Social Workers - Palliative Care Victoria, Palliative Care ...
Upload
miles-thomasCategory
view
219download
1
Palliative Care Overview
Fred Nelson BA, MSW, RSWPsychosocial Specialist, WRHA Palliative Care
Mike Harlos MD, CCFP, FCFPProfessor and Section Head, Palliative Medicine, University of ManitobaMedical Director, WRHA Adult and Pediatric Palliative CareClinical Lead, Canadian Virtual Hospice
Janice Nesbitt RN, MNClinical Nurse Specialist, WRHA Adult and Pediatric Palliative Care
Feb. 19, 2014

http://palliative.info


The presenters have no
conflicts of interest to
disclose

Objectives
• To provide an overview of various elements of palliative care, including communication and decision making, symptom management, supporting families, and self care
• Consider unique challenges in your specific care setting
• Review challenging cases, considering potential approaches to care


Communication In Palliative Care
A Foundation For Approaching Care

Anticipating Predictable Issues• Most palliative clinical issues & patient/family concerns are very
predictable and can be addressed proactively rather than reactively
• don’t assume that silence = no concerns
• engaging patients/families proactively conveys your understanding of their concerns and an ability to address them, e.g.:
functional decline (weakness, transfer problems, risk of falls) – pretty much 100% of patients
decreased food/fluid intake – virtually all patients affected and all families become concerned
are the meds causing the sleepiness, or the decline? would care be managed differently somewhere else? how long can this go on? what will things look like?

Potential Ways To Start Conversations
• “You might be wondering why your Mom is…
• “Many people in these type of situations wonder about…”
“Is this something you’d like to talk about?”

Be Clear
• people often speak “around” difficult topics
• messages need to be clear, though not brutally blunt.
• you can start with a “vague and gentle”, paced approach – however you may need to be increasingly direct
• intuitive approach to how blunt and direct you need to be
“The single biggest problem in communication is the illusion that it has taken place.”
George Bernard Shaw


12
Suggested Framework For Responding To Difficult Questions
1. Acknowledge/Validate and Normalize“That’s a very good question, and one that we should talk about. Many
people in these circumstances wonder about that…”
2. Is there a reason this has come up?“I’m wondering if something has come up that prompted you to ask this?”
3. Gently explore their thoughts/understanding • “It would help me to have a feel for your understanding of your
condition, and what you might expect”• “Sometimes when people ask questions such as this, they have an idea
in their mind about what the answer might be. Is that the case for you?”
4. Respond, if possible and appropriate• If you feel unable to provide a satisfactory reply, then be honest
about that and indicate how you will help them explore their concerns

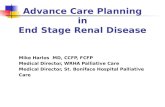
Day 1Day 1 FinalFinalDay 3Day 3Day 2Day 2
The Perception of the “Sudden Change”
Melting ice = diminishing reserves
Even in the context of a slowly progressive disease, when the reserves are depleted there is a sudden change, which to the family can seem shockingly abrupt
That was fast!

Helping Families At The Bedside
physical changes of dying (colour, breathing patterns) can be upsetting
do family members might want individual time alone?
can they hear us?
missed the death

Framing Decisions For Substitute Decision Makers
• Rather than asking family what they want done for their loved one, ask what their loved one would want for themselves if they were able to say (“If he could tell us…”)
• may seem like life-and-death decisions – however the underlying illness itself is not survivable… no decision can change that…
“I know that you’re being asked to make some very difficult choices about care, and it must feel that you’re having to make life-and-death decisions. You must remember that this is not a survivable condition, and none of the choices that you make can change that outcome.
We know that his life is on a path towards dying… we are asking for guidance to help us choose the smoothest path, and one that reflects an approach consistent with what he would tell us to do.”

Pain Assessment &
Management

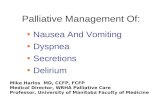
TYPES OF PAIN
NEUROPATHICNOCICEPTIVE
Somatic
• bones, joints• connective tissues• muscles• sharp• dull & aching• can localize site• may be worse with
movement (“incident pain”)
Visceral
• Organs – heart, liver, pancreas, gut, etc.
• may be crampy, or dull & aching
• referred pain• difficult to localize
• difficult to describe; not a typical “pain”
• numb; burning; tingling; crawling; stabbing; etc
• allodynia• consider it as a possible
element of any difficult pain syndrome

• Prevent SREs – zoledronate (may also help pain)
• consider spinal cord compression in back pain
• Analgesia- RadTX- Perhaps acetaminophen, though likely not potent enough- NSAIDs – cautiously - Opioids – consider renal function in selection- Neuropathic adjuvants for neuropathic or challenging pain- Perhaps corticosteroids
• Fracture risk?- Plain films of involved areas- Consider orthopedic opinion RE fracture risk, prophylactic
surgery
Palliative Approach To Bone Mets

Approach To Pain Control in Palliative Care
1. Thorough assessment• History – including detailed description of pain;
psychosocial, spiritual, & cultural context; concerns about what the pain means; medication history
• Physical Examination – don’t forget neuro exam
2. Pause here - discuss with patient/family the goals of care, hopes, expectations, anticipated course of illness. This will influence consideration of investigations and interventions
3. Investigations – X-Ray, CT, MRI, etc - if they will affect approach to care
4. Treatments – pharmacological and non-pharmacological; interventional analgesia (e.g.. Spinal)
5. Ongoing reassessment and review of options, goals, expectations, etc.

A Visual Analogue Scale Developed For Nonverbal Children – May Be Used In Nonverbal Adults

Strong Opioids• most commonly use morphine, hydromorphone, fentanyl,
methadone, oxycodone
• codeine not used; high variability in metabolizing to morphine
• usually reasonable to start with morphine, unless significant renal impairment
• caution when switching opioids – incomplete cross tolerance; consider dividing calculated dose by half
• usually divide by half when changing from oral to parenteral
• use short-acting drugs in unstable pain (or dyspnea)
• tolerance, physical dependence ≠ addiction
• prescribe laxatives concurrently

“Start Low, Go Slow”Fast”
• If you start cautiously with an anticipate ineffective dose, be prepared to titrate up quickly
• “first-dose survival test”
• Reassess early (perhaps later that day even), and consider increasing to a more “usual” dose
• Of course, rapid upwards titration of long acting drugs such as methadone or the fentanyl patch would be inappropriate; short-acting opioids are used to rapidly achieve analgesia

Opioid Dosing Considerations
• doses proportionate to the degree of distress are safe
• anticipate and preempt predictable (“incident”) pain
• dose increases 10% - 100%, depending on the context; usually should achieve steady state between increments
• breakthrough doses are 10-20% of total daily dose
• correct dose = “the one that works” within accepted adverse effects for both the regular and the breakthrough doses somewhere between “not enough” and “too much”; empirically
titrated to effect
• prn interval for breakthroughs should reflect pharmacology –i.e. when is it reasonable to repeat? (enteral 1 hr; subcut 30 min; IV 10-15 min; transmucosal 10-15 min)
• if you want to limit the # doses, do so by keeping a reasonable interval (allowing “stacking”), but limit the # doses over a period

Seizures,Death
Opioidtolerance
Mild myoclonus(eg. with sleeping)
Severe myoclonus
Delirium
Agitation
Misinterpretedas Pain
OpioidsIncreased
Hyperalgesia
Misinterpretedas Disease-Related Pain
OpioidsIncreased
Spectrum of Opioid-Induced Neurotoxicity

Adjuvant Analgesics
drugs which primarily have non pain indications but which may provide or potentiate analgesia in certain circumstances
used in pain poorly-responsive to opioids (eg. neuropathic pain), or to lower the total opioid dose and thereby mitigate opioid side effects
General / Non-specific: corticosteroids
Neuropathic Pain: gabapentin; antidepressants (TCAs; SNRIs- venlafaxine, duloxetene); ketamine; clonidine; cannabinoids
Bone Pain: bisphosphonates

Gabapentin
Common Starting Regimen
– 300 mg hs Day 1, 300 mg bid Day2, 300 mg tid Day 3, then gradually titrate to effect up to 1200 mg tid
Frail patients
– 100 mg hs Day 1, 100 mg bid Day 2, 100 mg tid Day 3, then gradually titrate to effect

Palliative Care In The Final Days

Final Common Pathway
Sudden Health ConditionsSudden Health Conditions
•non-survivable brain injury non-survivable brain injury (CVA, anoxia, trauma)(CVA, anoxia, trauma)
•sepsissepsis
•inoperable surgical conditions inoperable surgical conditions (ischemic gut or limbs)(ischemic gut or limbs)
Sudden Health ConditionsSudden Health Conditions
•non-survivable brain injury non-survivable brain injury (CVA, anoxia, trauma)(CVA, anoxia, trauma)
•sepsissepsis
•inoperable surgical conditions inoperable surgical conditions (ischemic gut or limbs)(ischemic gut or limbs)
Progressive IllnessProgressive Illness
•cancer, cancer, •neurodegenerative illnessneurodegenerative illness•organ failure (heart, organ failure (heart, kidney, lung, liver)kidney, lung, liver)
Progressive IllnessProgressive Illness
•cancer, cancer, •neurodegenerative illnessneurodegenerative illness•organ failure (heart, organ failure (heart, kidney, lung, liver)kidney, lung, liver)
• bedriddenbedridden• weak, swallowing impaired, poor airway weak, swallowing impaired, poor airway
protection, can’t clear secretions; protection, can’t clear secretions; pneumoniapneumonia – dyspnea, congestion – dyspnea, congestion
• deliriumdelirium – agitation – agitation
• bedriddenbedridden• weak, swallowing impaired, poor airway weak, swallowing impaired, poor airway
protection, can’t clear secretions; protection, can’t clear secretions; pneumoniapneumonia – dyspnea, congestion – dyspnea, congestion
• deliriumdelirium – agitation – agitation

Considerations In The Final Hours
1. Are there preexisting medical conditions needing attention in the final hours? not typically necessary to continue ongoing medical
management of underlying illnesses, with the possible exception of seizure disorder
2. What new symptoms might arise (typically dyspnea, congestion, agitated delirium – 80-90%), and related medication needs? Uncommon for pain to arise as a new symptom in final
hours What are the available routes of medications
administration?
3. Anticipated concerns of family

Role of the Health Care Provider
• Anticipate changes• Prepare a care plan for predictable issues, including:
plan for addressing loss of mobility, self-care, food/fluids medications by appropriate routes for potential symptoms Health Care Directive and/or Advance Care Plan, and
Letter of Anticipated Home Death for patients at home
• Preempt concerns/questions: what can we expect? how long can this go on? what will things look like? not eating/drinking; sleeping too much are medications causing the decline? how do we know they are comfortable? can they hear us? don’t want to miss being there at time of death

Management of SymptomsSymptomSymptom DrugDrug Non-Oral Route(s)Non-Oral Route(s)
Dyspnea opioid • sublingual (SL) – small volumes of high concentration; same dose as oral
• subcutaneous – supportable in most settings; same dose as IV = ½ po dose
• IV – limited to hospital settings• intranasal – fentanyl – lipid soluble
opioid; use same dose as IV to start• Note: Transdermal not quickly titratable
Pain opioid see above
Secretions scopolamine • subcutaneous• transdermal (patches; compounded gel)
glycopyrrolate • subcutaneous
Agitated Delirium
neuroleptic (methotrimeprazine;
haloperidol)
• SL– use same dose for all routes• subcutaneous (most settings); IV
(hospital)
lorazepam • SL – generally use with neuroleptic

● subjective experience of an uncomfortable awareness of breathing rather than an observation of increased work of breathing
● diverse potential causes - treat reversible causes, if appropriate
● oxygen can help in awake patients
● opioids: o main drug interventiono uncertain mechanismo comfort achieved before resp compromise; rate
often unchangedo may need rapid dose escalation in order to keep up
with rapidly progressing distress
Dyspnea

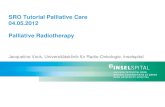
SUBCUTANEOUS MORPHINE INTERMINAL CANCER
Bruera et al. J Pain Symptom Manage. 1990; 5:341-344

Common Concerns About Aggressive Use of Opioids at End-Of-Life
• How do you know that the aggressive use of opioids for dyspnea doesn't actually bring about or speed up the patient's death?
• “I gave the last dose of morphine and he died a few minutes later… did the medication cause the death?”

1. Literature: the literature supports that opioids administered in doses proportionate to the degree of distress do not hasten death and may in fact delay death
2. Clinical context: breathing patterns usually seen in progression towards dying (clusters with apnea, irreg. pattern) vs. opioid effects (progressive slowing, regular breathing; pinpoint pupils)
3. Medication history: usually “the last dose” is the same as those given throughout recent hours/days, and was well tolerated

• Positioning
• ANTISECRETORY: − scopolamine 0.3-0.6 mg subcut q2h prn− glycopyrrolate 0.2-0.4 mg subcut q2h prn (less
sedating than scopolamine)
• Consider suctioning if secretions are: − distressing, proximal, accessible− not responding to antisecretory agents
Congestion in the Final Hours ("Death Rattle”)

1. Clinical factors: Refractory to available interventions, eg. recurrent
hypercalcemia after multiple bisphosphonate treatments
No therapeutic options available – eg. end-stage liver failure
2. Directive from patient/proxy that no further investigations be done and that interventions focus strictly on comfort
3. Limitations of care setting chosen by patient/family – e.g. a steadfast commitment to remain at home to die
What Makes A Delirium Irreversible At End Of Life?

38
● Meds titrated to effect… the correct dose is “the one that works”
● Tend to use a neuroleptic +/- benzodiazepine; subcutaneous route is most common, but can use SL
● Methotrimeprazine (Nozinan®) commonly used, as haloperidol is less sedating… however be aware that its anticholinergic effects may potentially aggravate the delirium
● Can add a benzodiazepine such as sublingual lorazepam
● Commonly need regular intermittently scheduled doses (eg. q4h or q6h) plus a prn dose of q1h prn
● prn medication orders must allow “stacking” doses… i.e. repeating a dose once its empirical effect should have occurred, yet before it has begun to lose effect
Sedation Considerations

39
● Neuroleptics methotrimeprazine (Nozinan®) 2.5 – 5 mg subcut/SL q4-8h
regularly plus q1h prn haloperidol 0.5 -1 mg subcut/SL q6-8h regularly plus q1h prn
● Benzodiazepines (not recommended for use without neuroleptic; may exacerbate agitated delirium)
lorazepam 0.5 – 1 mg SL q4-6h plus q1h prn
Examples of Sedation Orders in Final Hours
Note: •these are conservative starting doses… may need higher•some patients may just need prn dosing

40
● effective sedation changes the beside dynamics from one in which people are afraid to visit and there is no meaningful interaction to one in which people can talk, read, sing, play favourite music, pray, tell stories, touch.
● Health care team has a role in facilitating meaningful visits… family/friends may not know “the right things to do”
Supporting Families When Sedation Is Chosen

Understanding Families
Communication Patterns
Boundaries
Role flexibility
Alliances
Family rules

Resilient Families
Family Belief Systems: adversity perceived as a shared challenge; normalize distress as part of life, avoid blame
Organization Patterns: flexibility, ability to coordinate, support one another
Communication: elicit and share accurate information, tolerate and encourage open emotional expression
Zaider & Kissane(2007)

What Do Families Need?
Acknowledgement
Understanding
Trusting relationship
Communication
Teamwork
Healthy Caregivers

Reflective Activity
Am I taking care of myself well enough to do this kind of work?
Do I offer myself the same kind of compassion that I offer those in need?
When do I sit down to just sit with the reality of my vulnerability?
Chris Marchand (2008)

Exploring Obstacles to Self Care
Self care is selfish and that if you act selfishly you should feel guilty
Everyone else’s needs should be met first and then if you have time or energy left over you can look after yourself
Self care is a luxury for the rich and famous that requires huge amounts of time and money
Katherine Murray (2009)

Ask Yourself
Is this belief true?
Does this make sense?
Is this how I want things to be?
Does this belief serve me well?
Katherine Murray (2009)
Write down your favourite belief/reason for not taking care of yourself and then ask:

Self Care Begins with Self Awareness
“When we do not feel valued it is hard for us to value others.
When we feel invisible, it is hard for us to see and acknowledge others.
When our own spirits are dying of starvation, with no sign of nourishment in sight, it is impossible for us to feed and nurture the bodies and spirits of those in our care who are ill or dying.
We have nothing to give if we are literally running on empty.”
Elizabeth Causton

Exquisite Empathy
Highly present
Sensitively attuned
Well-boundaried
Heartfelt empathic engagement
Invigorated rather than depleted by connections
Kearney et al (2009)

Resources
• WRHA Palliative Care Physician Consultants are available 24/7 for physician-to-physician consults through St. Boniface Hospital Paging (204)-237-2053
• Canadian Virtual Hospice: http://virtualhospice.ca
• Hospice & Palliative Care Manitoba: http://manitobahospice.ca
• http://palliative.info - resources/presentations
• WRHA Palliative Care Education Rounds• Telehealth- every second Tuesday from 12:00-13:00• Call 204-235-3929 if questions