PAINWeek Journal, Vol 3, Q3
78
NEUROPATHIC ITCHP.20 3 WAY STREET: WHEN ACUTE PAIN BECOMES CHRONICP.36 A BANG OR A WHIMPER? HOW EXTROVERTS AND INTROVERTS MANAGE PAINP.46 DODGING ELUSIVE AND MISCALCULATED OPIOID RISKS P.56 vol.3 q 3 2015
description
Neuropathic Itch; 3 Way Street: When Acute Pain Becomes Chronic; A Bang or a Whimper? How Extroverts and Introverts Manage Pain; Dodging Elusive and Miscalculated Opioid Risks
Transcript of PAINWeek Journal, Vol 3, Q3

NEUROPATHIC ITCHP.20 3 WAY STREET: WHEN ACUTE PAIN BECOMES CHRONICP.36 A BANG OR A WHIMPER? HOW EXTROVERTS AND INTROVERTS MANAGE PAINP.46
DODGING ELUSIVE AND MISCALCULATED OPIOID RISKSP.56
vol. 3
q 3 2015
Please see Additional Warnings and Precautions on the following pages.Please read Brief Summary of Full Prescribing Information on the following pages, including Boxed Warning.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME; AND CYTOCHROME P450 3A4 INTERACTIONAddiction, Abuse, and MisuseHYSINGLA ER exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk prior to prescribing HYSINGLA ER, and monitor all patients regularly for the development of these behaviors or conditions [see Warnings and Precautions (5.1)].Life-Threatening Respiratory DepressionSerious, life-threatening, or fatal respiratory depression may occur with use of HYSINGLA ER. Monitor for respiratory depression, especially during initiation of HYSINGLA ER or following a dose increase. Instruct patients to swallow HYSINGLA ER tablets whole; crushing, chewing, or dissolving HYSINGLA ER tablets can cause rapid release and absorption of a potentially fatal dose of hydrocodone [see Warnings and Precautions (5.2)].Accidental IngestionAccidental ingestion of even one dose of HYSINGLA ER, especially by children, can result in
a fatal overdose of hydrocodone [see Warnings and Precautions (5.2)].Neonatal Opioid Withdrawal SyndromeProlonged use of HYSINGLA ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [see Warnings and Precautions (5.3)].Cytochrome P450 3A4 InteractionThe concomitant use of HYSINGLA ER with all cytochrome P450 3A4 inhibitors may result in an increase in hydrocodone plasma concentrations, which could increase or prolong adverse drug e� ects and may cause potentially fatal respiratory depression. In addition, discontinuation of a concomitantly used cytochrome P450 3A4 inducer may result in an increase in hydrocodone plasma concentration. Monitor patients receiving HYSINGLA ER and any CYP3A4 inhibitor or inducer [see Warnings and Precautions (5.11), Drug Interactions (7.1), and Clinical Pharmacology (12.3)].
INDICATIONS AND USAGE Hysingla ER (hydrocodone bitartrate) is indicated for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.Limitations of Use• Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, and because of
the greater risks of overdose and death with extended-release opioid formulations, reserve Hysingla ER for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineff ective, not tolerated, or would be otherwise inadequate to provide suffi cient management of pain.
• Hysingla ER is not indicated as an as-needed analgesic.
CONTRAINDICATIONS• Hysingla ER is contraindicated in patients with
signifi cant respiratory depression, acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment, known or suspected paralytic ileus and gastrointestinal obstruction, hypersensitivity to any component of Hysingla ER or the active ingredient, hydrocodone bitartrate.
WARNINGS AND PRECAUTIONSAddiction, Abuse, and Misuse• Hysingla ER contains hydrocodone, a Schedule II
controlled substance. Hysingla ER exposes users to the risks of opioid addiction, abuse, and misuse. As extended-release products such as Hysingla ER deliver the opioid over an extended period of time, there is a greater risk for overdose and death due to the larger amount of hydrocodone present. Addiction can occur at recommended doses and if the drug is misused or abused. Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing
Hysingla ER, and monitor all patients during therapy for the development of these behaviors or conditions. Abuse or misuse of Hysingla ER by crushing, chewing, snorting, or injecting the dissolved product will result in the uncontrolled delivery of the hydrocodone and can result in overdose and death.
Dosage and Administration • Hysingla ER tablets must be taken whole, one tablet
at a time, with enough water to ensure complete swallowing immediately after placing in the mouth. Crushing, chewing, or dissolving Hysingla ER tablets will result in uncontrolled delivery of hydrocodone and can lead to overdose or death.
Titration and Maintenance of Therapy• Continually re-evaluate patients receiving Hysingla ER
to assess the maintenance of pain control and the relative incidence of adverse reactions as well as monitoring for the development of addiction, abuse, or misuse.
For more information, visit HysinglaER.com hydrocodone
reengineered
Hysingla ER: The same opioid molecule your hydrocodone patients are familiar with• One tablet daily provides 24 hours of hydrocodone delivery
• Formulated with properties intended to make the tablet more di� cult to misuse and abuse– The in vitro data demonstrate that Hysingla ER has physical and chemical properties that are expected to
deter intranasal and intravenous abuse. The data from the clinical abuse potential studies, along with support from the in vitro data, also indicate that Hysingla ER has physicochemical properties that are expected to reduce intranasal abuse and oral abuse when chewed
– However, abuse of Hysingla ER by the intravenous, intranasal, and oral routes is still possible
– With parenteral abuse, the inactive ingredients in Hysingla ER can result in death, local tissue necrosis, infection, pulmonary granulomas, and increased risk of endocarditis and valvular heart injury
• Proven e� ective in a clinical trial
• Contains no acetaminophen
• Flexibility of 7 dosage strengths: 20, 30, 40, 60, 80, 100, and 120 mg tablets– The starting dose for patients who are not opioid tolerant is Hysingla ER 20 mg orally every 24 hours.
Opioid-tolerant patients are those receiving, for one week or longer, at least 60 mg oral morphine per day, 25 mcg transdermal fentanyl per hour, 30 mg oral oxycodone per day, 8 mg oral hydromorphone per day, 25 mg oral oxymorphone per day, or an equianalgesic dose of another opioid. Use of higher starting doses in patients who are not opioid tolerant may cause fatal respiratory depression
HYSINGLA™ ER: The fi rst and only once-daily hydrocodone
with abuse-deterrent properties and no acetaminophen
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 1 4/24/15 12:39 PM
Please see Additional Warnings and Precautions on the following pages.Please read Brief Summary of Full Prescribing Information on the following pages, including Boxed Warning.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME; AND CYTOCHROME P450 3A4 INTERACTIONAddiction, Abuse, and MisuseHYSINGLA ER exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk prior to prescribing HYSINGLA ER, and monitor all patients regularly for the development of these behaviors or conditions [see Warnings and Precautions (5.1)].Life-Threatening Respiratory DepressionSerious, life-threatening, or fatal respiratory depression may occur with use of HYSINGLA ER. Monitor for respiratory depression, especially during initiation of HYSINGLA ER or following a dose increase. Instruct patients to swallow HYSINGLA ER tablets whole; crushing, chewing, or dissolving HYSINGLA ER tablets can cause rapid release and absorption of a potentially fatal dose of hydrocodone [see Warnings and Precautions (5.2)].Accidental IngestionAccidental ingestion of even one dose of HYSINGLA ER, especially by children, can result in
a fatal overdose of hydrocodone [see Warnings and Precautions (5.2)].Neonatal Opioid Withdrawal SyndromeProlonged use of HYSINGLA ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [see Warnings and Precautions (5.3)].Cytochrome P450 3A4 InteractionThe concomitant use of HYSINGLA ER with all cytochrome P450 3A4 inhibitors may result in an increase in hydrocodone plasma concentrations, which could increase or prolong adverse drug e� ects and may cause potentially fatal respiratory depression. In addition, discontinuation of a concomitantly used cytochrome P450 3A4 inducer may result in an increase in hydrocodone plasma concentration. Monitor patients receiving HYSINGLA ER and any CYP3A4 inhibitor or inducer [see Warnings and Precautions (5.11), Drug Interactions (7.1), and Clinical Pharmacology (12.3)].
INDICATIONS AND USAGE Hysingla ER (hydrocodone bitartrate) is indicated for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.Limitations of Use• Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, and because of
the greater risks of overdose and death with extended-release opioid formulations, reserve Hysingla ER for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineff ective, not tolerated, or would be otherwise inadequate to provide suffi cient management of pain.
• Hysingla ER is not indicated as an as-needed analgesic.
CONTRAINDICATIONS• Hysingla ER is contraindicated in patients with
signifi cant respiratory depression, acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment, known or suspected paralytic ileus and gastrointestinal obstruction, hypersensitivity to any component of Hysingla ER or the active ingredient, hydrocodone bitartrate.
WARNINGS AND PRECAUTIONSAddiction, Abuse, and Misuse• Hysingla ER contains hydrocodone, a Schedule II
controlled substance. Hysingla ER exposes users to the risks of opioid addiction, abuse, and misuse. As extended-release products such as Hysingla ER deliver the opioid over an extended period of time, there is a greater risk for overdose and death due to the larger amount of hydrocodone present. Addiction can occur at recommended doses and if the drug is misused or abused. Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing
Hysingla ER, and monitor all patients during therapy for the development of these behaviors or conditions. Abuse or misuse of Hysingla ER by crushing, chewing, snorting, or injecting the dissolved product will result in the uncontrolled delivery of the hydrocodone and can result in overdose and death.
Dosage and Administration • Hysingla ER tablets must be taken whole, one tablet
at a time, with enough water to ensure complete swallowing immediately after placing in the mouth. Crushing, chewing, or dissolving Hysingla ER tablets will result in uncontrolled delivery of hydrocodone and can lead to overdose or death.
Titration and Maintenance of Therapy• Continually re-evaluate patients receiving Hysingla ER
to assess the maintenance of pain control and the relative incidence of adverse reactions as well as monitoring for the development of addiction, abuse, or misuse.
For more information, visit HysinglaER.com hydrocodone
reengineered
Hysingla ER: The same opioid molecule your hydrocodone patients are familiar with• One tablet daily provides 24 hours of hydrocodone delivery
• Formulated with properties intended to make the tablet more di� cult to misuse and abuse– The in vitro data demonstrate that Hysingla ER has physical and chemical properties that are expected to
deter intranasal and intravenous abuse. The data from the clinical abuse potential studies, along with support from the in vitro data, also indicate that Hysingla ER has physicochemical properties that are expected to reduce intranasal abuse and oral abuse when chewed
– However, abuse of Hysingla ER by the intravenous, intranasal, and oral routes is still possible
– With parenteral abuse, the inactive ingredients in Hysingla ER can result in death, local tissue necrosis, infection, pulmonary granulomas, and increased risk of endocarditis and valvular heart injury
• Proven e� ective in a clinical trial
• Contains no acetaminophen
• Flexibility of 7 dosage strengths: 20, 30, 40, 60, 80, 100, and 120 mg tablets– The starting dose for patients who are not opioid tolerant is Hysingla ER 20 mg orally every 24 hours.
Opioid-tolerant patients are those receiving, for one week or longer, at least 60 mg oral morphine per day, 25 mcg transdermal fentanyl per hour, 30 mg oral oxycodone per day, 8 mg oral hydromorphone per day, 25 mg oral oxymorphone per day, or an equianalgesic dose of another opioid. Use of higher starting doses in patients who are not opioid tolerant may cause fatal respiratory depression
HYSINGLA™ ER: The fi rst and only once-daily hydrocodone
with abuse-deterrent properties and no acetaminophen
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 1 4/24/15 12:39 PM

©2015 Purdue Pharma L.P.,Stamford, CT 06901-3431 B9935-A 4/15
Life-Threatening Respiratory Depression• Serious, life-threatening, or fatal respiratory depression
has been reported with modified-release opioids, even when used as recommended, and if not immediately recognized and treated, may lead to respiratory arrest and death. The risk of respiratory depression is greatest during the initiation of therapy or following a dose increase; therefore, closely monitor patients for respiratory depression. Proper dosing and titration of Hysingla ER are essential. Overestimating the Hysingla ER dose when converting patients from another opioid product can result in fatal overdose with the first dose. Accidental ingestion of even one dose of Hysingla ER, especially by children, can result in respiratory depression and death due to an overdose of hydrocodone.
Neonatal Opioid Withdrawal Syndrome• Prolonged use of Hysingla ER during pregnancy can
result in neonatal opioid withdrawal syndrome which may be life-threatening to the neonate if not recognized and treated, and requires management according to protocols developed by neonatology experts.
Interactions with Central Nervous System Depressants• Hypotension, profound sedation, coma, respiratory
depression, or death may result if Hysingla ER is used concomitantly with other CNS depressants, including alcohol or illicit drugs that can cause CNS depression. Start with a lower Hysingla ER dose than usual (i.e., 20-30% less), monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, and Debilitated Patients and Patients with Chronic Pulmonary Disease• Closely monitor elderly, cachectic, and debilitated
patients, and patients with chronic obstructive pulmonary disease because of the increased risk of life-threatening respiratory depression. Consider the use of alternative non-opioid analgesics in patients with chronic obstructive pulmonary disease if possible.
Use in Patients with Head Injury and Increased Intracranial Pressure• Monitor patients closely who may be susceptible to the
intracranial effects of CO2 retention (e.g., those with evidence of increased intracranial pressure or impaired consciousness). Opioids may obscure the clinical course in a patient with a head injury. Avoid the use of Hysingla ER in patients with impaired consciousness or coma.
Hypotensive Effect• Hysingla ER may cause severe hypotension, including
orthostatic hypotension and syncope in ambulatory patients. Monitor patients during dose initiation or titration. In patients with circulatory shock, Hysingla ER
may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of Hysingla ER in patients with circulatory shock.
Gastrointestinal Obstruction, Dysphagia, and Choking• Use caution when prescribing Hysingla ER for patients
who have difficulty swallowing, or have underlying gastrointestinal disorders that may predispose them to obstruction, dysphagia, or choking. Consider use of an alternative analgesic in these patients.
Decreased Bowel Motility• Hysingla ER is contraindicated in patients with
gastrointestinal obstruction, including paralytic ileus. Monitor for decreased bowel motility in post-operative patients receiving opioids. The administration of Hysingla ER may obscure the diagnosis or clinical course in patients with acute abdominal conditions. Hydrocodone may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis.
Cytochrome P450 3A4 Inhibitors and Inducers• Concomitant use of CYP3A4 inhibitors may prolong
opioid effects. Use with CYP3A4 inducers may cause lack of efficacy or development of withdrawal symptoms. If co-administration is necessary, evaluate patients frequently and consider dose adjustments until stable drug effects are achieved.
Driving and Operating Machinery• Hysingla ER may impair the mental or physical abilities
needed to perform potentially hazardous activities such as driving a car or operating machinery.
Interaction with Mixed Agonist/Antagonist Opioid Analgesics• Avoid the use of mixed agonist/antagonist analgesics in
patients who have received or are receiving Hysingla ER, as they may reduce the analgesic effect and/or precipitate withdrawal.
QTc Interval Prolongation• QTc prolongation has been observed following daily
doses of 160 mg of Hysingla ER. Avoid use in patients with congenital QTc syndrome. This observation should be considered in making clinical decisions regarding patient monitoring when prescribing Hysingla ER in patients with congestive heart failure, bradyarrhythmias, electrolyte abnormalities, or who are taking medications that are known to prolong QTc interval. In patients who develop QTc prolongation, consider reducing the dose.
ADVERSE REACTIONS• Most common treatment-emergent adverse reactions
(≥5%) reported by patients treated with Hysingla ER in the clinical trials were constipation, nausea, vomiting, fatigue, upper respiratory tract infection, dizziness, headache, and somnolence.
Please see Additional Warnings and Precautions on the preceding pages. Please read Brief Summary of Full Prescribing Information on the following pages, including Boxed Warning.
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 2 4/24/15 12:39 PM

©2015 Purdue Pharma L.P.,Stamford, CT 06901-3431 B9935-A 4/15
Life-Threatening Respiratory Depression• Serious, life-threatening, or fatal respiratory depression
has been reported with modified-release opioids, even when used as recommended, and if not immediately recognized and treated, may lead to respiratory arrest and death. The risk of respiratory depression is greatest during the initiation of therapy or following a dose increase; therefore, closely monitor patients for respiratory depression. Proper dosing and titration of Hysingla ER are essential. Overestimating the Hysingla ER dose when converting patients from another opioid product can result in fatal overdose with the first dose. Accidental ingestion of even one dose of Hysingla ER, especially by children, can result in respiratory depression and death due to an overdose of hydrocodone.
Neonatal Opioid Withdrawal Syndrome• Prolonged use of Hysingla ER during pregnancy can
result in neonatal opioid withdrawal syndrome which may be life-threatening to the neonate if not recognized and treated, and requires management according to protocols developed by neonatology experts.
Interactions with Central Nervous System Depressants• Hypotension, profound sedation, coma, respiratory
depression, or death may result if Hysingla ER is used concomitantly with other CNS depressants, including alcohol or illicit drugs that can cause CNS depression. Start with a lower Hysingla ER dose than usual (i.e., 20-30% less), monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, and Debilitated Patients and Patients with Chronic Pulmonary Disease• Closely monitor elderly, cachectic, and debilitated
patients, and patients with chronic obstructive pulmonary disease because of the increased risk of life-threatening respiratory depression. Consider the use of alternative non-opioid analgesics in patients with chronic obstructive pulmonary disease if possible.
Use in Patients with Head Injury and Increased Intracranial Pressure• Monitor patients closely who may be susceptible to the
intracranial effects of CO2 retention (e.g., those with evidence of increased intracranial pressure or impaired consciousness). Opioids may obscure the clinical course in a patient with a head injury. Avoid the use of Hysingla ER in patients with impaired consciousness or coma.
Hypotensive Effect• Hysingla ER may cause severe hypotension, including
orthostatic hypotension and syncope in ambulatory patients. Monitor patients during dose initiation or titration. In patients with circulatory shock, Hysingla ER
may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of Hysingla ER in patients with circulatory shock.
Gastrointestinal Obstruction, Dysphagia, and Choking• Use caution when prescribing Hysingla ER for patients
who have difficulty swallowing, or have underlying gastrointestinal disorders that may predispose them to obstruction, dysphagia, or choking. Consider use of an alternative analgesic in these patients.
Decreased Bowel Motility• Hysingla ER is contraindicated in patients with
gastrointestinal obstruction, including paralytic ileus. Monitor for decreased bowel motility in post-operative patients receiving opioids. The administration of Hysingla ER may obscure the diagnosis or clinical course in patients with acute abdominal conditions. Hydrocodone may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis.
Cytochrome P450 3A4 Inhibitors and Inducers• Concomitant use of CYP3A4 inhibitors may prolong
opioid effects. Use with CYP3A4 inducers may cause lack of efficacy or development of withdrawal symptoms. If co-administration is necessary, evaluate patients frequently and consider dose adjustments until stable drug effects are achieved.
Driving and Operating Machinery• Hysingla ER may impair the mental or physical abilities
needed to perform potentially hazardous activities such as driving a car or operating machinery.
Interaction with Mixed Agonist/Antagonist Opioid Analgesics• Avoid the use of mixed agonist/antagonist analgesics in
patients who have received or are receiving Hysingla ER, as they may reduce the analgesic effect and/or precipitate withdrawal.
QTc Interval Prolongation• QTc prolongation has been observed following daily
doses of 160 mg of Hysingla ER. Avoid use in patients with congenital QTc syndrome. This observation should be considered in making clinical decisions regarding patient monitoring when prescribing Hysingla ER in patients with congestive heart failure, bradyarrhythmias, electrolyte abnormalities, or who are taking medications that are known to prolong QTc interval. In patients who develop QTc prolongation, consider reducing the dose.
ADVERSE REACTIONS• Most common treatment-emergent adverse reactions
(≥5%) reported by patients treated with Hysingla ER in the clinical trials were constipation, nausea, vomiting, fatigue, upper respiratory tract infection, dizziness, headache, and somnolence.
Please see Additional Warnings and Precautions on the preceding pages. Please read Brief Summary of Full Prescribing Information on the following pages, including Boxed Warning.
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 2 4/24/15 12:39 PM
BRIEF SUMMARY OF PRESCRIBING INFORMATION (For complete details please see the Full Prescribing Information and Medication Guide.)
4 CONTRAINDICATIONS HYSINGLA ER is contraindicated in patients with: • Significant respiratory depression • Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment • Known or suspected paralytic ileus and gastrointestinal obstruction • Hypersensitivity to any component of HYSINGLA ER or the active ingredi-ent, hydrocodone bitartrate
5 WARNINGS AND PRECAUTIONS 5.1 Addiction, Abuse, and Misuse HYSINGLA ER contains hydrocodone, a Schedule II controlled substance. As an opioid, HYSINGLA ER exposes users to the risks of addiction, abuse, and misuse [see Drug Abuse and Dependence (9.1)]. As extended-release products such as HYSINGLA ER deliver the opioid over an extended period of time, there is a greater risk for overdose and death due to the larger amount of hydrocodone present. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed HYSINGLA ER and in those who obtain the drug illicitly. Addiction can occur at recommended doses and if the drug is misused or abused. Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing HYSINGLA ER, and monitor all patients receiving HYSINGLA ER for the development of these behaviors or conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol addiction or abuse) or mental illness (e.g., major depres-sion). The potential for these risks should not, however, prevent the pre-scribing of HYSINGLA ER for the proper management of pain in any given patient. Abuse or misuse of HYSINGLA ER by crushing, chewing, snorting, or injecting the dissolved product will result in the uncontrolled delivery of the hydrocodone and can result in overdose and death [see Drug Abuse and Dependence (9.1), and Overdosage (10)]. Opioid agonists are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing HYSINGLA ER. Strategies to reduce these risks include prescribing the drug in the smallest appropriate quantity and advising the patient on the proper disposal of unused drug [see Patient Counseling Information (17)]. Contact local state professional licensing board or state controlled sub-stances authority for information on how to prevent and detect abuse or diversion of this product. 5.2 Life-Threatening Respiratory Depression Serious, life-threatening, or fatal respiratory depression has been reported with the use of modified-release opioids, even when used as recommended. Respiratory depression from opioid use, if not immedi-ately recognized and treated, may lead to respiratory arrest and death. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status [see Overdosage (10.2)]. Carbon dioxide (CO2) retention from opioid-induced respiratory depression can exacerbate the
sedating effects of opioids. While serious, life-threatening, or fatal respi-ratory depression can occur at any time during the use of HYSINGLA ER, the risk is greatest during the initiation of therapy or following a dose increase. Closely monitor patients for respiratory depression when initiat-ing therapy with HYSINGLA ER and following dose increases. To reduce the risk of respiratory depression, proper dosing and titration of HYSINGLA ER are essential [see Dosage and Administration (2.1, 2.2)]. Overestimating the HYSINGLA ER dose when converting patients from another opioid product can result in fatal overdose with the first dose. Accidental inges-tion of even one dose of HYSINGLA ER, especially by children, can result in respiratory depression and death due to an overdose of hydrocodone. 5.3 Neonatal Opioid Withdrawal Syndrome Prolonged use of HYSINGLA ER during pregnancy can result in withdrawal signs in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life-threatening if not recognized and requires manage-ment according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing and amount of last maternal use, and rate of elimination of the drug by the newborn. 5.4 Interactions with Central Nervous System Depressants Hypotension, profound sedation, coma, respiratory depression, and death may result if HYSINGLA ER is used concomitantly with alcohol or other central nervous system (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, neuroleptics, other opioids). When considering the use of HYSINGLA ER in a patient taking a CNS depressant, assess the duration use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. Additionally, evaluate the patient’s use of alcohol or illicit drugs that cause CNS depression. If the decision to begin HYSINGLA ER is made, start with a lower HYSINGLA ER dose than usual (i.e., 20-30% less), monitor patients for signs of seda-tion and respiratory depression, and consider using a lower dose of the concomitant CNS depressant [see Drug Interactions (7.2)]. 5.5 Use in Elderly, Cachectic, and Debilitated Patients Life-threatening respira-tory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance compared to younger, healthier patients. Monitor such patients closely, particularly when initiating and titrating HYSINGLA ER and when HYSINGLA ER is given concomitantly with other drugs that depress respiration [see Warnings and Precautions (5.2)]. 5.6 Use in Patients with Chronic Pulmonary Disease Monitor patients with significant chronic obstructive pulmonary disease or cor pulmonale, and patients having a substantially decreased respiratory reserve, hypoxia, hypercapnia, or preexisting respiratory depression for respiratory depression, particularly when initiat-ing therapy and titrating with HYSINGLA ER, as in these patients, even usual therapeutic doses of HYSINGLA ER may decrease respiratory drive to the point of apnea [see Warnings and Precautions (5.2)]. Consider the use of alternative non-opioid analgesics in these patients if possible. 5.7 Use in Patients with Head Injury and Increased Intracranial Pressure In the presence of head injury, intracranial lesions or a preexisting increase in intracranial pressure, the possible respiratory depressant effects of opioid analgesics and their potential to elevate cerebrospinal fluid pressure (resulting from vasodilation following CO2 retention) may be markedly exaggerated. Furthermore, opioid analgesics can produce effects on pupillary response and consciousness, which may obscure neurologic signs of further increases in intracranial pressure in patients with head injuries. Monitor patients closely who may be susceptible to the intracranial effects of CO2 retention, such as those with evidence of increased intracranial pressure or impaired consciousness. Opioids may obscure the clinical course of a patient with a head injury. Avoid the use of HYSINGLA ER in patients with impaired consciousness or coma. 5.8 Hypotensive Effect HYSINGLA ER may cause severe hypotension includ-ing orthostatic hypotension and syncope in ambulatory patients. There is an added risk to individuals whose ability to maintain blood pressure has been compromised by a depleted blood volume, or after concurrent administration with drugs such as phenothiazines or other agents which compromise vasomotor tone. Monitor these patients for signs of hypotension after initiating or titrating the dose of HYSINGLA ER. In patients with circulatory shock, HYSINGLA ER may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of HYSINGLA ER in patients with circulatory shock. 5.9 Gastrointestinal Obstruction, Dysphagia, and Choking In the clinical studies with spe-cific instructions to take HYSINGLA ER with adequate water to swallow the tablet, 11 out of 2476 subjects reported difficulty swallowing HYSINGLA ER. These reports included esophageal obstruction, dysphagia, and chok-ing, one of which had required medical intervention to remove the tablet [see Adverse Reactions (6)]. Instruct patients not to pre-soak, lick, or otherwise wet HYSINGLA ER tablets prior to placing in the mouth, and to take one tablet at a time with enough water to ensure complete swallow-ing immediately after placing in the mouth [see Patient Counseling Information (17)]. Patients with underlying gastrointestinal disorders such Information (17)]. Patients with underlying gastrointestinal disorders such Information (17)]as esophageal cancer or colon cancer with a small gastrointestinal lumen are at greater risk of developing these complications. Consider use of an alternative analgesic in patients who have difficulty swallowing and patients at risk for underlying gastrointestinal disorders resulting in a small gastrointestinal lumen. 5.10 Decreased Bowel Motility HYSINGLA ER is contraindicated in patients with known or suspected gastrointestinal obstruction, including paralytic ileus. Opioids diminish propulsive peristal-tic waves in the gastrointestinal tract and decrease bowel motility. Monitor for decreased bowel motility in post-operative patients receiving opioids. The administration of HYSINGLA ER may obscure the diagnosis or clinical course in patients with acute abdominal conditions. Hydrocodone may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis. 5.11 Cytochrome P450 3A4 Inhibitors and Inducers Since the CYP3A4 isoenzyme plays a major role in the metabolism of HYSINGLA ER, drugs that alter CYP3A4 activity may cause changes in clearance of hydrocodone which could lead to changes
in hydrocodone plasma concentrations. The clinical results with CYP3A4 inhibitors show an increase in hydrocodone plasma concentrations and possibly increased or prolonged opioid effects, which could be more pronounced with concomitant use of CYP3A4 inhibitors. The expected clinical result with CYP3A4 inducers is a decrease in hydrocodone plasma concentrations, lack of efficacy or, possibly, development of an abstinence syndrome in a patient who had developed physical dependence to hydrocodone. If co-administration is necessary, caution is advised when initiating HYSINGLA ER treatment in patients currently taking, or discon-tinuing, CYP3A4 inhibitors or inducers. Evaluate these patients at frequent intervals and consider dose adjustments until stable drug effects are achieved [see Drug Interactions (7.1)]. 5.12 Driving and Operating Machinery HYSINGLA ER may impair the mental and physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Peak blood levels of hydrocodone may occur 14 – 16 hours (range 6 – 30 hours) after initial dosing of HYSINGLA ER tablet administration. Blood levels of hydrocodone, in some patients, may be high at the end of 24 hours after repeated-dose administration. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of HYSINGLA ER and know how they will react to the medication [see Clinical Pharmacology (12.3)]. 5.13 Interaction with Mixed Agonist/Antagonist Opioid Analgesics Avoid the use of mixed agonist/antagonist analgesics (i.e., pentazocine, nalbuphine, and butorphanol) in patients who have received, or are receiving, a course of therapy with a full opioid agonist analgesic, including HYSINGLA ER. In these patients, mixed agonist/antagonist analgesics may reduce the analgesic effect and/or may precipitate withdrawal symptoms. 5.14 QTc Interval Prolongation QTc prolongation has been observed with HYSINGLA ER following daily doses of 160 mg [see Clinical Pharmacology (12.2)]. This observation should be considered in making clinical decisions regarding patient monitoring when prescribing HYSINGLA ER in patients with conges-tive heart failure, bradyarrhythmias, electrolyte abnormalities, or who are taking medications that are known to prolong the QTc interval. HYSINGLA ER should be avoided in patients with congenital long QT syndrome. In patients who develop QTc prolongation, consider reducing the dose by 33 – 50%, or changing to an alternate analgesic.
6 ADVERSE REACTIONS The following serious adverse reactions are described elsewhere in the labeling: • Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)] • Life-Threatening Respiratory Depression Warnings and Precautions (5.1)] • Life-Threatening Respiratory Depression Warnings and Precautions (5.1)][see Warnings and Precautions (5.2)] • Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.3)] • Interactions with Other [see Warnings and Precautions (5.3)] • Interactions with Other [see Warnings and Precautions (5.3)]CNS Depressants [see Warnings and Precautions (5.4)] • Hypotensive [see Warnings and Precautions (5.4)] • Hypotensive [see Warnings and Precautions (5.4)]Effects [see Warnings and Precautions (5.8)] • Gastrointestinal Effects [see Warnings and Precautions (5.8)] • Gastrointestinal Effects [see Warnings and Precautions (5.8)][see Warnings and Precautions (5.9, 5.10)] 6.1 Clinical Trial Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. A total of 1,827 patients were treated with HYSINGLA ER in controlled and open-label chronic pain clinical trials. Five hundred patients were treated for 6 months and 364 patients were treated for 12 months. The clinical trial population consisted of opioid-naïve and opioid-experienced patients with persistent moderate to severe chronic pain. The common adverse reactions (≥2%) reported by patients in clinical trials comparing HYSINGLA ER (20-120 mg/day) with placebo are shown in Table 2 below:
Table 2: Adverse Reactions Reported in ≥2% of Patients during the Open-Label Titration Period and Double-Blind Treatment Period: Opioid-Naïve and Opioid-Experienced Patients
Open-label Double-blind Titration Period Treatment Period
MedDRA Placebo HYSINGLA ERPreferred Term (N=905) (N=292) (N=296)
(%) (%) (%)
Nausea 16 5 8
Constipation 9 2 3
Vomiting 7 3 6
Dizziness 7 2 3
Headache 7 2 2
Somnolence 5 1 1
Fatigue 4 1 1
Pruritus 3 <1 0
Tinnitus 2 1 2
Insomnia 2 2 3
Decreased appetite 1 1 2
Influenza 1 1 3
The adverse reactions seen in controlled and open-label chronic pain stud-ies are presented below in the following manner: most common (≥5%), common (≥1% to <5%), and less common (<1%).
The most common adverse reactions (≥5%) reported by patients treated with HYSINGLA ER in the chronic pain clinical trials were constipation, nausea, vomiting, fatigue, upper respiratory tract infection, dizziness, headache, somnolence.
The common (≥1% to <5%) adverse events reported by patients treated with HYSINGLA ER in the chronic pain clinical trials organized by MedDRA (Medical Dictionary for Regulatory Activities) System Organ Class were:
Ear and labyrinth disorders tinnitus
Gastrointestinal disorders abdominal pain, abdominal pain upper, diarrhea, dry mouth, dyspepsia, gastro-esophageal reflux disease
General disorders and administration chest pain, chills, edema site conditions peripheral, pain, pyrexia
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL
INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME; AND CYTOCHROME P450 3A4 INTERACTION
Addiction, Abuse, and MisuseAddiction, Abuse, and MisuseHYSINGLA™ ER exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk prior to pre-scribing HYSINGLA ER, and monitor all patients regularly for the development of these behaviors or conditions [see Warnings and Precautions (5.1)].Life-Threatening Respiratory DepressionLife-Threatening Respiratory DepressionSerious, life-threatening, or fatal respiratory depression may occur with use of HYSINGLA ER. Monitor for respiratory depres-sion, especially during initiation of HYSINGLA ER or following a dose increase. Instruct patients to swallow HYSINGLA ER tablets whole; crushing, chewing, or dissolving HYSINGLA ER tablets can cause rapid release and absorption of a potentially fatal dose of hydrocodone [see Warnings and Precautions (5.2)].Accidental IngestionAccidental IngestionAccidental ingestion of even one dose of HYSINGLA ER, espe-cially by children, can result in a fatal overdose of hydrocodone [see Warnings and Precautions (5.2)].Neonatal Opioid Withdrawal SyndromeNeonatal Opioid Withdrawal SyndromeProlonged use of HYSINGLA ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatol-ogy experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treat-ment will be available [see Warnings and Precautions (5.3)].Cytochrome P450 3A4 InteractionCytochrome P450 3A4 InteractionThe concomitant use of HYSINGLA ER with all cytochrome P450 3A4 inhibitors may result in an increase in hydrocodone plasma concentrations, which could increase or prolong adverse drug effects and may cause potentially fatal respiratory depres-sion. In addition, discontinuation of a concomitantly used cytochrome P450 3A4 inducer may result in an increase in hydrocodone plasma concentration. Monitor patients receiv-ing HYSINGLA ER and any CYP3A4 inhibitor or inducer [see Warnings and Precautions (5.11), Drug Interactions (7.1), and Clinical Pharmacology (12.3)].
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 3 4/24/15 12:39 PM

Infections and infestations bronchitis, gastroenteritis, gastroenteritis viral, influenza, nasopharyngitis, sinusitis, urinary tract infection
Injury, poisoning and procedural fall, muscle straincomplicationsMetabolism and nutrition disorders decreased appetite
Musculoskeletal and connective arthralgia, back pain, muscletissue disorders spasms, musculoskeletal pain,
myalgia, pain in extremity
Nervous system disorders lethargy, migraine, sedation
Psychiatric disorders anxiety, depression, insomnia
Respiratory, thoracic and mediastinal cough, nasal congestion, disorders oropharyngeal pain
Skin and subcutaneous tissue disorders hyperhidrosis, pruritus, rash
Vascular disorders hot flush, hypertension
Other less common adverse reactions that were seen in <1% of the patients in the HYSINGLA ER chronic pain clinical trials include the following in alphabetical order: abdominal discomfort, abdominal distention, agitation, asthenia, choking, confusional state, depressed mood, drug hypersensitivity, drug withdrawal syndrome, dysphagia, dyspnea, esophageal obstruction, flushing, hypogonadism, hypotension, hypoxia, irritability, libido decreased, malaise, mental impairment, mood altered, muscle twitching, edema, orthostatic hypotension, palpitations, presyncope, retching, syncope, thinking abnormal, thirst, tremor, and urinary retention.
7 DRUG INTERACTIONS 7.1 Drugs Affecting Cytochrome P450 Isoenzymes Inhibitors of CYP3A4 Co-administration of HYSINGLA ER with Inhibitors of CYP3A4 Co-administration of HYSINGLA ER with Inhibitors of CYP3A4ketoconazole, a strong CYP3A4 inhibitor, significantly increased the plasma concentrations of hydrocodone. Inhibition of CYP3A4 activity by inhibitors, such as macrolide antibiotics (e.g., erythromycin), azole-antifungal agents (e.g., ketoconazole), and protease inhibitors (e.g., ritonavir), may prolong opioid effects. Caution is advised when initiating therapy with, currently taking, or discontinuing CYP3A4 inhibitors. Evaluate these patients at fre-quent intervals and consider dose adjustments until stable drug effects are achieved [see Clinical Pharmacology (12.3)]. Inducers of CYP3A4 Inducers of CYP3A4 Inducers of CYP3A4 CYP3A4 inducers may induce the metabolism of hydrocodone and, therefore, may cause increased clearance of the drug which could lead to a decrease in hydrocodone plasma concentrations, lack of efficacy or, possibly, development of a withdrawal syndrome in a patient who had developed physical dependence to hydrocodone. If co-administration with HYSINGLA ER is necessary, monitor for signs of opioid withdrawal and consider dose adjustments until stable drug effects are achieved [see Clinical Pharmacology (12.3)]. 7.2 Central Nervous System Depressants The concomitant use of HYSINGLA ER with other CNS depressants including sedatives, hypnotics, tranquilizers, general anesthetics, phenothiazines, other opioids, and alcohol can increase the risk of respiratory depression, profound sedation, coma and death. Monitor patients receiving CNS depressants and HYSINGLA ER for signs of respiratory depression, sedation and hypotension. When combined therapy with any of the above medications is considered, the dose of one or both agents should be reduced [see Warnings and Precautions (5.4)]. 7.3 Interactions with Mixed Agonist/Antagonist and Partial Agonist Opioid Analgesics Mixed agonist/antagonist analgesics (i.e., pentazocine, nalbuphine, and butorphanol) and partial agonist analgesics (buprenorphine) may reduce the analgesic effect of HYSINGLA ER or precipitate withdrawal symptoms in these patients. Avoid the use of mixed agonist/antagonist and partial agonist analgesics in patients receiving HYSINGLA ER. 7.4 MAO Inhibitors HYSINGLA ER is not recommended for use in patients who have received MAO inhibitors within 14 days, because severe and unpredictable potentiation by MAO inhibitors has been reported with opioid analgesics. No specific interaction between hydrocodone and MAO inhibitors has been observed, but caution in the use of any opioid in patients taking this class of drugs is appropriate. 7.5 Anticholinergics Anticholinergics or other drugs with anticholinergic activity when used concurrently with opioid analgesics may increase the risk of urinary retention or severe constipation, which may lead to paralytic ileus. Monitor patients for signs of urinary retention and constipation in addition to respiratory and central nervous system depression when HYSINGLA ER is used concurrently with anticholinergic drugs. 7.6 Strong Laxatives Concomitant use of HYSINGLA ER with strong laxatives (e.g., lactulose), that rapidly increase gastrointestinal motility, may decrease hydrocodone absorption and result in decreased hydrocodone plasma levels. If HYSINGLA ER is used in these patients, closely monitor for the development of adverse events as well as changing analgesic requirements.
8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy Pregnancy Category C Risk Summary C Risk Summary C There are no adequate and well-controlled studies of HYSINGLA ER use during pregnancy. Prolonged use of opioid analgesics during pregnancy may cause neonatal opioid withdrawal syndrome. In animal reproduction studies with hydrocodone in rats and rabbits no embryotoxicity or teratogenicity was observed. However, reduced pup survival rates, reduced fetal/pup body weights, and delayed ossification were observed at doses causing maternal toxicity. In all of the studies conducted, the exposures in animals were less than the human exposure (see Animal Data). HYSINGLA ER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Clinical Considerations Considerations Considerations Fetal/neonatal adverse reactions Prolonged use of opioid analgesics during pregnancy for medical or nonmedical purposes can result in physical dependence in the neonate and neonatal opioid withdrawal syndrome shortly after birth. Observe newborns for symptoms of neonatal opioid withdrawal syndrome, such as poor feeding, diarrhea, irritability, tremor, rigidity, and seizures, and manage accordingly [see Warnings and Precautions (5.3)]. Data Animal Data No evidence of embryotoxicity or teratogenicity was observed after oral administration of hydrocodone throughout the period of organogenesis in rats and rabbits at doses up to 30 mg/kg/day (approximately 0.1 and 0.3-fold, respectively, the human hydrocodone dose of 120 mg/day based on AUC exposure comparisons).
However, in these studies, reduced fetal body weights and delayed ossifica-tion were observed in rat at 30 mg/kg/day and reduced fetal body weights were observed in in rabbit at 30 mg/kg/day (approximately 0.1 and 0.3-fold, respectively, the human hydrocodone dose of 120 mg/day based on AUC exposure comparisons). In a pre- and post-natal development study pregnant rats were administered oral hydrocodone throughout the period of gestation and lactation. At a dose of 30 mg/kg/day decreased pup viability, pup survival indices, litter size and pup body weight were observed. This dose is approximately 0.1-fold the human hydrocodone dose of 120 mg/day based on AUC exposure comparisons. 8.2 Labor and Delivery Opioids cross the placenta and may produce respiratory depression in neonates. HYSINGLA ER is not recommended for use in women immediately prior to and during labor, when use of shorter acting analgesics or other analgesic techniques are more appropriate. HYSINGLA ER may prolong labor through actions which temporarily reduce the strength, duration and frequency of uterine contractions. However, this effect is not consistent and may be offset by an increased rate of cervical dilatation, which tends to shorten labor. 8.3 Nursing Mothers Hydrocodone is present in human milk. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or to discontinue HYSINGLA ER, taking into account the importance of the drug to the mother. Infants exposed to HYSINGLA ER through breast milk should be monitored for excess sedation and respiratory depression. Withdrawal symptoms can occur in breast-fed infants when maternal administration of an opioid analgesic is stopped, or when breast-feeding is stopped. 8.4 Pediatric Use The safety and effectiveness of HYSINGLA ER in pediatric patients have not been established. Accidental ingestion of a single dose of HYSINGLA ER in children can result in a fatal overdose of hydrocodone [see Warnings and Precautions (5.2)]. HYSINGLA ER gradually forms a viscous hydrogel (i.e., a Precautions (5.2)]. HYSINGLA ER gradually forms a viscous hydrogel (i.e., a Precautions (5.2)]gelatinous mass) when exposed to water or other fluids. Pediatric patients may be at increased risk of esophageal obstruction, dysphagia, and choking because of a smaller gastrointestinal lumen if they ingest HYSINGLA ER [see Warnings and Precautions (5.9)]. 8.5 Geriatric Use In a controlled pharmacokinetic study, elderly subjects (greater than 65 years) compared to young adults had similar plasma concentrations of hydrocodone [see Clinical Pharmacology (12.3)]. Of the 1827 subjects exposed to HYSINGLA ER in the pooled chronic pain studies, 241 (13%) were age 65 and older (including those age 75 and older), while 42 (2%) were age 75 and older. In clinical trials with appropriate initiation of therapy and dose titration, no untoward or unexpected adverse reactions were seen in the elderly patients who received HYSINGLA ER. Hydrocodone may cause confusion and over-sedation in the elderly. In addition, because of the greater frequency of decreased hepatic, renal, or cardiac function, concomitant disease and concomitant use of CNS active medications, start elderly patients on low doses of HYSINGLA ER and monitor closely for adverse events such as respiratory depression, sedation, and confusion. 8.6 Hepatic Impairment No adjustment in starting dose with HYSINGLA ER is required in patients with mild or moderate hepatic impairment. Patients with severe hepatic impairment may have higher plasma concentrations than those with normal hepatic function. Initiate therapy with 1/2 the initial dose of HYSINGLA ER in patients with severe hepatic impairment and monitor closely for adverse events such as respiratory depression [see Clinical Pharmacology (12.3)]. 8.7 Renal Impairment No dose adjustment is needed in patients with mild renal impairment. Patients with moderate or severe renal impairment or end stage renal disease have higher plasma concentrations than those with normal renal function. Initiate therapy with 1/2 the initial dose of HYSINGLA ER in these patients and monitor closely for adverse events such as respiratory depression [see Clinical Pharmacology (12.3)].9 DRUG ABUSE AND DEPENDENCE 9.1 Controlled Substance HYSINGLA ER contains hydrocodone bitartrate, a Schedule II controlled substance with a high potential for abuse similar to fentanyl, methadone, morphine, oxycodone, and oxymorphone. HYSINGLA ER can be abused and is subject to misuse, abuse, addiction and criminal diversion. The high drug content in the extended-release formulation adds to the risk of adverse outcomes from abuse and misuse. 9.2 Abuse All patients treated with opioids require careful monitoring for signs of abuse and addiction, because use of opioid analgesic products carries the risk of addiction even under appropriate medical use. Drug abuse is the intentional non-therapeutic use of an over-the-counter or prescription drug, even once, for its rewarding psychological or physiological effects. Drug abuse includes, but is not limited to the following examples: the use of a prescription or over-the-counter drug to get “high,” or the use of steroids for performance enhancement and muscle build up. Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and include: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal. “Drug-seeking” behavior is very common to addicts and drug abusers. Drug seeking tactics include, but are not limited to, emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated claims of “loss” of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating physician(s). “Doctor shopping” (visiting multiple prescribers) to obtain additional prescriptions is common among drug abusers, people with untreated addiction, and criminals seeking drugs to sell. Preoccupation with achieving adequate pain relief can be appropriate behavior in a patient with poor pain control. Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true addiction. HYSINGLA ER can be diverted for non-medical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by law, is strongly advised. Proper assess-ment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures
that help to limit abuse of opioid drugs. Abuse may occur by taking intact tablets in quantities greater than prescribed or without legitimate purpose, by crushing and chewing or snorting the crushed formulation, or by injecting a solution made from the crushed formulation. The risk is increased with concurrent use of HYSINGLA ER with alcohol or other central nervous system depressants. Risks Specific to Abuse of HYSINGLA ER HYSINGLA ER is for oral use only. Abuse of HYSINGLA ER poses a risk of overdose and death.. Taking cut, broken, chewed, crushed, or dissolved HYSINGLA ER increases the risk of overdose and death. With parenteral abuse, the inactive ingredients in HYSINGLA ER can result in death, local tissue necrosis, infection, pulmonary granulomas, and increased risk of endocarditis and valvular heart injury. Parenteral drug abuse is commonly associated with transmission of infectious diseases, such as hepatitis and HIV. Abuse Deterrence Studies Summary The Summary The Summary in vitro data demonstrate in vitro data demonstrate in vitrothat HYSINGLA ER has physical and chemical properties that are expected to deter intranasal and intravenous abuse. The data from the clinical abuse potential studies, along with support from the in vitro data, also indicate in vitro data, also indicate in vitrothat HYSINGLA ER has physicochemical properties that are expected to reduce intranasal abuse and oral abuse when chewed. However, abuse of HYSINGLA ER by the intravenous, intranasal, and oral routes is still pos-sible. Additional data, including epidemiological data, when available, may provide further information on the impact of HYSINGLA ER on the abuse liability of the drug. Accordingly, this section may be updated in the future as appropriate. HYSINGLA ER contains hydrocodone, an opioid agonist and Schedule II controlled substance with an abuse liability similar to other opioid agonists, legal or illicit, including fentanyl, hydromorphone, methadone, morphine, oxycodone, and oxymorphone. HYSINGLA ER can be abused and is subject to misuse, addiction, and criminal diversion [See Warnings and Precautions (5.1) and Drug Abuse and Dependence (9)]. 9.3 Dependence Both tolerance and physical dependence can develop during chronic opioid therapy. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia (in the absence of disease progression or other external factors). Tolerance may occur to both the desired and undesired effects of drugs, and may develop at different rates for differ-ent effects. Physical dependence results in withdrawal symptoms after abrupt discontinuation or a significant dose reduction of a drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity, e.g., naloxone, nalmefene, or mixed agonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued opioid usage. HYSINGLA ER should be discontinued by a gradual downward titration [see Dosage and Administration (2.6)]. If HYSINGLA ER is abruptly discontinued in a physically dependent patient, an abstinence syndrome may occur. Some or all of the following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, piloerection, myalgia, mydriasis, irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, increased blood pressure, respiratory rate, or heart rate. Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms [see Warnings and Precautions (5.3) and Use in Specific Populations (8.3)]. 10 OVERDOSAGE 10.1 Symptoms Acute overdosage with opioids is often characterized by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and, sometimes, pulmonary edema, bradycardia, hypotension, and death. Marked mydriasis rather than miosis may be seen due to severe hypoxia in overdose situations [see Clinical Pharmacology (12.2)]. 10.2 Treatment In the treatment of HYSINGLA ER overdosage, primary attention should be given to the re-establishment of a patent airway and institution of assisted or controlled ventilation. Employ other supportive measures (including oxygen and vasopressors) in the management of circulatory shock and pulmonary edema accompanying overdose as indicated. Cardiac arrest or arrhythmias will require advanced life support techniques. The opioid antagonist naloxone hydrochloride is a specific antidote against respira-tory depression that may result from opioid overdosage. Nalmefene is an alternative opioid antagonist, which may be administered as a specific antidote to respiratory depression resulting from opioid overdose. Since the duration of action of HYSINGLA ER may exceed that of the antagonist, keep the patient under continued surveillance and administer repeated doses of the antagonist according to the antagonist labeling, as needed, to maintain adequate respiration. Opioid antagonists should not be administered in the absence of clinically significant respiratory or circulatory depression. Administer opioid antagonists cautiously to persons who are known, or suspected to be, physically dependent on HYSINGLA ER. In such cases, an abrupt or complete reversal of opioid effects may precipitate an acute abstinence syndrome. In an individual physically dependent on opioids, administration of the usual dose of the antagonist will precipitate an acute withdrawal syndrome. The severity of the withdrawal syndrome produced will depend on the degree of physical dependence and the dose of the antagonist administered. If a decision is made to treat serious respiratory depression in the physically dependent patient, administration of the antagonist should be initiated with care and by titration with smaller than usual doses of the antagonist.
CAUTION DEA FORM REQUIRED Healthcare professionals can telephone Purdue Pharma’s Medical Services Department (1-888-726-7535) for information on this product.
Purdue Pharma L.P. Stamford, CT 06901-3431
©2015, Purdue Pharma L.P.
U.S. Patent Numbers: 6,488,963; 6,733,783; 8,309,060; 8,361,499; 8,529,948; 8,551,520; 8,647,667 and 8,808,740.
This brief summary is based on Hysingla ER Prescribing Information 303511-0C, Revised 02/2015 (A)
02-13064A_R01_PHYD_JA_Asz_NewRemoved.indd 4 4/24/15 12:39 PM


8 | PWJ | www.painweek.org Q3 | 2015
EXECUTIVE EDITOR KEVIN L. ZACHAROFF MD, FACPE, FACIP, FAAP
PUBLISHER PAINWeek, 6 Erie Street, Montclair, NJ 07042
ART DIRECTOR DARRYL FOSSA
EDITORIAL DIRECTOR DEBRA WEINER
EDITOR HOLLY CASTER
Charles E. Argoff MD, CPE Professor of Neurology
Albany Medical College Department of Neurology
Director Comprehensive Pain Center
Albany Medical Center Department of Neurology
Albany, NY
Paul Arnstein RN, PhD, ACNS-BC, FNP-C, FAAN Clinical Nurse Specialist for Pain Relief
Massachusetts General Hospital Boston, MA
Said R. Beydoun MD, FAAN Professor of Neurology
Director of the Neuromuscular Program Keck Medical Center of
University of Southern California Los Angeles, CA
Jennifer Bolen JD Founder
Legal Side of Pain Knoxville, TN
Paul J. Christo MD, MBA Associate Professor
Johns Hopkins University School of Medicine Department of Anesthesiology and
Critical Care Medicine Baltimore, MD
Michael R. Clark MD, MPH, MBA Vice Chair, Clinical Affairs
Johns Hopkins University School of Medicine Department of Psychiatry and Behavioral Sciences
Director, Pain Treatment Programs Johns Hopkins Medical Institutions
Department of Psychiatry and Behavioral Sciences Baltimore, MD
Geralyn Datz PhD Affiliate
University of Southern Mississippi Department of Psychology
Clinical Director Southern Behavioral Medicine Associates
Hattiesburg, MS
Peter A. Foreman DDS, DAAPM Consultant
Rotorua Hospital and Private Practice Rotorua, New Zealand
Gary W. Jay MD, FAAPM Chief Officer
AdviseClinical Raleigh, NC
Mary Lynn McPherson PharmD, BCPS, CPE, FASPE Professor and Vice Chair
University of Maryland School of Pharmacy Department of Pharmacy Practice and Science
Hospice Consultant Pharmacist Baltimore, MD
Srinivas Nalamachu MD Clinical Assistant Professor
Kansas University Medical Center Department of Rehabilitation Medicine
Kansas City, KS President and Medical Director
International Clinical Research Institute Overland Park, KS
Bruce D. Nicholson MD Clinical Associate Professor Department of Anesthesia
Penn State College of Medicine Hershey Medical Center
Hershey, PA Director of Pain Specialists
Lehigh Valley Health Network Department of Anesthesiology
Allentown, PA
Marco Pappagallo MD Director of Medical Intelligence
Grünenthal USA Bedminster, NJ
Director Pain Management & Medical Mentoring
New Medical Home for Chronic Pain New York, NY
Steven D. Passik PhD Director of Clinical Addiction Research and Education
Millennium Laboratories San Diego, CA
John F. Peppin DO, FACP Chief Medical Officer Castle Medical, LLC
Smyrna, GA Director
The Center for Biotehics Pain Management and Medicine
University City, MO
Joseph V. Pergolizzi MD Adjunct Assistant Professor
Johns Hopkins University School of Medicine Department of Medicine
Baltimore, MD Senior Partner
Naples Anesthesia and Pain Medicine Naples, FL
Robert W. Rothrock PA-C, MPA University of Pennsylvania
Department of Anesthesiology and Critical Care Pain Medicine Division
Philadelphia, PA
Michael E. Schatman PhD, CPE, DASPE Executive Director
Foundation for Ethics in Pain Care Bellevue, WA
Sanford M. Silverman MD, PA CEO and Medical Director
Comprehensive Pain Medicine Pompano Beach, FL
Thomas B. Strouse MD Medical Director
Stewart and Lynda Resnick Neuropsychiatric Hospital at UCLA
Los Angeles, CA
EDITORIAL BOARD
Copyright © 2015, PAINWeek.
The opinions stated in the enclosed printed materials are those of the authors and do not necessarily represent the opinions of PAINWeek or its publication staff. PAINWeek does not give guarantees or any other representation that the printed material contained herein is valid, reliable, or accurate. PAINWeek does not assume any responsibility for injury arising from any use or misuse of the printed materials contained herein. The printed materials contained herein are assumed to be from
reliable sources, and there is no implication that they represent the only, or best, methodologies or procedures for the pain condition discussed. It is incumbent upon the reader to verify the accuracy of any diagnosis and drug dosage information contained herein, and to make modifications as new information arises.
All rights are reserved by PAINWeek to accept, reject, or modify any advertisement submitted for publication. It is the policy of PAINWeek to not endorse products. Any advertising herein may not be construed as an endorsement, either expressed or implied, of a product or service.

Global Education Group (Global) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education to physicians. Global Education Group designates this live activity for a minimum of 36.0 AMA PRA Category 1 Credit(s)TM. This activity will be approved for continuing pharmacy, psychology, nurse practitioner, nursing, and dentistry education. Applications for certification of social work NASW and family physician AAFP hours will be applied for. For more information and complete CME/CE accreditation details, visit our website at www.painweek.org.
The national conference on pain for frontline practitioners.

10 | PWJ | www.painweek.org Q3 | 2015
CONTENTS /PWJ/Q3/201514 | EXECUTIVE EDITOR’S LETTERby kevin l. Zacharoff
FEATURES
20 | NEUROLOGYNEUROPATHIC ITCHby charles e. Argoff
36 | EXPERT OPINION3 WAY STREET:when acute pain becomes chronicby kevin l. Zacharoff
46 | BEHAVIORALA BANG OR A WHIMPER?how extroverts and introverts manage painby michael r. Clark
56 | PHARMACOTHERAPYDODGING ELUSIVE AND MISCALCULATED OPIOID RISKSby jeffrey Fudin / thien c. Pham
64 | UPDATEPAINWEEK AT SEAby debra Weiner
SHORT CUTS
72 | ONE-MINUTE CLINICIANwith christopher m. Herndon , gary w. Jay , darren McCoy , mary lynn McPherson , mark d. Sullivan
73 | PAIN BY NUMBERS
74 | PUNDIT PROFILEwith michael m. Bottros

IndIcatIonsRELISTOR is indicated for the treatment of opioid-induced constipation in adult patients with chronic non-cancer pain. RELISTOR is indicated for the treatment of opioid-induced constipation in adult patients with advanced illness who are receiving palliative care, when response to laxative therapy has not been sufficient. Use of RELISTOR beyond four months has not been studied.IMPORTANT SAFETY INFORMATIONRELISTOR® (methylnaltrexone bromide) Subcutaneous Injection is contraindicated in patients with known or suspected gastrointestinal obstruction and patients at increased risk of recurrent obstruction, due to the potential for gastrointestinal perforation.Cases of gastrointestinal perforation have been reported in adult patients with opioid-induced constipation and advanced illness with conditions that may be associated with localized or diffuse reduction of structural integrity in the wall of the gastrointestinal tract (e.g., peptic ulcer disease, Ogilvie’s syndrome, diverticular disease, infiltrative gastrointestinal tract malignancies or peritoneal metastases). Take into account the overall risk-benefit profile when using RELISTOR
in patients with these conditions or other conditions which might result in impaired integrity of the gastrointestinal tract wall (e.g., Crohn’s disease). Monitor for the development of severe, persistent, or worsening abdominal pain; discontinue RELISTOR in patients who develop this symptom.If severe or persistent diarrhea occurs during treatment, advise patients to discontinue therapy with RELISTOR and consult their physician. Symptoms consistent with opioid withdrawal, including hyperhidrosis, chills, diarrhea, abdominal pain, anxiety, and yawning have occurred in patients treated with RELISTOR. Patients having disruptions to the blood-brain barrier may be at increased risk for opioid withdrawal and/or reduced analgesia and should be monitored for adequacy of analgesia and symptoms of opioid withdrawal. Avoid concomitant use of RELISTOR with other opioid antagonists because of the potential for additive effects of opioid receptor antagonism and increased risk of opioid withdrawal.RELISTOR may precipitate opioid withdrawal in a fetus and should be used during pregnancy only if the potential benefit justifies the potential
risk to the fetus. In nursing mothers, a decision should be made to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. In the clinical study in adult patients with opioid-induced constipation and chronic non-cancer pain, the most common adverse reactions (≥ 1%) were abdominal pain, nausea, diarrhea, hyperhidrosis, hot flush, tremor, and chills.In clinical studies in adult patients with opioid-induced constipation and advanced illness, the most common adverse reactions (≥ 5%) were abdominal pain, flatulence, nausea, dizziness, and diarrhea.Please see Brief Summary of complete Prescribing Information for RELISTOR on the adjacent page.References 1. Michna E, Blonsky ER, Schulman S, et al. Subcutaneous methylnaltrexone for the
treatment of opioid-induced constipation in patients with chronic nonmalignant pain: a randomized controlled study. J Pain. 2011;12(5):554-562.
2. RELISTOR® (methylnaltrexone bromide) Prescribing Information, Salix Pharmaceuticals, Inc.
www.salix.com 8510 Colonnade Center Drive, Raleigh, NC 27615 For additional information, call: 1-866-669-SLXP (7597) To report adverse events, call: 1-800-508-0024©2015 Salix Pharmaceuticals, Inc. All rights reserved. Printed in USA. REL-US-0099 v.3
RELIstoR helps provide chronic non-cancer pain patients with reliable and rapid relief from opioid-induced constipation–without compromising analgesia.1,2
• 6 out of 10 RELISTOR® (methylnaltrexone bromide) patients had at least 3 Spontaneous Bowel Movements (SBMs) per week1
• One-third of patients taking RELISTOR experienced an SBM within 4 hours of their first dose1
029757_salrep_sin_ad_pain_week_fa.indd 1 6/1/15 12:40 PM

The following is a brief summary only; see full Prescribing Information for complete product information.
INDICATIONS AND USAGEOpioid-Induced Constipation in Adult Patients with Chronic Non-Cancer Pain RELISTOR is indicated for the treatment of opioid-induced constipation in adult patients with chronic non-cancer pain. Opioid-Induced Constipation in Adult Patients with Advanced Illness RELISTOR is indicated for the treatment of opioid-induced constipation in adult patients with advanced illness who are receiving palliative care, when response to laxative therapy has not been sufficient.
Limitation of use: Use of RELISTOR beyond four months has not been studied in the advanced illness population.
CONTRAINDICATIONSRELISTOR is contraindicated in patients with known or suspected gastrointestinal obstruction and patients at risk of recurrent obstruction, due to the potential for gastrointestinal perforation.
WARNINGS AND PRECAUTIONSGastrointestinal PerforationCases of gastrointestinal perforation have been reported in adult patients with opioid-induced constipation and advanced illness with conditions that may be associated with localized or diffuse reduction of structural integrity in the wall of the gastrointestinal tract (e.g., peptic ulcer disease, Ogilvie’s syndrome, diverticular disease, infiltrative gastrointestinal tract malignancies or peritoneal metastases). Take into account the overall risk-benefit profile when using RELISTOR in patients with these conditions or other conditions which might result in impaired integrity of the gastrointestinal tract wall (e.g., Crohn’s disease). Monitor for the development of severe, persistent, or worsening abdominal pain; discontinue RELISTOR in patients who develop this symptom.Severe or Persistent DiarrheaIf severe or persistent diarrhea occurs during treatment, advise patients to discontinue therapy with RELISTOR and consult their healthcare provider.Opioid WithdrawalSymptoms consistent with opioid withdrawal, including hyperhidrosis, chills, diarrhea, abdominal pain, anxiety, and yawning have occurred in patients treated with RELISTOR. Patients having disruptions to the blood-brain barrier may be at increased risk for opioid withdrawal and/or reduced analgesia. Take into account the overall risk-benefit profile when using RELISTOR in such patients. Monitor for adequacy of analgesia and symptoms of opioid withdrawal in such patients.
ADVERSE REACTIONSClinical Trial ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.Opioid-Induced Constipation in Adult Patients with Chronic Non-Cancer PainThe safety of RELISTOR was evaluated in a double-blind, placebo-controlled trial in adult patients with opioid-induced constipation and chronic non-cancer pain receiving opioid analgesia. This study (Study 1) included a 4-week, double-blind, placebo controlled period in which adult patients were randomized to receive RELISTOR 12 mg once daily (150 patients) or placebo (162 patients). After 4 weeks of double-blind treatment, patients began an 8-week open-label treatment period during which RELISTOR 12 mg was administered less frequently than the recommended dosage regimen of 12 mg once daily. Adverse reactions in adult patients with opioid-induced constipation and chronic non-cancer pain receiving RELISTOR are shown in the following table. The adverse reactions in the table below may reflect symptoms of opioid withdrawal.
Adverse Reactions* in 4-Week Double-Blind, Placebo-Controlled Period of Clinical Study of RELISTOR in Adult Patients with Opioid-Induced Constipation and Chronic
Non-Cancer Pain
Adverse Reaction
RELISTOR12 mg once daily
n = 150
Placebon = 162
Abdominal Pain 21% 6%
Nausea 9% 6%
Diarrhea 6% 4%
Hyperhidrosis 6% 1%
Hot Flush 3% 2%
Tremor 1% < 1%
Chills 1% 0%* Adverse reactions occurring in ≥ 1 % of patients receiving RELISTOR 12 mg once daily and at an incidence greater than placebo.
During the 4-week double-blind period, in patients with opioid-induced constipation and chronic non-cancer pain that received RELISTOR 12 mg every other day, there was a higher incidence of adverse reactions, including nausea (12%), diarrhea (12%), vomiting (7%), tremor (3%), feeling of body temperature
change (3%), piloerection (3%), and chills (2%) as compared to daily RELISTOR dosing. Use of RELISTOR 12 mg every other day is not recommended in patients with OIC and chronic non-cancer pain. The rates of discontinuation due to adverse reactions during the double-blind period (Study 1) were higher in the RELISTOR once daily (7%) than the placebo group (3%). Abdominal pain was the most common adverse reaction resulting in discontinuation from the double-blind period in the RELISTOR once daily group (2%).The safety of RELISTOR was also evaluated in a 48-week, open-label, uncontrolled trial in 1034 adult patients with opioid-induced constipation and chronic non-cancer pain (Study 2). Patients were allowed to administer RELISTOR 12 mg less frequently than the recommended dosage regimen of 12 mg once daily, and took a median of 6 doses per week. A total of 624 patients (60%) completed at least 24 weeks of treatment and 477 (46%) completed the 48-week study. The adverse reactions seen in this study were similar to those observed during the 4-week double-blind period of Study 1. Additionally, in Study 2, investigators reported 4 myocardial infarctions (1 fatal), 1 stroke (fatal), 1 fatal cardiac arrest and 1 sudden death. It is not possible to establish a relationship between these events and RELISTOR.Opioid-Induced Constipation in Adult Patients with Advanced IllnessThe safety of RELISTOR was evaluated in two, double-blind, placebo-controlled trials in adult patients with opioid-induced constipation and advanced illness receiving palliative care: Study 3 included a single dose, double blind, placebo-controlled period, whereas Study 4 included a 14-day multiple dose, double-blind, placebo-controlled period.The most common (≥5%) adverse reactions in adult patients with opioid-induced constipation and advanced illness receiving RELISTOR are shown in the following table.
Adverse Reactions from all Doses in Double-Blind, Placebo-Controlled Clinical Studies of RELISTOR in Adult Patients with Opioid-Induced Constipation and Advanced Illness*
Adverse Reaction
RELISTORn = 165
Placebon = 123
Abdominal Pain 29% 10%
Flatulence 13% 6%
Nausea 12% 5%
Dizziness 7% 2%
Diarrhea 6% 2%
* Adverse reactions occurring in ≥ 5 % of patients receiving all doses of RELISTOR (0.075, 0.15, and 0.30 mg/kg/dose) and at an incidence greater than placebo.
The rates of discontinuation due to adverse events during the double-blind placebo controlled clinical trials (Study 3 and Study 4) were comparable between RELISTOR (1%) and placebo (2%).Postmarketing ExperienceThe following adverse reactions have been identified during post-approval use of RELISTOR. Because they are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.GastrointestinalPerforation, cramping, vomitingGeneral Disorders and Administrative Site DisordersDiaphoresis, flushing, malaise, pain. Cases of opioid withdrawal have been reported.
DRUG INTERACTIONSOther Opioid AntagonistsAvoid concomitant use of RELISTOR with other opioid antagonists because of the potential for additive effects of opioid receptor antagonism and increased risk of opioid withdrawal.Drugs Metabolized by Cytochrome P450 IsozymesIn healthy subjects, a subcutaneous dose of 0.30 mg/kg of methylnaltrexone did not significantly affect the metabolism of dextromethorphan, a CYP2D6 substrate.
USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category C There are no adequate and well-controlled studies with RELISTOR in pregnant women. The use of RELISTOR during pregnancy may precipitate opioid withdrawal in a fetus due to the immature fetal blood brain barrier. In animal reproduction studies, no effects on embryo-fetal development were observed with the administration of intravenous methylnaltrexone during organogenesis in rats and rabbits at doses up to 20 times and 26 times, respectively, the maximum recommended human dose (MRHD) of 0.2 mg/kg/day. RELISTOR should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Nursing MothersIt is not known whether RELISTOR is present in human milk. However, methylnaltrexone bromide is present in rat milk. Because of the potential for serious adverse reactions, including opioid withdrawal, in nursing infants, a decision should be made to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.Pediatric UseSafety and effectiveness of RELISTOR have not been established in pediatric patients.In juvenile rats administered intravenous methylnaltrexone bromide for 13 weeks, adverse clinical signs such as convulsions,
tremors and labored breathing were observed, and the juvenile rats were found to be more sensitive to the adverse effects of methylnaltrexone bromide when compared to adult animals. Juvenile dogs administered intravenous methylnaltrexone bromide for 13 weeks had a toxicity profile similar to adult dogs. Geriatric UseIn the double-blind studies, a total of 118 (14%) patients aged 65-74 years (79 methylnaltrexone bromide, 39 placebo) and a total of 108 (13%) patients aged 75 years or older (64 methylnaltrexone bromide, 44 placebo) were enrolled. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.Based on pharmacokinetic data, and safety and efficacy data from controlled clinical trials, no dose adjustment based on age is recommended.Renal ImpairmentNo dose adjustment is required in patients with mild or moderate renal impairment. Dose reduction by one-half is recommended in patients with severe renal impairment (creatinine clearance less than 30 mL/min as estimated by Cockcroft-Gault). Hepatic ImpairmentNo dose adjustment is required for patients with mild or moderate hepatic impairment.
OVERDOSAGEA study of healthy volunteers noted orthostatic hypotension associated with a dose of 0.64 mg/kg administered as an intravenous bolus. Monitor for signs or symptoms of orthostatic hypotension and initiate treatment as appropriate.If a patient on opioid therapy receives an overdose of RELISTOR, the patient should be monitored closely for potential evidence of opioid withdrawal symptoms such as chills, rhinorrhea, diaphoresis or reversal of central analgesic effect. Base treatment on the degree of opioid withdrawal symptoms, including changes in blood pressure and heart rate, and on the need for analgesia.
PATIENT COUNSELING INFORMATIONAdvise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).AdministrationAdvise all patients to:
• Inject RELISTOR subcutaneously in the upper arm, abdomen or thigh. Do not inject at the same spot each time (rotate injection sites).
• Safely dispose of needles by following the sharps disposal recommendations described in the RELISTOR Instructions for Use.
• Be within close proximity to toilet facilities once RELISTOR is administered.
• Discontinue RELISTOR if treatment with the opioid pain medication is also discontinued.
Advise chronic non-cancer pain patients receiving RELISTOR for opioid-induced constipation to:
• Discontinue all maintenance laxative therapy prior to initiation of RELISTOR. Laxative(s) can be used as needed if there is a suboptimal response to RELISTOR after three days.
• Inject one dose every day.• Inform their healthcare provider if their opioid regimen is
changed, to avoid adverse reactions, such as diarrhea.Advise patients with advanced illness receiving RELISTOR for opioid-induced constipation to:
• Inject one dose every other day, as needed, but no more frequently than one dose in a 24-hour period.
Gastrointestinal PerforationAdvise patients to discontinue RELISTOR and to promptly seek medical attention if they develop unusually severe, persistent, or worsening abdominal pain.Severe or Persistent DiarrheaAdvise patients to discontinue RELISTOR if they experience severe or persistent diarrhea.Opioid WithdrawalAdvise patients that symptoms consistent with opioid withdrawal may occur while taking RELISTOR, including sweating, chills, diarrhea, abdominal pain, anxiety, and yawning.PregnancyAdvise females of reproductive potential, who become pregnant or are planning to become pregnant that the use of RELISTOR during pregnancy may precipitate opioid withdrawal in a fetus due to the undeveloped blood brain barrier.NursingAdvise females who are nursing against breastfeeding during treatment with RELISTOR due to the potential for opioid withdrawal in nursing infants.You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.To report adverse events, a product complaint, or for additional information, call: 1-800-508-0024.Manufactured for: Under License from:
Salix Pharmaceuticals, Inc. Raleigh, NC 27615
Progenics Pharmaceuticals, Inc.Tarrytown, NY 10591
REL-RALAB56-102014
029757_salrep_sin_ad_pain_week_fa.indd 2 6/1/15 12:40 PM
pain
wee
kend
.org
Live conference 7.0 Ce/CMe credits
*2 day meeting = 14.0 AMA Category 1 Credits™.This activity is provided by Global Education Group. 7.o AMA Category 1 Credits™.This program was planned in accordance with AANP CE Standards and Policies and AANP Commercial Support Standard.
NeW ORLeANS LA 9.26MiLWAUKee WI 10.3WOODCLiFF LAKe NJ 10.3
SALT LAKe CiTY UT 10.10PiTTSBURGH PA 10.17BALTiMORe MD 10.24–25DALLAS TX 11.7
LeXiNGTON KY 11.7HOUSTON TX 11.14HONOLULU HI 12.5

14 | PWJ | www.painweek.org Q3 | 2015
Jeffrey Fudin and Thien Pham cover a subject that cannot and should not be overlooked in any patient with chronic pain being considered for chronic opioid therapy. I often refer to “opioid risk” as words that have morphed, over the past 10 to 15 years or more, from referring to adverse effects in the past, to aberrant drug-related behaviors in the present. I think we need to realize that probably both definitions of opioid risk are appropriate. Here, Drs. Fudin and Pham discuss opioid conversions and problems associated with a cookie-cutter approach, opioid rotation, and the physiology associated with opioid metabolism. Additional and important aspects of this piece: the role of UDT in assessing opioid risk; point of care testing that may help clinicians debunk UDT results; paths to better identifying appro-priate courses of treatment based on UDT analysis. The authors reinforce the idea that we sometimes need to think “outside the box” regarding things that can make pain treatment more safe and effective and, that despite our desire for consistency, every patient with every treatment is an individualized one.
The creation of my article about when acute pain becomes chronic pain was an educational journey for me, and I hope it will be for you. The major goal of this piece is to try to help understand the transitions that happen as the duration of pain increases, and some things we may be able to identify about patients and the likelihood of their acute pain becoming chronic, ie, “patients at risk.” I have tried to approach this in a way that combines the psychological and physical aspects of the often circuitous cycle of chronic pain, with the intention of helping the reader understand the cause and thereby understand the treatment. I compare the biomedical vs the biopsy-chosocial models for treating chronic pain, discuss the transition from acute to subacute and chronic, and, being the anesthesiologist that I am, use postoperative pain as a model. This is a complex dis-cussion, and I truly hope that, even though I have taken the liberty of oversimplifying in some cases, it is clinically relevant to you, and can make a difference in the patient’s treatment.
The Pundit Profile is something I thoroughly enjoy about every issue. This issue’s profile is with Michael M. Bottros. Dr. Bottros “had me at his first quote” of pain being such a fundamental part of medicine, and the educational deficit related to medical training about it. This is one of my particular passions and gives me hope about pain, its treatment and the future of pain management. I have to say that after reading this profile, I am experiencing the “Bottros effect.” Read this profile about this fascinating pain physician, his life, and his human aspects. After all, we are all the same and all different, but we’re all human, too.
Please do enjoy this issue. I hope to see you at the annual meeting and very much look forward to writing to you in the next issue.
—KEVIN L. ZACHAROFF
Kevin L. Zacharoff is Vice President of Medical Affairs, Inflexxion, and is a faculty member at SUNY Stony Brook School of Medicine.
KEVIN L.ZACHAROFF
MD, FACPE, FACIP, FAAP
elcome to the September issue of PWJ—PAINWeek Journal! This edition is very important to me as it coincides with the 9th PAINWeek National Conference taking place September 8–12 at The Cosmopol-itan of Las Vegas. People in the healthcare profession have individual preferences about the format in which they receive education—sometimes live, sometimes in print. I really do feel that PWJ is true to the spirit of the annual conference and a wonderful complement to it, all year long. I hope to see you in Las Vegas and get a chance to chat with you about this journal, future topics of interest, and other things relevant to pain and the “front line.”
Being the Executive Editor of PWJ is an innovative way for me to continue to learn things as well. Case in point is Charles Argoff’s article about a subject that may not come up that often, but may lie on the periphery (no pun intended) of neuropathy—neuropathic itch. I think we can all relate to the definition of itch as “an unpleasant sen-sation that induces the desire to scratch,” but we may not consider it to be something that develops after common pain related conditions, including herpes zoster, polyneuropathies, burns, keloids, etc. Dr. Argoff does a very informative job of covering the details, from defini-tion to pathophysiology to treatment and back, all with a clinical and therapeutic approach in mind. There’s a lot to be learned and I highly recommend saving the article long after the first read, if for nothing else but the medical and nonmedical treatment options.
Michael Clark, who plays an integral role in the annual meeting, discusses an engaging subject that I’ve heard him lecture about in person—patient personalities, chronic pain, and how the combi-nation of those variables may determine individual aspects of the clinician-patient relationship. This article strikes an important chord with me as it reinforces the idea that, while a mechanistic approach to treating people with pain makes sense, treating the person (as Dr. Dan Carr frequently points out) with pain from a humanistic perspective is better, especially from the point of view of personality variations or mental disorders. Dr. Clark does an excellent job of demystifying what many consider to be a complex issue regarding pain treatment and touches on things that should be considered in every case, with every patient. His position on tailoring therapies and
“helping patients shape responses instead of being a victim to them” are probably words we all need to hear more than once.
W

EXTREME LABORATORY SOLUTIONSeLab’s mission is to enable its customers by providing innovative technologies and
best of laboratory practices - with industry leading regulatory compliance.
eLab is investing today, to provide the extreme laboratory solutions which its customers will need to thrive in the ever-changing testing marketplace.
eLab continues to develop innovative software and solutions to manage critical test results data, the integration of test data with medical records systems, and to automate a wide variety of instrumentation and operational procedures for clinical reference and pain
management laboratories.
NOW OFFERING PHARMACOGENETIC TESTING FOR PATIENT DRUG METABOLISM
www.elabsolut ions.com | 866-990-ELAB (3522)

16 | PWJ | www.painweek.org Q3 | 2015
■ Jeffrey Fudin PharmD, DAAPM, FCCP, FASHP P.56Jeffrey Fudin is a Clinical Pharmacy Specialist, Pain Management, and Director, PGY2 Pain & Palliative Care Pharmacy Residency at Stratton VA Medical Center in Albany, New York. He is an adjunct associate professor at Western New England University College of Pharmacy (Springfield, MA); adjunct assistant professor of Pharmacy Practice, University of Connecticut School of Pharmacy (Storrs). Dr. Fudin coauthored his article with Thien C. Pham, PharmD, PGY2 Pharmacy Resident, Pain & Palliative Care, Stratton VA Medical Center in Albany, New York.
■ Michael R. Clark MD, MPH, MBA P.46Michael Clark is Vice Chair, Clinical Affairs, and Director of the Pain Treatment Program, Department of Psychiatry & Behavioral Sciences at Johns Hopkins Medicine in Baltimore, Maryland. Dr. Clark specializes in disorders of the special senses such as chronic pain and vestibular and balance dysfunction. He is the director of the Pain Treatment Program in the Department of Psychiatry & Behavioral Sciences and joint appointments in the Departments of Oto-laryngology/Head & Neck Surgery in the School of Medicine and Mental Health in the Johns Hopkins Bloomberg School of public health. He is a fellow of the Academy of Psychosomatic Medicine.
■ Kevin L. Zacharoff MD, FACPE, FACIP, FAAP P.36 Kevin L. Zacharoff is Vice President of Medical Affairs at Inflexxion, an active Faculty Member at the SUNY Stony Brook School of Medicine, and Chair of the Ethics Committee at St. Catherine of Siena Medical Center. He is the Executive Editor of PWJ, and firmly committed to the idea that education of frontline healthcare providers and patients is a critical component to safe, effective, and compassionate pain treatment.
■ Charles E. Argoff MD, CPE P.20Charles Argoff is Professor of Neurology, Albany Medical College.and Director, Comprehensive Pain Center, Albany Medical Center, Department of Neurology in New York. Dr. Argoff specializes in pain management and chronic headaches, predominately treating patients with chronic and neuropathic pain. Dr. Argoff’s goal is to offer patients a better quality of life through proper diagnosis and effective treatment.

PainCAS offers the “gold-standard” in opioid risk screeners, SOAPP and COMM*, as well as initial and follow up pain assessments. PainCAS produces clinician reports that track patient treatment over time and present opioid risk scores, risk stratification and monitoring recommendations
* The Screener and Opioid Assessment for Patients with Pain (SOAPP®) and the Current Opioid Misuse Measure (COMM®) are validated measures that assess the likelihood of aberrant drug-related behavior.
PainCAS, a web-based clinical tool for assessing pain and opioid risk in chronic pain patients, generates a clinician report that documents assessments for easy inclusion into the patient record.
Are you efficiently documenting pain and opioid risk assessments?
www.paincas.com 1.877.207.0645

PAINWeek® is an innovative single point of access designed specifically for frontline practitioners, recognized as a trusted resource for the latest pain management news, information, and education.
Visit www.painweek.org to access key opinion leader insights expressed via the following sections:
❶ Expert Opinion ❷ Key Topics ❸ One-Minute Clinician ❹ Pundit Profile ❺ PWJ—PAINWeek Journal
Brainfood is EVERYWHERE—at the live conferences—the PWJ—and www.painweek.org providing you with relevant information for your clinical and practice needs.
Explore the PAINWeek panorama today and get learned!
by Charles E. Argoff MD, CPE
“she scratched through her skull and meninges into her brain.”

“an unpleasant sensation that induces the desire to scratch.”
by Charles E. Argoff MD, CPE

NeUROLOGY
A 65-year-old woman with postherpetic neuralgia involving the left V1 trigeminal distribution presents to your office 12 months after the initial outbreak of herpes zoster. Al-though the rash has healed and she no longer experiences severe burning pain or tactile allodynia, she has experienced daily periods of intense itching and has been seen in an urgent care center twice because of 2 episodes of cellulitis caused by intense scratching and subsequent infection. Antihista-mines have not been helpful. Her quality of life has been significantly impaired by this persistent itch. Is this uncom-mon following PHN? Is it surprising that antihistamines are not helpful? Why is she experiencing such intense itching?
abstract: There has been much research over the past several de-cades highlighting new insights into the anatomy and physiology of itch and the clinical syndrome known as “neuropathic itch.” The purpose of this article is to review the defi-nition of the term neuropathic itch; describe proposed mechanisms, clinical conditions, and proposed treatments for neuropathic itch.
“Lesions of the peripheral nervous system are more likely to result in neuropathic itch than lesions of the central ner-vous system.”
22 | PWJ | www.painweek.org Q3 | 2015

www.painweek.org | PWJ | 23Q3 | 2015
DeFiNiTiONItch is defined as “an unpleasant sensation that induces the desire to scratch.” Although common, in some instances the
“itch” can be chronic and so intense that its presence impairs one’s quality of life.1 Itching may lead to scratching, which may lead to inflammatory changes leading to further itching. Itching can be viewed as a self-protective function, pro-tecting the skin from a possibly harmful events/substances. Although itch normally originates in the skin, the mucosa, and the conjunctiva, it can also arise from peripheral and/or central neurological lesions, such as in association with a peripheral neuropathic condition or stroke.2 Lesions of the peripheral nervous system (PNS) are more likely to result in neuropathic itch than lesions of the central nervous system (CNS). Conditions that may be associated with neuropathic pain—pain associated with a lesion or disease affecting the somatosensory system—may also be associated with neuropathic itch and, in fact, in neuropathic settings, some patients may experience pain only, pain and itch, or itch only.3,4
PATHOPHYSiOLOGYPruitogens—substances that stimulate itch—normally turn on skin receptors activating at least 2 types of C-fibers. The C-fibers that activate after local histamine application are insensitive to mechanical stimulation but are able to produce the perception of itch. Some of these C-fibers are also able to respond to heat stimuli, which may explain why heat worsens itch and cooling lessens it.5 A-delta fibers have been implicated in itch as well. The cell bodies of itch neu-rons are located in the PNS just outside the CNS; eg, for
facial itch in the trigeminal (or gasserian) ganglion or for thoracic regions in the dorsal root ganglia of spinal nerves. These ganglia send central axons into the CNS that trig-ger the perception of itch as well as the emotional aspects of the experience. As one might expect, uncontrolled and unremitting itch is NOT a pleasant experience; in fact, it can be quite disruptive.
Thus, these so-called “small fibers”—A-delta and C-fibers—have important activities not only related to pain sensations BUT also itch. They have important autonomic as well as other regulatory functions.5
Itch is the least understood of somatic sensations. Itch signal transduction involves nonneuronal mechanisms as well as sensory neurons. Keratinocytes express several neuronal sodium channels as well as TRPV3 (transient receptor potential cation channel, subfamily V, member 3) receptors that are believed to be important in creating the sensation of itch. In addition, nonneuronal cells such as mast cells are implicated in itch. Mast cells degranulate after injury, for example, releasing histamine, which in turn binds to specific receptors on small-fiber axon terminals initiating itch signal action potentials. By also releasing proinflam-matory cytokines from T-cells to further initiate inflam-mation and neural activation, and through the mast cell release of tryptase, activating the PAR-2 (protease-activated receptor 2) pathway, multiple itch augmenting processes become relevant and itch becomes more associated with his-tamine independent mechanisms. Other substances/recep-tors involved in “itch processing” include mast cell derived serotonin, several G-protein coupled receptors on primary
“Itch is the least under-stood of somatic sensations.”

24 | PWJ | www.painweek.org Q3 | 2015
afferent neurons, and the chloroquine receptor Mrgpr. The involvement of these other substances helps to explain why antihistamines and anti-inflammatory agents ARE NOT effective in the treatment of neuropathic itch!5
It is not exactly clear how information from pruritoceptive neurons travel from the PNS (skin) to the CNS (brain). Cur-rent evidence suggests that there are distinct itch neurons that process itch but not pain, as well as neurons that can process either itch or pain. Additional evidence supports that itch and pain neurons communicate with each other, eg, pain often inhibits itch and certain analgesics actually create pruritus. As previously mentioned, painful tempera-ture changes are known to modulate itch: hot (worse), cold (better). Considerable signal modulation occurs as informa-tion from itch neurons is processed through the spinal cord/brain stem to the brain. Spinal cord injuries can result in significant itching if the normal modulatory pathways are interrupted. Recent PET studies demonstrate activation of the primary but not secondary somatosensory cortex in normal adults with histamine-induced itch; very little is known about central mechanisms of neuropathic itch. The periaqueductal gray and the cingulate gyrus have also been implicated in itch.5
CLiNiCAL SYNDROMeS ASSOCiATeD WiTH NeUROPATHiC ITCHNeuropathic itch appears to be more likely to develop on the face, head, and neck compared with the lower extremities.
Many of the conditions causing neuropathic itch are accom-panied by other sensory complaints including both pain-ful and nonpainful paresthesias. One study suggested that chronic itch can impact a patient’s quality of life as sig-nificantly as chronic pain.2,5 Below are clinical conditions associated with neuropathic itch.
Postherpetic itch: more likely to occur following an out-break of shingles affecting the head or face vs thoracic dermatomes. This condition was first reported in a woman with postherpetic neuralgia involving the V1 distribution who over time, due to the severe itching, scratched through her skull and meninges into her brain. Skin biopsy around the affected site demonstrated significant cutaneous dener-vation, correlating with this patient’s apparent “painless” scratching.
Trigeminal trophic syndrome (TTS): characterized by uni-lateral itch-induced nostril erosion and ulceration with lower face anesthesia and paresthesia following trigeminal nerve surgery or alcohol injection. It has been reported in association with shingles as well. TTS can be caused by any process affecting the trigeminal ganglion and its pathways, including peripheral and central. CNS lesions resulting in TTS include multiple types of stroke (lateral medulla, lateral pons) as well as in association with various tumors.
Polyneuropathies: itch is reported to occur in approx-imately 30% of patients with peripheral neuropathies. Itch is a common side effect of certain chemotherapeutic
“…evidence supports that itch and pain neurons communicate with each other…”
NEUROLOGY

www.painweek.org | PWJ | 25Q3 | 2015
agents such as platinum compounds and paclitaxel-carbo-platin. Fabry disease, a condition with noted small-fiber (A-delta and C fiber) neuropathic changes, is also associ-ated with itch.
Brachioradial pruritus: itch combined with tingling, burn-ing, and stinging in the dorsolateral aspect of the upper arm. This condition is often associated with bilateral symptoms. Two proposed mechanisms include sun exposure (seasonal symptoms) and compression of spinal nerve roots (nonsea-sonal symptoms).
Keloids and burn scars: each of these conditions is associ-ated with cutaneous and other nerve injury and leads to itch and pain. Most patients with keloids (86%) experience itch, especially at the edge of the keloids. Some researchers have speculated small-fiber dysfunction as the cause of the itch.
Notalgia paresthetica: pruritus occurs with or without sen-sory loss in an area just medial to the scapula border often in a dermatomal distribution. This condition is believed to be associated with neuropathic changes within the posterior rami of the thoracic spinal nerves, most commonly between the 2nd and 6th thoracic vertebrae.
Spinal cord disorders: transverse myelitis, tumors, vas-cular malformations, posttraumatic and Brown-Séquard syndrome can result in neuropathic itch. Gliosis and hemo-siderin may provoke spontaneous activation of spinal itch neurons.2,5
PATieNT eVALUATiONSeveral important terms and phenomenon should be consid-ered when evaluating the patient experiencing neuropathic itch. The clinician must recognize that itch is a patient reported sensation. Nevertheless, the following terms and evaluations2 may be helpful in making the diagnosis of neu-ropathic itch:
❶ Itchy skin (alloknesis)—increased by light touch or brushing the skin around the site that itches
❷ Hyperknesis—enhanced when a prick is applied to the area that itches
❸ The scratch phenomenon—normally painful but may be actually (paradoxically) pleasurable in the setting of itch
The clinician should evaluate the patient with suspected neuropathic itch for medication and systemic medical as well as primary dermatological etiologies of neuropathic itch. An evaluation for specific neuropathic conditions associated with neuropathic itch should especially be com-pleted as well. A review of past effective and/or ineffective
treatments should be completed. It is quite likely, as noted above, that a patient experiencing neuropathic itch may respond minimally or not at all to anti-inflammatory agents or antihistamines. In some instances, referral to a neurolo-gist may be clinically helpful.
Neurodiagnostic testing such as electromyography and nerve conduction velocity studies (EMG/NCV) may be considered to evaluate for peripheral nervous system injury; however, the clinician must recognize that such testing evaluates only large myelinated nerve fibers and not small weakly myelinated or unmyelinated A-delta and C-fibers. Thus, given that neuropathic itch is an entity associated with abnormal small nerve fiber function, the EMG/NCV does not evaluate those fibers. Nevertheless, an abnormal EMG/NCV may be useful in establishing the presence of a polyneuropathy or other neuropathic state. Quantitative sensory testing (QST) is primarily a research tool used to measure thermal, mechanical, and vibratory sensory thresh-olds, and radiographic studies may at times be helpful. The emerging use of diagnostic skin biopsies to assess for the presence of small-fiber neuropathy may prove to be of great benefit in evaluating neuropathic itch.3
TReATMeNTThe treatment of neuropathic itch can be broadly divided into nonmedical and medical therapies.2,5-8
Nonmedical therapies include:
▸ Patient education re: nail cutting and wearing protective garments
▸ Use of moisturizers▸ Avoiding warm environments▸ Wearing loose fitting clothing▸ Ultraviolet B therapy (reported to benefit those with
notalgia paresthetica)
Medical therapies include:
▸ Capsaicin (8% patch)▸ Topical lidocaine, steroids, tacrolimus, amitriptyline/
ketamine cream▸ Gabapentin▸ Pregabalin, lamotrigine, carbamazepine, doxepin,
amitriptyline, nortriptyline, paroxetine (from anecdotal reports)
▸ Thalidomide, in refractory states▸ Subcutaneous botulinum toxin▸ Epidural clonidine/bupivacaine▸ Stellate ganglion blocks▸ Microsurgical decompression for notalgia paresthetica▸ Neurostimulation▸ Transcranial direct current stimulation▸ Low-dose naloxone

26 | PWJ | www.painweek.org Q3 | 2015
NEUROLOGY
Antihistamines generally do not help patients with neuropathic itch. There is currently no FDA approved treatment specifically for neuropathic itch, and the treatments noted above have been evaluated primarily in small clinical studies or case reports only; thus, the evidence base for treatment of neuropathic is lacking.
CONCLUSiONSNeuropathic itch is associated with multiple neuro-pathic conditions affecting both the peripheral and central nervous systems. Although the precise mech-anism(s) are uncertain, there is clear overlap as well as differences between neuropathic itch and pain. Given that it can be as disabling as chronic pain, it is important that neuropathic itch be recognized by a wide variety of clinicians, including primary care providers and specialists, so that the diagnosis can be made and available treatments can be implemented. Basic and clinical research opportunities abound and hopefully will lead to an improved understanding of the mechanism(s)—and more effective treatment—of neuropathic itch in the future.
References
1. Ikoma A. Updated neurophysiology of itch. Biol Pharm Bull. 2013;36(8):1235–1240.
2. Dhand A, Aminoff MJ. The neurology of Itch. Brain. 2014;137(pt 2):313–322.
3. Oaklander AL. Neuropathic itch. In: Carstens E, Akiyama T, eds. Itch: Mechanisms and Treatment. Boca Raton, FL: CRC Press; 2014.
4. Schmeltz M. Itch and pain differences and commonalities. Handb Exp Pharmacol. 2015;227:285–301.
5. Oaklander AL Common neuropathic itch syndromes. Acta Derm Venereol. 2012;92:118–125.
6. Knotkova H, Portenoy RK, Cruciani RA. Transcranial direct current stimulation (tDCS) relieved itching in a patient with chronic neuropathic pain. Clin J Pain. 2013;29(7):621–622.
7. Griffin JR, Davis MD. Amitriptylne/ketamine as therapy for neuropathic pruritus and pain secondary to herpes zoster. J Drugs Dermatol. 2015;14(2):115–118.
8. Misery L, Erfan N, Castela E, et al. Successful treatment of refractory neuropathic pruritus with capsaicin 8%: a bicentric retrospective study with long-term follow-up. Acta Derm Venereol. 2015; Mar 5. [Epub ahead of print]
Be more than an informed clinician.
LearnMore.VisitWWW. PAINEDUCATORS. ORG
AM
ERIC
AN
SO
CIE
TY
OF
PAIN
ED
UC
ATO
RS
Become a Certified Pain Educator

Endura MD Mass Spectrometer ClinQuan MD SoftwarePrelude MD HPLC
For in vitro diagnostic use. Not available in all countries.
Thermo Fisher Scientific, San Jose, CA USA is ISO 13485 Certified.
ISO 13485
AD64157-EN 0615S-Rev.C
© 2
015
Ther
mo
Fish
er S
cien
tific
Inc.
All
right
s re
serv
ed. A
ll tr
adem
arks
are
the
prop
erty
of
Ther
mo
Fish
er S
cien
tific
Inc.
and
its
subs
idia
ries.
Cop
yrig
hts
in a
nd to
imag
ery
are
owne
d by
third
par
ties
incl
udin
g S
hutt
erst
ock,
and
are
lice
nsed
for
limite
d us
e on
ly to
The
rmo
Fish
er S
cien
tific.
Confidence in ResultsAchieve greater productivity and confidence when providing laboratory-developed test results to
the healthcare professionals you serve. New Thermo Scientific™ high-performance Class I medical
devices for in vitro diagnostic use — Thermo Scientific™ Prelude LX-4 MD™ HPLC, Thermo Scientific™
Prelude MD™ HPLC, Thermo Scientific™ Endura MD™ mass spectrometer, and Thermo Scientific™
ClinQuan MD™ software – help you deliver LC-MS results easily, quickly, and with more confidence.
• thermoscientific.com/LCMS-IVD
LC-MS for in vitro diagnostic use
Prelude LX-4 MD HPLC

TIME TO DUAL
Limitations of Use• Because of the risks of addiction, abuse, and
misuse with opioids, even at recommended doses, and because of the greater risks of overdose and death with extended-release opioid formulations, reserve NUCYNTA® ER for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain
• NUCYNTA® ER is not indicated as an as-needed (prn) analgesic
Not an actual patient.
NUCYNTA® ER is the first and only FDA-approved long-acting opioid designed to control both nociceptive pain and the neuropathic pain associated with diabetic peripheral neuropathy (DPN).
NUCYNTA® ER is an opioid agonist indicated for the management of:
• pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate
• neuropathic pain associated with diabetic peripheral neuropathy (DPN) in adults severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate
Please see additional Important Safety Information and Brief Summary, including BOXED WARNING, on the following pages.
TWO SOURCESOF PAIN
ONE SOURCE OF RELIEF
PRESCRIBE NUCYNTA® ER FOR ONE SOURCE OF RELIEF • Proven efficacy in chronic low back pain and DPN1,2
- Based on efficacy demonstrated in a prospective, randomized, double-blind, active- and placebo-controlled, multicenter phase 3 chronic low back pain study (N=981) showing significant change in mean pain intensity from baseline in Week 15 (Week 12 of the maintenance phase) vs placebo1
- Based on efficacy demonstrated in a double-blind, parallel-group, enriched-enrollment randomized phase 3 DPN study (N=977) showing significant change in mean pain intensity over the last week of the 12-week, double-blind, maintenance phase vs placebo2
• 5 dosage strengths: 50 mg, 100 mg, 150 mg, 200 mg, and 250 mg3* Individualize dosing based on patient’s prior analgesic treatment experience and risk
factors for addiction, abuse, and misuse; titrate as needed to provide adequate analgesia and minimize adverse reactions
• Administer NUCYNTA® ER ~q12h3
*Please see full Prescribing Information for DOSAGE AND ADMINISTRATION.† Some restrictions and limitations apply. See full terms and conditions available at NUCYNTA.com. Available to commercially insured and cash-paying patients only. Patients covered by Medicare, Medicaid, or any other state- or federally funded benefit program are excluded. Patients must be 18 years of age or older. This promotion cannot be combined with any other programs, offers, or discounts. Depomed reserves the right to rescind, revoke, or amend this offer without further notice.
‡ Source: MMIT 2.0, May 2015.
References: 1. Buynak R, Shapiro DY, Okamoto A, et al. Efficacy and safety of tapentadol extended release for the management of chronic low back pain: results of a prospective, randomized, double-blind, placebo- and active-controlled Phase Ill study. Expert Opin Pharmocother. 2010;11(11):1787-1804. 2. Schwartz S, Etropolski M, Shapiro DY, et al. Safety and efficacy of tapentadol ER in patients with painful diabetic peripheral neuropathy: results of a randomized-withdrawal, placebo-controlled trial. Curr Med Res Opin. 2011;27(1):151-162. 3. NUCYNTA® ER [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2014.
COVERED FOR
94%OF COMMERCIALLY
INSURED PATIENTS.‡
PREFERRED FOR UNITEDHEALTH
GROUP AND SILVERSCRIPT/
CVS CAREMARK PART D PLANS‡
CONTRAINDICATIONS: Significant respiratory depression; acute or severe bronchial asthma or hypercarbia in an unmonitored setting or in the absence of resuscitative equipment; known or suspected paralytic ileus; hypersensitivity (e.g., anaphylaxis, angioedema) to tapentadol or to any other ingredients of the product; concurrent use of monoamine oxidase inhibitors (MAOIs) or use within the last 14 days.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and
INTERACTION WITH ALCOHOLSee full prescribing information for complete boxed warning.
• NUCYNTA® ER exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing, and monitor regularly for development of these behaviors or conditions. (5.1)
• Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Instruct patients to swallow NUCYNTA® ER tablets whole to avoid exposure to a potentially fatal dose of tapentadol. (5.2)
• Accidental ingestion of NUCYNTA® ER, especially in children, can result in fatal overdose of tapentadol. (5.2)
• Prolonged use of NUCYNTA® ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. (5.3)
• Instruct patients not to consume alcohol or any products containing alcohol while taking NUCYNTA® ER because co-ingestion can result in fatal plasma tapentadol levels. (5.4)
VISIT NUCYNTA.COM FOR MORE INFORMATION AND TO DOWNLOAD A NUCYNTA® ER SAVINGS CARD†
• $0 co-pay for first prescription of NUCYNTA® ER with a $25 co-pay on each additional prescription if eligible†
Nuc_PainWeekJourn.indd 1 7/27/15 11:40 AM
TIME TO DUAL
Limitations of Use• Because of the risks of addiction, abuse, and
misuse with opioids, even at recommended doses, and because of the greater risks of overdose and death with extended-release opioid formulations, reserve NUCYNTA® ER for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain
• NUCYNTA® ER is not indicated as an as-needed (prn) analgesic
Not an actual patient.
NUCYNTA® ER is the first and only FDA-approved long-acting opioid designed to control both nociceptive pain and the neuropathic pain associated with diabetic peripheral neuropathy (DPN).
NUCYNTA® ER is an opioid agonist indicated for the management of:
• pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate
• neuropathic pain associated with diabetic peripheral neuropathy (DPN) in adults severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate
Please see additional Important Safety Information and Brief Summary, including BOXED WARNING, on the following pages.
TWO SOURCESOF PAIN
ONE SOURCE OF RELIEF
PRESCRIBE NUCYNTA® ER FOR ONE SOURCE OF RELIEF • Proven efficacy in chronic low back pain and DPN1,2
- Based on efficacy demonstrated in a prospective, randomized, double-blind, active- and placebo-controlled, multicenter phase 3 chronic low back pain study (N=981) showing significant change in mean pain intensity from baseline in Week 15 (Week 12 of the maintenance phase) vs placebo1
- Based on efficacy demonstrated in a double-blind, parallel-group, enriched-enrollment randomized phase 3 DPN study (N=977) showing significant change in mean pain intensity over the last week of the 12-week, double-blind, maintenance phase vs placebo2
• 5 dosage strengths: 50 mg, 100 mg, 150 mg, 200 mg, and 250 mg3* Individualize dosing based on patient’s prior analgesic treatment experience and risk
factors for addiction, abuse, and misuse; titrate as needed to provide adequate analgesia and minimize adverse reactions
• Administer NUCYNTA® ER ~q12h3
*Please see full Prescribing Information for DOSAGE AND ADMINISTRATION.† Some restrictions and limitations apply. See full terms and conditions available at NUCYNTA.com. Available to commercially insured and cash-paying patients only. Patients covered by Medicare, Medicaid, or any other state- or federally funded benefit program are excluded. Patients must be 18 years of age or older. This promotion cannot be combined with any other programs, offers, or discounts. Depomed reserves the right to rescind, revoke, or amend this offer without further notice.
‡ Source: MMIT 2.0, May 2015.
References: 1. Buynak R, Shapiro DY, Okamoto A, et al. Efficacy and safety of tapentadol extended release for the management of chronic low back pain: results of a prospective, randomized, double-blind, placebo- and active-controlled Phase Ill study. Expert Opin Pharmocother. 2010;11(11):1787-1804. 2. Schwartz S, Etropolski M, Shapiro DY, et al. Safety and efficacy of tapentadol ER in patients with painful diabetic peripheral neuropathy: results of a randomized-withdrawal, placebo-controlled trial. Curr Med Res Opin. 2011;27(1):151-162. 3. NUCYNTA® ER [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2014.
COVERED FOR
94%OF COMMERCIALLY
INSURED PATIENTS.‡
PREFERRED FOR UNITEDHEALTH
GROUP AND SILVERSCRIPT/
CVS CAREMARK PART D PLANS‡
CONTRAINDICATIONS: Significant respiratory depression; acute or severe bronchial asthma or hypercarbia in an unmonitored setting or in the absence of resuscitative equipment; known or suspected paralytic ileus; hypersensitivity (e.g., anaphylaxis, angioedema) to tapentadol or to any other ingredients of the product; concurrent use of monoamine oxidase inhibitors (MAOIs) or use within the last 14 days.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and
INTERACTION WITH ALCOHOLSee full prescribing information for complete boxed warning.
• NUCYNTA® ER exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing, and monitor regularly for development of these behaviors or conditions. (5.1)
• Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Instruct patients to swallow NUCYNTA® ER tablets whole to avoid exposure to a potentially fatal dose of tapentadol. (5.2)
• Accidental ingestion of NUCYNTA® ER, especially in children, can result in fatal overdose of tapentadol. (5.2)
• Prolonged use of NUCYNTA® ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. (5.3)
• Instruct patients not to consume alcohol or any products containing alcohol while taking NUCYNTA® ER because co-ingestion can result in fatal plasma tapentadol levels. (5.4)
VISIT NUCYNTA.COM FOR MORE INFORMATION AND TO DOWNLOAD A NUCYNTA® ER SAVINGS CARD†
• $0 co-pay for first prescription of NUCYNTA® ER with a $25 co-pay on each additional prescription if eligible†
Nuc_PainWeekJourn.indd 1 7/27/15 11:40 AM

NUCYNTA® ER (tapentadol) IMPORTANT SAFETY INFORMATION (continued)
WARNINGS AND PRECAUTIONS: Addiction, Abuse, and Misuse: NUCYNTA® ER contains tapentadol, an opioid agonist and a Schedule II controlled substance that can be abused in a manner similar to other opioid agonists, legal or illicit. There is a greater risk for overdose and death due to the larger amount of tapentadol present in NUCYNTA® ER. Assess risk for opioid abuse or addiction prior to prescribing NUCYNTA® ER. Addiction can occur in patients appropriately prescribed NUCYNTA® ER at recommended doses; in those who obtain the drug illicitly; and if the drug is misused or abused. Therefore, routinely monitor for signs of misuse, abuse, and addiction. Patients at increased risk (e.g., patients with a personal or family history of substance abuse or mental illness) may be prescribed NUCYNTA® ER, but use in such patients necessitates intensive counseling about the risks and proper use along with intensive monitoring for signs of addiction, abuse, and misuse.
Life-threatening Respiratory Depression: Can occur at any time during the use of NUCYNTA® ER even when used as recommended. Respiratory depression from opioid use, if not immediately recognized and treated, may lead to respiratory arrest and death. To reduce the risk of respiratory depression, proper dosing and titration are essential. Overestimating the dose when converting patients from another opioid product can result in fatal overdose with the first dose. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status.
Neonatal Opioid Withdrawal Syndrome: Prolonged use of NUCYNTA® ER during pregnancy can result in withdrawal signs in the neonate, which may be life-threatening and require management according to protocols developed by neonatology experts. Neonatal opioid withdrawal syndrome presents as poor feeding, irritability, hyperactivity and abnormal sleep pattern, high-pitched cry, tremor, rigidity, seizures, vomiting, diarrhea, and failure to gain weight.
Interactions With Central Nervous System Depressants: Hypotension, profound sedation, coma, respiratory depression, and death may result if NUCYNTA® ER is used concomitantly with alcohol or other central nervous system (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, tranquilizers, general anesthetics, neuroleptics, other opioids). When considering the use of NUCYNTA® ER in a patient taking a CNS depressant, assess the duration of use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. If the decision to begin NUCYNTA® ER is made, start with NUCYNTA® ER 50 mg every 12 hours, monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, or Debilitated Patients: Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance. Because elderly patients are more likely to have decreased renal and hepatic function, consideration should be given to starting elderly patients in the lower range of recommended doses. Closely monitor these patients, particularly when initiating and titrating NUCYNTA® ER and when given concomitantly with other drugs that depress respiration.
Use in Patients With Chronic Pulmonary Disease: Patients with significant chronic obstructive pulmonary disease or cor pulmonale and patients having a substantially decreased respiratory reserve, hypoxia, hypercarbia, or pre-existing respiratory depression, should be monitored for respiratory depression particularly when initiating therapy and titrating with NUCYNTA® ER. Consider the use of alternative nonopioid analgesics in these patients.
Hypotensive Effect: May cause severe hypotension. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor for signs of hypotension during dose initiation or titration. Avoid use in patients with circulatory shock; may cause vasodilation that can further reduce cardiac output and blood pressure.
Use in Patients With Head Injury or Increased Intracranial Pressure: Monitor patients who may be susceptible to the intracranial effects of CO
2
retention (e.g., those with evidence of increased intracranial pressure or brain tumors) for signs of sedation and respiratory depression, particularly when initiating therapy. NUCYNTA® ER may reduce respiratory drive, and the resultant CO
2
retention can further increase intracranial pressure. Opioids may also obscure the clinical course in a patient with a head injury.
Seizures: May aggravate convulsions in patients with convulsive disorders and may induce or aggravate seizures. Monitor patients with a history of seizure disorders for worsened seizure control during therapy.
Serotonin Syndrome: Cases of life-threatening serotonin syndrome have been reported with the concurrent use of NUCYNTA® ER and serotonergic drugs. Serotonergic drugs comprise selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, drugs that affect the serotonergic neurotransmitter system, and drugs that impair metabolism of serotonin (including MAOIs). This may occur within the recommended dose. Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g.,
tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination), and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea) and can be fatal. If concomitant treatment with SSRIs, SNRIs, TCAs, or triptans is clinically warranted, careful observation of the patient is advised, particularly when initiating or titrating the dose.
Use in Patients With Gastrointestinal (GI) Conditions: Contraindicated in patients with Gl obstruction including paralytic ileus; may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms.
Avoidance of Withdrawal: Withdrawal symptoms (e.g., anxiety, sweating, insomnia, restlessness, pain, nausea, tremors, diarrhea, upper respiratory symptoms, piloerection) may occur:
• After abrupt discontinuation or a significant dose reduction of NUCYNTA® ER in physically dependent patients. When discontinuing NUCYNTA® ER, gradually taper the dose.
• If mixed agonist/antagonist (e.g., butorphanol, nalbuphine, pentazocine) and partial agonist (e.g., buprenorphine) analgesics are used in patients who have received or are receiving NUCYNTA® ER. Avoid use with mixed agonists/antagonists and partial agonists.
• If opioid antagonists (e.g., naloxone, nalmefene) are administered in physically dependent patients. Administration of the antagonist should be begun with care and by titration with smaller than usual doses of the antagonist.
Driving and Operating Heavy Machinery: May impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of NUCYNTA® ER and know how they will react to the medication.
Hepatic Impairment: Avoid use in patients with severe hepatic impairment (Child-Pugh Score 10 to 15). In patients with moderate hepatic impairment (Child-Pugh Score 7-9), initiate treatment with NUCYNTA® ER 50 mg no more than once every 24 hours, with a maximum dose of 100 mg per day. Monitor for respiratory and CNS depression when initiating and titrating NUCYNTA® ER.
Renal Impairment: Use in patients with severe renal impairment (CL
CR <30 mL/min) is not recommended
due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
DRUG INTERACTIONS
Alcohol: See BOXED WARNING.
Muscle Relaxants: Monitor patients receiving muscle relaxants and NUCYNTA® ER for signs of respiratory depression that may be greater than otherwise expected. Tapentadol may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression.
Anticholinergics: Use with anticholinergic products may increase the risk of urinary retention and/or severe constipation, which may lead to paralytic ileus.
USE IN SPECIFIC POPULATIONS
Pregnancy/Nursing Mothers: Pregnancy Category C. NUCYNTA® ER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Neonates born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms. Observe newborns for symptoms of neonatal opioid withdrawal syndrome. Withdrawal symptoms can occur in breast-feeding infants when maternal administration of NUCYNTA® ER is stopped.
Labor and Delivery: Opioids cross the placenta and may produce respiratory depression in neonates. NUCYNTA® ER is not for use in women during and immediately prior to labor, when shorter-acting analgesics or other analgesic techniques are more appropriate.
Use in Elderly, Renal Impairment, and Hepatic Impairment: See WARNINGS AND PRECAUTIONS.
DRUG ABUSE AND DEPENDENCE: See BOXED WARNING
OVERDOSAGE: Institute supportive measures to manage respiratory depression, circulatory shock, and pulmonary edema as required. The opioid antagonists, naloxone or nalmefene, are specific antidotes to respiratory depression.
ADVERSE REACTIONS: In clinical studies, the most common (≥10%) adverse reactions were nausea, constipation, vomiting, dizziness, somnolence, and headache.
Select Postmarketing Adverse Reactions: Anaphylaxis, angioedema, and anaphylactic shock have been reported very rarely with ingredients contained in NUCYNTA® ER. Advise patients how to recognize such reactions and when to seek medical attention. Panic attack has also been reported.
© July 2015, Depomed, Inc. All rights reserved. APL-NUCX-0029 Rev.2
Please see Brief Summary, including BOXED WARNING, on the following pages.
Nuc_PainWeekJourn.indd 2 7/27/15 11:40 AM

NUCYNTA® ER (tapentadol) IMPORTANT SAFETY INFORMATION (continued)
WARNINGS AND PRECAUTIONS: Addiction, Abuse, and Misuse: NUCYNTA® ER contains tapentadol, an opioid agonist and a Schedule II controlled substance that can be abused in a manner similar to other opioid agonists, legal or illicit. There is a greater risk for overdose and death due to the larger amount of tapentadol present in NUCYNTA® ER. Assess risk for opioid abuse or addiction prior to prescribing NUCYNTA® ER. Addiction can occur in patients appropriately prescribed NUCYNTA® ER at recommended doses; in those who obtain the drug illicitly; and if the drug is misused or abused. Therefore, routinely monitor for signs of misuse, abuse, and addiction. Patients at increased risk (e.g., patients with a personal or family history of substance abuse or mental illness) may be prescribed NUCYNTA® ER, but use in such patients necessitates intensive counseling about the risks and proper use along with intensive monitoring for signs of addiction, abuse, and misuse.
Life-threatening Respiratory Depression: Can occur at any time during the use of NUCYNTA® ER even when used as recommended. Respiratory depression from opioid use, if not immediately recognized and treated, may lead to respiratory arrest and death. To reduce the risk of respiratory depression, proper dosing and titration are essential. Overestimating the dose when converting patients from another opioid product can result in fatal overdose with the first dose. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status.
Neonatal Opioid Withdrawal Syndrome: Prolonged use of NUCYNTA® ER during pregnancy can result in withdrawal signs in the neonate, which may be life-threatening and require management according to protocols developed by neonatology experts. Neonatal opioid withdrawal syndrome presents as poor feeding, irritability, hyperactivity and abnormal sleep pattern, high-pitched cry, tremor, rigidity, seizures, vomiting, diarrhea, and failure to gain weight.
Interactions With Central Nervous System Depressants: Hypotension, profound sedation, coma, respiratory depression, and death may result if NUCYNTA® ER is used concomitantly with alcohol or other central nervous system (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, tranquilizers, general anesthetics, neuroleptics, other opioids). When considering the use of NUCYNTA® ER in a patient taking a CNS depressant, assess the duration of use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. If the decision to begin NUCYNTA® ER is made, start with NUCYNTA® ER 50 mg every 12 hours, monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, or Debilitated Patients: Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance. Because elderly patients are more likely to have decreased renal and hepatic function, consideration should be given to starting elderly patients in the lower range of recommended doses. Closely monitor these patients, particularly when initiating and titrating NUCYNTA® ER and when given concomitantly with other drugs that depress respiration.
Use in Patients With Chronic Pulmonary Disease: Patients with significant chronic obstructive pulmonary disease or cor pulmonale and patients having a substantially decreased respiratory reserve, hypoxia, hypercarbia, or pre-existing respiratory depression, should be monitored for respiratory depression particularly when initiating therapy and titrating with NUCYNTA® ER. Consider the use of alternative nonopioid analgesics in these patients.
Hypotensive Effect: May cause severe hypotension. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor for signs of hypotension during dose initiation or titration. Avoid use in patients with circulatory shock; may cause vasodilation that can further reduce cardiac output and blood pressure.
Use in Patients With Head Injury or Increased Intracranial Pressure: Monitor patients who may be susceptible to the intracranial effects of CO
2
retention (e.g., those with evidence of increased intracranial pressure or brain tumors) for signs of sedation and respiratory depression, particularly when initiating therapy. NUCYNTA® ER may reduce respiratory drive, and the resultant CO
2
retention can further increase intracranial pressure. Opioids may also obscure the clinical course in a patient with a head injury.
Seizures: May aggravate convulsions in patients with convulsive disorders and may induce or aggravate seizures. Monitor patients with a history of seizure disorders for worsened seizure control during therapy.
Serotonin Syndrome: Cases of life-threatening serotonin syndrome have been reported with the concurrent use of NUCYNTA® ER and serotonergic drugs. Serotonergic drugs comprise selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, drugs that affect the serotonergic neurotransmitter system, and drugs that impair metabolism of serotonin (including MAOIs). This may occur within the recommended dose. Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g.,
tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination), and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea) and can be fatal. If concomitant treatment with SSRIs, SNRIs, TCAs, or triptans is clinically warranted, careful observation of the patient is advised, particularly when initiating or titrating the dose.
Use in Patients With Gastrointestinal (GI) Conditions: Contraindicated in patients with Gl obstruction including paralytic ileus; may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms.
Avoidance of Withdrawal: Withdrawal symptoms (e.g., anxiety, sweating, insomnia, restlessness, pain, nausea, tremors, diarrhea, upper respiratory symptoms, piloerection) may occur:
• After abrupt discontinuation or a significant dose reduction of NUCYNTA® ER in physically dependent patients. When discontinuing NUCYNTA® ER, gradually taper the dose.
• If mixed agonist/antagonist (e.g., butorphanol, nalbuphine, pentazocine) and partial agonist (e.g., buprenorphine) analgesics are used in patients who have received or are receiving NUCYNTA® ER. Avoid use with mixed agonists/antagonists and partial agonists.
• If opioid antagonists (e.g., naloxone, nalmefene) are administered in physically dependent patients. Administration of the antagonist should be begun with care and by titration with smaller than usual doses of the antagonist.
Driving and Operating Heavy Machinery: May impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of NUCYNTA® ER and know how they will react to the medication.
Hepatic Impairment: Avoid use in patients with severe hepatic impairment (Child-Pugh Score 10 to 15). In patients with moderate hepatic impairment (Child-Pugh Score 7-9), initiate treatment with NUCYNTA® ER 50 mg no more than once every 24 hours, with a maximum dose of 100 mg per day. Monitor for respiratory and CNS depression when initiating and titrating NUCYNTA® ER.
Renal Impairment: Use in patients with severe renal impairment (CL
CR <30 mL/min) is not recommended
due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
DRUG INTERACTIONS
Alcohol: See BOXED WARNING.
Muscle Relaxants: Monitor patients receiving muscle relaxants and NUCYNTA® ER for signs of respiratory depression that may be greater than otherwise expected. Tapentadol may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression.
Anticholinergics: Use with anticholinergic products may increase the risk of urinary retention and/or severe constipation, which may lead to paralytic ileus.
USE IN SPECIFIC POPULATIONS
Pregnancy/Nursing Mothers: Pregnancy Category C. NUCYNTA® ER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Neonates born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms. Observe newborns for symptoms of neonatal opioid withdrawal syndrome. Withdrawal symptoms can occur in breast-feeding infants when maternal administration of NUCYNTA® ER is stopped.
Labor and Delivery: Opioids cross the placenta and may produce respiratory depression in neonates. NUCYNTA® ER is not for use in women during and immediately prior to labor, when shorter-acting analgesics or other analgesic techniques are more appropriate.
Use in Elderly, Renal Impairment, and Hepatic Impairment: See WARNINGS AND PRECAUTIONS.
DRUG ABUSE AND DEPENDENCE: See BOXED WARNING
OVERDOSAGE: Institute supportive measures to manage respiratory depression, circulatory shock, and pulmonary edema as required. The opioid antagonists, naloxone or nalmefene, are specific antidotes to respiratory depression.
ADVERSE REACTIONS: In clinical studies, the most common (≥10%) adverse reactions were nausea, constipation, vomiting, dizziness, somnolence, and headache.
Select Postmarketing Adverse Reactions: Anaphylaxis, angioedema, and anaphylactic shock have been reported very rarely with ingredients contained in NUCYNTA® ER. Advise patients how to recognize such reactions and when to seek medical attention. Panic attack has also been reported.
© July 2015, Depomed, Inc. All rights reserved. APL-NUCX-0029 Rev.2
Please see Brief Summary, including BOXED WARNING, on the following pages.
Nuc_PainWeekJourn.indd 2 7/27/15 11:40 AM

BRIEF SUMMARY OF FULL PRESCRIBING INFORMATION
This does not include all the information needed to use NUCYNTA® ER safely and effectively. See full Prescribing Information for NUCYNTA® ER.
INDICATIONS AND USAGE NUCYNTA® ER is indicated for the management of: • pain severe enough to require daily, around-the-clock, long-
term opioid treatment and for which alternative treatment options are inadequate
• neuropathic pain associated with diabetic peripheral neuropathy (DPN) in adults severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Limitations of Usage • Because of the risks of addiction, abuse, and misuse with
opioids, even at recommended doses, and because of the greater risks of overdose and death with extended-release opioid formulations, reserve NUCYNTA® ER for use in patients for whom alternative treatment options (e.g., nonopioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain.
• NUCYNTA® ER is not indicated as an as-needed (prn) analgesic.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY
DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME;
AND INTERACTION WITH ALCOHOL
See full prescribing information for complete boxed warning.
• NUCYNTA® ER exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing, and monitor regularly for development of these behaviors or conditions. (5.1)
• Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Instruct patients to swallow NUCYNTA® ER tablets whole to avoid exposure to a potentially fatal dose of tapentadol. (5.2)
• Accidental ingestion of NUCYNTA® ER, especially in children, can result in fatal overdose of tapentadol. (5.2)
• Prolonged use of NUCYNTA® ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. (5.3)
• Instruct patients not to consume alcohol or any products containing alcohol while taking NUCYNTA® ER because co-ingestion can result in fatal plasma tapentadol levels. (5.4)
CONTRAINDICATIONS Significant respiratory depression; acute or severe bronchial asthma or hypercarbia in an unmonitored setting or in the absence of resuscitative equipment; known or suspected paralytic ileus; hypersensitivity (e.g., anaphylaxis, angioedema) to tapentadol or to any other ingredients of the product; concurrent use of monoamine oxidase inhibitors (MAOIs) or use within the last 14 days.
WARNINGS AND PRECAUTIONS Addiction, Abuse, and Misuse NUCYNTA® ER contains tapentadol, a Schedule II controlled substance. As an opioid, NUCYNTA® ER exposes users to the risks of addiction, abuse, and misuse. As modified-release
products such as NUCYNTA® ER deliver the opioid over an extended period of time, there is a greater risk for overdose and death due to the larger amount of tapentadol present.
Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed NUCYNTA® ER and in those who obtain the drug illicitly. Addiction can occur at recommended doses and if the drug is misused or abused.
Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing NUCYNTA® ER, and monitor all patients receiving NUCYNTA® ER for the development of these behaviors or conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol addiction or abuse) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the prescribing of NUCYNTA® ER for the proper management of pain in any given patient. Patients at increased risk may be prescribed modified-release opioid formulations such as NUCYNTA® ER, but use in such patients necessitates intensive counseling about the risks and proper use of NUCYNTA® ER along with intensive monitoring for signs of addiction, abuse, and misuse.
Abuse or misuse of NUCYNTA® ER by crushing, chewing, snorting, or injecting the dissolved product will result in the uncontrolled delivery of tapentadol and can result in overdose and death.
Opioid agonists such as NUCYNTA® ER are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing NUCYNTA® ER. Strategies to reduce these risks include prescribing the drug in the smallest appropriate quantity and advising the patient on the proper disposal of unused drug. Contact local state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product.
Life-Threatening Respiratory Depression Serious, life-threatening, or fatal respiratory depression has been reported with the use of modified release opioids, even when used as recommended. Respiratory depression from opioid use, if not immediately recognized and treated, may lead to respiratory arrest and death. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status. Carbon dioxide (CO
2) retention from opioid-induced respiratory depression
can exacerbate the sedating effects of opioids.
While serious, life-threatening, or fatal respiratory depression can occur at any time during the use of NUCYNTA® ER, the risk is greatest during the initiation of therapy or following a dose increase.
Closely monitor patients for respiratory depression when initiating therapy with NUCYNTA® ER and following dose increases. To reduce the risk of respiratory depression, proper dosing and titration of NUCYNTA® ER are essential. Overestimating the NUCYNTA® ER dose when converting patients from another opioid product can result in fatal overdose with the first dose.
Accidental ingestion of even one dose of NUCYNTA® ER, especially by children, can result in respiratory depression and death due to an overdose of tapentadol.
Neonatal Opioid Withdrawal Syndrome Prolonged use of NUCYNTA® ER during pregnancy can result in withdrawal signs in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available.
Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing and amount of last maternal use, and rate of elimination of the drug by the newborn.
Interactions with Central Nervous System Depressants Patients must not consume alcoholic beverages or prescription or non-prescription products containing alcohol while on NUCYNTA® ER therapy. The co-ingestion of alcohol with NUCYNTA® ER may result in increased plasma tapentadol levels and a potentially fatal overdose of tapentadol.
Hypotension, profound sedation, coma, respiratory depression, and death may result if NUCYNTA® ER is used concomitantly with alcohol or other central nervous system (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, neuroleptics, other opioids).
When considering the use of NUCYNTA® ER in a patient taking a CNS depressant, assess the duration of use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. Additionally, evaluate the patient’s use of alcohol or illicit drugs that cause CNS depression. If the decision to begin NUCYNTA® ER is made, start with NUCYNTA® ER 50 mg every 12 hours, monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, and Debilitated Patients Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance compared to younger, healthier patients. Therefore, closely monitor such patients, particularly when initiating and titrating NUCYNTA® ER and when NUCYNTA® ER is given concomitantly with other drugs that depress respiration.
Use in Patients with Chronic Pulmonary Disease Monitor for respiratory depression those patients with significant chronic obstructive pulmonary disease or cor pulmonale, and patients having a substantially decreased respiratory reserve, hypoxia, hypercarbia, or pre-existing respiratory depression, particularly when initiating therapy and titrating with NUCYNTA® ER, as in these patients, even usual therapeutic doses of NUCYNTA® ER may decrease respiratory drive to the point of apnea. Consider the use of alternative non-opioid analgesics in these patients if possible.
Hypotensive Effect NUCYNTA® ER may cause severe hypotension. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor these patients for signs of hypotension after initiating or titrating the dose of NUCYNTA® ER. In patients with circulatory shock, NUCYNTA® ER may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of NUCYNTA® ER in patients with circulatory shock.
Use in Patients with Head Injury or Increased Intracranial Pressure Monitor patients taking NUCYNTA® ER who may be susceptible to the intracranial effects of CO
2 retention
(e.g., those with evidence of increased intracranial pressure or brain tumors) for signs of sedation and respiratory depression, particularly when initiating therapy with NUCYNTA® ER. NUCYNTA® ER may reduce respiratory drive, and the resultant CO
2 retention can
further increase intracranial pressure. Opioids may also obscure the clinical course in a patient with a head injury.
Avoid the use of NUCYNTA® ER in patients with impaired consciousness or coma.
Seizures NUCYNTA® ER has not been evaluated in patients with a predisposition to a seizure disorder, and such patients were excluded from clinical studies. The active ingredient tapentadol in NUCYNTA® ER may aggravate convulsions in patients with convulsive disorders, and may induce or aggravate seizures in some clinical settings. Monitor patients with a history of seizure disorders for worsened seizure control during NUCYNTA® ER therapy.
Serotonin Syndrome Cases of life-threatening serotonin syndrome have been reported with the concurrent use of tapentadol and serotonergic drugs. Serotonergic drugs comprise Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, drugs that affect the serotonergic neurotransmitter system (e.g. mirtazapine, trazodone, and tramadol), and drugs that impair metabolism of serotonin (including MAOIs). This may occur within the recommended dose. Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea) and can be fatal.
Use in Patients with Gastrointestinal Conditions NUCYNTA® ER is contraindicated in patients with GI obstruction, including paralytic ileus. The tapentadol in NUCYNTA® ER may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms.
Avoidance of Withdrawal Avoid the use of mixed agonist/antagonist (i.e., pentazocine, nalbuphine, and butorphanol) or partial agonist (buprenorphine) analgesics in patients who have received or are receiving a course of therapy with a full opioid agonist analgesic, including NUCYNTA® ER. In these patients, mixed agonists/antagonists and partial agonist analgesics may reduce the analgesic effect and/or may precipitate withdrawal symptoms.
When discontinuing NUCYNTA® ER, gradually taper the dose.
Driving and Operating Heavy Machinery NUCYNTA® ER may impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of NUCYNTA® ER and know how they will react to the medication.
Hepatic Impairment A study with an immediate-release formulation of tapentadol in subjects with hepatic impairment showed higher serum concentrations of tapentadol than in those with normal hepatic function. Avoid use of NUCYNTA® ER in patients with severe hepatic impairment. Reduce the dose of NUCYNTA® ER in patients with moderate hepatic impairment. Closely monitor patients with moderate hepatic impairment for respiratory and central nervous system depression when initiating and titrating NUCYNTA® ER.
Renal Impairment Use of NUCYNTA® ER in patients with severe renal impairment is not recommended due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
ADVERSE REACTIONS The following serious adverse reactions are discussed elsewhere in the labeling:
• Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)]
Nuc_PainWeekJourn.indd 3 7/27/15 11:40 AM

BRIEF SUMMARY OF FULL PRESCRIBING INFORMATION
This does not include all the information needed to use NUCYNTA® ER safely and effectively. See full Prescribing Information for NUCYNTA® ER.
INDICATIONS AND USAGE NUCYNTA® ER is indicated for the management of: • pain severe enough to require daily, around-the-clock, long-
term opioid treatment and for which alternative treatment options are inadequate
• neuropathic pain associated with diabetic peripheral neuropathy (DPN) in adults severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Limitations of Usage • Because of the risks of addiction, abuse, and misuse with
opioids, even at recommended doses, and because of the greater risks of overdose and death with extended-release opioid formulations, reserve NUCYNTA® ER for use in patients for whom alternative treatment options (e.g., nonopioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain.
• NUCYNTA® ER is not indicated as an as-needed (prn) analgesic.
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY
DEPRESSION; ACCIDENTAL INGESTION; NEONATAL OPIOID WITHDRAWAL SYNDROME;
AND INTERACTION WITH ALCOHOL
See full prescribing information for complete boxed warning.
• NUCYNTA® ER exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing, and monitor regularly for development of these behaviors or conditions. (5.1)
• Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Instruct patients to swallow NUCYNTA® ER tablets whole to avoid exposure to a potentially fatal dose of tapentadol. (5.2)
• Accidental ingestion of NUCYNTA® ER, especially in children, can result in fatal overdose of tapentadol. (5.2)
• Prolonged use of NUCYNTA® ER during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. (5.3)
• Instruct patients not to consume alcohol or any products containing alcohol while taking NUCYNTA® ER because co-ingestion can result in fatal plasma tapentadol levels. (5.4)
CONTRAINDICATIONS Significant respiratory depression; acute or severe bronchial asthma or hypercarbia in an unmonitored setting or in the absence of resuscitative equipment; known or suspected paralytic ileus; hypersensitivity (e.g., anaphylaxis, angioedema) to tapentadol or to any other ingredients of the product; concurrent use of monoamine oxidase inhibitors (MAOIs) or use within the last 14 days.
WARNINGS AND PRECAUTIONS Addiction, Abuse, and Misuse NUCYNTA® ER contains tapentadol, a Schedule II controlled substance. As an opioid, NUCYNTA® ER exposes users to the risks of addiction, abuse, and misuse. As modified-release
products such as NUCYNTA® ER deliver the opioid over an extended period of time, there is a greater risk for overdose and death due to the larger amount of tapentadol present.
Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed NUCYNTA® ER and in those who obtain the drug illicitly. Addiction can occur at recommended doses and if the drug is misused or abused.
Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing NUCYNTA® ER, and monitor all patients receiving NUCYNTA® ER for the development of these behaviors or conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol addiction or abuse) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the prescribing of NUCYNTA® ER for the proper management of pain in any given patient. Patients at increased risk may be prescribed modified-release opioid formulations such as NUCYNTA® ER, but use in such patients necessitates intensive counseling about the risks and proper use of NUCYNTA® ER along with intensive monitoring for signs of addiction, abuse, and misuse.
Abuse or misuse of NUCYNTA® ER by crushing, chewing, snorting, or injecting the dissolved product will result in the uncontrolled delivery of tapentadol and can result in overdose and death.
Opioid agonists such as NUCYNTA® ER are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing NUCYNTA® ER. Strategies to reduce these risks include prescribing the drug in the smallest appropriate quantity and advising the patient on the proper disposal of unused drug. Contact local state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product.
Life-Threatening Respiratory Depression Serious, life-threatening, or fatal respiratory depression has been reported with the use of modified release opioids, even when used as recommended. Respiratory depression from opioid use, if not immediately recognized and treated, may lead to respiratory arrest and death. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status. Carbon dioxide (CO
2) retention from opioid-induced respiratory depression
can exacerbate the sedating effects of opioids.
While serious, life-threatening, or fatal respiratory depression can occur at any time during the use of NUCYNTA® ER, the risk is greatest during the initiation of therapy or following a dose increase.
Closely monitor patients for respiratory depression when initiating therapy with NUCYNTA® ER and following dose increases. To reduce the risk of respiratory depression, proper dosing and titration of NUCYNTA® ER are essential. Overestimating the NUCYNTA® ER dose when converting patients from another opioid product can result in fatal overdose with the first dose.
Accidental ingestion of even one dose of NUCYNTA® ER, especially by children, can result in respiratory depression and death due to an overdose of tapentadol.
Neonatal Opioid Withdrawal Syndrome Prolonged use of NUCYNTA® ER during pregnancy can result in withdrawal signs in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available.
Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing and amount of last maternal use, and rate of elimination of the drug by the newborn.
Interactions with Central Nervous System Depressants Patients must not consume alcoholic beverages or prescription or non-prescription products containing alcohol while on NUCYNTA® ER therapy. The co-ingestion of alcohol with NUCYNTA® ER may result in increased plasma tapentadol levels and a potentially fatal overdose of tapentadol.
Hypotension, profound sedation, coma, respiratory depression, and death may result if NUCYNTA® ER is used concomitantly with alcohol or other central nervous system (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, neuroleptics, other opioids).
When considering the use of NUCYNTA® ER in a patient taking a CNS depressant, assess the duration of use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. Additionally, evaluate the patient’s use of alcohol or illicit drugs that cause CNS depression. If the decision to begin NUCYNTA® ER is made, start with NUCYNTA® ER 50 mg every 12 hours, monitor patients for signs of sedation and respiratory depression, and consider using a lower dose of the concomitant CNS depressant.
Use in Elderly, Cachectic, and Debilitated Patients Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance compared to younger, healthier patients. Therefore, closely monitor such patients, particularly when initiating and titrating NUCYNTA® ER and when NUCYNTA® ER is given concomitantly with other drugs that depress respiration.
Use in Patients with Chronic Pulmonary Disease Monitor for respiratory depression those patients with significant chronic obstructive pulmonary disease or cor pulmonale, and patients having a substantially decreased respiratory reserve, hypoxia, hypercarbia, or pre-existing respiratory depression, particularly when initiating therapy and titrating with NUCYNTA® ER, as in these patients, even usual therapeutic doses of NUCYNTA® ER may decrease respiratory drive to the point of apnea. Consider the use of alternative non-opioid analgesics in these patients if possible.
Hypotensive Effect NUCYNTA® ER may cause severe hypotension. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor these patients for signs of hypotension after initiating or titrating the dose of NUCYNTA® ER. In patients with circulatory shock, NUCYNTA® ER may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of NUCYNTA® ER in patients with circulatory shock.
Use in Patients with Head Injury or Increased Intracranial Pressure Monitor patients taking NUCYNTA® ER who may be susceptible to the intracranial effects of CO
2 retention
(e.g., those with evidence of increased intracranial pressure or brain tumors) for signs of sedation and respiratory depression, particularly when initiating therapy with NUCYNTA® ER. NUCYNTA® ER may reduce respiratory drive, and the resultant CO
2 retention can
further increase intracranial pressure. Opioids may also obscure the clinical course in a patient with a head injury.
Avoid the use of NUCYNTA® ER in patients with impaired consciousness or coma.
Seizures NUCYNTA® ER has not been evaluated in patients with a predisposition to a seizure disorder, and such patients were excluded from clinical studies. The active ingredient tapentadol in NUCYNTA® ER may aggravate convulsions in patients with convulsive disorders, and may induce or aggravate seizures in some clinical settings. Monitor patients with a history of seizure disorders for worsened seizure control during NUCYNTA® ER therapy.
Serotonin Syndrome Cases of life-threatening serotonin syndrome have been reported with the concurrent use of tapentadol and serotonergic drugs. Serotonergic drugs comprise Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, drugs that affect the serotonergic neurotransmitter system (e.g. mirtazapine, trazodone, and tramadol), and drugs that impair metabolism of serotonin (including MAOIs). This may occur within the recommended dose. Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea) and can be fatal.
Use in Patients with Gastrointestinal Conditions NUCYNTA® ER is contraindicated in patients with GI obstruction, including paralytic ileus. The tapentadol in NUCYNTA® ER may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms.
Avoidance of Withdrawal Avoid the use of mixed agonist/antagonist (i.e., pentazocine, nalbuphine, and butorphanol) or partial agonist (buprenorphine) analgesics in patients who have received or are receiving a course of therapy with a full opioid agonist analgesic, including NUCYNTA® ER. In these patients, mixed agonists/antagonists and partial agonist analgesics may reduce the analgesic effect and/or may precipitate withdrawal symptoms.
When discontinuing NUCYNTA® ER, gradually taper the dose.
Driving and Operating Heavy Machinery NUCYNTA® ER may impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of NUCYNTA® ER and know how they will react to the medication.
Hepatic Impairment A study with an immediate-release formulation of tapentadol in subjects with hepatic impairment showed higher serum concentrations of tapentadol than in those with normal hepatic function. Avoid use of NUCYNTA® ER in patients with severe hepatic impairment. Reduce the dose of NUCYNTA® ER in patients with moderate hepatic impairment. Closely monitor patients with moderate hepatic impairment for respiratory and central nervous system depression when initiating and titrating NUCYNTA® ER.
Renal Impairment Use of NUCYNTA® ER in patients with severe renal impairment is not recommended due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
ADVERSE REACTIONS The following serious adverse reactions are discussed elsewhere in the labeling:
• Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)]
Nuc_PainWeekJourn.indd 3 7/27/15 11:40 AM

• Life-Threatening Respiratory Depression [see Warnings and Precautions (5.2)]
• Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.3)]
• Interaction with Other CNS Depressants [see Warnings and Precautions (5.4)]
• Hypotensive Effects [see Warnings and Precautions (5.7)]
• Gastrointestinal Effects [see Warnings and Precautions (5.11)]
• Seizures [see Warnings and Precautions (5.9)]
• Serotonin Syndrome [see Warnings and Precautions (5.10)]
Clinical Trial Experience Commonly-Observed Adverse Reactions in Clinical Studies with NUCYNTA® ER in Patients with Chronic Pain due to Low Back Pain or Osteoarthritis
The most common adverse reactions (reported by ≥10 % in any NUCYNTA® ER dose group) were: nausea, constipation, dizziness, headache, and somnolence.
The most common reasons for discontinuation due to adverse reactions in eight Phase 2/3 pooled studies reported by ≥1% in any NUCYNTA® ER dose group for NUCYNTA® ER- and placebo-treated patients were nausea (4 % vs. 1%), dizziness (3% vs. <1%), vomiting (3% vs. <1%), somnolence (2% vs. <1%), constipation (1% vs. <1%), headache (1% vs. <1%), and fatigue (1% vs. <1%), respectively.
Commonly-Observed Adverse Reactions in Clinical Studies with NUCYNTA® ER in Patients with Neuropathic Pain Associated with Diabetic Peripheral Neuropathy
The most commonly reported ADRs (incidence ≥ 10% in NUCYNTA® ER-treated subjects) were: nausea, constipation, vomiting, dizziness, somnolence, and headache.
Postmarketing Experience The following adverse reactions, not above, have been identified during post approval use of tapentadol. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Psychiatric disorders: hallucination, suicidal ideation, panic attack Anaphylaxis, angioedema, and anaphylactic shock have been reported very rarely with ingredients contained in NUCYNTA® ER. Advise patients how to recognize such reactions and when to seek medical attention.
DRUG INTERACTIONSAlcohol Concomitant use of alcohol with NUCYNTA® ER can result in an increase of tapentadol plasma levels and potentially fatal overdose of tapentadol. Instruct patients not to consume alcoholic beverages or use prescription or non-prescription products containing alcohol while on NUCYNTA® ER therapy.
Monoamine Oxidase Inhibitors NUCYNTA® ER is contraindicated in patients who are receiving monoamine oxidase inhibitors (MAOIs) or who have taken them within the last 14 days due to potential additive effects on norepinephrine levels, which may result in adverse cardiovascular events.
CNS Depressants The concomitant use of NUCYNTA® ER with other CNS depressants including sedatives, hypnotics, tranquilizers, general anesthetics, phenothiazines, other opioids, and alcohol can increase the risk of respiratory depression, profound sedation, coma and death. Monitor patients receiving CNS depressants and NUCYNTA® ER for signs of respiratory depression, sedation and hypotension.
When combined therapy with any of the above medications is considered, the dose of one or both agents should be reduced.
Serotonergic Drugs There have been post-marketing reports of serotonin syndrome with the concomitant use of tapentadol and serotonergic drugs (e.g., SSRIs and SNRIs). Caution is advised when NUCYNTA® ER is coadministered with other drugs that may affect serotonergic neurotransmitter systems such as SSRIs, SNRIs, MAOIs, and triptans. If concomitant treatment of NUCYNTA® ER with a drug affecting the serotonergic neurotransmitter system is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose increases.
Muscle Relaxants Tapentadol may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression. Monitor patients receiving muscle relaxants and NUCYNTA® ER for signs of respiratory depression that may be greater than otherwise expected.
Mixed Agonist/Antagonist Opioid Analgesics Mixed agonist/antagonist analgesics (i.e., pentazocine, nalbuphine, and butorphanol) and partial agonists (e.g., buprenorphine) may reduce the analgesic effect of NUCYNTA® ER or precipitate withdrawal symptoms. Avoid the use of mixed agonist/antagonist analgesics in patients receiving NUCYNTA® ER.
Anticholinergics The use of NUCYNTA® ER with anticholinergic products may increase the risk of urinary retention and/or severe constipation, which may lead to paralytic ileus.
USE IN SPECIFIC POPULATIONS Pregnancy Clinical Considerations
Fetal/neonatal adverse reactions
Prolonged use of opioid analgesics during pregnancy for medical or nonmedical purposes can result in physical dependence in the neonate and neonatal opioid withdrawal syndrome shortly after birth. Observe newborns for symptoms of neonatal opioid withdrawal syndrome, such as poor feeding, diarrhea, irritability, tremor, rigidity, and seizures, and manage accordingly.
Teratogenic Effects - Pregnancy Category C
There are no adequate and well-controlled studies in pregnant women. NUCYNTA® ER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Labor and Delivery Opioids cross the placenta and may produce respiratory depression in neonates. NUCYNTA® ER is not for use in women during and immediately prior to labor, when shorter acting analgesics or other analgesic techniques are more appropriate. Opioid analgesics can prolong labor through actions that temporarily reduce the strength, duration, and frequency of uterine contractions. However this effect is not consistent and may be offset by an increased rate of cervical dilatation, which tends to shorten labor.
Nursing Mothers There is insufficient/limited information on the excretion of tapentadol in human or animal breast milk. Physicochemical and available pharmacodynamic/toxicological data on tapentadol point to excretion in breast milk and risk to the breastfeeding child cannot be excluded.
Because of the potential for adverse reactions in nursing infants from NUCYNTA® ER, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Withdrawal symptoms can occur in breast-feeding infants when maternal administration of NUCYNTA® ER is stopped.
Pediatric Use The safety and efficacy of NUCYNTA® ER in pediatric patients less than 18 years of age have not been established.
Geriatric Use Of the total number of patients in Phase 2/3 double-blind, multiple-dose clinical studies of NUCYNTA® ER, 28% (1023/3613) were 65 years and over, while 7% (245/3613) were 75 years and over. No overall differences in effectiveness or tolerability were observed between these patients and younger patients.
In general, recommended dosing for elderly patients with normal renal and hepatic function is the same as for younger adult patients with normal renal and hepatic function. Because elderly patients are more likely to have decreased renal and hepatic function, consideration should be given to starting elderly patients with the lower range of recommended doses.
Renal Impairment The safety and effectiveness of NUCYNTA® ER have not been established in patients with severe renal impairment (CL
CR <30 mL/min). Use of NUCYNTA® ER in patients
with severe renal impairment is not recommended due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
Hepatic Impairment Administration of tapentadol resulted in higher exposures and serum levels of tapentadol in subjects with impaired hepatic function compared to subjects with normal hepatic function. The dose of NUCYNTA® ER should be reduced in patients with moderate hepatic impairment (Child-Pugh Score 7 to 9).
Use of NUCYNTA® ER is not recommended in severe hepatic impairment (Child-Pugh Score 10 to 15).
DRUG ABUSE AND DEPENDENCE Controlled Substance NUCYNTA® ER contains tapentadol, a Schedule II controlled substance with a high potential for abuse similar to fentanyl, methadone, morphine, oxycodone, and oxymorphone. NUCYNTA® ER can be abused and is subject to misuse, addiction, and criminal diversion. The high drug content in the extended release formulation adds to the risk of adverse outcomes from abuse and misuse.
Abuse All patients treated with opioids require careful monitoring for signs of abuse and addiction, because use of opioid analgesic products carries the risk of addiction even under appropriate medical use.
Drug abuse is the intentional non-therapeutic use of an over-the-counter or prescription drug, even once, for its rewarding psychological or physiological effects. Drug abuse includes, but is not limited to the following examples: the use of a prescription or over-the-counter drug to get “high,” or the use of steroids for performance enhancement and muscle build up.
Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and include: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal.
“Drug-seeking” behavior is very common to addicts and drug abusers. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated claims of loss of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating physician(s). “Doctor shopping” (visiting multiple prescribers) to obtain additional prescriptions is common among drug abusers, and people suffering from untreated addiction. Preoccupation with achieving pain relief can be appropriate behavior in a patient with poor pain control.
Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true addiction.
NUCYNTA® ER, like other opioids, can be diverted for non-medical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by law, is strongly advised.
Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
Dependence Both tolerance and physical dependence can develop during chronic opioid therapy. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia (in the absence of disease progression or other external factors). Tolerance may occur to both the desired and undesired effects of drugs, and may develop at different rates for different effects.
Physical dependence results in withdrawal symptoms after abrupt discontinuation or a significant dose reduction of a drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity, e.g., naloxone, nalmefene, mixed agonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine), or partial agonists (buprenorphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued opioid usage.
NUCYNTA® ER should not be abruptly discontinued. If NUCYNTA® ER is abruptly discontinued in a physically-dependent patient, an abstinence syndrome may occur. Some or all of the following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, piloerection, myalgia, mydriasis, irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, increased blood pressure, respiratory rate, or heart rate.
Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms.
OVERDOSAGE Clinical Presentation Acute overdosage with opioids can be manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and sometimes pulmonary edema, bradycardia, hypotension and death. Marked mydriasis rather than miosis may be seen due to severe hypoxia in overdose situations.
Treatment of Overdose In case of overdose, priorities are the re-establishment of a patent and protected airway and institution of assisted or controlled ventilation if needed. Employ other supportive measures (including oxygen, vasopressors) in the management of circulatory shock and pulmonary edema as indicated. Cardiac arrest or arrhythmias will require advanced life support techniques.
© June 2015, Depomed, Inc. All rights reserved. APL-NUCX-0041
Nuc_PainWeekJourn.indd 4 7/27/15 11:40 AM

• Life-Threatening Respiratory Depression [see Warnings and Precautions (5.2)]
• Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.3)]
• Interaction with Other CNS Depressants [see Warnings and Precautions (5.4)]
• Hypotensive Effects [see Warnings and Precautions (5.7)]
• Gastrointestinal Effects [see Warnings and Precautions (5.11)]
• Seizures [see Warnings and Precautions (5.9)]
• Serotonin Syndrome [see Warnings and Precautions (5.10)]
Clinical Trial Experience Commonly-Observed Adverse Reactions in Clinical Studies with NUCYNTA® ER in Patients with Chronic Pain due to Low Back Pain or Osteoarthritis
The most common adverse reactions (reported by ≥10 % in any NUCYNTA® ER dose group) were: nausea, constipation, dizziness, headache, and somnolence.
The most common reasons for discontinuation due to adverse reactions in eight Phase 2/3 pooled studies reported by ≥1% in any NUCYNTA® ER dose group for NUCYNTA® ER- and placebo-treated patients were nausea (4 % vs. 1%), dizziness (3% vs. <1%), vomiting (3% vs. <1%), somnolence (2% vs. <1%), constipation (1% vs. <1%), headache (1% vs. <1%), and fatigue (1% vs. <1%), respectively.
Commonly-Observed Adverse Reactions in Clinical Studies with NUCYNTA® ER in Patients with Neuropathic Pain Associated with Diabetic Peripheral Neuropathy
The most commonly reported ADRs (incidence ≥ 10% in NUCYNTA® ER-treated subjects) were: nausea, constipation, vomiting, dizziness, somnolence, and headache.
Postmarketing Experience The following adverse reactions, not above, have been identified during post approval use of tapentadol. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Psychiatric disorders: hallucination, suicidal ideation, panic attack Anaphylaxis, angioedema, and anaphylactic shock have been reported very rarely with ingredients contained in NUCYNTA® ER. Advise patients how to recognize such reactions and when to seek medical attention.
DRUG INTERACTIONSAlcohol Concomitant use of alcohol with NUCYNTA® ER can result in an increase of tapentadol plasma levels and potentially fatal overdose of tapentadol. Instruct patients not to consume alcoholic beverages or use prescription or non-prescription products containing alcohol while on NUCYNTA® ER therapy.
Monoamine Oxidase Inhibitors NUCYNTA® ER is contraindicated in patients who are receiving monoamine oxidase inhibitors (MAOIs) or who have taken them within the last 14 days due to potential additive effects on norepinephrine levels, which may result in adverse cardiovascular events.
CNS Depressants The concomitant use of NUCYNTA® ER with other CNS depressants including sedatives, hypnotics, tranquilizers, general anesthetics, phenothiazines, other opioids, and alcohol can increase the risk of respiratory depression, profound sedation, coma and death. Monitor patients receiving CNS depressants and NUCYNTA® ER for signs of respiratory depression, sedation and hypotension.
When combined therapy with any of the above medications is considered, the dose of one or both agents should be reduced.
Serotonergic Drugs There have been post-marketing reports of serotonin syndrome with the concomitant use of tapentadol and serotonergic drugs (e.g., SSRIs and SNRIs). Caution is advised when NUCYNTA® ER is coadministered with other drugs that may affect serotonergic neurotransmitter systems such as SSRIs, SNRIs, MAOIs, and triptans. If concomitant treatment of NUCYNTA® ER with a drug affecting the serotonergic neurotransmitter system is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose increases.
Muscle Relaxants Tapentadol may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression. Monitor patients receiving muscle relaxants and NUCYNTA® ER for signs of respiratory depression that may be greater than otherwise expected.
Mixed Agonist/Antagonist Opioid Analgesics Mixed agonist/antagonist analgesics (i.e., pentazocine, nalbuphine, and butorphanol) and partial agonists (e.g., buprenorphine) may reduce the analgesic effect of NUCYNTA® ER or precipitate withdrawal symptoms. Avoid the use of mixed agonist/antagonist analgesics in patients receiving NUCYNTA® ER.
Anticholinergics The use of NUCYNTA® ER with anticholinergic products may increase the risk of urinary retention and/or severe constipation, which may lead to paralytic ileus.
USE IN SPECIFIC POPULATIONS Pregnancy Clinical Considerations
Fetal/neonatal adverse reactions
Prolonged use of opioid analgesics during pregnancy for medical or nonmedical purposes can result in physical dependence in the neonate and neonatal opioid withdrawal syndrome shortly after birth. Observe newborns for symptoms of neonatal opioid withdrawal syndrome, such as poor feeding, diarrhea, irritability, tremor, rigidity, and seizures, and manage accordingly.
Teratogenic Effects - Pregnancy Category C
There are no adequate and well-controlled studies in pregnant women. NUCYNTA® ER should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Labor and Delivery Opioids cross the placenta and may produce respiratory depression in neonates. NUCYNTA® ER is not for use in women during and immediately prior to labor, when shorter acting analgesics or other analgesic techniques are more appropriate. Opioid analgesics can prolong labor through actions that temporarily reduce the strength, duration, and frequency of uterine contractions. However this effect is not consistent and may be offset by an increased rate of cervical dilatation, which tends to shorten labor.
Nursing Mothers There is insufficient/limited information on the excretion of tapentadol in human or animal breast milk. Physicochemical and available pharmacodynamic/toxicological data on tapentadol point to excretion in breast milk and risk to the breastfeeding child cannot be excluded.
Because of the potential for adverse reactions in nursing infants from NUCYNTA® ER, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Withdrawal symptoms can occur in breast-feeding infants when maternal administration of NUCYNTA® ER is stopped.
Pediatric Use The safety and efficacy of NUCYNTA® ER in pediatric patients less than 18 years of age have not been established.
Geriatric Use Of the total number of patients in Phase 2/3 double-blind, multiple-dose clinical studies of NUCYNTA® ER, 28% (1023/3613) were 65 years and over, while 7% (245/3613) were 75 years and over. No overall differences in effectiveness or tolerability were observed between these patients and younger patients.
In general, recommended dosing for elderly patients with normal renal and hepatic function is the same as for younger adult patients with normal renal and hepatic function. Because elderly patients are more likely to have decreased renal and hepatic function, consideration should be given to starting elderly patients with the lower range of recommended doses.
Renal Impairment The safety and effectiveness of NUCYNTA® ER have not been established in patients with severe renal impairment (CL
CR <30 mL/min). Use of NUCYNTA® ER in patients
with severe renal impairment is not recommended due to accumulation of a metabolite formed by glucuronidation of tapentadol. The clinical relevance of the elevated metabolite is not known.
Hepatic Impairment Administration of tapentadol resulted in higher exposures and serum levels of tapentadol in subjects with impaired hepatic function compared to subjects with normal hepatic function. The dose of NUCYNTA® ER should be reduced in patients with moderate hepatic impairment (Child-Pugh Score 7 to 9).
Use of NUCYNTA® ER is not recommended in severe hepatic impairment (Child-Pugh Score 10 to 15).
DRUG ABUSE AND DEPENDENCE Controlled Substance NUCYNTA® ER contains tapentadol, a Schedule II controlled substance with a high potential for abuse similar to fentanyl, methadone, morphine, oxycodone, and oxymorphone. NUCYNTA® ER can be abused and is subject to misuse, addiction, and criminal diversion. The high drug content in the extended release formulation adds to the risk of adverse outcomes from abuse and misuse.
Abuse All patients treated with opioids require careful monitoring for signs of abuse and addiction, because use of opioid analgesic products carries the risk of addiction even under appropriate medical use.
Drug abuse is the intentional non-therapeutic use of an over-the-counter or prescription drug, even once, for its rewarding psychological or physiological effects. Drug abuse includes, but is not limited to the following examples: the use of a prescription or over-the-counter drug to get “high,” or the use of steroids for performance enhancement and muscle build up.
Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and include: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal.
“Drug-seeking” behavior is very common to addicts and drug abusers. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated claims of loss of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating physician(s). “Doctor shopping” (visiting multiple prescribers) to obtain additional prescriptions is common among drug abusers, and people suffering from untreated addiction. Preoccupation with achieving pain relief can be appropriate behavior in a patient with poor pain control.
Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true addiction.
NUCYNTA® ER, like other opioids, can be diverted for non-medical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by law, is strongly advised.
Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
Dependence Both tolerance and physical dependence can develop during chronic opioid therapy. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia (in the absence of disease progression or other external factors). Tolerance may occur to both the desired and undesired effects of drugs, and may develop at different rates for different effects.
Physical dependence results in withdrawal symptoms after abrupt discontinuation or a significant dose reduction of a drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity, e.g., naloxone, nalmefene, mixed agonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine), or partial agonists (buprenorphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued opioid usage.
NUCYNTA® ER should not be abruptly discontinued. If NUCYNTA® ER is abruptly discontinued in a physically-dependent patient, an abstinence syndrome may occur. Some or all of the following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, piloerection, myalgia, mydriasis, irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, increased blood pressure, respiratory rate, or heart rate.
Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms.
OVERDOSAGE Clinical Presentation Acute overdosage with opioids can be manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and sometimes pulmonary edema, bradycardia, hypotension and death. Marked mydriasis rather than miosis may be seen due to severe hypoxia in overdose situations.
Treatment of Overdose In case of overdose, priorities are the re-establishment of a patent and protected airway and institution of assisted or controlled ventilation if needed. Employ other supportive measures (including oxygen, vasopressors) in the management of circulatory shock and pulmonary edema as indicated. Cardiac arrest or arrhythmias will require advanced life support techniques.
© June 2015, Depomed, Inc. All rights reserved. APL-NUCX-0041
Nuc_PainWeekJourn.indd 4 7/27/15 11:40 AM

by Kevin L. Zacharoff FACPE, FACIP, FAAP

www.painweek.org | PWJ | 37Q3 | 2015
abstract: The comparison between acute and chronic pain may often be oversimpli-fied and only look at duration as a qualifying factor. In fact, the relationship may be much more complex requiring analysis from both a pathophysiologic and psychological per-spective. Many different aspects of the tran-sition from acute to chronic pain should be considered. Additionally, identifying risk factors and predicting which patients are at higher risk for developing chronic pain are important pain management strategies. Clinical approaches should be employed when possible to mitigate this transition and afford the person with pain the best oppor-tunity for successful treatment possible.
eXPeRT OPiNiON

38 | PWJ | www.painweek.org Q3 | 2015
The road from acute to chronic pain can be a complicated one, involving 1-way streets, 2-way streets, rotaries, and other complicated configurations. There are often many questions that need to be considered. First, one needs to explore the relationship between acute and chronic pain. At its simplest level, the distinction between acute and chronic pain often seems to be based on passage of time. Do we really think it’s that simple? The Webster Dictionary® defines chronic as marked by long duration or frequent recurrence: not acute. This definition implies that acute and chronic pain may be opposites of each other. Is that the case, or might one be the product of the other? The World Health Organization (WHO) defines a chronic disease as one of long duration with generally slow progression.1 This seems to imply that an acute condition may or may not precede a chronic one. An important question to consider is whether or not these definitions satisfy our thinking about the relationship between acute and chronic pain. If they don’t provide satisfactory paradigms regarding pain, what would? Other questions to consider are clinical ones—Are there specific patients that experience acute pain and are “at risk” of the transition to chronic pain? If so, what are the circumstances of this risk? Are there profiles of patients that could help identify them earlier? And lastly, what (if anything) can be done to prevent this transition
EXPERT OPINION

www.painweek.org | PWJ | 39Q3 | 2015
SOMe ANSWeRSSome think (including this author) that the relationship between acute and chronic pain involves “vicious circles” (see above) that intersect and “fuel” each other and make the relationship between acute and chronic pain a bit more complex than passage of time alone.
ACUTe VS CHRONiC PAiNAcute pain has some distinct characteristics that typically include onset that is generally sudden and certainly recent. The cause of acute pain is usually identifiable, such as an injury, disease state, or iatrogenic event (eg, surgery). Accepted time frame is usually ≤1 month in duration, with intensity that is often directly related to the severity of the underlying condition or disease state. The symptom pro-file of acute pain includes swelling, redness, and throbbing, with accompanying behaviors such as moaning, crying, and rubbing the affected area, etc.
Chronic pain is often much more difficult to manage than acute pain and is generally persistent (≥3 months in dura-tion) with an indeterminate time of onset. In contrast to acute pain, there may be no obviously identifiable cause, or the pain may be the result of some chronic disease state or situation. Chronic pain usually involves prolonged physi-cal and psychological functional impairment and may be associated with characteristic behaviors such as irritability, anorexia, depression, and insomnia.
Something we also need to consider, but often do not, is the possibility of subacute pain which chronologically falls somewhere between acute and chronic pain, with certain characteristic aspects of each. In fact, the subacute phase may actually be the place along the continuum that is most crit-ical to preventing the transition from acute to chronic pain.
PAiN MeCHANiSMS AND PeRCePTiONWhen we think about acute pain mechanisms, let’s consider postoperative pain as an example of acute pain, since it is often quite similar to traumatic painful episodes. Postop-erative pain typically varies according to intensity, quality, and of course the duration of the painful stimulus. There is activation of peripheral nociceptors and subsequent periph-eral sensitization.2 Simplistically, 5 things are necessary for nociceptors to relay pain information to the central nervous system (CNS):
❶ Transduction
❷ Action potential generation
❸ Transmission
❹ Signal transmission to the thalamus
❺ Signal transmission to the cerebral cortex
PSYCHOLOGICALVICIOUS CIRCLE
PHYSICALVICIOUS CIRCLE
pain ↓
anger, anxiety, fear, distress →impoverished mood →
depression → increased perception of pain →
↑ pain
pain ↓
activity avoidance →progressive deconditioning →
pain with decreasing activity → further activity avoidance →
further deconditioning →↑
pain

40 | PWJ | www.painweek.org Q3 | 2015
Each of these 5 events is controlled separately and can be considered distinct potential targets for pain treatment.3
PAiN MODeLSLet’s examine 2 pain models, the Biomedical Model and Biopsychosocial Model. Usually attempting to explain pain on the basis of its etiology, the Biomedical Model is probably oversimplified and often incomplete. Considering pain to be either nociceptive or neuropathic in nature, this model may lead to unrealistic treatment expectations of both clinicians and patients4. The Biopsychosocial Model is more complex and recognizes the combined role of both the pathophysiol-ogy and psychological state of the patient with chronic pain. Cultural background and social interactions in the work-place, home, and health system are considered as important variables.5
The intersection of these 2 models is important in negoti-ating the relationship between chronic pain and suffering, with both neuronal and mental states contributing to sensa-tion and perception of pain. These may then influence emo-tion and cognition, which then circulate between chronic pain and degree of suffering in a circuitous fashion.
The table below considers these models from the perspec-tive of clinical relevance:
If we superimpose this into what we may observe in patients from both a psychological and physical perspective, it starts
to identify what patterns or paths may exist to promote the transition from acute to chronic pain:
FATIGUE/PAIN ←→ rest/do less ←→ sleep more or less/less fit/muscle strength ←→ more fatigue & pain/thinking more
about symptoms ←→ do less/rest more ←→ notice more pain and fatigue when active ←→ do less/
rest more ←→ catastrophizing/thinking it’s terrible and won’t get better/problems coping ←→ feeling helpless, hopeless, frustrated, anxious, bad mood ←→ do more
when able/rest when not able ←→ FATIGUE/PAIN
It’s important to take note that each phase of this “cycle” is bidirectional and a potential opportunity for movement in the opposite direction.
PAiN TYPeSWhen thinking about the transition from acute to chronic pain, it is also important to consider some possible common types of pain. Nociceptive pain typically involves activation of high threshold peripheral neurons by noxious stimuli (eg, mechanical, chemical, thermal) and often fades in intensity at some point once the peripheral source is removed. Inflam-matory pain involves heightened sensitivity in response to tissue injury and inflammation, resulting from release of mediators that reduce pain threshold and, unlike nocicep-tive pain, can outlast tissue injury for longer periods of time6 (hours or days) due to nociceptor sensitization, threshold reduction, and “short-term” central sensitization. Neuro-pathic pain typically arises after injury to nerves or sensory transmitting systems in the CNS, involving both sensory loss and paradoxical hypersensitivity.6 In situations where nerve injury occurs during a surgical procedure, a neuro-pathic component of pain may develop and persist.
Two other important things involved in the perception of pain are: 1) the brain—people who are highly sensitive to pain may have greater activity in certain parts of the brain (anterior cingulate cortex), and people who are able to focus on things other than their pain may have less activ-ity in other parts of the brain (somatosensory cortex); and 2) hyperalgesia, an increased sensitivity to pain—can be primary (occurring in the periphery) or secondary (occur-ring within the CNS and preceding central sensitization).7
THe TRANSiTiON FROM ACUTe TO CHRONiC PAiNAnother key component of the transition from acute to chronic pain is neuroplasticity.3 This is a mechanism that allows for neurons in the brain to compensate for injury and disease, adjusting activity accordingly in response to new
Table
Biomedical Model
Biopsychosocial Model
Most appropriate for acute pain
More useful for chronic pain
Emphasizes peripheral nociception
Central mechanisms involved
Focuses on physical disease mechanisms
Focuses on illness behavior, including cognition and emotional response
“Reductionistic” approach
Multidimensional systems approach
Medical management approach
Self-management strategies important
EXPERT OPINION

www.painweek.org | PWJ | 41Q3 | 2015
situations or changes in environment. This phenomenon is thought to involve either reversible inflammatory changes or actual physical remodeling of neuronal architecture leading to decreased inhibition of pain modulation and ultimately central sensitization (neuronal hypersensitivity). When comparing modulation (reversible changes in primary sen-sory and central excitability) to modification (long-lasting changes in the expression of transmitters, receptors and ion channels, etc), it is more likely that modification is the link between acute and chronic pain.
Let’s now revisit postoperative pain as a model. We need to think about the distribution of patients who will experience acute pain (likely most if not all), and those that will go on to have chronic pain, and what falls into normal range of expec-tations vs abnormal or unexpected. Chronic postoperative pain is often poorly understood and also poorly characterized. The International Association for the Study of Pain (IASP) defines postprocedural pain as “a persistent pain state that is apparent more than 2 months after operation and cannot be explained by other causes.” There is usually a complex nature of postoperative pain and very little clear distinction of the transition from acute to chronic pain. Is there a neuropathic component? Is there an inflammatory component? Is there an ongoing nociceptive stimulus? It is thought that in many cases where postoperative pain becomes chronic pain that there is at least a neuropathic component as a contributing factor resulting from neuroplastic changes.8
One reason that postoperative pain is a good model to explore the transition from acute to chronic pain is that predisposing factors to this transition have been identified,3 including:
▸ Psychological status (eg, anxiety, depression) ▸ Pre-existing/recurrent pain (eg, amputees with severe preamputation pain)
▸ High pain sensitivity ▸ Genetics ▸ Gender (females may be predisposed ) ▸ Age? (possibly older people less likely) ▸ Coping skills (eg, catastrophizing) ▸ Comorbid conditions/disease type ▸ Adjuvant therapy (eg, radiation, chemotherapy) ▸ Other factors (eg, anesthetic technique, surgical approach, malignancy)
Postoperative pain is just one reasonably good example of how acute pain can pass through the subacute phase and transition to chronic pain, which could be significantly more difficult to manage. With each type of acute pain, the path to chronic pain could be at least a 3-way street.
CONCLUSiONSSo here are some key take-home messages for us to keep in mind about this complex subject. Thought should be given
about whether or not acute and chronic pain share the same starting point—they may or may not. Certainly, purely from the vantage point of duration, they do, but it’s also much more complicated than that. From the neurologic per-spective, the transition from acute to chronic pain occurs in discrete pathophysiological steps involving multiple sig-naling pathways. The duration and intensity of the initial stimulus can lead to both peripheral and central sensitization that may act synergistically to exacerbate pain perception, and a multimodal approach may be best suited to target the multiple mechanisms involved3 in order to stem the transition. The patient’s psychosocial circumstances may also play a significant role in the transition from acute to chronic pain as the physical and psychological “circles” are intimately related regarding pain. This makes communi-cation an invaluable part of assessment and management, especially in stratifying patients at risk for the transition.
Vigilance, and thinking about all possible causes of acute and subacute pain involving expeditious, effective, and multimodal approaches could be the best defense against preventing acute pain from becoming chronic. It can be like trying to navigate a 3-way street.
References
1. World Health Organization. Noncommunicable diseases. Available at: www.who.int/topics/noncommunicable_diseases/en/.
2. Costigan M, Woolf CJ. Pain: molecular mechanisms. J Pain. 2000;1(3 suppl):35–44.
3. Voscopoulos C, Lema M. When does acute pain become chronic? Br J Anaesth. 2010;105 suppl 1:i69-i85.
4. Linton S. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–1156.
5. State of California Department of Industrial Relations Medical Treat-ment Utilization Schedule. Chronic Pain Medical Treatment Guidelines, 2009.
6. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367:1618–1625.
7. Eisenach JC. Preventing chronic pain after surgery: who, how, and when? Reg Anesth Pain Med. 2006;31:13.
8. Macrae WA . Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101:77–86.

WARNING: ADDICTION, ABUSE and MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL EXPOSURE; and
NEONATAL OPIOID WITHDRAWAL SYNDROME
Addiction, Abuse, and Misuse
Butrans exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death.
Assess each patient’s risk prior to prescribing Butrans, and monitor all patients regularly for the development of these behaviors or
conditions [see Warnings and Precautions (5.1) and Overdosage (10)].
Life-Threatening Respiratory Depression
Serious, life-threatening, or fatal respiratory depression may occur with use of Butrans. Monitor for respiratory depression, especially
during initiation of Butrans or following a dose increase. Misuse or abuse of Butrans by chewing, swallowing, snorting or injecting
buprenorphine extracted from the transdermal system will result in the uncontrolled delivery of buprenorphine and pose a significant
risk of overdose and death [see Warnings and Precautions (5.2)].
Accidental Exposure
Accidental exposure to even one dose of Butrans, especially by children, can result in a fatal overdose of buprenorphine [see Warnings
and Precautions (5.2)].
Neonatal Opioid Withdrawal Syndrome
Prolonged use of Butrans during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not
recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required
for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that
appropriate treatment will be available [see Warnings and Precautions (5.3)].
Parentheses refer to sections in the Full Prescribing Information.
CONTRAINDICATIONS� Butrans is contraindicated in patients with:
significant respiratory depression; acute or severe
bronchial asthma in an unmonitored setting or in
the absence of resuscitative equipment; known or
suspected paralytic ileus; hypersensitivity (eg,
anaphylaxis) to buprenorphine
WARNINGS AND PRECAUTIONSAddiction, Abuse, and Misuse
� Butrans contains buprenorphine, a Schedule III
controlled substance. Butrans exposes users to
the risks of opioid addiction, abuse, and misuse.
As modified-release products such as Butrans
deliver the opioid over an extended period of
time, there is a greater risk for overdose and
death, due to the larger amount of buprenorphine
present. Addiction can occur at recommended
doses and if the drug is misused or abused.
Assess each patient’s risk for opioid addiction,
abuse, or misuse prior to prescribing Butrans, and
monitor all patients during therapy for the
development of these behaviors or conditions.
Abuse or misuse of Butrans by placing it in the
mouth, chewing it, swallowing it, or using it in
ways other than indicated may cause choking,
overdose and death
Life-Threatening Respiratory Depression
� Serious, life-threatening, or fatal respiratory
depression has been reported with modified-
release opioids, even when used as
recommended, and if not immediately recognized
and treated, may lead to respiratory arrest and
death. The risk of respiratory depression is
greatest during the initiation of therapy or
following a dose increase; therefore, closely
monitor patients for respiratory depression.
Proper dosing and titration of Butrans are
essential. Overestimating the Butrans dose when
converting patients from another opioid product
can result in fatal overdose with the first dose.
Accidental exposure to Butrans, especially in
children, can result in respiratory depression and
death due to an overdose of buprenorphine
Neonatal Opioid Withdrawal Syndrome
� Prolonged use of Butrans during pregnancy can
result in neonatal opioid withdrawal syndrome
which may be life-threatening to the neonate if
not recognized and treated, and requires
management according to protocols developed
by neonatology experts
Interactions with Central Nervous System
Depressants
� Hypotension, profound sedation, coma,
respiratory depression, or death may result if
Butrans is used concomitantly with other CNS
depressants, including alcohol or illicit drugs that
can cause CNS depression. Start with Butrans 5
mcg/hour patch, monitor patients for signs of
sedation and respiratory depression, and
consider using a lower dose of the concomitant
CNS depressant
Use in Elderly, Cachectic, and Debilitated
Patients and Patients with Chronic
Pulmonary Disease
� Closely monitor elderly, cachectic, and debilitated
patients, and patients with chronic obstructive
pulmonary disease because of the increased risk
of life-threatening respiratory depression.
Consider the use of alternative non-opioid
analgesics in patients with chronic obstructive
pulmonary disease if possible
QTc Prolongation
� Avoid in patients with Long QT Syndrome, family
history of Long QT Syndrome, or those taking
Class IA or Class III antiarrhythmic medications
Hypotensive Effects
� Butrans may cause severe hypotension, including
orthostatic hypotension and syncope in
ambulatory patients. Monitor patients during
dose initiation or titration
Use in Patients with Head Injury or
Increased Intracranial Pressure
� Monitor patients taking Butrans who may be
susceptible to the intracranial effects of CO2
retention for signs of sedation and respiratory
depression. Avoid the use of Butrans in patients
with impaired consciousness or coma
Application Site Skin Reactions
� In rare cases, severe application site skin reactions
with signs of marked inflammation including
“burn,” “discharge,” and “vesicles” have occurred
Anaphylactic/Allergic Reactions
� Cases of acute and chronic hypersensitivity to
buprenorphine have been reported both in
clinical trials and in the post-marketing experience
Application of External Heat
� Avoid exposing the Butrans application site and
surrounding area to direct external heat sources.
There is a potential for temperature-dependent
increases in buprenorphine released from the
system resulting in possible overdose and death
Use in Patients with Gastrointestinal Conditions
� Avoid the use of Butrans in patients with paralytic
ileus and other GI obstructions. Monitor patients
with biliary tract disease, including acute
pancreatitis, for worsening symptoms
ADVERSE REACTIONS� Most common adverse reactions (≥5%) reported
by patients treated with Butrans in the clinical
trials were nausea, headache, application site
pruritus, dizziness, constipation, somnolence,
vomiting, application site erythema, dry mouth,
and application site rash
Please read Brief Summary of Full Prescribing Information on the following pages.
©2015 Purdue Pharma L.P.
Stamford, CT 06901-3431
L8365-A 3/15
Butrans
®
(buprenorphine) Transdermal System is indicated for the management of pain severe
enough to require daily, around-the-clock, long-term opioid treatment and for which alternative
treatment options are inadequate.
Limitations of Use: Because of the risks of addiction, abuse and misuse with opioids, even at
recommended doses, and because of the greater risk of overdose and death with extended-release
opioid formulations, reserve Butrans for use in patients for whom alternative treatment options
(eg, non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be
otherwise inadequate to provide sufficient management of pain. Butrans is not indicated as an
as-needed (prn) analgesic.
Visit
Butrans.com
for more information
or to print Butrans
Savings Cards
The first transdermal system to
deliver 7 days of buprenorphine
Butrans is a Schedule III extended-release opioid analgesic
Butrans — 7 Days of
Buprenorphine Delivery
Scale: 1" = 1"Trim: 15.5" x 10.5"Live: 14.5" x 9.5"Bleed: 17.25" x 11.25"Gutter: 1"
VW1677_a01.inddModifi ed: March 17, 2015 1:52 PM
Client: Abelson TaylorJob: VW1677Brand: ButransOperator: BTRound: 1
L8365-A

WARNING: ADDICTION, ABUSE and MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL EXPOSURE; and
NEONATAL OPIOID WITHDRAWAL SYNDROME
Addiction, Abuse, and Misuse
Butrans exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death.
Assess each patient’s risk prior to prescribing Butrans, and monitor all patients regularly for the development of these behaviors or
conditions [see Warnings and Precautions (5.1) and Overdosage (10)].
Life-Threatening Respiratory Depression
Serious, life-threatening, or fatal respiratory depression may occur with use of Butrans. Monitor for respiratory depression, especially
during initiation of Butrans or following a dose increase. Misuse or abuse of Butrans by chewing, swallowing, snorting or injecting
buprenorphine extracted from the transdermal system will result in the uncontrolled delivery of buprenorphine and pose a significant
risk of overdose and death [see Warnings and Precautions (5.2)].
Accidental Exposure
Accidental exposure to even one dose of Butrans, especially by children, can result in a fatal overdose of buprenorphine [see Warnings
and Precautions (5.2)].
Neonatal Opioid Withdrawal Syndrome
Prolonged use of Butrans during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not
recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required
for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that
appropriate treatment will be available [see Warnings and Precautions (5.3)].
Parentheses refer to sections in the Full Prescribing Information.
CONTRAINDICATIONS� Butrans is contraindicated in patients with:
significant respiratory depression; acute or severe
bronchial asthma in an unmonitored setting or in
the absence of resuscitative equipment; known or
suspected paralytic ileus; hypersensitivity (eg,
anaphylaxis) to buprenorphine
WARNINGS AND PRECAUTIONSAddiction, Abuse, and Misuse
� Butrans contains buprenorphine, a Schedule III
controlled substance. Butrans exposes users to
the risks of opioid addiction, abuse, and misuse.
As modified-release products such as Butrans
deliver the opioid over an extended period of
time, there is a greater risk for overdose and
death, due to the larger amount of buprenorphine
present. Addiction can occur at recommended
doses and if the drug is misused or abused.
Assess each patient’s risk for opioid addiction,
abuse, or misuse prior to prescribing Butrans, and
monitor all patients during therapy for the
development of these behaviors or conditions.
Abuse or misuse of Butrans by placing it in the
mouth, chewing it, swallowing it, or using it in
ways other than indicated may cause choking,
overdose and death
Life-Threatening Respiratory Depression
� Serious, life-threatening, or fatal respiratory
depression has been reported with modified-
release opioids, even when used as
recommended, and if not immediately recognized
and treated, may lead to respiratory arrest and
death. The risk of respiratory depression is
greatest during the initiation of therapy or
following a dose increase; therefore, closely
monitor patients for respiratory depression.
Proper dosing and titration of Butrans are
essential. Overestimating the Butrans dose when
converting patients from another opioid product
can result in fatal overdose with the first dose.
Accidental exposure to Butrans, especially in
children, can result in respiratory depression and
death due to an overdose of buprenorphine
Neonatal Opioid Withdrawal Syndrome
� Prolonged use of Butrans during pregnancy can
result in neonatal opioid withdrawal syndrome
which may be life-threatening to the neonate if
not recognized and treated, and requires
management according to protocols developed
by neonatology experts
Interactions with Central Nervous System
Depressants
� Hypotension, profound sedation, coma,
respiratory depression, or death may result if
Butrans is used concomitantly with other CNS
depressants, including alcohol or illicit drugs that
can cause CNS depression. Start with Butrans 5
mcg/hour patch, monitor patients for signs of
sedation and respiratory depression, and
consider using a lower dose of the concomitant
CNS depressant
Use in Elderly, Cachectic, and Debilitated
Patients and Patients with Chronic
Pulmonary Disease
� Closely monitor elderly, cachectic, and debilitated
patients, and patients with chronic obstructive
pulmonary disease because of the increased risk
of life-threatening respiratory depression.
Consider the use of alternative non-opioid
analgesics in patients with chronic obstructive
pulmonary disease if possible
QTc Prolongation
� Avoid in patients with Long QT Syndrome, family
history of Long QT Syndrome, or those taking
Class IA or Class III antiarrhythmic medications
Hypotensive Effects
� Butrans may cause severe hypotension, including
orthostatic hypotension and syncope in
ambulatory patients. Monitor patients during
dose initiation or titration
Use in Patients with Head Injury or
Increased Intracranial Pressure
� Monitor patients taking Butrans who may be
susceptible to the intracranial effects of CO2
retention for signs of sedation and respiratory
depression. Avoid the use of Butrans in patients
with impaired consciousness or coma
Application Site Skin Reactions
� In rare cases, severe application site skin reactions
with signs of marked inflammation including
“burn,” “discharge,” and “vesicles” have occurred
Anaphylactic/Allergic Reactions
� Cases of acute and chronic hypersensitivity to
buprenorphine have been reported both in
clinical trials and in the post-marketing experience
Application of External Heat
� Avoid exposing the Butrans application site and
surrounding area to direct external heat sources.
There is a potential for temperature-dependent
increases in buprenorphine released from the
system resulting in possible overdose and death
Use in Patients with Gastrointestinal Conditions
� Avoid the use of Butrans in patients with paralytic
ileus and other GI obstructions. Monitor patients
with biliary tract disease, including acute
pancreatitis, for worsening symptoms
ADVERSE REACTIONS� Most common adverse reactions (≥5%) reported
by patients treated with Butrans in the clinical
trials were nausea, headache, application site
pruritus, dizziness, constipation, somnolence,
vomiting, application site erythema, dry mouth,
and application site rash
Please read Brief Summary of Full Prescribing Information on the following pages.
©2015 Purdue Pharma L.P.
Stamford, CT 06901-3431
L8365-A 3/15
Butrans
®
(buprenorphine) Transdermal System is indicated for the management of pain severe
enough to require daily, around-the-clock, long-term opioid treatment and for which alternative
treatment options are inadequate.
Limitations of Use: Because of the risks of addiction, abuse and misuse with opioids, even at
recommended doses, and because of the greater risk of overdose and death with extended-release
opioid formulations, reserve Butrans for use in patients for whom alternative treatment options
(eg, non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be
otherwise inadequate to provide sufficient management of pain. Butrans is not indicated as an
as-needed (prn) analgesic.
Visit
Butrans.com
for more information
or to print Butrans
Savings Cards
The first transdermal system to
deliver 7 days of buprenorphine
Butrans is a Schedule III extended-release opioid analgesic
Butrans — 7 Days of
Buprenorphine Delivery
Scale: 1" = 1"Trim: 15.5" x 10.5"Live: 14.5" x 9.5"Bleed: 17.25" x 11.25"Gutter: 1"
VW1677_a01.inddModifi ed: March 17, 2015 1:52 PM
Client: Abelson TaylorJob: VW1677Brand: ButransOperator: BTRound: 1
L8365-A
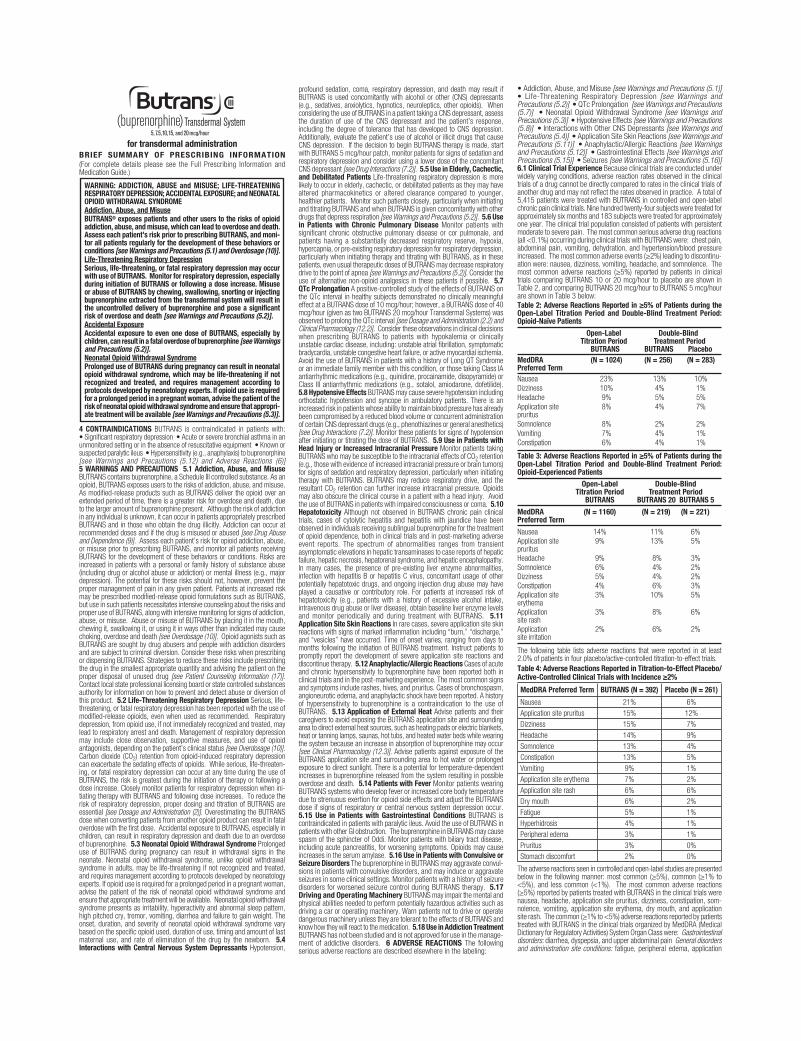
Scale: 1" = 1"Trim: 7.75" x 10.5"Live: 6.75" x 9.5"Bleed: 8.75" x 11.25"
VW1677_b01Modified: 17 March 2015 2:10 PM
Client: Abelson Taylor Job: VW1677 Brand: Butrans Operator: BTRound: 1
L8365-A
for transdermal administrationBRIEF SUMMARY OF PRESCRIBING INFORMATION (For complete details please see the Full Prescribing Information and Medication Guide.)
WARNING: ADDICTION, ABUSE and MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL EXPOSURE; and NEONATAL OPIOID WITHDRAWAL SYNDROME Addiction, Abuse, and MisuseBUTRANS® exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk prior to prescribing BUTRANS, and moni-tor all patients regularly for the development of these behaviors or conditions [see Warnings and Precautions (5.1) and Overdosage (10)].Life-Threatening Respiratory DepressionSerious, life-threatening, or fatal respiratory depression may occur with use of BUTRANS. Monitor for respiratory depression, especially during initiation of BUTRANS or following a dose increase. Misuse or abuse of BUTRANS by chewing, swallowing, snorting or injecting buprenorphine extracted from the transdermal system will result in the uncontrolled delivery of buprenorphine and pose a significant risk of overdose and death [see Warnings and Precautions (5.2)].Accidental ExposureAccidental exposure to even one dose of BUTRANS, especially by children, can result in a fatal overdose of buprenorphine [see Warnings and Precautions (5.2)].Neonatal Opioid Withdrawal SyndromeProlonged use of BUTRANS during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropri-ate treatment will be available [see Warnings and Precautions (5.3)].
4 CONTRAINDICATIONS BUTRANS is contraindicated in patients with: • Significant respiratory depression • Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment • Known or suspected paralytic ileus • Hypersensitivity (e.g., anaphylaxis) to buprenorphine [see Warnings and Precautions (5.12) and Adverse Reactions (6)] 5 WARNINGS AND PRECAUTIONS 5.1 Addiction, Abuse, and Misuse BUTRANS contains buprenorphine, a Schedule III controlled substance. As an opioid, BUTRANS exposes users to the risks of addiction, abuse, and misuse. As modified-release products such as BUTRANS deliver the opioid over an extended period of time, there is a greater risk for overdose and death, due to the larger amount of buprenorphine present. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed BUTRANS and in those who obtain the drug illicitly. Addiction can occur at recommended doses and if the drug is misused or abused [see Drug Abuse and Dependence (9)]. Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing BUTRANS, and monitor all patients receiving BUTRANS for the development of these behaviors or conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol abuse or addiction) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the proper management of pain in any given patient. Patients at increased risk may be prescribed modified-release opioid formulations such as BUTRANS, but use in such patients necessitates intensive counseling about the risks and proper use of BUTRANS, along with intensive monitoring for signs of addiction, abuse, or misuse. Abuse or misuse of BUTRANS by placing it in the mouth, chewing it, swallowing it, or using it in ways other than indicated may cause choking, overdose and death [see Overdosage (10)]. Opioid agonists such as BUTRANS are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing BUTRANS. Strategies to reduce these risks include prescribing the drug in the smallest appropriate quantity and advising the patient on the proper disposal of unused drug [see Patient Counseling Information (17)]. Contact local state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product. 5.2 Life-Threatening Respiratory Depression Serious, life- threatening, or fatal respiratory depression has been reported with the use of modified-release opioids, even when used as recommended. Respiratory depression, from opioid use, if not immediately recognized and treated, may lead to respiratory arrest and death. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status [see Overdosage (10)]. Carbon dioxide (CO2) retention from opioid-induced respiratory depression can exacerbate the sedating effects of opioids. While serious, life-threaten-ing, or fatal respiratory depression can occur at any time during the use of BUTRANS, the risk is greatest during the initiation of therapy or following a dose increase. Closely monitor patients for respiratory depression when ini-tiating therapy with BUTRANS and following dose increases. To reduce the risk of respiratory depression, proper dosing and titration of BUTRANS are essential [see Dosage and Administration (2)]. Overestimating the BUTRANS dose when converting patients from another opioid product can result in fatal overdose with the first dose. Accidental exposure to BUTRANS, especially in children, can result in respiratory depression and death due to an overdose of buprenorphine. 5.3 Neonatal Opioid Withdrawal Syndrome Prolonged use of BUTRANS during pregnancy can result in withdrawal signs in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing and amount of last maternal use, and rate of elimination of the drug by the newborn. 5.4 Interactions with Central Nervous System Depressants Hypotension,
profound sedation, coma, respiratory depression, and death may result if BUTRANS is used concomitantly with alcohol or other (CNS) depressants (e.g., sedatives, anxiolytics, hypnotics, neuroleptics, other opioids). When considering the use of BUTRANS in a patient taking a CNS depressant, assess the duration of use of the CNS depressant and the patient’s response, including the degree of tolerance that has developed to CNS depression. Additionally, evaluate the patient’s use of alcohol or illicit drugs that cause CNS depression. If the decision to begin BUTRANS therapy is made, start with BUTRANS 5 mcg/hour patch, monitor patients for signs of sedation and respiratory depression and consider using a lower dose of the concomitant CNS depressant [see Drug Interactions (7.2)]. 5.5 Use in Elderly, Cachectic, and Debilitated Patients Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance compared to younger, healthier patients. Monitor such patients closely, particularly when initiating and titrating BUTRANS and when BUTRANS is given concomitantly with other drugs that depress respiration [see Warnings and Precautions (5.2)]. 5.6 Use in Patients with Chronic Pulmonary Disease Monitor patients with significant chronic obstructive pulmonary disease or cor pulmonale, and patients having a substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression for respiratory depression, particularly when initiating therapy and titrating with BUTRANS, as in these patients, even usual therapeutic doses of BUTRANS may decrease respiratory drive to the point of apnea [see Warnings and Precautions (5.2)]. Consider the use of alternative non-opioid analgesics in these patients if possible. 5.7 QTc Prolongation A positive-controlled study of the effects of BUTRANS on the QTc interval in healthy subjects demonstrated no clinically meaningful effect at a BUTRANS dose of 10 mcg/hour; however, a BUTRANS dose of 40 mcg/hour (given as two BUTRANS 20 mcg/hour Transdermal Systems) was observed to prolong the QTc interval [see Dosage and Administration (2.2) and Clinical Pharmacology (12.2)]. Consider these observations in clinical decisions when prescribing BUTRANS to patients with hypokalemia or clinically unstable cardiac disease, including: unstable atrial fibrillation, symptomatic bradycardia, unstable congestive heart failure, or active myocardial ischemia. Avoid the use of BUTRANS in patients with a history of Long QT Syndrome or an immediate family member with this condition, or those taking Class IA antiarrhythmic medications (e.g., quinidine, procainamide, disopyramide) or Class III antiarrhythmic medications (e.g., sotalol, amiodarone, dofetilide). 5.8 Hypotensive Effects BUTRANS may cause severe hypotension including orthostatic hypotension and syncope in ambulatory patients. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics) [see Drug Interactions (7.2)]. Monitor these patients for signs of hypotension after initiating or titrating the dose of BUTRANS. 5.9 Use in Patients with Head Injury or Increased Intracranial Pressure Monitor patients taking BUTRANS who may be susceptible to the intracranial effects of CO2 retention (e.g., those with evidence of increased intracranial pressure or brain tumors) for signs of sedation and respiratory depression, particularly when initiating therapy with BUTRANS. BUTRANS may reduce respiratory drive, and the resultant CO2 retention can further increase intracranial pressure. Opioids may also obscure the clinical course in a patient with a head injury. Avoid the use of BUTRANS in patients with impaired consciousness or coma. 5.10 Hepatotoxicity Although not observed in BUTRANS chronic pain clinical trials, cases of cytolytic hepatitis and hepatitis with jaundice have been observed in individuals receiving sublingual buprenorphine for the treatment of opioid dependence, both in clinical trials and in post-marketing adverse event reports. The spectrum of abnormalities ranges from transient asymptomatic elevations in hepatic transaminases to case reports of hepatic failure, hepatic necrosis, hepatorenal syndrome, and hepatic encephalopathy. In many cases, the presence of pre-existing liver enzyme abnormalities, infection with hepatitis B or hepatitis C virus, concomitant usage of other potentially hepatotoxic drugs, and ongoing injection drug abuse may have played a causative or contributory role. For patients at increased risk of hepatotoxicity (e.g., patients with a history of excessive alcohol intake, intravenous drug abuse or liver disease), obtain baseline liver enzyme levels and monitor periodically and during treatment with BUTRANS. 5.11 Application Site Skin Reactions In rare cases, severe application site skin reactions with signs of marked inflammation including “burn,” “discharge,” and “vesicles” have occurred. Time of onset varies, ranging from days to months following the initiation of BUTRANS treatment. Instruct patients to promptly report the development of severe application site reactions and discontinue therapy. 5.12 Anaphylactic/Allergic Reactions Cases of acute and chronic hypersensitivity to buprenorphine have been reported both in clinical trials and in the post-marketing experience. The most common signs and symptoms include rashes, hives, and pruritus. Cases of bronchospasm, angioneurotic edema, and anaphylactic shock have been reported. A history of hypersensitivity to buprenorphine is a contraindication to the use of BUTRANS. 5.13 Application of External Heat Advise patients and their caregivers to avoid exposing the BUTRANS application site and surrounding area to direct external heat sources, such as heating pads or electric blankets, heat or tanning lamps, saunas, hot tubs, and heated water beds while wearing the system because an increase in absorption of buprenorphine may occur [see Clinical Pharmacology (12.3)]. Advise patients against exposure of the BUTRANS application site and surrounding area to hot water or prolonged exposure to direct sunlight. There is a potential for temperature-dependent increases in buprenorphine released from the system resulting in possible overdose and death. 5.14 Patients with Fever Monitor patients wearing BUTRANS systems who develop fever or increased core body temperature due to strenuous exertion for opioid side effects and adjust the BUTRANS dose if signs of respiratory or central nervous system depression occur. 5.15 Use in Patients with Gastrointestinal Conditions BUTRANS is contraindicated in patients with paralytic ileus. Avoid the use of BUTRANS in patients with other GI obstruction. The buprenorphine in BUTRANS may cause spasm of the sphincter of Oddi. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms. Opioids may cause increases in the serum amylase. 5.16 Use in Patients with Convulsive or Seizure Disorders The buprenorphine in BUTRANS may aggravate convul-sions in patients with convulsive disorders, and may induce or aggravate seizures in some clinical settings. Monitor patients with a history of seizure disorders for worsened seizure control during BUTRANS therapy. 5.17 Driving and Operating Machinery BUTRANS may impair the mental and physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of BUTRANS and know how they will react to the medication. 5.18 Use in Addiction Treatment BUTRANS has not been studied and is not approved for use in the manage-ment of addictive disorders. 6 ADVERSE REACTIONS The following serious adverse reactions are described elsewhere in the labeling:
• Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)] • Life-Threatening Respiratory Depression [see Warnings and Precautions (5.2)] • QTc Prolongation [see Warnings and Precautions (5.7)] • Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.3)] • Hypotensive Effects [see Warnings and Precautions (5.8)] • Interactions with Other CNS Depressants [see Warnings and Precautions (5.4)] • Application Site Skin Reactions [see Warnings and Precautions (5.11)] • Anaphylactic/Allergic Reactions [see Warnings and Precautions (5.12)] • Gastrointestinal Effects [see Warnings and Precautions (5.15)] • Seizures [see Warnings and Precautions (5.16)] 6.1 Clinical Trial Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. A total of 5,415 patients were treated with BUTRANS in controlled and open-label chronic pain clinical trials. Nine hundred twenty-four subjects were treated for approximately six months and 183 subjects were treated for approximately one year. The clinical trial population consisted of patients with persistent moderate to severe pain. The most common serious adverse drug reactions (all <0.1%) occurring during clinical trials with BUTRANS were: chest pain, abdominal pain, vomiting, dehydration, and hypertension/blood pressure increased. The most common adverse events (≥2%) leading to discontinu-ation were: nausea, dizziness, vomiting, headache, and somnolence. The most common adverse reactions (≥5%) reported by patients in clinical trials comparing BUTRANS 10 or 20 mcg/hour to placebo are shown in Table 2, and comparing BUTRANS 20 mcg/hour to BUTRANS 5 mcg/hour are shown in Table 3 below:Table 2: Adverse Reactions Reported in ≥5% of Patients during the Open-Label Titration Period and Double-Blind Treatment Period: Opioid-Naïve Patients Open-Label Double-Blind Titration Period Treatment Period BUTRANS BUTRANS PlaceboMedDRA (N = 1024) (N = 256) (N = 283)Preferred Term Nausea 23% 13% 10%Dizziness 10% 4% 1%Headache 9% 5% 5%Application site 8% 4% 7% pruritus Somnolence 8% 2% 2%Vomiting 7% 4% 1%Constipation 6% 4% 1%
Table 3: Adverse Reactions Reported in ≥5% of Patients during the Open-Label Titration Period and Double-Blind Treatment Period: Opioid-Experienced Patients Open-Label Double-Blind Titration Period Treatment Period BUTRANS BUTRANS 20 BUTRANS 5 MedDRA (N = 1160) (N = 219) (N = 221)Preferred Term Nausea 14% 11% 6%Application site 9% 13% 5% pruritus Headache 9% 8% 3%Somnolence 6% 4% 2%Dizziness 5% 4% 2%Constipation 4% 6% 3%Application site 3% 10% 5% erythema Application 3% 8% 6% site rash Application 2% 6% 2% site irritation
The following table lists adverse reactions that were reported in at least 2.0% of patients in four placebo/active-controlled titration-to-effect trials.Table 4: Adverse Reactions Reported in Titration-to-Effect Placebo/Active-Controlled Clinical Trials with Incidence ≥2%
MedDRA Preferred Term BUTRANS (N = 392) Placebo (N = 261)
Nausea 21% 6%Application site pruritus 15% 12%Dizziness 15% 7%Headache 14% 9%Somnolence 13% 4%Constipation 13% 5%Vomiting 9% 1%Application site erythema 7% 2%Application site rash 6% 6%Dry mouth 6% 2%Fatigue 5% 1%Hyperhidrosis 4% 1%Peripheral edema 3% 1%Pruritus 3% 0%Stomach discomfort 2% 0%
The adverse reactions seen in controlled and open-label studies are presented below in the following manner: most common (≥5%), common (≥1% to <5%), and less common (<1%). The most common adverse reactions (≥5%) reported by patients treated with BUTRANS in the clinical trials were nausea, headache, application site pruritus, dizziness, constipation, som-nolence, vomiting, application site erythema, dry mouth, and application site rash. The common (≥1% to <5%) adverse reactions reported by patients treated with BUTRANS in the clinical trials organized by MedDRA (Medical Dictionary for Regulatory Activities) System Organ Class were: Gastrointestinal disorders: diarrhea, dyspepsia, and upper abdominal pain General disorders and administration site conditions: fatigue, peripheral edema, application

site irritation, pain, pyrexia, chest pain, and asthenia Infections and infesta-tions: urinary tract infection, upper respiratory tract infection, nasopharyn-gitis, influenza, sinusitis, and bronchitis Injury, poisoning and procedural complications: fall Metabolism and nutrition disorders: anorexia Musculoskeletal and connective tissue disorders: back pain, arthralgia, pain in extremity, muscle spasms, musculoskeletal pain, joint swelling, neck pain, and myalgia Nervous system disorders: hypoesthesia, tremor, migraine, and paresthesia Psychiatric disorders: insomnia, anxiety, and depression Respiratory, thoracic and mediastinal disorders: dyspnea, pharyngolaryngeal pain, and cough Skin and subcutaneous tissue disorders: pruritus, hyperhi-drosis, rash, and generalized pruritus Vascular disorders: hypertension Other less common adverse reactions, including those known to occur with opioid treatment, that were seen in <1% of the patients in the BUTRANS trials include the following in alphabetical order: Abdominal distention, abdominal pain, accidental injury, affect lability, agitation, alanine aminotransferase increased, angina pectoris, angioedema, apathy, application site dermatitis, asthma aggravated, bradycardia, chills, confusional state, contact dermati-tis, coordination abnormal, dehydration, depersonalization, depressed level of consciousness, depressed mood, disorientation, disturbance in attention, diverticulitis, drug hypersensitivity, drug withdrawal syndrome, dry eye, dry skin, dysarthria, dysgeusia, dysphagia, euphoric mood, face edema, flatulence, flushing, gait disturbance, hallucination, hiccups, hot flush, hyperventilation, hypotension, hypoventilation, ileus, insomnia, libido decreased, loss of consciousness, malaise, memory impairment, mental impairment, mental status changes, miosis, muscle weakness, nervousness, nightmare, ortho-static hypotension, palpitations, psychotic disorder, respiration abnormal, respiratory depression, respiratory distress, respiratory failure, restlessness, rhinitis, sedation, sexual dysfunction, syncope, tachycardia, tinnitus, urinary hesitation, urinary incontinence, urinary retention, urticaria, vasodilatation, vertigo, vision blurred, visual disturbance, weight decreased, and wheezing. 7 DRUG INTERACTIONS 7.1 Benzodiazepines There have been a number of reports regarding coma and death associated with the misuse and abuse of the combination of buprenorphine and benzodiazepines. In many, but not all of these cases, buprenorphine was misused by self-injection of crushed buprenorphine tablets. Preclinical studies have shown that the combination of benzodiazepines and buprenorphine altered the usual ceiling effect on buprenorphine-induced respiratory depression, making the respiratory effects of buprenorphine appear similar to those of full opioid agonists. Closely monitor patients with concurrent use of BUTRANS and benzodiazepines. Warn patients that it is extremely dangerous to self-administer benzodiazepines while taking BUTRANS, and warn patients to use benzodiazepines concurrently with BUTRANS only as directed by their physician. 7.2 CNS Depressants The concomitant use of BUTRANS with other CNS depressants including sedatives, hypnotics, tranquilizers, general anesthetics, phenothiazines, other opioids, and alcohol can increase the risk of respiratory depression, profound sedation, coma and death. Monitor patients receiving CNS depressants and BUTRANS for signs of respiratory depression, sedation, and hypotension. When combined therapy with any of the above medications is considered, the dose of one or both agents should be reduced [see Dosage and Administration (2.2) and Warnings and Precautions (5.4)]. 7.3 Drugs Affecting Cytochrome P450 Isoenzymes Inhibitors of CYP3A4 and 2D6 Because the CYP3A4 isoenzyme plays a major role in the metabolism of buprenorphine, drugs that inhibit CYP3A4 activity may cause decreased clearance of buprenorphine which could lead to an increase in buprenorphine plasma concentrations and result in increased or prolonged opioid effects. These effects could be more pronounced with concomitant use of CYP2D6 and 3A4 inhibitors. If co-administration with BUTRANS is necessary, monitor patients for respiratory depression and sedation at frequent intervals and consider dose adjustments until stable drug effects are achieved [see Clinical Pharmacology (12.3)]. Inducers of CYP3A4 CYP450 3A4 inducers may induce the metabolism of buprenorphine and, therefore, may cause increased clearance of the drug which could lead to a decrease in buprenorphine plasma concentrations, lack of efficacy or, possibly, development of an abstinence syndrome in a patient who had developed physical dependence to buprenorphine. After stopping the treatment of a CYP3A4 inducer, as the effects of the inducer decline, the buprenorphine plasma concentration will increase which could increase or prolong both the therapeutic and adverse effects, and may cause serious respiratory depression. If co-administration or discontinuation of a CYP3A4 inducer with BUTRANS is necessary, monitor for signs of opioid withdrawal and consider dose adjustments until stable drug effects are achieved [see Clinical Pharmacology (12.3)]. 7.4 Muscle Relaxants Buprenorphine may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression. Monitor patients receiving muscle relaxants and BUTRANS for signs of respiratory depression that may be greater than otherwise expected. 7.5 Anticholinergics Anticholinergics or other drugs with anticholinergic activity when used concurrently with opioid analgesics may result in increased risk of urinary retention and/or severe constipation, which may lead to paralytic ileus. Monitor patients for signs of urinary retention or reduced gastric motil-ity when BUTRANS is used concurrently with anticholinergic drugs. 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy Clinical Considerations Fetal/neonatal adverse reactions Prolonged use of opioid analgesics during pregnancy for medical or nonmedical purposes can result in physical depen-dence in the neonate and neonatal opioid withdrawal syndrome shortly after birth. Observe newborns for symptoms of neonatal opioid withdrawal syndrome, such as poor feeding, diarrhea, irritability, tremor, rigidity, and seizures, and manage accordingly [see Warnings and Precautions (5.3)]. Teratogenic Effects - Pregnancy Category C There are no adequate and well-controlled studies in pregnant women. BUTRANS should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. In animal studies, buprenorphine caused an increase in the number of stillborn offspring, reduced litter size, and reduced offspring growth in rats at maternal exposure levels that were approximately 10 times that of human subjects who received one BUTRANS 20 mcg/hour, the maximum recommended human dose (MRHD). Studies in rats and rabbits demonstrated no evidence of teratogenicity fol-lowing BUTRANS or subcutaneous (SC) administration of buprenorphine during the period of major organogenesis. Rats were administered up to one BUTRANS 20 mcg/hour every 3 days (gestation days 6, 9, 12, & 15) or received daily SC buprenorphine up to 5 mg/kg (gestation days 6-17). Rabbits were administered four BUTRANS 20 mcg/hour every 3 days (gestation days 6, 9, 12, 15, 18, & 19) or received daily SC buprenorphine up to 5 mg/kg (gesta-tion days 6-19). No teratogenicity was observed at any dose. AUC values for buprenorphine with BUTRANS application and SC injection were approximately 110 and 140 times, respectively, that of human subjects who received the MRHD of one BUTRANS 20 mcg/hour. Non-Teratogenic Effects In a peri- and post-natal study conducted in pregnant and lactating rats, administration of buprenorphine either as BUTRANS or SC buprenorphine was associated with toxicity to offspring. Buprenorphine was present in maternal milk. Pregnant
rats were administered 1/4 of one BUTRANS 5 mcg/hour every 3 days or received daily SC buprenorphine at doses of 0.05, 0.5, or 5 mg/kg from gestation day 6 to lactation day 21 (weaning). Administration of BUTRANS or SC buprenorphine at 0.5 or 5 mg/kg caused maternal toxicity and an increase in the number of stillborns, reduced litter size, and reduced offspring growth at maternal exposure levels that were approximately 10 times that of human subjects who received the MRHD of one BUTRANS 20 mcg/hour. Maternal toxicity was also observed at the no observed adverse effect level (NOAEL) for offspring. 8.2 Labor and Delivery Opioids cross the placenta and may produce respiratory depression in neonates. BUTRANS is not for use in women during and immediately prior to labor, when shorter acting analgesics or other analgesic techniques are more appropriate. Opioid analgesics can prolong labor through actions that temporarily reduce the strength, duration, and frequency of uterine contractions. However this effect is not consistent and may be offset by an increased rate of cervical dilatation, which tends to shorten labor. 8.3 Nursing Mothers Buprenorphine is excreted in breast milk. The amount of buprenorphine received by the infant varies depending on the maternal plasma concentration, the amount of milk ingested by the infant, and the extent of first pass metabolism. Withdrawal symptoms can occur in breast-feeding infants when maternal administration of buprenorphine is stopped. Because of the potential for adverse reactions in nursing infants from BUTRANS, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. 8.4 Pediatric Use The safety and efficacy of BUTRANS in patients under 18 years of age has not been established. 8.5 Geriatric Use Of the total number of subjects in the clinical trials (5,415), BUTRANS was admin-istered to 1,377 patients aged 65 years and older. Of those, 457 patients were 75 years of age and older. In the clinical program, the incidences of selected BUTRANS-related AEs were higher in older subjects. The incidences of application site AEs were slightly higher among subjects <65 years of age than those ≥65 years of age for both BUTRANS and placebo treatment groups. In a single-dose study of healthy elderly and healthy young subjects treated with BUTRANS 10 mcg/hour, the pharmacokinetics were similar. In a separate dose-escalation safety study, the pharmacokinetics in the healthy elderly and hypertensive elderly subjects taking thiazide diuretics were similar to those in the healthy young adults. In the elderly groups evaluated, adverse event rates were similar to or lower than rates in healthy young adult subjects, except for constipation and urinary retention, which were more common in the elderly. Although specific dose adjustments on the basis of advanced age are not required for pharmacokinetic reasons, use caution in the elderly population to ensure safe use [see Clinical Pharmacology (12.3)]. 8.6 Hepatic Impairment In a study utilizing intravenous buprenorphine, peak plasma levels (Cmax) and exposure (AUC) of buprenorphine in patients with mild and moderate hepatic impairment did not increase as compared to those observed in subjects with normal hepatic function. BUTRANS has not been evaluated in patients with severe hepatic impairment. As BUTRANS is intended for 7-day dosing, consider the use of alternate analgesic therapy in patients with severe hepatic impairment [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)]. 9 DRUG ABUSE AND DEPENDENCE 9.1 Controlled Substance BUTRANS contains buprenorphine, a Schedule III controlled substance with an abuse potential similar to other Schedule III opioids. BUTRANS can be abused and is subject to misuse, addiction and criminal diversion [see Warnings and Precautions (5.1)]. 9.2 Abuse All patients treated with opioids require careful monitoring for signs of abuse and addiction, since use of opioid analgesic products carries the risk of addiction even under appropriate medical use. Drug abuse is the intentional non-therapeutic use of an over-the-counter or prescription drug, even once, for its rewarding psychological or physiological effects. Drug abuse includes, but is not limited to the following examples: the use of a prescription or over-the-counter drug to get “high”, or the use of steroids for performance enhancement and muscle build up. Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and includes: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal. “Drug-seeking” behavior is very common to addicts and drug abusers. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examina-tion, testing or referral, repeated claims of loss of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating physician(s). “Doctor shopping” (visiting multiple prescribers) to obtain additional prescriptions is common among drug abus-ers and people suffering from untreated addiction. Preoccupation with achieving adequate pain relief can be appropriate behavior in a patient with poor pain control. Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should be aware that addic-tion may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true addiction. BUTRANS, like other opioids, can be diverted for non-medical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by state law, is strongly advised. Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to reduce abuse of opioid drugs. Risks Specific to the Abuse of BUTRANS BUTRANS is intended for transdermal use only. Abuse of BUTRANS poses a risk of overdose and death. This risk is increased with concurrent abuse of BUTRANS with alcohol and other substances including other opioids and benzodiazepines [see Warnings and Precautions (5.4) and Drug Interactions (7.2)]. Intentional compromise of the transdermal delivery system will result in the uncontrolled delivery of buprenorphine and pose a significant risk to the abuser that could result in overdose and death [see Warnings and Precautions (5.1)]. Abuse may occur by applying the transdermal system in the absence of legitimate purpose, or by swallowing, snorting, or injecting buprenorphine extracted from the transdermal system. 9.3 Dependence Both tolerance and physical dependence can develop during chronic opioid therapy. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia (in the absence of disease progression or other external factors). Tolerance may occur to both the desired and undesired effects of drugs, and may develop at different rates for different effects. Physical dependence results in withdrawal symptoms after abrupt discon-tinuation or a significant dose reduction of a drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity, e.g., naloxone, nalmefene, or mixed agonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued opioid usage. BUTRANS should not be abruptly discontinued [see Dosage and Administration (2.3)]. If BUTRANS is abruptly discontinued in a physically-dependent patient, an abstinence syndrome may occur. Some or all of the
following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, myalgia, and mydriasis. Other signs and symptoms also may develop, including: irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, or increased blood pressure, respiratory rate, or heart rate. Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal symptoms [see Use in Specific Populations (8.1)]. 10 OVERDOSAGE Clinical Presentation Acute overdosage with BUTRANS is manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, bradycardia, hypotension, partial or complete airway obstruction, atypical snoring and death. Marked mydriasis rather than miosis may be seen due to severe hypoxia in overdose situations. Treatment of Overdose In case of overdose, priorities are the re-establish-ment of a patent and protected airway and institution of assisted or controlled ventilation if needed. Employ other supportive measures (including oxygen, vasopressors) in the management of circulatory shock and pulmonary edema as indicated. Cardiac arrest or arrhythmias will require advanced life support techniques. Naloxone may not be effective in reversing any respiratory depression produced by buprenorphine. High doses of naloxone, 10-35 mg/70 kg, may be of limited value in the management of buprenorphine overdose. The onset of naloxone effect may be delayed by 30 minutes or more. Doxapram hydrochloride (a respiratory stimulant) has also been used. Remove BUTRANS immediately. Because the duration of reversal would be expected to be less than the duration of action of buprenorphine from BUTRANS, carefully monitor the patient until spontaneous respiration is reliably re-established. Even in the face of improvement, continued medical monitoring is required because of the possibility of extended effects as buprenorphine continues to be absorbed from the skin. After removal of BUTRANS, the mean buprenorphine concentrations decrease approximately 50% in 12 hours (range 10-24 hours) with an apparent terminal half-life of approximately 26 hours. Due to this long apparent terminal half-life, patients may require monitoring and treatment for at least 24 hours. In an individual physically dependent on opioids, admin-istration of an opioid receptor antagonist may precipitate an acute withdrawal. The severity of the withdrawal produced will depend on the degree of physi-cal dependence and the dose of the antagonist administered. If a decision is made to treat serious respiratory depression in the physically dependent patient with an opioid antagonist, administration of the antagonist should be begun with care and by titration with smaller than usual doses of the antagonist. 17 PATIENT COUNSELING INFORMATION Advise the patient to read the FDA-approved patient labeling (Medication Guide and Instructions for Use). Addiction, Abuse, and Misuse Inform patients that the use of BUTRANS, even when taken as recommended, can result in addiction, abuse, and misuse, which could lead to overdose and death [see Warnings and Precautions (5.1)]. Instruct patients not to share BUTRANS with others and to take steps to protect BUTRANS from theft or misuse. Life-Threatening Respiratory Depression Inform patients of the risk of life-threatening respiratory depression, including information that the risk is greatest when starting BUTRANS or when the dose is increased, and that it can occur even at recommended doses [see Warnings and Precautions (5.2)]. Advise patients how to recognize respiratory depression and to seek medical attention if breathing difficulties develop. Accidental Exposure Inform patients that accidental exposure, especially in children, may result in respiratory depression or death [see Warnings and Precautions (5.2)]. Instruct patients to take steps to store BUTRANS securely and to dispose of unused BUTRANS by folding the patch in half and flushing it down the toilet. Neonatal Opioid Withdrawal Syndrome Inform female patients of reproductive potential that prolonged use of BUTRANS during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated [see Warnings and Precautions (5.3)]. Interaction with Alcohol and other CNS Depressants Inform patients that potentially serious additive effects may occur if BUTRANS is used with alcohol or other CNS depressants, and not to use such drugs unless supervised by a health care provider. Important Administration Instructions Instruct patients how to properly use BUTRANS, including the following: 1. To carefully follow instructions for the application, removal, and disposal of BUTRANS. Each week, apply BUTRANS to a different site based on the 8 described skin sites, with a minimum of 3 weeks between applications to a previously used site. 2. To apply BUTRANS to a hairless or nearly hairless skin site. If none are available, instruct patients to clip the hair at the site and not to shave the area. Instruct patients not to apply to irritated skin. If the application site must be cleaned, use clear water only. Soaps, alcohol, oils, lotions, or abrasive devices should not be used. Allow the skin to dry before applying BUTRANS. Hypotension Inform patients that BUTRANS may cause orthostatic hypotension and syncope. Instruct patients how to recognize symptoms of low blood pressure and how to reduce the risk of serious consequences should hypotension occur (e.g., sit or lie down, carefully rise from a sitting or lying position). Driving or Operating Heavy Machinery Inform patients that BUTRANS may impair the ability to perform potentially hazardous activities such as driving a car or operating heavy machinery. Advise patients not to perform such tasks until they know how they will react to the medication. Constipation Advise patients of the potential for severe constipation, including management instructions and when to seek medical attention. Anaphylaxis Inform patients that anaphylaxis has been reported with ingredients contained in BUTRANS. Advise patients how to recognize such a reaction and when to seek medical attention. Pregnancy Advise female patients that BUTRANS can cause fetal harm and to inform the prescriber if they are pregnant or plan to become pregnant. Disposal Instruct patients to refer to the Instructions for Use for proper disposal of BUTRANS. Patients can dispose of used or unused BUTRANS patches in the trash by sealing them in the Patch-Disposal Unit, following the instructions on the unit. Alternatively, instruct patients to dispose of used patches by folding the adhesive side of the patch to itself, then flushing the patch down the toilet immediately upon removal. Unused patches should be removed from their pouches, the protective liners removed, the patches folded so that the adhesive side of the patch adheres to itself, and immediately flushed down the toilet. Instruct patients to dispose of any patches remaining from a pre-scription as soon as they are no longer needed.Healthcare professionals can telephone Purdue Pharma’s Medical Services Department (1-888-726-7535) for information on this product.Distributed by: Purdue Pharma L.P., Stamford, CT 06901-3431Manufactured by: LTS Lohmann Therapy Systems Corp., West Caldwell, NJ 07006U.S. Patent Numbers 5681413; 5804215; 6264980; 6315854; 6344211; RE41408; RE41489; RE41571.© 2014, Purdue Pharma L.P. This brief summary is based on BUTRANS Prescribing Information 303385-0A, Revised 06/2014 (A)
Scale: 1" = 1"Trim: 7.75" x 10.5"Live: 6.75" x 9.5"Bleed: 8.75" x 11.25"
VW1677_c01Modified: 17 March 2015 2:12 PM
Client: Abelson Taylor Job: VW1677 Brand: Butrans Operator: BTRound: 1
L8365-A

by Michael R. Clark MD, MPH, MBA
A
or…
by Michael R. Clark MD, MPH, MBA

…a whimper?
How Extroverts and Introverts Manage Pain

48 | PWJ | www.painweek.org Q3 | 2015
abstract: Frontline practitioners are faced, every day, with managing patients in chron-ic pain. To exacerbate the issue, people in chronic pain come with different personality traits that produce unique individuals who often create obstructions to a successful ther-apeutic relationship and health outcome. This article examines common theories of temper-amental traits, the most typical personality disorders, and how specific profiles play out in the physician/patient relationship. Armed with this understanding of a patient in distress, the practitioner can follow some basic tech-niques for managing the patient’s vulnerabili-ties and guide the patient back into facing the challenge of chronic pain with greater like-lihood of successful response to treatment.
BeHAViORAL
This is the way the world endsThis is the way the world endsThis is the way the world endsNot with a bang but a whimper.
T.S. Eliot’s poem, The Hollow Men, the concluding verse presents us with a heralding warning:
In

www.painweek.org | PWJ | 49Q3 | 2015
William Osler is often quoted noting, “The good physician treats the disease; the great physician treats the patient who has the disease.” Osler is recognizing the impor-tance of the individual person in the practice of medicine. Of course, physicians should know a patient and appreciate his/her life story as they encounter a disease that has taken the patient’s own narrative in an unexpected direction of potential tragedy. However, what aspects of that particular individual might influence the way in which s/he responds to the plight of having a disease? How do specific personal-ity traits factor into the patient’s behavior while ill and the doctor-patient relationship as the disease follows its course and treatments are prescribed?
LeVeLS OF MeNTAL LiFeMcHugh and Slavney described 4 perspectives of psychiatry: diseases, dimensions, behaviors, and life stories.1 This frame-work facilitates a coherent conversation about how to formu-late the disorders of mental life and rests on the foundation of the components of psychological life. These components are hierarchical and interactive representing the domains of brain-based cerebral faculties, motivational drives, constitu-tional dimensions, and personal development.2
Mental disorders may be derived from each component.3 For example, psychiatric diseases emerge from pathological cere-bral faculties; behavioral disorders result from inappropriate motivations and distorted goals; problematic dispositions
evoke difficulty because of the constitutional composition; and disruptive life stories are the outcome of personal devel-opment gone awry. In general, psychiatric treatment aims to produce a remedy for disease, an interruption of disordered behaviors, guidance for the challenges of disposition, and rescripting of dissatisfying life stories.
In appreciating the role of the individual and their person-ality in sickness and suffering, the dimensional perspective focuses on “What the patient is.” The dimensions or traits of a person are derived by quantification and gradation along specific continuua. The application of the dimensional per-spective allows for the acceptance of measurable individual variation, interaction of distinct inherent traits, and their composition to produce uniqueness of person.
THe CONTRiBUTiON OF TRAiTSSigmund Freud commented, “Every normal person, in fact, is only normal on the average. His ego approximates to that of the psychotic in some part or other and to a greater or lesser extent.” Here Freud is describing how individuals exist along a spectrum or “normal” distribution. While most are at the center or possess average amounts of a given trait, some few exist at the extremes and will appear exceptional in certain contexts.
Constitutional dimensions are those universal features pres-ent in all people. They are graded in character from less
“Psychological traits resemble physical dispositional attributes such as the solubility of a substance or the electrical resistance of a wire.”
The poem is a call to meaningful action to create a life well-lived. The hollow men lack conviction and commitment. As a result, they contribute nothing and nothing comes of scrutinizing them. The implied comparison is the contrast with those individuals who make a difference and flourish in a world of their own making.

50 | PWJ | www.painweek.org Q3 | 2015
to more. They may exist in a number of realms: physical, psychological, cultural. These traits are axes of measured individual variation. The psychological vulnerabilities can in part derive as inherent dispositional potentials based on the distance an individual deviates from average on any given dimension.
Psychological dimensions are a subgroup of human con-stitutional dimensions. Expanding on Osler’s observation, the doing of foolish things may require a brain but the brain is not the problem. And, what patients choose to do often depends on who they are and not what they have. The excellent care provided by Osler’s “great physician” is for-mulated with contributions of perspectives beyond that of just diseases.
THe eFFeCT OF TRAiTSMartha Washington appreciated the role of temperament in a person’s own narrative. She said, “I am determined to be cheerful and happy in whatever situation I may find myself. For I have learned that the greater part of our misery or unhappiness is determined not by our circumstance but by our disposition.” The disposition referred to by Washington is the sum of inherent and latent characteristics evoked or brought to light by events that demand and challenge the individual’s capacities.
These traits manifest as a tendency to respond in a cer-tain manner under particular circumstances. Psychological traits resemble physical dispositional attributes such as the solubility of a substance or the electrical resistance of a wire. In order to elucidate the disposition of a patient, an exten-sive personal history is required to illuminate the hidden or presently unevoked factors. This explicit knowledge will help predict the individual’s capabilities under specific con-ditions such as being sick.
The prediction of how a patient may respond to an illness based on their personality requires a derivative exercise. The process of derivation produces an expression or for-mula that makes sense of a clinical event (symptom, sign, syndrome) as the outcome of some observable change in a basic source. Facts are collected and generative functions explain the transmogrifications between source, mediation, and result. For difficulties within the dimensional perspec-tive, a patient’s distress (neurotic symptoms) is the response to the provocation of life events on the potential of his per-sonality traits.
“The potential exists for a patient to meet the challenge of illness with grace or to succumb to the vicissitudes of health even when others would expect recovery.”
Potential
Personality Traits
Provocation
Life Events
Response
Neurotic Symptoms
‘X’
(‘f’ 1) (‘f’ 2)
Source
‘Y’
Mediation
‘Z’
Result
Aim: Fill in the unknowns with facts (X, Y, Z) and generative functions (‘f’ 1, ‘f’ 2).
❶ Operation Derivative
❷ Dimensions Derivative
BEHAVIORAL

www.painweek.org | PWJ | 51Q3 | 2015
ReALiZiNG POTeNTiALThe inherent vulnerabilities that lie dormant in traits pre-dispose patients to suffer beyond just what symptoms their disease would produce. The potential exists for a patient to meet the challenge of illness with grace or to succumb to the vicissitudes of health even when others would expect recov-ery. Henry Ford explains, “Life is a series of experiences, each one of which makes us bigger, even though sometimes it is hard to realize this. For the world was built to develop character, and we must learn that the setbacks and grieves which we endure help us in our marching onward.” The hollow men represent the missed opportunities afforded by experience. The hollow men lack an essential ingredient. They are a group of scarecrow-like individuals who exist in a state between life and death and suffer from a serious case of moral paralysis. Eliot’s poem is not so much about the end of the world as about the consequences of people who sit around and talk without ever trying to put their beliefs or ideas into practice.
The force behind realizing potential is temperament, par-ticularly affective dispositional characteristics. The affec-tive dimensions emerge in an individual’s interactions with others and his life history. The ultimate effects shape char-acter as expressed in matters such as judgment, trustwor-thiness, loyalty, commitments, and dependability. These achievements are the endproduct of combining endowment with experience. The patient’s character will influence how well they adapt to and compensate for their illness and its direct effects on health and function.
Just as the attainment of character is the outcome of gaining experience with one’s temperament under different circum-stances, other dimensions possess specific goals for how the person processes their experiences and their accompanying demands. Cognitive capacity is composed of both fluid and crystallized intelligences. If all goes well, the products are educational and vocational skills. In contrast, maturity in reasoning occurs over time as the brain grows and executive skill develops. Thus, judgment is the goal. Another example is evident in cultural affiliation. People express an affinity for norms and attachment that result in a sense of belonging to the group and loyalty to its members. When this recipe is followed, facilitated by analogous structures of guidance and remediation, an individual’s membership is granted.
THe TROUBLe WiTH TRAiTSHuman beings often fall short of their goals. Their aspira-tions and expectations do not match the reality and analy-sis of “How did this happen?” Peter de Vries captures this dissatisfaction stating, “The difficulty with marriage is that we fall in love with a personality, but must live with a char-acter.” In many instances when we are caring for patients in distress, they are responding with emotional or behavioral actions excessive in degree or frequency but not abnormal in kind. The patient is failing to grasp (either acknowledge or appreciate) their own contribution to the distress and how to manage or prevent it. In problems related to traits, the patient deviates to an extreme along one or more dimen-sions of human psychological variation. The causes may be
We are the hollow menWe are the stuffed menLeaning togetherHeadpiece filled with straw. Alas!

52 | PWJ | www.painweek.org Q3 | 2015
varied such as brain injuries, genetic constitution, and devel-opmental experience. Regardless, life events are provoking and sustaining responses rendered likely by the trait(s).
Personality disorders are the collection of common com-positions that predispose one to “an enduring pattern of inner experience and behavior that deviates markedly from the expectations of the individual’s culture” as defined in the Diagnostic and Statistical Manual (DSM) of psychia-try.4 The operationalized criteria for a personality disorder focus on clinically significant distress or impairment in important areas of functioning coupled with inflexibility and pervasiveness across a broad range of personal and social situations.
The difficulties of people with personality disorders are manifest in problems with impulse control; interpersonal functioning; range, intensity, lability, and appropriateness of emotional responses; and ways of perceiving and inter-preting oneself, other people, and events. Generally, clus-ters of these difficulties have been characterized in DSM as those who are exceptionally odd, dramatic, or anxious compared to individuals without a personality disorder. The clusters or types of personality disorders serve an efficient utility for diagnosis and general treatment approaches. However, categories formed from dimensional constructs are arbitrary cut-offs that fail to capture subtle variation.
TRAiTS AND TYPeSPersonality theory has long been debated and taken on a variety of forms.5 Jung described archetypes as universal
patterns and images that derive from the collective uncon-scious and are the psychic counterpart of instinct.6 He described dimensional potential and evoked responses as autonomous and hidden forms that are transformed once they enter consciousness and are given particular expression by individuals and their cultures. Jung understood arche-types as a collection of latent constructs noting that because they were unconscious, the existence of archetypes can only be deduced indirectly by examining behavior, images, art, myths, religions, or dreams.
The Myers-Briggs Type Indicator builds on Jung’s typolog-ical theories utilizing 4 principle psychological functions by which people experience the world: sensation, intuition, feeling, and thinking modified by attitude.7 The premise proposes naturally occurring differences in how people perceive the world and make decisions. These differences grouped by psychological function result in specific pref-erences in the way we construe individual experiences, and these preferences underlie personal interests, needs, values, and motivations.
Costa and McCrae developed the five-factor model of tem-perament.8 Their model builds on Eysenck’s dimensions of personality composed of 3 orthogonal trait axes: emotional stability, extroversion, and psychoticism.9 The five factors are similarly named and include neuroticism, agreeableness, extroversion, conscientiousness, and openness to experience. Neuroticism is a trait that encompasses the strength of emo-tions and the tendency to experience them intensely. Agree-ableness describes one’s orientation towards others as more altruistic as opposed to antagonistic. Conscientiousness is
“Extroverts are action oriented in contrast to introverts who are thought oriented. Extroverts seek breadth of knowledge and influence while introverts seek depth in these areas.”
BEHAVIORAL

www.painweek.org | PWJ | 53Q3 | 2015
a manifestation of an individual’s organization, motivation, and persistence in contrast to Openness which relates to the person’s appreciation of an experience for its own sake based on curiosity vs preference for consistency.
One consistent dimension of temperament described by mul-tiple scholars of personality is the Introversion–Extroversion spectrum. Extroverts are action oriented in contrast to intro-verts who are thought oriented. Extroverts seek breadth of knowledge and influence while introverts seek depth in these areas. Extroversion is described by some as the immediacy of emotions and speed of interpersonal interactions. Extroverts often prefer more frequent interactions whereas introverts seek out more substantial interactions. Usually extroverts are outgoing and energetic not solitary and reserved, who seek stimulation in the company of others. And, extroverts typically recharge their energy by spending time with people instead of introverts who receive energy by spending time alone.
TRAiT iNTeRACTiONSMoving from factors or axes to clusters or types and ulti-mately to detailed profiles or unique individuals is a pro-cess of complex interactions of numerous traits and made only more mysterious by the ongoing encounters with life events and other people. As noted by John Steinbeck, “It has always seemed strange to me... the things we admire in men, kindness and generosity, openness, honesty, understanding and feeling, are the concomitants of failure in our system. And those traits we detest, sharpness, greed, acquisitiveness, meanness, egotism and self-interest, are the traits of success. And while men admire the quality of the first they love the produce of the second.”
Hippocrates was likely the first to describe these interac-tions in his characterization of the 4 humors that appear to result from the 2x2 table of Eysenck’s axes of instability/stability and introversion/extroversion.10
As Jung described, indirect deduction helps to illuminate the odd and suspicious Cluster A personality disorders as more likely to be unstable and disagreeable introverts. The Clus-ter B personality disorders who are dramatic in form and characterized by emotional, aggressive, and self-centered tendencies are often noted to be unstable extroverts. But, the anxious Cluster C group are more likely to be composed as unstable, conscientious introverts as an explanation for their hypersensitive, inhibited and yet controlling natures.
In other words, thinking about the primary traits and their quantity in a particular individual, the physician may be able to predict the typical provoked responses of strong emotional reactions that would be exhibited under stressful conditions. Unstable extroverts are prone to explosive anger, depressive sulking, finger-pointing, and especially disrup-tive responses when intoxicated with alcohol or prescribed
medications such as opioids and benzodiazepines. In con-trast, unstable introverts are more easily demoralized with prolonged depressive responses coupled with anxiety over change anticipating the worst outcome. These patients also tend toward more obsessionality and scrupulosity (char-acterized by pathological guilt about moral or religious issues) that interferes with decision making and expending resources for their own benefit.
Another aspect to provoked responses relates to risk factors for ease of conditioning in learning or acquiring disruptive behaviors. For example, the unstable extrovert who seeks out social and pleasurable experiences is more likely to develop drug dependence, bulimia, hysterical conditions, and criminal behaviors. The unstable introvert, however, is more likely to develop anorexia nervosa, social phobias, and hypochondriasis that emerge as manifestations of their worry, shyness, and aversion to risk.
eXTROVeRSiON: BeST TRAiT eVeR!Best-selling author Susan Cain reminds that “All personal-ity traits have their good side and their bad side. But for a long time, we’ve seen introversion only through its negative side and extroversion mostly through its positive side.”11 She keeps the discussion of traits and their potentials on obser-vations of quantifying specific aspects of factors rather than judgments of what they are likely to produce.
For example, introverts are characterized by being solitary, reflective, internally-focused, analytical, living in the past or future, and punishment averse. These aspects of who introverts are is not good or bad nor an absolute strength or vulnerability but relative to the demands of the context in which the introvert is placed. Introverts suffering from pain are more likely to suffer in silence, wonder what is wrong, and become preoccupied with the details of somatic sensa-tions. Their ability to become detail-focused leads to doubts about what was missed in the past and what will go wrong in the future. Their general emotional stance is “I don’t want to feel bad.”
The extrovert possesses the traits of being externally focused, interactive, social, reactive, living in the moment, and dependent on rewards for motivation and reinforce-ment. Again, none are specifically good or bad but relative strengths and weaknesses under different circumstances. When in pain, extroverts will actively pursue health care hoping someone will figure out the problem. They repeat-edly tell their story often omitting important details with impatience as they expect immediate responses, stating, “I want to feel good now.”
These examples are not limited to introverts and extroverts and include other major factors such as neuroticism. The emotionally unstable or “neurotic” reacts poorly to stress

54 | PWJ | www.painweek.org Q3 | 2015
with unpredictable reactions that tend toward dramatic cat-astrophizing. This results in part because of their tendency to experience negative emotions more so than positive ones coupled with the ability of their emotions to be intense. They are sensitive to the withdrawal of attention from others and feel easily threatened. As expected, when in pain, introverts are easily distressed, defensive, and prone to attack others who are trying to help because they presume the worst is going to happen. In addition, their feelings dominate inter-personal interactions making the transfer of detailed facts difficult, and they are inconsistent and more likely to default to maladaptive coping strategies because they cannot focus on developing specific problem-solving skills.
THe ROLe OF eXPeRieNCeAlbert Einstein was quoted saying, “The only source of knowledge is experience.” The hollow men lack this crucial ingredient to a meaningful life.
This shadow has fallen between the potential for action and the action itself to prevent them from doing anything. The hollow men cannot bring their ideas into reality. They move but do not coordinate or inform their movements into action. The shadow has blocked their intentions.
Experience not only provides opportunity for action but also interacts with traits to influence future tendencies.
Extroverts are not as easily conditioned by punishments as introverts. They are poorly responsive to negative rein-forcements because they are reward-dependent. Rewards motivate extroverts who are quick to decondition or extin-guish behaviors in the absence of ongoing rewards. Intro-verts are more slow to extinguish due to their concern about what will go wrong. Therefore, they are motivated not so much by the opportunity of getting a reward but more so by wanting to avoid a potential punishment.
The cycle of dysfunction can intensify once certain dis-orders have taken hold of the patient. The unstable extro-vert who develops a substance use disorder finds it easier to ignore the punishments and negative consequences of drug use and pursue the reward-laden opportunities of intoxication. The unstable introvert with a social phobia will be more likely to overreact to both real and imagined punishments shying away from challenges regardless of the potential for a significant reward.
GUiDANCe AND ReMeDiATiON FOR THe VULNeRABLeThe immutability of trait endowments projects a sense of futility about treating these patients. However, hope and optimism lay in the physician’s role in generating specific experiences for them. The problem is not their dimensional foundation but helping them to deal with the
Between the ideaAnd the realityBetween the motionAnd the actFalls the Shadow
BEHAVIORAL

www.painweek.org | PWJ | 55Q3 | 2015
clinical problem by addressing the provocations of distress and learning to change their subsequent responses. The guidance offered provides a form of remediation that adds particular experiences that will enhance their coping skills.
Each major vulnerability requires a different form of help from the physician. Introverts need extra time for listening and providing more detailed information. Anxiety reduction techniques give the patient a task to focus on mastering and produce a sense of control over relevant symptoms. While introverts need reminders that the body is not a machine that is easily fixed, careful physical examinations with com-prehensive plans and predictable follow-up will be reassur-ing. However, excessive consultations and other sources of information such as performing Internet searches should be discouraged because they tend to introduce unfounded theories and vague suppositions that cannot be ruled out with confidence thereby increasing the introverts worry about the unknown.
The extrovert will need extra time to talk and will have the patience only for simple and confident explanations from the physician. Consultations may prove helpful to satisfy the extroverts need for more input and interaction with others. Similarly, appropriate support groups will help focus the patient and provide them with needed energy to address their illness and comply with treatments. Plans for that treatment should be provided to the patient in 1-step incre-ments with flexible appointments to facilitate engagement and success that can be easily rewarded by the physician in the moment.
The unstable or neurotic patient will benefit from a few modifications to the above recommendations. This patient should be instructed to act first and feel second. In other words, they should be reminded that they have large quanti-ties of intense emotions that are likely to derail their behav-ior. Their best outcome will occur if they can stick to the plan and then see if that does not help them to feel better. Modeling appropriate behavior rather than empathizing with them coupled with reminders that the worst has not actually occurred and avoiding upsetting theories just to offer reassurance will be most reinforcing for the purpose of decreasing their distress.
CONCLUSiONSTrait differences will manifest differently in pain manage-ment presenting challenges for the practitioner. Treatment will focus on the principles of guidance and remediation for the consequences of the targeted dimension, not the dimen-sion itself. Instruction should be provided to strengthen deficiencies while the life plan should be guided to avoid provocative people, places, and things. Tailoring treatment will be based on the particular vulnerabilities needing to be addressed such extroversion or neuroticism. Initially,
postponing exposure to challenging and conflict laden behaviors will foster maturity and judgment. Then, the goals of treatment shift to moderate the responses to prov-ocations, alter the contexts to minimize recurrence, and increase insight and understanding to promote prevention and sustainable change. Ultimately, the patient will evolve the ability and skill to shape their own responses instead of being a victim of them. The hollow men admonish that we are all individual compositions acting out unique narratives producing precious worlds to be savored and cherished.
References
1. McHugh PR, Slavney PR. Perspectives of Psychiatry. 2nd ed. Baltimore, MD: Johns Hopkins University Press; 1998:332.
2. McHugh PR, Clark MR. Diagnostic and classificatory dilemmas. In: Blumenfield M, Strain JJ, eds. Psychosomatic Medicine in the 21st Century. Baltimore, MD: Lippincott Williams & Wilkins; 2006:39–45.
3. Clark MR. Psychiatry and chronic pain: examining the interface and designing a structure for a patient-centered approach to treatment. Eur J Pain Suppl. 2009;3:95–100.
4. American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013:947.
5. Feist J, Feist GJ. Theories of Personality. New York, NY: McGraw-Hill; 2009:592.
6. Jung CG. The Archetypes and the Collective Unconscious. 2nd ed. Princeton, NJ: University Press; 1958:451.
7. Briggs Myers I, McCaulley MH, Quenk NL, et al. MBTI Step III Manual: Exploring Personality Development Using the Myers-Briggs Type Indicator Instrument. Mountain View, CA: Consulting Psychologists Press; 2009:119.
8. Costa PT Jr, McCrae RR. NEO PI-R Professional Manual. Odessa, FL: Psychological Assessment Resources, Inc.; 1992:101.
9. Eysenck HJ. Dimensions of Personality. London, England: Routledge & Kegan Paul; 1947:308.
10. Adams F. The Genuine Works of Hippocrates (tr. from the Greek). New York, NY: W. Wood & Co; 1886:466.
11. Cain S. Quiet: The Power of Introverts in a World That Can’t Stop Talking. New York, NY: Crown Publishers; 2012:333.
56 | PWJ | www.painweek.org Q3 | 2015
By Jeffrey Fudin PharmD, DAAPM, FCCP, FASHP Thien C. Pham PharmD

www.painweek.org | PWJ | 57Q3 | 2015
OPiOiD ASSOCiATeDMORBiDiTY
AND MORTALiTYHAS CAUSeDA NATiONAL
MOBiLiZATiON OFMeDiA MUCKRAKeRS,
SeNSATiONALiSTS,POLiTiCAL
OPPORTUNiSTS,AND eVeN MeDiCAL
PROFeSSiONALS…
58 | PWJ | www.painweek.org Q3 | 2015
abstract: Opioid associated morbidity and mor-tality has caused a national mobilization of media muckrakers, sensationalists, political opportun-ists, and even medical professionals, all of whom have largely ignored the pharmacotherapeutics that underpin the science for potential opioid casualties.1 This article summarizes validated risk stratification tools, the interpretation of unpre-dicted urine drug screen results by immunoas-say, and miscalculated opioid risks associated with dosing equivalents, drug interactions, and pharmacogenetics. While opioid conversion is not mathematically challenging, caring for real patients as individuals without following a pre-determined one-size-fits-all template or algorithm requires skillful proficiency.
PHARMACOTHERAPY

www.painweek.org | PWJ | 59Q3 | 2015
Despite several commentaries to the contrary,2-4 there are in fact patients who require chronic opioids, such as those pre-cluded from NSAIDs because of GI bleed risk or other complications; kidney dysfunction; diabetes mellitus (Type II) where we frequently see the triple whammy of NSAIDs, diuretics, and ACE inhibitors combined, in addition to several other drug interactions. For some patients serotonin-norepinephrine reuptake inhibitors and anticon-vulsants may be contraindicated or not indicated. Some chronic disorders often associated with chronic pain syndromes that may be nonresponsive to mediations other than opioids include certain forms of severe rheumatoid and osteoarthritis, medullary sponge kidney, arachnoiditis, failed back syndrome, Ehlers-Danlos syn-drome (depending on type), and many more. Anti-opioid zealots would be hard-pressed to deny necessary opioids for such conditions if exposed to these disorders personally.
Before initiating chronic opioid therapy (COT), validated risk stratification tools to assess for opioid abuse or misuse are in order and should be routinely employed.5-7 These stratification tools are questionnaires whereby answers are summed to establish associated patient risk prior to and following COT. Popular options are outlined in a recent Medical Clinics of North America supplement.8
OPiOiD CONVeRSiONSWhile there are several opioid options from which to choose, most guidelines encourage extended release (ER) products when chronic therapy is indicated.5-7 The ER formulations improve compliance, curtail “dose-creeping,” improve restful and consistent sleep, and avoid peaks and troughs associated with higher side effect risk. Popularized recently and encouraged by the FDA are the newer abuse-deterrent formulations: Hysingla® ER (hydrocodone bitar-trate), Embeda® (morphine sulfate/naltrexone hydrochloride), Oxy-Contin® (oxycodone hydrochloride), and Targiniq® ER (oxycodone hydrochloride/naloxone hydrochloride), Zohydro® (hydrocodone bitartrate). Clearly these are not the panacea to averting opioid risk, but they can help to discourage abuse and misuse of these partic-ular products. Nevertheless, substance abusers are quite proficient at moving on to other options such as high dose immediate release oxycodone 30 mg tablets, generic high dose oxymorphone ER, etc.9,10
Opioid rotation should be considered to provide more effective anal-gesia for poorly controlled pain with the inability to increase dose due to side effects, adverse event or toxicity with current opioid, rapid development of tolerance, or development of opioid-induced hyperalgesia (OIH). Of note, there is no definitive existing evidence
DeSPiTe SeVeRALCOMMeNTARieS
TO THe CONTRARY,2-4THeRe ARe
iN FACT PATieNTSWHO ReQUiRe
CHRONiC OPiOiDS…

60 | PWJ | www.painweek.org Q3 | 2015
to support OIH occurring in humans,11 but if we consider OIH to be an issue, a morphine-equivalent daily dose (MEDD) reduction due to interpatient response variability and incomplete cross-toler-ance is required. Here within lies potential for inherent unpredicted dose-associated risks. Consider the various metabolic pathways of assorted opioids, their half-lives, potential for drug interactions, and pharmacogenetics impact. For example, methadone has a very long and variable half-life, and has 6 enzyme-associated metabolic path-ways, each of which comes with potential for polymorphic phenotype variation. Added to that, methadone has 2 enantiomers, R and S.12 Should the S enantiomer accumulate for any reason, it could widen corrected QT (QTc) interval and result in fatal torsades de pointes especially in patients that are poor metabolizer 2B6 phenotypes.12
Adding insult to injury, it is stated in a review of opioid rotation practices by Webster et al that “Recent evidence suggests that the use of dose conversion ratios published in equianalgesic tables may lead to fatal or near-fatal opioid overdoses.”13 In fact, a study comparing 6 popular online opioid conversion calculators showed an astound-ing variation in MEDD from an underdose of 55% to an overdose of almost 250%, the highest disparities being fentanyl transdermal and oral methadone, respectively.14 Lack of MEDD consensus or even the probability that one could exist was further supported by Rennick and colleagues in an American Society of Health-System Pharmacists poster presentation15 that surveyed close to 400 med-ical providers and pharmacists nationwide asking each to provide a MEDD for 5 different opioids (hydrocodone 80 mg; fentanyl TD 75 mcg/hour; methadone 40 mg; oxycodone 120 mg; hydromorphone 48 mg)—and the outcome was disastrous. Considering the huge variability in provider opioid conversion calculations that were con-firmed by Shaw et al, fentanyl was 177 mg MEDD (+/-) 144 mg, and methadone 251 mg MEDD (+/-) 166 mg. In the case of fentanyl TD, the standard deviations (SD) were almost the same as the actual con-version and for methadone the assigned equivalents were similar. In either case, the SD alone are enough to result in death.15 Considering these findings, we cannot attribute methadone deaths only to the complex pharmacokinetics, misuse, and drug interactions. Moreover, it is no wonder that while methadone only accounts for less than 5% of opioid prescriptions, it is nonetheless associated with about one-third of all opioid-related deaths.16
Methadone conversions have traditionally been done using various mathematical schematics developed by Ripamonti,17 Ayonrinde,18 and Mercadante.19 While these provided some dosing guidance, all have significant flaws at their breaking points because each equiva-lency conversion schematic changes at 3 to 6 fixed doses.20 Because of this, a formula was developed by Fudin and colleagues that smooths out the curve for inclusion in opioid online calculators.20 (Go to painweek.org/fudin for figure and table].
OTHeR CONSiDeRATiONSWith all these considerations, even if the stars were aligned, if we could establish a “one conversion for any opioids fit all,” and control for food and drug interactions, body surface area, organ dysfunc-tion, and gender and age, it still doesn’t account for individualized
pharmacogenetics variations. Some of these include allele variants associated phenotypes such as poor, intermediate, extensive, and ultrarapid metabolizers21-23 all of which are particularly important when considering that most opioids require Phase I metabolism through the cytochrome P450 (CYP450) system. Metabolites may include active and/or inactive metabolites. For instance, oxycodone and hydrocodone are metabolized by 3A4 to their inactive forms of noroxycodone and norhydrocodone, respectively, but they are also converted to more potent active metabolites oxymorphone and hydro-morphone, respectively.24-26 Depending therefore on the specific indi-vidual patient phenotype for 2D6 and 3A4, several patients could have various phenotype combinations for each enzyme, metabolize these drugs poorly or rapidly, and the result could be more or less inactive and/or more or less potent metabolites.21,23,27 There are other genetic variations involving for example OPRM1 gene, COMT, and more, but a comprehensive discussion is beyond the scope of this commentary.28
URiNe DRUG TeSTiNGAll recent guidelines for COT suggest that urine drug tests (UDT) be employed as a routine part of any clinic.5-7,29 These are used to justify ongoing treatment by ensuring that patients are taking pre-scribed medications, and not taking prescription medications that are not prescribed and/or illicit substances.30-33
There are 3 elements to doing UDTs correctly starting with 1) chain of custody and 2) selecting the appropriate test. Consider that immu-noassay (IA) is a qualitative test with high potential for false negatives or positives, and that laboratory-based quantitative testing by gas or liquid chromatography mass spectrometry (GC-MS or LC-MS) is close to 100% accurate, and 3) make sure the sample is a “valid” sample by considering adulteration behavior checks and specimen validity testing.32
Adulteration behavior checks are helpful to discern if a patient has demonstrated aberrant behaviors in an effort to hoodwink their provider regarding drug use/misuse or to hide drug metabolites. The specimen can be tested for dilution, substitution, or the use of adulterants. Specimen validity testing is helpful to discern if an unexpected UDT result is from a medical condition such as a urinary infection or from changes in a medical condition, the latter of which necessitates further assessment.
Third party payors prefer UDT by IA because it is far less expensive compared to definitive testing by chromatography. IA does offer point of care (POC) in-office testing that could be advantageous, but the flip side is some providers have been accused of testing too frequently or with inadequate equipment with the intent to use POC testing as a revenue stream.34 This has placed significant strain on an already difficult clinical milieu resulting in third party payors denying or limiting payment for any of these tests.
False negative and positive results by IA present a significant chal-lenge to providers and are a reason to justify the use of definitive testing on a regular basis.35,36 Consider for example that quetiapine could cause a false positive methadone37-40 or that venlafaxine could
PHARMACOTHERAPY

www.painweek.org | PWJ | 61Q3 | 2015
result in a false positive phencyclidine (PCP).41,42 Or, low doses of common synthetic opioids most often are expected to test negative for “opiates” and several benzodiazepines will test negative for that drug class.32 This has caused many patients to be falsely accused of aberrant behavior and has allowed other dishonest patients to hoodwink providers.
Remitigate, LLC, which for purposes of disclosure was founded by one of the authors (JF) of this article, recently developed a compre-hensive software platform that analyzes prescribed medications by chemical class, dose, and drug-drug interactions against IA UDT results and generates a printable explanation of expected vs unex-pected results with guidance for when definitive testing should be considered and is justifiable.43
A CASe STUDYA 51-year-old Caucasian male with a history of heroin abuse is admit-ted to the hospital with endocarditis. His medications on admission included
▸ Oxacillin 2 g, infused over 30 min q4h IV▸ Hydromorphone 2 mg/1 mL q4h PRN IV▸ Nystatin 500,000 units/5 mL PO TID▸ Gentamicin 100 mg, infused over 30 min q8h▸ Warfarin 7.5 mg PO daily▸ Lactobacillus 1 tab PO BID▸ Omeprazole 40 mg PO BID▸ Enoxaparin 80 mg/0.8 mL BID SQ▸ Rifampin 600 mg PO daily
…PATieNTS COULD…MeTABOLiZe
THeSe DRUGSPOORLY OR
RAPiDLY, AND THe ReSULT COULD Be
MORe OR LeSSiNACTiVe AND/OR
LeSS POTeNTMeTABOLiTeS.

62 | PWJ | www.painweek.org Q3 | 2015
During admission he was switched to oral morphine to avoid the undesirable peaks and troughs associated with IV hydromorphone, which for all practical purposes would otherwise simulate inject-able heroin. He ultimately was placed on an oral dose of morphine extended release 75 mg orally (PO) every 8 hours. The expected serum level would be 83 ng/mL but was returned at 19 ng/mL. At first glance it would seem that the patient wasn’t taking his oral mor-phine, which was in fact intently observed. A significant drug inter-action was identified involving p-glycoprotein (pGP), morphine, and rifampin. Although rifampin is well known to induce CYP450 3A4 enzymes, there is no reason to suspect an issue by that mechanism for morphine because morphine does not undergo CYP450 metabolism. But, since rifampin also induces pGP and morphine depends on pGP for oral absorption, it is probable that serum free morphine levels would drop significantly. Imagine the potential disaster that could have occurred had this patient been admitted on oral morphine with rifampin and converted to an equivalent IV morphine dose—the result could have been overdose and death. Or, had the patient been receiving IV morphine in the hospital regularly and converted to a MEDD orally upon discharge, he would likely have significant withdrawal, which may have encouraged a relapse to heroin use.44
CONCLUSiONWe should carefully assess all patients prior to initiating COT and encourage the use of risk stratification tools. Slow escalation of opioid doses upon conversion to morphine equivalents is a key factor—and simple mathematical conversion all at once could be dangerous. We must recognize unique population variables and consider pharma-cogenetic-driven individualized therapy. And, finally, recognize the value of a pharmacist as an important team clinician to mitigate drug risks and encourage ongoing education.
References
1. Atkinson TJ, Schatman ME, Fudin J. The damage done by the war on opioids: the pendulum has swung too far. J Pain Res. 2014;7:265–268.
2. Franklin GM. Opioids for chronic noncancer pain: a position paper of the Ameri-can Academy of Neurology. Neurology. 2014;83(14):1277–1284.
3. Ballantyne JC, Shin NS. Efficacy of opioids for chronic pain: a review of the evidence. Clin J Pain. 2008;24(6):469–478.
4. Gupta S. Gupta: Let’s end the prescription drug death epidemic. 2012. Available at: www.cnn.com/2012/11/14/health/gupta-accidental-overdose/.
5. Manchikanti L, Abdi S, Atluri S, et al. American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: Part 2—guidance. Pain Physician. 2012;15(3 suppl):S67–116.
6. VA/DoD. Clinical practice guidelines for management of opioid therapy for chronic pain. 2010. Available at: www.healthquality.va.gov/guidelines/Pain/cot/COT_312_Full-er.pdf.
7. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113–130.
8. Brooks A, Kominek C, Pharm TC, et al. Exploring the use of chronic opioid ther-apy for chronic pain: when, how and for whom? Med Clin North Am. 2015. [In press]
9. Kirson NY, Shei A, White AG, et al. Societal economic benefits associated with an extended-release opioid with abuse-deterrent technology in the United States. Pain Med. 2014;15(9):1450–1454.
10. Twillman R, Fudin J. Potential cost-shifting and hidden costs and risks in the economic analysis of opioid abuse-deterrent formulations. Pain Med. 2014;15(9):1447–1449.
11. Eisenberg E, Suzan E, Pud D. Opioid-induced hyperalgesia (oih): a real clinical problem or just an experimental phenomenon? J Pain Symptom Manage. 2015;49(3):632–636.
12. Pham TC, Fudin J, Raffa RB. Is levorphanol a better option than methadone? Pain Med. 2015. [In press]
13. Webster LR, Fine PG. Review and critique of opioid rotation practices and associated risks of toxicity. Pain Med. 2012;13(4):562–570.
14. Shaw K, Fudin J. Evaluation and comparison of online equianalgesic opioid dose conversion calculators. Pract Pain Manage. 2013;13(7):61–66.
15. Rennick A, Atkinson T, Cimino N, et al. Variability in opioid equivalence. American Society of Health-System Pharmacists (ASHP) 2013 Midyear Clinical Meeting and Exhibition. Orlando, FL; 2013; Poster 9–236.
16. CDC. Vital signs: risk for overdose from methadone used for pain relief–United States, 1999–2010. MMWR. 2012;61(26):493–497.
17. Ripamonti C, Groff L, Brunelli C, et al. Switching from morphine to oral meth-adone in treating cancer pain: what is the equianalgesic dose ratio? J Clin Oncol. 1998;16(10):3216–3221.
18. Ayonrinde OT, Bridge DT. The rediscovery of methadone for cancer pain man-agement. Med J Aust. 2000;173(10):536–540.
19. Mercadante S, Casuccio A, Fulfaro F, et al. Switching from morphine to metha-done to improve analgesia and tolerability in cancer patients: a prospective study. J Clin Oncol. 2001;19(11):2898–2904.
20. Fudin J. Marcoux MD, Fudin JA . Mathematical model for methadone conversion examined. Pract Pain Manage. September 2012:46–51.
21. Kapur BM, Lala PK, Shaw JL. Pharmacogenetics of chronic pain management. Clin Biochem. 2014;47(13–14):1169–1187.
22. Jannetto PJ, Bratanow NC. Pharmacogenomic considerations in the opioid management of pain. Genome Med. 2010;2(9):66.
23. Janicki PK. Pharmacogenomics of pain management. comprehensive treatment of chronic pain by medical, interventional, and integrative approaches: the American Academy of Pain Medicine. 2013.
24. Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84(7):613–624.
25. Lotsch J. Opioid metabolites. J Pain Symptom Manage. 2005;29(5 suppl):S10–24.
26. Vallejo R, Barkin RL, Wang VC. Pharmacology of opioids in the treatment of chronic pain syndromes. Pain Physician. 2011;14(4):E343–360.
27. Nielsen LM, Olesen AE, Branford R, et al. Association between human pain- related genotypes and variability in opioid analgesia: an updated review. Pain Pract. 8 Sep 2014.
28. Kapur BM, Lala PK, Shaw JL. Pharmacogenetics of chronic pain management. Clin Biochem. 2014;47(13–14):1169–1187.
29. Federation of State Medical Boards (FSMB). Model policy on the use of opioid analgesics in the treatment of chronic pain. 2013. Available at: www.fsmb.org/Media/Default/PDF/FSMB/Advocacy/pain_policy_july2013.pdf.
30. Christo PJ, Manchikanti L, Ruan X, et al. Urine drug testing in chronic pain. Pain Physician. 2011;14(2):123–143.
31. Gourlay D, Heit HA . The art and science of urine drug testing. Clin J Pain. 2010;26(4):358.
32. Hammett-Stabler C WL. A clinical guide to urine drug testing: augmenting pain management and enhancing patient care. University of Medicine and Dentistry of New Jersay–Center for Continuing and Outreach Education. 2008.
PHARMACOTHERAPY

www.painweek.org | PWJ | 63Q3 | 2015
33. Heit HA, Gourlay DL. Urine drug testing in pain medicine. J Pain Symptom Manage. 2004;27(3):260–267.
34. Weaver C, Mathews AW. Doctors cash in on drug tests for seniors, and medicare pays the bill. 2014. Available at: www.wsj.com/articles/doctors-cash-in-on-drug-tests-for-seniors-and-medicare-pays-the-bill-1415676782.
35. Pesce A, West Cameron, Egan-City K, et al. Diagnostic accuracy and inter-pretation of urine drug testing for pain patients: an evidence-based approach, toxicity and drug testing. InTech; 2012. Available at: www.intechopen.com/books/toxicity-and-drug-testing/urine-drug-testing-in-pain-patients.
36. Reisfield GM, Salazar E, Bertholf RL. Rational use and interpretation of urine drug testing in chronic opioid therapy. Ann Clin Lab Sci. 2007;37(4):301–314.
37. Lasic D, Uglesic B, Zuljan-Cvitanovic M, et al. False-positive methadone urine drug screen in a patient treated with quetiapine. Acta Clinica Croatica. 2012;51(2):269–272.
38. Fischer M, Reif A, Polak T, et al. False-positive methadone drug screens during quetiapine treatment. J Clin Psychiatry. 2010;71(12):1696.
39. Cherwinski K, Petti TA, Jekelis A. False methadone-positive urine drug screens in patients treated with quetiapine. J Am Acad Child Adolesc Psychiatry. 2007;46(4):435–436.
40. Widschwendter CG, Zernig G, Hofer A. Quetiapine cross reactivity with urine methadone immunoassays. Am J Psychiatry. 2007;164(1):172.
41. Santos PM, Lopez-Garcia P, Navarro JS, et al. False positive phencyclidine results caused by venlafaxine. Am J Psychiatry. 2007;164(2):349.
42. Sena SF, Kazimi S, Wu AH. False-positive phencyclidine immunoassay results caused by venlafaxine and O-desmethylvenlafaxine. Clin Chem. 2002;48(4):676–677.
43. Fudin J. Demo Video. 2015. Available at: www.remitigate.com/tutorial/.
44. Fudin J, Fontenelle DV, Payne A. Rifampin reduces oral morphine absorption: a case of transdermal buprenorphine selection based on morphine pharmacokinetics. J Pain Palliat Care Pharmacother. 2012;26(4):362–367.
Q3 | 201564 | PWJ | www.painweek.org
By Debra Weiner
June 13–20

Q3 | 2015 www.painweek.org | PWJ | 65
ur maiden voyage on the Celebrity Equinox departed Athens on Saturday, June 13 on its way to Rhodes, Mykonos, Ephesus, Santorini, and Istanbul. Our (my) concerns about encountering a less than elegant environment were dispelled immediately upon arrival. The level of organization for a cruise ship of approximately 2500 passengers and 1200 crew members was staggering. The check-in and luggage drop-off was fairly seamless, and we were very surprised at how comfortable and spacious our cabin turned out to be. A balcony certainly helped, but compact does not necessarily mean claustrophobic, and it was a very charming space to occupy for 7 days.
Aside from the landscape, what made this event so special was the faculty that joined us. Charles Argoff, Michael Clark, and Doug Gourlay provided 12 hours of continuing medical education—enhanced enormously by their familiarity with each other after many years of working together at PAINWeek. We had an international group of 50 clinicians—from Australia, Canada, the Philippine islands, and the United States—who listened intently and asked good questions. An extra treat was the midweek cocktail reception where they and faculty had an opportunity to informally mingle and get to know each other.
POST
SCRI
PT
PHOTOGRAPHY: GREGORY HAZEL/DARRYL FOSSA
66 | PWJ | www.painweek.org Q3 | 2015
I had never been to Athens and was very surprised by how run-down everything looked. As a student of history, I was prepared to be enthralled by this ancient city. Sadly, it lacked the majestic nature of Rome, and while the people were lovely, you could feel an undercurrent of anxiety about the uncertainty of what lies ahead. The best part of our stay there was a fabulous dinner at the fish taverna Yannis, in the Chatzikiriakio neighborhood, southeast of the Piraeus port. We specifically wanted a whole fish, and were directed to the kitchen where we ordered from drawers of freshly caught fagri, lavraki, and sardines that would soon make their way to the grill. Over 4 hours, heaping plates of shrimp, tzatziki, Greek salad, smoked eggplant, wild greens, lemon potatoes and many rounds of tsipouro were consumed by 7 dazzled Americans.

www.painweek.org | PWJ | 67Q3 | 2015
We only saw a small part of the island and opted to spend the day at the beach where we swam in the slightly chilly Mediterranean. It was a bumpy bus
ride from port to sand, narrated by a good natured British ex-pat with teeth that were parallel with the floor.

68 | PWJ | www.painweek.org Q3 | 2015
www.painweek.org | PWJ | 69Q3 | 2015
We arrived in Kusadasi greeted by shimmering turquoise water, a sunny blue sky, and about 300 carpet vendors all of whom claimed to have rare silk carpets with certificates of authenticity. Aside from rugs and being a popular resort for Europeans, Kusadasi is famous for housing Ephesus, one of the best-preserved Roman archeological sites in the Mediterranean. While the walking surface of the ancient city was sloped and slippery, the temples, squares, amphitheaters, and Terrace Houses were spectacular. What is most amazing, is that despite its present magnitude, it is only 18% excavated!
One of the more amusing episodes of the cruise occurred on our stop at Santorini. For those of you who have not had the pleasure of visiting this island, everything begins at the top—literally. When you arrive, you have 3 choices: wait in a very long line for the gondola, hop on a donkey to climb the hillside, or trek uphill alongside the donkeys (not recommended). This particular day was very hot (90+ degrees). When we tendered up to the port I took one look at the 1200 people waiting in line and said, “We’re not getting off. Let’s go back to ship!” My instincts were spot on because later that evening we were regaled by stories of people who chose to climb up and down, retching and exhausted from the pernicious combination of donkey poo, heat, and dehydration.

70 | PWJ | www.painweek.org Q3 | 2015
Another humorous experience was dealing with taxi drivers in Istanbul.
They have a tendency to quote the fare initially in Turkish lira, but when you arrive
at your destination and pay the fare they tell you “No, it’s 20 euros, not 20
lira,” which can be 2 to 3 times as much. Istanbul is a huge and complex city that requires more days than we had to fully experience its richness. One of the best
moments was viewing the city from afar on our cabin balcony at midnight,
watching seagulls sing and swirl around the dome of the Blue Mosque,
illuminated solely by moonlight.
“One of the best moments was viewing the city from afar on our cabin balcony at midnight, watching seagulls sing and swirl around the dome of the Blue Mosque, illuminated solely by moonlight.”
www.painweek.org | PWJ | 71Q3 | 2015
The ship had a diversity of musical entertainment from jazz, folk, pop, and classical musicians. Among these offerings was a Beatles tribute show, which was a lot of fun, especially the audience. There were people standing, screaming, and cheering as if it were Shea Stadium 1964 and the lads were singing their hearts out to She Loves You. Later in the week they did a short set in a lounge sans costume and wigs, but still managed to attract a sizeable crowd. I honestly felt like we would see someone tear themselves away and run up to the band saying “John, please sign this— ‘To Freddie—who knows how to Let It Be.’”
While I don’t think of myself as a cruise person, I would definitely do it again and truly appreciated their attention to detail and generous hospitality. As for the actual CME activity, according to Continuing Education, Inc./University at Sea, the response to our program was impressive for an inaugural activity, and our learners seemed to agree!
“I really liked the speakers. I think the scheduling is great. You get to actually have a good vacation and also get credits. It’s very well organized, and you don’t feel like you’re missing anything and you’re still able to learn at sea.”
—Graciela Gallardo, MD
Debra Weiner is the Director of Program Development for PAINWeek, PAINWeekEnd, and PAINWeek at Sea.
72 | PWJ | www.painweek.org Q3 | 2015
Structuring Pain Care in the Primary Care PracticeChristopher M. Herndon, PharmD, BCPS, CPE
The chronic pain patient may make up 10% to 20% of your patient population, but will typically take up 80% to 90% of your staff and your other resources. There has to be some type of standardized approach so that we monitor to make sure we’re doing things safely and correctly. The primary care provider can do appropriate screening for psychi-atric comorbidities in our chronic pain population. In our practice, before the patient is seen by any of the members of the pain team, they’re asked to fill out a number of different assessment tools or screening tools in order to try to identify some potentially confounding psychiatric diagnosis that we may not have known about previously. That helps with our referral process and whether or not we need assistance from other professionals. Offering pain agreements or signed informed consent will not only keep you out of trouble from a provider standpoint, but it will also enable you as a clinician to provide better patient care.
Migraine Aura: Pathophysiology and Patient ImpactGary W. Jay, MD, FAAPM
Everybody focuses on visual migrainous aura but there’s an extraor-dinary number of auras that are not visual, that are sensory, that are cognitive, things that one would not expect. Another issue is that you can have more than one aura. You can have a visual aura that can last any-where from 5 to 15 to 60 minutes and then have a sensory aura which may last 20 to 30 minutes, and then have a third aura and then get your headache. The first time a patient has a neurological aura, particularly if there’s no history of migraine, that calls for a full neurological eval-uation—MRI, CT scan. The typical headache patient should not need any of these tests. It’s a clinical diagnosis. But if you know that there is a history of migraine, or a family history, that makes it a lot easier to determine that, unless something significant is discovered on exam, it’s not a problem.
Issues in Pain Management for Nurse PractitionersDarren McCoy, FNP-BC, CPE
Our goal, as part of the multidisciplinary team, is to help patients who have pain issues, treat them compassionately and effectively, minimize the burden to the patient and the family, maintain func-tional independence and help prevent damage to the community at large. Nurse practitioners have a variety of prescription privileges available with regard to treating pain. Some of those have to do with the amount of medication prescribed, some with the types of medication prescribed. That changes on a state by state basis, so we have to adjust patient treatment to what we have the ability to do. A nurse practitioner may encounter a number of complexities in treating a pain patient; it could be the magnitude of the dose that they’re taking, say in terms of morphine equivalent, and whether
1 |
2 |
3 |
the nurse practitioner can prescribe that. It could relate to side effects and the need to change medications. It could be the patient’s social situa-tion and the potential for substance abuse from elsewhere in the patient’s household. And it’s important to keep costs in mind and to use best prac-tices to make sure that patients are receiving appropriate care and not wasteful care.
Methadone: A Closer LookMary Lynn McPherson, PharmD, BCPS, CPE, FASPE
The important thing with methadone is safety first. I don’t think every-one is an ideal candidate for methadone therapy. We have to have a patient who’s very reliable, who will follow the plan of care and directions, someone who would not abuse the medication as prescribed by their physician or NP or PA. There are safety standards: we have to worry about the risk for cardiac arrhythmias; or a patient who has hypokalemia or hypomagnesemia; people who have congenital QTc prolongation or unexplained syncope. When you’re switching to methadone from a different opioid, there are published methods for doing conversion calculations. All work but you have to temper them with clinical judgment: is this an appropriate dose with this patient. Then monitor the patient intensively. The savvy practitioner will also be very familiar with the numerous drugs that interact with methadone. There are many drugs that will induce the metabolism of methadone giving you a lower serum concentration. Then there are many, many medications that will inhibit the metabolism of methadone increasing the methadone serum concentration.
Depression and Pain: Relationship, Assessment, and ResponseMark D. Sullivan, MD
There’s evidence that pain impedes treatment of depression. There’s evidence that depression impedes treatment of pain. They are distinct but related problems. The most widely used and useful tool is proba-bly the PHQ-9 Depression Assessment, a self-report assessment that closely parallels the criteria in DSM-IV and DSM-V for major depression. Patients will attribute many of their depressive symptoms directly to pain, which I think is fine, but they still count towards a diagnosis of depression. Sleep impairment, energy impairment, agitation, retarda-tion, guilt, hopelessness, which all can be attributed to pain, still count for depression and indicate that you want to do some independent treatment of depression. Antidepressants benefit people with chronic pain in 3 ways: 1) If they have occurring depression, it helps treat that. 2) There are people who may not quite meet criteria for major depression but have sleep disturbance, and antidepressants are a far superior treatment than benzodiazepines which also amplify opioid risks. 3) There is long and robust literature showing the antidepressants function as analgesics.
4 |
5 |
SHORT CUTS

www.painweek.org | PWJ | 73Q3 | 2015
75%
50%
among the reasons for 242 people
to enroll in a surgical weight loss
procedure study,
reported musculoskeletal
pain and
had poor functional status5
SHORT CUTS
1. http://ow.ly/NJqsv 2. http://ow.ly/NJrc7 3. http://ow.ly/NJqMv 4. http://pain.sh/Q2OoZ 5. http://ow.ly/NJF3d 6. http://ow.ly/NJqkj 7. http://ow.ly/NJpRJ
Of the 7609 participants,
or 63.5% had “bothersome pain” and
or 43.3% had pain that limited their activities. Of the participants without dementia, 54.5% had bothersome pain and 27.2% had pain-
limiting activities4
had dementia. Of those with dementia
670
802
347
4.5Dementia, including Alzheimer’s, afflicts more than
Americans, with the number expected to triple in the next 25 years. Currently, more than 75% of older
adults with dementia live in private homes4
MILLION
269ADULTS
with radicular pain of ≤3 months were randomly
assigned to a tapered course of either prednisone or
placebo, and no difference was recorded in lower extremity pain scores
between the 2 groups6
PEOPLE PER
West Virginia has the highest mortality rate from
overdose deaths—
—than all other states1
29100,000
60PE
RC
EN
T
of the 273 subjects at a medical cannabis clinic
in Michigan,
reported taking prescription pain medication in
conjunction with marijuana within the prior month2
40 PE
RC
EN
T
of patients fail to take biological
medications regularly as prescribed3
65P E R C E N T
of the neonatal abstinence syndrome (NAS) infants had
mothers who used legal opioid pain relievers. Treatment for
infants with NAS costs approx-imately $720 million a year7

74 | PWJ | www.painweek.org Q3 | 2015
with
Michael M.BottrosMD
Michael Bottros, MD, is Assistant Professor of Anesthesiology in the Division of Pain Management at Washington University School of Medicine in St. Louis, Missouri.
SHORT CUTS

www.painweek.org | PWJ | 75Q3 | 2015
What inspired you to become a healthcare provider?
Both my parents are physicians. I remember growing up as a young child with these medical text-books strewn about the floor. I recall so many people, like family friends, asking my parents’ opinions on medical problems. I was enamored by that sense of trust people could have with them and, by extension, physicians in general. People let their guard down when they speak with healthcare providers about their personal problems. I don’t know of many other professions where I have seen that.
Why did you focus on pain management?
It’s so primitive! I mean the understanding of it. We’ve come a long way, but boy do we have a lot further to go. I liken the current state of our understanding of pain mechanisms to what cardiology was like in the 1940s. Pain is such a fundamental part of medicine, but neither do we know much of it, nor are we trained well in medical school to treat it. I was fascinated by how many questions I had during my residency training that actually had no answers… even up until now.
Who were your mentors?
My parents and my grandmother were critical to my personal development. They instilled in me the qualities to strive to be a better person, and I owe everything I am to them. They were and still are
my best friends. Now that I’m married, my wife has embedded in me the qualities I love so much in her. She makes me want to be a better man.
Professionally, I cherish the mentorship that Alex Evers (chairman of the department of anesthesiology at Washington University School of Medicine) has provided me over the last several decades (yes, decades). The man is a visionary and is widely regarded as one of the best department chairmen in the country, creating an academic powerhouse. I am honored in being able to call him a friend. I also strive to be half the clinician that Robert Swarm is. He’s the clinical division chief of pain management at Washington University School of Medicine. That man is a saint. I have never seen a more caring physician who puts his patients first before anything else. I also owe a lot to the entire faculty that I trained with at Johns Hopkins: Srinivasa Raja, Paul Christo, Steven Cohen, Michael Erdek, and Kayode Williams were each amazing individuals in their own right. I still keep in touch with them.
If you weren’t a healthcare provider, what would you be?
I’ve always wanted to answer that question like George Costanza and say “Architect.” But really I probably would have gone into either being a Classics professor (based on my love of ancient languages) or a watchmaker (have you seen how beautiful, meticulously detailed, and ridiculously intricate some of those high-end watches can be?).
“Pain is such a fundamental part of medicine, but neither do we
know much of it, nor are we trained well in medical school to treat it.”

76 | PWJ | www.painweek.org Q3 | 2015
“My wife says I could sell ice to an Eskimo.”
What is your most marked characteristic?
I’m influential. My wife says I could sell ice to an Eskimo. I’ve been told by residents (and attendings) that people in the department of anesthesia talk of a “Bottros effect.” I think it’s the greatest asset that has helped me found the acute pain service, garnering the trust of surgeons, and changing the culture towards “pain management” here. The year I founded that service, almost half of the senior residency class decided on pursuing a pain fellowship, and they awarded me “Teacher of the Year.”
What do you consider your greatest achievement?
Being married for almost 5 years to the love of my life—and soon becoming a father!
What is your favorite language?
Koine Greek. It was the language spoken in much of the Mediterranean following the conquests of Alexander the Great during the Hellenistic period. The antiquity of that language and the sheer volume of work whose translations into English lose much of the subtle nuances make it a favorite for geeky Classics majors like me.
If you had to choose one book, one film, and one piece of music to take into space for an undetermined amount of time, what would they be?
Book: The Bible. It would bring me much solace if I really did find myself in space for an undetermined amount of time.
Film: It’s a toss-up between The Godfather: Part II and The Dark Knight. I know, I know…very different movies. The Godfather’s a classic, through and through; but there’s something about Heath Ledger’s performance that I can’t take my eyes off.
Music: There are very few bands whose albums I could enjoy the whole way through; however, anything by Vampire Weekend or Radiohead would work.
What would you like your legacy to be?
That I left the world a slightly better place. Whether it’s through lending an ear to a patient in a time of need, or that I may have been part of the reason why a student or trainee wins the Nobel Prize.
What is your motto?
While it may be cliché to quote Steve Jobs, people who know me know I try to live by this: “We don’t get a chance to do that many things, and every one should be really excellent. Because this is our life.”
PUNDIT PROFILE/MICHAEL BOTTROS

GRALISE® (gabapentin) tablets
BRIEF SUMMARY: For full prescribing information, see package insert.
INDICATIONS AND USAGEGRALISE is indicated for the management of Postherpetic Neuralgia (PHN). GRALISE is not interchangeable with other gabapentin products because of differing pharmacokinetic profiles that affect the frequency of administration.
DOSAGE AND ADMINISTRATIONPostherpetic neuralgia• GRALISE should be titrated to an 1800 mg dose taken orally once daily with the evening meal. GRALISE tablets should be
swallowed whole. Do not split, crush, or chew the tablets.• If GRALISE dose is reduced, discontinued, or substituted with an alternative medication, this should be done gradually
over a minimum of one week or longer (at the discretion of the prescriber).• Renal impairment: Dose should be adjusted in patients with reduced renal function. GRALISE should not be used
in patients with CrCl less than 30 or in patients on hemodialysis.• In adults with postherpetic neuralgia, GRALISE therapy should be initiated and titrated as follows:
Table 1 GRALISE Recommended Titration Schedule
Day 1 Day 2 Days 3-6 Days 7-10 Days 11-14 Day 15
Daily dose 300 mg 600 mg 900 mg 1200 mg 1500 mg 1800 mg
CONTRAINDICATIONSGRALISE is contraindicated in patients with demonstrated hypersensitivity to the drug or its ingredients.
Table 2 GRALISE Dosage Based on Renal Function
Once-daily dosing
Creatinine clearance (mL/min) GRALISE dose (once daily with evening meal) ≥ 60 1800 mg 30-60 600 mg to 1800 mg < 30 GRALISE should not be administered Patients receiving hemodialysis GRALISE should not be administered
WARNINGS AND PRECAUTIONSGRALISE is not interchangeable with other gabapentin products because of differing pharmacokinetic profiles that affect the frequency of administration. The safety and effectiveness of GRALISE in patients with epilepsy has not been studied. Suicidal Behavior and Ideation Antiepileptic drugs (AEDs), including gabapentin, the active ingredient in GRALISE, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Table 3 Risk by Indication for Antiepileptic Drugs (including gabapentin, the active ingredient in Gralise) in the Pooled Analysis
Indication Epilepsy Psychiatric Other Total
Placebo patients with events per 1000 patients 1.0 5.7 1.0 2.4Drug patients with events per 1000 patients 3.4 8.5 1.8 4.3Relative risk: incidence of events in drug patients/incidence in placebo patients 3.5 1.5 1.9 1.8Risk difference: additional drug patients with events per 1000 patients 2.4 2.9 0.9 1.9
The relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications. Anyone considering prescribing GRALISE must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which products containing active components that are AEDs (such as gabapentin, the active component in GRALISE) are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated. Patients, their caregivers, and families should be informed that GRALISE contains gabapentin which is also used to treat epilepsy and that AEDs increase the risk of suicidal thoughts and behavior and should be advised of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Behaviors of concern should be reported immediately to healthcare providers. Withdrawal of Gabapentin Gabapentin should be withdrawn gradually. If GRALISE is discontinued, this should be done gradually over a minimum of 1 week or longer (at the discretion of the prescriber). Tumorigenic Potential In standard preclinical in vivo lifetime carcinogenicity studies, an unexpectedly high incidence of pancreatic acinar adenocarcinomas was identified in male, but not female, rats. The clinical significance of this finding is unknown. In clinical trials of gabapentin therapy in epilepsy comprising 2,085 patient-years of exposure in patients over 12 years of age, new tumors were reported in 10 patients, and preexisting tumors worsened in 11 patients, during or within 2 years after discontinuing the drug. However, no similar patient population untreated with gabapentin was available to provide background tumor incidence and recurrence information for comparison. Therefore, the effect of gabapentin therapy on the incidence of new tumors in humans or on the worsening or recurrence of previously diagnosed tumors is unknown. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)/Multiorgan Hypersensitivity Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), also known as Multiorgan Hypersensitivity, has been reported in patients taking antiepileptic drugs, including GRALISE. Some of these events have been fatal or life-threatening. DRESS typically, although not exclusively, presents with fever, rash, and/or lymphadenopathy in association with other organ system involvement, such as hepatitis, nephritis, hematological abnormalities, myocarditis, or myositis, sometimes resembling an acute viral infection. Eosinophilia is often present. Because this disorder is variable in its expression, other organ systems not noted here may be involved. It is important to note that early manifestations of hypersensitivity, such as fever or lymphadenopathy, may be present even though rash is not evident. If such signs or symptoms are present, the patient should be evaluated immediately. GRALISE should be discontinued if an alternative etiology for the signs or symptoms cannot be established. Laboratory Tests Clinical trial data do not indicate that routine monitoring of clinical laboratory procedures is necessary for the safe use of GRALISE. The value of monitoring gabapentin blood concentrations has not been established.
ADVERSE REACTIONSClinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. A total of 359 patients with neuropathic pain associated with postherpetic neuralgia have received GRALISE at doses up to 1800 mg daily during placebo-controlled clinical studies. In clinical trials in patients with postherpetic neuralgia, 9.7% of the 359 patients treated with GRALISE and 6.9% of 364 patients treated with placebo discontinued prematurely due to adverse reactions. In the GRALISE treatment group, the most common reason for discontinuation due to adverse reactions was dizziness. Of GRALISE-treated patients who experienced adverse reactions in clinical studies, the majority of those adverse reactions were either “mild” or “moderate”. Table 4 lists all adverse reactions, regardless of causality, occurring in at least 1% of patients with neuropathic pain associated with postherpetic neuralgia in the GRALISE group for which the incidence was greater than in the placebo group.
Table 4 Treatment-Emergent Adverse Reaction Incidence in Controlled Trials in Neuropathic Pain Associated with Postherpetic Neuralgia (Events in at Least 1% of all GRALISE-Treated Patients and More Frequent Than in the Placebo Group)
Body system—preferred term GRALISE N = 359, % Placebo N = 364, %
Ear and Labyrinth Disorders Vertigo 1.4 0.5 Gastrointestinal Disorders Diarrhea 3.3 2.7 Dry mouth 2.8 1.4 Constipation 1.4 0.3 Dyspepsia 1.4 0.8 General Disorders Peripheral edema 3.9 0.3 Pain 1.1 0.5
Infections and Infestations Nasopharyngitis 2.5 2.2 Urinary tract infection 1.7 0.5 Investigations Weight increased 1.9 0.5 Musculoskeletal and Connective Tissue Disorders Pain in extremity 1.9 0.5 Back pain 1.7 1.1 Nervous System Disorders Dizziness 10.9 2.2 Somnolence 4.5 2.7 Headache 4.2 4.1 Lethargy 1.1 0.3
In addition to the adverse reactions reported in Table 4 above, the following adverse reactions with an uncertain relationship to GRALISE were reported during the clinical development for the treatment of postherpetic neuralgia. Events in more than 1% of patients but equally or more frequently in the GRALISE-treated patients than in the placebo group included blood pressure increase, confusional state, gastroenteritis viral, herpes zoster, hypertension, joint swelling, memory impairment, nausea, pneumonia, pyrexia, rash, seasonal allergy, and upper respiratory infection. Postmarketing and Other Experience with other Formulations of Gabapentin In addition to the adverse experiences reported during clinical testing of gabapentin, the following adverse experiences have been reported in patients receiving other formulations of marketed gabapentin. These adverse experiences have not been listed above and data are insufficient to support an estimate of their incidence or to establish causation. The listing is alphabetized: angioedema, blood glucose fluctuation, breast hypertrophy, erythema multiforme, elevated liver function tests, fever, hyponatremia, jaundice, movement disorder, Stevens-Johnson syndrome. Adverse events following the abrupt discontinuation of gabapentin immediate release have also been reported. The most frequently reported events were anxiety, insomnia, nausea, pain and sweating.
DRUG INTERACTIONSCoadministration of gabapentin immediate release (125 mg and 500 mg) and hydrocodone (10 mg) reduced hydrocodone Cmax
by 3% and 21%, respectively, and AUC by 4% and 22%, respectively. The mechanism of this interaction is unknown. Gabapentin AUC values were increased by 14%; the magnitude of this interaction at other doses is not known. When a single dose (60 mg) of controlled-release morphine capsule was administered 2 hours prior to a single dose (600 mg) of gabapentin immediate release in 12 volunteers, mean gabapentin AUC values increased by 44% compared to gabapentin immediate release administered without morphine. The pharmacokinetics of morphine were not affected by administration of gabapentin immediate release 2 hours after morphine. The magnitude of this interaction at other doses is not known. An antacid containing aluminum hydroxide and magnesium hydroxide reduced the bioavailability of gabapentin immediate release by about approximately 20%, but by only 5% when gabapentin was taken 2 hours after antacids. It is recommended that GRALISE be taken at least 2 hours following antacid administration. There are no pharmacokinetic interactions between gabapentin and the following antiepileptic drugs: phenytoin, carbamazepine, valproic acid, phenobarbital, and naproxen. Cimetidine 300 mg decreased the apparent oral clearance of gabapentin by 14% and creatinine clearance by 10%. The effect of gabapentin immediate release on cimetidine was not evaluated. This decrease is not expected to be clinically significant. Gabapentin immediate release (400 mg three times daily) had no effect on the pharmacokinetics of norethindrone (2.5 mg) or ethinyl estradiol (50 mcg) administered as a single tablet, except that the Cmax
of norethindrone was increased by 13%. This interaction is not considered to be clinically significant. Gabapentin immediate release pharmacokinetic parameters were comparable with and without probenecid, indicating that gabapentin does not undergo renal tubular secretion by the pathway that is blocked by probenecid.
USE IN SPECIFIC POPULATIONSPregnancy Pregnancy Category C: Gabapentin has been shown to be fetotoxic in rodents, causing delayed ossification of several bones in the skull, vertebrae, forelimbs, and hindlimbs. There are no adequate and well-controlled studies in pregnant women. This drug should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. To provide information regarding the effects of in utero exposure to GRALISE, physicians are advised to recommend that pregnant patients taking GRALISE enroll in the North American Antiepileptic Drug (NAAED) Pregnancy Registry. This can be done by calling the toll free number 1-888-233-2334, and must be done by patients themselves. Information on the registry can also be found at the website http://www.aedpregnancyregistry.org/. Nursing Mothers Gabapentin is secreted into human milk following oral administration. A nursed infant could be exposed to a maximum dose of approximately 1 mg/kg/day of gabapentin. Because the effect on the nursing infant is unknown, GRALISE should be used in women who are nursing only if the benefits clearly outweigh the risks. Pediatric Use The safety and effectiveness of GRALISE in the management of postherpetic neuralgia in patients less than 18 years of age has not been studied. Geriatric Use The total number of patients treated with GRALISE in controlled clinical trials in patients with postherpetic neuralgia was 359, of which 63% were 65 years of age or older. The types and incidence of adverse events were similar across age groups except for peripheral edema, which tended to increase in incidence with age. GRALISE is known to be substantially excreted by the kidney. Reductions in GRALISE dose should be made in patients with age-related compromised renal function. [see Dosage and Administration]. Hepatic Impairment Because gabapentin is not metabolized, studies have not been conducted in patients with hepatic impairment. Renal Impairment GRALISE is known to be substantially excreted by the kidney. Dosage adjustment is necessary in patients with impaired renal function. GRALISE should not be administered in patients with CrCL between 15 and 30 or in patients undergoing hemodialysis [see Dosage and Administration].
DRUG ABUSE AND DEPENDENCEThe abuse and dependence potential of GRALISE has not been evaluated in human studies.
OVERDOSAGEA lethal dose of gabapentin was not identified in mice and rats receiving single oral doses as high as 8000 mg/kg. Signs of acute toxicity in animals included ataxia, labored breathing, ptosis, sedation, hypoactivity, or excitation. Acute oral overdoses of gabapentin immediate release in humans up to 49 grams have been reported. In these cases, double vision, slurred speech, drowsiness, lethargy and diarrhea were observed. All patients recovered with supportive care. Gabapentin can be removed by hemodialysis. Although hemodialysis has not been performed in the few overdose cases reported, it may be indicated by the patient’s clinical state or in patients with significant renal impairment.
CLINICAL PHARMACOLOGYPharmacokinetics Absorption and Bioavailability Gabapentin is absorbed from the proximal small bowel by a saturable L-amino transport system. Gabapentin bioavailability is not dose proportional; as the dose is increased, bioavailability decreases. When GRALISE (1800 mg once daily) and gabapentin immediate release (600 mg three times a day) were administered with high fat meals (50% of calories from fat), GRALISE has a higher Cmax
and lower AUC at steady state compared to gabapentin immediate release. Time to reach maximum plasma concentration (T
max) for GRALISE is 8 hours, which is about 4-6 hours longer compared to gabapentin immediate release.
NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of Fertility Gabapentin was given in the diet to mice at 200, 600, and 2000 mg/kg/day and to rats at 250, 1000, and 2000 mg/kg/day for 2 years. A statistically significant increase in the incidence of pancreatic acinar cell adenoma and carcinomas was found in male rats receiving the high dose; the no-effect dose for the occurrence of carcinomas was 1000 mg/kg/day. Peak plasma concentrations of gabapentin in rats receiving the high dose of 2000 mg/kg/day were more than 10 times higher than plasma concentrations in humans receiving 1800 mg per day and in rats receiving 1000 mg/kg/day peak plasma concentrations were more than 6.5 times higher than in humans receiving 1800 mg/day. The pancreatic acinar cell carcinomas did not affect survival, did not metastasize and were not locally invasive. The relevance of this finding to carcinogenic risk in humans is unclear. Studies designed to investigate the mechanism of gabapentin-induced pancreatic carcinogenesis in rats indicate that gabapentin stimulates DNA synthesis in rat pancreatic acinar cells in vitro and, thus, may be acting as a tumor promoter by enhancing mitogenic activity. It is not known whether gabapentin has the ability to increase cell proliferation in other cell types or in other species, including humans. Gabapentin did not demonstrate mutagenic or genotoxic potential in 3 in vitro and 4 in vivo assays. No adverse effects on fertility or reproduction were observed in rats at doses up to 2000 mg/kg (approximately 11 times the maximum recommended human dose on an mg/m2 basis).
© December 2012, Depomed, Inc. All rights reserved. GRA-410-P.1
PainWeekJournal_V2.indd 2 6/3/15 2:17 PM

Indication and Usage GRALISE is indicated for the management of postherpetic neuralgia (PHN). GRALISE is not interchangeable with other gabapentin products because of differing pharmacokinetic profiles that affect the frequency of administration.
Important Safety Information Antiepileptic drugs, including gabapentin, the active ingredient of GRALISE, increase the risk of suicidal thoughts or behavior. Increased seizure frequency may occur in patients with seizure disorders if GRALISE is rapidly discontinued. Withdraw GRALISE gradually over a minimum of 1 week. The most common adverse reaction to GRALISE (≥5% and twice placebo) is dizziness.
Please see adjacent page for Brief Summary of Prescribing Information. Full Prescribing Information and Medication Guide are available at GRALISE.com.
FOR NIGHT & DAY
References: 1. Argoff CE, Chen C, Cowles VE. Clinical development of a once-daily gastroretentive formulation of gabapentin for treatment of postherpetic neuralgia: an overview. Expert Opin Drug Deliv. 2012;9:1147-1160. 2. Data on file, 2013. Depomed Inc. 3. Gupta A, Li S. Safety and efficacy of once-daily gastroretentive gabapentin in patients with postherpetic neuralgia aged 75 years and over. Drugs Aging. 2013;30:999-1008. 4. GRALISE [prescribing information]. Newark, CA: Depomed Inc.; December 2012.
© April 2015, Depomed Inc. All rights reserved. APL-GRA-0173
GRALISE THE NIGHT RELEASE THE DAY
When your PHN patients face challenges by Night and DayGRALISE is indicated for the management of postherpetic neuralgia (PHN).
&
• Side effects that are transient1
• Dizziness (10.9%) and somnolence (4.5%) were the most common side effects, and declined during the 2-week titration period to reach sustained low levels thereafter
• In clinical trials, 9.7% of GRALISE patients discontinued prematurely due to adverse reactions versus 6.9% for placebo4
• Dosage adjustment of GRALISE is necessary in patients with impaired renal function. GRALISE should not be administered in patients with creatinine clearance <30 mL/min or in patients undergoing hemodialysis. Reductions in GRALISE dose should be made in patients with age-related compromised renal function.
Once-daily GRALISE delivers 24-hour pain control, Night and Day1
Elderly patients experienced consistent results by Night and Day - even those over 753
• At night, when pain is at its worst1
• GRALISE is taken with the evening meal
NIGHTTIME DAYTIME EVENINGMEAL
TAKE WITH
PainWeekJournal_V2.indd 1 6/3/15 2:17 PM