Page 1 Use of modest financial incentives to improve engagement of drug users in HIV testing and...
18
Page 1 Use of modest financial incentives to improve engagement of drug users in HIV testing and post-test follow-up: results of a randomized controlled trial Mark Hull 1 , Charles Otieno 1 , Marianne Harris 1 , Joel Singer 2 , Erin Ding 1 , Julia Zhu 1 , Thomas Kerr 1 , Evan Wood 1 , Kate Shannon 1 , Rolando Barrios 1 , Robert Hogg 1 , Nancy Petry 3 , Julio Montaner 1 1. BC Centre for Excellence in HIV/AIDS, Vancouver, BC 2. CIHR Canadian HIV Trials Network, Vancouver, BC 3. University of Connecticut Health Center, Farmington, CT, USA
-
Upload
erin-eaton -
Category
Documents
-
view
214 -
download
1
Transcript of Page 1 Use of modest financial incentives to improve engagement of drug users in HIV testing and...
Page 1
Use of modest financial incentives to improve engagement of drug users in HIV testing and post-test follow-up: results of a randomized controlled
trial Mark Hull1, Charles Otieno1, Marianne Harris1, Joel Singer2, Erin
Ding1, Julia Zhu1, Thomas Kerr1, Evan Wood1, Kate Shannon1, Rolando Barrios1, Robert Hogg1, Nancy Petry3, Julio Montaner1
1. BC Centre for Excellence in HIV/AIDS, Vancouver, BC2. CIHR Canadian HIV Trials Network, Vancouver, BC
3. University of Connecticut Health Center, Farmington, CT, USA

Page 2
Background• A significant proportion of HIV+ individuals
(~25% in BC1) are not linked to medical care– Either have not been tested for HIV, or if HIV+
have not been assessed for ART eligibility• Interventions to improve HIV testing rates
among at-risk populations are required to strengthen the HIV care cascade
1. Montaner et al., CROI 2013, #1029

Page 3
Background• Conditional cash transfers (Incentives) have been
used successfully to improve goal-related activities amongst IDU populations– Improved rates of completion of TB screening processes
Chaisson, R et al. JAIDS 1996;11:455 , Perlman, D et al J. Urban Health 2003;80:428.– Completion of hepatitis B vaccine series
• Randomized trial of monetary incentive vs. outreach nurses, 69% vs. 23% completion. Seal, K et al. Drug and Alcohol Depend 2003; 71:127.
• Use of incentives for completion of HIV screening has been shown to increase return rates amongst participants in an ED-based program Haukoos, J. Acad Emerg Med 2005;7:617.
Page 4
Objective
• To evaluate the efficacy of offering a modest financial incentive linked to HIV testing and post-test counseling in a substance-using population– To evaluate the efficacy of incentives in assessing
ART-eligibility amongst HIV+ individuals not currently engaged in care
Page 5
MethodsEntry criteria:• Inclusion
– Age >19 years– At risk for HIV, or HIV+ by self-report with no recent evaluation of
HIV status (CD4 cell count or HIV VL)– Reside in Vancouver– Report drug use at least once in the past 3 months
• alcohol, heroin, cocaine, cocaine/heroin combinations, methamphetamines, injectable morphine and codeine, but excluding isolated marijuana use
• Exclusion– Known HIV with use of antiretrovirals in the past 12 months

Page 6
Sample Population
N=301
Control Arm
Incentives Arm
Standard of care counseling and HIV testing plus financial incentive
Randomized 1:1
Standard of care counseling and HIV testing without financial incentive
Study Design
Visit 1(Laboratory
Testing)
Visit 2(Results)
Timeline of follow-up
Incentives
$10 – Laboratory testing
$15 – Returning for results and post-test counseling
within 4 weeks
Participants recruited between February and August 2012
Page 7
• The protocol and informed consent form were approved by the UBC/Providence Health Care Research Ethics Board
•The study is supported by the National Institute on Drug Abuse and the CIHR Canadian HIV Trials Network
–registered on ClinicalTrials.gov (NCT01526421)

Page 8
Statistical analysis• Chi-square test or Fisher’s exact test were used for
analysis of categorical variables• Wilcoxon rank-sum test was used for continuous
variables• A multivariate logistic regression model considering
possible confounders was used to estimate the probability of completing testing and returning for test results, with the variable of interest being receipt of incentives

Page 9
Baseline DemographicsVariable Control Group
(N=150)Incentive Group
(N=151)p value
Median age (IQR), years 43 (36-50) 45 (36-51) 0.604
Male gender, N (%) 103 (68.7%) 98 (64.9%) 0.488
Ethnic group, N (%)CaucasianAboriginalBlackAsianHispanic/Latino Other
82 (54.7%)58 (38.7%)
4 (2.7%)1 (0.7%)0 (0%)
2 (3.3%)
85 (56.3%)62 (41.1%)
3 (2.0%)0 (0%)
1 (0.7%)0 (0%)
0.628
Housing , N (%)HomelessUnstable (SRO)
23 (15.3%)60 (40.0%)
32 (21.2%)90 (59.6%)
0.983
IQR, Interquartile rangeSRO, Single-room occupancy hotel
Page 10
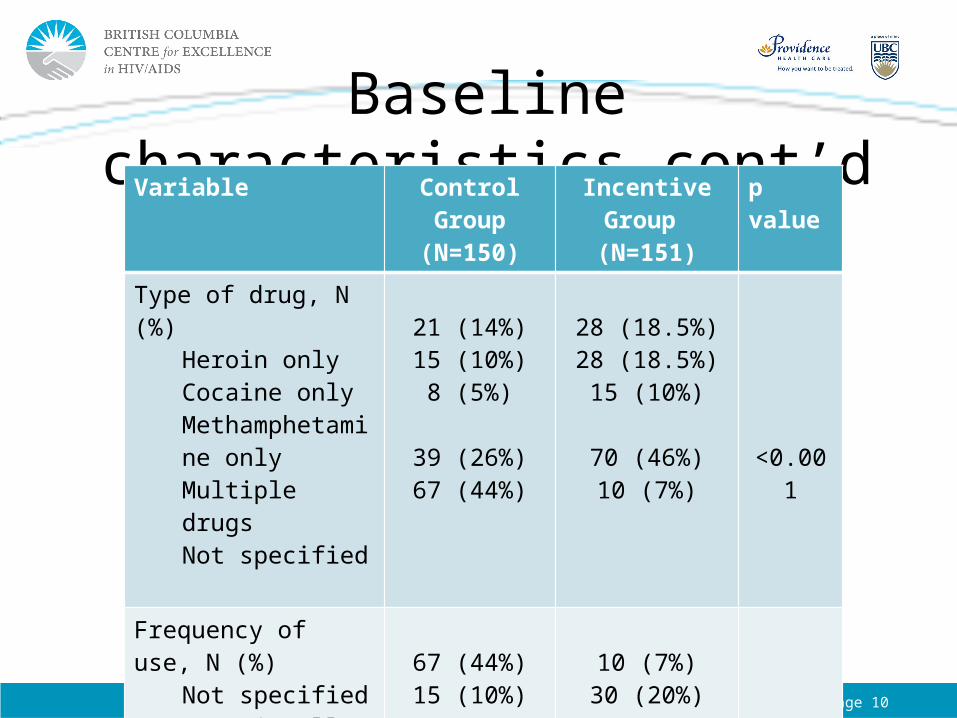
Baseline characteristics cont’dVariable Control Group
(N=150)Incentive Group
(N=151)p value
Type of drug, N (%)Heroin onlyCocaine onlyMethamphetamine onlyMultiple drugsNot specified
21 (14%)15 (10%)
8 (5%)
39 (26%)67 (44%)
28 (18.5%)28 (18.5%)15 (10%)
70 (46%)10 (7%)
<0.001
Frequency of use, N (%)Not specifiedOccasionallyRegularlyDaily
67 (44%)15 (10%)23 (15%)45 (30%)
10 (7%)30 (20%)43 (28%)68 (45%)

Page 11
HIV Testing and post-test counseling
P<0.001 P<0.001

Page 12
Factors associated with HIV Screening completion
Variable Odds Ratio (95% CI) p value
Randomized study armControl armIncentives arm
1.0031.83 (15.63, 64.80)
<0.001
Adjusted for age, gender, ethnicity, housing and frequency of drug useCI, Confidence interval

Page 13
HIV eligibility screening among known HIV+ cases
Variable Control Group (N=17) Incentive Group (N=13) p value
Completed lab testingN (%)
9 (52.9%) 13 (100%) 0.004
Returned for post-test counselingN (%)
5 (29.4%) 12 (92.3%) 0.001
CD4 count (cells/mm3) Median (IQR)
440 (290-680) 315(120-535) 0.881
HIV RNA (copies/mL) Median (IQR)
19,175 (1,353-34,972) 19,657 (239-48,458) 0.170

Page 14
Hepatitis C Screening• 122 individuals were found to be HCV
Antibody positive– 98 in incentives arm (64% tested), 24 in control
arm (50% tested) p. 0.06
• Of 122 individuals, only 71 (58%) had self-reported known HCV+ status at study entry

Page 15
Limitations
• Single centre study• Relatively circumscribed drug-using
population in the DTES neighbourhood of Vancouver– No new HIV cases identified
• Drug use patterns missing for subjects, notably in the control arm

Page 16
Future Directions
• Phase 2 of this study is underway to examine the effect of incentives on increasing engagement and retention in ART programs– Evaluation of incentive-linked testing in a non-
randomized fashion– Incentives linked to clinic visits and achieving
undetectable plasma viral load

Page 17
Conclusion
• The use of modest financial incentives increased rates of HIV testing and post-test follow-up among drug users
• Significantly more individuals with known HIV but no engagement in care completed laboratory studies to evaluate ART eligibility
• Incentive-linked testing may be a strategy for engaging hard-to-reach populations such as drug users in HIV testing interventions as a component of “Treatment as Prevention” programs– Cost-effectiveness of this incentives strategy must still be
determined

Page 18
Acknowledgement
We would like to thank all participants and study personnel
This study was funded by National Institutes of Health – National Institute on Drug Abuse