Pancoast syndrome: A case report. - bjkines.combjkines.com/vol10dec18/paper5d18fulltext.pdf · due...
4
BJKin 24 p-ISSN:2231-6140, e Pancoast syndrome: A case Dr. Amit Bhandari 1* , Dr. Pooja P 1,2 Resident Doctor, 3 Assistant Pro Hospital, Ahmedabad, Gujarat, Indi Introduction: Pancoast syndrome is a impairment of the brachial plex bodies), first/second thoracic ne due to a tumor in the superior symptoms are pain in the should muscle hypotrophy. Horner’s clinically manifesting as ptosis included in the spectrum of Panc have non-small cell bronchogen objective of this report is to disc imaging in the diagnosis, determ this condition. Case Report: A 55year old male patie Orthopaedic OPD with comp shoulder pain radiating to arm complaint of cough occasionally history of fever, trauma or heavy Patient also had the history of c since 40 years. On Examination, patient right upper eyelid and constr pupil. [Image 1] Abstract: Pancoast tumor (Superior outcome. Due to its localization in t the brachial plexus, first ribs, verte with irradiation, chemotherapy, and most cases. To accurately determin need a detailed knowledge of the cli Key words: Brachial plexus, Imagin nes-NJBAS Volume-10(2), December 201 e-ISSN:2395-7859 C e report. Prajapati 2 , Dr. Vasant Rathod 3 ofessor, Department of Radiology, B. J. Medical ia. a set of signs & symptoms secondary to th xus, parietal pleura, first/second ribs (and adjac erves, paravertebral sympathetic chain and stell r sulcus, also known as a Pancoast tumor. C der and ipsilateral affected arm progressing to w syndrome, which involves stellate ganglion s, miosis, enophthalmos and ipsilateral anhidr coast syndrome features. Most patients with Pan nic carcinoma, most often squamous / adenoca cuss the clinical presentation, imaging presenta mining the extent of involvement and further ma ent presented in plaints of right m. He also had y. There was no y weight lifting. chronic smoking had drooping of riction of right r sulcus tumor) is associated in most cases with a p the apex of the lung, it has a potential of invasion of the l ebrae, subclavian vessels or stellate ganglion. Multimoda d surgery offers the best possibility for long-term survival ne tumor resectability and to help optimize the treatment, inical and imaging manifestations of disease. ng, Pancoast tumor, Superior sulcus tumor. * Corresponding Author: Dr. Amit Bhandari E-mail: bhandariamit92@ QR Code: 18 2018 Case Report College, Civil he neoplastic cent vertebral late ganglion, Clinically, the weakness and impairment, rosis, can be ncoast tumors arcinoma. The ation &role of anagement of poor clinical lower part of ality therapy l and cure in , radiologists @gmail.com
Transcript of Pancoast syndrome: A case report. - bjkines.combjkines.com/vol10dec18/paper5d18fulltext.pdf · due...

BJKines
24 p-ISSN:2231-6140, e
Pancoast syndrome: A case report.
Dr. Amit Bhandari 1*, Dr. Pooja Prajapati1,2 Resident Doctor, 3Assistant Professor, Department of Radiology, B. J. Medical College, Civil Hospital, Ahmedabad, Gujarat, India.
Introduction:
Pancoast syndrome is a set of signs & symptoms secondary to the neoplastic impairment of the brachial plexus, parietal pleura, first/second ribs (and adjacent vertebral bodies), first/second thoracic nervesdue to a tumor in the superior sulcus, also known as a Pancoast tumor. Clinically, the symptoms are pain in the shoulder and ipsilateral affected arm muscle hypotrophy. Horner’s syndrome, which involves stellate ganglion impairment, clinically manifesting as ptosis, included in the spectrum of Pancoast syndrome features. Most patients with Pancoast tumors have non-small cell bronchogenic carcinoma, most often squamousobjective of this report is to discuss the clinical presentation, imaging presentation &role of imaging in the diagnosis, determining the extent of involvementthis condition.
Case Report:
A 55year old male patient presented in Orthopaedic OPD with complaints of right shoulder pain radiating to arm. He also had complaint of cough occasionally.history of fever, trauma or heavy weight lifting.Patient also had the history of chronic smoking since 40 years.
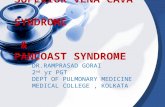
On Examination, patient had drooping of right upper eyelid and constriction of right pupil. [Image 1]
Abstract:
Pancoast tumor (Superioroutcome. Due to its localization in the apex of the lung, it has a potential of invasion of the lower part of the brachial plexus, first ribs, vertebrae, subclavian vessels or swith irradiation, chemotherapy, and surgery offers the best possibility for longmost cases. To accurately determine tumor resectability and to help optimize the treatment, radiologists need a detailed knowledge of the clinical and imaging manifestations of disease
Key words: Brachial plexus, Imaging, Pancoast tumor, Superior sulcus tumor
BJKines-NJBAS Volume-10(2), December 201
e-ISSN:2395-7859 Case Report
case report.
, Dr. Pooja Prajapati2, Dr. Vasant Rathod3
Assistant Professor, Department of Radiology, B. J. Medical College, Civil Hospital, Ahmedabad, Gujarat, India.
Pancoast syndrome is a set of signs & symptoms secondary to the neoplastic impairment of the brachial plexus, parietal pleura, first/second ribs (and adjacent vertebral bodies), first/second thoracic nerves, paravertebral sympathetic chain and stellate ganglion, due to a tumor in the superior sulcus, also known as a Pancoast tumor. Clinically, the symptoms are pain in the shoulder and ipsilateral affected arm progressing to weakness and
rner’s syndrome, which involves stellate ganglion impairment, tosis, miosis, enophthalmos and ipsilateral anhidrosis, can be Pancoast syndrome features. Most patients with Pancoast tumors
small cell bronchogenic carcinoma, most often squamous / adenocarcinoma. The objective of this report is to discuss the clinical presentation, imaging presentation &role of
, determining the extent of involvement and further managem
A 55year old male patient presented in Orthopaedic OPD with complaints of right shoulder pain radiating to arm. He also had complaint of cough occasionally. There was no history of fever, trauma or heavy weight lifting. Patient also had the history of chronic smoking
On Examination, patient had drooping of eyelid and constriction of right
Superior sulcus tumor) is associated in most cases with a poor clinical outcome. Due to its localization in the apex of the lung, it has a potential of invasion of the lower part of the brachial plexus, first ribs, vertebrae, subclavian vessels or stellate ganglion. Multimodality therapy with irradiation, chemotherapy, and surgery offers the best possibility for long-term survival and cure in
To accurately determine tumor resectability and to help optimize the treatment, radiologists a detailed knowledge of the clinical and imaging manifestations of disease.
Brachial plexus, Imaging, Pancoast tumor, Superior sulcus tumor.
* Corresponding Author: Dr. Amit Bhandari E-mail: [email protected]
QR Code:
2018 2018
Case Report
Assistant Professor, Department of Radiology, B. J. Medical College, Civil
Pancoast syndrome is a set of signs & symptoms secondary to the neoplastic impairment of the brachial plexus, parietal pleura, first/second ribs (and adjacent vertebral
, paravertebral sympathetic chain and stellate ganglion, due to a tumor in the superior sulcus, also known as a Pancoast tumor. Clinically, the
weakness and rner’s syndrome, which involves stellate ganglion impairment,
anhidrosis, can be Pancoast syndrome features. Most patients with Pancoast tumors
/ adenocarcinoma. The objective of this report is to discuss the clinical presentation, imaging presentation &role of
management of
is associated in most cases with a poor clinical outcome. Due to its localization in the apex of the lung, it has a potential of invasion of the lower part of
tellate ganglion. Multimodality therapy term survival and cure in
To accurately determine tumor resectability and to help optimize the treatment, radiologists
BJKines
25 p-ISSN:2231-6140, e
Image 1 Drooping of right eyelid.
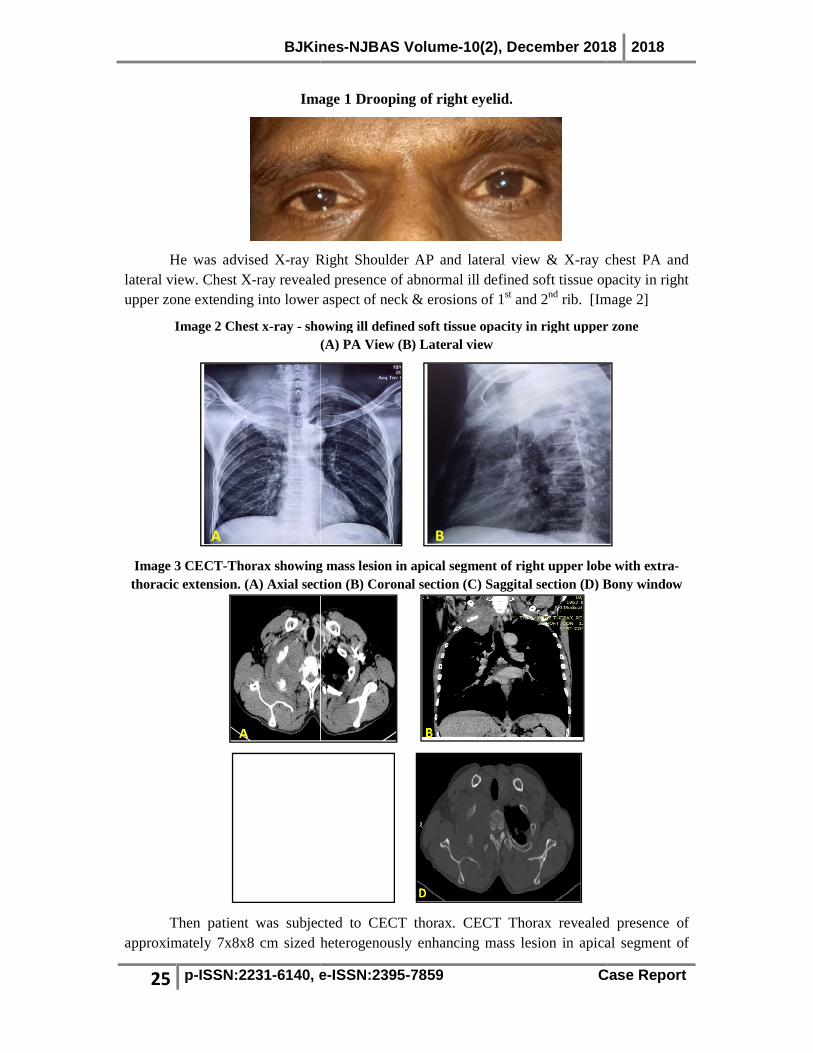
He was advised X-ray Right Shoulder AP and lateral viewlateral view. Chest X-ray revealed presence of abnormal ill defined soft tissue opacity in upper zone extending into lower aspect of neck & erosions of 1
Image 2 Chest x-ray - showing ill defined soft tissue opacity in right upper (A) PA View (B) Lateral view
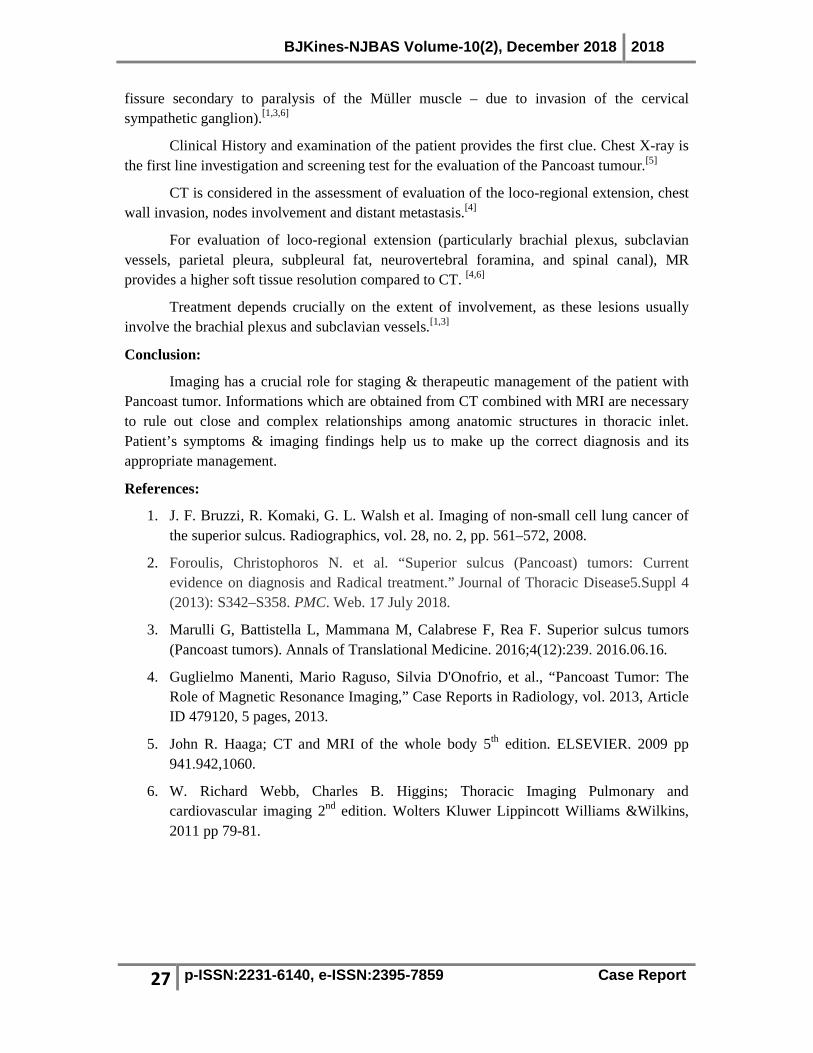
Image 3 CECT-Thorax showing mass lesion in thoracic extension. (A) Axial section (
Then patient was subjected to CECT thorax.approximately 7x8x8 cm sized heterogenously enhancing mass lesion in apical segment of
BJKines-NJBAS Volume-10(2), December 201
e-ISSN:2395-7859 Case Report
Image 1 Drooping of right eyelid.
Right Shoulder AP and lateral view & X-ray chest PA and revealed presence of abnormal ill defined soft tissue opacity in
upper zone extending into lower aspect of neck & erosions of 1st and 2nd rib. [Image 2]
showing ill defined soft tissue opacity in right upper (A) PA View (B) Lateral view
showing mass lesion in apical segment of right upper lobe with extra) Axial section (B) Coronal section (C) Saggital section (D) Bony window
Then patient was subjected to CECT thorax. CECT Thorax revealed presence of sized heterogenously enhancing mass lesion in apical segment of
2018 2018
Case Report
chest PA and revealed presence of abnormal ill defined soft tissue opacity in right
[Image 2]
showing ill defined soft tissue opacity in right upper zone
apical segment of right upper lobe with extra-) Bony window
CECT Thorax revealed presence of sized heterogenously enhancing mass lesion in apical segment of

BJKines
26 p-ISSN:2231-6140, e
right upper lobe extending into lower aspect of right side of neck.of 1st and 2nd ribs. The lesion shows extrainvades right sided longus colli, scalene muscles, spinal cervices and semispinalis capitis.It encases thyrocervical trunk and displaces righenlarged enhancing right hilar, mediastinal, supraclavicular lymphnodes were se
Further, MRI brachial plexus was done which revealed presence of mass lesion in right lower aspect of neck with presence of abnormal T2 hyperintensity along right brachial plexus and non visualisation of cords separately s[Image 4]
Image 4: MRI brachial plexus T2WI (Arrow indicate Normal brachial plexus on left side)
(A) Saggital section (B) Coronal section
These findings were suggestive of thoracic extension into muscles of neck, involvement of brachial plexus on right side and erosions of right 1st& 2nd rib and metastatic lymphadenopathy. Imaging features with clinical presentation of the patient made the diagnosis of Pancoast Syndrome.
CT guided FNAC of the lesion was done which revealed squamous cell carcinoma.Patient has currently been started on com
Discussion:
Pancoast tumors are non–cause signs and symptoms known collectively as Pancoast syndrome.
Adenocarcinomas account for 2/3 of all Pancoast are squamous cell and large cell carcinomas.
They invade through tissue contiguity the apical chest wall and the structures of the thoracic inlet (parietal pleura, 1st and 2nd ribs or periosteum and adjacent 1st andvertebral bodies, the lower nerve roots of the brachial plexus, the upper sympathetic chain and stellate ganglion, the subclavian vein and artery), producing a clinical picPancoast syndrome.[2]
The clinical features include pain in the ssyndrome(miosis, ptosis and ipsilateral anhidrosis of the face with narrowing of the palpebral
BJKines-NJBAS Volume-10(2), December 201
e-ISSN:2395-7859 Case Report
right upper lobe extending into lower aspect of right side of neck. The lesion causes erosion The lesion shows extra-thoracic extension upto C7 vertebral level and
s right sided longus colli, scalene muscles, spinal cervices and semispinalis capitis.It encases thyrocervical trunk and displaces right subclavian artery anteriorly. enlarged enhancing right hilar, mediastinal, supraclavicular lymphnodes were se
Further, MRI brachial plexus was done which revealed presence of mass lesion in right lower aspect of neck with presence of abnormal T2 hyperintensity along right brachial plexus and non visualisation of cords separately suggestive of invasion by the mass lesion.
Image 4: MRI brachial plexus T2WI - showing mass lesion in right lower aspect of neck(Arrow indicate Normal brachial plexus on left side)
(A) Saggital section (B) Coronal section
These findings were suggestive of malignant mass of right upper lobe with extrathoracic extension into muscles of neck, involvement of brachial plexus on right side and
rib and metastatic lymphadenopathy. Imaging features with clinical presentation of the patient made the diagnosis of Pancoast Syndrome.
CT guided FNAC of the lesion was done which revealed squamous cell carcinoma.Patient has currently been started on combination of chemotherapy and radiotherapy.
–small cell carcinomas. They originate in the lung apex and cause signs and symptoms known collectively as Pancoast syndrome. [1]
Adenocarcinomas account for 2/3 of all Pancoast tumors, while the rest of the tumors ll and large cell carcinomas. [2]
They invade through tissue contiguity the apical chest wall and the structures of the thoracic inlet (parietal pleura, 1st and 2nd ribs or periosteum and adjacent 1st andvertebral bodies, the lower nerve roots of the brachial plexus, the upper sympathetic chain and stellate ganglion, the subclavian vein and artery), producing a clinical picture known as
The clinical features include pain in the shoulder girdle and arm[2]
syndrome(miosis, ptosis and ipsilateral anhidrosis of the face with narrowing of the palpebral
2018 2018
Case Report
The lesion causes erosion thoracic extension upto C7 vertebral level and
s right sided longus colli, scalene muscles, spinal cervices and semispinalis capitis. t subclavian artery anteriorly. Multiple
enlarged enhancing right hilar, mediastinal, supraclavicular lymphnodes were seen. [Image 3]
Further, MRI brachial plexus was done which revealed presence of mass lesion in right lower aspect of neck with presence of abnormal T2 hyperintensity along right brachial
n by the mass lesion.
mass lesion in right lower aspect of neck.
mass of right upper lobe with extra-thoracic extension into muscles of neck, involvement of brachial plexus on right side and
rib and metastatic lymphadenopathy. Imaging features with clinical
CT guided FNAC of the lesion was done which revealed squamous cell carcinoma. bination of chemotherapy and radiotherapy.
small cell carcinomas. They originate in the lung apex and
tumors, while the rest of the tumors
They invade through tissue contiguity the apical chest wall and the structures of the thoracic inlet (parietal pleura, 1st and 2nd ribs or periosteum and adjacent 1st and 2nd vertebral bodies, the lower nerve roots of the brachial plexus, the upper sympathetic chain
ture known as
[2] and Horner syndrome(miosis, ptosis and ipsilateral anhidrosis of the face with narrowing of the palpebral
BJKines-NJBAS Volume-10(2), December 2018 2018
27 p-ISSN:2231-6140, e-ISSN:2395-7859 Case Report
fissure secondary to paralysis of the Müller muscle – due to invasion of the cervical sympathetic ganglion).[1,3,6]
Clinical History and examination of the patient provides the first clue. Chest X-ray is the first line investigation and screening test for the evaluation of the Pancoast tumour.[5]
CT is considered in the assessment of evaluation of the loco-regional extension, chest wall invasion, nodes involvement and distant metastasis.[4]
For evaluation of loco-regional extension (particularly brachial plexus, subclavian vessels, parietal pleura, subpleural fat, neurovertebral foramina, and spinal canal), MR provides a higher soft tissue resolution compared to CT. [4,6]
Treatment depends crucially on the extent of involvement, as these lesions usually involve the brachial plexus and subclavian vessels.[1,3]
Conclusion:
Imaging has a crucial role for staging & therapeutic management of the patient with Pancoast tumor. Informations which are obtained from CT combined with MRI are necessary to rule out close and complex relationships among anatomic structures in thoracic inlet. Patient’s symptoms & imaging findings help us to make up the correct diagnosis and its appropriate management.
References:
1. J. F. Bruzzi, R. Komaki, G. L. Walsh et al. Imaging of non-small cell lung cancer of the superior sulcus. Radiographics, vol. 28, no. 2, pp. 561–572, 2008.
2. Foroulis, Christophoros N. et al. “Superior sulcus (Pancoast) tumors: Current evidence on diagnosis and Radical treatment.” Journal of Thoracic Disease5.Suppl 4 (2013): S342–S358. PMC. Web. 17 July 2018.
3. Marulli G, Battistella L, Mammana M, Calabrese F, Rea F. Superior sulcus tumors (Pancoast tumors). Annals of Translational Medicine. 2016;4(12):239. 2016.06.16.
4. Guglielmo Manenti, Mario Raguso, Silvia D'Onofrio, et al., “Pancoast Tumor: The Role of Magnetic Resonance Imaging,” Case Reports in Radiology, vol. 2013, Article ID 479120, 5 pages, 2013.
5. John R. Haaga; CT and MRI of the whole body 5th edition. ELSEVIER. 2009 pp 941.942,1060.
6. W. Richard Webb, Charles B. Higgins; Thoracic Imaging Pulmonary and cardiovascular imaging 2nd edition. Wolters Kluwer Lippincott Williams &Wilkins, 2011 pp 79-81.