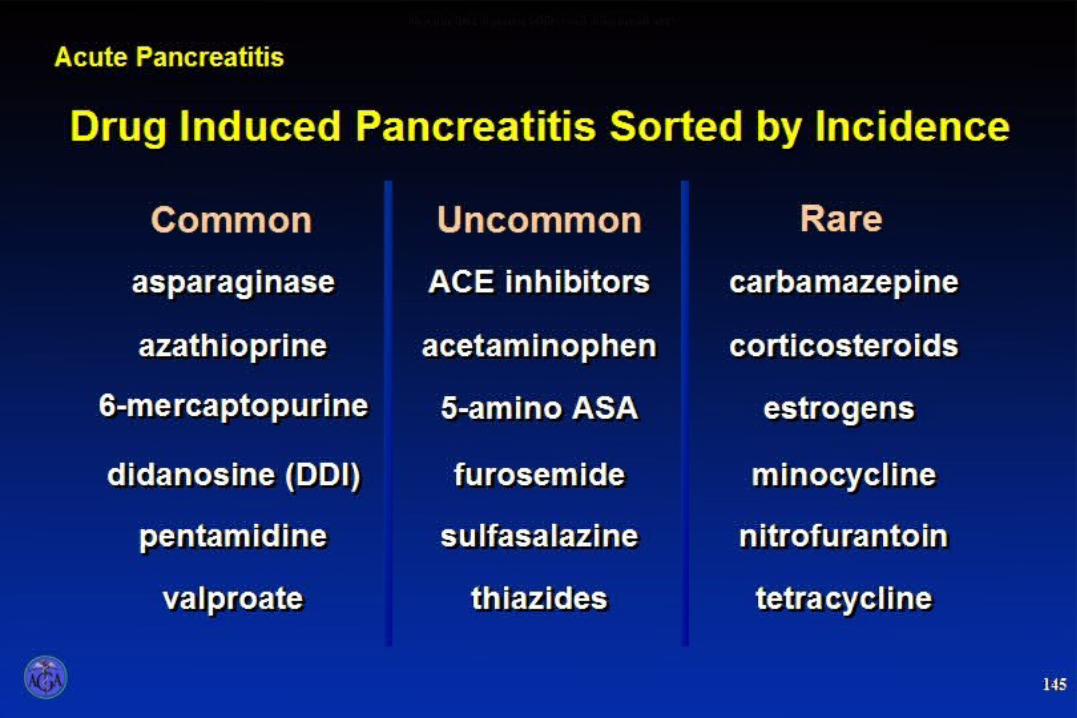
Acute PancreatitisDrug induced pancreatitis sorted by incidence
Drug Induced Acute Pancreatitis 2009
Isoniazid Pegylated interferon alfa-2b Clarithromycin Metronidazole Trimethoprim - sulfamethoxazole
Atorvastatin, Rosuvastatin, Simvastatin
Estrogen/Tamoxifen Propofol
Jawaid Q, et al. Dig Dis Sci 2002;47(3):614-17
Tosun E, et al. Acta Cardiol 2004;59(5):571-572
Chow KM, et al. Van Zuiden Communications 2004;62(1)
Cecchi E, et al. Emergency Medicine Australasia 2004;16:473-475
Schouwenberg BJJW, Deinum J. van Zuiden Communication 2003;61(7)
Singh S, et al. JOP J Pancreas 2004;5(6):502-504
Perego E, et al. JOP J Pancreas 2004;5(5):353-356
Nigwekar SU, Casey KJ. JOP J Pancreas 2004;5(6):516-519
Neth J med 2005;63:275
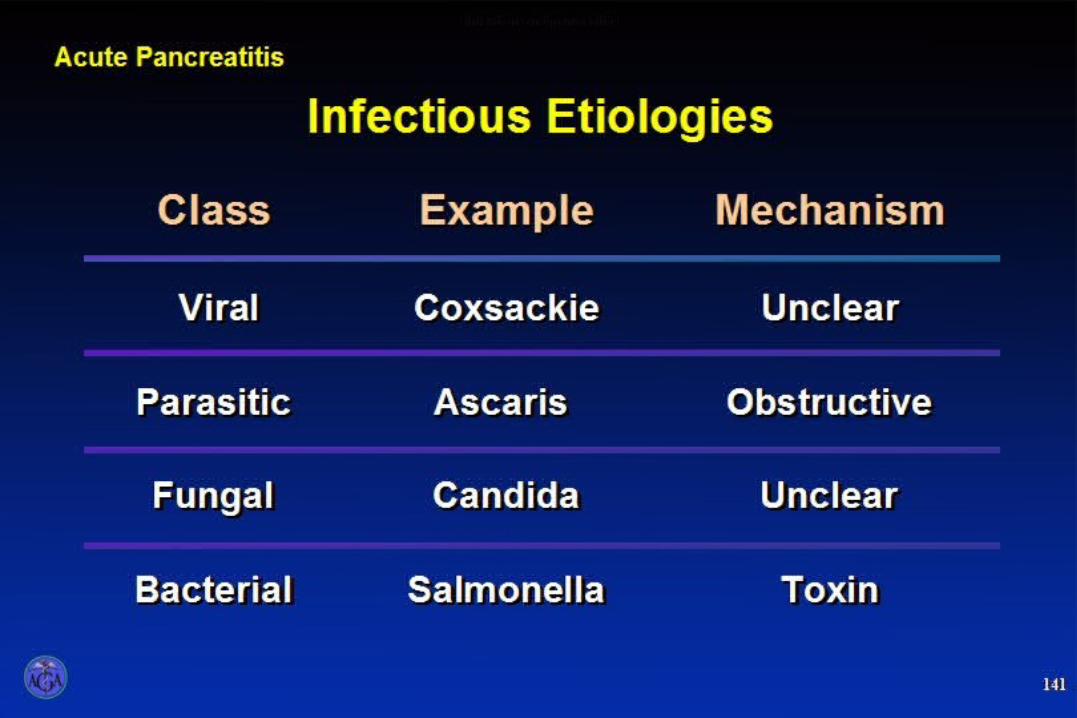
Acute Pancreatitis
Infections and pancreatitis
Infectious Causes of Acute Pancreatitis:2003-2009
Measles Herpes Simplex Hepatitis
A B, C E
HIV
Takebayashi K, et al. Trop Gastroenterol 2003Khanna S, Viji JC. Trop Gastroenterol 2003;24(1):25-6
Makharia GK, et al Trop Gastroenterol 2003;24(4):200-01Tyner R, Turett G. South Med J 2004;97(4):393-94
Shintaku M, et al. Arch Pathol Lab Med 2003;127:231-234

Other Causes of Acute Pancreatitis
Inflammatory bowel disease – Crohn’s (not 5 ASA) – 4-foldUlcerative colitis 1.5 fold
Ischemia – systemic lupus sickle cell crisis Preeclampsia-eclampsia
Toxins – carbofuran insecticides Organophosphates
Fan HC, et al. J Microbial Immunol Infect 2003;36(3):212-4Ahmed S,et al. Am J Hematol 2003 73(3):190-3
Parmar MS. JOP 2004;5(2):101-4Rizos E, et al. JOP 2004;5(1):44-7
Munk AM J Gastro 2004

Acute Pancreatitis
• Rare cause of acute pancreatitis
• Serum triglycerides usually >1000 mg/dL
• May cause chronic disease
• Can be drug-induced:
Alcohol, estrogens,isotretinoin, HIV-protease inhibitors
TG
TG lipase
Free fatty acids
Cell damage
Hypertriglyceridemia

Tumors as Causes of Acute Pancreatitis:
Primary Pancreatic adenocarcinoma IDPMT Ampullary tumors Lymphoma Adult T-cell leukemia/lymphoma
Metastases Lung
Salva R, et al. Ann Surg 2004;239(5):678-85
Adv Thr 2005;22:225
Mori A, 2003 DDS
Acute Biliary Pancreatitis
Goals are to identify:
1. patients whose stones have not passed
2. patients with complications of stones – cholangitis
ERCP is done only if there is biliary obstruction with cholangitis

Biliary Pancreatitis: What happens to CBD stones?
Stone or concretion is found in CBD
a) within 48 hours after admission in 62% – 75%
a) After 48 hours post admission CBD stones are found in 3% – 33%
The natural history of CBD stones is passage
The Value of Magnetic Resonance Cholangio-pancreatography in Predicting CBD Stones in Patients with Gallstone Disease
Results: CBD stones were demonstrated in 43 (12%) of 366
patients
MRCP had – an observed sensitivity of 95% specificity of 100% positive predictive value of 100% and negative predictive value of 98%
Topal B, et al. Br J Surg 2003;90:42-47

Treatment Guideline VIIIRole of ERCP and Biliary Sphincterotomy in Gallstone Pancreatitis
Indicated for clearance of bile duct stones in patients with severe pancreatitis, in those with cholangitis
ERCP should be performed primarily in patients with high suspicion of bile duct stones when therapy is indicated
EUS or MRCP can be used to identify common bile duct stones
Level of Evidence: I
ACG Practice Guidelines in Acute Pancreatitis. Am J Gastroenterol 2006;101:2379-2400
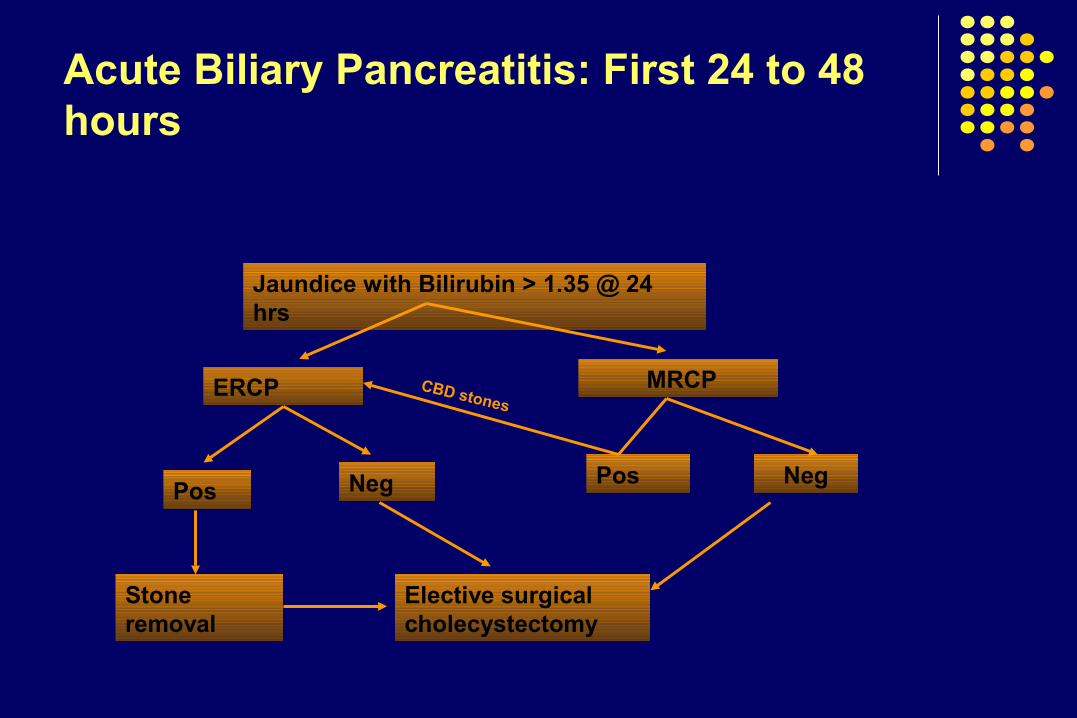
Acute Biliary Pancreatitis: First 24 to 48 hours
Jaundice with Bilirubin > 1.35 @ 24 hrs
ERCP MRCP
PosNeg
Stone removal
Elective surgical cholecystectomy
CBD stones
Neg Pos
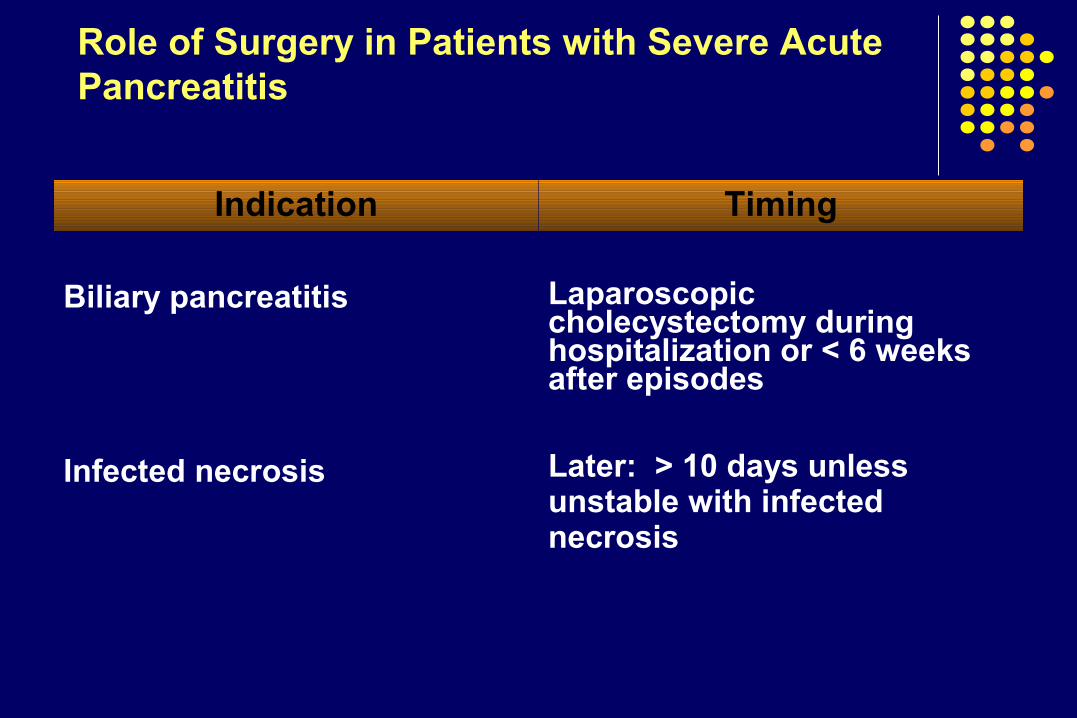
Role of Surgery in Patients with Severe Acute Pancreatitis
Indication Timing
Biliary pancreatitis
Infected necrosis
Laparoscopic cholecystectomy during hospitalization or < 6 weeks after episodes
Later: > 10 days unless unstable with infected necrosis
Early versus Late Necrosectomy in Severe Necrotizing Pancreatitis
Patients were randomly allocated to two treatment arms as follows: Group A included early necrosectomy (within 48 to 72 hours of
onset) Group B included late necrosectomy (at least 12 days after onset)
Results: Difference in the mortality rate (58% vs. 27%) was not
statistically significant, the odds ratio for mortality was much higher in the early operation group
Early surgery in severe acute pancreatitis is only required in cases with proven early infection of the pancreatic necrosis (and not stable) Mier J, et al. Am J Surg 1997;173:71-7
Buchler MW, et al Dig Dis 1992;10:354-62Mai G, et al Berlin, Blackwell Science 1999;475-85
ROLE OF PROPHYLACTIC ANTIBIOTICS IN PATIENTS WITH SEVERE ACUTE
PANCREATITIS
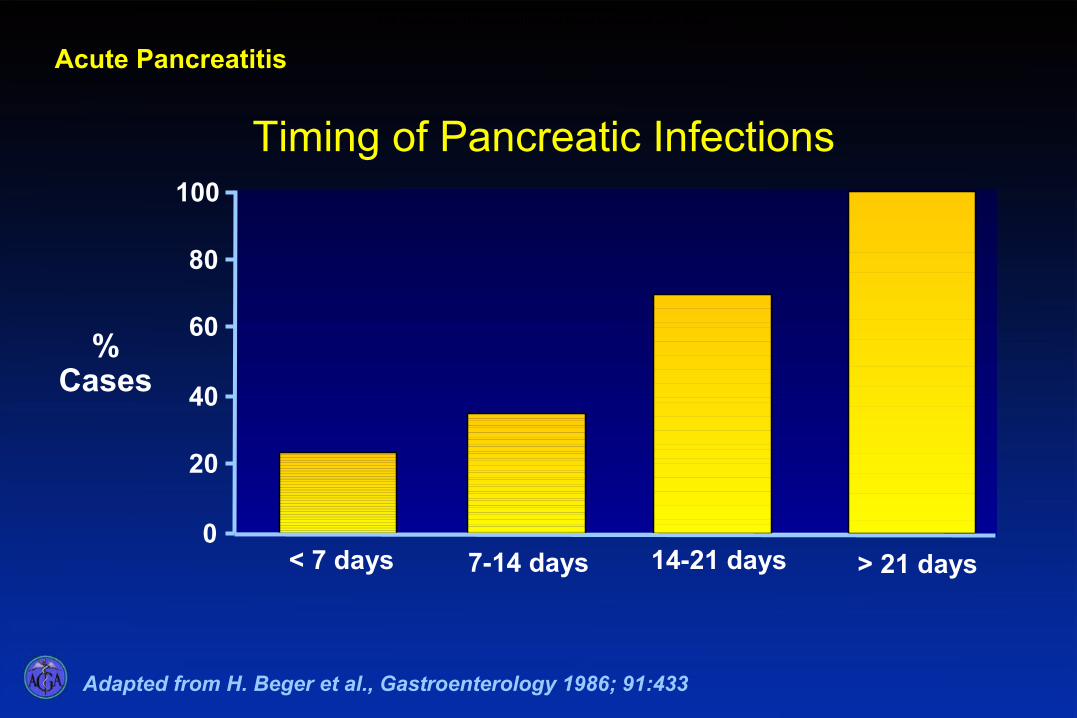
Adapted from H. Beger et al., Gastroenterology 1986; 91:433
Acute Pancreatitis
Timing of Pancreatic Infections
%Cases
0
20
40
60
80
100
< 7 days 7-14 days 14-21 days > 21 days
The incidence of pancreatic infections increases with time

Local and Systemic Infections in Acute Pancreatitis
After week 1, the prognosis . is mainly determined by bacterial infection of pancreatic and peripancreatic necrosis
Mortality increases from 5% - 25% in patients with sterile necrosis to 15% - 28% in patients with infected necrosis
Rau B, et al. J Am Coll Surg 1995;181:279-288
Rau B, et al. World j Surg 1997;21:155-161
Isenmann R, et al.Br J Surg 1999;86:1020-1024
Wilson PG, et al. J Antimicrob Chemother 1998;41(suppl A):51-63
Tenner S, et al. Gastroenterology 1997;113:899-903
Buchler MW, et al. Ann Surg 2000;232:619-626

Preoperative morbidity in patients with infected and sterile necrosis
Bacteriologically positive (45 pts)
n %
Bacteriologically negative (69 pts)
n %
P value
Cardiovascular complications (systemic Pa <80 mm Hg for > min 14 31.0 5 7.3 0.001*
Pulmonary insufficiency (Pa02<60mm Hg) 18 40.0 10 14.3 0.01
Renal insufficiency (creatinine >120 µM) 19 42.2 15 21.7 0.02Sepsis (rectal temperature >38.5°C; leukocytes <4,000 or >12,000/mm3; platelets <150,000/mm3: base excess >-4 16 35.6 6 8.7 0.001*Gastrointestinal bleeding 8 17.8 4 5.8 0.05
*P=0.05 by Holm’s rejective multiple test procedure
Ref: Beger, et al. Pancreatology 2005;5:10-19
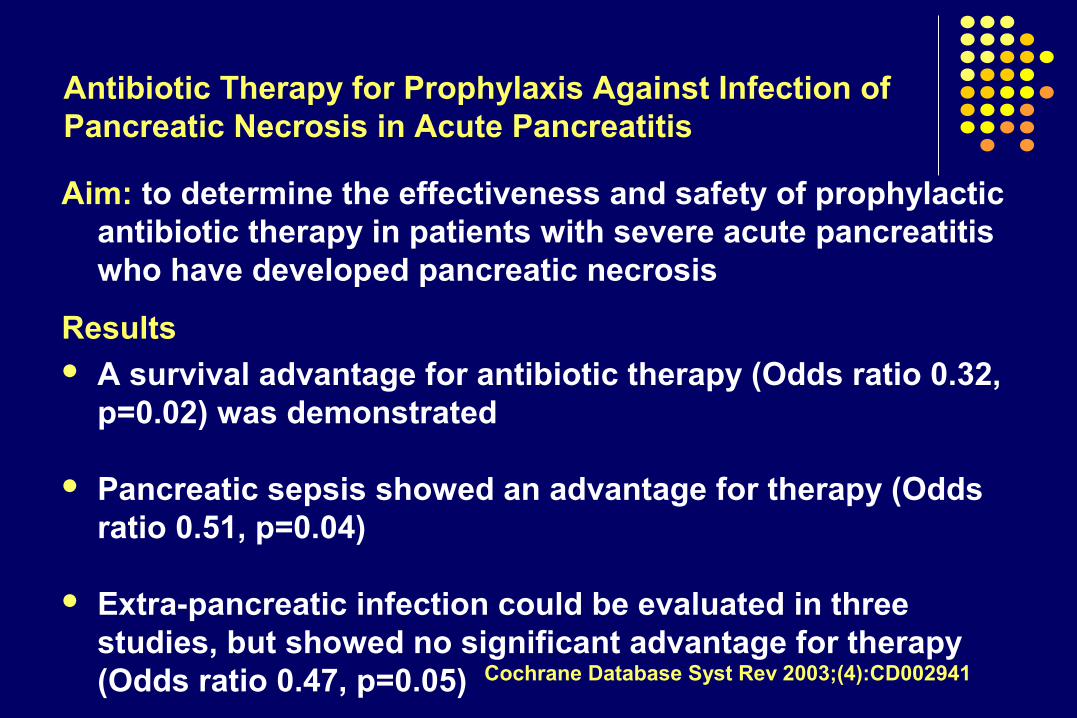
Antibiotic Therapy for Prophylaxis Against Infection of Pancreatic Necrosis in Acute Pancreatitis
Aim: to determine the effectiveness and safety of prophylactic antibiotic therapy in patients with severe acute pancreatitis who have developed pancreatic necrosis
Results A survival advantage for antibiotic therapy (Odds ratio 0.32,
p=0.02) was demonstrated
Pancreatic sepsis showed an advantage for therapy (Odds ratio 0.51, p=0.04)
Extra-pancreatic infection could be evaluated in three studies, but showed no significant advantage for therapy (Odds ratio 0.47, p=0.05) Cochrane Database Syst Rev 2003;(4):CD002941
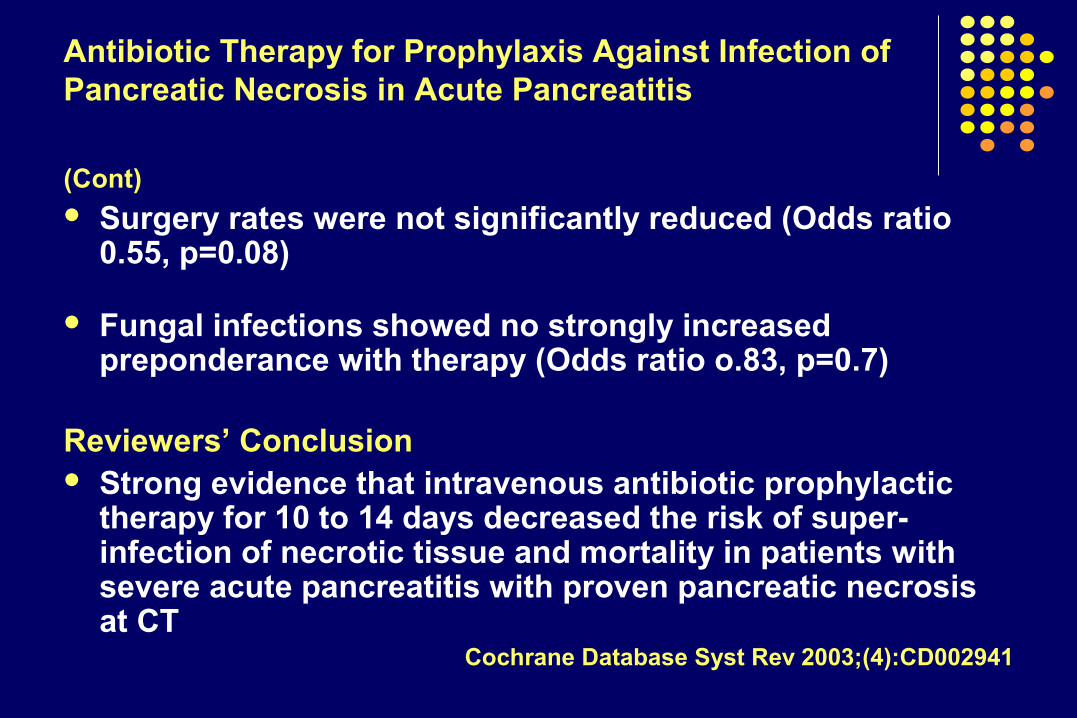
Antibiotic Therapy for Prophylaxis Against Infection of Pancreatic Necrosis in Acute Pancreatitis
(Cont) Surgery rates were not significantly reduced (Odds ratio
0.55, p=0.08)
Fungal infections showed no strongly increased preponderance with therapy (Odds ratio o.83, p=0.7)
Reviewers’ Conclusion Strong evidence that intravenous antibiotic prophylactic
therapy for 10 to 14 days decreased the risk of super-infection of necrotic tissue and mortality in patients with severe acute pancreatitis with proven pancreatic necrosis at CT
Cochrane Database Syst Rev 2003;(4):CD002941
Prophylactic Antibiotic Treatment in Patients with Predicted Severe Acute Pancreatitis: A placebo-controlled, double-blind trial
Method 114 patients with acute pancreatitis in combination with a
serum C-reactive protein exceeding 150 mg/L and/or necrosis on contrast-enhanced CT scan, were enrolled
Patients received either intravenous CIP (2 x 400 mg/day) + MET (2 x 500 mg/day) or PLA
Study medication was discontinued and switched to open antibiotic treatment when infectious complications, multiple organ failure sepsis or systemic inflammatory response syndrome (SIRS) occurred

Ciprofloxacin plus metronidazole vs. placebo in severe acute pancreatitis
Intention-to-treat analysis(114 patients)
Ciprofloxacin/ placeboMetronidazole (56 patients)(58 patients)
Necrotizing pancreatitis on contrast-enhanced CT scan(76 patients)
Ciprofloxacin/ placeboMetronidazole (35 patients)(41 patients)
MortalitySurgical treatmentInfected pancreatic necrosis
5% 7% 17% 11% 12% 9%
7% 11% 24% 19% 17% 14%
Isenmann R, et al. Gastroenterology 2004;126:997-1004

Prophylactic Antibiotic Use in Severe Acute Pancreatitis (SAP): Hemlock, Help or Hype?
Concerns A large number of subjects in the treatment arm (16 of 58)
had their antibiotics switched from the study medicines
Many individuals in the control group (26 of 56) were started on antibiotic therapy during the trial period
Number of subjects in each of the comparison groups was very small and the study was likely underpowered to detect a difference in the secondary endpoints
Brown A. Gastroenterology 2004;1195-1198
Early Antibiotic Treatment for Severe Acute Necrotizing Pancreatitis
Methods Multicenter, prospective, double-blind, placebo-controlled randomized
study set in 32 centers
Participants One hundred patients with necrotizing pancreatitis; 50 received
meropenem and 50 received placebo
Outcome Measures infection within 42 days
Results Pancreatic or peripancreatic infections developed in 18% (9/50) of
patients in the meropenem group compared with 12% (6 /50) in the placebo group
Dellinger EP, et al. Ann Surg 2007;245;674-683

As Good As it Gets:The Study of Prophylactic Antibiotics in Severe Acute Pancreatitis
The studies suffered from a high percentage of patients in the placebo group (Isenmann study, 46%; Dellinger study 54%) who were treated with intravenous antibiotics, although in the Dellinger study, these were used late, on average, nearly 3 weeks following randomization
Placebo group infection rates in both studies were only 17% (7/41) in the Isenmann study and 12% (6/50) in the Dellinger study
Howard TJ. Ann Surg 2007;245 (5): 684-85
Treatment Guideline IVAntibiotics in Necrotizing Pancreatitis
Level of Evidence III Not recommended at this time in patients with necrotizing pancreatitis
During the first 7 – 10 days, patients with pancreatic necrosis may appear septic with leukocytosis, fever, and/or organ failure
Antibiotic therapy is appropriate while an evaluation for a source of infection is undertaken
Once blood and other cultures (including CT-guided fine needle aspiration) are found to be negative, discontinue antibiotic therapy
ACG Practice Guidelines in Acute Pancreatitis. Am J Gastroenterol 2006;101:2379-2400
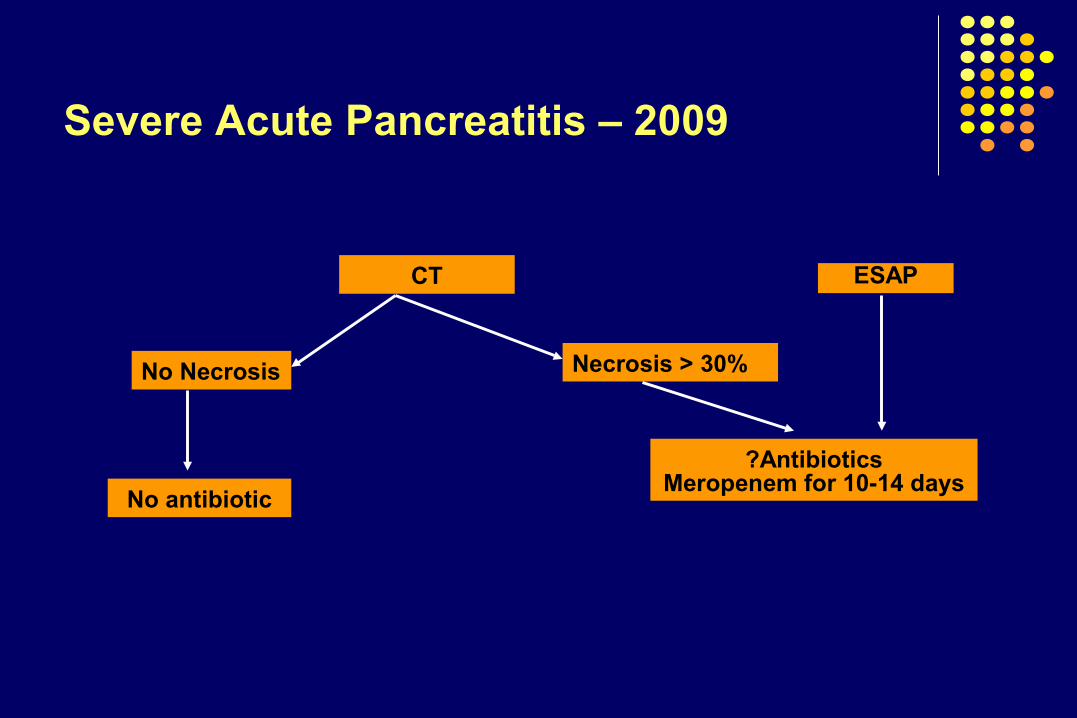
Severe Acute Pancreatitis – 2009
CT
No Necrosis Necrosis > 30%
No antibiotic
?AntibioticsMeropenem for 10-14 days
ESAP

Management of Pancreatitis Prior to CT-FNA
The extent of leukocytosis or temperature does not reliably distinguish severe sterile from infected necrosis
The development of organ failure (or multi-system organ failure) and serum markers are not reliable indicators of infected necrosis
Buchler MW, et al. Ann Surg 2000;232(5):619-26Mier J, et al. Am J Surg 1997;173(2):71-5Rau B, et al. Br J Surg 1998;85(2):179-84

Infected NecrosisSuspicion
Tº > 100 F elevated WBC unresolved organ failure Recurrence of SIRS or persistence > 7 days
Diagnosis CT guided aspirate for gram stain and Culture and
sensitivity
Severe Acute Pancreatitis: Role of CT-guided Needle Aspiration
Percutaneous Aspiration of Pancreatic Fluid Collection – Gram stain and Culture
10% aspirate gram stain negative and culture positive
No history of antibiotic administered
Aspirant gram stain positive with negative cultures in 2
of 34 (6%) patients
Effect of antibiotics on aspirate
Barkin JS, et al. Dig Dis Sci 1981;26(7):585Freeny PC, et al AJR 1998;170:969-975
Value of Percutaneous Aspiration of the Pancreas (CT-FNA)
CT-FNA is safe and accurate in distinguishing sterile from infected necrosis
CT-FNA results dictate that appropriate antibiotics can be initiated based on the results of culture and sensitivity and surgical debridement
Observation and support to overcome organ failure should be maintained during the first several weeks of acute pancreatitis in patients with sterile necrosis based on CT-FNA therapy because of the high mortality associated with early surgical debridementPappas TN. Am J Gastroenterol 2005;100:2371-2374

Treatment Guideline V:Treatment of Infected Necrosis
CT-guided percutaneous aspiration with Gram’s stain and culture aspirate is recommended when infected necrosis is suspected
Treatment of choice in infected necrosis is surgical debridement
Level of Evidence III
ACG Practice Guidelines in Acute Pancreatitis. Am J Gastroenterol 2006;101:2379-2400
Route of Alimentation
TPN
Cost – high
No pancreas stimulation
Increased infections
Electrolyte disturbances
Detrimental to gut integrity
Enteral
Cost – moderate
May stimulate pancreas
Reduced infections
Electrolytes undisturbed
May retain gut integrity
Acute Pancreatitis: Nutrition
Route of Alimentation
Acute Pancreatitis
Negative effects of TPN Increased gut permeability Increased central catheter-related sepsis Immunosuppressive effects Increased incidence of septic complications Greatly increased costs
Total Parenteral Nutrition (TPN) andEnteral Nutrition (EN)
TPN – causes intestinal mucosal atrophy alterations in the gut associated lymphoid tissue (GALT) system and a reduction in intestinal secretory IgA (S-IgA) levels
EN – prevents hypermetabolism, maintains immunocompetence and improves wound healing; considered to reduce septic complications, shorten hospital stay and reduce the risk of death
Levine GM, et al Gastro 1974:67:975King BK, et al. Arch Surg
Kudsk KA, et al Ann Surg 1996:223:629Mochizuk H, et al Ann Surg 1984;200:297-310
Alverdy J, et al. Ann Surg 1985;202:681Schroeder D, et al JPEN 1991;15:376
Moore FA, et al. J Trauma 1989;29:916.
Safe and well-tolerated:Elemental diet causes less pancreas stimulation
Demonstrated Benefits:Reduced infectionsFewer metabolic complications
Shorter length of stay
Potential benefits: Improved intestinal permeability
Reduced systemic inflammatory response
Acute Pancreatitis: Nutrition
Enteral Feeding
Enteral Feeding

Marik PE BMJ 2004; doi:10.1136/bmj
Enteral vs Parenteral Nutrition Favors FavorsStudy enteral parenteral
Infection
0.1 1 10
Complications other than infection
Surgical interventions
Mortality
Acute Pancreatitis
Enteral vs Parenteral Nutrition

Meta-analysis of Parenteral Nutrition versus Enteral Nutrition in Patients with Acute Pancreatitis
Aim: To compare the safety and clinical outcomes of enteral and parenteral nutrition in patients with acute pancreatitis
Method 263 participants in the 6 randomized controlled studies were analyzed
Data Synthesis Enteral nutrition was associated with a significantly lower incidence of
infections (relative risk 0.45; 98% confidence interval 0.26 to 0.78, P=0.004), reduced surgical interventions to control pancreatitis (0.48, 0.22 to 1.0; P=0.05)
A reduced hospital stay (mean reduction 2.9 days, 1.6 days to 4.3 days, P<0.001)
There were no significant differences in mortality (relative risk ).66, 0.32 to 1.37, P=0.3) or non-infectious complications (0.61, 0.31 to 1.22, P=0.16) between the two groups Marik, PE, Zaloga GP. BMJ 2004;328:1407-09

Infections
Favors FavorsStudy enteral TPN
Abou-Assi
Gupta
Kalfarentzo
McClave
Olah
Windsor
0.01 0.1 1 10 100
Total (95% CI)
Marik PE, Zaloka GP. BMJ 2004; 328:1407
Nutritional Support and InfectionAcute Pancreatitis
Nutritional Support and Infection
Treatment Guideline IIINutritional Support
Enteral feeding rather than total parenteral nutrition is suggested for patients who require nutritional support
Level of Evidence II In severe necrotizing pancreatitis (especially when most or
all of the pancreas is necrotic) provide potent pancreatic enzymes and then evaluate later in the course
It is prudent to use a proton pump inhibitor because of the likelihood that bicarbonate secretion by the pancreas is severely diminished
ACG Practice Guidelines in Acute PancreatitisAm J Gastroenterol 2006;101:2379-2400

Treatment Guideline I:Supportive Care
Level of Evidence III
1. Carefully monitored during the first 24 h of vital signs, oxygen saturation and fluid balance - hypoxemia and inadequate fluid resuscitation may be unrecognized for prolonged periods of time
Result: Early aggressive fluid resuscitation and improved delivery of oxygen prevent or minimize pancreatic necrosis and improve
survival
2. Consequence of hypovolemia is intestinal ischemia, which increases intestinal permeability to bacteria and endotoxin
Result: Translocation of bacteria cause secondary pancreatic infection and contribute to on-going pancreatic injury and also to organ failure ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
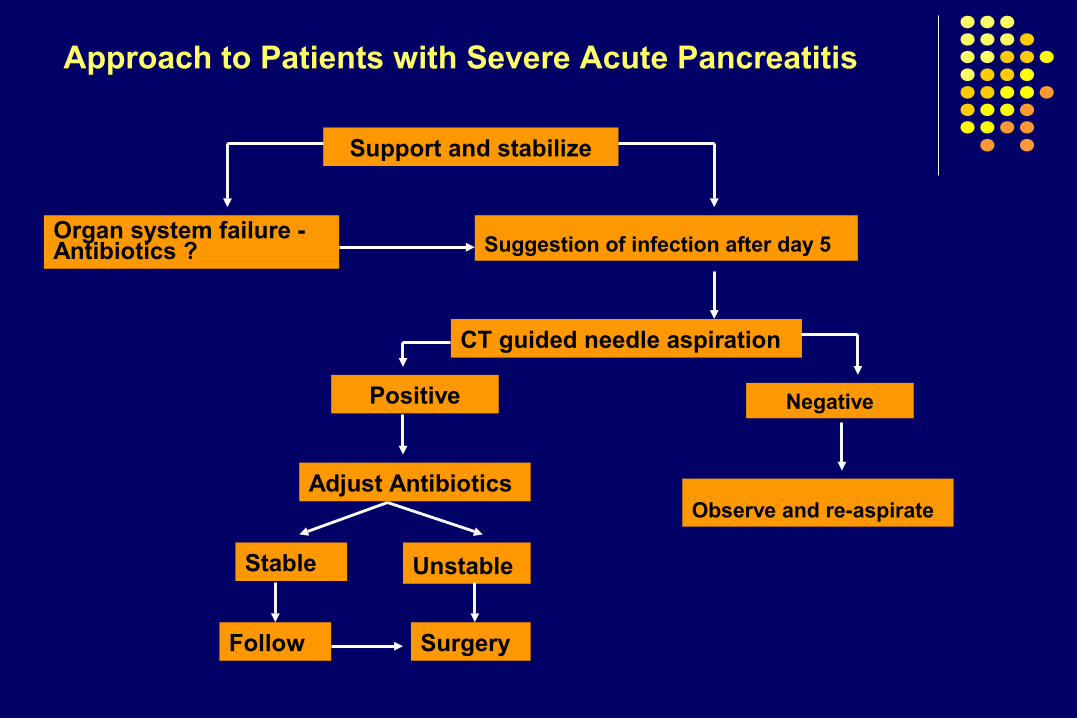
Positive
Suggestion of infection after day 5
Support and stabilize
Approach to Patients with Severe Acute Pancreatitis
.
Negative
Observe and re-aspirate
Organ system failure -Antibiotics ?
CT guided needle aspiration
Adjust Antibiotics
Stable
Follow
Unstable
Surgery

THANK YOU!