
Page | 482 Abnormal CVP...
3
Page | 482 Letters to Editor Vol. 7, Issue 4, October-December 2013 Saudi Journal of Anaesthesia Abnormal CVP waveform Sir, A 52-year-old male patient was scheduled for coronary artery bypass grafting. Patient’s echocardiography findings revealed no tricuspid regurgitation or stenosis with good right ventricular function. Preoperatively central venous line was inserted through right internal jugular vein. After insertion, central venous pressure (CVP) waveform showed Access this article online Quick Response Code: Website: www.saudija.org DOI: 10.4103/1658-354X.121060 Figure 1: Abnormal CVP waveform marked with arrow Figure 2: CVP waveform after pulling central venous catheter abnormal large a-c wave complex (Figure 1 – marked with red arrow) and CVP value was in the range of 10-12 mm Hg. Such wave pattern may resemble a cannon “a” wave of CVP. [1,2] Transesophageal echocardiography was done which demonstrated lower end of central venous catheter getting abutted with tricuspid valve early in the systole. This explained the mechanism of such abnormal CVP waveform. When central venous catheter was pulled back at the insertion point, CVP waveform showed normal waves and CVP values was in the range of 4-6 mm Hg [Figure 2]. It is important to ascertain the position of central venous line before interpreting waveform. Monish S. Raut, Arun Maheshwari Department of Cardiac Anaesthesia, Sir Ganga Ram Hospital, New Delhi, India Address for correspondence: Dr. Monish S. Raut, Department of Cardiac Anaesthesia, Sir Ganga Ram Hospital, New Delhi, India. E-mail: [email protected] REFERENCES 1. Barbeito A, Mark JB. Arterial and central venous pressure monitoring. Anesthesiol Clin 2006;24:717-35. 2. Rodes A, Grounds RM, Bennett ED. Hemodynamic monitoring. In: Fink MP, Abraham E, Vincent JL, Kochanek PM, editors. Textbook of Critical Care. 5 th ed. Philadelphia, PA: Elsevier Saunders; 2005. p. 736. Bifid uvula: Anesthetist don’t take it lightly! Sir, Bifid uvula means a cleft in uvula. It is often considered as a marker for sub mucous cleft palate. Compared to the normal one, it has fewer amounts of muscular tissues. It is commonly noticed in infants and is rarely found in adult. It can cause problems in ear. Sometimes it is unable to reach the posterior pharyngeal wall during swallowing, causing [Downloaded free from http://www.saudija.org on Wednesday, March 26, 2014, IP: 197.39.229.60] || Click here to download free Android application for this journal
Transcript of Page | 482 Abnormal CVP...

Page | 482Letters to Editor
Vol. 7, Issue 4, October-December 2013 Saudi Journal of Anaesthesia
Abnormal CVP waveform
Sir,
A 52-year-old male patient was scheduled for coronary arterybypassgrafting.Patient’sechocardiographyfindingsrevealed no tricuspid regurgitation or stenosis with good right ventricular function. Preoperatively central venous line was inserted through right internal jugular vein. After insertion, central venous pressure (CVP) waveform showed
Access this article onlineQuick Response Code:
Website:
www.saudija.org
DOI:
10.4103/1658-354X.121060
Figure 1: Abnormal CVP waveform marked with arrow
Figure 2: CVP waveform after pulling central venous catheter
abnormal large a-c wave complex (Figure 1 – marked with red arrow) and CVP value was in the range of 10-12 mm Hg. Such wave pattern may resemble a cannon “a” wave of CVP.[1,2] Transesophageal echocardiography was done which demonstrated lower end of central venous catheter getting abutted with tricuspid valve early in the systole. This explained the mechanism of such abnormal CVP waveform. When central venous catheter was pulled back at the insertion point, CVP waveform showed normal waves and CVP values was in the range of 4-6 mm Hg [Figure 2]. It is important to ascertain the position of central venous line before interpreting waveform.
Monish S. Raut, Arun MaheshwariDepartment of Cardiac Anaesthesia, Sir Ganga Ram Hospital,
New Delhi, India
Address for correspondence: Dr. Monish S. Raut,
Department of Cardiac Anaesthesia, Sir Ganga Ram Hospital, New Delhi, India.
E-mail: [email protected]
ReFeRenceS
1. Barbeito a, Mark JB. arterial and central venous pressure monitoring. anesthesiol Clin 2006;24:717-35.
2. rodes a, Grounds rM, Bennett Ed. Hemodynamic monitoring. in: Fink MP, abraham E, Vincent Jl, Kochanek PM, editors. textbook of Critical Care. 5th ed. Philadelphia, Pa: Elsevier Saunders; 2005. p. 736.
Bifid uvula: Anesthetist don’t take it lightly!
Sir,
Bifiduvulameansacleftinuvula.Itisoftenconsideredas a marker for sub mucous cleft palate. Compared to the
normal one, it has fewer amounts of muscular tissues. It is commonly noticed in infants and is rarely found in adult. It can cause problems in ear. Sometimes it is unable to reach the posterior pharyngeal wall during swallowing, causing
[Downloaded free from http://www.saudija.org on Wednesday, March 26, 2014, IP: 197.39.229.60] || Click here to download free Android application for this journal
zaheer
Rectangle
Page | 483Letters to Editor
Saudi Journal of Anaesthesia Vol. 7, Issue 4, October-December 2013
regurgitation.Itmayproducevelopharyngealinsufficiencyand nasal intonation.[1] It does not cause many problems in view of airway management. It may be associated with aneurysm in different vascular bed like coronary and abdominal aortic aneurysm. We are presenting herein a case of bifiduvulawithnormalairwayanatomythatwasinitiallyposted for retinal surgery, postoperatively diagnosed as cerebral aneurysm rupture, and later underwent a clipping surgery. To the best of our knowledge, there is no report on theassociationof cerebralaneurysminbifiduvulapatientwith such a devastating complication in a 16-year-old boy. We obtained written consent from the parent of the patient to report this case.
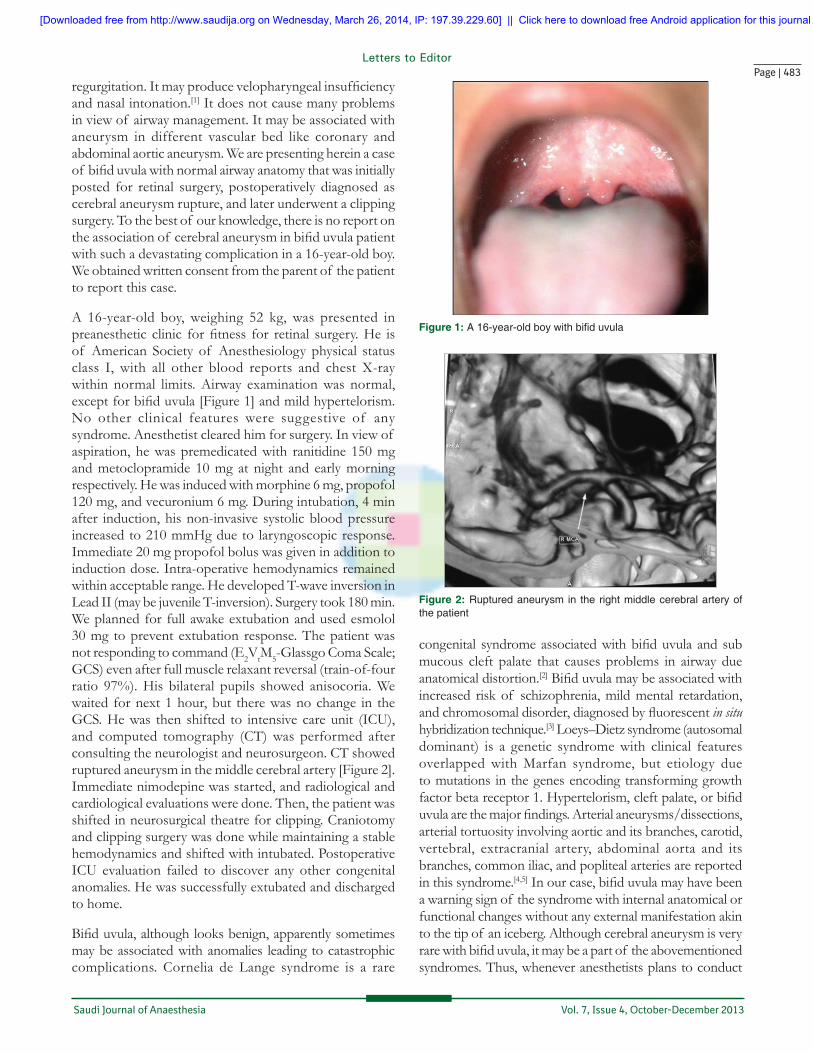
A 16-year-old boy, weighing 52 kg, was presented in preanesthetic clinic forfitness for retinal surgery.He isof American Society of Anesthesiology physical status class I, with all other blood reports and chest X-ray within normal limits. Airway examination was normal, exceptforbifiduvula[Figure1]andmildhypertelorism.No other clinical features were suggestive of any syndrome. Anesthetist cleared him for surgery. In view of aspiration, he was premedicated with ranitidine 150 mg and metoclopramide 10 mg at night and early morning respectively. He was induced with morphine 6 mg, propofol 120 mg, and vecuronium 6 mg. During intubation, 4 min after induction, his non-invasive systolic blood pressure increased to 210 mmHg due to laryngoscopic response. Immediate 20 mg propofol bolus was given in addition to induction dose. Intra-operative hemodynamics remained within acceptable range. He developed T-wave inversion in Lead II (may be juvenile T-inversion). Surgery took 180 min. We planned for full awake extubation and used esmolol 30 mg to prevent extubation response. The patient was not responding to command (E2VtM5-GlassgoComaScale;GCS) even after full muscle relaxant reversal (train-of-four ratio 97%). His bilateral pupils showed anisocoria. We waited for next 1 hour, but there was no change in the GCS. He was then shifted to intensive care unit (ICU), and computed tomography (CT) was performed after consulting the neurologist and neurosurgeon. CT showed ruptured aneurysm in the middle cerebral artery [Figure 2]. Immediate nimodepine was started, and radiological and cardiological evaluations were done. Then, the patient was shifted in neurosurgical theatre for clipping. Craniotomy and clipping surgery was done while maintaining a stable hemodynamics and shifted with intubated. Postoperative ICU evaluation failed to discover any other congenital anomalies. He was successfully extubated and discharged to home.
Bifiduvula,althoughlooksbenign,apparentlysometimesmay be associated with anomalies leading to catastrophic complications. Cornelia de Lange syndrome is a rare
congenital syndromeassociatedwithbifiduvula and submucous cleft palate that causes problems in airway due anatomical distortion.[2]Bifiduvulamaybeassociatedwithincreased risk of schizophrenia, mild mental retardation, andchromosomaldisorder,diagnosedbyfluorescent in situ hybridization technique.[3] Loeys–Dietz syndrome (autosomal dominant) is a genetic syndrome with clinical features overlapped with Marfan syndrome, but etiology due to mutations in the genes encoding transforming growth factorbetareceptor1.Hypertelorism,cleftpalate,orbifiduvulaarethemajorfindings.Arterialaneurysms/dissections,arterial tortuosity involving aortic and its branches, carotid, vertebral, extracranial artery, abdominal aorta and its branches, common iliac, and popliteal arteries are reported in this syndrome.[4,5]Inourcase,bifiduvulamayhavebeena warning sign of the syndrome with internal anatomical or functional changes without any external manifestation akin to the tip of an iceberg. Although cerebral aneurysm is very rarewithbifiduvula,itmaybeapartof theabovementionedsyndromes. Thus, whenever anesthetists plans to conduct
Figure 1: A 16‑year‑old boy with bifid uvula
Figure 2: Ruptured aneurysm in the right middle cerebral artery of the patient
[Downloaded free from http://www.saudija.org on Wednesday, March 26, 2014, IP: 197.39.229.60] || Click here to download free Android application for this journal

Page | 484Letters to Editor
Vol. 7, Issue 4, October-December 2013 Saudi Journal of Anaesthesia
significance of bifid uvula Pediatrics 1985;75:553‑61.2. Callea M, Montanari M, radovich F, Clarich G, Yavuz i.
Bifid uvula and submucous cleft palate in cornelia de lange syndrome. J int dent Med res 2011;4:74.
3. Vorstman Ja, de ranitz aG, Udink ten Cate FE, Beemer Fa, Kahn RS. A bifid uvula in a patient with schizophrenia as a sign of 22q11 deletion syndrome. Ned tijdschr Geneeskd 2002;146:2033-6.
4. loeys Bl, Schwarze U, Holm t, Callewaert Bl, thomas GH, Pannu H, et al. aneurysm syndromes caused by mutations in the tGF-beta receptor. N Engl J Med 2006;355:788-98.
5. Johnson Pt, Chen JK, loeys Bl, dietzd HC, Fishman EK. loeys-dietz Syndrome: MdCt angiography Findings. aJr am J roentgenol 2007;189:29-35.
a case with bifid uvula (even though non-syndromic), they must ask for detailed family and genetical history, clinical examination relevant investigations, and specialty consultation. Adequate preoperative preparation and, accordingly, intra-operative management can prevent unexpected complications in such patients.
Sukhen Samanta, Sujay Samanta1
Department of Critical Care Medicine, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Luckow, Uttar Pradesh,
1Department of Anaesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Chandigarh, India
Address for correspondence: Dr. Sukhen Samanta,
17, Dr. A N Paul Lane, Bally, Howrah - 711 201, West Bengal, India. Email: [email protected]
ReFeRenceS
1. Shprintzen rJ, Schwartz rH, daniller a, Hoch l. Morphologic
Access this article onlineQuick Response Code:
Website:
www.saudija.org
DOI:
10.4103/1658-354X.121061
Methanol toxicity following esmolol infusion in a post‑operative case of pheochromocytoma resection
Sir,
Esmolol is an ultra-short acting beta-adrenergic receptor blocker used in anesthesia for its cardio-selective anti-adrenergic effects.[1,2] It is known that esmolol is metabolized by plasma and red blood cell esterase to methanol in a low concentration.[1] We are reporting herein a case of inadvertent methanol toxicity following esmolol infusion in a postoperative case of pheochromocytoma. The patient’s family reviewed this report and gave written consent for publication.
A 14-year-old girl with a diagnosed case of right-sided adrenal pheochromocytoma (sporadic) was posted for open resection [Figure 1]. Preoperatively, she was of American Society of Anesthesiology physical status class II (hypertensive) on oral antihypertensive medication (prazocin 3 mg and metoprolol 50 mg, twice daily). Preoperative electrocardiogram (ECG) showed sinus tachycardia and left ventricular hypertrophy. Transthoracic echocardiography (TTE) showed hypertrophic left ventricle with 50% left ventricular ejection fraction.
Figure 1: Contrast‑enhanced computed tomography scan of abdomen of the patient showing right adrenal pheochromocytoma (arrow)
She was premedicated with previously prescribed drugs and alprazolam 0.25 mg. Under basic monitoring (ECG, non-invasive blood pressure, pulse-oximetry), thoracic epidural was placed at T10-11 level. Arterial line was
[Downloaded free from http://www.saudija.org on Wednesday, March 26, 2014, IP: 197.39.229.60] || Click here to download free Android application for this journal
zaheer
Rectangle


















