Pages - EduLancheAnswers 1. IMAGE-BASED QUESTIONS 1-18 2. IMAGING SIGNS IN RADIOLOGY 19-38 3....
17
Transcript of Pages - EduLancheAnswers 1. IMAGE-BASED QUESTIONS 1-18 2. IMAGING SIGNS IN RADIOLOGY 19-38 3....


Answers
1. IMAGE-BASED QUESTIONS 1-18
2. IMAGING SIGNS IN RADIOLOGY 19-38
3. GENERAL RADIOLOGY 39-72 � X-rays 40 � Computed Tomography 47 � Ultrasound Imaging 52 � MRI Basics 58 � Contrast Media in Radiology 65 � Multiple Choice Questions 70 � Explanations to Questions 72
4. RESPIRATORY SYSTEM 73-112 � Normal Findings on a Chest Radiograph 74 � Silhouette Sign and Lung Infections 79 � Pleural Abnormalities 84 � Lobar Collapse and Airway Disorders 89 � Mediastinum 93 � Lung Tumors 97 � HRCT Thorax 100 � Miscellaneous Topics 102 � Multiple Choice Questions 106 � Explanations to Questions 112
5. CARDIAC IMAGING 113-124 � Imaging in Congenital Heart Disease 114 � Imaging in Acquired Heart Disease 117 � Imaging in Pulmonary and Aortic Diseases 119 � Multiple Choice Questions 121 � Explanations to Questions 124
6. GASTRO-INTESTINAL TRACK IMAGING 125-158 � Peritoneal Abnormalities 126 � Imaging in Foregut 129 � Small and Large Bowel Abnormalities 132 � Imaging in Hepatobiliary System 140 � Pancreatic Imaging 145 � Miscellaneous Abdominal Imaging 147 � Multiple Choice Questions 150 � Explanations to Questions 156
7. GENITOURINARY TRACT IMAGING 159-180 � Urolithiasis Imaging 160 � Renal Parenchymal Abnormalities Including
Infections 161 � Renal Masses 163 � Congenital Anomalies of Genitourinary System 165 � Prostate Imaging 167 � Miscellaneous GUT 168
� Male Reproductive System 171 � Gynecologic Imaging 172 � Multiple Choice Questions 175 � Explanations to Questions 180
8. MUSCULOSKELETAL IMAGING 181-209 � Bone and Joint Infection 182 � Bone Tumors 184 � Arthritis 189 � Systemic Bone Disorders 194 � Skeletal Dysplasia 198 � Miscellaneous Musculoskeletal Imaging 201 � Multiple Choice Questions 202 � Explanations to Questions 208
9. CENTRAL NERVOUS SYSTEM IMAGING 211-246 � Stroke Imaging 212 � Head Injury 219 � CNS Infections 223 � CNS Neoplasms 227 � White Matter Diseases 231 � Phakomatoses 232 � Miscellaneous Topics 234 � Multiple Choice Questions 238 � Explanations to Questions 245
10. WOMEN’S IMAGING 247-262 � Breast Imaging 248 � Obstetric Imaging 252 � Multiple Choice Questions 259 � Explanations to Questions 262
11. RADIONUCLIDE IMAGING AND RADIOTHERAPY 263-280 � Radionuclide Imaging 264 � Radiotherapy 271 � Multiple Choice Questions 278
12. HIGH YIELD TOPICS 281-306 � Tuberculosis 282 � Hydatid Cyst 287 � Skeletal Trauma 290 � Radiation Exposure, Protection and Guidelines 301 � Multiple Choice Questions 303 � Explanations to Questions 306
13. NORMAL IMAGING ATLAS—BRAIN, CHEST AND ABDOMEN 307-318 � Brain Sectional Anatomy 308 � CT Chest Anatomy 312 � CT Anatomy Abdomen 316
APPENDIX: Scientists and Important Discoveries in Radiology 319
Radiology – though a distinct specialty now – is indeed inseparable from the clinical sciences. Hence, we have taken some extra effort and designed this book in a particular manner; grouping together related conditions in a logical order. This topic-wise table of contents will not only help you cruise through this book when you study Radiology, but also when you study your other clinical subjects. Keep this book handy when you study Medicine, Surgery, Pediatrics and OBG and easily find a specific condition in this table – complete your preparation of any topic by going through its imaging findings then-and-there. Welcome to what we call the – Integrated learning experience!
Contents
Sample
Pages
of R
adiol
ogy,
2/e

Answers
1. B. Cerebellum 2. D. Barium meal follow-through
3. B. Ischemia 4. C. Lacunar infarct
5. D. Blow-out fracture 6. C. Chemotherapy is treatment…
1. Identify the structure marked in the image:
A. Cerebrum B. Cerebellum C. Brainstem D. Corpus callosum 2. A patient presented with recurrent abdominal pain.
Identify the investigation in this image:
A. Barium meal B. Barium swallow C. Barium enema D. Barium meal follow-through 3. A 67-year-old hypertensive and diabetic male presents
with left sided hemiplegia. Diagnosis based on this CT is:
A. Hypertensive bleed B. Ischemia C. SAH D. Lacunar Infarct
4. Diagnosis based on this image is:
A. Basal ganglia hemorrhage B. Intraventricular bleed C. Lacunar infarct D. Multiple sclerosis 5. A patient presented with history of trauma followed by
periorbital swelling and diplopia. Diagnosis based on this CT image is:
A. Le fort fracture B. Fracture zygoma C. Tripod fracture D. Blow-out fracture 6. Incorrect statement regarding this condition:
A. Meta-epiphyseal location B. Eccentric location C. Chemotherapy is treatment of choice D. Has distinct margins
Recent Pattern Questions 2019
Sample
Pages
of R
adiol
ogy,
2/e

Con
cept
ual R
evie
w o
f Rad
iolo
gy
20
Imag
ing
Sign
s in
Rad
iolo
gy
Respiratory System and Cardiac Imaging
1. Split Pleura Sign
Refers to the enhancing appearance of both visceral and parietal pleura on CE-CT seen in empyema. Helps to distinguish it from lung abscess. An abscess is usually round – oval and within the lungs. Non inflamed pleura in simple pleural effusion does not enhance like empyema.
Imaging Signs in Radiology
2. Pleural Meniscus Sign Homogenous opacity in the left lower zone with an upward ill defined concavity – look like a Meniscus on the surface of water in a test-tube/capillary tube. Classical of in pleural effusion. A clear horizontal air-fluid levelQ is seen in Hydro-pneumothorax.
3. Visceral Pleural Line and Deep Sulcus Sign Visualization of the sharp visceral pleural surface (Blue arrow) due to presence of air in pleural space – Differential radiographic density theoryQ – in PneumothoraxQ.Unusually deep ipsilateral costo-phrenic angle (yellow arrow) seen in Pneumothorax due to mass effect on the dome of diaphragm pushing it downwards.Other signs seen in Pneumothorax include – Hyperlucent hemithorax with absent vascular markingsQ and Mediastinal shift towards opposite sideQ.
4. Golden S Sign Named after R. Golden - refers to the typical S shape of Horizontal fissure seen in right upper lobe collapseQ (mostly due to central hilar mass). The lateral concavity (yellow arrow) is seen due to RUL collapse as it pulls the horizontal fissure upwards whereas the medial convexity (blue arrow) is seen due to horizontal fissure outlining the centrally located mass lesion. Other sign seen in RUL collapse is Juxta phrenic peak signQ.
One of the most fascinating things about studying Radiology is the highly imaginative and exciting world of Named/Eponymous signs/appearances. When your study schedule becomes long, tedious and tiring….it is these signs that can really help us get refreshed a bit! The language of radiology is rich with descriptions of imaging findings, often metaphorical, which are used commonly in the day-to-day practice. These “classic signs” give us confidence in our diagnosis. Use this section as a refresher. When you get tired going through your other subjects/systems….come to these pages….have a look at these classical images and be amazed! Each of these images is a SPOTTER and will help you solve numerous MCQs in your exams. Let’s Rock Radiology!
Sample
Pages
of R
adiol
ogy,
2/e

Mul
tiple
Cho
ice
Que
stio
ns
70
Con
cept
ual R
evie
w o
f Rad
iolo
gy X-rays1. X-rays were discovered by? A. Ian Donald B. Godfrey Hounsfield C. Wilhelm Röntgen D. Marie curie2. International radiology day is celebrated on? A. 1st May B. 22nd August C. 8th November D. 1st December3. The main difference between X-rays and Light is? (AI 2010) A. Energy B. Mass C. Speed D. Type of wave4. X-rays are produced when? (AIIMS NOV 2002) A. Electron beam strikes nucleus. B. Electron beam strikes anode. C. Electron beam reacts with electromagnetic field. D. Electron beam strikes cathode.5. Atomic number of Tungsten? (JIPMER May 2016) A. 42 B. 181 C. 74 D. 826. Which of the following X-ray interaction is the most common
of all X-ray interactions and is responsible for almost all scatter radiation?
A. Photo-electric effect B. Compton effect C. Pair production D. Photodisintegration7. Atoms with same mass number and atomic number but with
different nuclear energies are called as? (JIPMER 2016) A. Isomers B. Isotones C. Isobars D. Isotopes8. Contrast of a radiographic image is determined by? A. kVp B. mAs C. Both D. None9. Which of the following is/are present inside nucleus of an
atom? (PGI May 2018) A. Electron B. Proton C. Neutron D. Photon E. None of the above10. Unit of absorbed radiation is/are? (PGI NOV 2017) A. Rem B. Gray C. Curie D. Rad E. Bequeral11. Which of the following statements about “Stochastic effects”
of radiation is true? A. Severity of effect is a function of dose B. Probability of effect is a function of dose C. It has a threshold D. Erythema and cataract are common examples12. Mammography uses? (JIPMER May 2016) A. Continuous spectrum radiation/Bremsstrahlung B. Characteristic radiation C. Electrons D. Gamma rays13. Acute Hematological syndrome occurs at an exposure of? A. 2 Gy B. 10 Gy C. 20 Gy D. 50 Gy14. SI unit of Radiation exposure is? (JIPMER May 2016) A. Joule/Kg B. Rad C. Roentgen D. Coulomb/kg
15. The ALARA principle applies to what aspect of Radiology? A. Contrast media safety B. Quality control and assurance C. Radiation safety D. Workplace ethics16. The 10 day rule applies to? A. Children B. Young females C. Elderly males D. Elderly females
Computed Tomography17. The first generation CT scanner developed by Sir Godfrey
Hounsfield was what type? A. Translate-Rotate B. Rotate-Rotate C. Rotate—Fixed D. Electron beam type18. Continuous helical acquisition of data in CT scanners, with
360 degree continuous rotation of the gantry was possible because of introduction of?
A. Advanced X-ray tubes B. Slip-ring technology C. Spring technique D. Mobile detectors19. CT Number of water and bones respectively?
(JIPMER May 2016) A. 100 and 0 B. 0 and - 1000 C. 0 and + 1000 D. + 1000 and - 10020. Walls of CT scanner room are coated with? (AI 2010) A. Lead B. Glass C. Tungsten D. Iron21. Calcification is best detected by? A. USG B. CT C. MRI D. Fluoroscopy22. 128 slice CT scanner is a? A. 1st generation scanner B. 2nd generation scanner C. Multi-detector CT scanner D. Portable CT scanner23. Which of the following appears hypodense on CT? A. Acute blood B. Bone C. Calcification D. CSF24. CTDI represents? A. CT Densitometry index B. CT Dose index C. CT Duplication index D. CT Detection index25. Mean Transit Time (MTT) is measured in? A. CT Angiography B. HRCT C. Perfusion CT D. CT Densitometry26. Q-CT is used for? A. Cardiac assessment B. Interstitial lung disease C. Bone mineral density measurement D. Brain perfusion
Ultrasound Imaging27. Harmonic imaging is used in? A. USG B. CT C. MRCP D. Nuclear imaging28. In color Doppler the Intensity of red/blue color is determined by? A. Direction if flow B. Amount of flow C. Velocity of flow D. Temperature29. Piezoelectric effect is used in which modality? A. X-ray diffraction B. USG C. NMR D. DEXA scan
Multiple Choice Questions
Sample
Pages
of R
adiol
ogy,
2/e
Expl
anat
ions
to Q
uest
ions
72
Con
cept
ual R
evie
w o
f Rad
iolo
gy
62. Heparinization is required to prevent the risk of thrombo-embolic phenomena when using?
A. High osmolar contrast B. Low osmolar contrast C. Gadolinium D. USG contrast63. All of the following are negative contrast media except? A. Air B. Water C. Mannitol D. Barium64. Absolute contraindication for use of Barium is? A. Obstruction B. Hernia C. Perforation D. Ascites65. Most commonly used Barium compound is? A. BaSO4 B. BaPO4 C. BaS D. BaCl66. Which of the following has the lowest Iodine—Particle ratio? A. Ionic monomers B. Ionic dimers C. Non-ionic monomers D. Non-ionic dimers 67. USG Contrast media are? A. Gel microbubbles B. Air microbubbles C. Nano-colloid particles D. None of above68. Most important risk factor for development of CIN is? A. Elderly age B. Pre-existing CKD C. Diabetes mellitus D. Anemia69. Best preventive strategy for CIN is? A. Precontrast hydration B. N-Acetyl cysteine C. Bicarbonates D. Statins70. Markers of CIN include? A. Serum Cystatin C B. Serum creatinine C. eGFR D. All of above
71. Gadolinium is? A. Ferromagnetic B. Diamagnetic C. Paramagnetic D. Supermagnetic72. NSF stands for? A. Nephrogenic sodium failure B. Nephrogenic systemic fibrosis C. Nephrogenic salt failure D. Nephrogenic superficial fibrosis73. Most common contrast agent associated with NSF is? A. Gadopentetate B. Gadodiamide C. GadoDTPA D. Gadovistate
Answers 1. C2. C3. A4. B5. C6. B7. A8. C9. B,C
10. B,D11. B12. B13. A
14. D15. C16. B17. A18. B19. C20. A21. B22. C23. D24. B25. C26. C
27. A28. C29. B30. B31. C32. C33. B34. C35. B36. B37. D38. D39. B
40. B41. A42. C43. D44. C45. B46. D47. A,B, C,D48. B49. A,B, C50. D
51. D52. C53. D54. A55. C56. B57. B58. C59. A60. D61. D62. B63. D
64. C65. A66. A67. B68. B69. A70. D71. C72. B73. B
3. Both light and X rays are electromagnetic radiation and thus have same speed and type of wave. Being energies they do not have mass and hence cannot differ in terms of mass. They however have differing energies and frequencies.
12. In mammography we need good differentiation of low contrast structures and very high spatial resolution for micro-calcifications
Hence we use material that produces Characteristic x-rays with energies of 17-20 keV (20-30 keV for larger breasts) to produce the best contrast.
The commonly used material is Molybdenum (characteristic X-rays at 17.5 and 19.6 keV). Lower energy photons have a higher probability of interacting with matter and, therefore, produces better contrast. In mammography characteristic radiation forms 80% of the beam.
23. Out of the given options CSF which has water like composition appears hypodense while rest all options will appear as hyperdense. This density is measured with respect to density of gray matter in brain and that of skeletal muscles in rest of the body.
26. Q-CT stands for quantitative CT scan and is a non invasive technology to measure bone mineral density.
27. Harmonic imaging is an advancement in ultrasound technology where only the harmonic sets of images are used for image creation resulting in a better quality image.
28. Assignment of color to frequency shifts is usually based on direction (for example, red for Doppler shifts towards the
ultrasound beam and blue for shifts away from it) and magnitude (different color hues or lighter saturation for higher frequency shifts). Since the frequency shift are inturn determined by the velocity of blood flow the best answer here would be Velocity.
53. Magnets used for MRI are of three types: permanent, resistive and superconductive. These days almost all higher strength magnets are superconductive magnets. Both permanent and resistive MRI scanners are limited to low-field applications, primarily open MRI and extremity scanners. These magnets are useful for claustrophobic patients.
54. Hydrogen has the highest gyromagnetic ratio and is abundantly seen in the human body and is hence used for MR imaging.
58. In esophageal perforation there is risk of mediastinitis while performing any contrast study. Here an iodinated contrast is preferred and amongst ionic and non ionic the latter one are preferred for less risk of aspiration pneumonia
60. Low osmolar contrast has actually osmolarity similar to human blood and thus exert no extra osmolar load on kidneys and thus considered to be least nephrotoxic of all.
61. Myelography consists of either subarachnoid or intra thecal administration of contrast.
64. Administration of barium in a case of perforation will result in dreaded complication of barium(chemical) peritonitis – it is absolute contra-indication for use of barium.
Explanations to Questions
Sample
Pages
of R
adiol
ogy,
2/e

Norm
al F
indi
ngs
on a
Che
st R
adio
grap
h
78
Con
cept
ual R
evie
w o
f Rad
iolo
gy
INCIDENTAL FINDINGS AND NORMAL VARIANTS ON A CXR
Before we jump into studying abnormalities on a CXR, let us have a look at a few interesting incidental findings and normal variants. Though asymptomatic in most of the cases, recognizing these findings is clinically important as they may affect clinical decisions. Let us try and form a visual impression
Cervical Rib: Left sided cervical rib is seen here. These are supernumerary ribs arising from C7 vertebra. Though asymptomatic in most cases the may cause “Thoracic outlet syndrome” causing compression of Brachial plexus nerve roots or the Subclavian vessels
Situs Inversus: Always pay attention to the side marker (R/L) placed on the radiograph. Dextrocardia is isolated right sided cardiac apex. Here if you watch carefully the lucency of the gastric/fundic bubble is seen below the dome of diaphragm on right side–suggesting Situs Inversus
Left Mastectomy: Well defined soft tissue density is seen overlapping the lower part of the right hemithorax – suggestive of breast shadow. It is missing on the left side – suggests possibility of Left mastectomy. In an elderly female most of the times it suggests surgery for Carcinoma breast.
Scoliosis: Look beyond the chest and you can see that the dorsal spine has a lateral curvature – with a convexity towards right in its upper half and convexity towards left in lower part – suggests Scoliosis. Though idiopathic in most of the cases the diagnosis once established will help in the follow-up evaluation to determine if it is progressive.
Chilaiditi syndrome: Colon interposed between the liver and the right hemidiaphragm – is a cause of Pseudo-pneumoperitoneum. The colonic wall markings are seen here and hence this is not true pneumoperitoneum. Just the presence of this imaging findings is known as Chilaiditi sign. If the patient has pain along with it, it is termed as Chilaiditi syndrome
Azygos fissure: Most common accessory fissureQ. The portion of the lung medial to this fissure is called as Azygos lobeQ – is not a true lobeQ as it does not have its own bronchus. When left sided it contains an accessory hemiazygos vein
Sample
Pages
of R
adiol
ogy,
2/e
Stro
ke Im
agin
g
212
Con
cept
ual R
evie
w o
f Rad
iolo
gy
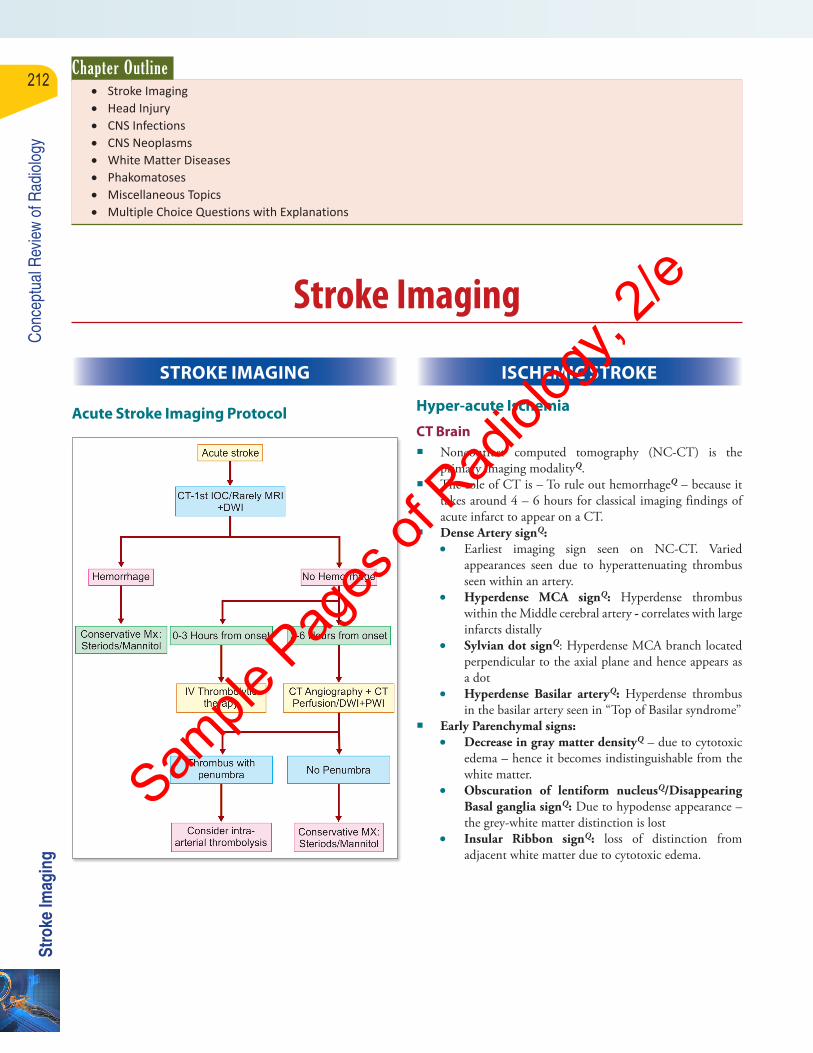
STROKE IMAGING
Acute Stroke Imaging Protocol
Stroke Imaging
ISCHEMIC STROKE
Hyper-acute Ischemia
CT Brain � Noncontrast computed tomography (NC-CT) is the
primary imaging modalityQ. � The role of CT is – To rule out hemorrhageQ – because it
takes around 4 – 6 hours for classical imaging findings of acute infarct to appear on a CT.
� Dense Artery signQ: • Earliest imaging sign seen on NC-CT. Varied
appearances seen due to hyperattenuating thrombus seen within an artery.
• Hyperdense MCA signQ: Hyperdense thrombus within the Middle cerebral artery - correlates with large infarcts distally
• Sylvian dot signQ: Hyperdense MCA branch located perpendicular to the axial plane and hence appears as a dot
• Hyperdense Basilar arteryQ: Hyperdense thrombus in the basilar artery seen in “Top of Basilar syndrome”
� Early Parenchymal signs: • Decrease in gray matter densityQ – due to cytotoxic
edema – hence it becomes indistinguishable from the white matter.
• Obscuration of lentiform nucleusQ/Disappearing Basal ganglia signQ: Due to hypodense appearance – the grey-white matter distinction is lost
• Insular Ribbon signQ: loss of distinction from adjacent white matter due to cytotoxic edema.
Chapter Outline • Stroke Imaging • Head Injury • CNS Infections • CNS Neoplasms • White Matter Diseases • Phakomatoses • Miscellaneous Topics • Multiple Choice Questions with Explanations
Sample
Pages
of R
adiol
ogy,
2/e

Brai
n Se
ctio
nal A
nato
my
310
Con
cept
ual R
evie
w o
f Rad
iolo
gy
Axial Section at the Level of Midbrain
Axial Section at the Level of Pons
Axial Section at the Level of Medulla
Sample
Pages
of R
adiol
ogy,
2/e

Remembering names and discoveries (that could be asked as MCQs)—is indeed a headache for students preparing for entrance examinations. Here is a short and relevant list in radiology. Each of these names is a legend of its own and has a very interesting story behind their respective discoveries/inventions. We are indebted to them for their pioneering work.
Wilhelm Röntgen • German physicist: Produced and detected X-rays (Röntgen rays) in 1895, an achievement that earned him the first Nobel Prize in Physics in 1901.
Antoine Henri Becquerel • French physicist and Nobel laureate: Discovered radioactivity.
Thomas Alva Edison • American inventor and businessman: Discovered that calcium tungstate screens produced brighter X-ray images than before and based on this he invented the first commercially available fluoroscope which enabled real-time moving images of internal structures of the body.
Frédéric Joliot-Curie and Irène Joliot-Curie (Daughter of Marie Curie)
• Artificially produced radionuclides (radioisotopes)—radioactive isotopes used in nuclear medicine for diagnosis, treatment, and research.
John Lawrence • American physicist and physician: Used phosphorus-32 (radioactive isotope of phosphorus) to treat leukemia.
David E. Kuhl • American scientist: Invented positron emission tomography (PET)—an imaging technique that produces a three-dimensional image of the inside of the body by using gamma rays.
Ian Donald • Scottish physician: Invented the ultrasound and tested with it, one year later, a pregnant woman.
Charles Dotter • American vascular radiologist: Known as the “Father of Interventional Radiology”; introduced image-guided medical procedures. For pioneering this technique he was nominated for the Nobel Prize in Physiology or Medicine in 1978.
Godfrey Hounsfield and Allan Cormack
• English electrical engineer and South African-American physicist respectively, invented CT scanner and shared the Nobel Prize for Medicine in 1979 for the invention of CT scanning. Computed tomography (CT) or computed axial tomography (CAT), is a medical imaging method employing computer processing which is used to generate a 3D images of the inside of an object from a large series of 2D X-ray images.
Felix Bloch and Edward Purcell • The Nobel Prize in Physics in 1952, which went to Felix Bloch and Edward Purcell, was for the development of nuclear magnetic resonance (NMR), the scientific principle behind MRI. However, for decades magnetic resonance was used mainly for studying the chemical structure of substances.
Raymond Vahan Damadian • Armenian-American medical practitioner and inventor: Built the first commercial MRI scanner— not awarded the Nobel Prize!
Paul Lauterbur and Peter Mansfield
• The Nobel Prize in Physiology or Medicine 2003 was awarded jointly to Paul C. Lauterbur and Sir Peter Mansfield “for their discoveries concerning magnetic resonance imaging”
• Lauterbur used the idea of Robert Gabillard (developed in his doctoral thesis, 1952) of introducing gradients in the magnetic field which allows for determining the origin of the radio waves emitted from the nuclei of the object of study. This spatial information allows two-dimensional pictures to be produced.
Marie and Pierre Curie • Marie and Pierre Curie were married scientists who discovered radium (on December 21, 1898). They announced their findings a week later, on the 28th of December.
• After forty-five months of additional work, the pair first isolated radioactive radium salts (from mineral pitchblende) at their Paris laboratory (on the 20th of April, 1902). The following year, they shared the Nobel Prize in science for their ground-breaking work.
• In 1910, with Debierne, she finally succeeded in isolating pure, metallic radium. For this achievement, she was the sole recipient of the 1911 Nobel Prize in Chemistry, making her the first person to win a second Nobel Prize.
Charles Dotter • Father of Interventional Radiology
Ernest Rutherford • Father of Nuclear Physics
John Caffey • Father of Pediatric Radiology
SCIENTISTS AND IMPORTANT DISCOVERIES IN RADIOLOGY
Appendix
Sample
Pages
of R
adiol
ogy,
2/e
X-ra
ys
40
Con
cept
ual R
evie
w o
f Rad
iolo
gy
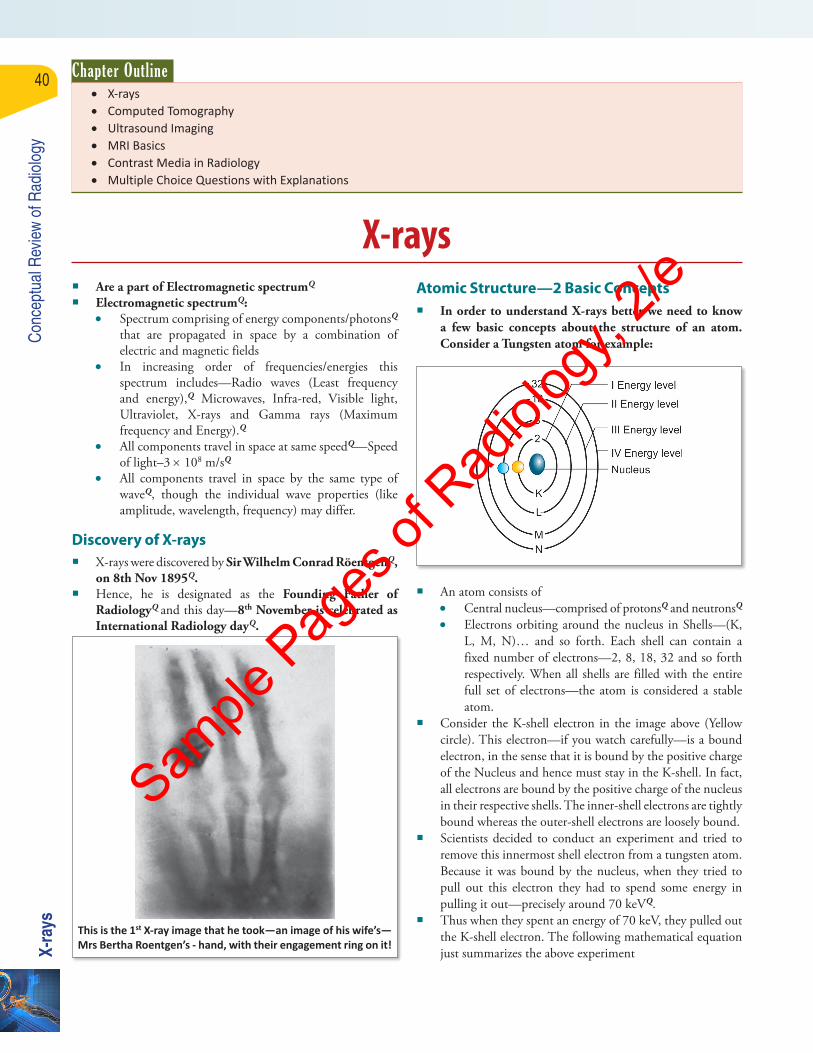
� Are a part of Electromagnetic spectrumQ
� Electromagnetic spectrumQ: • Spectrum comprising of energy components/photonsQ
that are propagated in space by a combination of electric and magnetic fields
• In increasing order of frequencies/energies this spectrum includes—Radio waves (Least frequency and energy),Q Microwaves, Infra-red, Visible light, Ultraviolet, X-rays and Gamma rays (Maximum frequency and Energy).Q
• All components travel in space at same speedQ—Speed of light–3 × 108 m/sQ
• All components travel in space by the same type of waveQ, though the individual wave properties (like amplitude, wavelength, frequency) may differ.
Discovery of X-rays � X-rays were discovered by Sir Wilhelm Conrad RöentgenQ,
on 8th Nov 1895Q. � Hence, he is designated as the Founding Father of
RadiologyQ and this day—8th November is celebrated as International Radiology dayQ.
This is the 1st X-ray image that he took—an image of his wife’s—Mrs Bertha Roentgen’s - hand, with their engagement ring on it!
Atomic Structure—2 Basic Concepts � In order to understand X-rays better we need to know
a few basic concepts about the structure of an atom. Consider a Tungsten atom for example:
� An atom consists of • Central nucleus—comprised of protonsQ and neutronsQ
• Electrons orbiting around the nucleus in Shells—(K, L, M, N)… and so forth. Each shell can contain a fixed number of electrons—2, 8, 18, 32 and so forth respectively. When all shells are filled with the entire full set of electrons—the atom is considered a stable atom.
� Consider the K-shell electron in the image above (Yellow circle). This electron—if you watch carefully—is a bound electron, in the sense that it is bound by the positive charge of the Nucleus and hence must stay in the K-shell. In fact, all electrons are bound by the positive charge of the nucleus in their respective shells. The inner-shell electrons are tightly bound whereas the outer-shell electrons are loosely bound.
� Scientists decided to conduct an experiment and tried to remove this innermost shell electron from a tungsten atom. Because it was bound by the nucleus, when they tried to pull out this electron they had to spend some energy in pulling it out—precisely around 70 keVQ.
� Thus when they spent an energy of 70 keV, they pulled out the K-shell electron. The following mathematical equation just summarizes the above experiment
X-rays
Chapter Outline • X-rays • Computed Tomography • Ultrasound Imaging • MRI Basics • Contrast Media in Radiology • Multiple Choice Questions with Explanations
Sample
Pages
of R
adiol
ogy,
2/e

X-ra
ys
41
Con
cept
ual R
evie
w o
f Rad
iolo
gy
X (initial energy of electron) + 70 keV = Free electron in space (has energy level of Zero)
SoX + 70 = 0
ThusX = –70
� X = –70 thus represents the initial energy level of the K-shell electron. It is also the energy level of the K shell itself.
� Remember that each and every shell in an atom has its own fixed energy level. All electrons in that shell are at exactly that energy level, which is in K shell of tungsten atom. The energy levels of all electrons is –70.
� If amount of energy required to remove K-shell electron was 70 keV, the amount of energy required to remove an L-shell electron would be less than that (as it is located away from the nucleus) and it was found to be 12 keV. Similarly for M shell it was further less at 2 keV.
Basic Concept 1
• Every shell in an atom has its own fixed Energy level associated with it.Q
• All electrons in that shell lie at that fixed Energy level• Energy levels for inner shells in a Tungsten atom are:
K - shell –70 keV
L - shell –12 keV
M - shell –2 keV
� Now look what happens after the removal of the K-shell electron. In the K-shell there is just one electron left. Because of a deficient electron, an electron void/empty space is created in innermost shell, thus making the atom unstable. The atom wants to become stable, but how? Think.
� What happens is that an outer shell electron jumps to the inner shell that is L-shell to K-shell. Subsequently outer shell electrons jump to the underlying inner shells and finally a free electron in space fills the outermost shell—making the atom stable again.
� Look at the jumping L shell electron— • L-shell energy level is –12 • K-shell energy level is –70
� Thus if an electron has to jump from L-shell (–12) to K-shell (–70) it will have to lose some energy so that it comes to an energy level of –70. Thus the energy lost is equal to the energy difference between the shells, here it is 58 keV.
Basic Concept 2
• Whenever an electron jumps from an outer shell to inner shell, it has to lose some of its energyQ
• The amount of energy lost is equal to the difference between the energy levels of the two shells
K-shell energy level –70 keVL-shell energy level –12 keVIf electron jumps from L shell to K shell it will have to release
58 keV of energy
These 2 concepts will help us understand X-ray better!
Tungsten Because Tungsten is a very important component of an X-ray tube, let us quickly review few important aspects:
� Symbol—WQ
� Atomic number—74Q
� Atomic mass—183.8Q
� Atomic mass number—184Q
� Classified as Transitional metalQ in the Periodic table
X-ray Tube Structure � These are Glass tubes with vacuum inside and 2 electrodes � Cathode:
• Made of Tungsten filament/coilQ—hence called as Cathode filament
• Given very high negative potentialQ � Anode: Given a very high positive potentialQ
• Conventional X-ray tubes—TungstenQ
• Recent X-ray tubes Tungsten (90%) + Rhenium (10%)Q MolybdenumQ
• Anode may be stationary or Rotating anode (better)
� Large potential difference—is applied across the anode and cathode—very important in production of X-rays
Production of X-rays It will be very easy to understand and remember using the following Flow chart:
Sample
Pages
of R
adiol
ogy,
2/e

X-ra
ys
42
Con
cept
ual R
evie
w o
f Rad
iolo
gy
Mechanism of Production of X-rays
1. Continuous spectrum radiation/BremsstrahlungQ: Based on Law of thermodynamics—Energy can never be created, nor can it be destroyed. But it can be converted from one form into another.
Thus kinetic energy of the electron—is converted into energy of X-rays
2. Characteristic spectrum radiation: Based on the 2 Basic concepts regarding structure of atom that we have discussed
Thus the amount of energy lost when an outer shell electron jumps to an inner shell is converted into energy of X-rays
Sample
Pages
of R
adiol
ogy,
2/e

Bone
Tum
ors
186
Con
cept
ual R
evie
w o
f Rad
iolo
gy
Periosteal ReactionIt is nonspecific reaction that occurs due to irritation of periosteum from underlying inflammatory or neoplastic process. The type of reactions follow a gradient from being suggestive of benign to a more malignant behavior. Rather than just mugging them up – let us look at actual images and try and form a visual impression.
Contd…Contd…
Matrix Mineralization
Chondroid matrix Osteoid matrix
Rings-and-arcs, popcorn, focal stippled or flocculent type of matrixQ
Seen in Enchondroma, Chondrosarcoma
Tubular ossification pattern in benign lesions and amorphous cloud like increase in density seen in malignant lesionsQ
Seen in Osteoid osteoma, Osteosarcoma
Benign Bone Tumors
Osteoid osteoma
• Cortical lesion with a radiolucent nidusQ (< 1 cm in diameter) surrounded by dense sclerosis
• FemurQ—Most common site• In spine—Lumbar spineQ is commonest site,
usually presenting as a Ivory pedicle • Nidus shows intense vascular blushQ on
Angiography
Osteochon-droma/exostosis
• Most common benign bone tumorQ
• Bony outgrowth, continuous with adjacent cortex, covered with a cap of Hyaline cartilageQ
• Malignant degenerationQ - � Occurs in 1% � Cartilage cap > 3 cm thick
• Coat hanger exostosisQ–Large exostosis projecting away from the joint
Hereditary multiple exostosis (HME)/Diaphyseal aclasia
• Autosomal dominant• Multiple exostosis ~ 10 in numberQ
• Malignancy risk–20%Q • Bayonet hand deformityQ–Seen at wrist due to
growth retardation
Skeletal heman-gioma
• Most common benign bone tumor of spineQ
• Striated vertebra/Corduroy cloth appearanceQ–coarse vertical striations in vertebral body
• Sunburst/Spokewheel appearanceQ–Hemangioma of skull bone
• Polka dot sign: Axial CT Scan of vertebraOsteoma • Most common benign tumor of nose and
paranasal sinusesQ
• Round/Oval well defined radio-opaque lesion• Association: Gardner’s syndromeQ:
� GI polyposis � Multiple osteomasQ, Epidermal cystsQ,
Desmoid tumorsQ and Fibromatosis � Extra-intestinal manifestations precede the
colonic polyps Osteoblas-toma
• Neural arch of spineQ–Most common site• Lucent expansile lesions in neural archQ
• Thin peripheral cortical rim—no sclerosisQ
Enchon-droma
• Most common benign bone tumor of handQ
• Geographic lucent lesion in phalanges, with mild expansion
• Stippled, punctuate calcification may be seenOllier’s disease
• Multiple enchondromatosisQ • Higher rate of malignant degeneration–10%Q
Maffucci’s syndrome
• Enchondromatosis + Soft tissue cavernous hemangiomasQ
• Higher risk of malignant transformation–25%Q
Chondro-blastoma/Codman’s tumorQ
• Epiphyseal lesionQ occurring before physeal closure
• Proximal femurQ–Most common site• Chicken wire type calcificati on microscopically• Fluffy cotton woolQ like calcification on
radiographs
Sample
Pages
of R
adiol
ogy,
2/e

Bone
Tum
ors
187
Con
cept
ual R
evie
w o
f Rad
iolo
gy
Simple bone cyst/unicameral bone cyst
• Proximal humeral metaphysisQ—Most common site
• Geographic lucent defectQ
• Fallen fragment signQ—after a pathologic fracture, the fragment falls to the dependent portion
• Hinged fragment signQ—Incomplete cortical fracture
Aneurys-mal bone cyst
• 5–20 years• Eccentric, metaphyseal lucent lesion–that may
cross the physeal plate• Blown-out appearanceQ/Finger-in-the-balloon
signQ–Cortical ballooning seen in ABC• Fluid-fluid levelsQ–on MRI
Intraosse-ous lipoma
• Osteolytic lesion with well-defined/sclerotic border
• Cockade signQ/TargetQ/Doughnut shaped sequestrumQ–central radio-opacity within a calcaneal lipoma
Brodie’s Abscess versus Osteoid OsteomaQ
Distinct feature Brodie’s abscess Osteoid osteoma
Clinical history Nocturnal pain relievedQ by analgesics
Nocturnal pain NOT relievedQ by analgesics
Central radiolucency/nidus
>10 mmQ in size Usually < 10 mmQ in size
Central vascularity None–as it is liquefied abscess
Central vascular blushQ seen on angiography
Vertebral body hemangioma – giving rise to typical Striated. Corduroy cloth appearance and the Polka Dot sign
Typical cortical sclerotic lesion with a central radiolucent nidus – Osteoid osteoma
Calcaneal lipoma – Lucent lesion with a central
dense calcification – Cockade/
Target/Doughnut sequestrum sign
Mildly expansile, lytic lesion in phalanges with stippled internal calcification – Enchondroma
Eccentric, metaphyseal
lucent lesion in an Immature skeleton with
fluid-fluid levels on MRI – Aneurysmal
Bone cyst Sample
Pages
of R
adiol
ogy,
2/e

Bone
Tum
ors
188
Con
cept
ual R
evie
w o
f Rad
iolo
gy
Malignant Bone Tumors:
Metasta-sis
• Most common malignant bone tumorQ
• Breast cancerQ–most common primary in females• Prostate cancerQ—most common primary in
males overall. Also most common cause of Blastic metastasesQ
• Lung cancerQ–most common cause of lytic bone metastasis
• 99m–Tc–MDP Bone scanQ—most sensitive/Best technique for detection–appear as Hot spots
• Central/Axial skeletonQ—most commonly involved• Blow out lesionsQ—highly expansile bone
lesions. Seen in primaries form RCC/Thyroid/Lung malignancy
• Cookie bite lesionQ—cortical metastatic deposit with scalloping of cortex. Seen in Lung–Breast–Kidney cancer
• Lytic lesionsQ—permeative/Moth eaten destructive lesion
• Snowball appearanceQ—multiple blastic/radiodense lesions
• One-eyed pedicleQ/Winking owl signQ JIPMER May 2018 Pattern–Destruction of single pedicle, pedicle not seen on AP radiograph
• Blind vertebraQ—bilateral pedicle destruction• Ivory vertebraQ—densely sclerotic vertebra• Extrapleural signQ—obtuse angled opacity due to
deposit in chest wall/ribs• Sunburst lesionQ/Spiculated lesion of skull
vaultQ–seen in Neuroblastoma metastasisMultiplemyeloma
• Most common primary malignant bone tumorQ
• SpineQ—most common site• 99m–Tc–MDP Bone scanQ—appear as cold spotsQ
• Diffuse osteopenia with multiple punched out lytic lesions
• Raindrop skullQ NEET JAN 2018 PATTERN —multiple uniformly sized punched-out lytic lesions in skull
• Vertebra plana/Wrinkled vertebraQ—vertebral body collapse
• Pedicle sign of myelomaQ—as pedicles are poor in red marrow, hence are spared
• Refer to Image 38 in “Imaging sings in Radiology”• Solitary plasmacytomaQ:
� Localized plasma cell proliferation � Geographic lucent expansile lesion—soap
bubble internal architectureQ
Osteosar-coma
• 2nd most common primary malignant bone tumorQ
• 10–25 years age group—Metaphyseal locationQ
• FemurQ—most common site• Permeative/Ivory medullary lesion in metaphysisQ
with cortical disruptionQ and soft tissue extensionQ
• Sunray/Sun-burst periosteal reactionQ seen• Codman’s triangleQ—elevated periosteum–not
specific for osteosarcoma• Cumulus cloud appearanceQ—eccentric lobulated
soft tissue mass adjacent to bone• Cannonball ossifying lung metastasisQ—may be seen
Multiple diffusely scattered dense
sclerotic bone lesions – Sclerotic bone
metastases in a known case of Prostatic
carcinoma
Osteosarcoma – Irregular humeral metaphysic lesion with a wide zone
of transition, Sunray/Spiculated periosteal reaction
(yellow arrows) and Codman’s triangles
(blue arrows)
Contd…
Parosteal/ Juxta-cortical osteosar-coma
• Well differentiated osteosarcoma located on bone surfaceQ
• Presents at 30–50 years• Posterior surface of distal femur–most common site• Cleavage plane sign/String signQ–radiolucent cleft
between the mass and the underlying cortex
Second-ary osteo-sarcoma
• Seen in cases of pre-existing bone disease like: � Paget’s diseaseQ
� Polyostotic fibrous dysplasiaQ
� Hereditary multiple exostosisQ/Diaphyseal aclasiaQ
� EnchondromatosisQ/Ollier’s diseaseQ
Chondro-sarcoma
• Most common primary malignant bone tumor of hand and chestQ
• Occurs after 40 years of ageQ
• Pelvis and proximal femur–most common site • Large radiolucent ill-defined lesion with internal
popcornQ/fluffyQ/stippledQ/cotton-woolQ/rings and broken arcsQ calcification
Ewing’s sarcoma
• Diaphyseal lesion presenting at 10–25 years• FemurQ–most common site• Originates from primitive blue round cells along
with other similar tumors like PNET, Askin tumor, neuroepithelioma, medulloblastoma
• Permeative lesion in diaphysisQ with Laminated/Onion peel periosteal reactionQ
• Cortical saucerizationQ seen• Groomed/Trimmed whiskers effectQ- spiculated
periosteal reaction• Skip lesionsQ may be seen• Refer to Q. No. 44 in Image-Based Questions
Contd…
Sample
Pages
of R
adiol
ogy,
2/e








![[2016] Computed Tomography Imaging in Oncology.](https://static.fdocuments.in/doc/165x107/577c7d591a28abe0549e6f04/2016-computed-tomography-imaging-in-oncology.jpg)