Pancreatic Ductal Adenocarcinoma (PDAC)crukcambridgecentre.org.uk/sites/default/files/Teaching...
45
Pancreatic Ductal Adenocarcinoma (PDAC) The Clinical Problem and Current Drug Treatment Duncan Jodrell Professor of Cancer Therapeutics CRUK Cambridge Institute Li Ka Shing Centre, University of Cambridge
Transcript of Pancreatic Ductal Adenocarcinoma (PDAC)crukcambridgecentre.org.uk/sites/default/files/Teaching...
Pancreatic Ductal Adenocarcinoma (PDAC) The Clinical Problem and Current Drug Treatment
Duncan Jodrell
Professor of Cancer Therapeutics
CRUK Cambridge Institute
Li Ka Shing Centre,
University of Cambridge
The clinical problem
• The 10th most common cancer, but the 4th most common killer
• Using current trends in outcome, PDAC is projected to become the 2nd most common cancer killer by 2030
• Why?
– Presents late:
• Non specific symptoms; weight loss, epigastric pain
• only 10-20% of patients suitable for operation at presentation (usually those presenting with obstructive jaundice)
– Considered to be relatively resistant to chemotherapy (average survival
< 12 months, following a diagnosis of metastatic disease)
– Debilitating effects often preclude aggressive treatment:
• Pain, anorexia, biliary obstruction, duodenal obstruction, cachexia
7/1
1/1
3
17
/01
/14
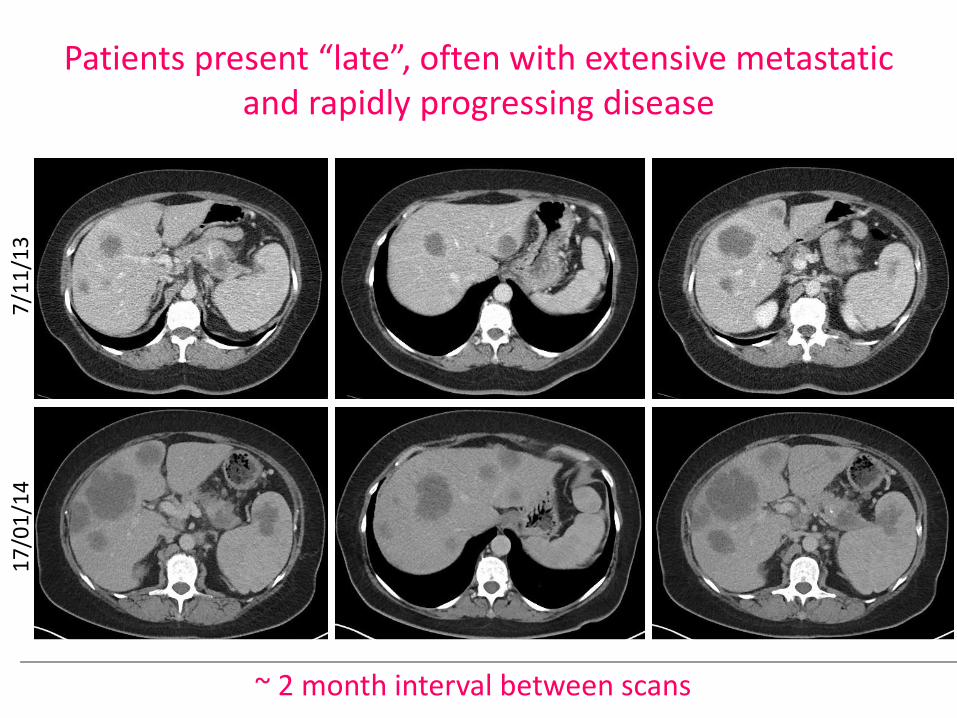
Patients present “late”, often with extensive metastatic and rapidly progressing disease
~ 2 month interval between scans
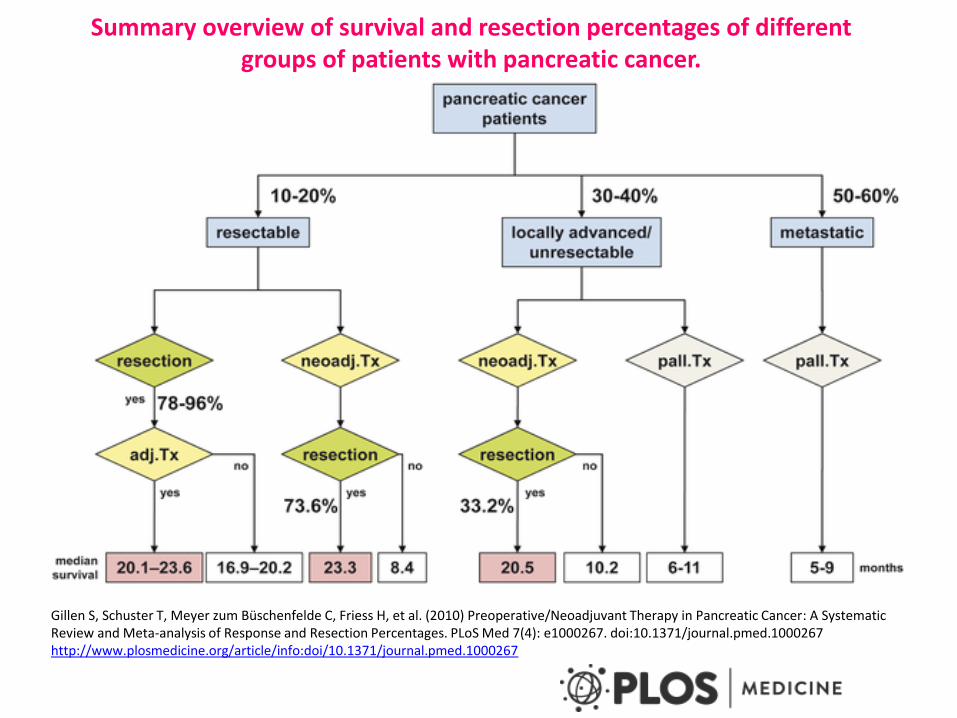
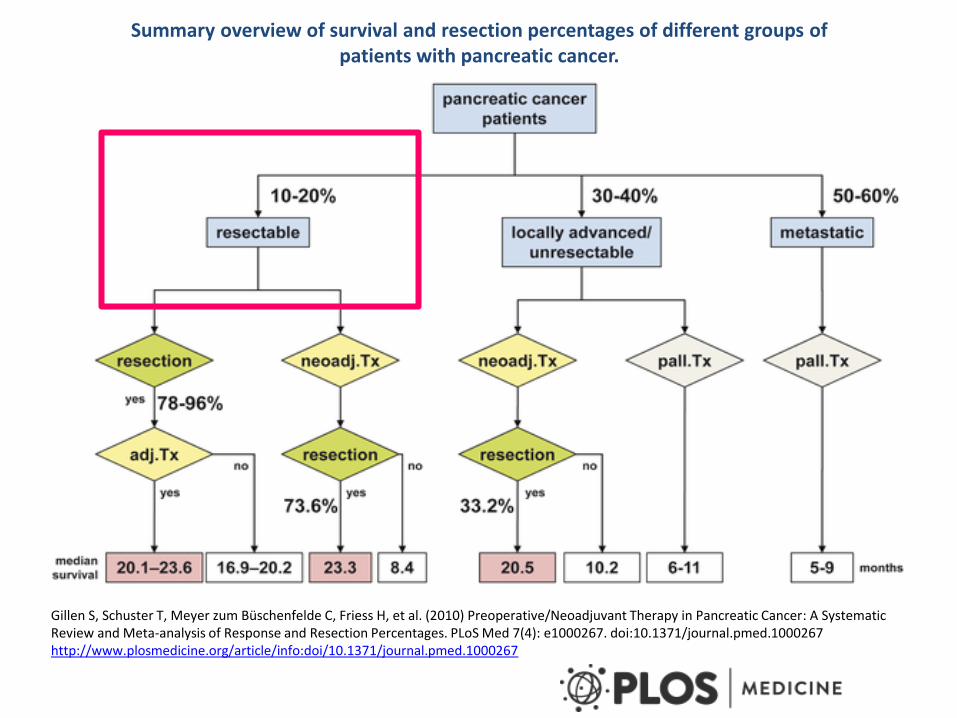
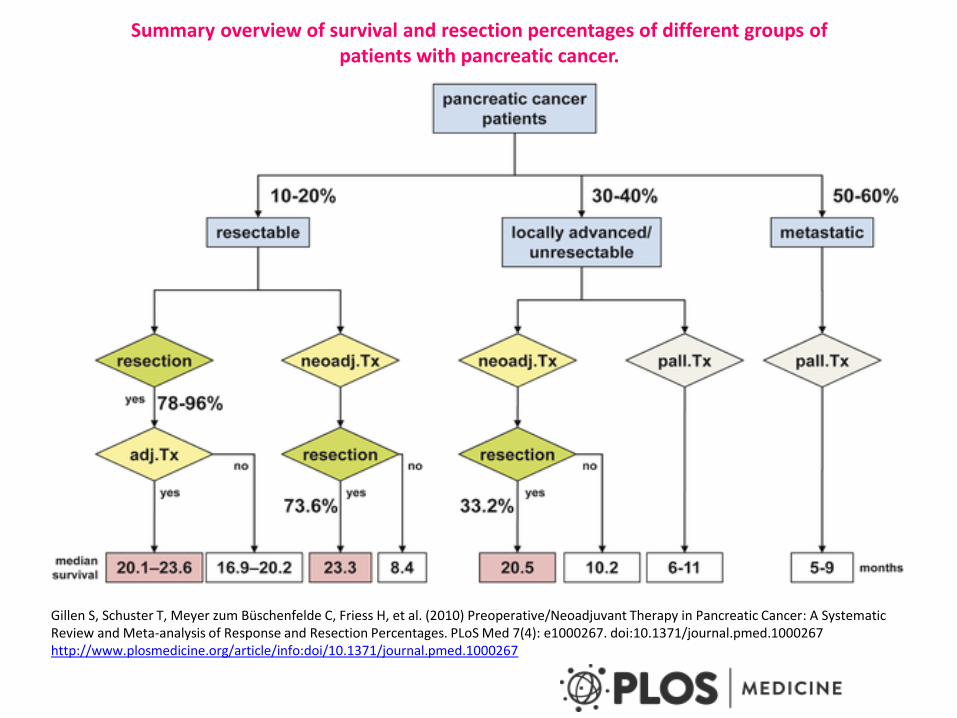
Summary overview of survival and resection percentages of different groups of patients with pancreatic cancer.
Gillen S, Schuster T, Meyer zum Büschenfelde C, Friess H, et al. (2010) Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med 7(4): e1000267. doi:10.1371/journal.pmed.1000267 http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1000267
Established treatments for advanced disease
• Gemcitabine (Burris et al, JCO, 1997)
– Clinical benefit response was experienced by 23.8% of gemcitabine-treated patients compared with 4.8% of 5-FU treated patients (P = .0022)
– The median survival durations were 5.65 and 4.41 months for gemcitabine treated and 5-FU treated patients, respectively (P = .0025).
– The survival rate at 12 months was 18% for gemcitabine patients and 2% for 5-FU patients.
• Gemcitabine plus erlotinib • Gemcitabine plus capecitabine • Gemcitabine plus nab-paclitaxel (2013)
• Not to mention multiple, negative GEM plus X Phase III trials!
• FOLFIRINOX (2013)
Gemcitabine plus erlotinib
(Moore et al, 2007)
569 patients HR was 0.82 for survival (p=0.038) This translates into a median survival advantage of 0.33 months Q: can molecular phenotyping or genotyping identify the small number of patients who benefit from erlotinib? e.g. “EGF addicted” tumours
Gemcitabine plus capecitabine
(Cunningham et al, 2009) 533 patients HR (survival) = 0.86 (p=0.08) compared to gemcitabine alone 935 patients were included in a meta-analysis of 3 studies, confirming the HR of 0.86 (p=0.02) On this basis, GEMCAP became the standard of care in the UK
The positive outcome of the Phase III (MPACT) study was presented at ASCO 2013 861 patients HR was 0.72, leading to an improvement in overall survival of 1.8 months
Gemcitabine/nab-paclitaxel (AbraxaneTM)
(Von Hoff et al, 2013)
FOLFIRINOX
(Conroy et al, 2013)
342 patients HR of 0.57, leading to a survival advantage of 4.3 months 2 weekly regimen: Oxaliplatin (85 mg m-2) Irinotecan (180 mg m-2) Folinic acid (400 mg m-2) Bolus 5FU (400 mg m-2) Infusional 5FU (2400 mg m-2 over 46 hours) ….. plus G-CSF (filgastrim) s.c. in 43%
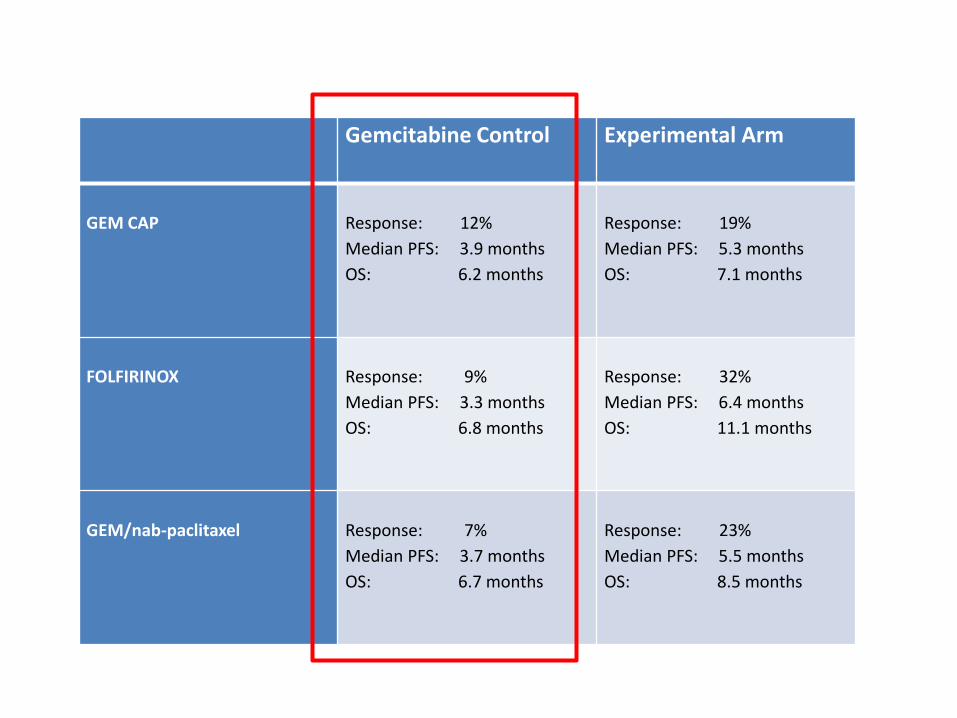
Gemcitabine Control Experimental Arm
GEM CAP
Response: 12%
Median PFS: 3.9 months
OS: 6.2 months
Response: 19%
Median PFS: 5.3 months
OS: 7.1 months
FOLFIRINOX
Response: 9%
Median PFS: 3.3 months
OS: 6.8 months
Response: 32%
Median PFS: 6.4 months
OS: 11.1 months
GEM/nab-paclitaxel
Response: 7%
Median PFS: 3.7 months
OS: 6.7 months
Response: 23%
Median PFS: 5.5 months
OS: 8.5 months
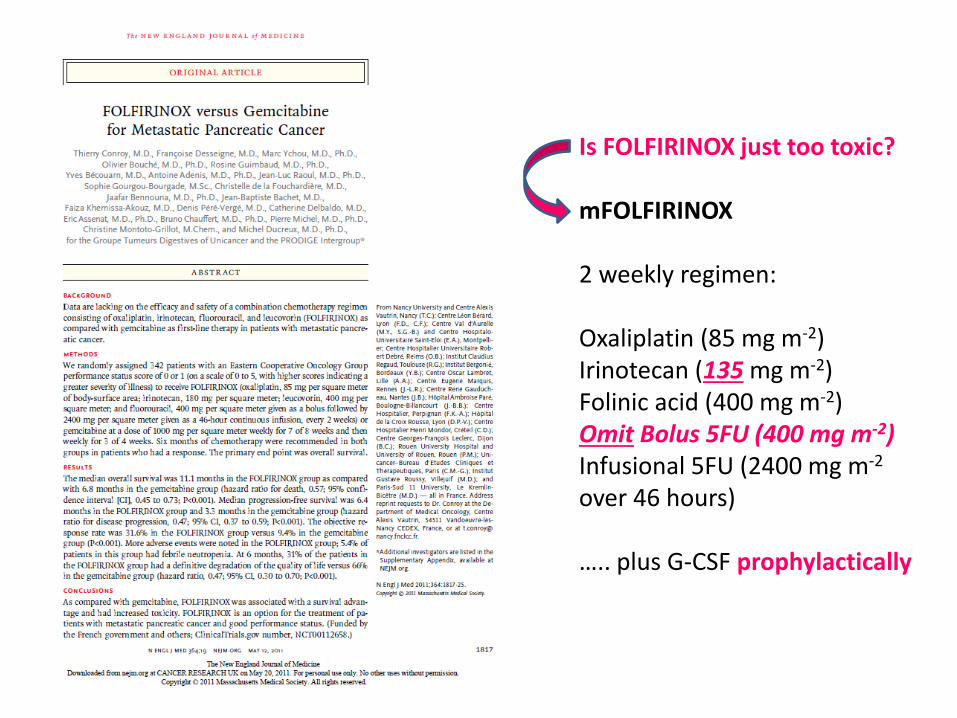
Is FOLFIRINOX just too toxic? mFOLFIRINOX 2 weekly regimen: Oxaliplatin (85 mg m-2) Irinotecan (135 mg m-2) Folinic acid (400 mg m-2) Omit Bolus 5FU (400 mg m-2) Infusional 5FU (2400 mg m-2
over 46 hours) ….. plus G-CSF prophylactically
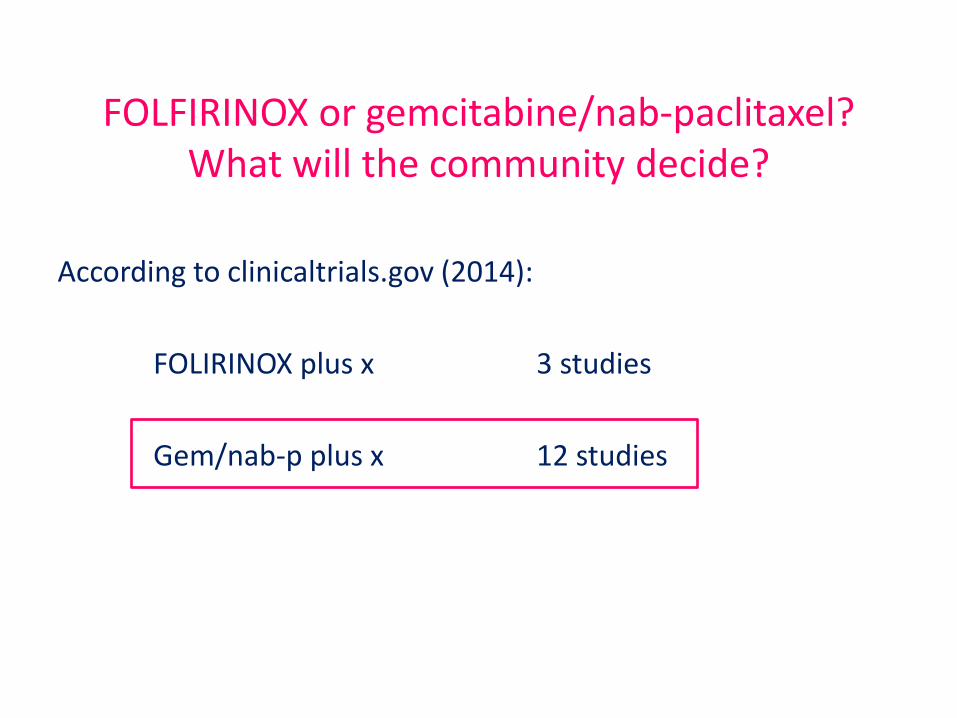
FOLFIRINOX or gemcitabine/nab-paclitaxel? What will the community decide?
According to clinicaltrials.gov (2014):
FOLIRINOX plus x 3 studies
Gem/nab-p plus x 12 studies
Summary overview of survival and resection percentages of different groups of patients with pancreatic cancer.
Gillen S, Schuster T, Meyer zum Büschenfelde C, Friess H, et al. (2010) Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med 7(4): e1000267. doi:10.1371/journal.pmed.1000267 http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1000267
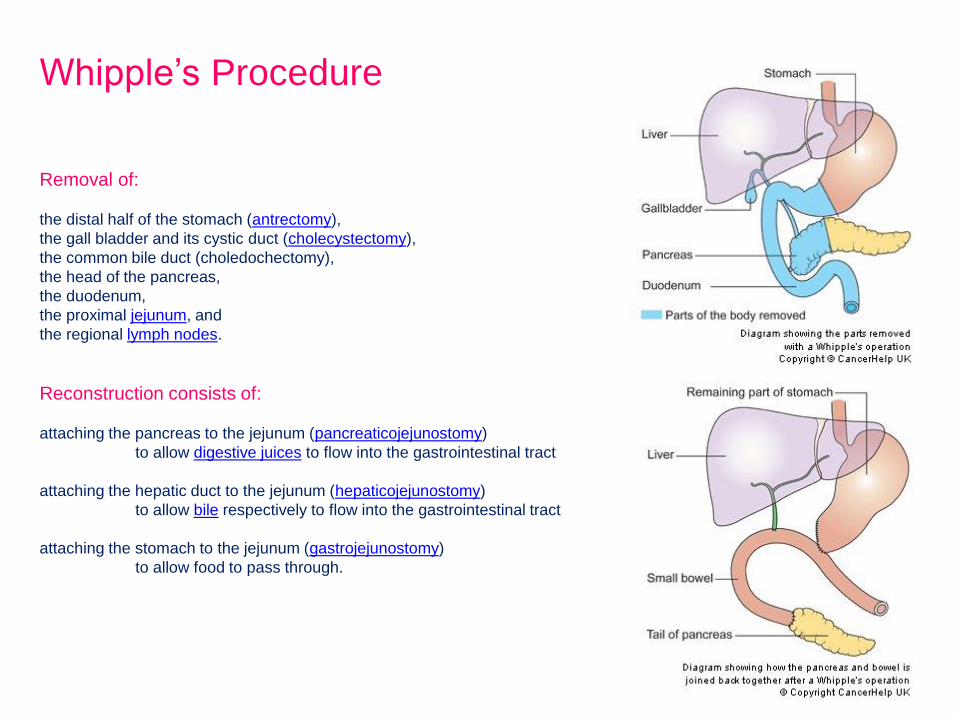
Removal of:
the distal half of the stomach (antrectomy),
the gall bladder and its cystic duct (cholecystectomy),
the common bile duct (choledochectomy),
the head of the pancreas,
the duodenum,
the proximal jejunum, and
the regional lymph nodes.
Reconstruction consists of:
attaching the pancreas to the jejunum (pancreaticojejunostomy)
to allow digestive juices to flow into the gastrointestinal tract
attaching the hepatic duct to the jejunum (hepaticojejunostomy)
to allow bile respectively to flow into the gastrointestinal tract
attaching the stomach to the jejunum (gastrojejunostomy)
to allow food to pass through.
Whipple’s Procedure
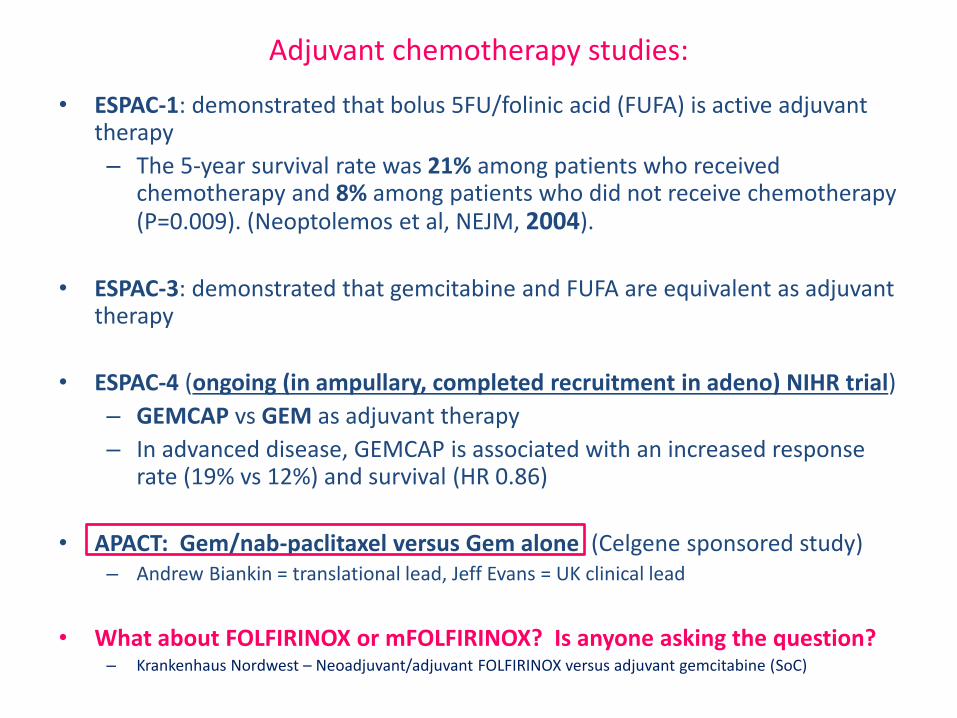
Adjuvant chemotherapy studies:
• ESPAC-1: demonstrated that bolus 5FU/folinic acid (FUFA) is active adjuvant therapy
– The 5-year survival rate was 21% among patients who received chemotherapy and 8% among patients who did not receive chemotherapy (P=0.009). (Neoptolemos et al, NEJM, 2004).
• ESPAC-3: demonstrated that gemcitabine and FUFA are equivalent as adjuvant therapy
• ESPAC-4 (ongoing (in ampullary, completed recruitment in adeno) NIHR trial)
– GEMCAP vs GEM as adjuvant therapy
– In advanced disease, GEMCAP is associated with an increased response rate (19% vs 12%) and survival (HR 0.86)
• APACT: Gem/nab-paclitaxel versus Gem alone (Celgene sponsored study) – Andrew Biankin = translational lead, Jeff Evans = UK clinical lead
• What about FOLFIRINOX or mFOLFIRINOX? Is anyone asking the question? – Krankenhaus Nordwest – Neoadjuvant/adjuvant FOLFIRINOX versus adjuvant gemcitabine (SoC)
Summary overview of survival and resection percentages of different groups of patients with pancreatic cancer.
Gillen S, Schuster T, Meyer zum Büschenfelde C, Friess H, et al. (2010) Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med 7(4): e1000267. doi:10.1371/journal.pmed.1000267 http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1000267
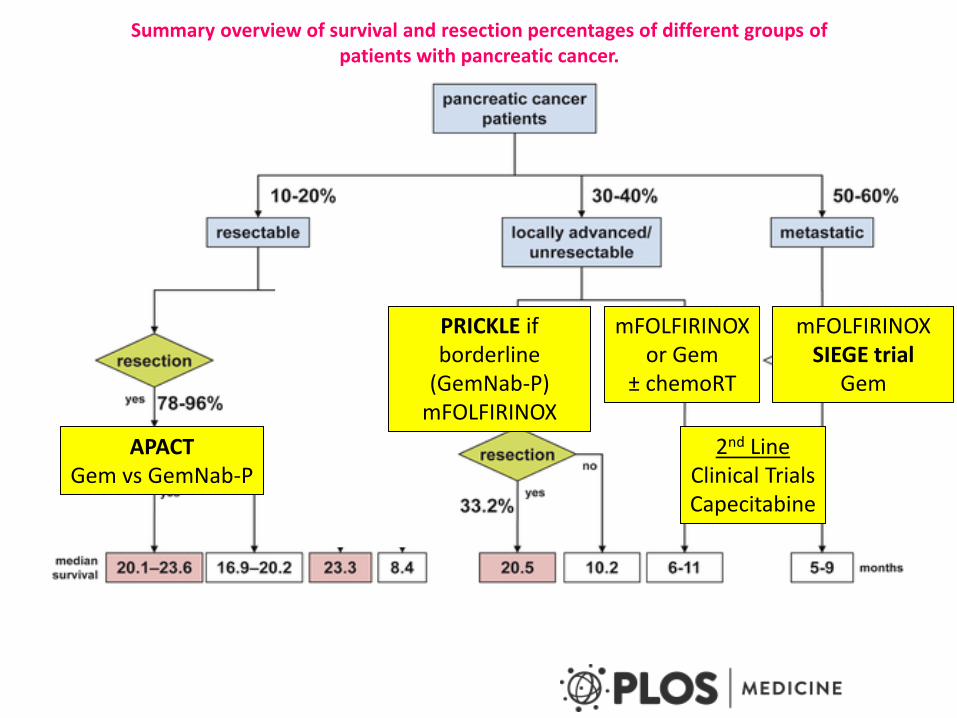
APACT Gem vs GemNab-P
mFOLFIRINOX or Gem
± chemoRT
mFOLFIRINOX SIEGE trial
Gem
2nd Line Clinical Trials Capecitabine
PRICKLE if borderline
(GemNab-P) mFOLFIRINOX
Summary overview of survival and resection percentages of different groups of patients with pancreatic cancer.
How does nanoparticle albumin–bound (nab)-paclitaxel potentiate gemcitabine activity?
PDAC is a stromal-rich tumour and it expresses high levels of secreted protein acidic and rich in cysteine (SPARC)
One hypothesis was that SPARC may act as an albumin-binding protein, sequestering the nab-paclitaxel, to concentrate the drug intra-tumourally
SPARC expression was therefore suggested to be a potential predictive biomarker for nab-paclitaxel activity (Von Hoff, J. Clin Oncol. 2011)
… but subsequently, review of the MPACT Phase III data discounted this (Hidalgo, World GI, 2014)markers
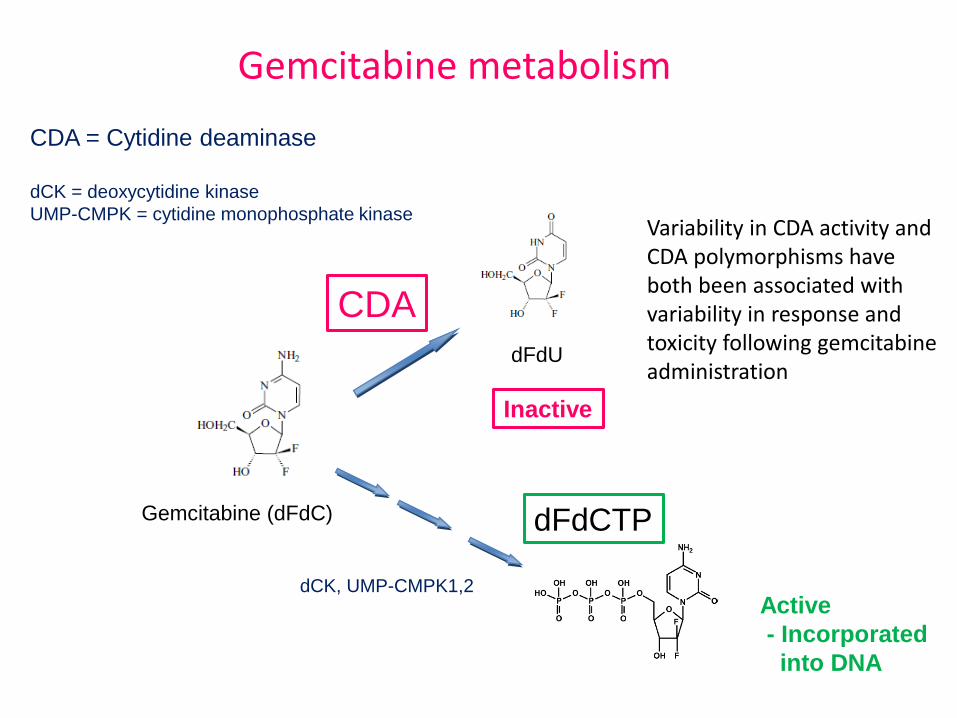
Gemcitabine metabolism
dFdU
Gemcitabine (dFdC) dFdCTP
Inactive
Active
- Incorporated
into DNA
CDA = Cytidine deaminase
dCK = deoxycytidine kinase
UMP-CMPK = cytidine monophosphate kinase
dCK, UMP-CMPK1,2
CDA
Variability in CDA activity and CDA polymorphisms have both been associated with variability in response and toxicity following gemcitabine administration
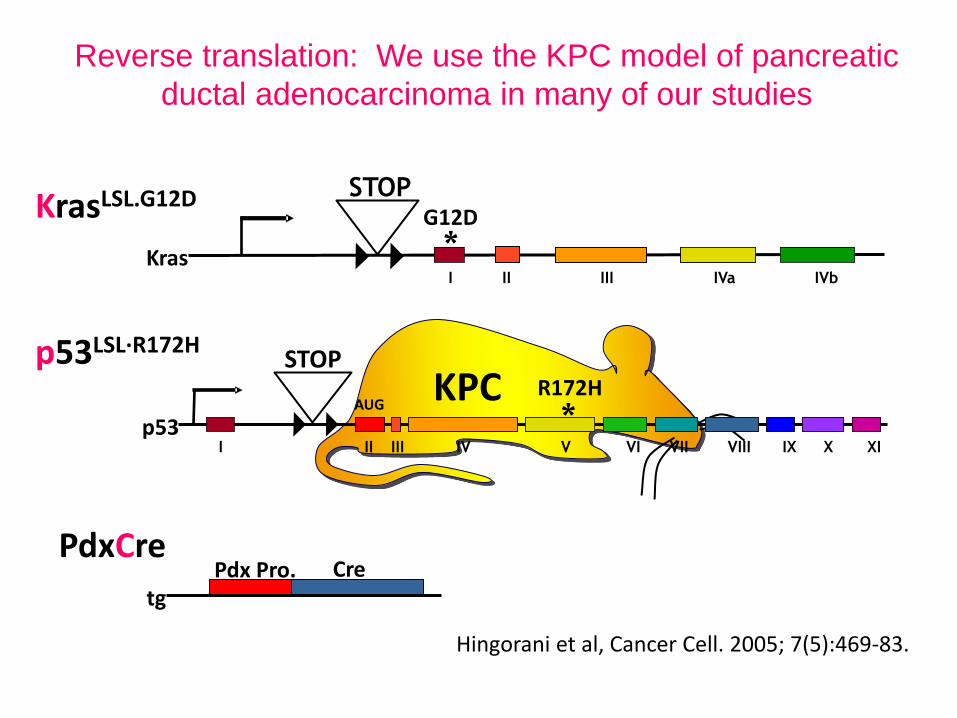
Reverse translation: We use the KPC model of pancreatic
ductal adenocarcinoma in many of our studies
KPC
KrasLSL.G12D
p53LSL·R172H
* R172H
II III IV V VI VII VIII IX XI X I
STOP
AUG
p53
PdxCre Pdx Pro. Cre
tg
II III IVa I
STOP
IVb
* Kras
G12D
Hingorani et al, Cancer Cell. 2005; 7(5):469-83.
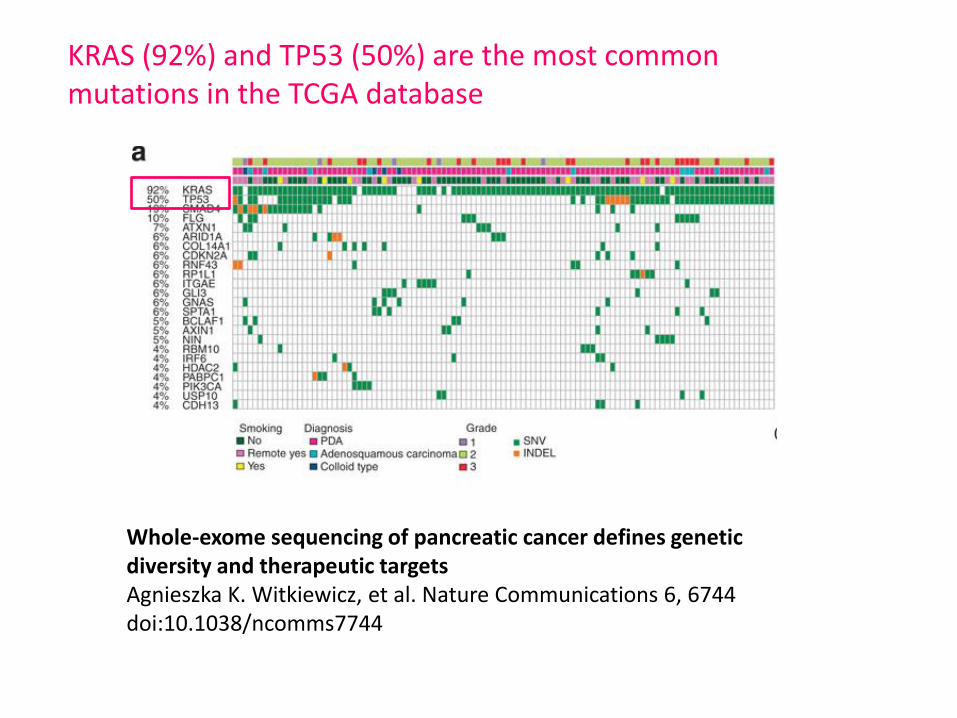
Whole-exome sequencing of pancreatic cancer defines genetic diversity and therapeutic targets Agnieszka K. Witkiewicz, et al. Nature Communications 6, 6744 doi:10.1038/ncomms7744
KRAS (92%) and TP53 (50%) are the most common mutations in the TCGA database
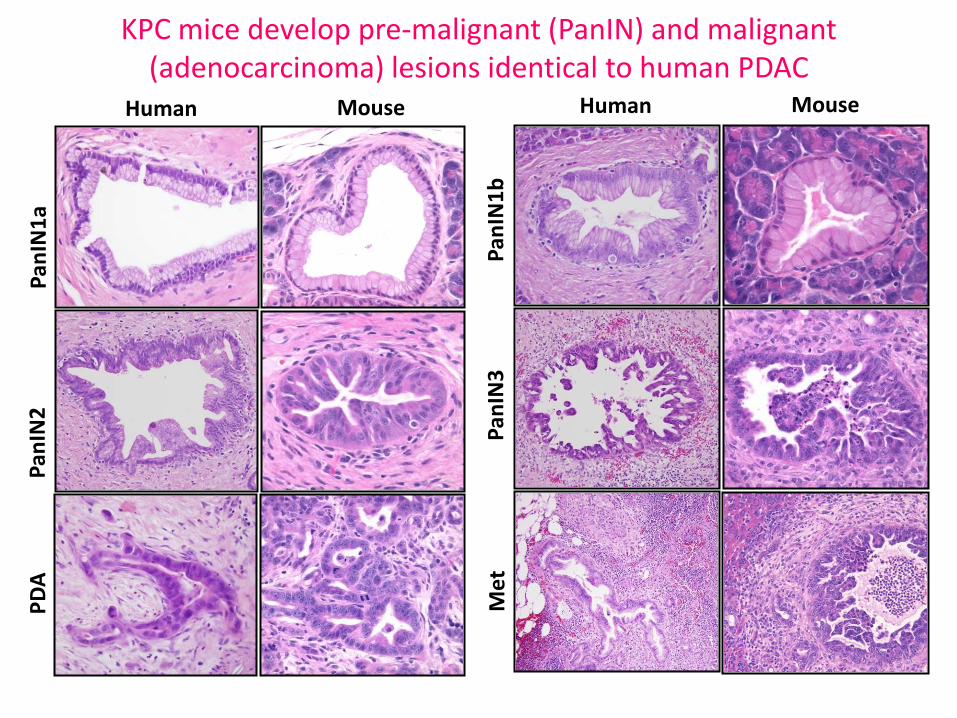
KPC mice develop pre-malignant (PanIN) and malignant (adenocarcinoma) lesions identical to human PDAC
Human Mouse Human Mouse
Pan
IN1
a P
anIN
2
PD
A
Pan
IN1
b
Pan
IN3
M
et
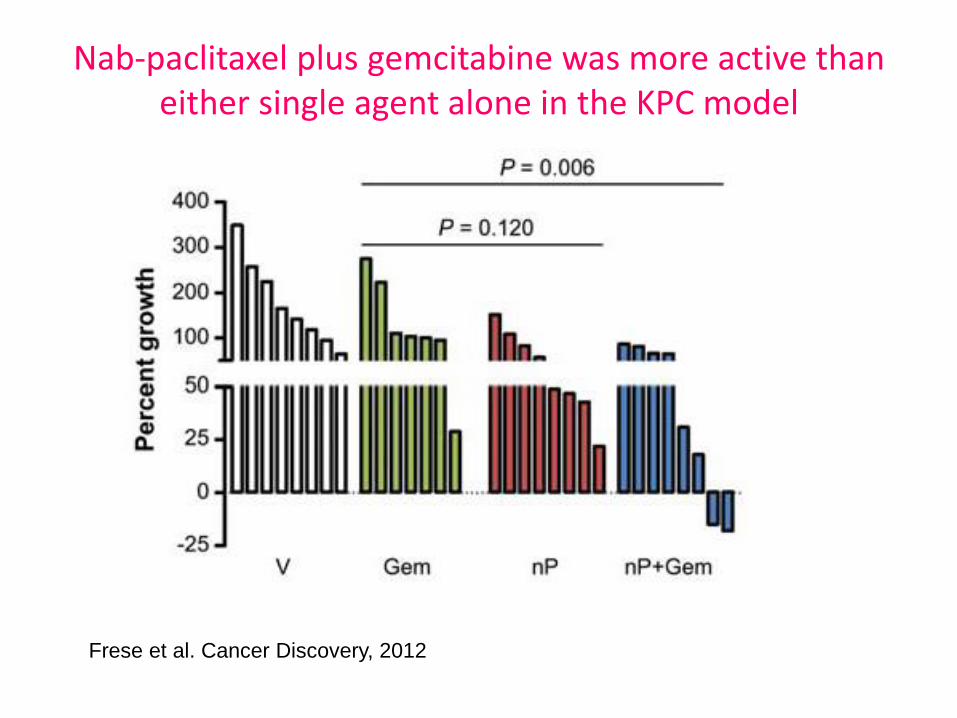
Nab-paclitaxel plus gemcitabine was more active than either single agent alone in the KPC model
Frese et al. Cancer Discovery, 2012
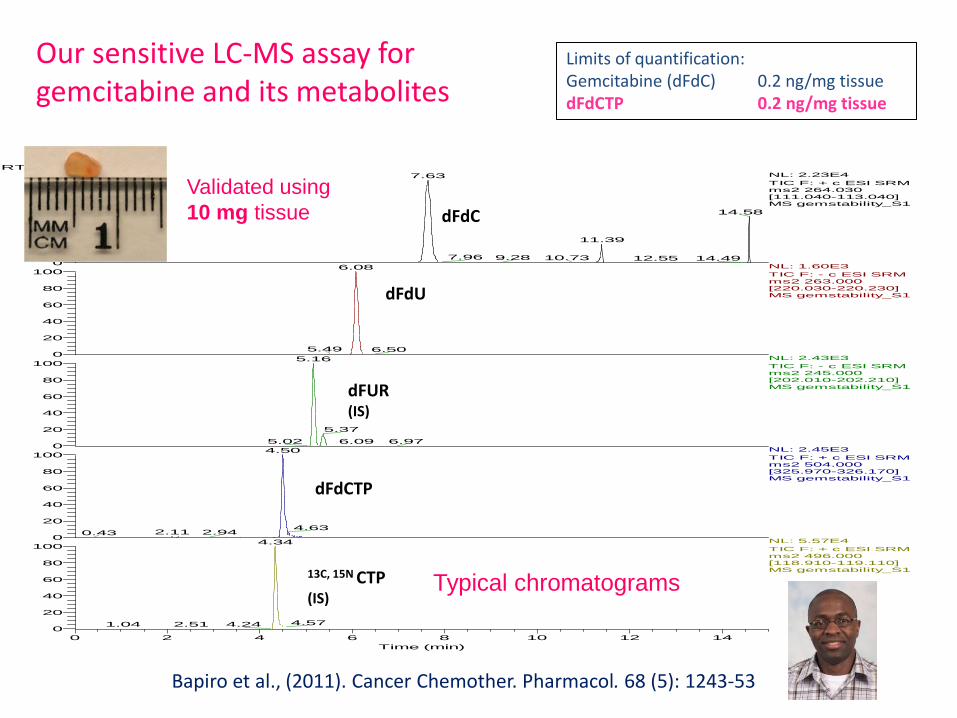
Typical chromatograms
RT: 0.00 - 15.00
0 2 4 6 8 10 12 14
Time (min)
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
Relativ
e Abun
dance
0
20
40
60
80
100
0
20
40
60
80
1007.63
14.58
11.39
7.96 9.28 10.73 12.55 14.49
6.08
5.49 6.50
5.16
5.37
5.02 6.09 6.97
4.50
4.632.11 2.940.43
4.34
4.574.242.511.04
NL: 2.23E4
TIC F: + c ESI SRM ms2 264.030 [111.040-113.040] MS gemstability_S1
NL: 1.60E3
TIC F: - c ESI SRM ms2 263.000 [220.030-220.230] MS gemstability_S1
NL: 2.43E3
TIC F: - c ESI SRM ms2 245.000 [202.010-202.210] MS gemstability_S1
NL: 2.45E3
TIC F: + c ESI SRM ms2 504.000 [325.970-326.170] MS gemstability_S1
NL: 5.57E4
TIC F: + c ESI SRM ms2 496.000 [118.910-119.110] MS gemstability_S1
dFdC
dFUR (IS)
dFdU
13C, 15N CTP (IS)
dFdCTP
Bapiro et al., (2011). Cancer Chemother. Pharmacol. 68 (5): 1243-53
Limits of quantification: Gemcitabine (dFdC) 0.2 ng/mg tissue dFdCTP 0.2 ng/mg tissue
Our sensitive LC-MS assay for gemcitabine and its metabolites
Validated using
10 mg tissue
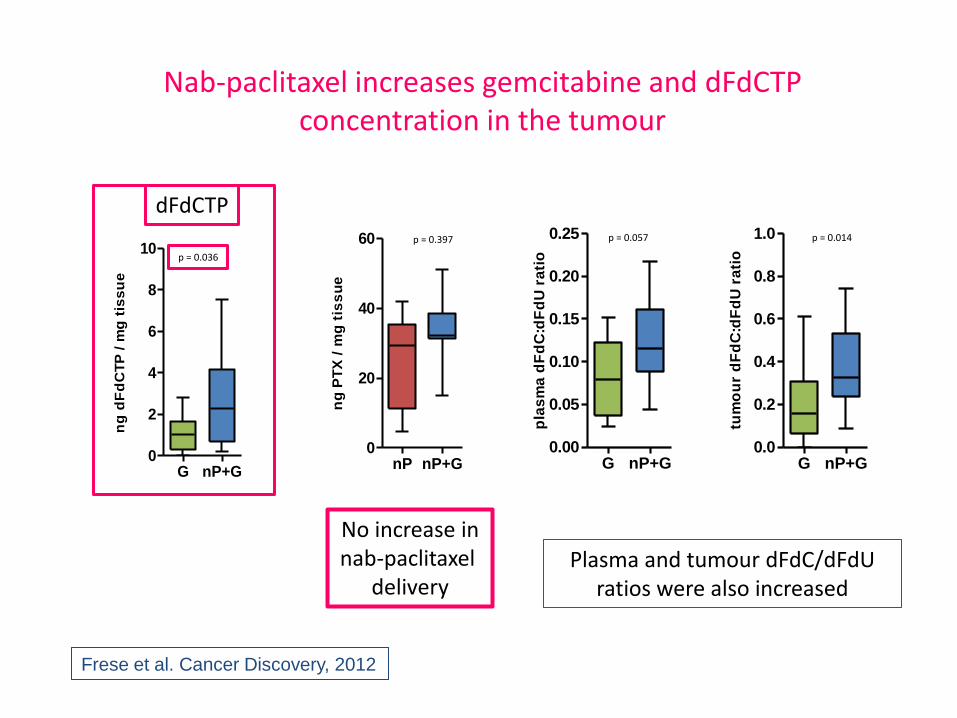
Nab-paclitaxel increases gemcitabine and dFdCTP concentration in the tumour
G nP+G0.00
0.05
0.10
0.15
0.20
0.25
pla
sm
a d
Fd
C:d
Fd
U r
ati
o
p = 0.057
G nP+G0.0
0.2
0.4
0.6
0.8
1.0
tum
ou
r d
Fd
C:d
Fd
U r
ati
o
p = 0.014
nP nP+G0
20
40
60
ng
PT
X /
mg
tis
su
e
p = 0.397
Plasma and tumour dFdC/dFdU ratios were also increased
G nP+G0
2
4
6
8
10
ng
dF
dC
TP
/ m
g t
iss
ue
p = 0.036
dFdCTP
No increase in nab-paclitaxel
delivery
Frese et al. Cancer Discovery, 2012
Gemcitabine nab-PTX + Gem Vehicle nab-PTX
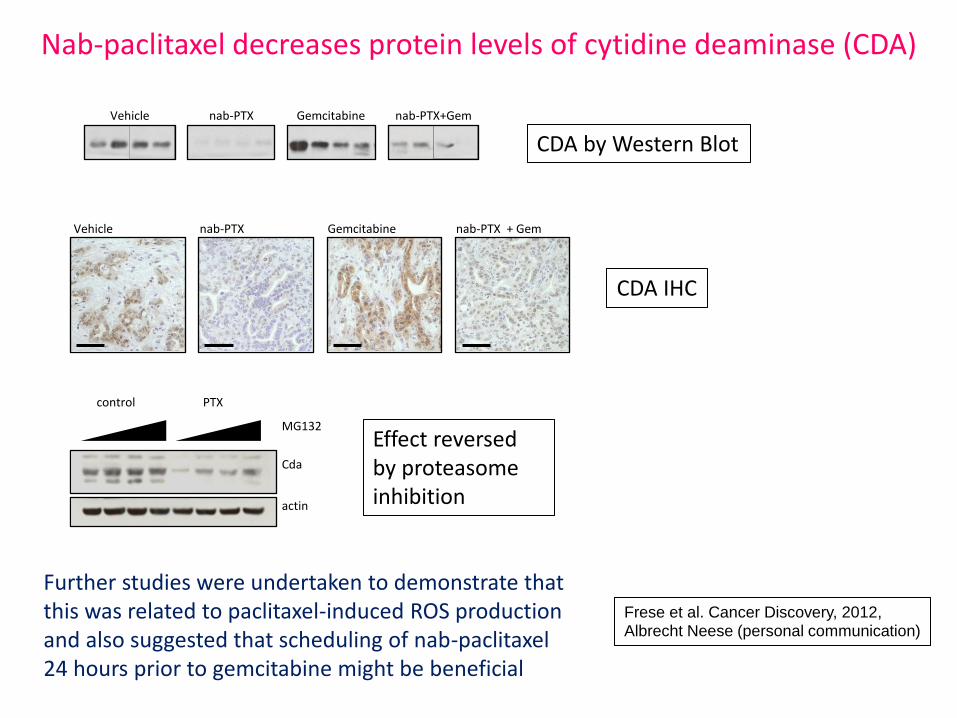
Nab-paclitaxel decreases protein levels of cytidine deaminase (CDA)
CDA by Western Blot
Vehicle nab-PTX Gemcitabine nab-PTX+Gem
control PTX
Cda
actin
MG132
Further studies were undertaken to demonstrate that this was related to paclitaxel-induced ROS production and also suggested that scheduling of nab-paclitaxel 24 hours prior to gemcitabine might be beneficial
CDA IHC
Effect reversed by proteasome inhibition
Frese et al. Cancer Discovery, 2012, Albrecht Neese (personal communication)
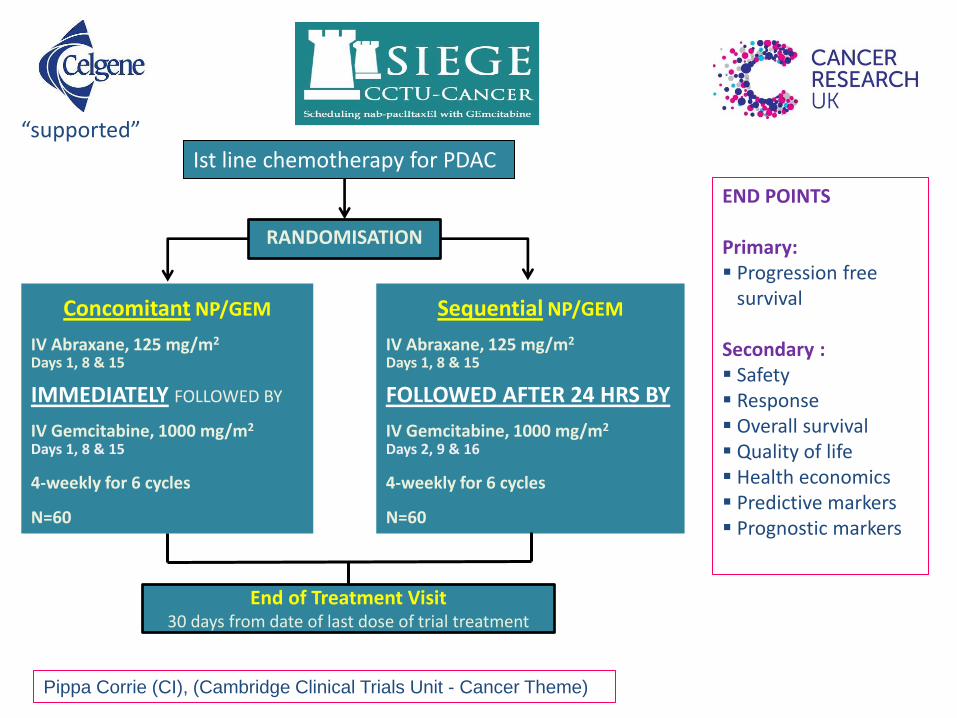
END POINTS
Primary: Progression free survival Secondary : Safety Response Overall survival Quality of life Health economics Predictive markers Prognostic markers
Pippa Corrie (CI), (Cambridge Clinical Trials Unit - Cancer Theme)
RANDOMISATION
Concomitant NP/GEM
IV Abraxane, 125 mg/m2
Days 1, 8 & 15 IMMEDIATELY FOLLOWED BY IV Gemcitabine, 1000 mg/m2
Days 1, 8 & 15 4-weekly for 6 cycles N=60
Sequential NP/GEM
IV Abraxane, 125 mg/m2
Days 1, 8 & 15 FOLLOWED AFTER 24 HRS BY IV Gemcitabine, 1000 mg/m2
Days 2, 9 & 16 4-weekly for 6 cycles N=60
End of Treatment Visit 30 days from date of last dose of trial treatment
“supported”
Ist line chemotherapy for PDAC
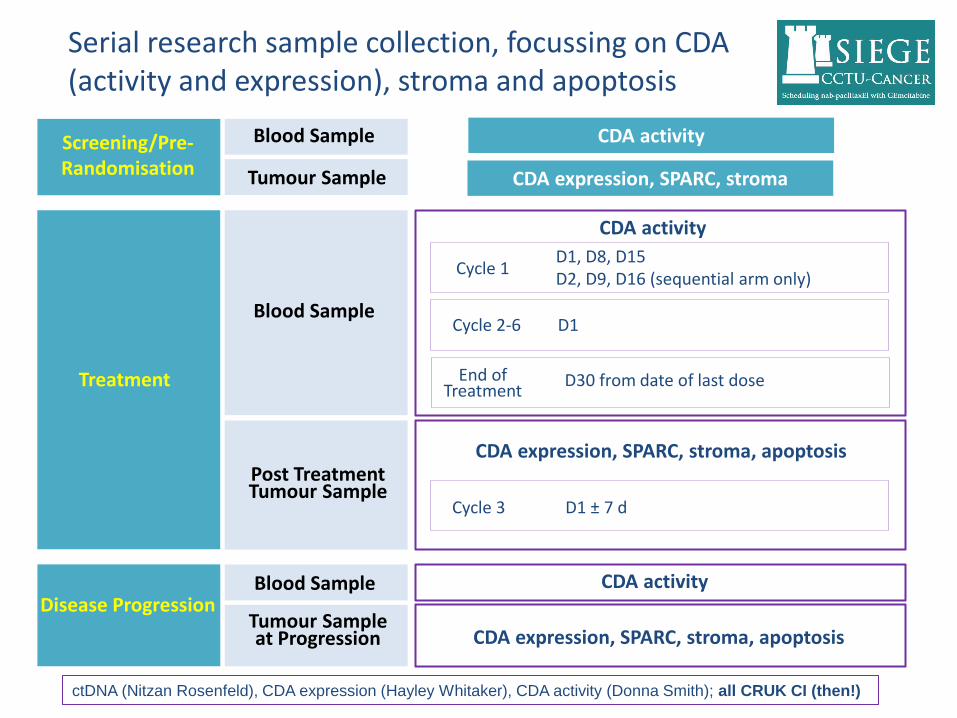
Serial research sample collection, focussing on CDA (activity and expression), stroma and apoptosis
Screening/Pre-Randomisation
Blood Sample
Tumour Sample
CDA activity
CDA expression, SPARC, stroma
Disease Progression
CDA expression, SPARC, stroma, apoptosis
Blood Sample
Tumour Sample at Progression
CDA activity
Treatment
Blood Sample
Post Treatment Tumour Sample
CDA activity
CDA expression, SPARC, stroma, apoptosis
Cycle 1 D1, D8, D15 D2, D9, D16 (sequential arm only)
Cycle 2-6 D1
End of Treatment
D30 from date of last dose
Cycle 3 D1 ± 7 d
ctDNA (Nitzan Rosenfeld), CDA expression (Hayley Whitaker), CDA activity (Donna Smith); all CRUK CI (then!)

What about immunotherapy?
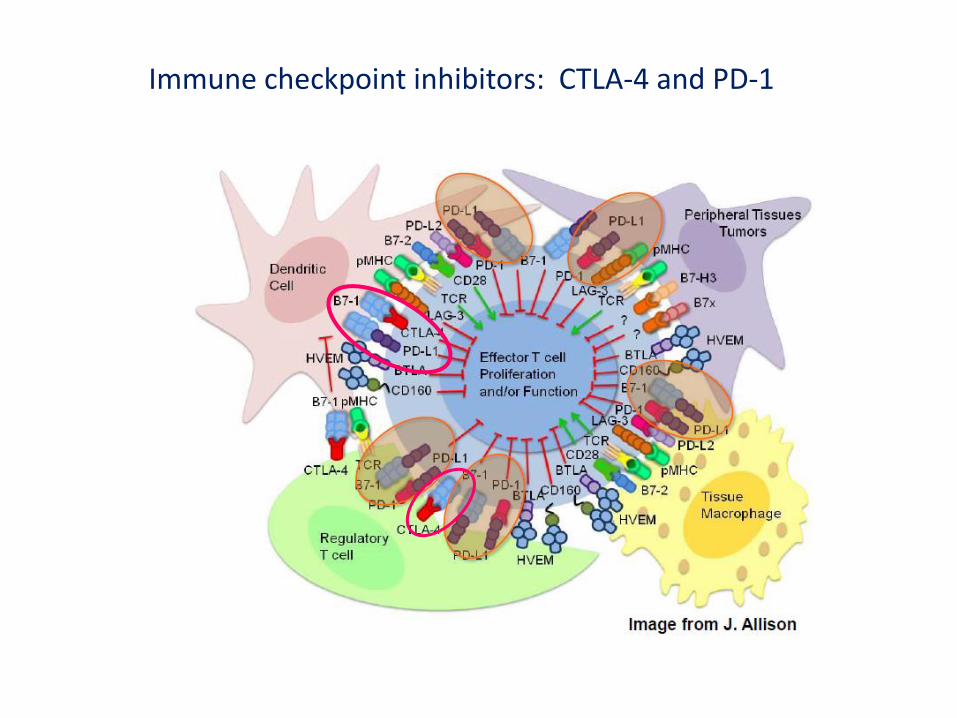
Immune checkpoint inhibitors: CTLA-4 and PD-1
Anti PD-1 antibody therapy
• Nivolumab (anti PD-1) acts as an immunomodulator, by blocking ligand activation of the programmed cell death 1 (PD-1) receptor on activated T cells.
• Common adverse events with nivolumab included fatigue, rash, diarrhea, decreased appetite, nausea, and pruritus.
• Grade 3-4 toxicity occurred in 41 of 296 patients (14%), with 3 deaths attributed to treatment-related pneumonitis.
• Multiple phase III clinical trials are being performed (e.g. kidney, lung and melanoma)
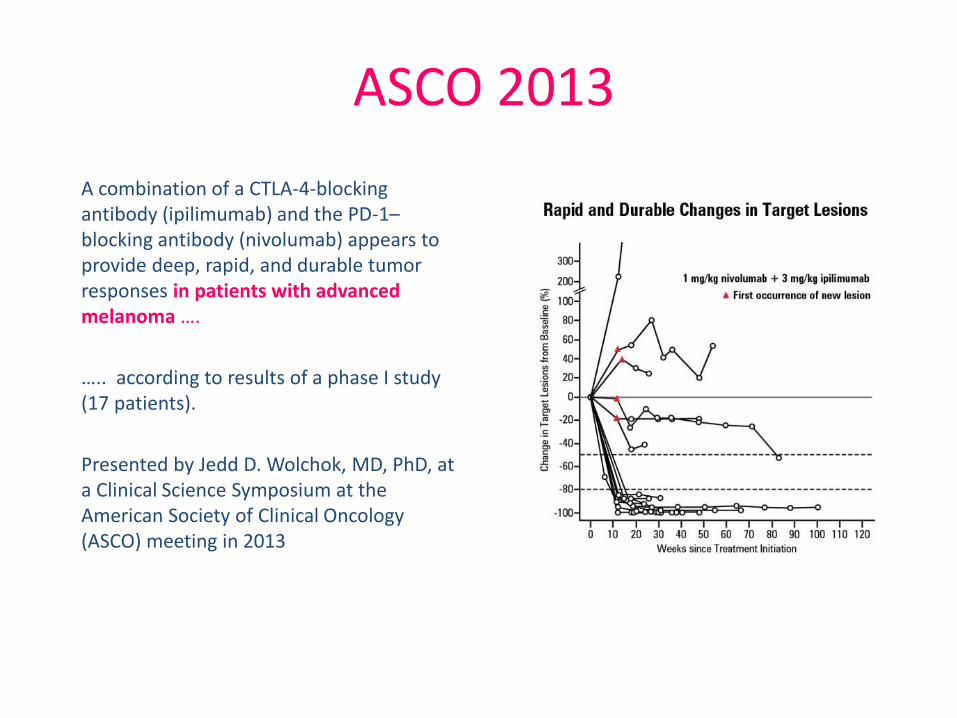
ASCO 2013
A combination of a CTLA-4-blocking antibody (ipilimumab) and the PD-1–blocking antibody (nivolumab) appears to provide deep, rapid, and durable tumor responses in patients with advanced melanoma ….
….. according to results of a phase I study (17 patients).
Presented by Jedd D. Wolchok, MD, PhD, at a Clinical Science Symposium at the American Society of Clinical Oncology (ASCO) meeting in 2013
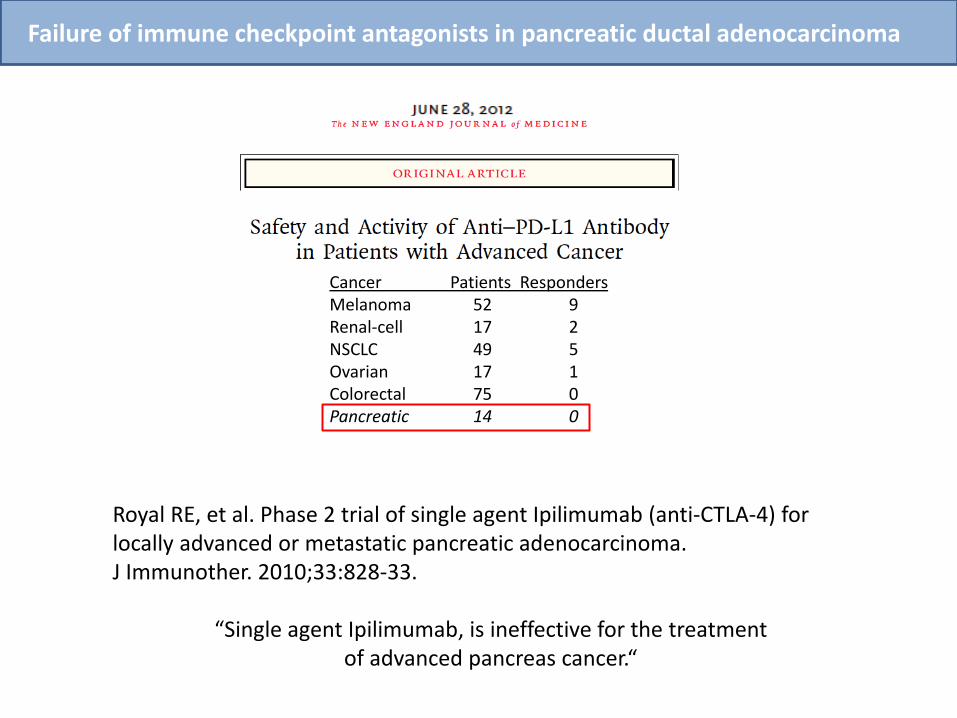
Royal RE, et al. Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locally advanced or metastatic pancreatic adenocarcinoma. J Immunother. 2010;33:828-33.
“Single agent Ipilimumab, is ineffective for the treatment of advanced pancreas cancer.“
Failure of immune checkpoint antagonists in pancreatic ductal adenocarcinoma
Cancer Patients Responders Melanoma 52 9 Renal-cell 17 2 NSCLC 49 5 Ovarian 17 1 Colorectal 75 0 Pancreatic 14 0
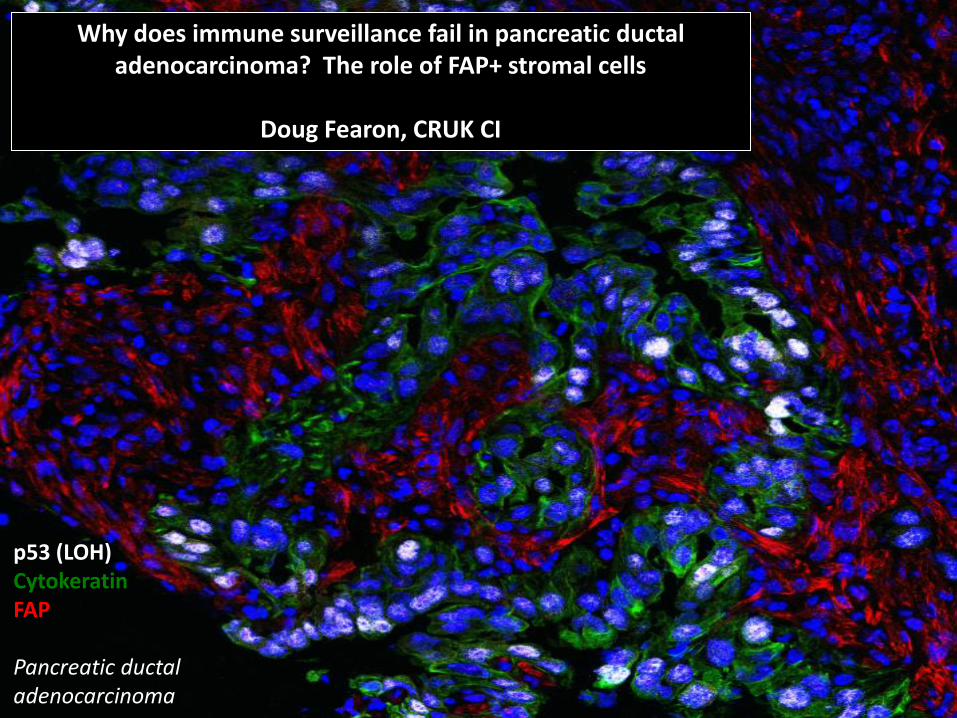
Why does immune surveillance fail in pancreatic ductal adenocarcinoma? The role of FAP+ stromal cells
Doug Fearon, CRUK CI
p53 (LOH) Cytokeratin FAP Pancreatic ductal adenocarcinoma
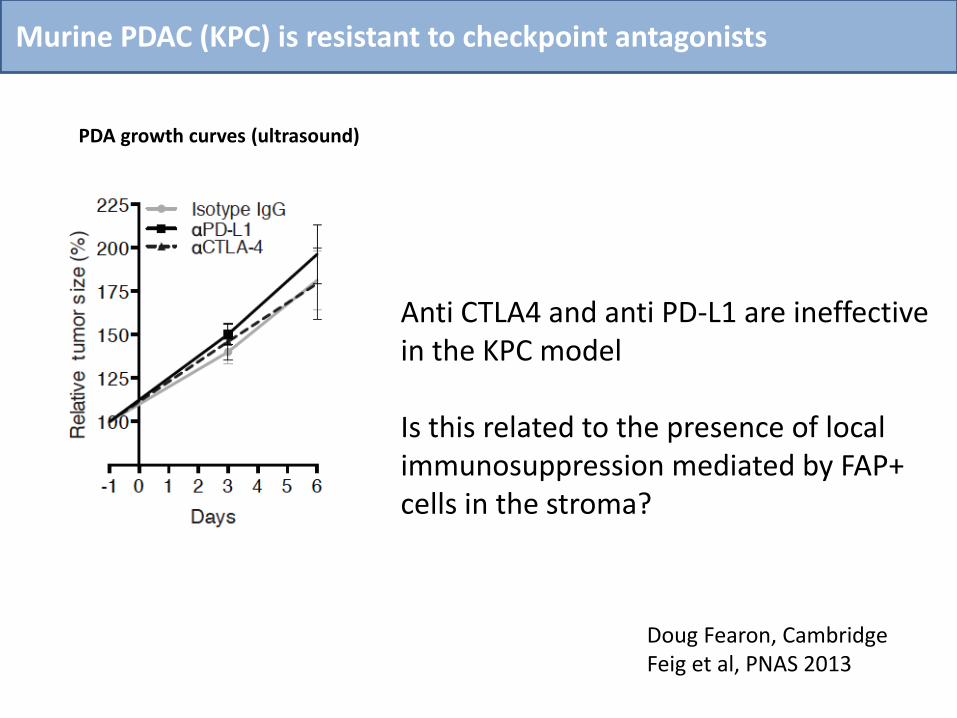
Murine PDAC (KPC) is resistant to checkpoint antagonists
Anti CTLA4 and anti PD-L1 are ineffective in the KPC model
Is this related to the presence of local immunosuppression mediated by FAP+ cells in the stroma?
PDA growth curves (ultrasound)
Doug Fearon, Cambridge Feig et al, PNAS 2013
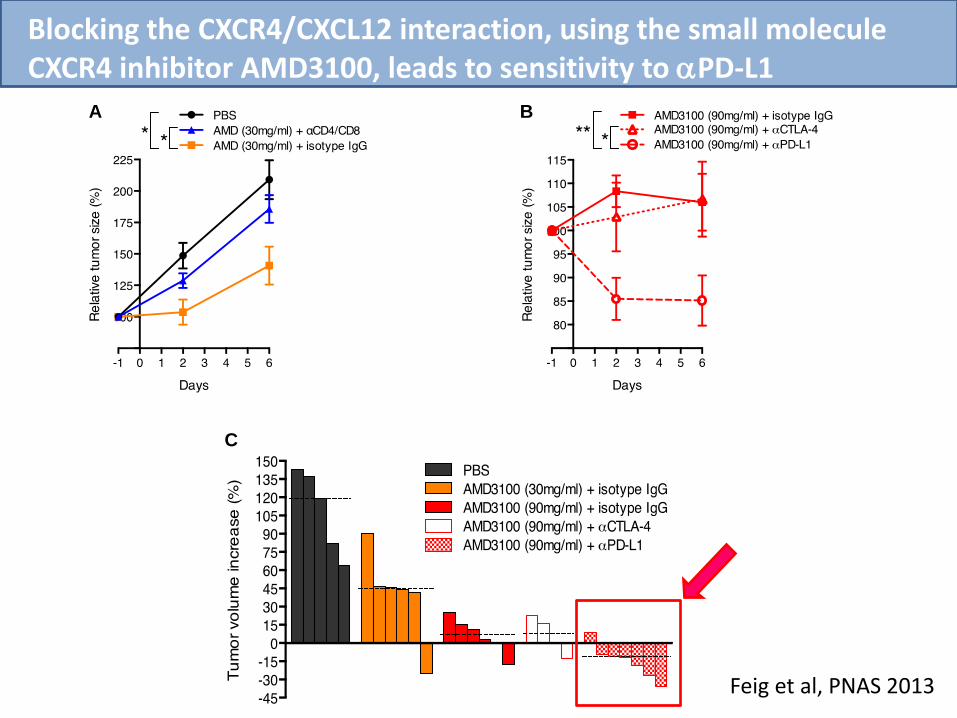
A B
C
Blocking the CXCR4/CXCL12 interaction, using the small molecule CXCR4 inhibitor AMD3100, leads to sensitivity to aPD-L1
Feig et al, PNAS 2013
Single agent Phase I trial: CXCR4 antagonism with AMD3100 (plerixafor,
MobizilTM), administered to patients with histologically confirmed, incurable
PDAC and other cancers.
Started trial #1 in Q3 2015. 8 patients treated to date.
Combination Phase I trial: AMD3100 administered in combination with anti-
PD1 or anti-PD-L1 antibody in the same population
The studies will assess safety, as well as aiming to demonstrate the proof of
mechanism in patients by documenting alterations in T-cell tumour distribution,
ideally associated with tumour cell killing (loss of p53 positive tumour cells) and
reduction in FDG-PET uptake.
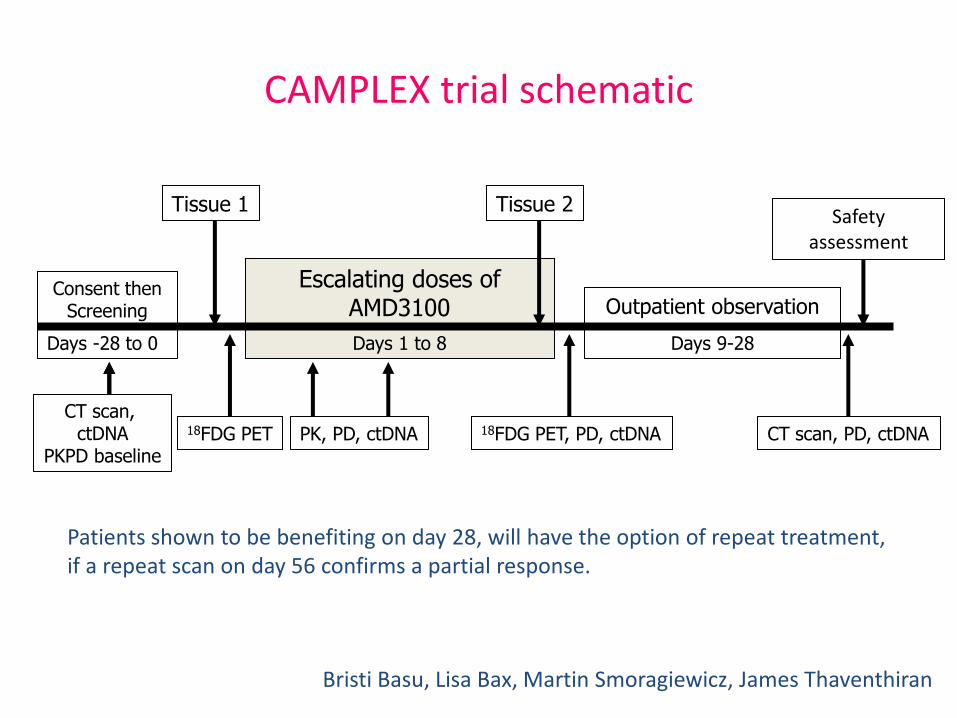
Tissue 1 Tissue 2
Escalating doses of AMD3100
18FDG PET 18FDG PET, PD, ctDNA
Consent then Screening
Days 1 to 8 Days -28 to 0
CT scan, ctDNA
PKPD baseline CT scan, PD, ctDNA
Outpatient observation
Days 9-28
Safety assessment
PK, PD, ctDNA
Patients shown to be benefiting on day 28, will have the option of repeat treatment, if a repeat scan on day 56 confirms a partial response.
CAMPLEX trial schematic
Bristi Basu, Lisa Bax, Martin Smoragiewicz, James Thaventhiran
Am I going too fast?
No animals were harmed in the making of this slide
Personalised medicine
Precision medicine
Individualised therapy

Founding members of
PRECISION-PANC
3 CRUK Major Centres
2 CRUK Centres focussing on PDAC
NCRI Studies Group
CRUK
Major Pharma
BOTH laboratory research
and clinical trials
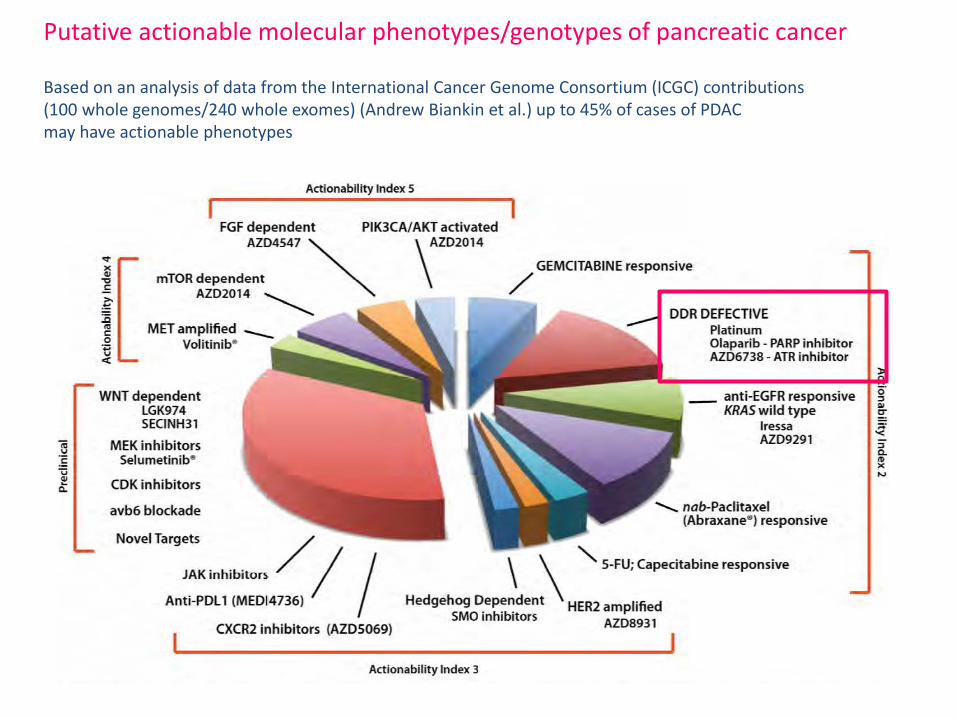
Putative actionable molecular phenotypes/genotypes of pancreatic cancer Based on an analysis of data from the International Cancer Genome Consortium (ICGC) contributions (100 whole genomes/240 whole exomes) (Andrew Biankin et al.) up to 45% of cases of PDAC may have actionable phenotypes
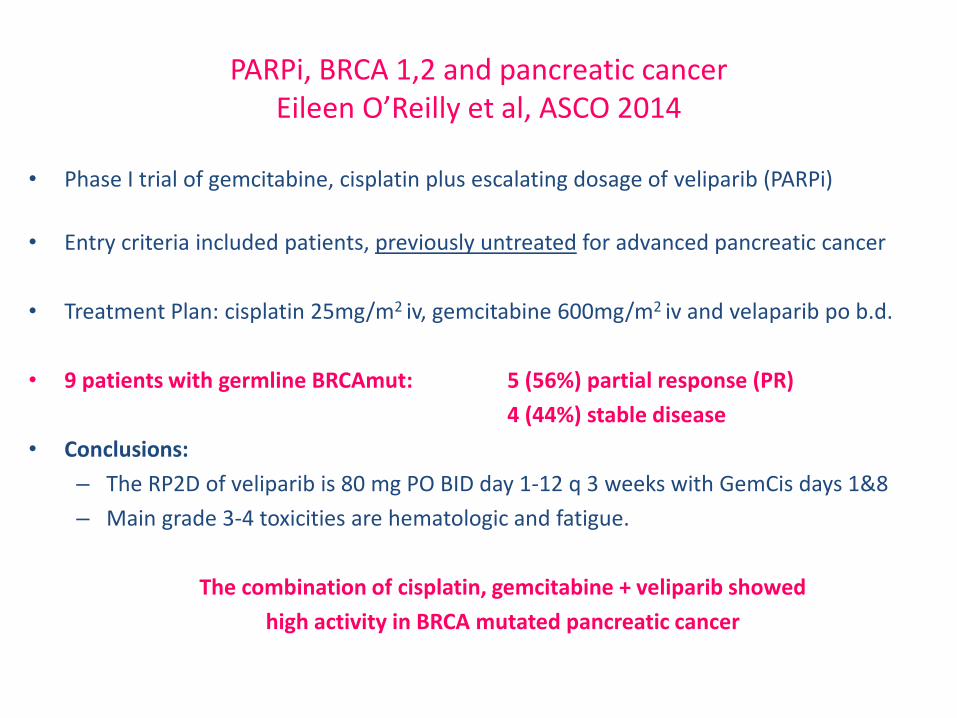
PARPi, BRCA 1,2 and pancreatic cancer Eileen O’Reilly et al, ASCO 2014
• Phase I trial of gemcitabine, cisplatin plus escalating dosage of veliparib (PARPi)
• Entry criteria included patients, previously untreated for advanced pancreatic cancer
• Treatment Plan: cisplatin 25mg/m2 iv, gemcitabine 600mg/m2 iv and velaparib po b.d.
• 9 patients with germline BRCAmut: 5 (56%) partial response (PR)
4 (44%) stable disease
• Conclusions:
– The RP2D of veliparib is 80 mg PO BID day 1-12 q 3 weeks with GemCis days 1&8
– Main grade 3-4 toxicities are hematologic and fatigue.
The combination of cisplatin, gemcitabine + veliparib showed
high activity in BRCA mutated pancreatic cancer
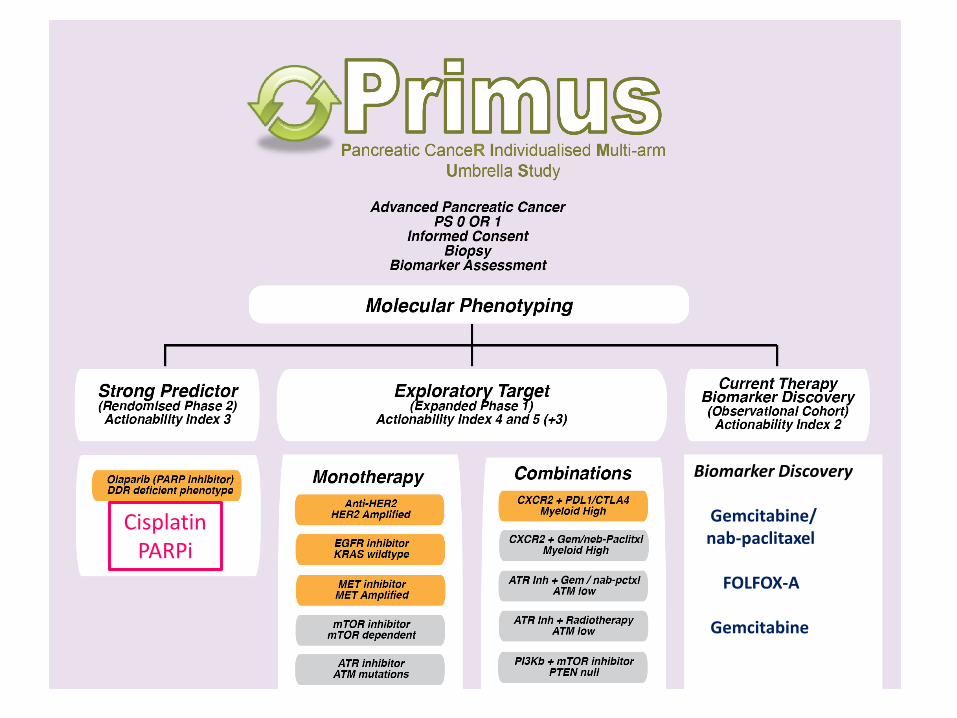
Biomarker Discovery Gemcitabine/ nab-paclitaxel FOLFOX-A Gemcitabine
Cisplatin PARPi

PDDG
Frances Richards
Tashinga Bapiro
Jo Bramhall
Jenny Harrington
Aarthi Gopinathan
Siang Boon Koh
Séverine Mollard
Graham Mills
Tobias Janowitz
Yann Wallez
James Thaventhiran
(Immunology, CIMR)
Dave Tuveson
Natalie Cook
Kris Freese
Albrecht Neesse
Christine Feig
Doug Fearon
James Jones
Matt Kraman
Richard Wells
Derek Chan
Claire Connell
Thomas Flint
Cambridge Pancreatic Cancer Centre, Clinical and Research staff: Raaj Praseedom, Pippa Corrie, Bristi Basu, Neville Jamieson, Asif Jah, Simon Harper, Emmanuel
Huguet, Nicholas Carroll, Rebecca Brais, Martina Lofthouse, Debbie Pitfield, Joanna Calder, Lisa Bax,
Katy Dalchau, Burcu Babaoglan, Alkida Bucaj
CRUK Cambridge Institute
Core Facilities
PK/Bioanalysis: Donna-Michelle
BRU and TMC
Microscopy
Histopathology
Genomics
….. and our patient volunteers.