
Comprehensive preoperative assessment of pancreatic carcinoma Dr. Muhammad Bin Zulfiqar
Upload
jibran-mohsinCategory
view
705download
1
Pancreatic Carcinoma
Jibran Mohsin
Resident, Surgical Unit I
SIMS/Services Hospital Lahore

Outline
• Introduction• Pathophysiology• Etiology• Epidemiology• Clinical Presentation• Workup• Staging • Treatment• Prognosis

Introduction
• Worldwide, ranks 13th in incidence
• BUT 8th as a cause of cancer death
• Worst prognosis of all malignancies
DISTRIBUTION
• Head(Periampullary) or Neck 66-75 %
• Body 15-20%
• Tail 5-10 %

Introduction
Classification of Pancreatic Tumors
Parenchymal
Exocrine tumors
Endocrine tumors
Stromal

Introduction
Classification of Pancreatic Tumors• Exocrine (95%)Tumors-WHO classification
– Benign• Serous cystadenoma• Mucinous cystadenoma• Intraductal papillary-mucinous adenoma• Mature cystic teratoma
– Borderline• Mucinous cystic tumor with moderate dysplasia• Intraductal papillary mucinous tumor with moderate dysplasia• Solid pseudopapillary tumor
– Malignant• Ductal Adenicarcinoma (75-80% of all exocrine tumor)• Serous/mucinous cystadenoma• Intraductal mucinous papillary tumor

Introduction
Classification of Pancreatic Tumors
• Endocrine Tumors
• Primary Connective tissue cancers– Lymphomas
Endocrine Tumor Source Clinical Presentation
Insulinoma Beta cells Whipple’s triad
Gastrinoma G cells Peptic ulcer
Glucagonoma Alpha cells Diabetes, Necrolytic Migratory erythema
Vipoma-Pancreatic Cholera(Verner Morrison Syndrome)
Watery DiarrheaHypokalemia
Achlorhydria ( WDHA syndrome)
Somatostatinoma Delta/S cells Diabetes, Steatorrhea, Gallstones

Introduction
Periampullary Carcinoma
Type of Carcinoma Frequency
Adenocarcinoma of head of pancreas 50 %
Tumor from ampulla of vater 30%
Distal bile duct carcinoma 10%
Duodenal carcinoma adjacent to ampulla 10%

Pathophysiology

Pathophysiology
SPREAD• Typically, metastasizes to regional lymph nodes, then to liver and
less commonly to lungs
• Also directly invade surrounding viscera– Duodenum, stomach, and colon
• Metastasize to any surface in abdominal cavity via peritoneal spread ( ascites- ominous prognosis)
• Spread to skin as painful nodules
• Metastasis to bone is uncommon
• Rare spread to brain but can produce meningeal carcinomatosis
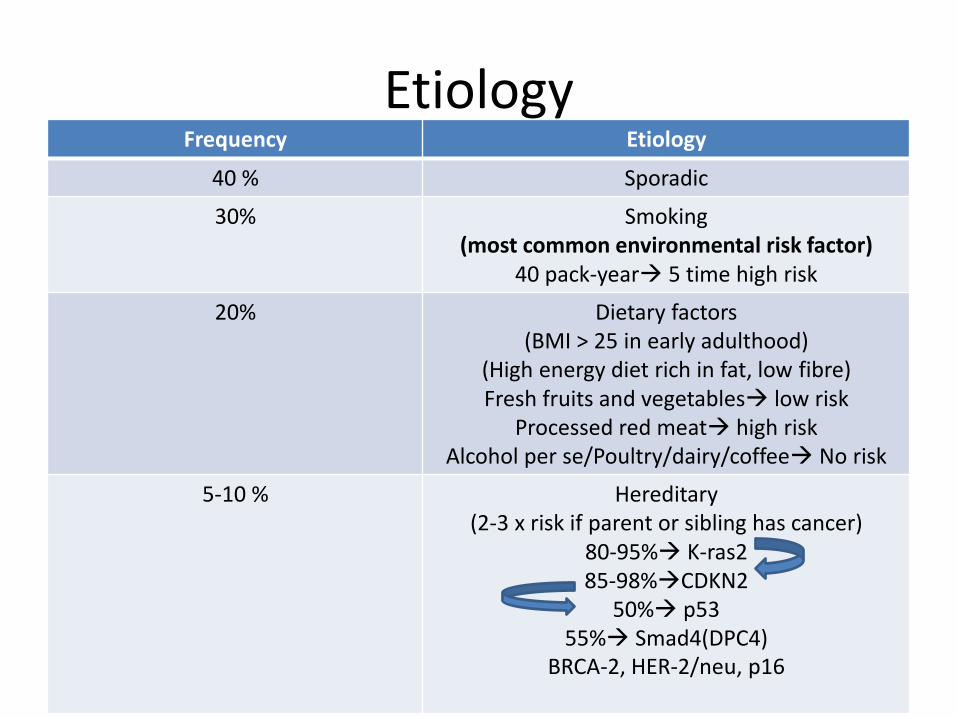
EtiologyFrequency Etiology
40 % Sporadic
30% Smoking(most common environmental risk factor)
40 pack-year 5 time high risk
20% Dietary factors(BMI > 25 in early adulthood)
(High energy diet rich in fat, low fibre)Fresh fruits and vegetables low risk
Processed red meat high riskAlcohol per se/Poultry/dairy/coffee No risk
5-10 % Hereditary(2-3 x risk if parent or sibling has cancer)
80-95% K-ras285-98%CDKN2
50% p5355% Smad4(DPC4)
BRCA-2, HER-2/neu, p16

Etiology
• Diabetes– DM of 5 year duration 2 fold high risk
• Chronic Pancreatitis– 26 fold high risk– Of 20 year duration 4 % cases develop Pancreatic CA
• Hereditary Pancreatitis– Mutation in PRSS1 gene– 50 fold high risk– 40 % develop CA by age of 70

EtiologyASSOCIATIONS
• Peutz Jegher syndrome
• Multiple endocrine neoplasia(MEN I)
• Hereditary Nonpolyposis Colonic Cancer(HNPCC)-controversial-MSH2/MLH1 gene
• Familial Adenomatous Polyposis(FAP)- APC gene
• Gardner Syndrome
• Familial atypical multiple mole melanoma syndrome (FAMMM)-CDKN2A gene
• Von Hippel-Lindau (VHL) syndrome-VHL tumor suppressor gene
• Ataxia telangiectasia
• Hereditary breast(BRCA 2> BRCA 1) and ovarian cancers

Epidemiology
INCIDENCE
• Worldwide8-12 cases per 100, 000 persons per year

Epidemiology
RACE
• Highest incidence African American males
GEOGRAPHICAL
• High in Native Hawaiian males, men of korean, Czech, Latvian and New zealand Maori
ancestry

Epidemiology
GENDER
Male > Female
AGE
Median age at diagnosis in whites 69 years
Median age at diagnosis in blacks 65 years
Mean 60-65 years

Clinical Presentation
• Early clinical diagnosis difficult due to nonspecific symptoms and subtle in onset
• Typically present as gradual onset of nonspecific symptoms such as anorexia, malaise, nausea, fatigue, and midepigastric or back pain
• Significant weight loss characteristic feature
LOCATION CLINICAL PRESENTATION
HEAD(peri ampullary) and NECK Weight loss and Painless Obstructive jaundice
BODY and TAIL Weight loss, PAIN and Mass

Clinical Presentation
MIDEPIGASTRIC PAIN– can be in RHC/LHC depending on location of tumor– Most common presenting symptom– Mild-moderate(1/3rd cases) –severe(1/3rd cases)– Unrelenting in nature– More at night– Increased by food intake and lying flat– Often but always radiating to midback or lower-back
• Indicates invasion of retroperitoneal splanchnic nerve plexus OR
• Pancreatic duct obstruction/stasis OR• Disruption of nerve sheath

Clinical Presentation
WEIGHT LOSS• Cancer-associated anorexia
• Subclinical malabsorption from pancreatic exocrine insufficiency caused by pancreatic duct obstruction– Diarrhea, Steatorrhoea
• Nausea and early satiety from GOO and delayed gastric emptying

Clinical Presentation
(PAINLESS*) OBSTRUCTIVE JAUNDICE• Most characteristic sign of CA head of pancreas• Get medical attention before tumor size enlarges to cause pain
• Short duration, severe, progressive• Intermittent if necrosis of tumor occurs• preceded by pruritis-skin bile salt deposition
– Scratch marks
• Acholic/clay colored stools• Tea colored/Darkening of urine_______________________________________________________________
*To distinguish it from choledcholithiasis BUT this aphorism is not accurate
Clinical Presentation
OTHERS• Depression
– More common in pancreatic cancer than other abdominal tumors
– 11 times increase risk of suicide especially early postoperative period
• Migratory thrombophlebitis– Trousseau sign of malignancy OR– Trousseau syndrome– Seen in 10 % cases– Due to release of PAF(Platelet aggregating
factors) from tumor or its necrotic material
Trousseau himself died of CA pancreas who had migratory thrombophlebitis

Trousseau syndrome
(Migratory thrombophlebitis)

Clinical Presentation
OTHERS
• Venous thrombosis
• Marantic endocarditis
• New onset of diabetes within 1 year in old age
• 1st episode of acute pancreatitis in old age

……………………..
Rule out Pancreatic Cancer in patient older than 60 years
with NEW diagnosis of DM or increase in insulin reqirement in
pre existind diabetes and without any other diabetic risk
factors

……………………………………
Rule out pancreatic cancer in an elderly patient presenting for
1st time with acute pancreatitis without any known
precipitating factors

Clinical Presentation-Examination
• Epigastric Mass– Non mobile, smooth, soft/hard, (non)tender, not moving
with respiration
• Palpable gallbladder(+clinical jaundice)– i.e. Courvoisier sign– Nontender, soft globular, smooth, moving with respiration,
mobile horizontally, dull on percussion– 25-30 % cases of CA head of pancreas– 50 % cases of periampullary CA
• Ascites– Shifting dullness and fluid thrill

Clinical Presentation
• Hepatomegaly– Enlarged+ smooth, firm and nontender
Hydrohepatosis• Dilated bilairy channels
– Multiple hard nodulesMets
• Splenomegaly– due to portal/splenic vein thrombosis
– Seen in 10 % cases

Clinical Presentation
• Sister Mary Joseph nodule(s)/node/sign– Subcutaneous metastases– Paraumbilical region– Signifies advanced disease– spread of cancer cells to the umbilicus include
• direct transperitoneal spread, • via the lymphatics which run alongside the obliterated umbilical vein• hematogenous spread, or • via remnant structures such as the faclciform ligament, median umbilical ligament, or a
remnant of the vitelline duct.
• Mass in rectovesical pouch(Blumer’s Shelf)– Metastatic mass, palpable on DRE
*Sister Mary Joseph Dempsey was the surgical assistant of William J. Mayo at St. Mary’s Hospital n Rochester, Minnesota from 1890 to 1915. She drew Mayo's
attention to the phenomenon, and he published an article about it in 1928. The eponymous term Sister Mary Joseph nodule was coined in 1949 by Hamilton
Bailey.

Clinical Presentation
• Virchow’s node*(or Signal node)– Called Troisier’s sign**– Left supraclavicular palpable lymph node– Behind the medial end of left clavicle
Right: Charles Émile TroisierLeft:Rudolf Carl Virchow
* Rudolf Virchow(1821–1902), the German pathologist who first described the gland and its association with gastric
cancer in 1848. **TheFrench pathologist Charles Emile Troisier noted in 1889 that other abdominal cancers, too, could spread to the node.

Clinical Presentation
Sister Mary Joseph nodule Virchow/signal node

Differential diagnosis
• Retroperitoneal masss/tumor/LN
• Advanced adherent CA stomach
• Advanced CA transverse colon
• CBD stone
• Bile duct stricture
• LN compressing CBD
• Cholangiocarcinoma of CBD
• Chronic pancreatitis

Workup
• Hematological Investigations
• Serological Investigations
• Radiological Investigations
• Histopathological investigation

Hematological Investigations
• CBC– Anemia of chronic disease– Thrombocytosis
• Liver Function Test– Raised total/conjugated (van den Bergh’s test)bilirubin– Raised ALP/GGTP– Low albumin and altered PT/INR
• Serum amylase/lipase*– Raised in < 50 % cases of resectable tumor v/s– 25 % cases of irresectable tumor
*5% cases present initially with acute pancreatitis

Serological Investigations
• Carbohydrate Antigen(CA) 19-9 (<33-37 U/mL)– Sialylated oligosaccharide most commonly found on circulating
mucins in cancer patients
– Also normally produced within cells of biliary tract• Can be elevated in 10% cases of benign diseases of pancreas, liver and
bile ducts
– Elevated in 75-85 % cases of pancreatic CA• 5-10 % patients lack CA 19-9 producing enzyme
– In absence of biliary obstruction, intrinsic liver disease, or benign pancreatic disease, value> 100 U/mL highly specific for malignancy especially pancreatic

Serological Investigations
• Carbohydrate Antigen(CA) 19-9 – Used along with imaging studies to determine
resectability potential• <4% cases with CA 19-9 > 300 U/mL have resectable
tumors
– Demerit:• Least sensitive for small, early stage pancreatic
carcinomas i.e. not effective as screening tool or early detection– 0.2 % positive results in asymptomatic cases
– 4.3 % positive in early symptomatic cases

Serological Investigations
• Carbohydrate Antigen(CA) 19-9
– Used in staging and follow up
• Case with <100 U/mL unlikely to have occult metastatic disease and may not need staging lapsroscopy prior to resection
• Surrogate marker for clinical response to therapy
• Preoperative >50 U/mL associated with higher chances of recurrence

Serological Investigations
• Carcinoembryonic antigen(CEA)
– High molecular weight glycoprotein found normally in fetal tissues
– Elevated in only 40-45 % of cases of pancreatic CA
– NOT sensitive or specific for pancreatic CA
• As it is also elevated in others benign and malignant conditions
Sensitivity Specificity
CA 19-9 NO YES
CEA NO NO

Radiological InvestigationsComputed Tomography Scan
• Mainstay of initial diagnostic modalities used for assessing patients suspected to have pancreatic carcinoma
• Triple-phase spiral/3D CT scan 90 % accurate in determining resectability potential (as accurate as EUS)
• To detect size, extent, nodal status , portal vein involvement
• More accurate than EUS in predicting involvement of SMA
• Malignant tumors appear as lower density lesions
• CT guided FNA can also be done• Demerit:
– Small tumors still be missed even with most advanced CT scanning

CT scan findings suggestive of unresecatable disease
• Invasion of hepatic artery or SMA
• Enlarged LN outside boundaries of resection
• Ascites
• Distant metastases

CT scan showing a pancreatic adenocarcinoma
• Gallbladder (gb) is distended because of biliary obstruction. The superior mesenteric artery (sma) is surrounded by tumor, making this an unresectable T4 lesion.
• 2-cm pancreatic adenocarcinoma (mass) causing obstruction of both the common bile duct (cbd) and pancreatic duct (pd).

Radiological InvestigationsTranscutaneous Ultrasonography
• Less useful than CT because – pancreas is often obscured by overlying gas from stomach,
duodenum and colon.– Depth of pancreas from anterior abdominal wall limits imaging
to lower(2-5 MHz) frequency, hence lower resolution– Detect only 60-70 % of pancreatic CA– >40% lesions <3 cm missed(similar to CT)
• Only useful as an initial screening test in evaluating patients who present with possible obstructive jaundice– However, other studies should then be performed to definitively
diagnose the source of biliary obstruction.– Use to visualize gall bladder, liver , CBD size, LN, portal vein,
ascites

Radiological InvestigationsEndoscopic Ultrasonography
• Obviates the physical limitations of TUS– High frequency USG(7.5-12 MHz) with very high resolution (subcentimeter)
images
• INDICATED if high suspicion of pancreatic CA and CT is normal
• MOST SENSITIVE and SPECIFIC diagnostic test for pancreatic cancer– Negative EUS is nearly 100 % specific at ruling out presence of a pancreatic
neoplasm– Detection rates of 99-100 % for all pancreatic carcinomas including <3 cm– As accurate as ERCP or MRCP for assessing etiology of obstructive jaundice– Equivalent to dual-phase spiral CT for assessing tumor resectability potential– Superior to CT as mean of assessing T stage of tumor e.g. portal vein/ SMV
involvement
• EUS-guided FNA can also be done at time of EUS diagnosis• Demerit:
– Inferior to CT in assessing arterial involvement and distant metastases– Poor at detecting occult nodal involvement(same as CT)

Endoscopic ultrasound of a 2.2-cm pancreatic adenocarcinoma of the head of the pancreas obstructing the common bile duct
(CBD) but not invading the portal vein (PV) or superior mesenteric vein (SMV).

Radiological InvestigationsEndoscopic Retrograde Cholangiopancreatography
• Highly sensitive means of detecting pancreatic +/- biliary ductal abnormalities in pancreatic cancer– 90-95 % cases have ERCP findings– Brush cytology and forceps biopsy can be taken(< 50 % yield)
• Demerits:– Findings not always highly specific for pancreatic cancer– Difficult to differ from changes of chronic pancreatitis– More invasive and carries 5-10 % risk of significant
complications• Reserved as therapeutic procedure for biliary obstruction OR for
diagnosis of unusual neoplasm such as intraductal pancreatic mucinous neoplasms(IPMN)
– Limited staging information

Radiological Investigations
Magnetic Resonant Imaging
• NOT superior to spiral CT scanning in diagnosing and staging pancreatic cancer
Magnetic Resonant Cholangiopancreatography
• Noninvasive method for imaging the biliary tree and pancreatic duct

Radiological Investigations
Positron Emission Tomography
• Uses 18F-fluorodeoxyglucose(FDG) to image primary tumor and metastatic disease
• Useful in detecting occult metastatic disease
• Alone offer no additional benefits over high-quality CT
• PET-CT more sensitive than conventional imaging for detection of pancreatic cancer

Needle Aspiration
IN FAVOUR
• Provide proof of pathology pre operatively
• Exclude unusual pathology
• Evidence of disease before initiation of multidisciplinary treatment e.g. neoadjuvantchemotherapy
AGAINST
• Biopsy will not alter therapy
• May result in seeding*, infection, bleeding, fistula and leak
• Interfere with definitive surgery
• Increases the cost of care
*Risk of peritoneal contamination with CT guided biospy(50-85 % yeild) is uncommon*EUS guided aspiration done through tissue that would ultimately included in operative field and resected. Thus, it is MOST EFFECTIVE(85-95 % accurate) means for getting biopsy
_____________________________________________________________________________

Needle Aspiration
• Tissue diagnosis before performing pancreatoduodenectomy is not essential– Negative biopsy doesn't rule out malignancy in face of
clinical and radiological clues
• Tissue diagnosis mandatory if– Neoadjuvant/adjuvant chemotherapy to be given
– Clinical presentation more suggestive of alternative diagnosis such as lymphoma or pancreatic islet cell tumors

Staging
• Once probable diagnosis has been established, next issue is whether lesion is amenable to surgical resection
• Pancreatic masses characterized as– Resectable( only 20 % of all cases)– Borderline resectable (based on experience/skill of surgeon and
overall health of patient)– Irresectable
• Noncurative resections for pancreatic cancer provide no survival benefits
• Hence, WHEN NOT TO OPERATE decision requires accurate preoperative staging

American Joint Committee on Cancer (AJCC)- 2002Tumor (T)
• TX - Primary tumor cannot be assessed• T0 - No evidence of primary tumor• Tis - Carcinoma in situ• T1 - Tumor limited to the pancreas, 2 cm or smaller in greatest dimension• T2 - Tumor limited to the pancreas, larger than 2 cm in greatest dimension• T3 - Tumor extension beyond the pancreas (eg, duodenum, bile duct, portal or
superior mesenteric vein) but not involving the celiac axis or superior mesenteric artery
• T4 - Tumor involves the celiac axis or superior mesenteric arteries
Regional lymph nodes (N)• NX - Regional lymph nodes cannot be assessed• N0 - No regional lymph node metastasis• N1 - Regional lymph node metastasis
Distant metastasis (M)• MX - Distant metastasis cannot be assessed• M0 - No distant metastasis• M1 - Distant metastasis

T staging for pancreatic carcinoma

American Joint Committee on Cancer (AJCC)- 2002
Stage T N M Description
0 Tis N0 M0
IA T1 N0 M0 Limited to pancreas≤ 2 cm
IB T2 N0 M0 Limited to pancreas > 2 cm
IIA T3 N0 M0 Extends beyond pancreas but doesn't involve arteries
IIB T1-3 N1 M0 Any tumor without artery involvement with LN +
III T4 Any N M0 Tumor involves arteries (unresectable)
IV Any T Any N M1 Any tumor with distant metastases
• Stage grouping for pancreatic cancer is as follows:

Staging
Stage at time of presentation Frequency of cases
Stage I disease-confined to primary site 7 %
Locally advanced disease 26%
Metastatic to distant nodes/sites 52%
Unknown 15%

StagingMODALITIES
• According to 2011 NCCN guideline, CT scan primary mean for staging– Triphasic multidetector spiral(helical) dynamic contast-enhanced CT with
thin-slice, cross sectional imaging is recommended i.e. pancreas protocol CT scanning
• EUS 70-80 % accurate for correct staging/predicting resecatbility
• Staging Laparoscopy (with US 98 % accurate)– Some use it routinely in all patients with pancreatic caner– Others, including NCCN 2011 guidelines, advise selective approach with any of
following criteria:• CA 19-9 > 1000 U/mL or marked wt loss• Low volume ascites• Body/tail of pancreas tumor• Borderline resectable tumors/equivocal findings of metastsis• Size> 4 cm• CBD lymphadenopathy
– Doesnot show vascular invasion or retroperitoneal invasion which makes apparently resectable tumor irresectable one

Evaluation Algorithm

Treatment
• Surgery
– primary mode of treatment
• Chemoradiation
– Adjuvant or neoadjuvant therapy
– Irresectable disease
• Palliative therapy

Treatment
SURGERY• Typically, extrapancreatic disease precludes curative
resection and surgical treatment may be palliative at best
• Invasion of SMV/portal vein NOT absolute contraindication– Can be resected partially with as much as 50 % narrowing of
lumen– Complete reconstruction is possible e.g. using native veins as
replacement( internal jugular, greater saphenous or splenic)
• Invasion of SMA/celiac/hepatic arteries still barrier to resection

Treatment
SURGERY• In operable cases
– Whipple Procedure– Traverso-Longmire pylorus preserving
pancreaticoduodenectomy(PPPD)– Fortner’s regional pancreatectomy (extended
whipple’s)– Total pancreatectomy– Distal pancreatectomy
• In inoperable cases– Roux en Y choledochojejunostmoy

Whipple Procedure
• Indicated for periampullary tumors
• Involves removal of– Pancreatic head and neck– 40 % distal stomach + C loop of duodenum + 10 cm proximal jejunum– Lower end of CBD with gall bladder– Peripancreatic + pericholedochal + paraduodenal + perihepatic nodes
• Contiuity maintained by– Choledochojejunostomy– Pancreaticojejunostomy ( or pancreatogastrostomy)– Gastrojejunostomy

Whipple Procedure

Whipple Procedure
• Mortality 2-8 %
• Complications– Delayed gastric emptying-25 %
• Require NG decompression
– Pancreatic fistula -14 %– Infection- intraabdominal abscess, wound infection,
cholangitis, pancreatitis, pneumonia– Bile/pancreatic anastomotic leak
• Preoperative biliary drainage (ERCP) increases the rate of complications

Surgery
Traverso-Longmire pylorus preserving pancreaticoduodenectomy(PPPD)
• Duodenum is cut 2 cm distal to pylorus
• Continuity maintained by anastomosing with jejunum
Fortner’s regional pancreatectomy(extended Whipple’s)
• Resection like whipple’s along with removal of segment of SMV and clearance of all regional nodes
• Portal vein continuity maintained by synthetic vascular graft

Surgery
Total Pancreatectomy• Least commonly performed procedure• Morbidity comparable to that of whipple procedure• Highest mortality rate i.e. 8.3 %• Indicated in pancreatic neck tumor• Merits:
– Possibility of multicentric disease– Recurrence after whipple procedure– No morbidity due to pancreatic fistula or pancreatitis– Malignant cell may present in pancreatic duct
• Complication– Severe resistant brittle diabetes mellitus

Surgery
Distal Pancreatectomy• Lower mortality(3.5 %) than standard whipple
• Indicated for tumor located in body and tail of pancreas
• Limited curative resection as these tumor present later with higher unresectability rate
• Involves isolation of distal portion of pancreas containing tumor followed by resection of that segment, with over sewing of distal pancreatic duct
• Complications: Pancreatic stump leak, hemorrhage, endocrine insufficiency

Surgery
Roux en Y choledochojejunostomy
• Palliative procedure done along with gastrojejunostomy after doing cholecystectomy
• Better than cholecystojejunostomy as it may get blocked either by tumor infiltration or by bile sludge or inflammation

Chemoradiotherapy-Palliative• Indicated in advanced irresectable/metastatic
pancreatic cancer – Gemcitabine(1000 mg/m2 over 1 hour IV) montherapy
• 1st line therapy (NCCN 2011 guidelines) in poor performance status
– FOLFIRINOX ( LV5-FU + oxaliplatin +irinotecan)• 1st line therapy (NCCN 2011 guidelines) in good performanc status
– Gamcitabine + nab(nanoparticle ablumin bound)-paclitaxel• Indicated if FOLFIRINOX contraindicated
– Capecitabine +/- erlotinib• Second line therapy if refactory to gemcitabine
– OTHERS• Gamcitabine + docetaxel + capecitabine (GTX regimen)• Gemcitabine +/- erlotinib-FDA approved
/capecitabine(controversial)

Chemoradiotherapy-Palliative
• Daily use aspirin over a period of 5 years reduces death caused by several cancers including pancreatic cancer

Chemoradiotherapy- Adjuvant
• Gemcitabine
• S-1(Taiho Pharmaceutical, Japan)
Chemoradiation-Neoadjuvant
No form of neoadjuvant therapy is regarded as standard form of therapy( NCCN 2011)

Palliative TherapyPAIN
• Nacrotic analgesics used early and in adequate dosages– Combining with TCAs or antiemetics potentiate their analgesic effect– Sustainted release Morphine sulfate
• Neurolysis of celiac ganglion if refactory pain– Performed transthoracically or transabdominally by invasive radiology
or anesthesiology, transgastrically using EUS-guided Fine needle injection or intra operatively
• Radiation therapy(4000 cGy units) can palliate pain but does not affect patients survival
• ERCP- stent if pain due to obstruction of pancreatic/bilairy tract

Palliative Therapy
JAUNDICE• Warrants palliation if patient has pruritus or RHC
pain or developed cholangitis• Endoscopic placement of plastic(replace every 3
months) or metal (5 months) stents• Surgical biliary decompression/bypass
DUODENAL OBSTRUCTION-20%• Endoscopic stenting(poor operative candidates)• Gastrojejunostomy

PROGNOSIS…….fatal disease
5 year survival after successful surgery NOT guarantee of CURE
Without Surgery Successful curative resection(about 20 % patients)
Median survival rate 4-6 months 12-19 months
1 year survival rate 24 %
Overall 5 year survival rate 5 % 15-20 %
Location Time of presentation Prognosis
HEAD and NECK Early presentation-obstructive jaundice
Better prognosis
Body and Tail Late presentation(Mass) Worse prognosis

PROGNOSIS…….fatal disease
Stage 5 year survival rate
Localized stage 20.3 %
Regional stage 8.0 %
Distant stage 1.7%
Unknown stage 4.1%
PROGNOSIS…….fatal disease
POOR PROGNOSTIC FACTORS• Growth > 3 cm*• Nodal involvement*
– Ratio of positive nodes to total nodes removed more important than margin positivity
• Portal vein infiltration• Liver /Lung mets*• Ascites*/Trousseau’s sign/Left supraclavicular LN spread• White bile on table• Associated problems like pancreatitis, DM• Liver dysfunction*
*Present in patient mentioned in case summary

Future Therapy
• Immunotherapeutic gene therapy– To assist immune system in recognizing cancer cells
• Replacement of tumor suppressor gene function
• Inactivation of oncogenes
• Suicide gene therapy– Transgene introduced that converts an inactive notoxic drug
into active cytotoxic agent– E.g. Herpes simplex virus-thymidine kinase system

Case Summary
• 60 year old male, resident of Nankana Sahib presented with pain in epigastrium for last 1 year, – chronic in onset, progressive, boring in nature, radiating directly to back,
aggravated with food intake, relieved temporarily with medication, mild initially then moderate in intensity,
– associated weight loss, anorexia, yellowish discoloration of sclera, dark color urine, abdominal distension
• Past medical history shows HCV + with chronic liver disease
• Examination revealed elderly male of lean physique with abdominal distension, vitally stable, with Jaundice +, BUT no pallor/bruises/palpable lymphadenopathy
• Abdominal Examination revealed it to be distended, tensed, tender(upper portion) with horizontally compressed umbilicus, splenomegaly, fluid thrill +, NO paraumblical nodule

Case Summary
• Hematological investigations showed
Parameter Value
Hemoglobin 13.5
Total leucocyte Count 6.2
Platelet count 172
Sodium/potassium 137/3.8
Urea/creatinine 70/0.9
Prothromin time 14/13 (INR 1.1)
Total bilirubin 14.2
Conjugated bilirubin 11.0
Alkaline phosphatase 340
Gamma GT 202
Total protein/Albumin 5.6/2.0
ALT/AST 46/41

Case Summary
• Transcutaneous Ultrasound showed– Liver normal in size and echotexture.No focal lesion
seen
– Biliary channels/CBD/portal vein normal
– Gall Bladder distended full of thick sludge and debrinous
– Pancreas showed 46x24x57 mm heterogenous area into body and tail
– Spleen measures 14.5 cm and mildly enlarged
– Minimal abdominopelvic ascites

Case Summary• Pancreas protocol CT scan showed
– Infiltrative primary pancreatic mass involving its body and tail which would be most concerning for a primary pancreatic cancer.
– Associated upper abdominal lymphadenopathy– Significant intra and extra hepatic biliary dilation probably secondary
to upper abdominal lymphadenopathy– Gall Bladder distended with no primary GB mass– Obvious slightly irregular focal low density in segment 4 of liver, most
consistent with liver metastases– Significant abdominopelvic ascites– Nodularity/thickening along peritoneal reflection and omental
infiltration– Multiple basal pulmonary nodules regarded as metastasis– Sclerotic focus in right ischial bone, may represent bone mets___________________________________________________________
IMPRESSION: Metastatic primary T4 pancreatic cancer (Stage 4)

Case Summary
• Currently, patient is on following treatment
Rationale Medication
Partial Parenteral NutritionInf 10 % D/W 1000 ml IV OD
Inf Aminovil 500 mg IV BD
Pain Inj Toradol IV TDSInj N/M diluted in 10 ml N/S, give 3 ml IV TDS
Vomiting Inj gravinate IV TDS Inj Onset IV TDS
Stress ulcers Inj Novoteph 40 mg IV BD
Antibiotic Inj oxidil 1g IV BD
Ascites Inj Lasix 20 mg IV ODTab aldactone 100 mg PO OD
Tab Inderal 10 mg PO TDS Inj Albumin 100 ml IV OD for 3 days
Malabsorption of vit K(fat soluble) Inj Vit K IM OD for 3 days

Case Summary
• As a palliative measure for biliary decompression, ERCP planned on 24th March
2014

THANK YOU…………………..

Surgical Triad
Measure Thrice
Think twice
Cut once




![th Anniversary Special Issues (14): Pancreatic cancer ...€¦ · carcinomas are classified as pancreatic ductal adeno-carcinoma (PDAC)[4]. An activating mutation in a key proto-oncogene](https://static.fdocuments.in/doc/165x107/5f92b3c623023e07b6622eec/th-anniversary-special-issues-14-pancreatic-cancer-carcinomas-are-classified.jpg)




![Duct-like Morphogenesis of Longnecker Pancreatic Acinar ...[CANCER RESEARCH 46, 347-354, January 1986] Duct-like Morphogenesis of Longnecker Pancreatic Acinar Carcinoma Cells Maintained](https://static.fdocuments.in/doc/165x107/5e5986bea237161eef27ccc5/duct-like-morphogenesis-of-longnecker-pancreatic-acinar-cancer-research-46.jpg)








