PAIN MANAGEMENT QUESTIONNAIRE
13
Revised 2/28/18 PAIN MANAGEMENT QUESTIONNAIRE Date: ________ / ________ / ________ Patient Name: ____________________________________________ DOB: ________ / ________ / ________ Referring Physician: ________________________________________________________________________ Primary Care Physician: _____________________________________________________________________ Pharmacy: ________________________________________________________________________________ Have you had any imaging of the area you are here to have evaluated: □ Yes □ No If Yes, When: __________ / __________ / __________ Where: _______________________________________________________________________ Reason for appointment/Reason you were referred: □ Back Pain □ Neck Pain □ Arm/Leg Pain □ Shingles □ Abdominal Pain □ Cancer □ Headaches □ CRPS □ Other: __________ ***Please fill out the rest of this form only for the pain associated with the area you marked above *** ! Have you had this pain before: □ Yes □ No If Yes, When: ________________________________ ! Please describe how your pain began: _______________________________________________________ ! Do you have weakness of your extremities: □ Yes □ No If Yes, Where: □ Left Leg □ Right Leg □ Left Arm □ Right Arm ! Do you have numbness (inability to feel): □ Yes □ No If Yes, Where: __________________________________________ ! Do you have tingling: □ Yes □ No If Yes, Where: ______________________________________ ! Do you have loss of control of your: □ Bowel □ Bladder If Yes, Have you experienced this for a long time: □ Yes □ No Does it only happen with coughing/sneezing: □ Yes □ No Is it difficult to go: □ Yes □ No Have you had any accidents: □ Yes □ No If Yes, How often: _________ Page 1
Transcript of PAIN MANAGEMENT QUESTIONNAIRE

Revised 2/28/18
PAINMANAGEMENTQUESTIONNAIRE
Date:________/________/________PatientName:____________________________________________DOB:________/________/________
ReferringPhysician:________________________________________________________________________
PrimaryCarePhysician:_____________________________________________________________________
Pharmacy:________________________________________________________________________________
Haveyouhadanyimagingoftheareayouareheretohaveevaluated:□Yes□No IfYes,When:__________/__________/__________Where:_______________________________________________________________________
Reasonforappointment/Reasonyouwerereferred:□BackPain□NeckPain□Arm/LegPain□Shingles
□AbdominalPain□Cancer□Headaches□CRPS□Other:__________
***Pleasefillouttherestofthisformonlyforthepainassociatedwiththeareayoumarkedabove***! Haveyouhadthispainbefore:□Yes□NoIfYes,When:________________________________
! Pleasedescribehowyourpainbegan:_______________________________________________________
! Doyouhaveweaknessofyourextremities:□Yes□NoIfYes,Where:□LeftLeg□RightLeg□LeftArm□RightArm
! Doyouhavenumbness(inabilitytofeel):□Yes□NoIfYes,Where:__________________________________________
! Doyouhavetingling:□Yes□NoIfYes,Where:______________________________________
! Doyouhavelossofcontrolofyour:□Bowel□Bladder IfYes,
Haveyouexperiencedthisforalongtime:□Yes□NoDoesitonlyhappenwithcoughing/sneezing:□Yes□NoIsitdifficulttogo: □Yes□NoHaveyouhadanyaccidents: □Yes□NoIfYes,Howoften:_________
Page1
Revised 2/28/18
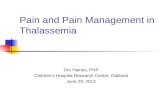
PatientName:_____________________________________________________________________________! Doesthepaininterruptyoursleep:□Yes□No
! Haveyouhadanyun-purposeful□Weightloss□WeightgainIfYes,Howmuch:_________pounds Whendidthisoccur:______________________________
! Doyouwakeupatnightsweatingorsoakingwet:□Yes□NoIfYes,Howoften:______________ Howlonghaveyoubeenexperiencing:______________
! Haveyoubeenseenbyanotherpainclinicinthepast:□Yes□NoIfYes,When:__________/__________/__________-__________/__________/__________
Who/Where:__________________________________________________________________
! Haveyouhadanypreviouspainmanagementinjections:□Yes□No IfYes,Whattype:___________________________________________Didithelp:□Yes□No ___________________________________________Didithelp:□Yes□No ___________________________________________Didithelp:□Yes□No
! Haveyouhadphysicaltherapy:□Yes□No IfYes,When:__________/__________/__________-__________/__________/__________Who/Where:__________________________________________________________________ Didyoulearnahometherapyprogram:□Yes□No
! Haveyouseenachiropractor:□Yes□No IfYes,When:__________/__________/__________-__________/__________/__________Who/Where:__________________________________________________________________
! Haveyouseenapainpsychologist:□Yes□No IfYes,When:__________/__________/__________-__________/__________/__________Who/Where:__________________________________________________________________ Didyoulearn:□Biofeedback□Copingskills□Relaxationmethods
! Haveyouhadacupuncture:□Yes□NoIfYes,When:__________/__________/__________Didithelp:□Yes□No
! HaveyouusedaTENSunit(electricalstimulationoftheskin):□Yes□NoIfYes,When:__________/__________/__________Didithelp:□Yes□No
Page2

Revised 2/28/18
PatientName:_____________________________________________________________________________
PainLocation-Onthefiguresbelow,usingthesymbolslsitedbelow,pleasemarktheareasofyourbodywhereyoufeel:
Numbness==== Stabbing//// BurningxxxxPin&Needlesoooo Aching(((( Areawhereithurtsthemost√
Page3

Revised 2/28/18
PatientName:_____________________________________________________________________________
AddressingthePersonalSideofLivingwithChronicPain
Asanindividuallivingwithpersistentchronicpaineveryday,youarefullyawarethatyourPAINdoesNOTjustaffectyouphysically.Chronicpaintoucheseverypartofyourlife.Yourpainaffectsyouemotionally,mentallyandspiritually.Livingwithpainhasanimpactonyourrolesinlife,yourrelationships,yourwork,yourhobbies,yourrecreationalactivitiesandtheoverallqualityofyourlife.Therefore,forustoeffectivelyaddresshelpingyoumanageyourpain,pleaseanswerthefollowingquestions.
1. Haveyoustruggledtomanageyourpainbyusingthe“olestiffupperlip” □Yes□Noor“toughitout”method?
2. Haveyoulostyourjob,missedasignificantamountofworkorstopped □Yes□No
physicalorrecreationalactivities?
3. Doyoufeelyouhavelostmeaningandpurposeinyourlife? □Yes□No
4. Haslivingwithpainchangedyourrolesinlifeasanemployee,spouse, □Yes□Noparent,etc.?
5. Doyoufeelyouhavefailedorletotherdownbynotbeingableto“DO” □Yes□Noasyouoncedid?
6. Doyoufeelyourpainisoftenincontrolofyourlife:? □Yes□No
7. Doyoufindyourmoodsbouncingaround,attimesyoufeeldepressed, □Yes□Noangryoranxious?
8. Dofamily/friendsseemtostruggletounderstandwhatitislikeforyou □Yes□Notolivewithchronicpain?
9. Doyoufeeljudgedattimes? □Yes□No
10. Doyoustrugglesometimesmakingadecisionaboutanactivityworrying □Yes□No
thatitwillresultina“flareup”?
11. Haveyounoticedthatasyourstresslevelincreasessodoesyourpain? □Yes□No
12. Doyoufinditdifficultto“relax”or“calm”yourselfasyougothrough □Yes□Noyourdaywithpain?
Pleasesharewithusanycommentsyouhaveregardingthescreeningquestionsoranypersonalconcernsordifficultiesyouhavelivingwithyourpain:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Page4

Revised 2/28/18
PatientName:_____________________________________________________________________________
BACKPAIN
! Isyourwalkinglimited:□Yes□No
Ifyes,howfarcanyouwalkwithoutstoppingtorest:___________________________blocks/miles
! Doesbendingoverholdingontoashoppingcart,etc.allowyoutowalkfarther:□Yes□No
! Whatpercentageinintheback:________%Whatpercentageisintheleg(s):________%
Pleasecheckallthatapply.
(whatcausedonsetofpain)
Page5

Revised 2/28/18
PatientName:_____________________________________________________________________________
ABDOMINALPAIN
Pleasecheckallthatapply.
(whatcausedonsetofpain)
Page5

Revised 2/28/18
PatientName:_____________________________________________________________________________
NECKPAIN
! Whatpercentageinintheneck:________%
! Whatpercentageisinthearm(s):________%
Pleasecheckallthatapply.
(whatcausedonsetofpain)
Page5
Revised 2/28/18
PatientName:_____________________________________________________________________________
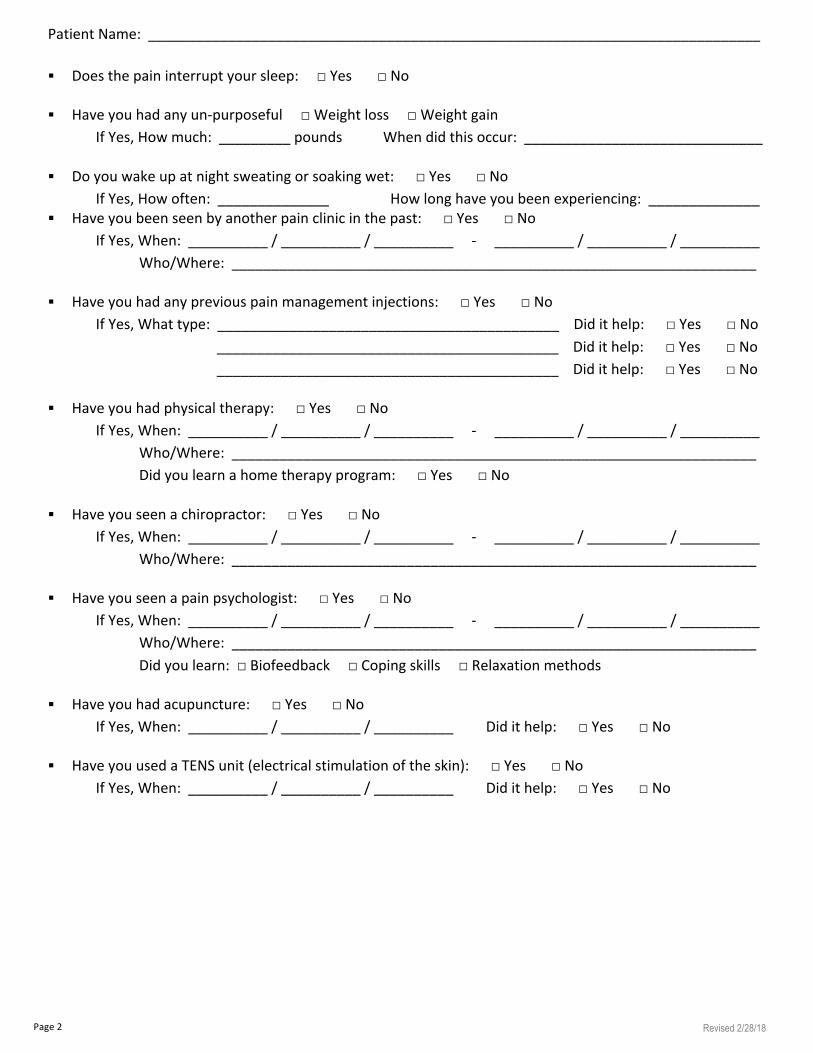
ARM/LEGPAIN
! Doesyouraffectedextremitychangecolor:□Yes□No
! Doesyouraffectedextremityfeel:□warmer□colder
! Doesyouraffectedextremityswell:□Yes□No
! Doeslighttouchworsenyourpain(puttingonsocks,sheetsonthebed):□Yes□No
! Haveyounoticed□hair□nailgrowthontheaffectedextremity:□Yes□No
Pleasecheckallthatapply.
Whatcausedonsetofpain:
Page5
Revised 2/28/18
PatientName:_____________________________________________________________________________
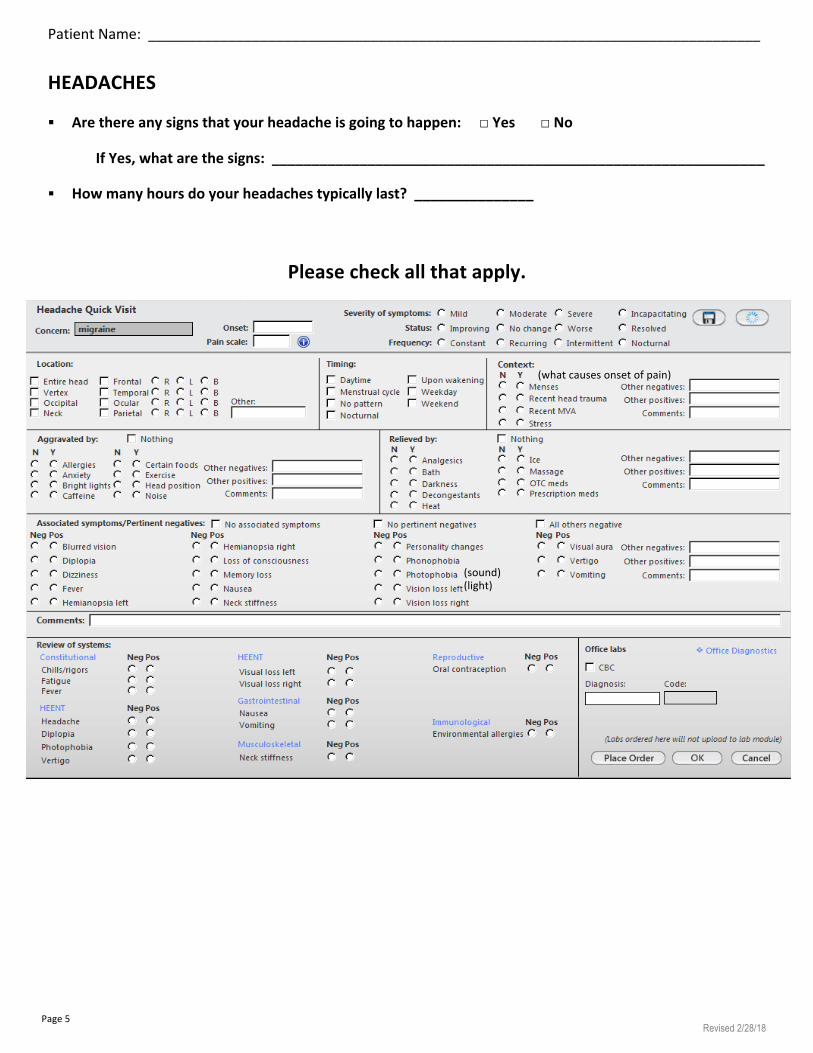
HEADACHES
! Arethereanysignsthatyourheadacheisgoingtohappen:□Yes□No
IfYes,whatarethesigns:______________________________________________________________
! Howmanyhoursdoyourheadachestypicallylast?_______________
Pleasecheckallthatapply.
PatientName:_____________________________________________________________________________
0=NoPain10=Painasbadasyoucanimagine
(sound)(light)
(whatcausesonsetofpain)
Page5

Revised 2/28/18
PatientName:_____________________________________________________________________________(0=Nopain/10=Painasbadasyoucanimagine)
MEDICATIONS-PleaselistALLmedications,includingherbalandover-the-counter:
Drug Dose PrescribingProvider
ALLERGIES-Drug/Item Reaction
Page6
Revised 2/28/18
PatientName:_____________________________________________________________________________
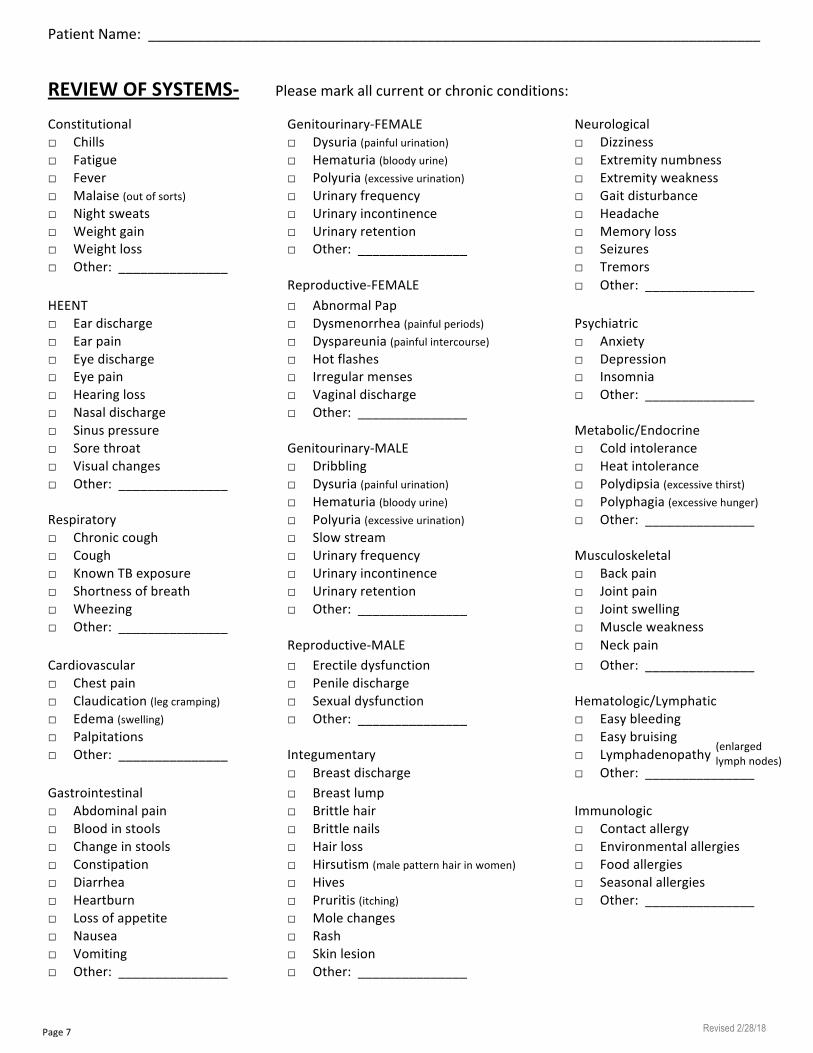
REVIEWOFSYSTEMS-Pleasemarkallcurrentorchronicconditions:
Constitutional Genitourinary-FEMALE Neurological□Chills □Dysuria(painfulurination) □Dizziness□Fatigue □Hematuria(bloodyurine) □Extremitynumbness□Fever □Polyuria(excessiveurination) □Extremityweakness□Malaise(outofsorts) □Urinaryfrequency □Gaitdisturbance□Nightsweats □Urinaryincontinence □Headache□Weightgain □Urinaryretention □Memoryloss□Weightloss □Other:_______________ □Seizures□Other:_______________ □Tremors Reproductive-FEMALE □Other:_______________HEENT □AbnormalPap□Eardischarge □Dysmenorrhea(painfulperiods) Psychiatric□Earpain □Dyspareunia(painfulintercourse) □Anxiety□Eyedischarge □Hotflashes □Depression□Eyepain □Irregularmenses □Insomnia□Hearingloss □Vaginaldischarge □Other:_______________□Nasaldischarge □Other:_______________ □Sinuspressure Metabolic/Endocrine□Sorethroat Genitourinary-MALE □Coldintolerance□Visualchanges □Dribbling □Heatintolerance□Other:_______________ □Dysuria(painfulurination) □Polydipsia(excessivethirst) □Hematuria(bloodyurine) □Polyphagia(excessivehunger)Respiratory □Polyuria(excessiveurination) □Other:_______________□Chroniccough □Slowstream□Cough □Urinaryfrequency Musculoskeletal□KnownTBexposure □Urinaryincontinence □Backpain□Shortnessofbreath □Urinaryretention □Jointpain□Wheezing □Other:_______________ □Jointswelling□Other:_______________ □Muscleweakness Reproductive-MALE □NeckpainCardiovascular □Erectiledysfunction □Other:_______________□Chestpain □Peniledischarge□Claudication(legcramping) □Sexualdysfunction Hematologic/Lymphatic□Edema(swelling) □Other:_______________ □Easybleeding□Palpitations □Easybruising□Other:_______________ Integumentary □Lymphadenopathy □Breastdischarge □Other:_______________Gastrointestinal □Breastlump□Abdominalpain □Brittlehair Immunologic□Bloodinstools □Brittlenails □Contactallergy□Changeinstools □Hairloss □Environmentalallergies□Constipation □Hirsutism(malepatternhairinwomen) □Foodallergies□Diarrhea □Hives □Seasonalallergies□Heartburn □Pruritis(itching) □Other:_______________□Lossofappetite □Molechanges□Nausea □Rash□Vomiting □Skinlesion□Other:_______________ □Other:_______________
(enlargedlymphnodes)
Page7

Revised 2/28/18
PatientName:_____________________________________________________________________________
PREVIOUSSURGERIES-Pleasebeasspecificaspossible:Surgery Date Location/Physician
MEDICALHISTORY-Pleasebeasspecificaspossible:Condition Management TreatmentOutcome
FAMILYHISTORY-! Isyourmotherliving:□Yes□No IfYes,Age:_______________IfNo,Ageatdeath:_______________
Listallmedicalproblems:______________________________________________________________
! Isyourfatherliving:□Yes□No IfYes,Age:_______________IfNo,Ageatdeath:_______________
Listallmedicalproblems:______________________________________________________________
! Siblings: □Brother□SisterLiving:□Yes□No
IfYes,Age:_______________IfNo,Ageatdeath:_______________Listallmedicalproblems:________________________________________________________
□Brother□SisterLiving:□Yes□NoIfYes,Age:_______________IfNo,Ageatdeath:_______________Listallmedicalproblems:________________________________________________________
□Brother□SisterLiving:□Yes□NoIfYes,Age:_______________IfNo,Ageatdeath:_______________Listallmedicalproblems:________________________________________________________
Page8

Revised 2/28/18
PatientName:_____________________________________________________________________________
SOCIAL-! Haveyouhadanyrecentsocialchanges(marriage,divorce,employment,etc.):□Yes□No
IfYes,describe:______________________________________________________________________
! Areyoumarried:□Yes□NoIfYes,HowLong:_______________Nameofspouse:______________________________________
! Isyourspousedeceased:□Yes□NoIfYes,When:__________/__________/__________
! Haveyoubeendivorced:□Yes□NoIfYes,Howmanytimes:_______________
! Areyoucurrentlyemployed:□Yes□No IfYes,Howlong:_______________ Occupation:__________________________________! Areyoureceivingdisability:□Yes□No
! Isthispainbeingtreatedbyaworkerscompensationclaim:□Yes□No
! Haveyoutakenanylegalactioninregardstoyourpain:□Yes□No
! Haveyoueverbeenabused:□Yes□NoIfYes,□Physical□Sexual□Emotional
HABITS-! Doyousmoke:□Yes□No □Quit When:__________/__________/__________
IfYes,Packsperday:_______________Years:_______________
! Doyousmokeapipe:□Yes□No□Quit When:__________/__________/__________IfYes,Howmuch:_______________Years:_______________
! Doyouchewtobacco:□Yes□No□Quit When:__________/__________/__________IfYes,Howmuch:_______________Years:_______________
! Doyoudrinkalcohol:□Yes□No□QuitWhen:__________/__________/__________IfYes,Howmuch:_______________Years:_______________
! Doyouuseillegaldrugs:□Yes□No□Quit When:__________/__________/__________IfYes,Howmuch:_______________Years:_______________Whattypes:____________________________________________________________________
! Doyouconsumecaffeine:□Yes□NoIfYes,
□Coffee _______________cups/day□Tea _______________cups/day□Soda _______________cups/day□EnergyDrinks_______________cups/day
Page9