
Pain Management in Anaesthesia
67
-
Upload
annan-agyekum-joshua -
Category
Documents
-
view
222 -
download
0
Transcript of Pain Management in Anaesthesia
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 1/67

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 2/67
Background 50% of all consultations in primary
healthcare are pain-related
40% have suffered more than 3 months85% suffer from musculoskeletal pain
Chronic pain = poor quality of life, suffering,
reduced ability to work and poorer socialfunction
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 3/67
Why treat pain? Untreated pain increases anxiety and pain perception.
Stress response is invoked by pain (andanxiety!).Neuroendocrine response (ACTH, Epi, NE,glucagon, etc increased)
Results: Increased VO2, CO2 production, catabolic state
The more pronounced the stress response, the higher the
mortality. Animal models show that repeated pain during “infancy”
causes alterations in the adult brain: Altered painsensitivity, anxiety, hyperactivity, impaired social skills,self-destructive behavior.
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 4/67
As anaesthetists We need to understand pain
We need to prevent pain and chronification – perioperative analgesia!
When needed, we have to know how to treat chronic
pain conditions

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 5/67
Agenda Physiology of pain
Acute and chronic pain
Nociceptiv versus neuropathic pain
Strategies for the treatment of established painconditions
Some pharmacological principles for analgetic drugs
Conclusion

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 6/67
Definition IASP (International Assosiation for the Study of Pain):
Pain is an unpleasant sensory and emotionalexperience associated with actual or potenial tissuedamage, or described in terms of such damage.
Pain is what the patient describes as painful.

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 7/67
Pain
Depression/anxiety Sleep disturbance
The pain triangle

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 8/67
Pain has a purpopse
Localise pain stimulus aninitialise responses in order
to reduse tissue damage
Initialise actions andaffective reactions that can
influence future behavior
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 9/67
Pain has a purpose ? But:
Intense and prolonged pain signals will lead to changes
in the pain signal pathways that may lead to thedevelopment of chronic pain!

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 10/67
Chronic pain after surgeryPerkins and Kehlet, Anesthesiology 93:1123, 2000
11 %Inguinal hernia
3 –
56 %Gallbladder surgery
11 – 57 %Mamma surgery
47 %Thoracotomy
30 – 81 %Extremety amp.
IncidenseSurgery

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 11/67
And this is one reason to Optimise the perioperative analgesia
Preemptive/preventive analgesia-premedication
Intraoperative analgesia Postoperative analgesia
Basics – paracetamol + NSAIDs
PCA/NCA
Epidurals or continuous regional blocks Loco-regional analgesia
Field blocks
Thoracic epidurals
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 12/67
Pain
Acute - chronic
Physiologic
Somatic nociceptiv
Neuropathic
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 13/67
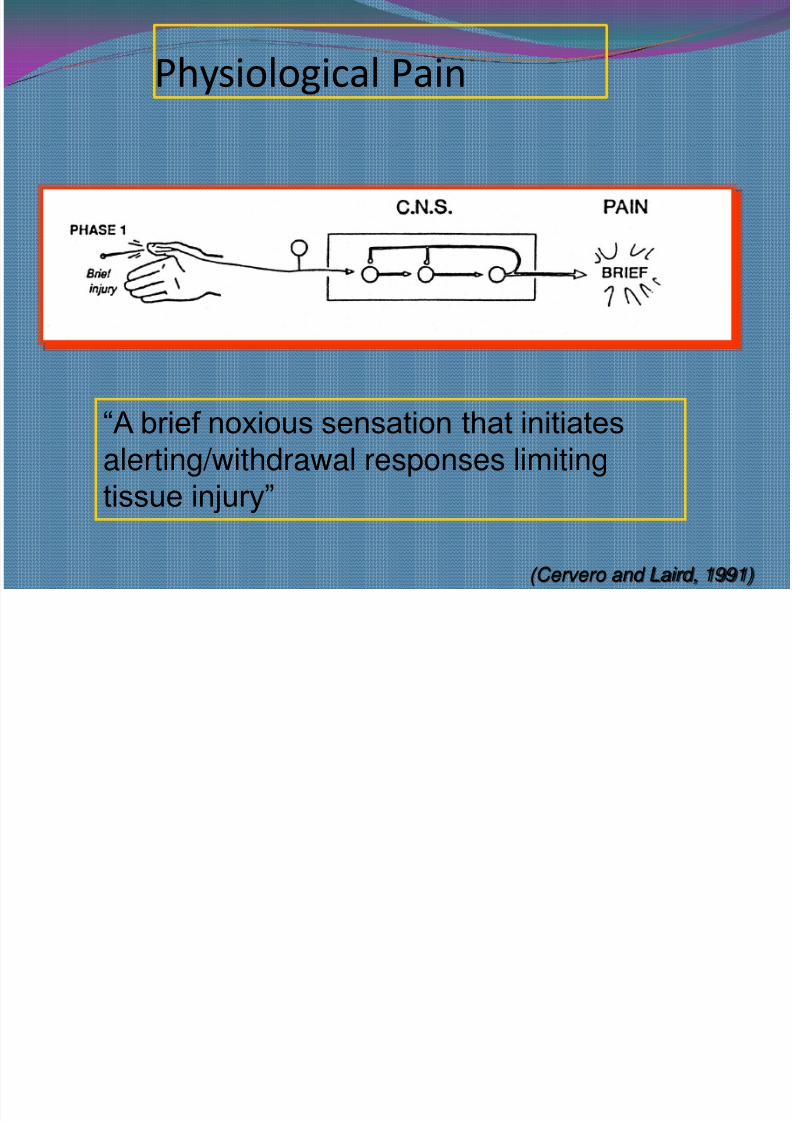
Physiological Pain
(Cervero and Laird, 1991)
“A brief noxious sensation that initiatesalerting/withdrawal responses limitingtissue injury”
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 14/67
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 15/67
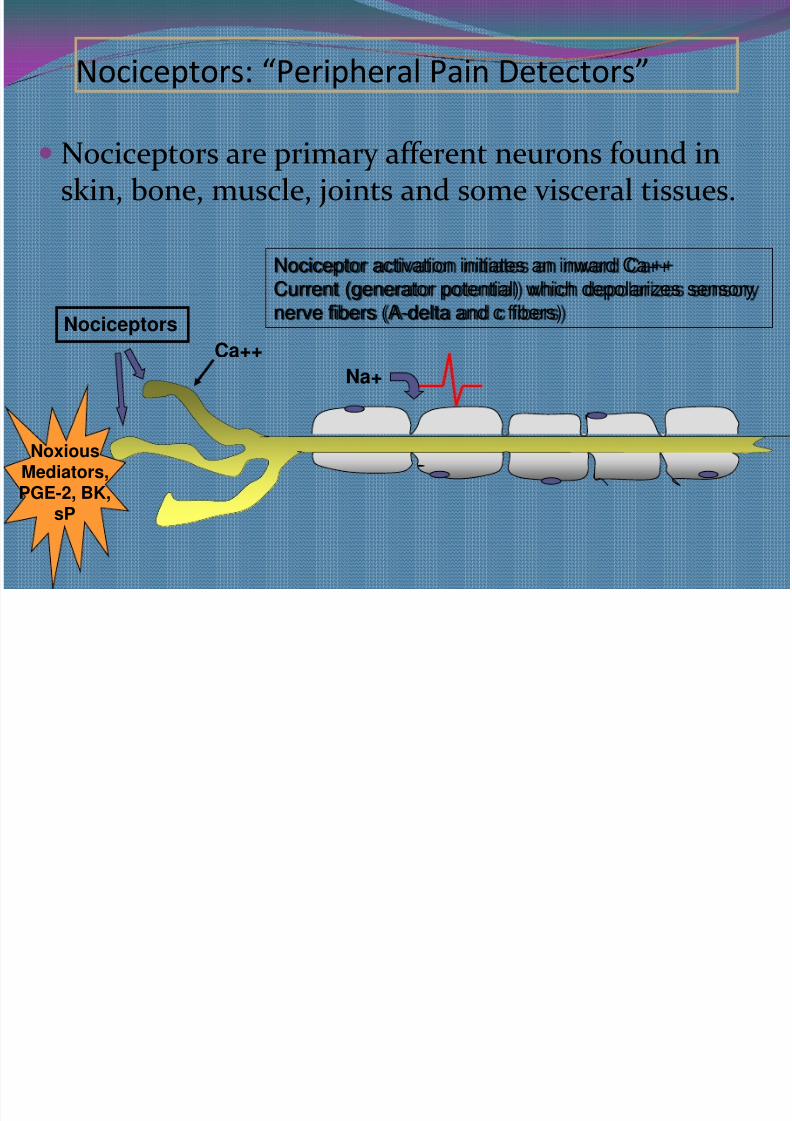
Nociceptors: “Peripheral Pain Detectors”
Nociceptors are primary afferent neurons found inskin, bone, muscle, joints and some visceral tissues.
Nociceptors
Nociceptor activation initiates an inward Ca++Current (generator potential) which depolarizes sensorynerve fibers (A-delta and c fibers)
Ca++
NoxiousMediators,PGE-2, BK,
sP
Na+

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 16/67
Nociceptive (Somatic) Pain
Activation of nerve endings in somaticstuctures (skin, muscle, bone) in
response to irritation or injury Pain is persistent, well localized, sharp
or crushing
Includes: trauma, surgical pain, tumorinvasion, arthritis and muscle spasm

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 17/67
Nociceptive (Visceral) Pain
Activation of nerve endings in gastro-intestinal organs and peritoneum in
response to irritation or distentionPain is persistent, poorly localized
cramping, periodic (colicky)
Includes: bowel or urethral obstruction,peritonitis and appendicitis

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 18/67
The primary noxiousmediator released fromdamaged tissue isprostaglandin (PG)
PG is responsible fornociceptor activationand sensitization
PG plays a major rolein peripheralinflammation
Nociceptor Activation (Transduction)
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 19/67
Is modulated by the number of chemical substances.
Mediators influence ;
Degree of nerve activity
Intensity of pain sensation
Repeated stimulation causes sensitization of the nerve
fibers causing; Lower pain threshold
Spontaneous pain
Chemical signaling protect the injury area by producing behaviours that keep away from thestimulus.

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 20/67
Sensitization:
Tissue Injury
Repetitive Stimulation of C-fibers
Progressive Increase in Action Potentials
Prolonged Increase in Spinal Cord Excitability

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 21/67
Neural Responses to Tissue Injury
Primary hyperalgesia:
- Increased pain sensitivity at the injury site
- Related to peripheral release of cellular orhumoral noxious mediators
Secondary hyperalgesia:
- Increased pain sensitivity at adjacent,uninjured sites
- Related to changes in excitability of spinalneurons
Urban and Gebhart, Med Clin North Am 1999; 83: 585
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 22/67
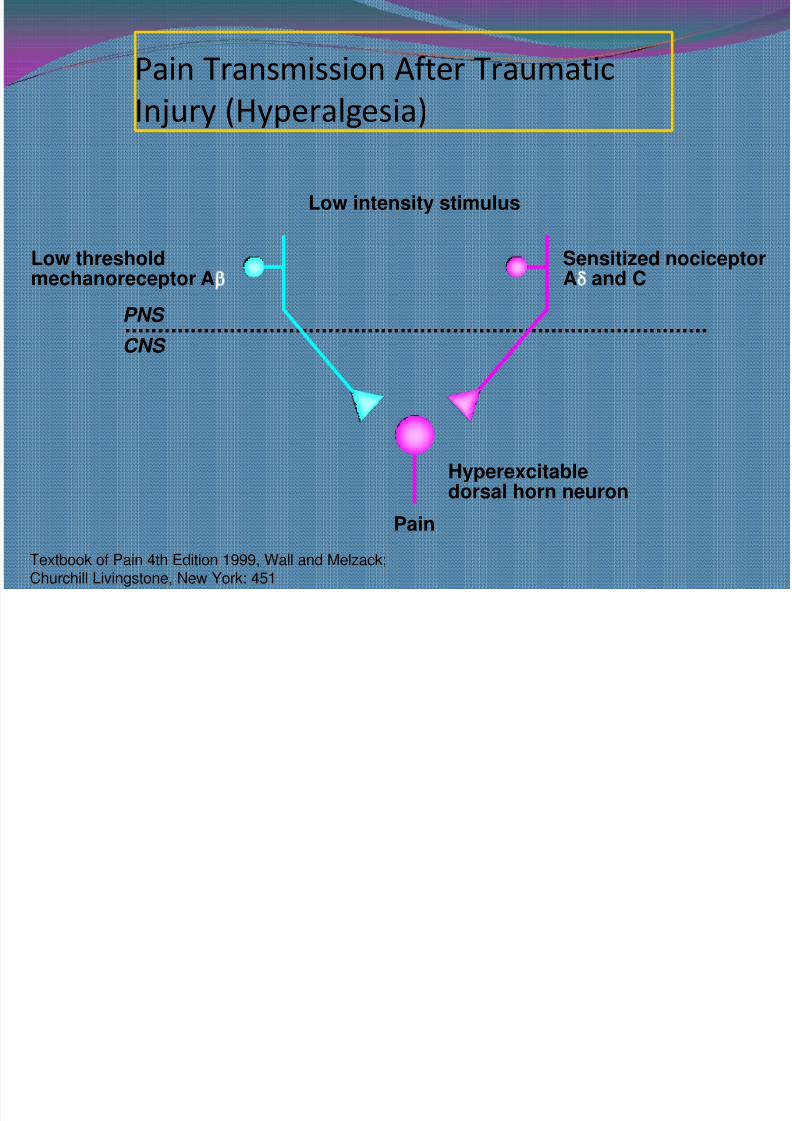
Pain Transmission After Traumatic
Injury (Hyperalgesia)
Textbook of Pain 4th Edition 1999, Wall and Melzack;Churchill Livingstone, New York: 451
PNS
CNS
Pain
Low intensity stimulus
Hyperexcitabledorsal horn neuron
Sensitized nociceptor
A and C
Low threshold
mechanoreceptor A

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 23/67
Action potential is produced
Transmitted by nociceptive nerve fibers to the dorsalroute of the spinal cord.
The fibers synapse with ascending spinothalamicfibers to the CNS
These spinothalamic fibers are clustered into two
specific pathways; A delta fibers innervates cells of the lamina I (MARGINAL
ZONE)
C fiber innervates cells of the lamina ii (SUBSTANSIA GELATINOS)
Through synapsing of nociceptive fibers with motorfibers in the SC muscle rigidity can occur. It can lead tohypoventilation and hypoxemia.
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 24/67
signals can be altered by electrochemical means tomodulate the sensation, either to amplify it ordiminish it.
significant areas for modulation are at the junction of
the peripheral and central nervous systems, at thedorsal horn, and in the ascending and descendingtracts to and from the brain
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 25/67
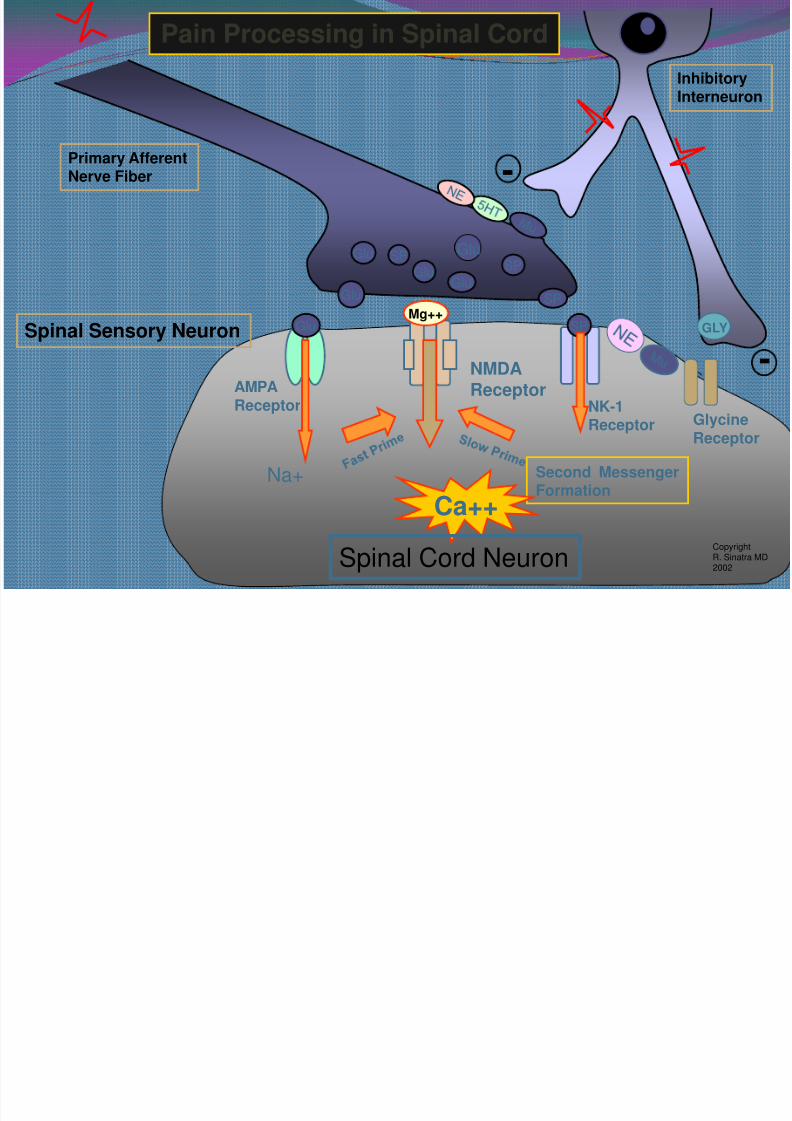
Glu
Glu
Glu
SP
GluSP
SP
Glu
SP
Mg++
-
-
NK-1Receptor
AMPAReceptor
NMDAReceptor
Primary AfferentNerve Fiber
Spinal Sensory Neuron
InhibitoryInterneuron
Pain Processing in Spinal Cord
Second MessengerFormation
Ca++
Glu
Na+
Copyright
R. Sinatra MD2002Spinal Cord Neuron
GlycineReceptor
GLY
Neurochemical Anatomical Alterations

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 26/67
A-fiberConnections
AxonSprout
Synaptic
Removal
MicroglialCells
NOS
Nitric Oxide
2nd Messengers, (IP, PK, cGMP)
Genome Activation, RNA& Protein Synthesis,Hyperexcitability, Toxicity
NONO
NO
NO, PG
Aracadonic Acid
COX-2
PGE2, PGI2
InterneuronCell Death
Inflammation
HyperexcitabilityToxicity?
NMDA
PG
PG
PG
NO,
PG
Neurochemical-Anatomical AlterationsLeading to Persistent Pain
++
Ca++
sPGlu
Glu
CopyrightR. SinatraMD, 2002
Spinal Sensory Neuron
Primary AfferentNerve Fiber
Interneuron
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 27/67
The neurochemistry of these processes involves anextraordinary array of compounds, including
endorphins
neurokininsprostaglandins,
biogenic amines,
GABA,neurotensin
cannabinoids
purines and many others

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 28/67
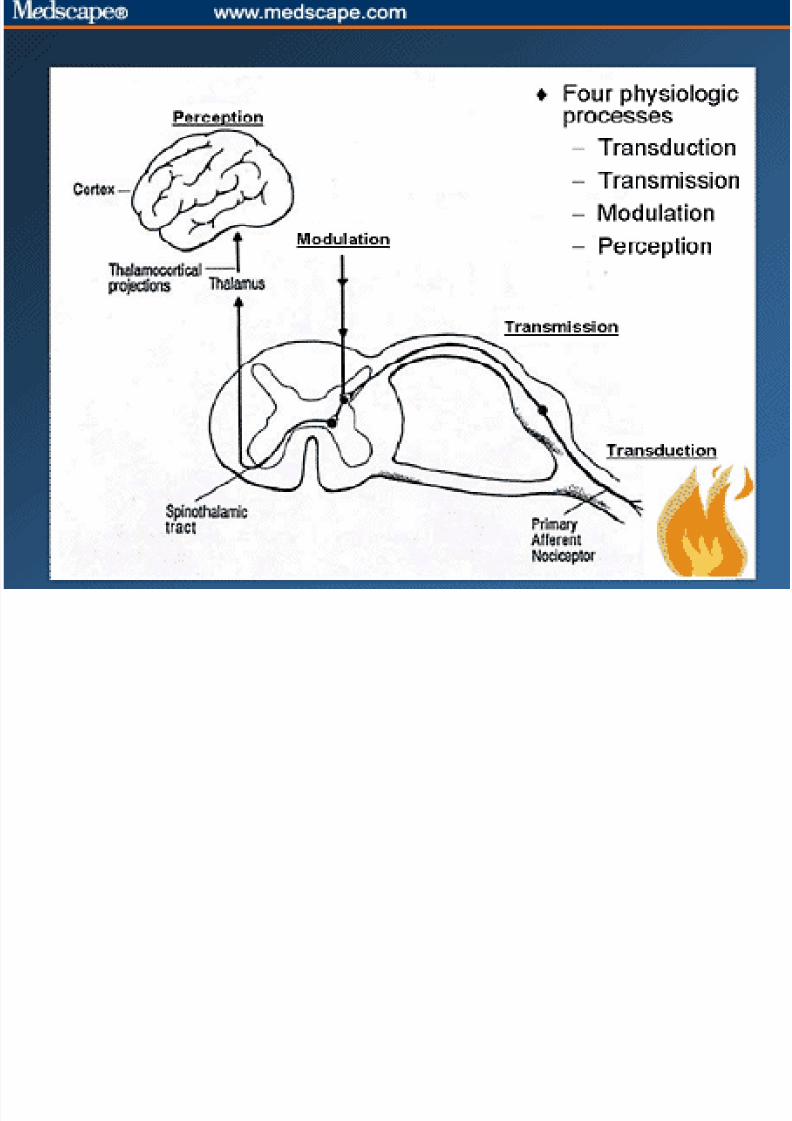
PERCEPTION Pain message reaches the center of the brain where is
percieved.
Pain sensation transmitted by the marginal zonereaches the thalamus, while those by the substansiagelatinos reaches the brainstem, hypothalamus andthalamus.
Projections is made to the limbic system then tothesensory cortex in the parietal lobe and allow clientto describe the sensory characteristics of the pain
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 29/67
MODULATION Production of endogenous opoids by the CNS such as
beta-endophins.
It inhibits the production of substance p and blocktransmission of pain sensation in the spinal cord andproduces analgesia.
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 30/67
Neuropathic Pain
Pain caused by irritation(inflammation!) or direct injury
or dysfunction of the peripheralor central nervous system.
Neuropathic pain is usually continuous and described asburning, electrical and shooting
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 31/67
It may mimic the quality of somatic pain, but also isfrequently described in terms that warrant thedescriptor “dysesthetic:” an uncomfortable, unfamiliar
sensation such as burning, shock-like or tingling. Neuropathic pain syndromes may be associated with
referred pain, allodynia (pain induced by non-noxiousstimuli, e.g. light touch), hyperalgesia (increased
response to a noxious stimuli), or hyperpathia(exaggerated pain responses following a stimulus, oftenwith aftersensation and intense emotional reaction).

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 32/67
Treatment of pain patients; a practical
approach
Investigation and examination
Diagnosis
Treatment-strategy
Pre-op
Intra-op
Post-op
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 33/67
Importance of Perioperative Pain Management
Prevention and effective relief of acute perioperativepain may:
Improve clinical outcomes
Decrease complications
Improve quality of life
Improve patient satisfaction

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 34/67
NMDA-Antagonists
Ketamine 0.2-0.5mg/kg
Acetaminophen- 650mg maxi◦ Mechanism of action uncertain
◦ Peripheral Decreased prostaglandin synthesis
Interference with NO pathways
◦ Central Modulation of descending pain pathways Modulation of dynorphin release
◦ Excellent safety profile at doses of 1g Q 6 hours
◦ Toxicity (>4g/d)
Hepatotoxicity
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 35/67
NSAIDs
◦ Advantages: Anti-inflammatory, analgesic, limited sedation,non-addicting, +cheap, available OTC
◦ Concerns: available OTC in multiple preps, GI effects, renal and hepatic toxicity, platelet effects, f luid retention
Ketorolac◦
Potent analgesic◦ Mild anti-inflammatory ◦ Absence of ventilatory or cardiac depression◦ May cause excessive GI bleeding (limit course to 5d)◦ Meta-analysis
36% reduction in opiate requirements Ketorolac 10-30mg equivalent to Morphine 10-12 mg Onset less than 10 min Duration 6-8hrs
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 36/67
Anticonvulsants
Pro: Neuropathic pain: lancinating, burning
Con: Ataxia, sedation, confusion (esp elderly)
DrugsCarbamazepine (Tegretol) Gabapentin (Neurontin), Pregabolin (Lyrica)
Lamotrigine (Lamictal)
Topiramate (Topomax), Zonisamide (Zonegran)
Oxcarbazepine (Trileptal), Clonazepam (Klonapin)**
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 37/67
Intra op and post op Regional anesthesia
◦ Spinal◦ Epidural
◦ Peripheral nerve blocks
Local anesthesia◦ Well documented
◦ Injection of triggerpoints and myoses◦ Should be used routinely on all operations◦ Long duration preferrable◦ Combination with steroids
D d i i t ti

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 38/67
Drug administration
NSAIDs-Coxibs Paracetamol
Steroids
Co-analgetics Opioids
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 39/67
Paracetamol and NSAIDs Both groups are ”weak analgesics” – former peripheral
analgesics
Both over-the-counter
Both are combined by many
NSAIDs vs. coxibs

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 40/67
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 41/67
Paracetamol: do we use enough?
Dosage:
Children: 15 mg/kg, recommended daily dose 45 mg/kg,max 60-75 mg/kg
Does not divide between per-oral and rectal
Adults: 500-1000 mg X 3
70 kg = 14,3 mg/kg, max daily dose 43 mg/kg

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 42/67
Facts ?
Anti-pyretic effect: 12-15 mg/l – central effect!
Analgesia ??
Relative bio-availibility of rectal administration = 0.54(Anesthesiology 1999; 90: 411-421)
Relative prolonged upptake (35 vs. 4,5 min) rectal,upptake starts later (40min)
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 43/67
Facts?
Analgesic effect is correlated to peak plasmaconcentration – transfer to CSF?
Intravenous>peroral>>rectal
Longer halflife in CSF than plasma (3.2 hours versus
2.4, Br J Clin Pharmacol 1992; 34: 79-81)
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 44/67
Paracetamol dosing
Acute pain, adults >50 kg: 1,5-2g, then 1gx4
Acute pain, adults < 50 kg: 1-1,5g, then 1gx4
Children, suppositories: first dose: 30-40mg/kg, then15mg/kg x 4
Children, per-oral: first dose 20-30mg/kg,then 15 mg/kg x 4
* Iv paracetamol!
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 45/67
Experience on patients
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 46/67
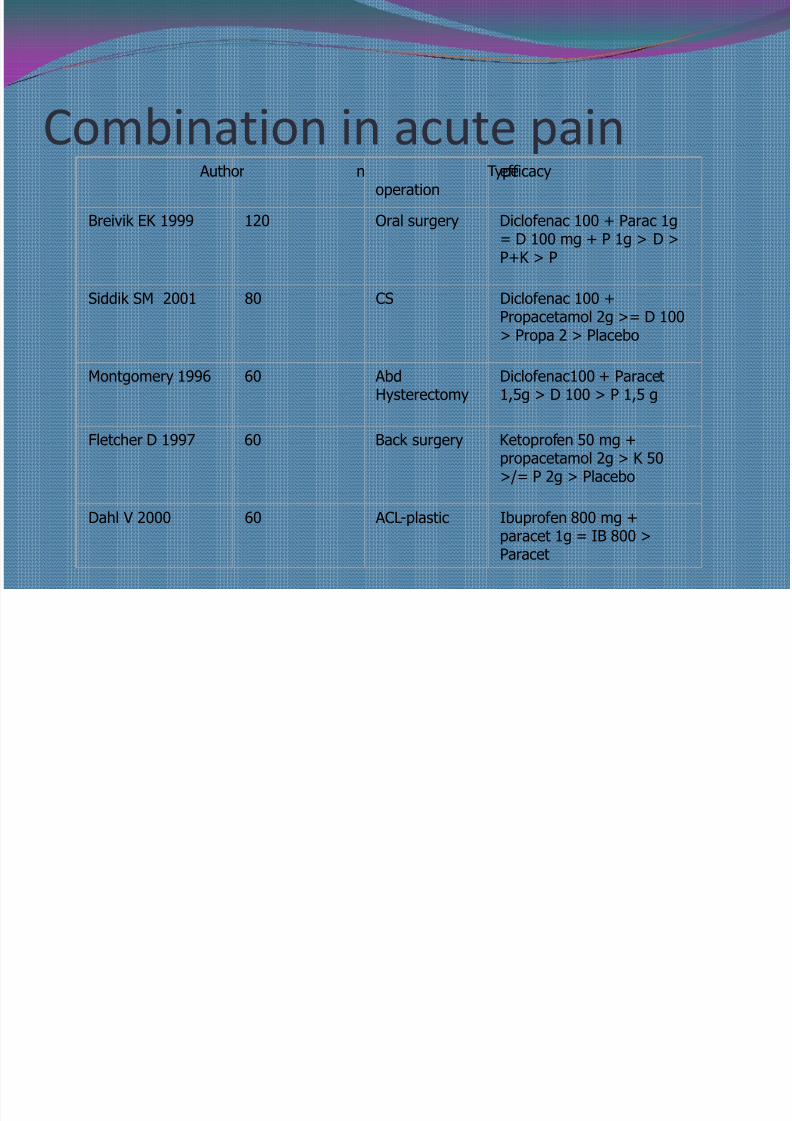
Combination in acute pain Author n Typeoperation
efficacy
Breivik EK 1999 120 Oral surgery Diclofenac 100 + Parac 1g= D 100 mg + P 1g > D >P+K > P
Siddik SM 2001 80 CS Diclofenac 100 +Propacetamol 2g >= D 100> Propa 2 > Placebo
Montgomery 1996 60 AbdHysterectomy
Diclofenac100 + Paracet1,5g > D 100 > P 1,5 g
Fletcher D 1997 60 Back surgery Ketoprofen 50 mg +propacetamol 2g > K 50>/= P 2g > Placebo
Dahl V 2000 60 ACL-plastic Ibuprofen 800 mg +paracet 1g = IB 800 >
Paracet

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 47/67
Steroids Well documented in surgery and other acute pain
conditions
Analgesia and less PONV
Metabolic effect: Good against kacheksia?
Cheap
Little side-effects in short-time use
Dexamethasone 8mg iv

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 48/67
Opioids: The Alternative Buffet

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 49/67

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 50/67
Opioids most opioids = μ-receptor agonists
Genetically codet several subunits μ-receptors
Patients are different – different efficacy and side-effects of the different opioids
Dose/response varies from patient to patient
Combination with paracetamol/NSAIDs

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 51/67
Sites of Opioid Action Peripheral nerve endings◦ Stim of peripheral opioid receptors may block central transmission
and release of inflammatory mediators (beta endorphin,proenkephalin A)
Dorsal horn, spinal cord◦ Dynorphin, enkephalin rich
Midbrain, brainstem, thalamus◦ Dynorphin, enkephalin rich,◦
Receive beta endorphin innervation from hypothalamus
Limbic system, cortex◦ Emotional dimension of pain, rich in dynorphin, enkephalin,
have beta endorphin input as well

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 52/67
Opioids Effects Nausea, vomiting Ileus, constipation
Pruritis Sedation, confusion Respiratory depression Bradycardia Cough respiration Tolerance Dependence Addiction

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 53/67
”Weak” opioids Codeine (Kodein®, Pinex Forte®)
Tramadol (Nobligan®)
Buprenorfin (Temgesic®, Subutex®, Norspan®)

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 54/67
”strong” Opioids Morphine (inj, epidural, oral, Dolcontin®) Ketobemidone Pethidine Oxycodone (Oxynorm®,Oxycontin®) Pentazocin (Fortralin®)
Hydromorfon (Palladon®)
Fentanyl (Leptanal®, ActiQ®, Durogesic® )
Sufentanil (Sufenta®)
Alfentanil (Rapifen®)
Remifentanil (Ultiva®)

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 55/67
Opiates
Effective Analgesics
Variety of Administration Routes
Adverse events with opiate usage Drowsiness and sedation (30%)
Nausea and Vomitting (31%)
Pruiritis (18%)
Urinary Retention(17%) Ventilatory Depression(3%)
Tolerance

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 56/67
Morphine Prototypical opioid
Slower onset (5-10min)
Causes histamine release
Careful in renal patients IV, PO, epidural, spinal
Dosage; 1-4mg IV bolus
1-10mg IV infusion
Duration;
3-4hrs
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 57/67
Hydromorphone
Congener of morphine
Less accumulation in renal/hepatic insufficiency
Faster onset than Morphine (3-5min) More potent than Morphine
Dosage;
0.2-1mg bolus
0.2-2mg infusion

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 58/67
Fentanyl Synthetic, highly lipid soluble
Fast onset(1-5min), short duration(0.5-4hrs)
IV, respiratory depression can be profound, but brief due to redistribution of drug
Transcutaneous—stable drug level at 12- 24 hr; IV, PO,Epidural, spinal
Dosage; 25-100mcg bolus
25-200mcg infusion

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 59/67
Meperedine
Less potent than morphine
Onset; 5-10min
Duration; 2-4hrs
May actually cause tachycardia
Active metabolite-normeperidine—CNS excitation,
seizures Dosage;
75-100mg IM

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 60/67
Opioids As little as possible
Opioid rotation
Avoid combination preparations
Per-oral, slow release
For non-malign pain: make agreements withthe patient ( WHO guidelines)
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 61/67
WHO-guidelines
• All other treatment options must havebeen tried
• The pain must be opioid sensitive
• Psychosocial status must be known
• Written agreement
• Preferrably long-acting opioids
• Treatment must be monitored
Eija Kalso, SASP, WHO
B e
E l ti

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 62/67
eh a n d l i n g
Evaluation• Pain intensity:
numeric (NRS):
or visual analog scale (VAS):
• Psychometric methods (HAD, GHQ)
• Quality og life (SF-36, EORTC)
Ingen
smerter
Verst
tenkelige
smerte
(10 cm)
Ingen
smerter
Verst
tenkelige
smerte
0 1 2 3 4 5 6 7 8 9 10
5. PerceptionM l i d l A l i

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 63/67
5 e cept o
3. Transmission
1. Transduction
Multimodal Analgesia
--
Copyright R. Sinatra MD.2002
6. CNS Responses
Muscle Relaxants,Beta Blockers
NSAIDS, COX-2 Inhibitors, Anti-Histamines, TopicalLocal Anesthetics
Peripheral Nerve Block
Local Anesthetics
Epidural BlockLocal Anesthetics
Opioids,Clonidine,
COX-2 Inhibitors
Opioids, Paracetamol,Clonidine, Ketamine,Gabapentin, Tricyclics
PAIN
4. Modulation
2. Conduction

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 64/67
Conclusion 1
Pain is what the patient say it is
Acute pain may become chronic pain, especially when
under-treated
Neuropathy: Pain caused by pathology in the painsignalling system
Patient investigation: Nociceptive, neuropathic ormixed pain?
8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 65/67

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 66/67
Conclusion 2 Time limited plan for treatment
Multimodal pharmacological treatment
Multidisciplinary treatment
Simultaneousness

8/2/2019 Pain Management in Anaesthesia
http://slidepdf.com/reader/full/pain-management-in-anaesthesia 67/67


















