Pain Management and Safe Prescribing › content › dam › nursing › docs...Ohio and U.S....
104
Pain Management and Safe Prescribing Cleanne Cass, D. O., FAAFP, FAAHPM Appointed Member, Governor’s Cabinet Opioid Action Team Co Chair, Treatment Work Group Ohio Prescription Drug Abuse Task Force
Transcript of Pain Management and Safe Prescribing › content › dam › nursing › docs...Ohio and U.S....

Pain Management and Safe Prescribing
Cleanne Cass, D. O., FAAFP, FAAHPMAppointed Member, Governor’s Cabinet Opioid Action TeamCo Chair, Treatment Work GroupOhio Prescription Drug Abuse Task Force

Why are we here today?
2

Today:An “Epidemic of Opioid Overdoses in
the United States and in Ohio?
3

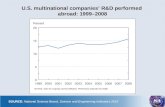
Ohio and U.S. Unintentional Drug Overdose Death Rates per 100,000 Population
1999-2006 U.S. /1999-2008 Ohio
4

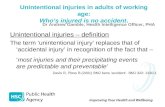
Number of Deaths from Motor Vehicle Traffic, Suicide and Unintentional Drug Poisonings by Year in Ohio 1999 – 2008
5

Contributing Factors to Rising Fatal Drug Death Rates
6

Unintentional Fatal Drug Poisoning Rates and Distribution of Prescription Opioids in grams per 100,000 Population by Year -
Ohio 1997 – 2007
7

Unintentional Drug/Medication Poisoning Death Rates per 100,000 by County 2004 – 2008
8

In Ohio:
Over 931,000 adult and 231,000 children with chronic malignant and non-malignant painOhio Compassionate Care Task Force, 2004
9

The Provider’s Dilemma:“Twin serpents in the Caduceus”
Undertreated Pain and related costs:- Nationally 100 million Americans with
chronic pain at a cost of >635 billion dollars
IOM Report on Pain - 2011
Opioid Abuse and related costs- Nationally > 6 million Americans abusing
opioids at a cost of 70 billion per year Money Magazine
10

THE CHALLENGE : How to prevent abuse and diversion and still safely treat the over 1million Ohioans who live with chronic pain
11

As the gatekeepers of prescription medications physicians are being charged with fighting on two fronts: combating pain while defending against misuse of opioid medications!
Is Pharmaco Vigilance more than we can ask of Physicians ??
12

Review of death certificates: majority of opioid related deaths involve other substances -marijuana, cocaine, alcohol
Chronic pain patients not the ones dying from opioid overdoses
Millions of opioid doses are reaching the wrong hands!!
13
Examining the data more closely:

“ It is unclear how much abuse, diversion and addiction is the result of well meaning but under-educated or under-informed physicians.”
Fish, P8
14

Institute of Medicine Report – June, 2011
Treating pain is a moral imperativeImproved efforts to prevent pain are needed Increased research/ education on pain is neededA biopsychosocial model of pain management improves outcomesA transformation is needed in our cultural view of pain
15

Treating Pain –A Moral Imperative
Eighty percent of patients presenting for health care have pain
Undertreated acute pain may become chronic disabling pain: complex regional pain syndrome
Under treatment of pain can lead to alcohol and substance abuse; isolation, depression, and institutionalization in the elderly
16

“Physicians need training and experience in pain management if issues of access and under treatment are going to be addressed”National Pain Care Policy Act of 2009 Incorporated into the Obama Healthcare Reform Bill
The real issue for prescribers in Ohio’s Pain Epidemic is not whether or not to treat pain but how!
17

Two imperatives:
To treat pain in a manner that is safe and effective for the patient
To understand and implement Ohio’s regulatory oversight in order to protect our prescriptive rights
18

Today’s DiscussionRegulatory Oversight in Ohio
Safe and Effective Pain Management
19

Regulatory Oversight
CDC guidelinesOhio’s Automated Rx Regulatory SystemOhio’s Intractable/Chronic pain lawEmerging actions: Emergency Department Guidelines for Pain Management
20

CDC Guidelines: Epidemic: Responding to America's Prescription
Drug Abuse Crisishttp://www.cdc.gov/mmwr/preview/mmwhtml/m
mwrhtml/mm6101a3htm? cid=6101a3wSpecifically address the concern of access to
care for patients and the need to address the significant concern and expense of untreated pain
These serve as guidepost for the states – they are specifically Guidelines and not Laws
21

CDC Guidelines
Epidemic: Responding to America's Prescription Drug Abuse Crisis, The Administration's plan for addressing prescription drug abuse released in April 2011: four components:education, tracking and monitoringproper medication disposal,enforcement.
22

Ohio Automated Rx Regulatory System: OARxRS
Ohio Revised Code – 4729.75-4729.84Tool for prescribers, pharmacists to identify and prevent abuse and addictionTool for law enforcement to deter diversionPharmacists must enter data electronically weeklyReported drugs: schedule CII, CIII, CIV ,V,
Carisoprodol (Soma)& tramadol ( Ultram)
23

OARxRS
Who can access OARRS?Pharmacist – own customer onlyPhysician – current patient onlyPhysician’s non licensed designee (HB93)Individual – own reportLicensing boards – own licensee
Law enforcement - only as part of a certified active investigation of suspected diversion, abuse or drug trafficking
24

OARxRS: HB 93 expanded use
Physician’s designee may obtain dataPhysician dispensing reported drugs from office must enter data into OARRSRestricted dosage units furnished per month by prescriberPhysician dispensing of reported drugs limited to a 72 hour emergency supply
25

HB 93 April 2012 expanded use of OARRS:
Wholesalers must enter all salesPenalties for abuse/ misuse of OARRSLicensing boards must develop rules governing the use of OARRs by their licensees OSMA, OSBP, etcCoroners must report deaths
26

HB 93 April 2012 expanded required use of OARRS: Medical Board Rule
4731-11-11
Mandated OSMA to develop rules for when physicians must access OARRS:
1. If patient exhibiting signs of drug abuse or addiction
2. Treatment of patient with reported drugs >12wks
3. At least annually if using reported drugs.12wks or more per year
27

HB 93 expanded use of OARRS: Medical Board Rule
4731-11-11 FAQ Document
Signs of abuse or addiction:Patient with un expected drug screen Forging/adulterating script
Stealing/borrowing medsHistory of illegal drug use/ conviction
28

Signs of Abuse/Misuse –Mandate OARRS Check:
- Selling drugs- Increasing the dose without permission- Multiple prescribers identified/suspected- Family member, friend or other professional
raises issue of patieint abuse/misuse
29

“Red Flags” –Suggested to check OARxRS but not
mandated:
History of chemical abuse/addictionPatient appears sedated /impaired in officeLoosing scripts or requesting early refillsED visits for refillsSharing drugsRequesting drugs by name ???
30

OARxRSThe report is privileged health information (HIPPA), not a public record, not evidenceYou may not share the information with other professionals unless they use the same chartYou may show the patient the data but not give it to themYou must keep OARRS report in non reproducible part of chartYou may not use OARRS to screen employees or potential employees
31

OARxRS
Exemptions:
Prescribers of patients with a terminal illness
32

OARxRS is meant to be and is a useful tool in pain mangement!
OARRS can be a useful tool for initial or ongoing patient assessment
OARRS is just one more piece of the clinical assessment; it does not replace your medical judgment
33

Ohio Automated Rx Regulatory System: OARxRS
In 2011 :Ohio Population approximately 11million
Scripts in OARRS:46.9 million#of patients in OARRS: 5.7 million
Time to get report: 98% within 23 seconds5% 5mins -3hrs reports available 24/7 Lag time of 1-10 days from dispensing of
medication until report available
34

Signing up for OARxRSGoogle OARxRSHome page – “Register”
- registration takes about 15 minutes
More information – Questions??Danna E. Droz, J.D., R.Ph.PMP Administrator
614-466-4131 option 1oarrsadmin@ohiopmp./gov
35

Ohio’s Intractable (Chronic) Pain Law
Chapter 4731-21 Drug treatment of intractable pain Effective date: November 11, 1998Changed to “Chronic” in HB 93Currently under review with expected new rules to be developed by the Govenor’s Cabinet Opioid Action TeamHotly debated issue: will recommendations of the team be “guidelines” or “rules”? –
Should vs. Shall!
36

Ohio’s Intractable (Chronic) Pain Law
Current “Shalls” in the law:Initial evaluation documented in the reordMedical diagnosis establishedIndividualized treatment plan formulated and documentedAppropriate consultationSigned consent to treatment and agreement to conditions of prescribing
37

Ohio’s Intractable (Chronic) Pain Law
Patients shall be seen at appropriate intervalsDocumentation of effects of treatment on the functional capacity and efficacy of the treatmentMonitoring for compliance if needed ( drug screen, etc)Referral to addiction specialist if indicated
38

Ohio’s Intractable (Chronic) Pain Law
Exemptions : 4731-21-06Treatment of patients with a terminal illness
or treatment of pain associated with a progressive disease that in the normal course of progression may reasonably be expected to become terminal
39

Governor’s Opioid Action Team
Ohio Emergency and Acute Care Facility Prescribing Guidelines: Opioids and Other Controlled Substances (OOCS) These are guidelines, not rules: shouldand not shallDeveloped to assist ED physicians who are struggling to deal with the impact of chronic pain patients on the ED, as well as the ever present drug diverter and abuser
40

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
OOCS for pain will be prescribed only after evaluation of patient and risk of addiction
OOCS should be given P.O., not IM/IV
No Rx if patient seen within the last month or had Rx from another prescriber within last month for the same problem
41

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
Meperidine ( Demerol) use discouragedED clinicians will not routinely provide replacement scripts for OOCS that were lost, stolen or destroyedReplacement doses of Suboxone, Subutex, or methadone will not be given for patients in treatment programs
42

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
Long acting or controlled release formulations such as oxycodone SR, fentanyl patches methadone will not be routinely provided
43

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
Prior to deciding whether or not to treat with an OOCS the ED clinician or the facility: Should access OARRSCheck a photo ID or photograph patient for the chartReserve the right to perform a drug screen
44

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
ED clinicians should consider contacting the physician who routinely prescribes for the patientRequest a Palliative Care or pain consult, or other appropriate subspecialty service Perform case management on patients repeatedly seen in ED
45

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
Request medical and prescription records from other hospitals/prescribersRequire that the patient sign a pain agreement outlining expectations of the ED department regarding the patient’s use of the OOCSUse EMR to communicate with other providers regarding patient care
46

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
Limit the Rx of OOCS to a 3 day supply except in unusual circumstances
Discharge instructions to patients given an OOCS Rx should include information on addiction risk, dangers of misuse, appropriate storage/disposal of OOCS
47

Ohio Emergency and Acute Care Facility Prescribing Guidelines: OOCS
ED and other facilities should maintain a list of clinics that provide primary care services and pain managementED and other facilities should display signage that reflects these prescribing guidelines and states the facility position regarding the prescribing of opioids and other controlled substances
48

Ohio Emergency and Acute Care Facility Prescribing Guidelines
Endorsed by:OOAOSMAOHOOhio Pharmacists AssociationOhio Chapter of the American College of Emergency PhysiciansOhio Association of Health PlansOhio Association of Physician AssistantsOhio BWC
49

8 Steps to Safe and Successful Pain Management
Step 1: Reframing the discussion –realistic expectationsStep 2: Utilizing a biopsychosocial model of pain management vs. the biomedical modelStep 3 Evaluation of the pain patientStep 4 Evaluation of the pain
50

Steps for Successful Pain Management
Step 5 Multimodal pain managementStep 6 Initiating opioid therapy when neededStep 7 Monitoring ongoing opioid therapyStep 8 Celebrate Success!
Extracted in part from Scott Fish: Responsible Opioid Prescribing
51

Step 1: Set Realistic Expectations
52
• A good outcome is achieved if the patient’s pain is reduced by 30 points on a 100 point scale, or by 2-3 /10
• Success should be measured in terms of improvement in lifestyle and function
• Set realistic expectations from the start: what is it that the patient would like to do that pain is preventing? Take mini steps toward achieving goal

Step 2: Utilize a Biopsychosocial Model vs a Biomedical Model of Pain Management
53
What does this mean?
Treat the patient instead of the pain!

When evaluating patients do so in terms of the affects of the pain on lifestyle, function, productivity: ask the patient:“How does this pain affect you – What can’t you do that you want to do? What can’t you do that you need to do?”
54

Assess the “meaning of the pain”to the patient:
Secondary gain or alienation from family, work or society may be hindering patient’s response to treatment
Patients living with pain have depression that is chemically medicated – depression is a proven biologic outcome of chronic pain - address openly with the patient!
assure the patient that you don’t think the pain is “all in his head”, but that addressing depression will be part of treatment plan
55

Assess sleep, activity, sexual response in relation to the pain; fatigue will increase pain, pain is worse at night
Actualize patients’ personal satisfaction in their ability to manage their pain’s psychosocial implications: reward gains in function and activity
Utilize interdisciplinary case management as early as possible: pain psychologists, PT, OT, vocational counselors
56

Tools for assessing pain in terms of function and lifestyle:
Pain / disability indexSickness Impact Scale
Documentation of improvement in function and activity as a result of using opioids justifies their use for reviewers
57

Step 3: Evaluation of the Chronic Pain Patient
• Requires time to evaluate the patient as well as the pain and to build a trusting relationship
• Requires utilizing staff and assessment tools when appropriate to evaluate the patient and the patient’s appropriateness for treatment
58

Patient Assessment
One out of every ten patients with no history of addiction is at risk for opioid addictionGenetic incidence similar to prevalence for alcohol addictionEducate patients and families about genetic risk (use handouts from ODADAS) and take a history of family addictions
59

Tools to assess risk for addiction
SBIRTOpioid Risk Tool (ORT)D.I.R.E. Score: patient selection for chronic opioid useCAGE-AID – alcohol assessment tool adapted to include drugsSOAPP-R –SODQ
60

Patient Assessment
Use OARxRSMandated Use:
1. If patient exhibiting signs of drug abuse or addiction
2. Treatment of patient with reported drugs >12wks3. At least annually if using reported drugs.12wks
61

Patient Assessment
“Red Flags”: optional use of OARxRS
OARxRS can be a useful tool for initial or ongoing patient assessmentDocument the use of tools in your medical record – may be mandated in state guidelinesPatients with terminal illness/ illness that may become terminal are exempted from OARxRS
62

Patient Assessment
Physical examination of the patient: never prescribe an opioid for a patient without documenting a physical exam
4731-21-02, O.A.C.
63

Step 4: Pain Assessment
In order to manage pain, the prescriber must be able to determine the anatomical origins of the pain; somatic , visceral, neuropathic
Detailed history and listening to your patient’s describers of the pain will reveal its anatomical origin
64

Patients with chronic pain will have more than one type of pain –
Ability to control pain depends on choosing the correct medication for each type of pain the patient describes
65

Mnemonic for Pain Assessment
P – palliating/precipitatingQ – quality of the painR – region/radiationS – severityT – temporal relationshipsU – impact of the pain on you
66

67
Anatomical Origins of Pain
Somatic pain
Visceral pain
Neuropathic pain
Complex neuronal pain
67

Anatomical Origins of Pain: What is Chronic pain??
Complex Neuronal Pain – Chronic painWhen patients live with pain, the brain’s
response to the pain changes d/t changes in neurotransmitters and neuroreceptors
Down regulation of Mu receptors (opioid receptors) up regulation of Delta, P, NMDA receptors (neuropathic receptors)
Therefore, in chronic pain, patients are less receptive to opioids and more receptive to neuropathic pain medications 68

Complex Neuronal Pain
Primary neuronal deathLoss of myelin sheathCentral sensitizationChanges in neurotransmitters, neuroreceptors
Opioid receptor down-regulationincreased importance of NMDA receptors, glutamate
69

Acute vs Chronic Pain
Acute pain is very easy to localize and describeUp regulation of the sympathetic nervous system leads to physiologic response of the body that can be measured: increase in BP, pulse, respirations, anxietyIn chronic pain: less response of the SNSPain descriptors become more vague and pain more diffuse, patients use neuropathic pain descriptors and have flat affects
70

Step 4: Develop a treatment plan
Use a biopsychosocial model of pain management: integrative (integrative) medicineSelect appropriate medications that address the patients multifaceted painEmphasize achievable goals directed at function that are taken in “baby steps”The sooner, in the course of the illness, the function is addressed and the patient increases activity, the more likely the treatment will be successful
71

Develop a Treatment Plan
Discuss the plan with the patient/familyEmphasize lifestyleSet the rules – consider a pain contract/ patient agreement, informed consent?When you see a patient in acute pain, get the patient moving as quickly as possible!
72

Step 5:Utilize Multimodal Pain Management
Physicians often equate pain management with opioids or interventions by pain specialists.
Good pain management is “multimodal”and can be accomplished in the office of the attending physician.
73

Multimodal Medication Therapy
Pure opioids, weak opioids and Adjuvant medications chosen to address the specific aspects of the patients “total pain”including psychosocial aspects of the pain (depression, sleep, anxiety)Initially treat without an opioid if possible, or with limited quantities of opioids
74

Analgesic Classes
Non opioidsWeak opioidsPure opioidsAdjuvants
75

What are Adjuvants in pain management?
Adjuvants may be analgesics themselves, or medications not commonly considered to be analgesics, such as anticonvulsants, anxiolytics, and antidepressantsEnhance or augment the main analgesicReduce the total opioid load if an opioid is neededAddress different aspects of the patient’s total pain
76

77
Adjuvant Medications…NSAIDS:
Examples: Naproxen, Motrin, Celebrex, Toradol *relieves bone, muscle, or joint pain * often better than Morphine for bone pain
Antidepressants:Tricyclics – Examples: Elavil, Doxepin
*increases endomorphins*helps neuropathic pain*may provide appetite stimulation, mood elevation
SSRIs – Examples: Paxil, Prozac, Zoloft*improve sleep, mood appetite*have not been shown to help neuropathic pain
SNRI – Example: duloxetine (Cymbals),venlafaxine
Topical Agents:capsaicin, lidocaine patch, EMLA

78
Adjuvant Medications…
Anticonvulsants:Examples: Tegretol, Dilantin, Neurontin
*relieves neuropathic pain
Steroids:Examples: Decadron, Prednisone
* reduces swelling in brain or visceral lesion* improves appetite* may improve mood* relieves neuropathic pain* serves as an anti-inflammatory if NSAIDs are contraindicated to reduce joint or bone pain
Antianxiety Medications:Examples: Ativan, Xanax, Haldol
* treats agitation, restlessness, extremely helpful in dyspnea, COPD, terminal delirium
* important adjuvant in controlling pain of all etiologies

79
Adjuvant Medications…
GABA Agonists* Baclofen
NMDA Antagonists* Dextromethorphan, ketamine
Scopolamine: Patch or SQ, Levsin PO, Atropine PO or SQ* treats terminal secretions, relieves death rattle, may help
stomach, colic spasms* motion induced nausea, dizziness
Bisphosphates, Miacalcin, Arida, Zometa* bone pain* may retard bone fracture* treat hyperkalemia* hypercalcemia

80
Adjuvant Medications…Alpha 2 –adrenergic agonists:
* Clonidine
Neuroleptics* olanzapine* Haloperidol* mirtazapine
Muscle Relaxants – Flexeril, Baclofen
Adjuvants may be analgesics themselves, or medications not commonly considered to be analgesics, such as anticonvulsants, anxiolytics, and antidepressants

81
The Concept of Total PainTumor – 60% of pain directly related to tumor
19-28% of pain is secondary to side effects of treatment
Pain from debilitation, malnutrition (bedsores)
Pre-existing Pain
Brain Mets
Radiation
Surgery
Chemo
Bone MetsVisceral Mets
Total PainOncology

82
End Stage Cardiac Disease
Pleural Effusion
Peripheral Edema
Cardiac Cachexia Wasting,
Bedsores, Debilitation
Dyspnea
Ischemic Coronary Artery Disease
Aortic Insufficiency –Chest Pressure
Co-MorbiditiesIschemic Bowel Peripheral Vascular DiseaseRenal NeuropathiesOsteoporosisVenous Insufficiency
Medication Induced Hypokalemia Hyponatremia
Total Pain In
Cardiac Disease
Acute/Chronic Angina
Depression
Chest Wall Pain

83
Chronic Obstructive Pulmonary Disease
Chronic anxiety, depression
Wasting, cachexia,Chronic debilitation, bedsores
Osteoporosis
Chest wall pain, chronic pleuritis
Chronic racking cough
RHF – Chronic tissue edema hepatomegaly
Peripheral vascular diseaseVenous insufficiency
Total Pain in
COPD
Pain in COPD is a combination of the pathophysiology of the primary process and the multiple common co-morbidities
Pain from pre-existing etiologies
Tachypnea

84
WHO 3-step Ladder
1 mild
2 moderate
ASA
Acetaminophen
NSAIDS
+ Adjuvants
3 severe
A/Codeine
A/Hydrocodone
A/Oxycodone
A.Dihydrocodeine
Tramadol
+ Adjuvants
Morphine
Hydromorphone
Methadone
Levorphanol
Fentanyl
Oxycodone
+ Adjuvants
< 4
> 4 - < 7
> 7

Treatment of Acute Pain
Failure to treat acute pain preemptively can lead to development of chronic pain such as complex regional pain (RSD)Plan for successful management rather than reacting to failed treatment!
85

Treatment of Acute Pain Case Study
Case scenario: middle aged patient with ankle pain comes in the office on a crutch after an injury playing basketball. Patient rates his pain as a “6/10.” No history of opioid use or drug/alcohol abuse
86

Treatment of Acute Pain – case study:
Screen for abuse potential using appropriate tools
Check OARxRS if any “Red Flags” or just because “who can tell!”
Physical exam is compatible with the history; 2nd degree ankle sprain
87

Treatment of Acute pain
Goal of treatment is to reduce the pain to the point that patient can remain functional and able to say that he can move about comfortably with minimal pain and is able to sleep through the night
One recipe: Naproxen 500mg 2xday p.o RTC for 10 days, hydrocodone 5/500 Tab 1 q4hrs prn p.o. for severe pain breakthru – dispense 16 pills gabapentin 200mg qhs p.o to address the neuropathic component of the pain ..
88

Treatment of Acute Pain
Patient advised to call you ASAP if not meeting the expectations/goals described above
See patient back in the office in one week - prescribe very few if any opioids and start PT/OT – set goals for return to activity
89

Treatment of Acute pain
This is “multimodal” because instead of using only the opioid/ acetaminophen combination you are also using an anti-inflammatory for the somatic pain and gabapentin for the neuropathic component of the pain. You are scheduling the naproxen and using the hydrocodone/acet prn so that you are giving both RTC continuous relief but sparing the opioid use.
90

Treatment of Chronic Non Malignant Pain
Case scenario: Beth has chronic pancreatitis and a pancreatic pseduo cyst. She has had repeated surgeries and has abdominal adhesions. Beth is also diabetic and has significant peripheral neuropathy. She is frequently hospitalized, losing weight, depressed and sleeps poorly. Beth sees several specialists but looks to you to manage her pain.
91

Treatment of Chronic Pain
Does Beth qualify as having “intractable pain” under the guidelines of Ohio SHB 187, “The Intractable Pain Law”?
Does Beth have pathology that could result in a terminal condition?
If so, then you and Beth are excluded from the regulatory scrutiny of pain contracts, urine screens, pill counts.
92

Treatment of Chronic Pain
Document heavily, particularly the beneficial effects of your treatment on Beth’s lifestyle and function
93

Treatment of Chronic PainOne multimodal recipe for Beth:
Beth has been on oxy/IR 10 mg 6xday for several months, now her pain is worse and she wakes up at night with leg pain and numbness. Convert the oxy IR to oxycodone SR, 20mg 2x day; and continue the oxycodone IR for “break thru pain” every 2-4 hours prn, Start gabapentin for the neuropathic pain in her legs starting with 100mg 3xday, gradually titrate to comfort by increasing the dose in tolerated increments until acceptable relief of neuropathy pain is achieved, taking into consideration Beth’s GFRSRNI for neuropathic pain and depression and sleep Anticholangeric for bowel spasms
94

Treatment of Chronic Pain
Use of the gabapentin will not only help the diabetic neuropathy, it will also potentiate the effect of the opioid and address the “complex neuronal pain”which develops when pain becomes chronicUse of the adjuvants reduces the total mgs of opioid needed to provide comfort
95

Step 6: Initiating opioid therapy for Chronic pain when necessary
Criteria: goals without opioids have been disappointing, reason to believe they are indicated (pathology involved, physical exam, pt’s need for relief in order to obtain function)Assessment of patient, screening indicates patient is appropriate candidate for opioid therapyA pain contract, patient agreement, consent to treat as appropriate are in place and documented
96

Initiating opioid therapy for chronic pain
Pretreatment urine screening if appropriate is complete and documentedEducate the patient about the possible side effects of opioids and how to manage: sedation, confusion, itching ,nausea hypogonadism, secondary osteoporosisInitiate a “ trial period’ with set goals and expectations of the patient’s functionEstablish a plan to taper and d/c opioids when appropriate
97

Initiating Opioid therapy
Discuss safe storage of medications and review concerns about diversion in the household by friends and relatives
Discuss safe disposal of unused medications – office handout on these subjects
98

Step 7:Monitoring ongoing Opioid Therapy
Utilize “Universal Precautions for Pain”Monitoring plan is in place and initiated prior to start of therapyComply with established and evolving state and federal regulations Comply with OARxRsDocument monitoring, compliance on part of patient, improvement in function, achievement in goals especially work related
99

Monitoring ongoing therapy
Continue all integrative medicine as appropriateContinue to use a biopsychosocial model of patient and family managementPositive reinforcement of patients improved coping and lifestyle skills
100

Step 8: Celebrate Success!!
Document the improvement in terms of sleep, function , ADLs, independence in the elderly
Taper and d/c opioids as patient’s overall condition and coping skills improve
Positive feed back to patient, family and staffHave ODADAS send you handouts, signs for office and update info regularly
101

Safe and effective pain management
Trust your real patients, and if you don’t, don’t treatHelp your real patients who have substance use problems success is improvement in function/ productivityUse adjuvants to treat complex painPrescribe opioids in appropriate quantities and address issues of diversion/ drug disposal with patients.
102

References
Fishman, Scott M. Responsible Opioid Prescribing, 2nd edition, Waterford Life Sciences, 2012 pp 1-129Institute of Medicine: Relieving Pain in America, a Blueprint for transforming prevention, care, education and research. Report Brief, June 2011APS- AAPM Clinical Guidelines for Opioid Use in Chronic Non Cancer Pain 2009
103

References
AAFP Monograph: Balancing Clinical and Risk Management Considerations for Chronic Pain Patients on Opioid Therapy, October, 2008Office of National Drug Control Policy Action Plan epidemic: Responding to America’s Prescription Drug Abuse Crisis, 2011Veteran’s Affairs/Department of Defense; Clinical Practice Guidelines Summary Management of Opioid Therapy for Chronic Pain, 2010
104