Pain pharma
51
PHARMACOLOGICAL ASPECTS OF PAIN MANAGEMENT DR.SOURAV CHAKRABARTY, (1 ST YR PGT),DEPT OF PHARMACOLOGY, B.S.MEDICAL COLLEGE
-
Upload
souravpharma -
Category
Health & Medicine
-
view
378 -
download
1
description
A presentation of pharmacological management of pain
Transcript of Pain pharma

PHARMACOLOGICAL ASPECTS OF PAIN MANAGEMENT
DR.SOURAV CHAKRABARTY,(1ST YR PGT),DEPT OF PHARMACOLOGY,
B.S.MEDICAL COLLEGE

“But pain is a perfect misery
The worst of evils
Excessive overturns
All patience”
John Milton
In Paradise Lost

What is Pain?
• Medical Definition
“Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”
• Operative Definition
“Pain is whatever the experiencing person says it is, existing whenever he/she says it does.”

.
• Basically a protective mechanism.
• It guides physician to the actual tissue damaging process.
• Pain management should be rapid & effective, simultaneously associated with treatment of the condition that leads to pain.
• So our motto is NOT TO KILL THE PAIN BUT TO HEAL THE PAIN…………..

Types of Pain‘Nociceptive’• Normal physiology • Beneficial• Treated with conventional analgesics (NSAID,
acetaminophen, opioids)• If Unrelieved, it becomes deleterious
‘Neuropathic’• Aberrant physiology• Poor quality of life• Difficult to treat

Normal Pain Pathways
Tissue injury
• Histamine
• Bradykinin
•Prostaglandin.
Primary
Afferent
Lateral spino-
thalamic tract

PAG(periaqueductal gray)
Raphe Nuclei
locus ceruleus
Enkephalin-containinginterneuron
Normal Pain Pathways

Opioids
(m, d, k)
Local anaesthatics
(voltage gated Na+ channels)
NSAIDs

Analgesic at different levelSites of Action Medications
Peripherally (at the nociceptor)
Cannabinoids, NSAIDs, Opioids, Tramadol, Vanilloid
receptor antagonists(i.e., capsaicin)
Peripherally(along the nociceptive nerve)
Local anesthetics, Anticonvulsants (except the
gabapentinoids)
Centrally (various parts of the brain)
Acetaminophen Anticonvulsants (except the
gabapentinoids), Cannabinoids. Opioids, Tramadol
Descending Inhibitory
pathway in the spinal cord
Cannabinoids, Opioids, Tramadol, Tricyclic
antidepressants, SNRIs
Dorsal horn of the spinal
cord
Anticonvulsants, Cannabinoids, Gabapentinoids, NMDA
receptor antagonists, Opioids,. Tramadol, Tricyclic
antidepressants, SNRIs

Classification of drugs
(Opiates):
Agonist:oMorphine agonist:
oMorphine
oHydromorphone
oOxymorphone
o Levorphanol
oCodeine
oHydrocodone
oOxycodone
oMeperidine agonists:oMeperidineoFentanyl.
o Methadone agonists:oMethadoneoPropoxyphene.

oMixed agonist-antagonisto Pentazocine
o Butorphanol
o Nalbuphine
o Buprenorphine
o Dezocine
o Antagonists:
o Naloxone
o Central analgesics:
o Tramadol
o Tapendalol

Non-opiates
NSAIDSA- nonselective COX inhibitors (conventional nsaids)
• Salicylates: aspirin, diflunisal.
• Pyrazolone derivatives: phenylbutazone,oxyphenbutazone.
• Indole derivatives: indomethacin, sulindac.
• Propionic acid derivatives: ibuprofen, naproxen, ketoprofen, flurbiprofen.
• Anthranilic acid derivative: mephenamic acid.
• Aryl-acetic acid derivatives: diclofenac.
• Oxicam derivatives: piroxicarn, tenoxicam.
• Pyrrole-pyrrole derivative: ketorolac.

B- Preferential COX-2 inhibitors
Nimesulide, Meloxicam, Nabumetone
C- Selective COX-2 inhibitors
Celecoxib, Rofecoxib, Valdecoxib
D- Analgesic- antipyretics with poor antiinflammatory action
Paraaminophenol derivative: Paracetamol(Acetaminophen).
Pyrazolone derivatives: Metamizol (Dipyrone), Propiphenazone.
Benzoxazocine derivative: Nefopam.

• Anticonvulsants
–Gabapentin
–Pregabalin
–Phenytoin
–Carbamazapine
–Oxcarbamazapine
–Clonazepam
• Antidepressants
–Doxepine
–Amitriptyline
–Imipramine
–Nortriptyline
–Desipramine
–Venlafaxine
–Duloxetine

• Local anaesthetics:
o Esters:
o Procaine
o Chlorprocaine
o Tetracaine
o Amides:
o Bupivacaine.
o Mepivacaine.
o Ropivacaine
o Prilocaine
o Etidocaine
• Muscle relaxant
o Smooth muscle relaxants
o Hyoscine butylbromide
o Dicylomine
o Oxybutrinine
o Darifenacine
o Solifenacine
o Flavoxate
o Skeletal muscle relaxants
o Baclofen
o Thiocolchicoside
o Chlorzoxazone
o Diazepam
o Mephenesine

Opioids
• "Among the remedies which it has pleased Almighty God to give to man to relieve his sufferings, none is so universal and so efficacious as opium.“
• Sydenham, 1680

.The term opioid refers broadly to allcompounds related to opium. The wordopium is derived from opos, the Greekword for "juice," the drug being derivedfrom the juice of the opium poppy,Papaver somniferum.

Endogenous Opoid Peptides
OPIOID
RECEPTOR
CLASS
EFFECTSASSOCIATED ENDOGENOUS
ENDORPHIN
Mu 1
Euphoria, supraspinal analgesia,
confusion, dizziness, nausea, low
addiction potential
Endormorphin 1,2=Beta-endorphin
>Enkephalin=Dynorphin
Mu 2Respiratory depression, CVS and GI
effects, miosis, urinary retention
Beta-endorphin=Endormorphin
1,2>Enkephalin=Dynorphin
Delta
Spinal analgesia,Opioid renforcement
CVS depression, decreased brain and
myocardial oxygen Demand
Enkephalin=Beta-endorphin>Dynorphin
Kappa
Supraspinal,Spinal ,Peripheral
analgesia, dysphoria, psychomimetic
effects, feedback inhibition of
endorphin system
Dynorphin A=beta-
endorphin>Enkephalin


Spinal sites of opioid action.
reduce transmitter releasefrom presynaptic terminals of nociceptive
primary afferents
hyperpolarizesecond-order pain transmission neurons by increasing
K+ conductance, evoking an inhibitorypostsynaptic potential

Analgesic features of morphine
Efficacy:• Morphine is a strong analgesic.
• Higher doses can mitigate even severe pain
• Degree of analgesia increasing with dose.
• Simultaneous action at spinal and supraspinal sites greatly amplifies
the analgesic action.
Selectivity:
• Suppression of pain perception is selective
• No affect on other sensations
• proportionate generalized CNS depression (contrast general anaesthetics).

• Type of pain:
• Dull, visceral pain > sharply defined somatic pain.
• Nociceptive pain>neuritic pain.
• Mood & subjective effects:• Mood changes, euphoria, tranquility, mental clouding,
drowsiness, indifference to surroundings as well as to our body.
• Morphine has a calming effect.

OTHER CNS EFFECTS
• Effects on the Hypothalamus:Body temperature usually falls slightly.
.Neuroendocrine Effects.
• GnRH,CRH, LH,FSH,ACTH,Testosteron,Cortisol.
• Prolactin.
• Miosis
• Convulsion

EFFECTS ON OTHER SYSTEMS
• Respiratory depression. ( Responsiveness of the brainstem respiratory centers to carbon dioxide)
• Cough.
• Nausea
• Peripheral vasodilatation, reduced peripheral resistance, and an inhibition of baroreceptor reflexes.
• Gastric motility.
• Biliary, pancreatic, and intestinal secretions and delays digestion of food in the small intestine.
• Constipation.
• Immunosupression.
• Bronchoconstriction
• Uterus may be relaxed
• Mild hyperglycemia due to central sympathetic stimulation .
• Weak anticholinesterase action

Tolerance
Onset• Develops rapidly and can be detected within 12 – 14 hours of
morphine administration .• within 3 days the equianalgesic dose is increased 5 fold • Mainly developes to depressant effects NOT to stimulant effects.
• Two proposed mechanisms– upregulation of cAMP system– Downregulation of μ receptors
• uncoupling between μ receptor and G proteins
Reversal of second messenger (cAMP) and ion channel system• Blocked by NMDA antagonists and nitric oxide synthase inhibitors.

Degrees of Tolerance
High Moderate Minimal or None
Analgesia Bradycardia Miosis
Euphoria, dysphoria Constipation
Mental clouding Convulsions
Sedation
Respiratory depression
Antidiuresis
Nausea and vomiting
Cough suppression

Dependence Two components
• Physical dependence: Withdrawal symptoms
– sweating ,lacrimation, dehydration ,
– Fear, anxiety , restlessness
–Mydriasis , tremor , colic
– Hypertension , tachycardia, weight loss.Methadone is used to relieve withdrawal syndrome.
• Psychological dependence:– Associated with craving, lasting for months or years.
– Opioids facilitate DA transmission in mesolimbic/mesocortical pathways and activate endogenous reward pathways in brain.

Pharmacokinetics
• Modestly absorbed from the GI tract
t1/2 of morphine is ~2 hours.
• Metabolised as Morphine-6-glucuronide
• Excreted by the kidney
• Satisfactory analgesia in cancer patients is associated with a very
broad range of steady-state concentrations of morphine in plasma
(16-364 ng).
POTENTANALGESIC

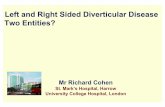
Routes of administration
IV
Pla
sm
a C
oncentr
ation
po / pr
SC/IM
0Half life time

Dosing formulation
Liposome-encapsulated extended release morphine
• –Single epidural injection lasting 48h
• –S/E –vomiting, pruritus, O2 desaturation
Intranasal opioid aerosols
• –Fentanyl, Morphine
• –Breath activated nebuliser
• –Rapid onset, deep-lung dosing
• –Variable bioavailability
DepoFoam™Particle(diameter: 15 microns)
The non-concentric vesicles are surrounded by
a lipid membrane, and each contains an internal
aqueous chamber with morphine sulfate solution

Oxycodone
• Semi-synthetic derivative synthesized from Thebaine
• κ-opioid agonist
• After a dose of conventional oral oxycodone, peak plasma levels of
the drug are attained in about one hour
• Oxycodone is metabolized to α and β oxycodone The oral
bioavailability is 60% to 87%
• t ½ -4.5 hours
• mainly excreted in the urine and sweat
• Dependence, addiction and withdrawal.
• Oral/iv 10 mg, 15 mg, 20 mg, 30 mg, 40 mg, 60 mg, and 80 mg
• Controlled release

Fentanyl and Congeners• Synthetic opioid related to the phenylpiperidines• Extremely potent analgesics• Very short duration of action
• Pharmacological action• Rigidity • Respiratory depression : onset is more rapid. . • Neuroexcitation• Do not release histamine .• Direct depressant effects on the myocardium are minimal.
• Pharmacokinetics
• Highly lipid soluble and rapidly cross the blood-brain barrier.
• t1/2, 3-4 hours. Fentanyl and sufentanil
• Hepatic metabolism and renal excretion.
• Higher doses/ prolonged infusions- these clearance mechanisms become progressively saturated.
Sufentanil
Remifentanil
Alfentanil

Fentanyl and Congeners(contd)
• Ramifentanyl• t1/2 of 8-20 minutes
• metabolized by plasma esterases
• Elimination is independent of hepatic metabolism or renal excretion
• Remifentanil acid, has 0.05-0.025% of the potency of the parent compound, and is excreted renally.
• Short, painful procedures that require intense analgesia and blunting of
stress responses
• Continuous IV infusion
• Short duration of action makes bolus administration impractical
• Not used intraspinally
• Therapeutic Uses
• 1. Postoperative pain management,• 2.Labor analgesia• 3.Chronic pain treatment

Iontophoresis transdermal system
Electrotransport delivery platform technology (E-TRANS/IONSYS)
• Hydrogel reservoir into the skin
• Low-intensity direct current
• Bolus dose 40 ug
• Dose interval 10 min
• Upto 24 hours or a maximum of 80 doses
• Audible beep & LED light indicator
Transdermal patches - sustained release of
fentanyl for 48-72hrs
Trans buccal absorption by the use of buccal
tablets, soluble buccal film, and lollypop-like
lozenges permits rapid absorption,

Meperidine• Synthetic opioid.
• Biotransformed by liver to
Normeperidine, it is potentially
neurotoxic metabolite.
• Half life is 3 hr.
• Accumulation of normeperidine
can precipitate tremulousness,
myoclonus & Seizures.
• C/I in patients receiving MAO
inhibitors.
Methadone Synthetic opioid.
Long acting MOR.Broadspectrum opioid µ receptor agonist.
NMDA antagonist.
Inhibitors of Monoamine transmitter reuptake.
Exactly identical pharmacodynamics as that of Morphine in equi-analgesic doses.
Opioid rotation is done to restore analgesic sensitivity in highly tolerant patient.

Pentazocine-κ1 agonist
-Produces Spinal level analgesia
• Less sedation,drowsiness &respiratory depression. Due to σ
stimulation it causes
– Dysphoria, hallucinations, diaphoresis & psychotomimetic effects
– Increases BP/ HR/ pulmonary artery pressure
• Indicated in post operative pain, moderately severe pain in burns,
trauma, fractures etc
• Tablets available in fixed-dose combinations with acetaminophen or
naloxone combination
weak antagonist or partial agonist
at opioidreceptors.

Tramadol
Synthetic codeine analog. Weak MOR agonist
1. Produces antinociception via predominantly, a mu-opioid receptor
mechanism.
2. No respiratory depression, sedation, or constipation, as observed with other
opiates.
3. No analgesic tolerance
4. No psychological dependence or euphoric effects in long-term clinical trials
1. Novel mechanism of analgesic action is partially due to
its adrenergic action
2. Enhanced secretion of serotonin and inhibits the
reuptake of serotonin in the CNS
OPIOD ACTIVITY
Monoaminergic
Activity

Pharmacokinetics
1. Effective and well-tolerated analgesic in all 3 forms of administration
2. PO,IV,PR
3. Onset of analgesia is within 30 minutes.
4. Duration of action from 3 to 7 hours
5. Drowsiness - most frequent side effect
6. Transformation by the cytochrome P450 complex to the metabolically active O-
desmethyl-tramadol
Withdrawal symptoms after abrupt discontinuation or reduction of dose
DependenceSerotonin Syndrome

TapentadolCentrally acting analgesic with 2 mechanisms of action in a single
molecule:
• mu-opioid agonism
• norepinephrine reuptake inhibition
• four stereoisomers .RR, SS,RS and SR forms and RR form - approved as analgesic.
Oral absorption rapid
• Crosses the blood–brain barrier; a rapid onset of action
• t ½ = 4hrs
Is present in the serum in the form of conjugated metabolites
Excretion was exclusively renal
FDA approved tapentadol in 2008
moderate-to-severe acute pain in patients older than 18 years

Opiod antagonist
• Naloxone,Naltrexone, Nalmefene.
• Small doses (0.4 to 0.8 mg) i.m. or i.v. prevent or promptly reverse the effects of Mu receptor agonists.
• In morphine dependent ,small s.c doses of naloxone (0.5 mg) precipitate a moderate-to-severe withdrawal syndrome.
• In the neonate, the initial dose is 10 microgm/kg given intravenously, intramuscularly, or subcutaneously.

Therapeutic uses of opiods
• Analgesia
• Acute pulmonary edema
• Cough
• Diarrhea
• Shivering
• Applications in anesthesia.
Sir William Osler called morphine "God's own medicine."

APPROXIMATE
EQUI-ANALGESIC
APPROXIMATE
EQUI-ANALGESIC
RECOMMENDED STARTING DOSE
(adults > 50 kg)
DRUG ORAL DOSE PARENTERAL DOSE ORAL PARENTERAL
Opioid Agnoists
Morphine
30 mg q3-4h (around-the-clock dosing) 60
mg q3-4h (single dose or intermittent
dosing)
10 mg q3-4h 15 mg q3-4h 5 mg q3-4h
Codeine 130 mg q3-4h 75 mg q3-4h 30 mg q3-4h 30 mg q2h (1M/SC)
Hydrocodone 7.5 mg q3-4h 1.5 mg q3-4h 4 mg q3-4h 1 mg q3-4h
Hydrocodone ( typically with acetominophen)
30 mg q3-4h Not available 5 mg q3-4h Not available
Levorphanol 4 mg q6-8h 2 mg q6-8h 2 mg q3-4h 1 mg q6-8h
Meperidine 300 mg q2-3h 100 mg q3h Not recommended 50 mg q3h
Methadone 20 mg q6-8h 10 mg q6-8h 2.5 mg q12h 2.5 mg q12h
Oxycodone 30 mg q3-4h Not available 5 mg q3-4h Not available
Oxymorphone Not available 1 mg q3-4h Not available 1 mg q3-4h
Propoxyphene 130 mg Not available 65 mg q4-6h Not available
Tramadol 100 mg 100 mg 50-100 mg q6h 50-100 mg q6h

Patient Controlled Analgesia (PCA)

PCASelf adminastration of opiod agonist by parenteral route.
• Fentanyl is the preferred opioid in most circumstances.
• Morphine or hydromorphone are alternative choices.
• One hr max dose :Max amount of drug that PCA pump will deliver in 1 hour
• Continuous infusion
• Morphine 0.075 mg/kg
• Fentanyl 0.75 mcg/kg
• Freedom to self assess the need to push a tailored dose of an opiod
• Paradoxically less dependance.

Adverse Effects of the Opioid Analgesics
Behavioral restlessness, tremulousness, hyperactivity (in dysphoric reactions)
Respiratory depression
Nausea and vomiting
Increased intracranial pressure
Postural hypotension accentuated by hypovolemia
Constipation
Urinary retention
Itching around nose, urticaria (more frequent with parenteral and spinal administration)

Precautions
H5B3 conditions.
• Hypotension
• Hepatic damage
• Hypertrophy of prostate
• Head injury
• Hypothyroidism
• Bronchial asthma
• Biliary colic
• Babies
1. Not with corticosteriodas it increases
immunosupression.2. Partial agonist + pure
agonist=severe withdrawal symptoms.
3. Not with MAO inhibitors.
4. Not with sedatives.

NMDA antagonists
• Memantine
• Amantadine
• Ketamine

Indications
• Windup pain
• Opioid tolerance
• Opioid induced hyperalgesia
• Pain threshhold reduction
• Longterm potentiation

Ketamine
• A congener of phencyclidine
Non-competitive glutamate NMDA receptor antagonist.
• At low doses, the analgesia effects of ketamine are mediated
by antagonism on the NMDA receptors.
• Management of moderate to severe pain.
• Used in conjunction with opioids
• Norketamine, rapid clearance, large Vd
The ketamine-induced cataleptic state -nystagmus with
pupillary dilation, salivation,
lacrimation.

References
• Basic & Clinical Pharmacology,Katzung(12th
edition),2012.
• Goodman & Gilman’s the pharmacological basis of therapeutics(12th),2011
• Pharmacotherapy Hand book(6th
edition),B.Wells.

THANK YOUFor listening…….